Back to Journals » Orthopedic Research and Reviews » Volume 13
Utilization of Tranexamic Acid in Surgical Orthopaedic Practice: Indications and Current Considerations
Authors Haratian A ![]() , Shelby T, Hasan LK
, Shelby T, Hasan LK ![]() , Bolia IK
, Bolia IK ![]() , Weber AE, Petrigliano FA
, Weber AE, Petrigliano FA ![]()
Received 13 July 2021
Accepted for publication 5 October 2021
Published 19 October 2021 Volume 2021:13 Pages 187—199
DOI https://doi.org/10.2147/ORR.S321881
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Clark Hung
Aryan Haratian, Tara Shelby, Laith K Hasan, Ioanna K Bolia, Alexander E Weber, Frank A Petrigliano
USC Epstein Family Center for Sports Medicine at Keck Medicine of USC, Los Angeles, CA, USA
Correspondence: Frank A Petrigliano
USC Epstein Family Center for Sports Medicine at Keck Medicine of USC, Los Angeles, CA, USA
Tel +1 323 442-5822
Email [email protected]
Abstract: Tranexamic acid (TXA) is a lysine analog that exhibits an anti-fibrinolytic effect by directly preventing the activation of plasminogen as well as inhibiting activated plasmin from degrading fibrin clots, thereby promoting hemostasis and reducing the duration and quantity of blood loss. The aims of this study were to summarize the indications, routes of administration, safety, and clinical outcomes of TXA use throughout the different subspecialities in orthopedic surgery. Given that orthopedic procedures such as TKA, THA, fracture fixation, and various spine surgeries involve significant intraoperative blood loss, TXA is indicated in providing effective perioperative hemostasis. Additionally, use of TXA in orthopedic trauma has been indicated as a measure to reduce blood loss especially in a group with potential for hemodynamic compromise. TXA has been implicated in reducing the risk of blood transfusions in orthopedic trauma, joint surgery, and spine surgery, although this effect is not seen as prominently in sports medicine procedures. There remains disagreement in literature as to whether TXA via any route of administration can improve other clinically significant outcomes such as hospital length of stay and total operative time. Procedures that rely extensively on clarity on visualization of the surgical field such as knee and shoulder arthroscopies can greatly benefit from the use of TXA, thereby leading to less intraoperative bleeding, with better visual clarity of the surgical field. While most studies agree thrombosis due to TXA is unlikely, new research in cells and animal models are evaluating whether TXA can negatively impact other aspects of musculoskeletal physiology, however with conflicting results thus far. As of now, TXA remains a safe and effective means of promoting hemostasis and reducing intraoperative blood loss in orthopedic surgery.
Keywords: tranexamic acid, TXA, orthopaedic surgery, operative blood loss, transfusion rate, outcomes
Introduction
Tranexamic acid (TXA) is a lysine analog that exhibits an anti-fibrinolytic effect by directly preventing the activation of plasminogen as well as inhibiting activated plasmin from degrading fibrin clots.1 These properties of TXA promote hemostasis and thereby can reduce the duration and quantity of blood loss.1,2 As such, TXA has been listed on the World Health Organization’s (WHO) List of Essential Medicines and has been utilized in various fields of medicine including Obstetrics, General Surgery, and Orthopedic Surgery.3–7 Given the nature of surgical procedures, with the need to maximize hemostasis for patient stability as well as for adequate visualization of the surgical field, the use of adjunctive TXA perioperatively has become more widely implemented in recent years. The CRASH-2 trial was the first large scale randomized controlled trial (RCT) that evaluated the use of TXA in over 20,000 trauma patients.8 A similar study explored the use of intravenous TXA in military personnel with combat injuries (MATTERs study) and noted that those receiving TXA had lower mortality particularly in patients that necessitated large quantities of blood transfusions.9 The promising results from these studies have prompted greater utilization of the drug and stimulated further investigations to better elucidate the role of TXA in surgical practice.
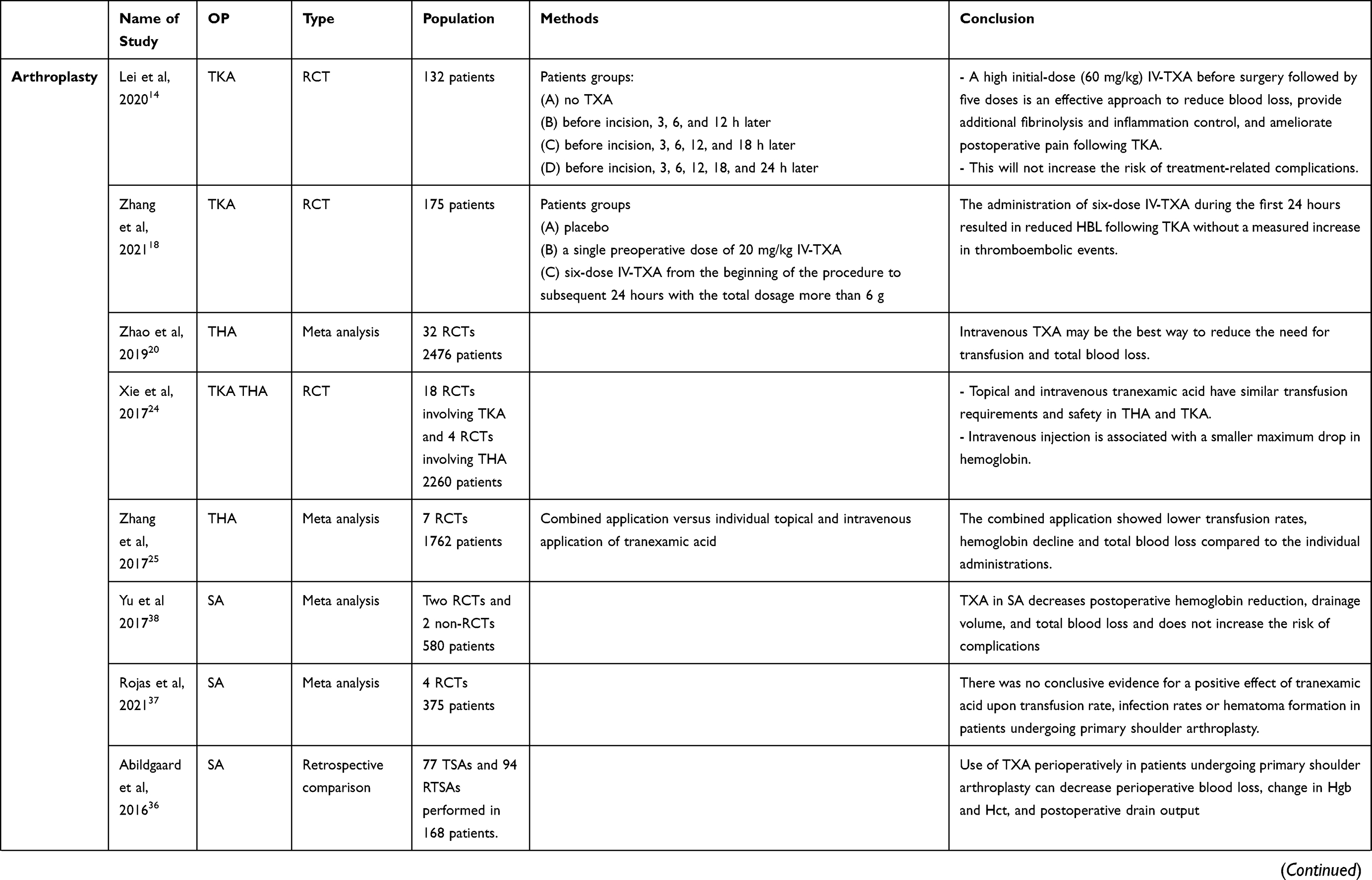
Multiple routes of TXA administration have been described in current surgical practice including intravenous (IV) most commonly; however, topical and intra-articular (IA) administration in the case of joint surgery have also described. Various dosing regimens have also been used including bolus vs continuous, and single vs multiple doses, as well as variations in the timing of dose administration in the preoperative, intraoperative, or postoperative period. This review intends to summarize current evidence on the use of TXA in surgical orthopedic practice, evaluating indications, routes of administration, safety, and patient outcomes. The results of our review are summarized in Table 1.
