")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Utilization of Primary Health Care Under National Health Insurance in Samarinda Municipality, East Kalimantan Province, Indonesia
Authors Astuti D , Kongsin S , Jiamton S, Prakongsai P , Hearnden SR
Received 30 October 2023
Accepted for publication 22 February 2024
Published 9 March 2024 Volume 2024:17 Pages 1025—1039
DOI https://doi.org/10.2147/JMDH.S447332
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Dewi Astuti,1 Sukhontha Kongsin,2 Sukhum Jiamton,3 Phusit Prakongsai,4 Scott Robert Hearnden5
1Faculty of Public Health, Mahidol University, Bangkok, Thailand; 2Department of Public Health Administration, Faculty of Public Health, Mahidol University, Bangkok, Thailand; 3Department of Dermatology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand; 4Department of Community Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 5Department of Social and Political Sciences (Peace and Conflict Studies), Faculty of Arts and Social Sciences, University of Sydney, Camperdown (Sydney), NSW, Australia
Correspondence: Sukhontha Kongsin, Email [email protected]; [email protected]
Aim: In Indonesia, basic community health services are provided to all citizens through Primary Health Care (PHC) settings under the National Health Insurance (NHI) scheme. The insurance is compulsory and provides basic community health needs. Based on a gatekeeper concept, the PHC is deemed to be the first contact point for all basic healthcare needs. Despite the commencement of services through PHC settings in 2014 under this concept, utilization in PHC settings remains lower than in hospital settings. This study aimed to assess factors associated with utilization of PHC under National Health Insurance in Samarinda Municipality, East Kalimantan Province, Indonesia.
Materials and Methods: The research examined the utilization of services over six months. It employed a cross-sectional method and included 382 NHI participants in 10 districts of Samarinda Municipality. Each district was divided into urban and semi-urban areas based upon local government indicators representing the whole research area. A two-stage random sampling and purposive sampling approach was implemented to select the sample. The participants were interviewed using a structured questionnaire. Chi-square and multiple logistic regressions were conducted to determine the impact of factors on the utilization of PHC.
Results: Only 17.3% of participants used PHC services regularly. Three constitutive factors, type of NHI participants (Adj. OR: 2.62; p< 0.005), accommodation (Adj. OR: 2.18; p< 0.005) and awareness (Adj. OR: 3.27; p< 0.005) most profoundly influenced the under-utilization of PHC by NHI participants.
Conclusion: The study found that the type of NHI participant and the utilization factors of accommodation and awareness significantly influenced the degree of utilization of PHC facilities by NHI participants and that the differences arose from variations in knowledge and experience. Strengthening these factors will rely upon an expanded role of government and community collaboration, emphasizing the needs of NHI participants.
Keywords: Indonesia, National Health Insurance, primary health care, utilization
Introduction
Universal Health Coverage (UHC) is the World Health Organization’s (WHO) framework aimed at promoting equitable healthcare systems at the country level. The framework focuses on ensuring universal access to healthcare services and achieving greater equity across healthcare systems.1 The UHC program has three dimensions: a) population (who to cover?); b) services (what to cover?); and c) affordability (how to reduce the cost of care).2 This program aims to improve the quality and utilization of health services while simultaneously protecting users financially by minimizing out-of-pocket expenses.
The 2030 Sustainable Development Goals (SDGs) have set targets for achieving Universal Health Coverage (UHC) worldwide. The SDGs aim to have 1 billion more people added to the coverage by 2025. In Indonesia, the National Health Insurance (NHI) scheme, known as the Jaminan Kesehatan Nasional (JKN) has been implemented since 2014 to achieve this goal. Each country implements the program based on its own particular cultural, socio-demographic, and socio-economic factor.3
The Social Security Agency for Health (or Badan Penyelenggara Jaminan Sosial Kesehatan) established the NHI scheme, which is a compulsory insurance for all citizens, irrespective of their socio-economic background. The NHI scheme has two types of membership: 1) contributing members – those who are self-employed individuals and families, formal sector employees, employees, and their family members, or retirees (called non-government subsidized; non-PBI group); and 2) non-contributing members – those who are living in poverty or living with a disability and whose membership is subsidized and/or funded by Indonesia’s government (called government-subsidized; PBI group).4,5
By the end of 2019, NHI coverage had reached an impressive 80% of the country’s population (221 million people). The NHI program was supported by more than twenty-three thousand Primary Health Care (PHC) facilities that were strategically located within communities across the country. The Indonesian Ministry of Health classifies health facilities for NHI participants across three levels: primary (community) health care (PHC); secondary health care, through hospital facilities; and, tertiary health care which includes provincial hospitals and sub-specialist facilities.6
This research primarily focused on the first level of service delivery through PHC, which includes Community Health Centers, clinics, general practitioners, and dentists. Service delivery is executed on a “gatekeeper” concept approach, which implies that PHC facilities serve as the first contact point to provide basic health care for NHI participants. These services include: medical check-ups, home visits, dental, family planning, mother and child health, chronic diseases, outpatient and screening as well as health prevention and promotion.7 The Indonesian Ministry of Health Regulation number 5 of 2014 states the competency standards that doctors and PHC facilities must demonstrate to ensure a minimum level of service delivery. It also refers to the attainment of those competencies for the most common 144 diagnoses and 11 medical conditions.8
Additionally, if a PHC facility is unable to provide a specific service due to lack of required competencies or equipment, it may refer NHI participants to another appropriate health facility. This could be another PHC facility possessing the necessary competency or a facility at a different level, such as a level 2 or 3 hospital, if deemed necessary. However, there is a maximum limit of referral of only 15% for the total number of people seeking PHC services that can be referred to another facility in any given month.9 The research also noted that in emergencies, NHI participants are exempted from PHC attendance and may go directly to a hospital without a referral letter from a PHC facility.
