Back to Journals » Vascular Health and Risk Management » Volume 22
Utility of Novel Lipid Parameters for Risk Stratification in Patients with Diabetes and STEMI–from a Prospective Study
Authors Zhao X, Chen R ![]() , Li J, Zhou J, Li N, Xue L, Yan S, Liu C, Zhou P, Chen Y, Song L, Zhao H, Yan H
, Li J, Zhou J, Li N, Xue L, Yan S, Liu C, Zhou P, Chen Y, Song L, Zhao H, Yan H ![]()
Received 15 August 2025
Accepted for publication 16 January 2026
Published 30 January 2026 Volume 2026:22 560787
DOI https://doi.org/10.2147/VHRM.S560787
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Harry Struijker-Boudier
Xiaoxiao Zhao,1 Runzhen Chen,1 Jiannan Li,1 Jinying Zhou,1 Nan Li,1 Linghan Xue,1 Shaodi Yan,2 Chen Liu,1 Peng Zhou,1 Yi Chen,1 Li Song,1 Hanjun Zhao,1 Hongbing Yan1,3
1Department of Cardiology, Fuwai Hospital, National Center for Cardiovascular Diseases, Peking Union Medical College & Chinese Academy of Medical Sciences, Beijing, People’s Republic of China; 2Fuwai Hospital, Chinese Academy of Medical Sciences, Shenzhen, People’s Republic of China; 3Beijing Amcare Hospital, Beijing, People’s Republic of China
Correspondence: Hongbing Yan, Department of Cardiology, Beijing Amcare Hospital, Beijing, People’s Republic of China, Tel +86-13701339287, Email [email protected] Hanjun Zhao, Department of Cardiology, Fuwai Hospital, Chinese Academy of Medical Sciences, Beijing, People’s Republic of China, Tel +86-15210020808, Email [email protected]
Introduction: Abnormalities in glucose and lipid metabolism are prevalent among individuals suffering from myocardial infarction, with insulin resistance playing an integral role in these pathological processes. This study aims to follow up on incident ischemic stroke events to evaluate whether any alterations in risk estimation merit a reassessment of therapeutic strategies. Herein, we present findings derived from a prospective cohort engaged in this ongoing investigation.
Material and Methods: In our analysis, three novel lipid biomarkers—namely proprotein convertase subtilisin/kexin type 9, fatty acid-binding protein 4, and Resolvin D1—emanating from diverse pathophysiological pathways were meticulously evaluated alongside six conventional lipid parameters within a population cohort comprising 1580 individuals, both diabetic and non-diabetic.
Results: 1) Furthermore, among DM patients, group 1 (0– 1 lipid parameters increased) and group 2 (2– 4 lipid parameters increased) had significantly better ischemic stroke-free survival than other groups (p=0.025) when TyG index ≥median. 2) Adding novel lipid associated parameters and TyG index to the conventional lipid risk factors model in the cohort validated it by improved net reclassification index (p< 0.05) and integrated discrimination improvement and led to significant reclassification of individuals into risk categories.
Conclusion: The incorporation of a biomarker score that encompasses innovative lipid-associated biomarkers alongside the TyG index into a traditional risk assessment framework significantly enhanced the evaluation of ischemic stroke events within myocardial infarction populations afflicted by diabetes mellitus.
Keywords: triglyceride–glucose index, ischemic stroke, myocardial infarction, proprotein convertase subtilisin/kexin type 9, fatty acid-binding protein 4, Resolvin D1, lipid parameters
Introduction
Current guidelines from the American Heart Association/American Stroke Association (2018) emphasize intensive lipid-lowering therapy for the secondary prevention of ischemic stroke of atherosclerotic origin following transient ischemic attack (TIA) or ischemic stroke.1,2 Despite these established recommendations, residual cardiovascular risk remains substantial, particularly among patients with concurrent metabolic diseases. This persistent risk landscape underscores the critical need to refine and enhance risk stratification paradigms, moving beyond traditional lipid profiles to identify high-risk individuals who may benefit from more targeted or intensive therapeutic interventions. Within this context, the intricate interplay between glucose and lipid metabolism emerges as a pivotal area of investigation. Metabolic disturbances are highly prevalent in patients with established cardiovascular disease, such as myocardial infarction, with insulin resistance (IR) serving as a central pathophysiological mechanism.3–5 IR contributes significantly to endothelial dysfunction, atherogenic dyslipidemia, and a prothrombotic state, establishing it as a fundamental risk factor for both the onset and progression of cerebrovascular events.6–8 While the hyperinsulinemic-euglycemic clamp test remains the gold standard for quantifying IR, its clinical utility is severely constrained by procedural complexity, time demands, and cost.9 Consequently, the triglyceride-glucose (TyG) index, derived from readily available fasting triglyceride and glucose measurements, has emerged as a validated, practical, and reliable surrogate marker for IR assessment in both research and clinical settings.10 Its strong correlation with clamp-measured IR and proven prognostic value across cardiovascular outcomes makes it an ideal tool for large-scale risk stratification.
The pursuit of enhanced risk prediction has further stimulated interest in novel lipid-associated biomarkers that reflect distinct aspects of atherogenesis beyond conventional cholesterol measurements. These biomarkers potentially offer insights into diverse biological pathways, including cholesterol metabolism, inflammatory processes within plaques, and the resolution of inflammation. Preclinical evidence has demonstrated a significant upregulation of Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) in the brain following experimental ischemic stroke induced by transient middle cerebral artery occlusion, suggesting a role in the cerebral response to ischemia that extends beyond its established function in hepatic LDL receptor degradation.11,12 Simultaneously, Fatty Acid-Binding Protein 4 (FABP4), a lipid chaperone predominantly expressed in adipocytes and macrophages, has been implicated in vascular inflammation and plaque destabilization. Comprehensive genomic and histopathological analyses confirm its elevated expression within macrophages infiltrating carotid atherosclerotic plaques, particularly at sites of plaque rupture.13–15 FABP4 contributes to lipid accumulation, inflammatory cytokine production, and impaired endothelial function, thereby accelerating atherosclerosis progression. Notably, pharmacological inhibition of FABP4 in experimental stroke models has demonstrated therapeutic potential, effectively reducing ischemic lesion volume, mitigating cerebral edema, and preserving blood-brain barrier integrity during the acute phase of stroke.16,17
Furthermore, the role of specialized pro-resolving lipid mediators in the inflammatory aftermath of stroke has gained recognition. Resolvin D1 (RvD1), biosynthesized from the omega-3 fatty acid docosahexahexaenoic acid (DHA), plays a crucial role in actively terminating sterile inflammation and promoting tissue repair.18 In the context of cerebral ischemia, RvD1 enhances the phagocytic clearance of apoptotic neutrophils and cellular debris by microglia, reduces pro-inflammatory signaling, and facilitates neurological recovery. This mechanism represents a fundamental shift in understanding post-stroke inflammation, highlighting endogenous resolution programs as a critical therapeutic target.
