")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Utility and Safety of Endobronchial Ultrasound-Guided Transbronchial Needle Aspiration in the Diagnosis of Isolated Mediastinal Masses
Authors Pan F , Lu AT , Mao XW , Chen Y, Zhao Y, Han B
Received 30 April 2021
Accepted for publication 7 July 2021
Published 3 August 2021 Volume 2021:14 Pages 2047—2052
DOI https://doi.org/10.2147/JMDH.S317060
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Feng Pan,1,* Ai-Ting Lu,1,2,* Xiaowei Mao,1,* Yefeng Chen,3 Yizhuo Zhao,1 Baohui Han1
1Department of Pulmonary Medicine, Shanghai Chest Hospital, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 2Department of Nursing, Shanghai Chest Hospital, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 3Department of Respiratory Medicine, Shaoxing People’s Hospital (Shaoxing Hospital, Zhejiang University School of Medicine), Shaoxing, Zhejiang, 312000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Baohui Han; Yizhuo Zhao
Department of Pulmonary Medicine, Shanghai Chest Hospital, Shanghai Jiao Tong University, Shanghai, People’s Republic of China
Email [email protected]; [email protected]
Background: Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) is a valuable tool for diagnosing pulmonary disease due to its efficiency and safety. We retrospectively analyzed patients with mediastinal masses who underwent diagnostic EBUS-TBNA at Shanghai Chest Hospital, and evaluated the clinical accuracy of EBUS-TBNA in the diagnosis mediastinal masses.
Method: From 2009 and 2014, patients who received EBUS-TBNA to diagnose a isolated mediastinal mass were enrolled. Clinical follow-up was performed to ascertain the patient’s final diagnosis.
Results: Forty-six patients were enrolled in this study. Thirty-seven were diagnosed with an oncologic disease, 3 were diagnosed with a mediastinal infection, and 2 were found to have a mediastinal goiter. The overall sensitivity, specificity, positive predictive value, negative predictive value, diagnostic yield was 63.6%, 100%, 100%, 42.9%, and 71.4%, respectively.
Conclusion: EBUS-TBNA is a safe and effective means of diagnosing mediastinal masses.
Keywords: EBUS-TBNA, mediastinum, diagnosis
Introduction
Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) is a valuable tool for diagnosing thoracic disease due to its efficiency and safety.1 It has excellent sensitivity and specificity, and a low incidence of complications.2,3 The latest National Comprehensive Cancer Network (NCCN) guidelines for non-small cell lung cancer recommend EBUS-TBNA for diagnosis and staging.4
The mediastinum is the central compartment of the thoracic cavity. It is uncontained and surrounded by loose connective tissue that contains the heart and its vessels as well as the esophagus, trachea, phrenic and cardiac nerves, thoracic duct, thymus and lymph nodes of the central chest.5 It is a common site for lymphoma, thymoma, germ cell tumors, neurogenic tumors, mediastinal goiters and other mass-manifesting diseases.6,7 A precise diagnosis of mediastinal disease is necessary to direct appropriate treatment.8–10
Several modalities have been developed for diagnosing mediastinal masses, including mediastinoscopy and CT-guided percutaneous biopsy.11,12 The diagnostic yield of these techniques is similar, but transthoracic needle biopsy is more attractive due to its minimally invasive nature. Also a minimally invasive biopsy technique, Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA), has been recently evaluated for its ability to diagnose mediastinal masses.13–17 Yasufuku et al14 reported a high diagnostic value of EBUS-TBNA (93.6%). However, Zhu et al15 reported a diagnostic yield of only 62%. This difference may be the result of different patient samples, as up to 70% of the patients in Yasufuku et al’s cohort had benign disease.14 Gulla et al17 studied the utility and safety of EBUS-TBNA in children, reporting a moderate diagnostic value. However, this work enrolled only a limited number of patients and had a short follow-up period of 2 years.
In this study we retrospectively analyzed patients with mediastinal masses who underwent EBUS-TBNA at Shanghai Chest Hospital from 2009 to 2014 and had > 5 year follow-up, and evaluated the clinical utility of EBUS-TBNA in the diagnosis of mediastinal masses.