PHC facilities are available in Indonesia’s rural, semi-urban and urban areas, classified based on local government criteria such as population density, the percentage of agricultural households and availability of, or access to, urban facilities.10 For this study, the researcher focused on four sub-districts that encompassed both semi-urban and urban areas, without distinguishing them for the results.
The Statistics of People’s Welfare Report (2018) revealed that only 49.1% of people attending healthcare facilities in Indonesia opted for PHC, while 51.15% preferred hospitals. The report also highlights a high referral rate of 16.6% of NHI participants referred from PHC facilities to hospitals. This can be attributed to several factors such as inadequate availability of PHC facilities; lack of qualified human resources within PHC facilities; improper patient referral; and patients’ lack of comprehension of the referral system.11,12 Poor performance of PHC is likely to be the leading cause of low utilization in these facilities. PHC plays a crucial role in providing referral letters that can help prevent unnecessary burdens on healthcare resources and economic constraints on hospitals.13 This highlights the importance of PHC in effectively managing healthcare services and resources.
Utilization is a key factor in assessing the strength of healthcare systems. It is measured by outcomes such as availability of services, economic indicators, health resources, and interaction between health personnel and patients. Good access to health facilities is the primary factor that increases utilization. Most utilization theories determine that utilization is developed around questions of access.14
In this study, the concept of access to healthcare is defined by scholars Roy Penchansky and J. William Thomas as the degree of fit between the user and the health service being provided, taking into account various dimensions of access.15 Deborah Russel16 and Jean-Frederic Levesque added “awareness” to this framework to evaluate access to the PHC including users’ knowledge and health literacy.17,18 Scholars propose that “utilization” is best understood across six-dimensions: related accessibility; availability; acceptability; affordability; accommodation; and awareness.
Samarinda Municipality has over 500,000 NHI participants with 79 PHC units in urban and semi-urban areas. Only 38.44% of residents in both areas used health services in PHC facilities in 2018 while 41.73% used hospitals.11,19 Dewi Astuti and Anisa Gyardani found that patients’ satisfaction with the “availability” of services directly affects PHC utilization.20,21
Accordingly, this study examined the utilization of PHC facilities over six months through the prisms of six constitutive sub-variables, which influenced the under-utilization of services in PHC settings in Samarinda Municipality, East Kalimantan Province, Indonesia.
Materials and Methods
Study Design
A cross-sectional study design was conducted in Samarinda Municipality, Indonesia.
Potential Participants
The municipality consists of 10 districts each further administratively divided into urban and semi-urban areas. Of these 10 districts, 2 were randomly selected for the sample. Two sub-districts were then randomly selected within each of the 2 districts (4 sub-districts). NHI participants utilizing PHC across the 4 sub-districts were then subjected to a further purposive set of selection criteria, as discussed below, to assess their final suitability, and thus inclusion, in the sample. It is worth noting that there were no rural areas identified within any of the 4 sub-districts selected. Hence the targets area to which the results relate include a cohort of participants who lived in urban or semi-urban areas only. The distinguishing features between these two populations are population density, percentage of agricultural households, and availability of, or the access to, urban facilities. Both areas represent the whole region in Samarinda Municipality, which must be included in this research. The population of interest was 564,359 NHI participants aged > 18 years.