 |
 |
 |
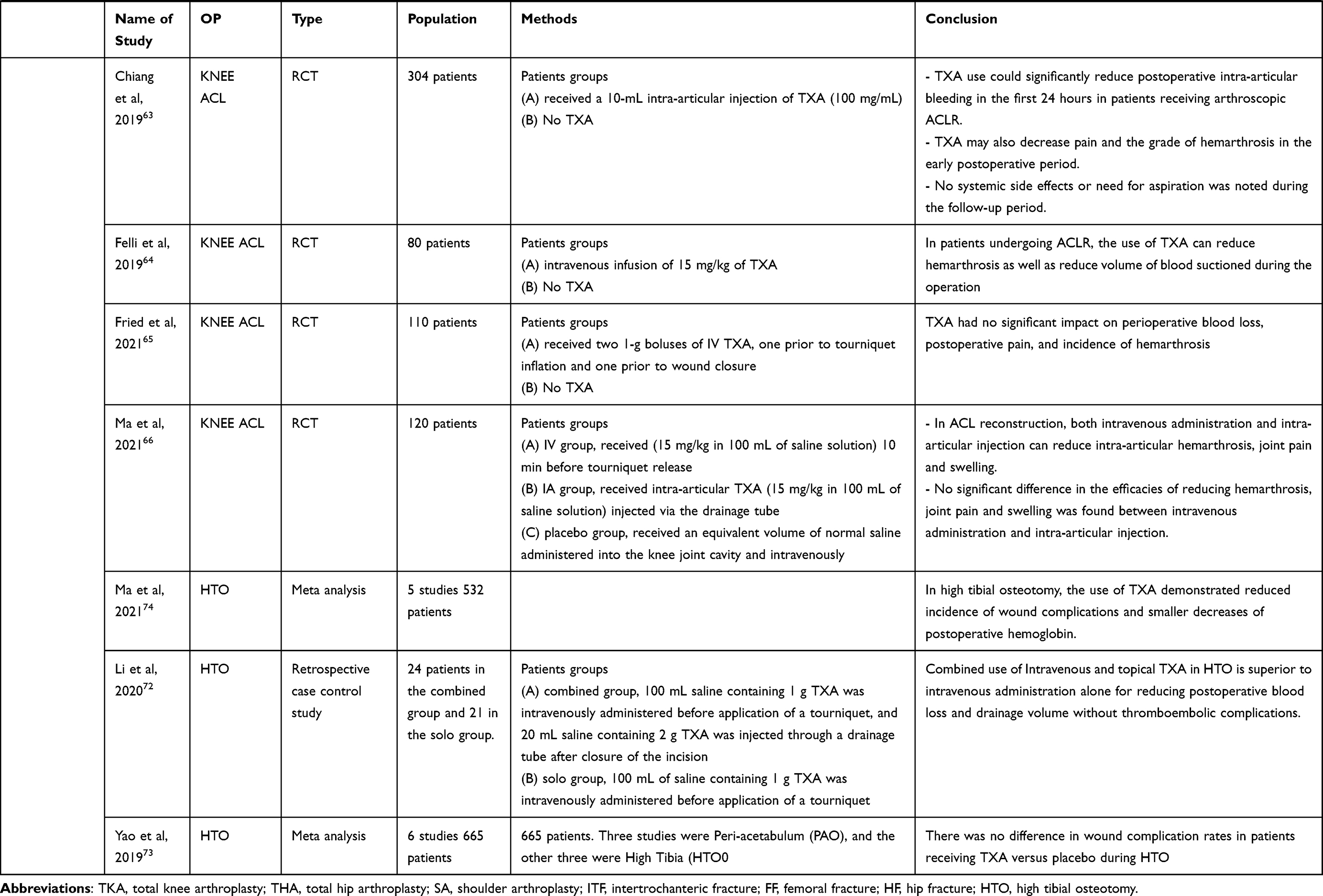 |
Table 1 Summary of Current Evidence on Use of TXA in Orthopedic Surgery |
Joint Replacement Surgery
Hip and Knee Arthroplasty
Outside of General Surgery, the use of TXA has been well documented in Orthopedic Surgery, most predominantly in total hip arthroplasty (THA) and total knee arthroplasty (TKA). Both procedures are linked to substantial blood loss, influencing procedure outcomes such as hospital stay length and the need for costly allogenic blood transfusions that can lead to both transfusion reactions and secondary infections further putting strain on hospital resources as well as the cost of patient care.10−13 Various routes of TXA administration in arthroplasty have been discussed in literature, with the most prominent being intravenous (IV), topical, and oral.
While optimal route of delivery remains controversial, IV remains the most common route of TXA administration. Various regimens of IV dosages and timings have been offered, with studies showing multiple administrations to be more effective than a single dose.14–17 Lei et al in a RCT of 132 patients undergoing TKA demonstrated a reduction in blood loss, postoperative pain, and markers of inflammation such as C-Reactive Protein (CRP) and interleukin-6 (IL-6) using a relatively high dosage bolus of 60 mg/kg preoperatively, followed by five subsequent administrations of TXA intraoperatively.15 Zhang et al conducted a RCT of 175 TKA patients receiving a total of six doses of IV TXA also demonstrated decreased hidden blood loss all without a significant increase in incidence of thromboembolic events as compared to the placebo and single-dose TXA groups.18
Several studies and meta-analyses have shown that IV and topical use have similar safety and efficacy during both TKA and THA.12,19,20 A meta-analysis of 32 randomized control trials conducted by Zhao et al showed IV TXA use in THA as superior in decreasing transfusion need and topical TXA as superior in reducing total blood loss.20 A direct comparison resulted in no significant differences between the two deliveries, which is consistent with previous meta-analyses in delivery of TXA in THA procedures.20–22 The authors recognized short follow-up times of the RCTs potentially confounded the number of postoperative complications. Alternatively, while Wei et al also found the two delivery methods to show no significant differences in blood loss or postoperative differences in thromboembolic events in TKA, the topical group showed a significantly lower pain score than the IV group which the authors believe warrant further investigation.12 These results were further validated in a study by Laoruengthana et al that demonstrated a reduction in postoperative morphine requirement as well as subjective visual analog scale (VAS) pain scores after the use of IA TXA intraoperatively with the proposed mechanism of pain reduction speculated to be a decrease in postoperative inflammation and surgical site swelling.23 A meta-analysis conducted by Xie et al of 18 RCTs of TXA on TKA and THA found IV to be associated with smaller decreases in hemoglobin before and after subgroup analysis.24
Other routes of administration, such as combined and oral, are gaining prominence. Combined administration of topical and IV have been shown to not only match but possibly exceed the efficacy of the administration individually.25–27 Zhang et al conducted a meta-analysis of seven studies showed lower transfusion rates, hemoglobin decline and total blood loss in the combined group compared to the individual administrations.25 Authors cite the need for higher quality RCTs to support recommendations of combined delivery.