Despite these compelling individual associations, a significant knowledge gap persists. It remains ambiguous whether the integration of a multi-biomarker panel—encompassing PCSK9, FABP4, and RvD1—can synergistically improve the precision of ischemic stroke risk assessment in high-risk populations, particularly among patients with diabetes mellitus (DM) where IR is a dominant feature. Furthermore, the incremental prognostic value of such a panel, when combined with the practical TyG index, over conventional lipid risk factors has not been systematically evaluated in a prospective cohort. Most critically, it is uncertain whether this refined risk stratification would yield clinically meaningful reclassification of patients, potentially informing more personalized secondary prevention strategies.
Therefore, this prospective study aims to determine whether a biomarker score incorporating PCSK9, FABP4, and RvD1, combined with the TyG index, significantly improves the estimation of incident ischemic stroke risk in a diabetic population with established cardiovascular disease, beyond conventional lipid parameters. We further seek to evaluate whether this integrated approach results in significant net reclassification improvement, thereby providing a framework for future tailored therapeutic interventions.
Materials and Methods
Cohort Description
The China Risk, Genetics, Archiving, and Monograph (CRGAM) project is a longitudinal and prospective population-based study aimed at individuals aged 18 years and older who have experienced ST-Elevation Myocardial Infarction (STEMI) and are undergoing primary Percutaneous Coronary Intervention (PCI). This study was initially designed to develop cardiovascular risk scores based on established conventional risk factors, while also assessing whether the integration of genetic or biomarker variations could improve these risk scores.
The research was carried out in a large-volume national tertiary care institution—Fuwai Hospital in Beijing, China—which specializes in cardiovascular diseases. The hospital has consecutively enrolled patients who underwent emergency coronary angiography following a diagnosis of Acute Myocardial Infarction (AMI) from March 2017 to January 2020 (as illustrated in Figure 1). The project’s objectives and detailed descriptions of the cohorts have been published elsewhere.19,20 The primary endpoint is defined as the first occurrence of a major cardiovascular event during the follow-up period. This encompasses recurrent fatal or non-fatal definite myocardial infarction; all-cause or unclassifiable death; ischemic stroke; cardiac revascularization; heart failure; or unstable angina.
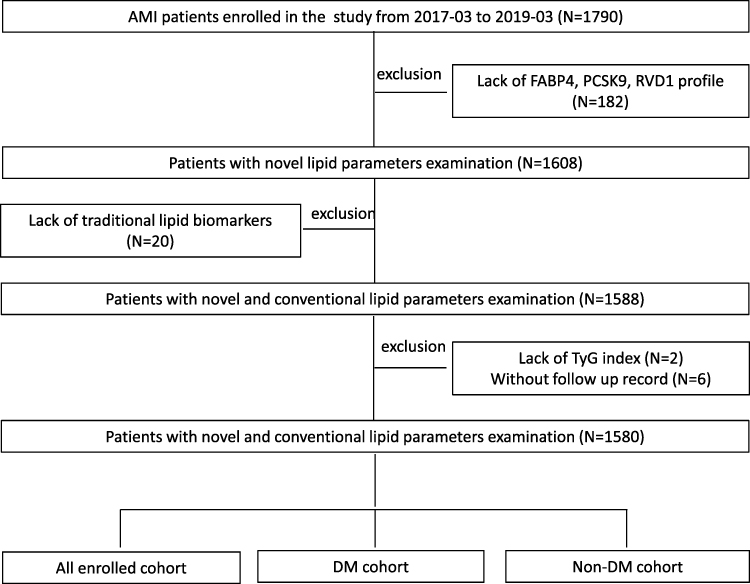 |
Figure 1 Flow chart. Abbreviations: DM, diabetes mellitus; FABP4, Fatty acid-binding protein 4; PCSK9, proprotein convertase subtilisin/kexin type 9; RvD1, Resolvin D1. |
Exclusion criteria encompassed a history of serum creatinine levels exceeding 2.5 mg/dL, signs of cardiogenic shock, absence of measurements for traditional plasma lipid parameters as well as FABP4, PCSK9, Resolvin D1, and lack of follow-up records. The study protocol adhered to the principles outlined in the Declaration of Helsinki and received approval from the ethics committee at our institution (No. 2017–866). Written informed consent was obtained from all participants.
We evaluated biomarkers to assess the discriminative capacity achieved by combining six traditional lipid markers with three novel biomarkers—specifically FABP4, PCSK9, and Resolvin D1—in enhancing risk prediction within the studied cohorts. Notably, this combination demonstrated superior performance relative to traditional lipid markers in terms of discrimination and calibration among diabetes patients included in the discovery set. These three novel biomarkers exhibit low correlation amongst one another and represent distinct biological pathways: Resolvin D1 serves as a marker for vascular function and neurohormonal activity; PCSK9 is an inflammatory marker associated with plaque development and progression; while FABP4 indicates myocardial injury.
Blood Samples Collection and Measurements
Venous blood samples for complete blood count, basic metabolic panel (including parameters such as creatinine and glucose), cardiac troponin I (cTnI), and N-terminal prohormone of brain natriuretic peptide (NT-proBNP) were collected into tubes containing ethylene diamine tetraacetate (EDTA) prior to percutaneous coronary intervention (PCI). These samples were subsequently centrifuged at 2000 × g for 15 minutes at room temperature, and the resulting plasma was frozen for PCSK9 analysis and stored at −80 °C until further examination. Enzyme-linked immunosorbent assays (ELISA) were conducted on the MultiSkan MK3 instrumental platform (Thermo Scientific).
Blood cell counts were performed using an automatic hematology analyzer (XT-1800i; Sysmex Corporation). The concentrations of blood glucose and creatinine were measured with an automatic biochemistry analyzer (Hitachi 7150, Tokyo, Japan), following standard protocols established by the core laboratory. Blood samples for the determination of FABP4, RvD1, and PCSK9 levels were obtained via radial or femoral access before the initiation of coronary angiography using vacutainer tubes containing EDTA. These samples underwent immediate centrifugation at 2000 × g for 15 minutes at room temperature for plasma isolation, followed by storage at −80 °C until subsequent analysis. Measurements of plasma FABP4 (HK321; HyCult Biotechnology, Uden, Netherlands) and PCSK9 (DY3888; R&D Systems, Minneapolis, MN, USA) were performed utilizing enzyme-linked immunosorbent assays according to manufacturer’s instructions; results were compared with purified human PCSK9 standards. Additionally, blood samples for lipid profiles and other routine tests were collected from the cubital vein immediately upon patient admission to the coronary care unit. The plasma concentrations of triglycerides, LDL-C, and HDL-C were assessed using an automatic biochemistry analyzer (Hitachi 7150, Tokyo, Japan). Serum levels of lipoprotein(a) [lp(a)] were determined via the immunoturbidimetry method (LASAY Lp(a) auto, SHIMA Laboratories Co., Ltd., Tokyo, Japan). Hemoglobin A1c (HbA1c) levels were measured with the Tosoh Automated Glycohemoglobin Analyzer (HLC-723G8, Tokyo, Japan). The level of high-sensitivity C-reactive protein was quantified using immunoturbidimetry (Beckmann Assay, Bera, CA, USA).
Baseline data, encompassing patient clinical demographics such as age, sex, smoking status, and medical history (including hypertension, diabetes, hyperlipidaemia, and chronic kidney disease), as well as details regarding percutaneous coronary intervention (PCI), laboratory results, primary PCI procedures, and pharmacological treatments were extracted from hospital records. Serum levels of fatty acid-binding protein 4 (FABP4), lipid profiles, and inflammatory biomarkers were assessed using standard laboratory techniques at Fuwai Hospital.