Sample Size and Sampling Procedure
Two stage random sampling was adopted to select the sample (Figure 1). Simple random sampling was applied to select two districts. The same approach was used to then select two sub-districts within each district. Hence four sub-districts were selected. Proportionate stratified random sampling, based on a proportion to size of NHI participants, was calculated for each sub-district. The purposive sampling was adopted by following the inclusion and exclusion criteria considered by the researcher.
 |
Figure 1 Profile of sample selection, Samarinda Municipality East Kalimantan, Indonesia (n=382). |
The inclusion criteria were as follows: (1) NHI participants; (2) >_ 18 years; (3) at least one experience at PHC; (4) was living in one of the 4 sub-districts of the target area; and, (5) provided the researcher with written informed consent to voluntarily participate in the study. Exclusion criteria were as follows: (1) participants were becoming unwell at the interview; and (2) participants could not communicate well. The 382 NHI participants selected served as the target population in this study.
Research Instruments
A structured questionnaire was developed to collect data based on the literature review and consisted of eight parts: (1) socio-demographic characteristics (age, marital status, level of education, level of income, and type of NHI); (2) utilization of PHC was classified regular and non-regular (regular, ie, means frequency of visits to health services > 2 times in PHC, and non-regular, ie, means frequency of visits to health services < 2 times) and also subject to the utilization patterns; (3) accessibility (the distance, travel time, and mode of transportation); (4) affordability was concerned with respondents’ perception of financial matters, including incidental costs associated with the provision of services at the PHC (whether they were considered inexpensive, normal, and expensive; others answered “yes” or “no”); (5) availability (whether sufficient services and resources were available); (6) acceptability (the attitudes of health personnel, characteristics of services and social concerns of participants); (7) accommodation (hours of operation, referral system, the appointment system and facilities of PHC); and, (8) awareness (effective communication and sustainability of information strategies related to services). These variables were scored using a three-point Likert scale method ranging from 1 (disagree), 2 (not sure), and 3 (agree) and calculated based on the total score. The following criteria were applied to categorize the results by using a percentile cut-off-scale: a) >80% total score signified a high level of utilization; b) 60–79% total score signified a moderate level of utilization; and c) <60% score signified a low level of utilization.
Validity and Reliability
The questionnaire was translated from English to Indonesian and was tested for validity and reliability using Cronbach Alpha with a value of > 0.7.
Ethical Considerations
The Ethics Review Committee approved this study for Human Research, Faculty of Public Health, Mahidol University, on March 16th, 2020 (Approval number 41/2563) and from the Research and Community Engagement Ethical Committee of the Unity of Nations and Politics on April 1st, 2020 (Approval number 070/237/IV-BKP/IV/2020). All respondents provided written informed consent before enrolment in the study.
Data Collection
The study was carried out from April 2020 to May 2020. The researcher visited and identified the participants based on inclusion and exclusion criteria in public areas. The face-to-face interviews were conducted using a structured questionnaire after obtaining written informed consent.
Data Analysis
The research used “descriptive statistics” to describe study variables. For example, proportions, percentages, mean and standard deviation (SD) were used. The Chi-squared test was performed for bivariate analyses in order to determine whether a statistical association exists between two variables and to see the different proportions by using a cross-tabulation table.
Descriptive analysis was done first to describe study variables. This value helped to find the proportions, percentage, mean, and standard deviation (SD). The Chi-squared test was performed for bivariate analyses in order to determine whether a statistical association exists between two variables. Multivariate logistic regression analysis was then performed on the p-value less than 0.20 in order to find associations between dependent and independent variables by using Enter method. Biological and socio-demographic variables, such as age and gender, were retained in the final model.
All data analyses were performed using the Statistical Software for the Social Sciences IBM SPSS Statistics v. 25 which is recommended for bivariate and multivariate analyses.22 A two-sided p-value <0.05 was considered statistically significant because it means that the null hypothesis is statistically significant.
Results
This study was conducted across four sub-districts, with a total of 382 NHI participants. The dependent variable was analyzed by measuring its constituent parts as a percentage of the total sample. This included socio-demographic characteristics as well as six dimensions of “utilization”. The results are presented in Tables 1 and 2.