Multiple studies have also cited the clinical efficacy (lower total blood loss, transfusion rates, limited thromboembolic events, and positive clinical outcomes) for oral administration compared to no-TXA use for both TKA and THA.28–32 In addition, comparisons have been made directly to intravenous administration.30,33 Han et al and Chen et al found similar outcomes when conducting meta-analyses comparing oral to IV administration in both THA and TKA patients, with.33,34 There were no significant differences in total blood loss, Hb loss, DVT rate, and total blood loss.33,34 These findings are promising as the oral TXA dosage is a cheaper option, costing 70–90% less than the equivalent IV dose, however further research is needed given the relatively low frequency of oral TXA use.35
Shoulder Arthroplasty
In addition to hip and knee arthroplasty, a few studies have explored the use of TXA in shoulder arthroplasty.36–38 Patients receiving shoulder arthroplasty are susceptible to large quantities of blood loss, with one study estimating a blood transfusion rate of over 7% postoperatively, and thus supplemental TXA is viewed as an attractive option for support of intraoperative hemostasis.39 An early retrospective study reported on the outcomes of patients given IV TXA during total shoulder arthroplasty (TSA) and reverse total shoulder arthroplasty (rTSA) and reported a reduction of total blood loss and total drop in hemoglobin in patients given TXA.36 A meta-analysis of 4 studies evaluating TXA use in shoulder arthroplasty found that TXA reduced total blood loss and hemoglobin reduction postoperative, with no increased risk of complications.38 However, the authors also noted that TXA did not reduce the risk of blood transfusions, operation time, or hospital length of stay.38 A more recent meta-analysis supported this claim and emphasized the lack of reduction in the risk of blood transfusions among patients receiving TXA for shoulder arthroplasty.37 Both studies, however, were limited by the relatively low number of primary studies included and may have been potentially underpowered in detecting a significant difference in blood transfusion rates in those receiving TXA versus placebo.37,38 This further stresses the need for larger investigations to better elucidate whether TXA improves clinical outcomes such as risk of blood transfusions, wound infections, pain, and hematoma formation after shoulder arthroplasty.
Orthopedic Trauma
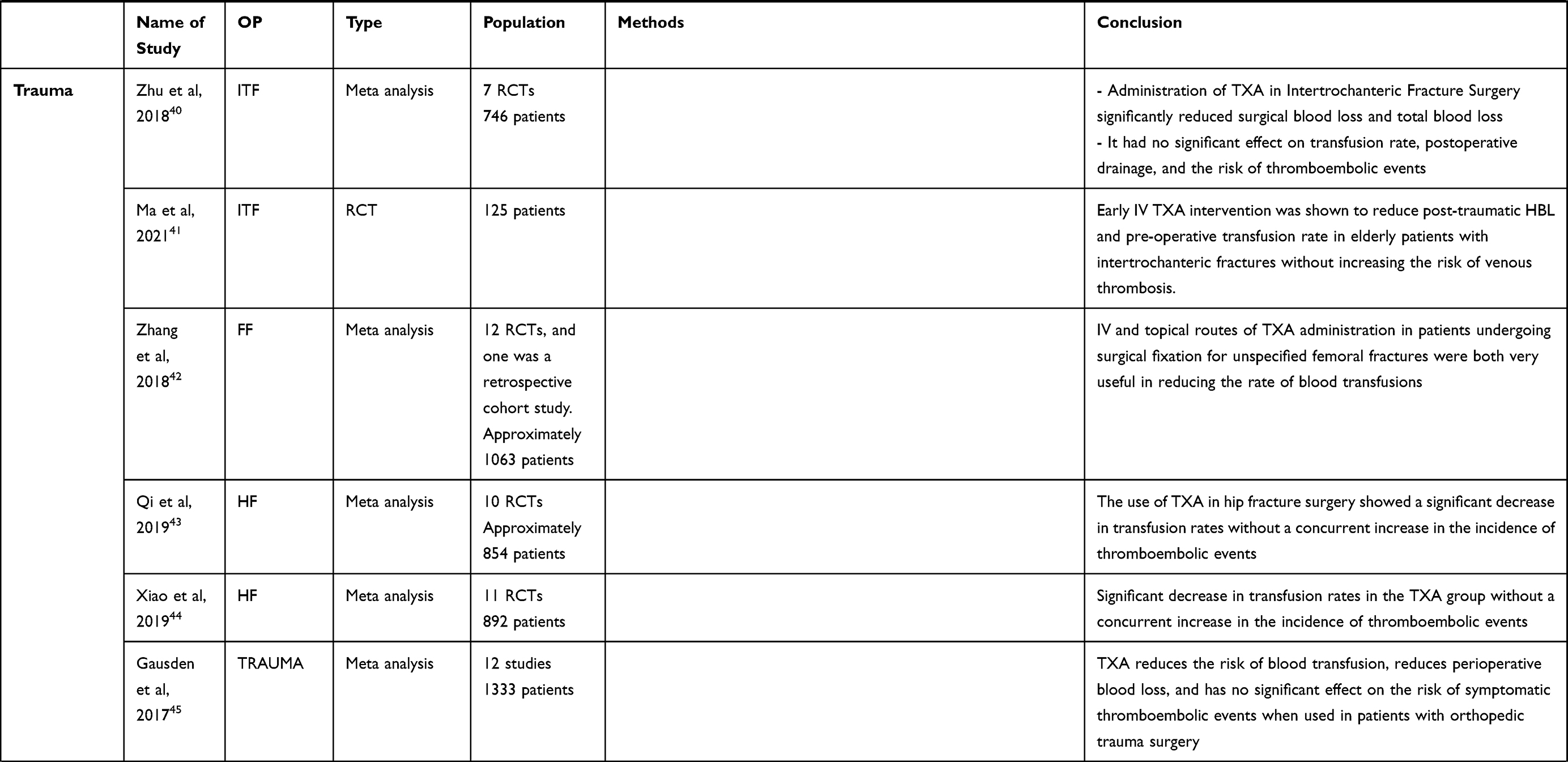
Orthopedic trauma patients, particularly those with multiple open fractures and significant blood loss preoperatively, are predisposed to hypotension, anemia, and often are at risk of necessitating one or more blood transfusions.4 Given these constellation of risk factors, additional intraoperative blood loss during surgical fixation of fractures can potentially exacerbate the deficit and increase the likelihood of further patient complications, thus highlighting the need for effective intraoperative hemostasis. For these reasons, multiple studies have explored the use of supplemental TXA to provide promote hemostasis in orthopedic trauma surgery.40–45 One such meta-analysis by Zhu et al aggregated data from 7 RCTs with a total of 746 patients who received either TXA (through either intravenous or intramuscular routes of administration), or placebo while undergoing operative fixation for an intertrochanteric fracture.40 Patients receiving TXA had reduced blood loss during the operation and higher average hemoglobin levels, all without increased risk of thromboembolic events.40 While some studies included in the meta-analysis demonstrated decreased risk of blood transfusion, the analysis overall concluded that TXA did not reduce the risk of a needing a transfusion.40 These results contrasted with a meta-analysis of 13 RCTs consisting of either IV or topical routes of TXA administration in patients undergoing surgical fixation for unspecified femoral fractures which concluded that while those receiving IV TXA exhibited a significant reduction in postoperative transfusion, patients receiving topical TXA had no significant reduction in transfusion rates and postoperative hemoglobin levels.42 A different study of 125 elderly patients with intertrochanteric fractures who received 1g of IV TXA instead reported on the degree of hidden posttraumatic blood loss and preoperative transfusion rates. The significant reduction in hidden blood loss, as determined by hemoglobin levels, as well as the reduction in preoperative transfusions in the TXA group highlights the potential of the drug in improving patient stability and reducing the likelihood of complications associated with acute trauma.41 Two more meta-analyses reported on patients receiving TXA while undergoing surgical fixation for unspecified hip fractures, and both noted a significant decrease in transfusion rates in the TXA group without a concurrent increase in the incidence of thromboembolic events.43,44 A meta-analysis by Gausden et al included studies with a variety of orthopedic trauma pathologies including femoral neck, hip, intertrochanteric, calcaneal, acetabular, and femoral shaft fractures.45 Studies consisted of those giving purely IV TXA, purely topical TXA, or a combination of IV and topical, and patients given TXA in any form had a significantly decreased blood loss and risk of blood transfusion without increased risk of thromboembolic events relative to controls.45
Spine Surgery
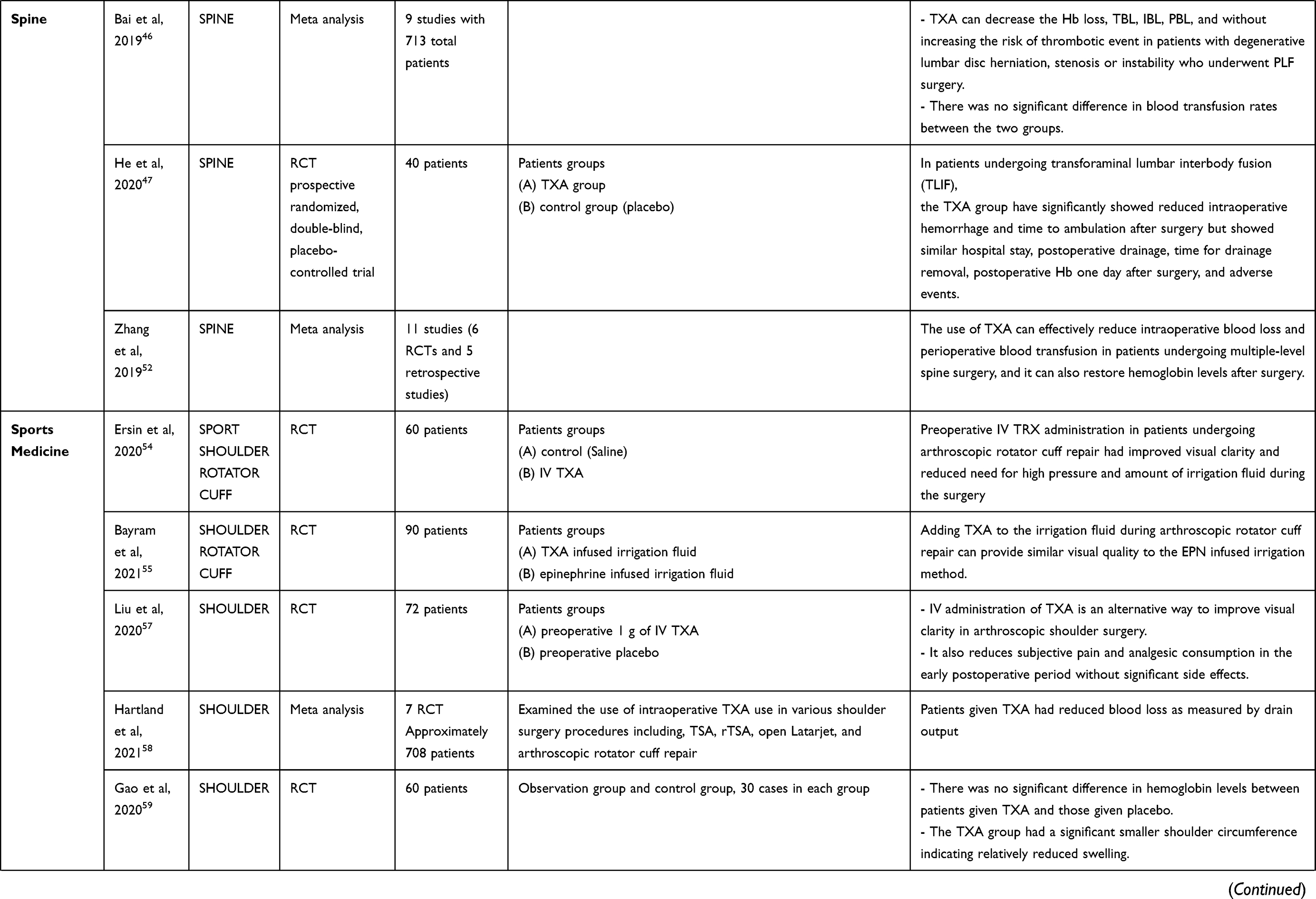