Endpoints and Follow-Up
Ischemic vascular events were defined as a composite outcome encompassing ischemic stroke, non-fatal myocardial infarction (MI), and cardiovascular mortality. Stroke was diagnosed based on the presence of rapidly developing focal or widespread neurological dysfunction lasting more than 24 hours or resulting in death, with non-vascular causes excluded. Non-fatal MI was identified through typical chest pain symptoms or alterations observed in serial electrocardiograms, corroborated by positive cardiac troponin levels.
A clinical follow-up assessment was conducted after three years utilizing direct interviews, telephone calls, and hospital discharge records or clinical notes pertaining to cases of death. This follow-up process involved well-trained physicians and nurses who engaged with the participants enrolled in the study. Approval for the follow-up protocol was obtained from the Institutional Review Board of Fuwai Hospital. The trained physicians overseeing follow-up assessed primary endpoints including angina pectoris, cardiac death, all-cause mortality, non-fatal MI, revascularization procedures, heart failure incidents, ischemic strokes, hemorrhagic strokes, and bleeding events. They systematically identified and extracted relevant data concerning these endpoints from hospital records, laboratory reports, emergency records, medical charts, and clinical notes that were necessary to be submitted to our centers. Confirmation of clinical endpoints was performed by more than two independent professional physicians who remained blinded to both clinical data and angiographic findings.
Statistical Analysis
The distribution of outcome variables was evaluated using the Kolmogorov–Smirnov test. Continuous data are presented as median values (median ± standard deviation) in cases of both normal and non-normal distributions. Between-group differences were analyzed employing either an independent samples t-test or the Mann–Whitney U-test, corresponding to normally and non-normally distributed data, respectively. Categorical data are reported as counts (percentages) and were compared using Pearson’s chi-squared (χ2) test or Fisher’s exact test, as appropriate. Multivariable Cox proportional hazards regression models, adjusted for confounding factors, were utilized to assess the associations between lipid parameters combined with TyG and the incidence of ischemic cardiovascular events. Kaplan-Meier survival curves were constructed to evaluate the incidence rates of major adverse cardiovascular events (MACE) and ischemic cardiovascular events among groups stratified by the number of risk lipid factors. Discrepancy rates of cumulative events were compared utilizing the Log rank test. The discriminative ability of multivariable models was assessed by computing the c statistic, Integrated Discrimination Improvement (IDI), and Net Reclassification Index (NRI), which were compared using a nonparametric approach. Analyses were conducted with SAS version 9.1.3 (SAS Institute Inc., Cary, NC). The authors had complete access to all data and take full responsibility for its integrity. All authors have read and agreed upon the manuscript as written. Statistical analyses employed SPSS (version 20.0; IBM Corp., Armonk, NY, USA), R Programming Language X64 4.0.4 (R Foundation for Statistical Computing, Vienna, Austria), and MedCalc version 18.2.1 (MedCalc Software, Ostend, Belgium). Statistical significance was set at P < 0.05; all P values are two-tailed.
We searched the MR Base database (http://www.mrbase.org/), which houses a comprehensive collection of summary statistic data from numerous genome-wide association studies (GWASs). As our exposure, we employed the publicly available summary statistics data sets from GWAS meta-analyses focused on FABP4 in individuals of European descent (n = 3394; ID: prot-b-71). A two-sample Mendelian randomization study was conducted using genetic variants associated with BMI as instrumental variables (IVs) to enhance inference, applying a P-value threshold of 5.00E-08 for genome-wide significance. We obtained summary statistics, including beta coefficients and standard errors, for two single nucleotide polymorphisms (SNPs) linked to FABP4 from the relevant GWAS. The outcome variable was derived from publicly available summary statistic data sets corresponding to self-reported ischemic stroke cases included in the IEU GWAS QC Report (total n = 440328; cases = 34217, controls = 406111; ID: ebi-a-GCST005843) (see Supplement Tables 1 and 2). This analysis was performed using R Programming Language version X64 4.0.4.
Results
Baseline Biomarkers and Baseline Characteristics
A total of 1790 patients met the initial inclusion criteria, 6 (0.34%) of whom were lost to follow-up and 204 (11.6%) of whom were not available baseline measurements of traditional and novel lipid parameters. The baseline characteristics of the 210 patients were similar to the patients enrolled in this cohort. The detailed baseline characteristics of the final cohort are shown in Table 1 and baseline measurements of traditional and novel lipid parameters were available in 1580 patients. Among 1580 patients, 1037 (65.6%) patients were non-DM and 543 (34.4%) patients were DM. 1032 (65.3%) patients had a history of hypertension, 1426 (90.3%) had hyperlipidemia, 1109 (70.6%) had current smoking. The median concentration of FABP4 was 5.9ng/mL, and the 25th and 75th percentiles were 2.9 and 9.8ng/mL, respectively. Notably, when baseline characteristics were evaluated according to history of DM, those with DM had significantly higher mean FABP4 levels (means and interquartile ranges [IQRs]; 6.2 [2.9, 11.2] versus 5.8 [2.8, 9.4], p=0.028), higher mean Resolvin D1 levels (IQRs: 168.2 [74.4, 341.7] versus 142.6 [67.3, 306.6], p=0.044), and a more frequent cluster of common cardiovascular risk factors (elderly, hypertension, Hyperlipidemia, History of MI, higher active greater triglyceride levels, higher hs-CRP levels, and higher level of inflammation index including pentraxin 3, Lipoxin A4 and hs-CRP levels). The prevalence of individual medical and demographic characteristics and the intersections of lipid parameters risk factors and TyG index according to history of DM (Figure 2A) and non-DM (Figure 2B). During a mean follow-up period of 2.16 ± 1.17 years (median, 2.02 years), a total of 449 (28.4%) patients reached the primary endpoint, of whom 109 (6.9%) patients had all-cause mortality (61 had cardiac death), 88 (5.6%) patients had recurrence MI, 62 (3.9%) had ischemic stroke.