 |
Table 1 Characteristics and Patterns of PHC Utilization Among NHI Participants in Samarinda Municipality (n=382) |
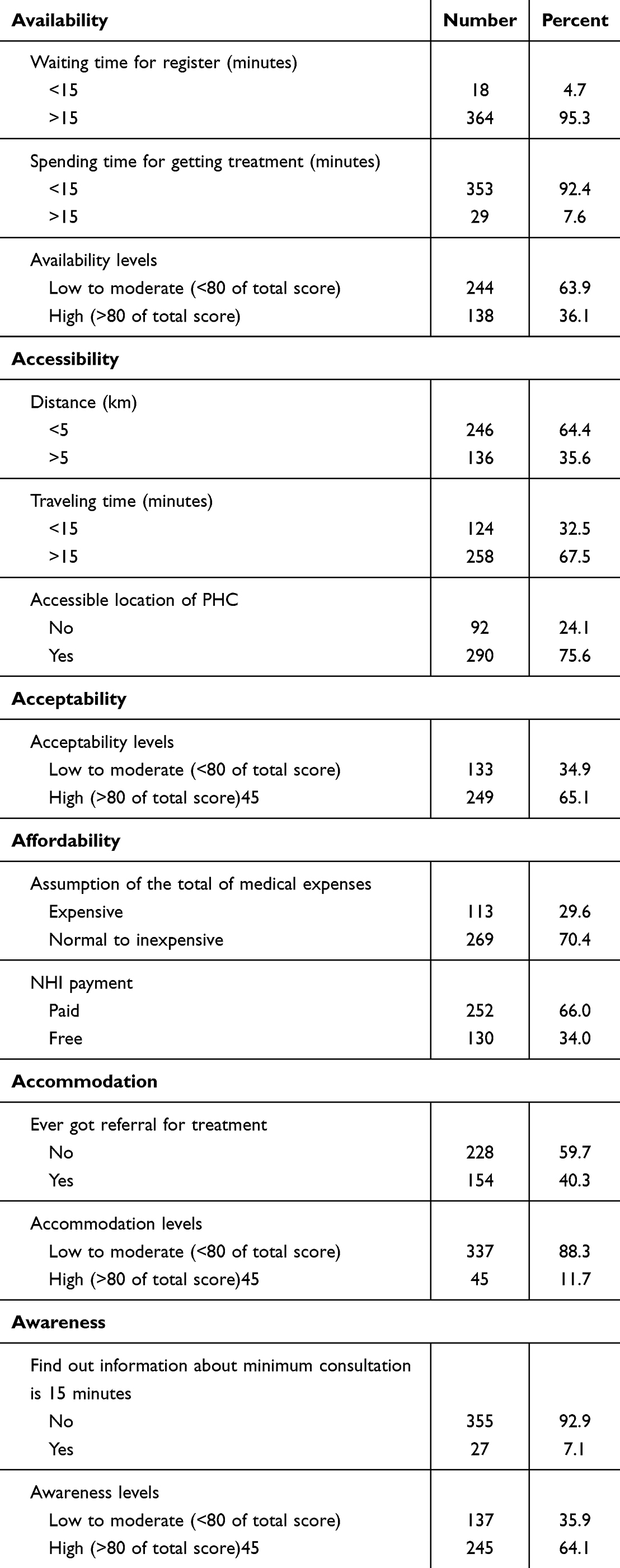 |
Table 2 Characteristics and Patterns of PHC Utilization Among NHI Participants in Samarinda Municipality (n=382) |
Table 1 presents the health conditions and utilization patterns of participants. The data shows that a significant number of participants (37.4%) had experienced non-communicable diseases. Furthermore, the utilization was low, with only 17.3% of participants regularly using their insurance in the past six months. This trend was more pronounced in the government-subsidized group (PBI group), which had the lowest utilization of their health insurance services, despite the services being free. The Non-PBI group had a higher utilization (80.3%), indicating that financial barriers may not be the only reason for low utilization of PHC.
Independent Variables
Socio-Demographic Characteristics
The research sample included both male and female participants, with females comprising 59.2% of the total sample. The mean age of participants were over the age of 35. The educational background of the participants was diverse, with 76.5% having completed high school or higher education. Most participants (68.1%) were employed and married. The majority of participants (58.9%) reported low monthly income. These findings indicate that the sample was representative of a diverse group from different demographic backgrounds.
Accessibility in Utilization
The accessibility factor in this study was based on three variables: traveling time, actual distance, and mode of transportation. The study found that most respondents (64.4%) lived within a distance of less than 5 km from the PHC facility, indicating that most of the population has easy access to PHC services. Regarding travel time, about 67.5% of participants took less than 15 minutes to travel to the PHC. This could be due to various reasons, such as traffic congestion, poor road conditions, and inadequate public transportation. About 75.6% of participants considered the PHC location to be easily accessible. However, it is essential to note that travel time and accessibility to the PHC are still within an acceptable range and poses a manageable barrier to accessing PHC services.