Surgical procedures involving the spine have a high propensity to cause significant blood loss leading to both the increased risk of intraoperative and postoperative patient hypotension and anemia necessitating a blood transfusion, as well as the potential for significant loss of surgical field visibility thereby prolonging and complicating procedures. To this end, multiple studies have assessed the benefit of TXA for various procedures in spine surgery.46–53 A meta-analysis consisting of 9 studies with 713 total patients examined the use of TXA in patients undergoing posterior lumbar fusion (PLF).46 Those receiving TXA had a significant decrease in intraoperative and postoperative blood loss, and hemoglobin decline, without any increased risk of thromboembolic events. However, it is important to note that there were no significant differences between the rates of transfusions in those given TXA versus controls. A more recent randomized controlled trial specifically examined the outcomes in patients undergoing transforaminal lumbar interbody fusion (TLIF) treated with both an IV bolus of TXA preoperatively, followed by a continuous infusion of 6–8 mg/kg/hr intraoperatively up to a maximum allotted dose of 15 mg/kg.47 Patients given TXA had less intraoperative blood loss and were able to resume ambulation quicker than the control group. However, the authors noted that there were no significant differences in terms of hospital length of stay, hemoglobin levels, and volume of postoperative drainage.47 Postoperative complications were similar between the two groups as well. Even in more complex, multi-level spine procedures that are especially associated with significant blood loss and can often require blood transfusions, TXA can significantly reduce blood loss and the risk of transfusions in patients undergoing these procedures.52,53 More recent meta-analyses have aggregated RCTs, most prominently those giving IV TXA, in patients undergoing some form of spine surgery, and have further demonstrated that TXA can reduce the risk of blood transfusions in a dose-dependent manner without significantly increasing thrombosis in any circumstance.48,51 However, these results were not observed in a similar meta-analysis including only studies where TXA was given topically, potentially indicating that the route of TXA administration can play a role in the drug’s effectiveness in reducing the risk of transfusions, which contrasts with similar studies in joint surgery.20–22,49
Orthopedic Sports Medicine
Shoulder, Knee, and Hip Arthroscopy
Continuous and adequate visualization of the surgical field is a necessity for efficiently conducting many Sports Medicine operations such as shoulder, knee, and hip arthroscopy, as excessive bleeding can prolong and complicate procedures. TXA has been utilized via both intra-articular (IA) and IV routes of administration in shoulder surgery to promote hemostasis. A randomized controlled trial by Ersin et al involved 60 patients undergoing arthroscopic rotator cuff repair who were given either a bolus of IV TXA or saline, with attending surgeons rating the visual clarity of the field on a scale of 1–10 at the end of the procedure.54 Those given intravenous TXA had significantly higher visual clarity scores and required lower volumes of high-pressure irrigation as compared to those given saline.54 Another study did a comparison of TXA versus epinephrine infused irrigation fluid on visual clarity during arthroscopic rotator cuff repair.55 Visual clarity was quantified using a VAS given to the operating surgeon, and no significant differences were noted between the TXA and epinephrine groups in VAS scores.55,56 Liu et al conducted a randomized controlled trial involving a total of 72 patients who were received either 1 g of IV TXA or placebo preoperatively.57 Visual clarity was measured through a Numeric Rating Scale given to the operating surgeon that ranged from 1 to 3 (poor-clear) every 15 minutes during the procedure and patient pain was quantified through subjective pain scores and postoperative analgesic consumption measured in morphine equivalents.57 The authors noted a significantly higher visual clarity score as measured by percent of grade 3 scores and lower postoperative analgesic use, however there was no significant difference in degree of shoulder swelling, operative time, and perioperative blood loss.57 A meta-analysis conducted by Hartland et al included a total of 7 studies with examined the use of intraoperative TXA use in various shoulder surgery procedures including, TSA, rTSA, open Latarjet, and arthroscopic rotator cuff repair, and concluded that patients given TXA had reduced blood loss as measured by drain output.58 However, there was no significant change in hemoglobin levels between those treated with TXA and those without.58 Another study in shoulder arthroscopy had similar findings indicating no significant difference in hemoglobin levels between patients given TXA and those given placebo, however the TXA group had a significantly smaller shoulder circumference indicating relatively reduced swelling.59 Similar results were seen in patients given IV TXA while undergoing knee arthroscopy leading to decreased knee swelling and pain as well as quicker return to functionality.60,61 Patients undergoing hip arthroscopy for treatment of femoroacetabular impingement who were given TXA had decreased total blood loss, but no differences were noted in postoperative pain and operation time.62 The effect of TXA on total blood loss and hemoglobin is less appreciated and pronounced in arthroscopy, as evidenced by the mixed results in studies, however it is possible that this might be due to the nature of arthroscopic procedures, which generally have much less blood loss on average as compared to trauma and spine procedures. That said, all studies reviewed agreed that TXA vastly improved surgical field clarity in arthroscopic procedures. Future research should also explore the link between postoperative complications due to hematoma and overall pain scores as decreased hematoma formation through the use of TXA may influence pain.