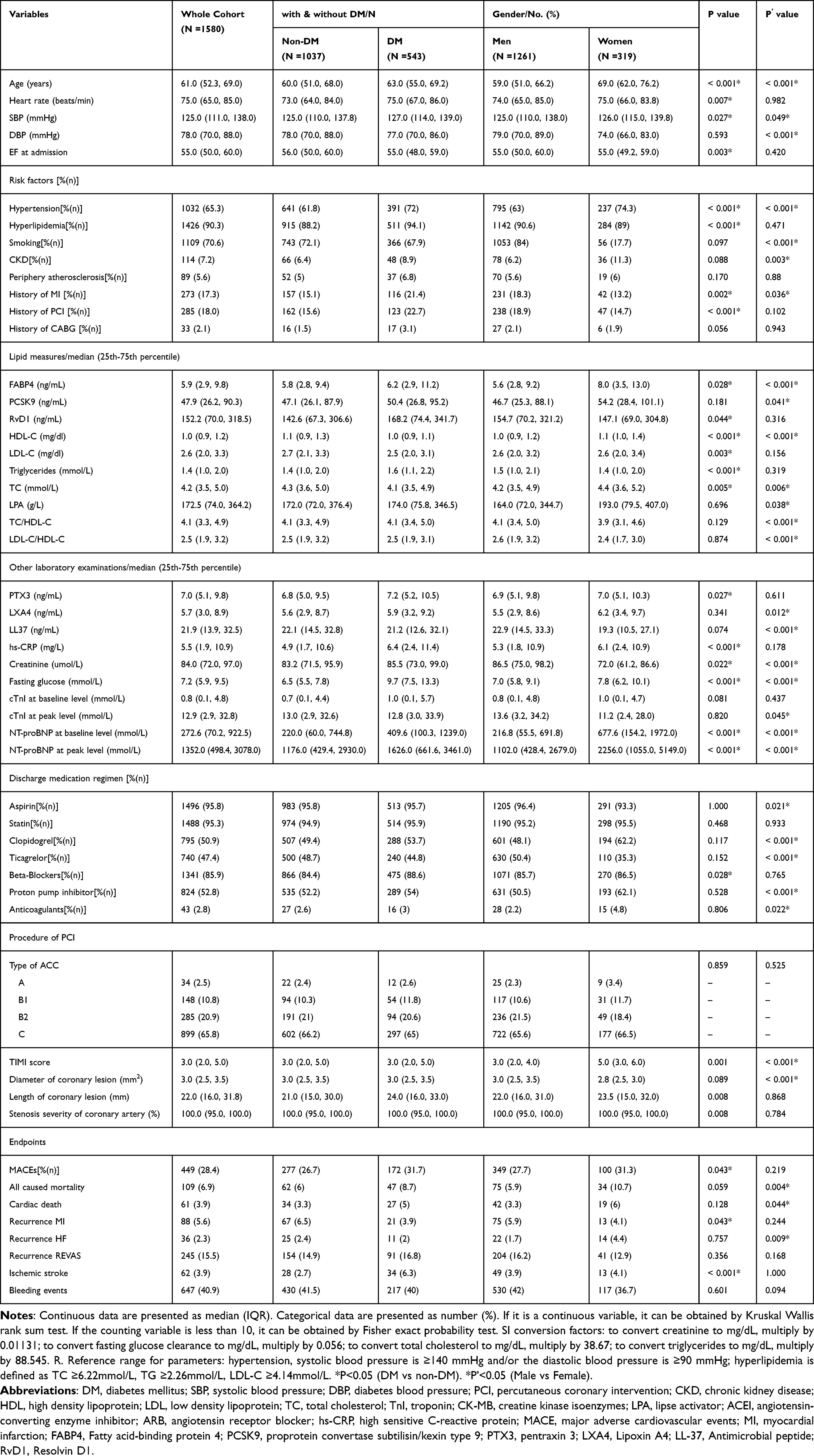 |
Table 1 Baseline Clinical and Laboratory Characteristics of the Study Population |
 |
Figure 2 Upset plot of factors and intersections of traditional and novel lipid parameters (group of TG, LDL, TC, ration of TC to HDL-C, ratio of LDL-C to HDL-C, lpa, FABP4, PCSK9, RvD1) and TyG index according to history of DM (A) and non-DM (B). Abbreviations: TyG, triglyceride glucose; DM, diabetes mellitus; HDL, high density lipoprotein; LDL, low density lipoprotein; Lpa, lipse activator; TC, total cholesterols, TG, triglyceride; FABP4, Fatty acid-binding protein 4; PCSK9, proprotein convertase subtilisin/kexin type 9; RvD1, Resolvin D1. |
Association of Traditional and Novel Lipid Parameters with Incident Cardiovascular Events in Subgroups
We describe the fully adjusted multivariable relationships between major adverse cardiovascular events (MACEs), stratified by the number of elevated lipid parameters and risk factor subgroups among patients with diabetes mellitus (DM) (see Supplement Table 3) and non-diabetes mellitus (non-DM) populations (see Supplement Table 4). We categorized the subjects into four distinct groups based on the number of lipid parameters assessed. These parameters included traditional lipid biomarkers 【LDL-C (median value=1.80 mg/dl), triglycerides (median value=2.31 mmol/L), total cholesterol (median value=5.19 mmol/L), lipoprotein(a) (median value=141g/L), TC/HDL-C ratio (median value=4.06), and LDL-C/HDL-C ratio (median value=2.53)】 as well as novel lipid-associated indices FABP4 (median value=5.87 ng/mL), PCSK9 (median value=47.99 ng/mL) and RvD1 (median value=152.21 ng/mL). The groups are sequentially defined as follows: the first group consists of 0–1 elevated lipid parameters; the second group includes 2–4 elevated parameters; the third group encompasses 5–7 elevated parameters; and the fourth group comprises 8–9 elevated lipid parameters. In the group with lower TyG levels, we observed a significant decrease in MACEs in the first group within the DM population (hazard ratio [HR]: 0.31; 95% confidence interval [CI]: 0.12–0.81; P = 0.017), whereas no such association was found among patients with higher TyG levels. Moreover, in male patients specifically, an increasing number of elevated lipid parameter indices was associated with a progressively greater incidence of MACEs over time: for group two HR was indicated at 0.27 (95% CI: 0.12–0.59; P = 0.001); for group three HR stood at 0.42 (95% CI: 0.19–0.90; P =0.0026), as determined by our fully adjusted Cox regression models.
Biomarker Improvement in Cardiovascular Risk Estimation
The forest plot displaying fully adjusted hazard ratios for biomarker associations with incident cardiovascular events is presented in Figure 3. Kaplan-Meier curves illustrate cumulative stroke rates over a median follow-up period of 2.02 years, stratified by the number of increased lipid parameters in patients with and without DM, based on the median level of the TyG index (Figure 4). Among DM patients, there were no significant differences observed when the TyG index was below the median (Figure 4A). Conversely, among DM patients, Group 1 (0–1 lipid parameters increased) and Group 2 (2–4 lipid parameters increased) demonstrated significantly improved ischemic stroke-free survival compared to other groups when the TyG index was at or above its median value (p = 0.025; Figure 4B). Additionally, among non-DM patients, the Kaplan-Meier curve revealed no significant differences regarding the number of increased lipid parameters when the TyG index was below the median (Figure 4C). Similarly, for non-DM patients, significant differences in stroke-free survival were noted concerning the number of elevated lipid parameters when the TyG index reached or exceeded its median threshold (p < 0.001; Figure 4D). In our Kaplan–Meier analysis, we found no statistically significant differences in major adverse cardiovascular events (MACE) and ischemic stroke survival either among all enrolled participants or specifically within non-DM individuals (all P > 0.05; see Supplementary Figure 1A–H).