Availability in Utilization
The variable of “availability” comprises waiting time, doctor services, and the PHC environment (Table 2). The findings reveal that a substantial number of participants, almost 95% had to wait for over 20 minutes during the registration process before seeing a doctor. However, the duration of time spent with the doctor was relatively shorter, with only 7.6% of participants spending more than 15 minutes. With regard to knowledge score relating to the “availability” factor, the majority of participants (63.9%) displayed only a moderate level of understanding.
Acceptability in Utilization
Acceptability includes the attitude of health personnel, characteristics of services, and social concerns. Around 65.1% of NHI participants had a high level of acceptability knowledge. However, the remaining 34.9% displayed only a moderate level of knowledge.
Affordability in Utilization
According to the result of this study, a significant majority of participants (68.3%) indicated that the total cost of medical expenses, which included direct costs for tuition fees and transportation costs, was within the normal range. Additionally, the government provided subsidies to approximately 34% of the study participants, covering a portion of their healthcare expenses.
Accommodation in Utilization
The accommodation variable comprises the responsiveness of facility structures to participants’ needs, hours of operation, referral and appointment systems. Around 40.3% of participants reported receiving a referral letter to another health facility at some point. Merely 11.8% of participants demonstrated a high level of knowledge in relation to accommodation-related queries.
Awareness in Utilization
Awareness plays a crucial role in the effectiveness of communication and information strategies related to services. According to the result, a large percentage of participants (92.9%) were unaware of their right to a minimum consultation period of 15 minutes per visit with the doctor or health personnel. Although 64.1% of participants had a high level of knowledge, only a tiny fraction (1.3%) had a low level of awareness. These findings highlight the need to increase awareness among the general public about their rights and entitlements when it comes to PHC services.
Factors Associated with Utilization of PHC Under NHI Among Samarinda Municipality
According to Tables 3 and 4, the Chi-Square test results indicate a statistically significant relationship between the two types of NHI participants and their utilization of PHC. In addition, the availability, acceptability, affordability, accommodation, and awareness factors are also significantly related to PHC use among NHI participants (p < 0.05) in Samarinda Municipality. However, gender, age, marital status, occupation, education, and monthly income were not found to be significant factors.
 |
Table 3 Bivariate Analysis of PHC Utilization Among NHI Participants in Samarinda Municipality (N= 382) |
 |
Table 4 Bivariate Analysis of PHC Utilization Among NHI Participants in Samarinda Municipality (N= 382) |
Based on Table 5, the most common reason behind the low utilization rate among the PBI group members is the distance from the PHC. Over a third of the PBI group respondents lived more than 5 km away from the PHC, with 72.3% taking more than 15 minutes to travel and 32.4% considering the PHC inaccessible. Additionally, the majority of the PBI group had little or no income, with around 10% having to pay for medical expenses not covered by NHI. Furthermore, approximately 34.6% of the PBI group incurred travel costs to access PHC. Most of the respondents were below 35 years of age and were less likely to visit PHC regularly. Another contributing factor was the PBI group’s low level of knowledge regarding accommodation and awareness levels, which were 32.9% and 34.3%, respectively, compared to the non-PBI group.
 |
Table 5 Bivariate Analysis of PHC Utilization in Terms of Type of NHI Participants in Samarinda Municipality (N= 382) |
The study utilized Multiple Logistic Regression to examine the utilization of NHI type (Table 6). The analysis revealed that the non-government subsidized group (Non-PBI group) had 2.6 times higher odds of utilizing PHC services than the government-subsidized group (PBI group) (p-value = 0.005).
 |
Table 6 Multivariate Analysis of PHC Utilization Among NHI Participants in Samarinda Municipality (N= 382) |
Furthermore, the study found that participants with the highest level of accommodation had 2.18 times higher odds of utilizing PHC services compared to other groups (p-value = 0.036).
In addition, respondents with a high level of awareness had three times higher odds of utilizing PHC services than those with a low to moderate level of awareness (p-value = 0.002). This suggests that awareness plays a crucial role in the utilization of PHC services, and those with higher levels of awareness are more likely to utilize these services than those with lower levels of awareness. Taken together, these results highlight the importance of understanding the factors that influence the utilization of PHC services, such as NHI status, level of accommodation, and level of awareness.
Discussion
This study demonstrated a significant correlation between the two types of National Health Insurance (NHI) membership and the utilization of primary healthcare (PHC). The study revealed that only 17.3% of the participants had visited PHC regularly in the past 6 months, with the majority of them belonging to the non-PBI group. Even though the government offers full subsidies to the PBI group, only a meager 19.7% of them utilized PHC services. This pattern is consistent with Yoharani’s findings in Jambi Municipality, where the coverage of the PBI group was higher than that of the non-PBI group, but the utilization rate was still relatively low at 38.7%. The PBI group’s low utilization rate could be attributed to their lack of knowledge about their entitlements regarding PHC services and the NHI information.23,24
As per the regulations set by the Indonesian Ministry of Health, regular health check-ups are recommended for elderly groups and individuals with non-communicable diseases such as hypertension and diabetes. These check-ups should be carried out at least four times per month at the Primary Health Care (PHC) centers.