Knee Surgery
The use of TXA has been documented in patients undergoing anterior cruciate ligament reconstruction (ACLR), with studies seeking to compare both intravenous and IA routes of administration.63–69 Chiang et al carried out a RCT evaluating IA administration of TXA in patients undergoing arthroscopic ACLR.63 Postoperative bleeding was significantly reduced in the TXA group thereby decreasing the grade of hemarthrosis, and patients in the TXA group reported decreased pain.63 A different study utilized an IV route of TXA administration in patients undergoing ACLR and noted reduced hemarthrosis as well as reduced volume of blood suctioned during the operation.64 The patients who received intravenous TXA had better range of motion (ROM) and quadriceps strength postoperatively.64 However, a more recent study by Fried et al examining use of IV TXA in patients receiving ACLR concluded that TXA had no significant impact on perioperative blood loss, postoperative pain, and incidence of hemarthrosis.65 Furthermore, these two studies further disagreed on whether IV TXA improves ROM or quadriceps reactivation.64,65 A recent RCT directly compared the efficacy of IV versus IA TXA in ACLR and concluded that both routes were equally effective in terms of reducing hemarthrosis, knee swelling, and knee pain.66 These results are further backed by other studies that have consistently reported decreased postoperative blood loss, decreased incidence of knee aspiration postoperatively, as well as improved pain scores with administration of TXA during ACLR.67–69 Similar to ACLR, high tibial osteotomies (HTO) carry a risk of hemorrhage given the necessity to expose cancellous bone during the procedure.70–72 In addition to risk of anemia necessitating blood transfusions, the resulting hemorrhage can potentially lead to the creation of hematomas and thereby delaying postoperative healing.70,72 In an effort to avoid these complications, TXA has been utilized both preoperatively and intraoperatively in patients receiving HTO.72–75 While all studies reported decreased operative blood loss without increased incidence of thromboembolic events in patients receiving TXA, they also agreed that the use of TXA was not associated with a decreased risk of blood transfusion.72–75 The most recent of these studies, a meta-analysis by Ma et al, also demonstrated reduced incidence of wound complications and smaller decreases of postoperative hemoglobin in patients receiving TXA, however these results contrasted from an earlier meta-analysis by Yao et al that indicated no difference in wound complication rates in patients receiving TXA versus placebo during HTO.73,74 This observed contrast in results highlights the need for larger and more robust studies to evaluate the true impact of TXA in patient outcomes in sports medicine procedures such as ACLR and HTO.
Dosage and Optimal Timing of TXA Administration
Previous studies have explored differences in dosages and optimal timing of TXA administration in the perioperative period. A large multicenter RCT reported on multiple different dosing regimens for TXA in patients receiving THA including (1) single 1 g IV TXA given prior to incision, (2) 1 g IV TXA given both prior to incision and after wound closure, (3) 1 g of IV TXA preoperatively, followed by 1 g of intraoperative topical TXA, and (4) 3 doses of oral TXA with a total dose of 1.95g given.76 All regimens were noted to be equivalent in regard to transfusion rates, postoperative hemoglobin reduction, and complication rates implying a similar hemostatic effect among the different routes of administration.76 A prospective cohort study by Balachandar and Abuzakuk explored the use of preoperative versus intraoperative single dose of IV TXA in patients undergoing bilateral TKA and noted that while patients in the intraoperative group had a significantly lesser decrease in hemoglobin on the first day postoperatively, no significant difference was appreciated with respect to transfusion rates and drain blood loss volume.77
Risk of Thrombosis and Contraindications of TXA
Although TXA promotes coagulation, nearly all studies agree that there are no appreciable adverse effects in terms of pathological coagulation.12,18,40–53,63–69 This finding has been consistent with all routes of TXA administration including IV, topical/intra-articular, oral, and even in cases where patients were given TXA through more than one route.20–22,25–27,63–69 The most frequently described contraindications to TXA administration include patients with histories of allergic reactions to TXA, seizures, and patients with immediate acute renal failure and chronic kidney disease.78 Although most studies have shown no increased risk of thromboembolic events with administration of TXA, patient history of venous or arterial thrombosis continues to remain a contraindication.78 A large-scale meta-analysis of 9067 patients involving a variety of orthopedic procedures including THA, TKA, and those involving the lower extremity showed no significant difference in incidence of thromboembolic events when compared across all orthopedic surgical procedures included, and when analyzed by individual procedure further substantiating the claim that clinical use of TXA is not associated with an increased risk of thrombosis.79 However, a retrospective study by Myers et al conducted in a single Level I trauma center retrospective study noted threefold increased odds of venous thromboembolism in patients receiving without any benefit in survival.80 While this study was not specifically done on patients necessitating orthopedic surgery, the contraindication displayed in the results relative to studies included in this review for orthopedic trauma surgery indicates the need for larger and more robust studies with longer follow-up times to better assess the safety of TXA in this patient group.
Other Safety Considerations and Recent Avenues in Research
While TXA is frequently implemented in current orthopedic practice and is generally considered safe, recent animal studies have yielded conflicting results regarding other previously unconsidered potential side effects from this drug. An in vitro study indicated increased cell death when human periarticular tissue was exposed to TXA at concentration of 100 mg/mL after an hour of exposure, however, there remains a question of how well these results translate to a single administration of TXA perioperatively.81 Another in vitro study supported this conclusion and indicated that TXA has dose-dependent cytotoxicity to chondrocytes, with exposure to TXA above a dose of 20 mg/mL resulting in morphological changes promoting chondrocyte cell death.82 However, a similar study involving in vitro assessment of clinical concentrations of TXA on osteochondral explants from an animal model concluded that there was no measurable cytotoxicity from the agent, although it is important to note that the highest concentration of TXA used in this study was 4 mg/mL.83 An in vivo study using a rat model indicated poorer tendon healing when TXA was administered compared to placebo, although another similar study indicated that local and systemic TXA administration had no effect on healing of the Achilles tendon in rats.84,85 Another study has examined whether TXA affects the rate of bone healing after fracture fixation in animal models and concluded that both IV and topical TXA exhibited no effect on fracture healing based on evaluation of imaging obtained 2–3 weeks postoperatively.86 Given the mixed results and the implications that these potential musculoskeletal side effects can carry in the practice of orthopedic surgery, more studies, especially those in humans, are needed to clarify these results.