 |
Figure 3 Fully adjusted HRs of biomarkers for incident cardiovascular events. Adjusted confounders include gender, age, smoking status, hypertension, hyperlipidemia, diabetes mellitus, stroke history, white blood cell count, hemoglobin level, platelet count, serum creatinine level, fasting glucose level, glycosylated hemoglobin level, high-sensitivity C-reactive protein levels and discharged medications including Aspirin, Ticagrelor, Clopidogrel, ACEI&ARB agents; β blockers; statins; along with a history of chronic renal disease; peripheral arteriosclerosis; myocardial infarction; coronary stent implantation; coronary artery bypass grafting; height; weight; heart rate; systolic and diastolic blood pressure at baseline. |
 |
Figure 4 Kaplan-Meier curves illustrating cumulative stroke rates over a median of 2.02 years based on the number of increased lipid parameters in patients with and without DM, categorized by TyG levels. (A) displays curves for DM patients when TyG < median. (B) shows curves for DM patients when TyG ≥ median. (C) presents curves for non-DM patients when TyG < median. (D) depicts curves for non-DM patients when TyG ≥ median. Abbreviations: DM, diabetes mellitus; TyG, triglyceride glucose. |
Discrimination of Biomarker Score and Improvement in Cardiovascular Risk Estimation
We computed detailed results for the Net Reclassification Improvement (NRI), Integrated Discrimination Improvement (IDI), and median improvement in the risk model associated with a conventional risk-estimation model that utilized classic risk factors alone. These results were then compared to models incorporating both traditional risk factors and each biomarker individually. Detailed findings regarding NRI, IDI, median improvement in the risk model, and hazard ratios are presented in Table 2 for both traditional and novel lipid-related markers as well as the TyG index. In our cohort, adding novel lipid-associated parameters alongside the TyG index to the conventional lipid risk factors model validated its effectiveness by demonstrating improved NRI (p < 0.05) and IDI (p < 0.05), which resulted in significant reclassification of individuals into different risk categories. Notably, among patients experiencing incidence events, biomarkers such as FABP4, PCSK9, RvD1 (p < 0.05), and the TyG index (p < 0.05) independently contributed to an increase in median improvement of the risk score related to future cardiovascular risks. However, these findings were not consistently replicated across all enrolled cohorts exhibiting major adverse cardiovascular events (MACE). Overall, when considering IDI metrics comprehensively across incidents of ischemic stroke within all enrolled subjects—regardless of diabetes status—it was observed that lipid biomarkers and TyG index significantly enhanced model discrimination.
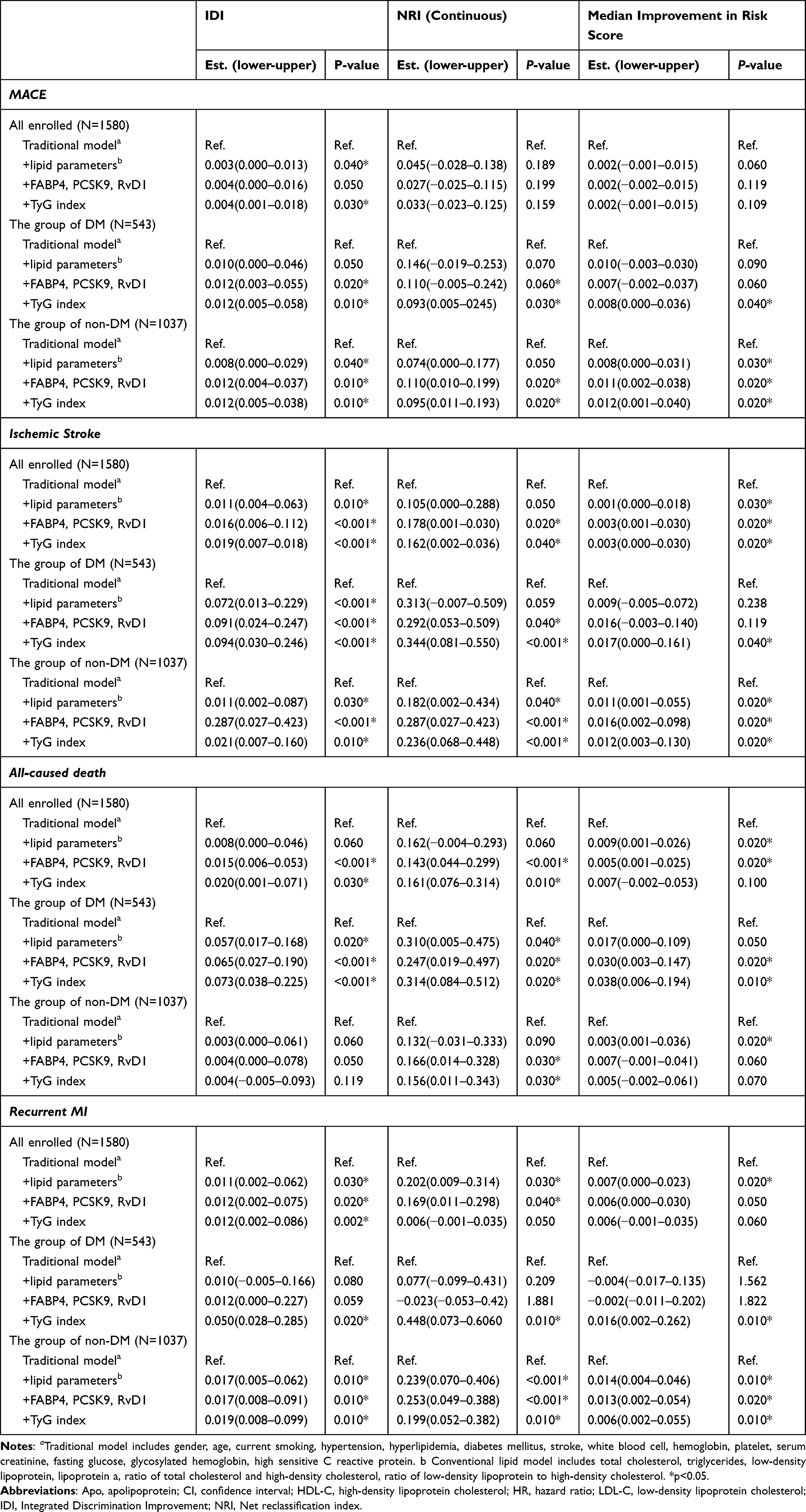 |
Table 2 Discrimination, and Calibration Estimates of Different Lipid Measures for Coronary Heart Disease During Follow-Up |
Discussion
We meticulously computed an array of detailed results encompassing the Net Reclassification Improvement (NRI), Integrated Discrimination Improvement (IDI), and the median enhancement within the risk model, all stemming from a conventional risk-estimation framework that exclusively relied on traditional risk factors. These insightful findings were then juxtaposed with models that integrated both classical risk determinants and each biomarker in isolation. Comprehensive data regarding NRI, IDI, median improvement in the risk model, as well as hazard ratios are delineated in Table 2 for both established and novel lipid-related biomarkers, including the TyG index. Within our cohort, the integration of innovative lipid-associated parameters along with the TyG index into the traditional lipid risk factor model not only validated its efficacy but also manifested significant advances in NRI (p < 0.05) and IDI (p < 0.05). This integration facilitated substantial reclassification of individuals across divergent risk strata. Remarkably, among patients who experienced incident events, biomarkers such as FABP4, PCSK9, RvD1 (p < 0.05), alongside the TyG index (p < 0.05), independently contributed to a notable elevation in median enhancements of future cardiovascular risk scores. However, it is imperative to note that these findings were not consistently replicated across all enrolled cohorts experiencing major adverse cardiovascular events (MACE). In summation—when scrutinizing IDI metrics holistically across cases of ischemic stroke amongst all enrolled subjects—that do not discriminate based on diabetes status—it became evident that lipid biomarkers coupled with the TyG index significantly bolstered model discrimination capabilities.