The utilization of PHC services is typically higher among individuals who do not belong to the PBI type membership, as they are more aware of the benefits of the NHI and use it to maintain a healthy lifestyle. Additionally, the convenience of accessing PHC also plays a role in their decision to utilize these services.
However, this research did not find any significant impact of factors such as gender, age, marital status, occupation, education, and income on the utilization of primary health care. This could be due to the fact that most of the respondents were of productive age (18 to 34) and in relatively good health during the study, which led to less utilization of PHC services. This finding is consistent with previous studies by Nasution (2017) and Manalu (2018), which also found no significant association between occupation and education.25,26
This study found that a high level of accommodation is significantly associated with high utilization of Primary Health Care (PHC) services. Those with adequate accommodation were 2.8 times more likely to regularly utilize PHC services. A previous study also reported a similar relationship between accommodation and health care utilization in PHC.27 These findings suggest that improving accommodation for individuals seeking PHC services can lead to increased utilization and improved health outcomes.
The validity of respondents’ perceptions regarding services was found to be adequate based on their knowledge of the subject matter. The majority of the respondents referred to the challenges they faced while scheduling appointments (45.3%) and the complex regulatory environment of the National Health Insurance (NHI) system (36.1%) when answering questions about their experiences with health services. Specifically, the reasons provided included extended waiting periods, overcrowding, and insufficient regulatory information related to primary healthcare.
The issue of inadequate healthcare facilities remains a persistent challenge, as evidenced by a high percentage (40.3%) of patients being referred from primary healthcare centers (PHCs) to higher-level facilities. In line with the Gatekeeper Concept, the maximum monthly ratio of referrals to hospitals should not exceed 5%. To mitigate potential deficits and alleviate the workload of hospitals, it is necessary to strengthen the role of PHCs and reduce unnecessary referrals,4 consistent with the goals and the objectives of the National Health Insurance (NHI) system.
The potential user of Primary Health Care (PHC) plays a critical role in creating awareness about National Health Insurance (NHI). The level of awareness of the respondents significantly influences the utilization of PHC services (p-value=0.002). Respondents with a high level of awareness had a 3.76 times higher probability of regularly utilizing PHC services compared to those with less awareness. A previous study highlights the importance of awareness in influencing the utilization of PHC services in Lebanon.28 A further Indonesian study established a strong correlation between public awareness and the utilization of health services.29
The study indicated that, while a majority of patients (80.4%) engaged in regular utilization of health services, there was a notable lack of awareness regarding the National Health Insurance (NHI) through various media channels, including social media and television advertisements, within the community.7 Furthermore, the majority of respondents were unaware of a standard NHI regulation requiring a minimum consultation time of 15 minutes. This outcome is consistent with a similar study conducted in West Lombok Regency, Indonesia, which demonstrated that individuals who received information regarding health services were more likely to utilize them.30,31
An examination of the consultation process was undertaken by reference to the gatekeeper concept. It focused on the promotion and prevention services that participants could access. The information might change users’ perceptions and encourage people to utilize PHC and NHI better. Understanding these factors enabled a closer examination of the function of PHC.
Strengths and Limitations
This research was the first to examine factors associated with using PHC under NHI in this study area. The cross-sectional nature of the study as well as the adoption of multivariate analysis resulted in the researchers being able to reach the target population within a short period, and with minimal resources. This research has found that to improve the utilization of services in the PHC, two constitutive factors of utilization (accommodation and awareness) significantly contributed to the underutilization of PHC by NHI participants. The corollary of this finding is that if the health care system and the government of Indonesia direct greater attention on the needs of people who use PHC under NHI, especially regarding issues relating to accommodation and awareness, then the system’s performance will improve. The research found that other anticipated improvements will include: an increased knowledge of the system by potential NHI participants; fewer unwarranted referrals; improved relationships between health care professionals and NHI participants; and, overall better community utilization of services.
The research was also strengthened by the methods selected. This included the application of a broad cross-sectional study which employed multivariate analysis illuminating the gaps in the system. The research employed numerical and statistical reasoning to understand the “utilization” of PHC facilities. It offers one approach to the interpretation of utilization which can be used for projections into the future. Such a conclusion means that the information gleaned from this research not only strengthens knowledge of the target area, but that the findings can be used to leverage further improvements more broadly.