Most studies exploring the safety of TXA clinically often exclude high-risk patients prior to randomization, which in turn limits the generalizability of TXA to all orthopedic patients. Two studies have examined the use of TXA patients in high-risk patients. Porter et al conducted an institutional retrospective analysis of 38220 patients including 8877 that were classified as high risk for thrombotic complications based on their comorbidities that underwent TKA or THA and received TXA.87 The authors reported no significant differences in both the odds of adverse outcomes and rates of thromboembolic complications between high and low risk patients. These results were supported by a similar study that noted no significant increase in thromboembolic events with TXA use in patients with severe predisposing comorbidities all while decreasing transfusion rates.88 Although more research is needed to fully substantiate these results, these conclusions suggest that TXA may be safe to use even in patients with comorbidities that place them at a high baseline risk for thromboembolic complications.
Conclusion
TXA is widely utilized in nearly all Orthopedic Surgery subspecialties including trauma, joint, sports medicine, and spine. Many orthopedic procedures such as TKA, THA, fracture fixation, and various spine surgeries involve significant intraoperative blood loss highlighting the need for effective hemostasis, and TXA has been shown to decrease both total and/or intraoperative blood loss in all studies reviewed. Additionally, TXA has been implicated in reducing the risk of blood transfusions in orthopedic trauma, joint surgery, and spine surgery although this effect is not seen as prominently in sports medicine procedures. Additionally, there is disagreement in literature as to whether TXA via any route of administration can improve other clinically significant outcomes such as hospital length of stay, and total operative time. Procedures that rely extensively on clarity in visualization of the surgical field such as knee and shoulder arthroscopies can greatly benefit from the use of TXA, thereby leading to less intraoperative bleeding, with multiple studies showing a significantly higher subjective rating of visual clarity by surgeons as well as a lower volume of irrigation required during these procedures. While most studies agree thrombosis due to TXA is unlikely, new research in cells and animal models is evaluating whether TXA can negatively impact other aspects of musculoskeletal physiology such as bone and tendon healing, however with conflicting results thus far. As of now, TXA continues to remain a safe and effective means of promoting hemostasis and reducing intraoperative blood loss in orthopedic surgery.
Disclosure
All of the authors report no financial disclosures and no conflicts of interest for this work.
References
1. Hunt BJ. The current place of tranexamic acid in the management of bleeding. Anaesthesia. 2015;70(Suppl 1):50–53,e18. doi:10.1111/anae.12910
2. Tengborn L, Blomback M, Berntorp E. Tranexamic acid–an old drug still going strong and making a revival. Thromb Res. 2015;135(2):231–242.
3. World Health O. World Health Organization Model List of Essential Medicines: 21st List 2019. Geneva: World Health Organization; 2019.
4. Jennings JD, Solarz MK, Haydel C. Application of tranexamic acid in trauma and orthopedic surgery. Orthop Clin North Am. 2016;47(1):137–143.
5. Franchini M, Mengoli C, Cruciani M, et al. Safety and efficacy of tranexamic acid for prevention of obstetric haemorrhage: an updated systematic review and meta-analysis. Blood Transfus. 2018;16(4):329–337.
6. Sentilhes L, Lasocki S, Ducloy-Bouthors AS, et al. Tranexamic acid for the prevention and treatment of postpartum haemorrhage. Br J Anaesth. 2015;114(4):576–587.
7. Cai J, Ribkoff J, Olson S, et al. The many roles of tranexamic acid: an overview of the clinical indications for TXA in medical and surgical patients. Eur J Haematol. 2020;104(2):79–87.
8. collaborators C-T; Shakur H, Roberts I, et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet. 2010;376(9734):23–32.
9. Morrison JJ, Dubose JJ, Rasmussen TE, Midwinter MJ. Military Application of Tranexamic Acid in Trauma Emergency Resuscitation (MATTERs) study. Arch Surg. 2012;147(2):113–119.
10. Lemaire R. Strategies for blood management in orthopaedic and trauma surgery. J Bone Joint Surg Br. 2008;90-B(9):1128–1136. doi:10.1302/0301-620X.90B9.21115
11. Wei Z, Liu M. The effectiveness and safety of tranexamic acid in total hip or knee arthroplasty: a meta-analysis of 2720 cases. Transfus Med. 2015;25(3):151–162. doi:10.1111/tme.12212
12. Wei W, Dang S, Duan D, Wei L. Comparison of intravenous and topical tranexamic acid in total knee arthroplasty. BMC Musculoskelet Disord. 2018;19(1):191. doi:10.1186/s12891-018-2122-7
13. Yang Y, Wang Z, Wang F, et al. Prospective, randomised, controlled study on the efficacy and safety of different strategies of tranexamic acid with total blood loss, blood transfusion rate and thrombogenic biomarkers in total knee arthroplasty: study protocol. BMJ Open. 2021;11(2):e038399. doi:10.1136/bmjopen-2020-038399
14. Lei Y, Xie J, Huang Q, Huang W, Pei F. Additional benefits of multiple-dose tranexamic acid to anti-fibrinolysis and anti-inflammation in total knee arthroplasty: a randomized controlled trial. Arch Orthop Trauma Surg. 2020;140(8):1087–1095. doi:10.1007/s00402-020-03442-2
15. Lei YT, Xie JW, Huang Q, Huang W, Pei FX. The antifibrinolytic and anti-inflammatory effects of a high initial-dose tranexamic acid in total knee arthroplasty: a randomized controlled trial. Int Orthop. 2020;44(3):477–486.
16. Akgul T, Buget M, Salduz A, et al. Efficacy of preoperative administration of single high dose intravenous tranexamic acid in reducing blood loss in total knee arthroplasty: a prospective clinical study. Acta Orthop Traumatol Turc. 2016;50(4):429–431.
17. Whiting DR, Sierra RJ. Efficacy of combined use of intraarticular and intravenous tranexamic acid in total knee arthroplasty. Ann Transl Med. 2015;3(Suppl 1):S39.
18. Zhang S, Xie J, Cao G, Lei Y, Huang Q, Pei F. Six-dose intravenous tranexamic acid regimen further inhibits postoperative fibrinolysis and reduces hidden blood loss following total knee arthroplasty. J Knee Surg. 2021;34(2):224–232.
19. Wang H, Shen B, Zeng Y. Comparison of topical versus intravenous tranexamic acid in primary total knee arthroplasty: a meta-analysis of randomized controlled and prospective cohort trials. Knee. 2014;21(6):987–993.
20. Zhao Z, Ma J, Ma X. Comparative efficacy and safety of different hemostatic methods in total hip arthroplasty: a network meta-analysis. J Orthop Surg Res. 2019;14(1):3.
21. Chen Y, Chen Z, Cui S, Li Z, Yuan Z. Topical versus systemic tranexamic acid after total knee and hip arthroplasty: a meta-analysis of randomized controlled trials. Medicine (Baltimore). 2016;95(41):e4656.
22. Li J, Zhang Z, Chen J. Comparison of efficacy and safety of topical versus intravenous tranexamic acid in total hip arthroplasty: a meta-analysis. Medicine (Baltimore). 2016;95(36):e4689.
23. Laoruengthana A, Rattanaprichavej P, Rasamimongkol S, Galassi M, Weerakul S, Pongpirul K. Intra-articular tranexamic acid mitigates blood loss and morphine use after total knee arthroplasty. A randomized controlled trial. J Arthroplasty. 2019;34(5):877–881.
24. Xie J, Hu Q, Huang Q, Ma J, Lei Y, Pei F. Comparison of intravenous versus topical tranexamic acid in primary total hip and knee arthroplasty: an updated meta-analysis. Thromb Res. 2017;153:28–36.
25. Zhang P, Liang Y, Chen P, Fang Y, He J, Wang J. Combined application versus topical and intravenous application of tranexamic acid following primary total hip arthroplasty: a meta-analysis. BMC Musculoskelet Disord. 2017;18(1):90.