Recommendations for individuals who have experienced a stroke, informed by insights garnered from the Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) trial, suggest a noteworthy 16% relative risk reduction associated with the daily administration of 80 mg atorvastatin compared to placebo among stroke patients devoid of known coronary artery disease. Moreover, an analytical sub-study unveiled a remarkable relative risk reduction of 33% in those participants randomly assigned with carotid stenosis.21 It is particularly important to highlight that patients suffering from strokes concurrently afflicted by diabetes mellitus (DM) constitute approximately 20% of ischemic stroke cases across Europe, soar to 25% in Asia, and can reach as high as 38% in certain locales.22 Within the SPARCL trial focusing on diabetic patients receiving a regimen of 80 mg atorvastatin per day versus placebo, an impressive 30% diminution was observed in the five-year relative risk of recurrent strokes. Furthermore, there was a marked decrease amounting to 50% concerning any coronary heart disease event and an astonishing reduction of 64% related to revascularization procedures.23 Nonetheless, while an uptick in hemorrhagic stroke incidence over five years was documented—an effect insufficient to overshadow the therapeutic advantages conferred by atorvastatin—this facet merits meticulous contemplation within clinical practice contexts.24 Another significant adverse occurrence noted during treatment was approximately a 30% rise in newly diagnosed DM cases.25 Our data aligns consistently with findings derived from various population-based studies that illustrate associations between multiple biomarkers and emerging cardiovascular events. Notably, we meticulously constructed our biomarker score within an extensive prospective cohort concentrated on myocardial infarction subsequent to primary percutaneous coronary intervention (PCI). This methodological framework empowered us to exhibit significantly enhanced parameters regarding discrimination, calibration, and reclassification metrics.
It has been substantiated that PCSK9 may exert a profound influence on glucose homeostasis and the risk of type 2 diabetes, thereby unveiling an alternative pathway through which it could impact neurodegenerative diseases.26 Furthermore, insulin resistance can precipitate endothelial dysfunction directly,27 representing a pivotal pathophysiological mechanism in the progression of atherosclerosis. This dysfunction is likely to compromise cardiac autonomic function and amplify sympathetic nervous system activity.28 Human genetic investigations have elucidated connections between numerous gain-of-function mutations in the PCSK9 gene and an augmented risk of ischemic stroke correlated with elevated plasma LDL-C levels. Recent scholarly discourse surrounding Chinese patients afflicted by cerebral ischemic stroke underscored gain-of-function variants rs1711503 and rs2479408 as exhibiting strong correlations with this affliction.29 Additionally, analysis from the Belgium Stroke Study scrutinized the rs505151 variant among Central Europeans enduring small-vessel occlusion or large-vessel atherosclerosis. The findings revealed that this variant was associated with heightened plasma LDL-C levels, exacerbated severity of coronary atherosclerosis, and increased risk for stroke.30,31 Furthermore, supplementary randomized controlled trials (RCTs) examining the efficacy of PCSK9 inhibitors in patients already receiving maximum tolerable doses of statins or those exhibiting statin intolerance have revealed significant reductions in the incidence of stroke within populations categorized as high and very high cardiovascular risk.32 Mice with a Pcsk9–/– genotype manifest hyperglycemia, hypo-insulinemia, and compromised glucose tolerance, which incite apoptosis and inflammation within endocrine cells.33 The promotion of ischemic pathogenesis in cerebral regions stems from mechanisms associated with impaired insulin secretion and signaling pathways—resulting in protein hyperphosphorylation, elevated production of inflammatory cytokines, followed by consequent oxidative stress.34 Our investigation employed a pioneering strategy for gauging cardiovascular disease risk among adults through the integration of promising biomarkers derived from multiple testing modalities. This innovative approach encompassed the evaluation of three advanced lipid biomarkers arising from distinct pathophysiological pathways, alongside six conventional lipid metrics. The study cohort comprised 1580 individuals diagnosed with diabetes mellitus (DM) as well as non-DM participants who experienced myocardial infarctions; over a median follow-up duration spanning 2.02 years, a total of 449 new cardiovascular events were documented—including both fatal and non-fatal incidents related to coronary events or ischemic strokes.
The quantification of FABP4 in vulnerable human plaques35 and genome-wide expression analyses of isolated macrophages14 have shown that the expression levels of FABP4 are elevated in ruptured and vulnerable plaques. In contrast, a naturally occurring low-expression variant of FABP4 has been associated with enhanced plaque stability, thus reducing the risk of cardiovascular events.36,37 When comparing control ApoE-knockout mice to FABP4/ApoE double-knockout mice, notable reductions in atherosclerosis progression were observed without significant differences in serum lipids or insulin sensitivity.14 These findings suggest that FABP4 plays a critical role in the development of atherosclerosis; moreover, macrophage-derived FABP4 may exert marked local pathogenic effects related to this condition independent from its established roles in systemic glucose or lipid metabolism. The effect of FABP4 on vascular stability following ischemic stroke is particularly noteworthy due to its association with bleeding, edema, and blood-brain barrier damage—all factors contributing to clinical deterioration and adverse outcomes. A considerable body of literature indicates that the activity of FABP4 affects c-Jun N-terminal kinase signaling pathways along with metalloproteinase-9; these appear to be crucial mediators within the detrimental cascade initiated by upregulation of FABP4 during stroke events.37
A previous study18 focused on the effects of RvD1 on microglial phagocytosis of neutrophils during ischemic stroke. It explored how RvD1 regulates microglial energy metabolism to elucidate its underlying mechanisms.38 The findings indicated that RvD1 not only promoted microglial phagocytosis of neutrophils but also reprogrammed energy metabolism, thereby alleviating neurological injury and neuro-inflammation associated with ischemic stroke. Recent studies have further established that RvD1 plays a crucial role in mitigating neuroinflammation across various neurological ailment, including ischemic stroke.38 Additionally, RvD1 was found to reduce neutrophil accumulation and neuroinflammation following ischemic stroke by enhancing tight junction protein expression and protecting the blood-brain barrier during subarachnoid hemorrhage.18 Notably, administration of RvD1 resulted in decreased neutrophil accumulation, reduced NET formation, preservation of neuronal survival, and improvements in motor function as well as memory ability—all contributing to an alleviation of neuroinflammation post-stroke.
Limitation
Several limitations of the present study warrant consideration. First, although biomarkers were measured at baseline, their temporal variability and the potential influence of acute phase reactions following myocardial infarction on levels of PCSK9, FABP4, and RvD1 cannot be entirely ruled out, despite standardized pre-PCI sampling. Serial measurements could provide valuable insights into their stability and dynamic relationship with risk. Second, the study cohort comprised exclusively Chinese patients with STEMI undergoing primary PCI—a population characterized by intrinsically high cardiovascular risk. This specificity limits the generalizability of our findings to other ethnic groups or to patients with non-STEMI or stable coronary artery disease, as well as in primary prevention contexts. The external validity of the derived biomarker panel necessitates validation in independent multi-ethnic cohorts. Third, despite meticulous adjustment for a comprehensive set of clinical confounders, there remains a possibility of residual confounding from unmeasured or imperfectly quantified factors (eg, diet, physical activity, medication adherence beyond discharge), which is an inherent limitation in any observational study. Fourth, while our clinical data suggest a synergistic effect between the biomarker panel and the TyG index—particularly among diabetic individuals—the underlying mechanisms remain inadequately elucidated. Further experimental and mechanistic studies are essential to unravel the pathophysiological interplay between insulin resistance and represented pathways (hepatic LDL metabolism via PCSK9; macrophage-driven inflammation via FABP4; inflammation resolution via RvD1) concerning cerebrovascular risk. Finally, although our Mendelian randomization analysis for FABP4 supports a potential causal role within this context, similar genetic instrumentation for PCSK9 and RvD1 was not conducted; thus it warrants future investigation to strengthen causal inference across the entire panel.