However, this research is not devoid of limitations. The cross-sectional study was conducted in an urban and semi-urban setting: thus the findings could not be generalised to the whole country. In addition, due to time constraints, there were many challenges, including conducting interviews during the Covid-19 pandemic. In Indonesia, large-scale social restrictions meant that most people stayed at home, and away from public areas. Notwithstanding these restrictions, efforts were made to gather the targeted number of participants as planned.
Conclusion
This study investigated the utilization patterns of Primary Health Care (PHC) facilities under the National Health Insurance (NHI) program in two districts of Samarinda Municipality, East Kalimantan Province, Indonesia.
While the results showed a low utilization across both groups, it also found that the non-PBI group utilized PHC facilities more frequently than the PBI group. The major differences between the two groups were variations in their knowledge and experiences. Although PBI groups do not need to pay for their medical expenses, financial barriers were not the only reason for the low utilization of PHC services. The study identified common reasons for poor utilization, such as difficulty in making appointments, the complexity of the NHI regulatory environment, crowded healthcare settings, lack of available information, and high level of referrals away from PHC, which were often made incorrectly. The types of NHI, accommodation and awareness (two of the six factors of utilization), significantly influenced the degree of utilization of PHC facilities by NHI participants.
In conclusion, all types of NHI participants showed low utilization of PHC. However, the study result showed that in terms of basic needs, the PBI group requires a higher targeted level of prioritization than the non-PBI group. In particular, the study showed that the two factors of utilization most in need of addressing are accommodation, and awareness.
Recommendations
Policymakers could leverage these findings to help improve health insurance utilization in Samarinda Municipality as well as regions with similar characteristics. All types of NHI participants should be prioritized. However, interventions should focus on strategies that both retain existing NHI participants whilst concomitantly distinguishing between the different needs of PBI and non-PBI clients of PHC services with a view to encouraging broader participation. Interventions should prioritize strategies that strengthen utilization of services with particular focus on “accommodation and awareness” factors.
Importantly, the findings could also guide stakeholders when planning and redesigning the existing health insurance scheme in accordance with the Gatekeeper Concept. The research suggests that prevention services could be significantly improved through information sharing and distribution on social media and other platforms. Moreover, the study suggests that by strengthening the capacity and quality of PHC settings, there will also be a reduction in the number of erroneous/incorrect referrals.
Further studies should employ a qualitative research design to observe other factors related to PHC utilization. It is also recommended that further comparative studies be undertaken in another region of Indonesia with a different target population to illuminate common and/or distinguishable issues experienced by other people under the NHS framework.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. World Health Organization. Universal Health Coverage: Moving Towards Better Health: Action Framework for the Western Pacific Region. Manila: WHO Regional Office for the Western Pacific; 2016.
2. Stuckler D, Feigl A, Basu S, Mckee M. The political economy of universal health coverage. Montreux, Switzerland: Background paper for the global symposium on health systems research. the First Global Symposium on Health Systems Research; 2010.
3. World Health Organization. Universal Health Coverage (UHC): World Health Organization; 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/universal-health-coverage-(uhc).
4. Agustina R, Dartanto T, Sitompul R, et al. Universal health coverage in Indonesia: concept, progress, and challenges. Lancet. 2018.
5. Health and Social Security Agency. Panduan Layanan Bagi Peserta JKN-KIS: BPJS Kesehatan; 2020.
6. Ministry of Health Indonesia. Health Services Regulation of National Health Insurance; 2013.
7. Health and Social Security Agency. Gatekeeper Concept Guideline. Jakarta, Indonesia; 2014. Available from: https://bpjs-kesehatan.go.id/.
8. Ministry of Health Indonesia. Guidelines for Clinical Practice for Doctors in Primary Health Care Facilities; 2014.
9. Health Social Security Agency. Buku Panduan Praktis Sistem Rujukan Berjenjang 2014. Available from: https://www.bpjs-kesehatan.go.id/bpjs/arsip/detail/37.
10. Badan Pusat Statistik (Central Bureau of Statistics). Urban and Rural Classification in Indonesia. Number. 2010;37:ed2010.
11. Badan Pusat Statistik (Central Bureau of Statistics). Statistik Kesejahteraan Rakyat (Statistics of People’s Welfare). Catalog. Jakarta, Indonesia: BPS-Statistics Indonesia; 2018. 2018-11-26. Contract No.: 04210.1814.