26. Mei L, Li H, Zhu W, Luo Y, Mao X. Efficacy and safety of tranexamic acid in unilateral major revision total hip arthroplasty. Ann Palliat Med. 2020;9(5):2466–2473.
27. Liu X, Liu J, Sun G. A comparison of combined intravenous and topical administration of tranexamic acid with intravenous tranexamic acid alone for blood loss reduction after total hip arthroplasty: a meta-analysis. Int J Surg. 2017;41:34–43.
28. Wang D, Wang HY, Luo ZY, Pei FX, Zhou ZK, Zeng WN. Finding the optimal regimen for oral tranexamic acid administration in primary total hip arthroplasty: a randomized controlled trial. J Bone Joint Surg Am. 2019;101(5):438–445.
29. Wang D, Wang HY, Luo ZY, et al. Blood-conserving efficacy of multiple doses of oral tranexamic acid associated with an enhanced-recovery programme in primary total knee arthroplasty: a randomized controlled trial. Bone Joint J. 2018;100-B(8):1025–1032.
30. Wang D, Zhu H, Meng WK, et al. Comparison of oral versus intra-articular tranexamic acid in enhanced-recovery primary total knee arthroplasty without tourniquet application: a randomized controlled trial. BMC Musculoskelet Disord. 2018;19(1):85.
31. Zhang LK, Ma JX, Kuang MJ, et al. The efficacy of tranexamic acid using oral administration in total knee arthroplasty: a systematic review and meta-analysis. J Orthop Surg Res. 2017;12(1):159.
32. Tang Y, Wen Y, Li W, Li H, Yang Y, Liu Y. The efficacy and safety of multiple doses of oral tranexamic acid on blood loss, inflammatory and fibrinolysis response following total knee arthroplasty: a randomized controlled trial. Int J Surg. 2019;65:45–51.
33. Han X, Gong G, Han N, Liu M. Efficacy and safety of oral compared with intravenous tranexamic acid in reducing blood loss after primary total knee and hip arthroplasty: a meta-analysis. BMC Musculoskelet Disord. 2018;19(1):430.
34. Chen X, Zheng F, Zheng Z, Wu X, Wu C. Oral vs intravenous tranexamic acid in total-knee arthroplasty and total hip arthroplasty: a systematic review and meta-analysis. Medicine (Baltimore). 2019;98(20):e15248.
35. Kayupov E, Fillingham YA, Okroj K, et al. Oral and intravenous tranexamic acid are equivalent at reducing blood loss following total hip arthroplasty: a randomized controlled trial. J Bone Joint Surg Am. 2017;99(5):373–378.
36. Abildgaard JT, McLemore R, Hattrup SJ. Tranexamic acid decreases blood loss in total shoulder arthroplasty and reverse total shoulder arthroplasty. J Shoulder Elbow Surg. 2016;25(10):1643–1648.
37. Rojas J, Srikumaran U, McFarland EG. Inconclusive evidence for the efficacy of tranexamic acid in reducing transfusions, postoperative infection or hematoma formation after primary shoulder arthroplasty: a meta-analysis with trial sequential analysis. Shoulder Elbow. 2021;13(1):38–50.
38. Yu BF, Yang GJ, Li Q, Liu LL. Tranexamic acid decreases blood loss in shoulder arthroplasty: a meta-analysis. Medicine (Baltimore). 2017;96(33):e7762.
39. Hardy JC, Hung M, Snow BJ, et al. Blood transfusion associated with shoulder arthroplasty. J Shoulder Elbow Surg. 2013;22(2):233–239.
40. Zhu Q, Yu C, Chen X, et al. Efficacy and safety of tranexamic acid for blood salvage in intertrochanteric fracture surgery: a meta-analysis. Clin Appl Thromb Hemost. 2018;24(8):1189–1198.
41. Ma H, Wang H, Long X, et al. Early intravenous tranexamic acid intervention reduces post-traumatic hidden blood loss in elderly patients with intertrochanteric fracture: a randomized controlled trial. J Orthop Surg Res. 2021;16(1):106.
42. Zhang P, Bai J, He J, Liang Y, Chen P, Wang J. A systematic review of tranexamic acid usage in patients undergoing femoral fracture surgery. Clin Interv Aging. 2018;13:1579–1591.
43. Qi YM, Wang HP, Li YJ, et al. The efficacy and safety of intravenous tranexamic acid in hip fracture surgery: a systematic review and meta-analysis. J Orthop Translat. 2019;19:1–11.
44. Xiao C, Zhang S, Long N, Yu W, Jiang Y. Is intravenous tranexamic acid effective and safe during hip fracture surgery? An updated meta-analysis of randomized controlled trials. Arch Orthop Trauma Surg. 2019;139(7):893–902.
45. Gausden EB, Qudsi R, Boone MD, O’Gara B, Ruzbarsky JJ, Lorich DG. Tranexamic acid in orthopaedic trauma surgery: a meta-analysis. J Orthop Trauma. 2017;31(10):513–519.
46. Bai J, Zhang P, Liang Y, Wang J, Wang Y. Efficacy and safety of tranexamic acid usage in patients undergoing posterior lumbar fusion: a meta-analysis. BMC Musculoskelet Disord. 2019;20(1):390.
47. He B, Li Y, Xu S, Ou Y, Zhao J. Tranexamic acid for blood loss after transforaminal posterior lumbar interbody fusion surgery: a double-blind, placebo-controlled, randomized study. Biomed Res Int. 2020;2020:8516504.
48. Li ZJ, Fu X, Xing D, Zhang HF, Zang JC, Ma XL. Is tranexamic acid effective and safe in spinal surgery? A meta-analysis of randomized controlled trials. Eur Spine J. 2013;22(9):1950–1957.
49. Luo W, Sun RX, Jiang H, Ma XL. The efficacy and safety of topical administration of tranexamic acid in spine surgery: a meta-analysis. J Orthop Surg Res. 2018;13(1):96.
50. Yang L, Jia X, Yang J, Kang J. Tranexamic acid reduces blood cost in long-segment spinal fusion surgery: a randomized controlled study protocol. Medicine (Baltimore). 2020;99(37):e22069.
51. Yuan L, Zeng Y, Chen ZQ, et al. Efficacy and safety of antifibrinolytic agents in spinal surgery: a network meta-analysis. Chin Med J (Engl). 2019;132(5):577–588.
52. Zhang Y, Liu H, He F, Chen A, Yang H, Pi B. Does tranexamic acid improve bleeding, transfusion, and hemoglobin level in patients undergoing multilevel spine surgery? A systematic review and meta-analysis. World Neurosurg. 2019;127:289–301.
53. Zhao Y, Xi C, Xu W, Yan J. Role of tranexamic acid in blood loss control and blood transfusion management of patients undergoing multilevel spine surgery: a meta-analysis. Medicine (Baltimore). 2021;100(7):e24678.
54. Ersin M, Demirel M, Büget M, Edipoğlu İS, Atalar AC, Erşen A. The effect of intravenous tranexamic acid on visual clarity during arthroscopic rotator cuff repair: a randomized, double-blinded, placebo-controlled pilot study. Acta Orthop Traumatol Turc. 2020;54(6):572–576.
55. Bayram E, Yıldırım C, Ertürk AK, Yılmaz M, Atlıhan D. Comparison of the efficacy of irrigation with epinephrine or tranexamic acid on visual clarity during arthroscopic rotator cuff repair: a double-blind, randomized-controlled study. Jt Dis Relat Surg. 2021;32(1):115–121.
56. Avery DM
57. Liu YF, Hong CK, Hsu KL, et al. Intravenous administration of tranexamic acid significantly improved clarity of the visual field in arthroscopic shoulder surgery. a prospective, double-blind, and randomized controlled trial. Arthroscopy. 2020;36(3):640–647.