Conclusion
In this prospective cohort of patients with established cardiovascular disease, we demonstrate that a multi-biomarker panel integrating PCSK9, FABP4, and RvD1—reflecting distinct pathways of lipid metabolism, vascular inflammation, and inflammation resolution—provides significant incremental prognostic value for incident ischemic stroke risk beyond conventional lipid parameters, particularly in individuals with diabetes mellitus. Crucially, the combination of this biomarker panel with the practical TyG index, a surrogate of insulin resistance, yielded substantial improvement in risk discrimination and led to clinically meaningful net reclassification of patients. These findings underscore the pivotal interplay between dysglycemia and multifaceted lipid-inflammatory pathways in propagating residual cerebrovascular risk. Our results advocate for a paradigm shift in risk stratification post-myocardial infarction, moving beyond low-density lipoprotein cholesterol-centric approaches.
The integrated use of the TyG index and a novel lipid-associated biomarker score holds promise for identifying a high-risk phenotype that may benefit from intensified surveillance and potentially from targeted therapies modulating the PCSK9, FABP4, or specialized pro-resolving mediator pathways. Future randomized trials are essential to determine whether therapeutic strategies guided by this refined risk assessment can effectively improve stroke outcomes in this vulnerable population.
Ethics Approval and Consent to Participate
The ethics committee of the Department of Cardiology, Fuwai Hospital, National Center for Cardiovascular Diseases, Peking Union Medical College, China approved this study.
Consent for Publication and Data Availability
Written informed consent for publication was obtained from all participants. The datasets used and/or analyzed during this study are available from the corresponding author Hongbing Yan on reasonable request.
Acknowledgments
The authors gratefully acknowledge all individuals who participated in this study. This paper has been uploaded to ResearchSquare as a preprint: https://www.researchsquare.com/article/rs-4331946/v1.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by National Natural Science Foundation of China (number:82400410); the National Clinical Research Center of Cardiovascular Diseases, Shenzhen. Fuwai Hospital Chinese Academy of Medical Sciences, Shenzhen (Grant No NCRCSZ-2024-003); Shenzhen Clinical Research Center for Cardiovascular Disease Fund (No.20220819165348002); CAMS Innovation Fund for Medical Sciences (2023-I2M-C&T-B-069); Fund of “Sanming” Project of Medicine in Shenzhen (number: SZSM201911017) and Shenzhen Key Medical Discipline Construction Fund(number: SZXK001).
Disclosure
No potential conflicts of interest are declared by the authors.
References
1. Loh HC, Lim R, Lee KW, et al. Effects of vitamin E on stroke: a systematic review with meta-analysis and trial sequential analysis. Stroke Vasc Neurol. 2021;6:109–17. doi:10.1136/svn-2020-000519
2. American Heart Association Stroke Council; Powers WJ, Rabinstein AA, Ackerson T, et al. 2018 guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2018;49(3):e46–e110. doi:10.1161/STR.0000000000000158
3. Fonseca AC, Merwick Á, Dennis M, et al. European Stroke Organisation (ESO) guidelines on management of transient ischaemic attack. Eur Stroke J. 2021;6(2):CLXIII–CLXXXVI. doi:10.1177/2396987321992905
4. Di Pino A, DeFronzo RA. Insulin resistance and atherosclerosis: implications for insulin-sensitizing agents. Endocr Rev. 2019;40:1447–1467.
5. Beverly JK, Budof MJ. Atherosclerosis: pathophysiology of insulin resistance, hyperglycemia, hyperlipidemia, and inflammation. J Diabetes. 2020;12:102–104. doi:10.1111/1753-0407.12970
6. Bornfeldt KE, Tabas I. Insulin resistance, hyperglycemia, and atherosclerosis. Cell Metab. 2011;14:575–585. doi:10.1016/j.cmet.2011.07.015
7. Poznyak A, Grechko AV, Poggio P, et al. The diabetes mellitus-atherosclerosis connection: the role of lipid and glucose metabolism and chronic inflammation. Int J Mol Sci. 2020;21(5):1835. doi:10.3390/ijms21051835
8. Huo RR, Liao Q, Zhai L, et al. Interacting and joint effects of triglyceride-glucose index (TyG) and body mass index on stroke risk and the mediating role of TyG in middle-aged and older Chinese adults: a nationwide prospective cohort study. Cardiovasc Diabetol. 2024;23(1):30. doi:10.1186/s12933-024-02122-4
9. Cersosimo E, Solis-Herrera C, Trautmann M, et al. Assessment of pancreatic β-cell function: review of methods and clinical applications. Curr Diabetes Rev. 2014;10(1):2–42. doi:10.2174/1573399810666140214093600
10. Hong S, Han K, Park CY. The triglyceride glucose index is a simple and low-cost marker associated with atherosclerotic cardiovascular disease: a population-based study. BMC Med. 2020;18:361. doi:10.1186/s12916-020-01824-2
11. Katsuki S, K. Jha P, Lupieri A. Proprotein Convertase Subtilisin/Kexin 9 (PCSK9) promotes macrophage activation via LDL receptor-independent mechanisms. Circ Res. 2022;131(11):873–889. doi:10.1161/CIRCRESAHA.121.320056
12. Wang J, Li S, Ren Y, et al. The impact of PCSK9 gene polymorphisms on ischemic stroke: a systematic review and meta-analysis. J Integr Neurosci. 2024;23(3):62. doi:10.31083/j.jin2303062
13. Huang Y, Hertzel AV, Fish SR, et al. TP53/p53 facilitates stress-induced exosome and protein secretion by adipocytes. Diabetes. 2023;72(11):1560–1573. doi:10.2337/db22-1027
14. Lee K, Santibanez-Koref M, Polvikoski T, et al. Increased expression of fatty acid binding protein 4 and leptin in resident macrophages characterises atherosclerotic plaque rupture. Atherosclerosis. 2013;226(1):74–81. doi:10.1016/j.atherosclerosis.2012.09.037
15. Llano A, Chan A, Kuk C, et al. Carcinoma In Situ (CIS): is there a difference in efficacy between various BCG strains? A comprehensive review of the literature. Cancers. 2024;16(2):245. doi:10.3390/cancers16020245
16. Jabs M, Rose AJ, Lehmann LH, et al. Inhibition of endothelial notch signaling impairs fatty acid transport and leads to metabolic and vascular remodeling of the adult heart. Circulation. 2018;137(24):2592–2608. doi:10.1161/CIRCULATIONAHA.117.029733