12. Ramadhani SN. Studi Literatur: analisis Faktor Penyebab Tingginya Angka Rujukan di Puskesmas Pada Era JKN Analysis of Factors Causing High Referral Rates at Primary Health Center in the JKN Era: a Literature Review. Media Gizi Kesmas. 2020;9(2):57. doi:10.20473/mgk.v9i2.2020.57-66
13. Werni S Gambaran Faktor Penyebab Rujukan Di Puskesmas Kota Depok. Buletin Penelitian Sistem Kesehatan. Buletin Penelitian Sistem Kesehatan. 2019.
14. Da Silva RB, Contandriopoulos A-P, Pineault R, Tousignant P. A Global Approach to Evaluation of Health Services Utilization: concepts and Measures. Healthcare Policy. 2011;6(28):106.
15. Penchansky R, Thomas JW. The concept of access: definition and relationship to consumer satisfaction. Med Care. 1981;19(2):127–140. doi:10.1097/00005650-198102000-00001
16. Russell DJ, Humphreys JS, Ward B, et al. Helping Policy‐makers Address Rural Health Access Problems. Aust J Rural Health. 2013;21(28):61–71. doi:10.1111/ajr.12023
17. Levesque J, Harris MF, Russell G. Patient-centred access to health care: conceptualising access at the interface of health systems and populations. Int J Equity Health. 2013;12:12. doi:10.1186/1475-9276-12-12
18. Saurman E. Improving access: modifying Penchansky and Thomas’s Theory of Access. J Health Services Res Policy. 2016;21(28):36–39. doi:10.1177/1355819615600001
19. Badan Pusat Statistik. Statistik Kesejahteraan Rakyat Kota Samarinda. Contract No.: 4101002.6472. Samarinda, Indonesia: Statistic of Samarinda City; 2019.
20. Astuti D The Correlation Between Health Services with Patient Satisfaction of JKN-KIS Participants in Primary Clinics Samarinda City. Bachelor thesis (Samarinda City: Mulawarman University). 2017.
21. Gyardani NA The Relationship between Healthcare Quality with Patient Satisfaction of BPJS Kesehatan at Individual Practice Physicians Service in 5 District of Samarinda. Bachelor thesis (Samarinda City: Mulawarman University). 2016.
22. IBM CORP. IBM SPSS Statistics for Windows. Version 25.0 Ed. Armonk, NY: IBM Corp; 2017.
23. Ministry of Health. Minimum Standard Services in Health Sector, 43. Sect. 2016;43.
24. Mayeka Y, Dwi, N, Rizalia, W. Determinan Pemanfaatan Pelayanan Kesehatan pada Peseta Jaminan Kesehatan Nasional (JKN) Kelompok PBI di Kota Jambi Tahun 2021. JIK-Jurnal Ilmu Kesehatan. 2022;6(2):294–301.
25. Manalu N. Determinan Pemanfaatan Pelayanan Kesehatan Oleh Peserta Penerima Bantuan Iuran (PBI) di Puskesmas Desa Lalang Kecamatan Medan Sunggal Tahun 2018: Universitas Sumatera Utara. 2019.
26. Nasution ZH. Faktor-Faktor yang Mempengaruhi Pemanfaatan Puskesmas oleh Peserta Penerima Bantuan Iuran Jaminan Kesehatan Nasional (JKN) di Kota Pematangsiantar Tahun. 2017. Universitas Sumatera Utara. 2018.
27. Rumengan DS, Umboh J, Kandou G. Faktor-faktor yang berhubungan dengan pemanfaatan pelayanan kesehatan pada peserta BPJS kesehatan di Puskesmas Paniki Bawah Kecamatan Mapanget Kota Manado. Jikmu. 2015;5(2):56.
28. Health Social Security Agency. The Norms for Determination of Capitation Amount and Capitalization Payment based on Fulfilment of Services Commitments at the Primary Health Care. 2015;2.
29. Wulandari C, Saptaputra S. Faktor yang berhubungan dengan pemanfaatan pelayanan kesehatan di UPTD puskesmas langara kecamatan wawonii barat kabupaten konawe kepulauan tahun 2016: haluoleo University. Asian Pacific Journal of Cancer Prevention: APJCP. 2016;17(3):1539–1546. doi:10.7314/apjcp.2016.17.3.1539
30. Truppa C, Leresche E, Fuller AF, et al. Utilization of primary health care services among Syrian refugee and Lebanese women targeted by the ICRC program in Lebanon: a cross-sectional study. Conflict and Health. 2019;13(1):7. doi:10.1186/s13031-019-0190-4
31. Utami SM, Swarjana IK, Satriani NLA. Factors associated with the utilization of health services among patients with hypertension during the Covid-19 pandemic: a cross-sectional study in West Lombok Regency, Indonesia. J Public Health Dev. 2022;20.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.