58. Hartland AW, Teoh KH, Rashid MS. Clinical effectiveness of intraoperative tranexamic acid use in shoulder surgery: a systematic review and meta-analysis. Am J Sports Med. 2021;49:363546520981679.
59. Gao HL, Zhang JC, He Y, Zhai WT, Xiao LB, Shi Q. [Clinical study on the control of intra-articular hemorrhage by tranexamic acid after shoulder arthroscopy]. Zhongguo Gu Shang. 2020;33(3):238–241. Chinese.
60. Belk JW, McCarty EC, Houck DA, Dragoo JL, Savoie FH, Thon SG. Tranexamic acid use in knee and shoulder arthroscopy leads to improved outcomes and fewer hemarthrosis-related complications: a systematic review of Level I and II studies. Arthroscopy. 2021;37(4):1323–1333.
61. Nugent M, May JH, Parker JD, et al. Does tranexamic acid reduce knee swelling and improve early function following arthroscopic meniscectomy? A double-blind randomized controlled trial. Orthop J Sports Med. 2019;7(8):2325967119866122.
62. Li N, Qin LW, Jiang HJ. [Clinical effects of tranexamic acid in arthroscope for femoroacetabular impingement]. Zhongguo Gu Shang. 2021;34(2):121–125. Chinese.
63. Chiang ER, Chen KH, Wang ST, et al. Intra-articular injection of tranexamic acid reduced postoperative hemarthrosis in arthroscopic anterior cruciate ligament reconstruction: a prospective randomized study. Arthroscopy. 2019;35(7):2127–2132.
64. Felli L, Revello S, Burastero G, et al. Single intravenous administration of tranexamic acid in anterior cruciate ligament reconstruction to reduce postoperative hemarthrosis and increase functional outcomes in the early phase of postoperative rehabilitation: a randomized controlled trial. Arthroscopy. 2019;35(1):149–157.
65. Fried JW, Bloom DA, Hurley ET, et al. Tranexamic ACID has no effect on postoperative hemarthrosis or pain control after anterior cruciate ligament reconstruction using bone-patellar tendon-bone autograft: a double-blind, randomized, controlled trial. Arthroscopy. 2021;37(6):1883–1889.
66. Ma R, Wu M, Li Y, et al. The comparative efficacies of intravenous administration and intra-articular injection of tranexamic acid during anterior cruciate ligament reconstruction for reducing postoperative hemarthrosis: a prospective randomized study. BMC Musculoskelet Disord. 2021;22(1):114.
67. Tan TK, Ng KT, Lim HJ, Radic R. Effect of tranexamic acid in arthroscopic anterior cruciate ligament repair: a systematic review and meta-analysis of randomised clinical trials. J Orthop Surg (Hong Kong). 2021;29(2):23094990211017352.
68. Karaaslan F, Karaoğlu S, Yurdakul E. Reducing intra-articular hemarthrosis after arthroscopic anterior cruciate ligament reconstruction by the administration of intravenous tranexamic acid: a prospective, randomized controlled trial. Am J Sports Med. 2015;43(11):2720–2726.
69. Johns WL, Walley KC, Hammoud S, Gonzalez TA, Ciccotti MG, Patel NK. Tranexamic acid in anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Am J Sports Med. 2021;363546521988943. doi:10.1016/j.arthro.2021.07.030
70. Martin R, Birmingham TB, Willits K, Litchfield R, Lebel ME, Giffin JR. Adverse event rates and classifications in medial opening wedge high tibial osteotomy. Am J Sports Med. 2014;42(5):1118–1126.
71. Pape D, Dueck K, Haag M, Lorbach O, Seil R, Madry H. Wedge volume and osteotomy surface depend on surgical technique for high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2013;21(1):127–133.
72. Li S, Lu Q, Guo X, et al. Intravenous combined with topical tranexamic acid administration has no additional benefits compared with intravenous administration alone in high tibial osteotomy: a retrospective case-control study. Orthop Surg. 2020;12(2):515–523.
73. Yao RZ, Gao WQ, Wang BW, Wang GL, Wu CX, Efficacy YDAM. Safety of tranexamic acid in reducing blood loss of lower extremity osteotomy in peri-acetabulum and high tibia: a systematic review and meta-analysis. Orthop Surg. 2019;11(4):545–551.
74. Ma J, Lu H, Chen X, Wang D, Wang Q. The efficacy and safety of tranexamic acid in high tibial osteotomy: a systematic review and meta-analysis. J Orthop Surg Res. 2021;16(1):373.
75. Ni J, Liu J, Zhang J, Jiang J, Dang X, Shi Z. Tranexamic acid is beneficial for blood management of high tibial osteotomy: a randomized controlled study. Arch Orthop Trauma Surg. 2020;141(9):1463–1472.
76. Sershon RA, Fillingham YA, Abdel MP, et al. The optimal dosing regimen for tranexamic acid in revision total hip arthroplasty: a multicenter randomized clinical trial. J Bone Joint Surg Am. 2020;102(21):1883–1890.
77. Balachandar G, Abuzakuk T. Is there an optimal timing of administration of single-dose intravenous tranexamic acid in bilateral total knee arthroplasty? A comparison between preoperative and intraoperative dose. J Orthop Surg (Hong Kong). 2019;27(3):2309499019880915.
78. Tengborn L, Blombäck M, Berntorp E. Tranexamic acid–an old drug still going strong and making a revival. Thromb Res. 2015;135(2):231–242.
79. Reale D, Andriolo L, Gursoy S, Bozkurt M, Filardo G, Zaffagnini S. Complications of Tranexamic acid in orthopedic lower limb surgery: a meta-analysis of randomized controlled trials. Biomed Res Int. 2021;2021:6961540.
80. Myers SP, Kutcher ME, Rosengart MR, et al. Tranexamic acid administration is associated with an increased risk of posttraumatic venous thromboembolism. J Trauma Acute Care Surg. 2019;86(1):20–27. doi:10.1097/TA.0000000000002061
81. McLean M, McCall K, Smith IDM, et al. Tranexamic acid toxicity in human periarticular tissues. Bone Joint Res. 2019;8(1):11–18.
82. Parker JD, Lim KS, Kieser DC, Woodfield TBF, Hooper GJ. Is tranexamic acid toxic to articular cartilage when administered topically? What is the safe dose? Bone Joint J. 2018;100-b(3):404–412.
83. Ambra LF, de Girolamo L, Niu W, Phan A, Spector M, Gomoll AH. No effect of topical application of tranexamic acid on articular cartilage. Knee Surg Sports Traumatol Arthrosc. 2019;27(3):931–935.
84. Çıraklı A, Gürgör PN, Uzun E, Erdem H, Çankaya S, Baş O. Local application of tranexamic acid affects tendon healing negatively in the late period. Eklem Hastalik Cerrahisi. 2018;29(1):20–26.
85. Sarı A, Dinçel YM, Karabağ S, Çetin M. Histopathological and immunohistochemical investigation of the local and systemic effects of tranexamic acid on the healing of the Achilles tendon in rats. Jt Dis Relat Surg. 2021;32(1):152–161.
86. Balkanli B, Copuroglu C, Copuroglu E. The effects of intravenous and local tranexamic acid on bone healing: an experimental study in the rat tibia fracture model. Injury. 2020;51(12):2840–2845.
87. Porter SB, White LJ, Osagiede O, Robards CB, Spaulding AC. Tranexamic acid administration is not associated with an increase in complications in high-risk patients Undergoing Primary Total Knee or Total Hip Arthroplasty: a Retrospective Case-Control Study of 38,220 patients. J Arthroplasty. 2020;35(1):45–51.e43.
88. Whiting DR, Gillette BP, Duncan C, Smith H, Pagnano MW, Sierra RJ. Preliminary results suggest tranexamic acid is safe and effective in arthroplasty patients with severe comorbidities. Clin Orthop Relat Res. 2014;472(1):66–72.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.