17. Furuhashi M, Tuncman G, Gorgun CZ, et al. Treatment of diabetes and atherosclerosis by inhibiting fattyacid-binding protein aP2. Nature. 2007;447:959–965. doi:10.1038/nature05844
18. Li L, Cheng SQ, Sun YQ, et al. Resolvin D1 reprograms energy metabolism to promote microglia to phagocytize neutrophils after ischemic stroke. Cell Rep. 2023;42(6):112617. doi:10.1016/j.celrep.2023.112617
19. Zhao X, Song L, Li J, et al. Effect of triglyceride-glucose indices and circulating PCSK9-associated cardiovascular risk in STEMI patients with primary percutaneous coronary artery disease: a prospective cohort study. J Inflamm Res. 2023;16:269–282. doi:10.2147/JIR.S389778
20. Zhao X, Wang Y, Chen R, et al. Triglyceride glucose index combined with plaque characteristics as a novel biomarker for cardiovascular outcomes after percutaneous coronary intervention in ST-elevated myocardial infarction patients: an intravascular optical coherence tomography study. Cardiovasc Diabetol. 2021;20(1):131. doi:10.1186/s12933-021-01321-7
21. Sherlock L, Lee SF, Katsanos AH, et al. Cognitive performance following stroke, transient ischaemic attack, myocardial infarction, and hospitalisation: an individual participant data meta-analysis of six randomised controlled trials. Lancet Healthy Longev. 2023;4(12):e665–e674. doi:10.1016/S2666-7568(23)00207-6
22. Amarenco P, Lavallee PC, Labreuche J, et al. Prevalence of coronary atherosclerosis in patients with cerebral infarction. Stroke. 2011;42:22–29. doi:10.1161/STROKEAHA.110.584086
23. SPARCL Investigators; Callahan A, Amarenco P, Goldstein LB, et al. Risk of stroke and cardiovascular events after ischemic stroke or transient ischemic attack in patients with type 2 diabetes or metabolic syndrome: secondary analysis of the Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) trial. Arch Neurol. 2011;68:1245–1251. doi:10.1001/archneurol.2011.146
24. Renedo D, Acosta JN, Leasure AC, et al. Burden of ischemic and hemorrhagic stroke across the US from 1990 to 2019. JAMA Neurol. 2024;81(4):394–404. doi:10.1001/jamaneurol.2024.0190
25. Waters DD, Ho JE, DeMicco DA, et al. Predictors of new-onset diabetes in patients treated with atorvastatin: results from 3 large randomized clinical trials. J Am Coll Cardiol. 2011;57:1535–1545. doi:10.1016/j.jacc.2010.10.047
26. Schmidt AF, Swerdlow DI, Holmes MV, et al. PCSK9 genetic variants and risk of type 2 diabetes: a mendelian randomisation study. Lancet Diabetes Endocrinol. 2017;5(2):97–105. doi:10.1016/S2213-8587(16)30396-5
27. Prasad M, Jayaraman S, Veeraraghavan VP. An intriguing role of circular RNA in insulin resistance and endothelial dysfunction: the future perspectives. Hypertens Res. 2022;45(11):1843–1845. doi:10.1038/s41440-022-01006-y
28. Poon AK, Whitsel EA, Heiss G, et al. Insulin resistance and reduced cardiac autonomic function in older adults: the atherosclerosis risk in communities study. BMC Cardiovasc Disord. 2020;20:217. doi:10.1186/s12872-020-01496-z
29. Han D, Ma J, Zhang X, et al. Correlation of PCSK9 gene polymorphism with cerebral ischemic stroke in Xinjiang Han and Uygur populations. Med Sci Monit. 2014;20:1758–1767. doi:10.12659/MSM.892091
30. Au A, Griffiths LR, Cheng -K-K, et al. The influence of OLR1 and PCSK9 gene polymorphisms on ischemic stroke: evidence from a meta-analysis. Sci Rep. 2015;5(1):18224. doi:10.1038/srep18224
31. Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376(18):1713–1722. doi:10.1056/NEJMoa1615664
32. Khan SU, Yedlapati SH, Lone AN, et al. PCSK9 inhibitors and ezetimibe with or without statin therapy for cardiovascular risk reduction: a systematic review and network meta-analysis. BMJ. 2022;377:e069116. doi:10.1136/bmj-2021-069116
33. Mbikay M, Sirois F, Mayne J, et al. PCSK9-deficient mice exhibit impaired glucose tolerance and pancreatic islet abnormalities. FEBS Lett. 2010;584(4):701–706. doi:10.1016/j.febslet.2009.12.018
34. Da Dalt L, Ruscica M, Bonacina F, et al. PCSK9 deficiency reduces insulin secretion and promotes glucose intolerance: the role of the low-density lipoprotein receptor. Eur Heart J. 2018;40(4):357–368. doi:10.1093/eurheartj/ehy357
35. Peeters W, de Kleijn DP, Vink A, et al. Adipocyte fatty acid binding protein in atherosclerotic plaques is associated with local vulnerability and is predictive for the occurrence of adverse cardiovascular events. Eur Heart J. 2011;32:1758–1768. doi:10.1093/eurheartj/ehq387
36. Saksi J, Ijäs P, Mäyränpää MI, et al. Low-expression variant of fatty acidbinding protein 4 favors reduced manifestations of atherosclerotic disease and increased plaque stability. Circ Cardiovasc Genet. 2014;7:588–598. doi:10.1161/CIRCGENETICS.113.000499
37. Lee CH, Cheung CYY, Woo YC, et al. Prospective associations of circulating adipocyte fatty acid-binding protein levels with risks of renal outcomes and mortality in type 2 diabetes. Diabetologia. 2019;62(1):169–177. doi:10.1007/s00125-018-4742-8
38. Luo B, Han F, Xu K, et al. Resolvin D1 programs inflammation resolution by increasing TGF-beta expression induced by dying cell clearance in experimental autoimmune neuritis. J Neurosci. 2016;36:9590–9603. doi:10.1523/JNEUROSCI.0020-16.2016
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Risk of Arterial and Venous Thrombotic Events Among Patients with COVID-19: A Multi-National Collaboration of Regulatory Agencies from Canada, Europe, and United States
Lo Re III V, Cocoros NM, Hubbard RA, Dutcher SK, Newcomb CW, Connolly JG, Perez-Vilar S, Carbonari DM, Kempner ME, Hernández-Muñoz JJ, Petrone AB, Pishko AM, Rogers Driscoll ME, Brash JT, Burnett S, Cohet C, Dahl M, DeFor TA, Delmestri A, Djibo DA, Duarte-Salles T, Harrington LB, Kampman M, Kuntz JL, Kurz X, Mercadé-Besora N, Pawloski PA, Rijnbeek PR, Seager S, Steiner CA, Verhamme K, Wu F, Zhou Y, Burn E, Paterson JM, Prieto-Alhambra D
Clinical Epidemiology 2024, 16:71-89
Published Date: 10 February 2024
Exosomes as Vehicles for Noncoding RNA in Modulating Inflammation: A Promising Regulatory Approach for Ischemic Stroke and Myocardial Infarction
Lai Z, Ye T, Zhang M, Mu Y
Journal of Inflammation Research 2024, 17:7485-7501
Published Date: 21 October 2024