Methods
Patient Selection
This study was performed at the clinical center for thoracic medicine at our hospital. Patients who received care from 2009 to 2014 and met our eligibility criteria (Table 1) were included in this work.
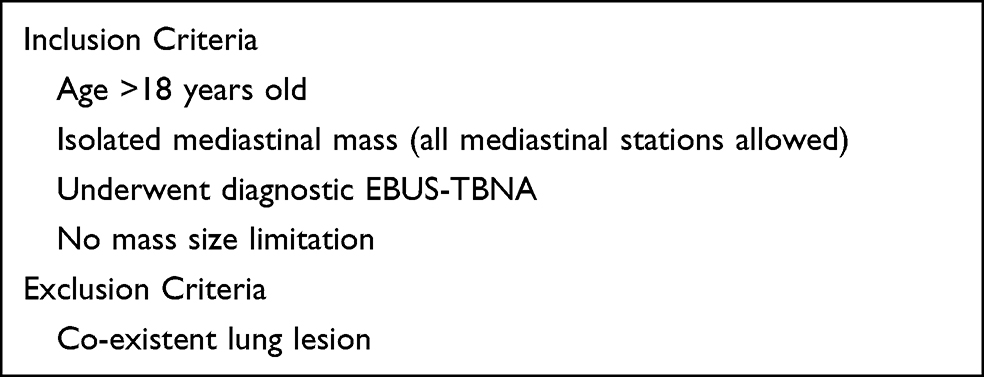 |
Table 1 Inclusion and Exclusion Criteria |
The ethics committee of Shanghai Chest Hospital approved this retrospective study (KS1970). All researchers followed the Helsinki declaration. Informed consent was obtained from all patients before they received EBUS-TBNA, and they were willing to receiving a medical following-up.
EBUS-TBNA
Food and water were forbidden for at least 6 hours before EBUS-TBNA. EBUS-TBNA was performed using an ultrasound system and a linear ultrasonic bronchoscope (BF-UC260F-OL8, Olympus Ltd, Tokyo, Japan). All patients received local anesthesia with lidocaine. EBUS-TBNA was performed by senior doctors in all cases. White light bronchoscopy was performed prior to examination of the target mass and peripheral vessels with EBUS. A 22-gauge needle was used to biopsy the target mass under real-time ultrasound guidance. Two or three aspirations were typically required in order to obtain enough histology specimens. Cytology and histology were performed by two independent pathologists. No onsite cytologic evaluation was performed.18,19
Pathology Evaluation
Cytology and histology specimens were sent to the pathology department at Shanghai Chest Hospital for evaluation. All specimens were examined by two senior pathologists. Hematoxylin and eosin staining were routinely performed. There are many types of mediastinal diseases so immunohistochemistry was commonly required.
Clinical Follow-Up
Clinical follow-up was pursued to understand the final diagnosis of each case. At least 5 years of follow up was performed. Other diagnostic modalities such as surgery, mediastinoscopy, and CT-guided percutaneous transthoracic biopsy were recorded. Lab and imaging data and clinical treatment records were also collected. The final diagnosis was based on the results of the EBUS-TBNA and the clinical follow-up.
Statistical Analysis
If malignant cells were found in the mediastinal mass post-resection and malignant cells were noted in the EBUS-TBNA specimen, this was defined as a true positive result. No false positives are possible due the nature of EBUS-TBNA. However, if the final mass was found to be malignant and no malignant cells were found in the EBUS-TBNA specimen, this was considered a false negative result. If the final diagnosis was benign disease and no malignant cells were found in the EBUS-TBNA specimen, this was defined as a true negative result.
The sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic yield were calculated. All analyses were performed using SPSS 12.0 (SPSS Inc., Chicago, IL, USA).
Results
A total of 46 patients were enrolled in this study, of whom 34 were male and the others were female. Patient age ranged from 18 to 77 years old. All patients successfully underwent EBUS-TBNA examination, defined as EBUS-TBNA obtaining enough of a sample to permit pathologic evaluation. Thirty-seven patients were diagnosed with tumors, 3 were diagnosed with a mediastinal infection, and 2 had a mediastinal goiter No complications were observed. (Table 2).
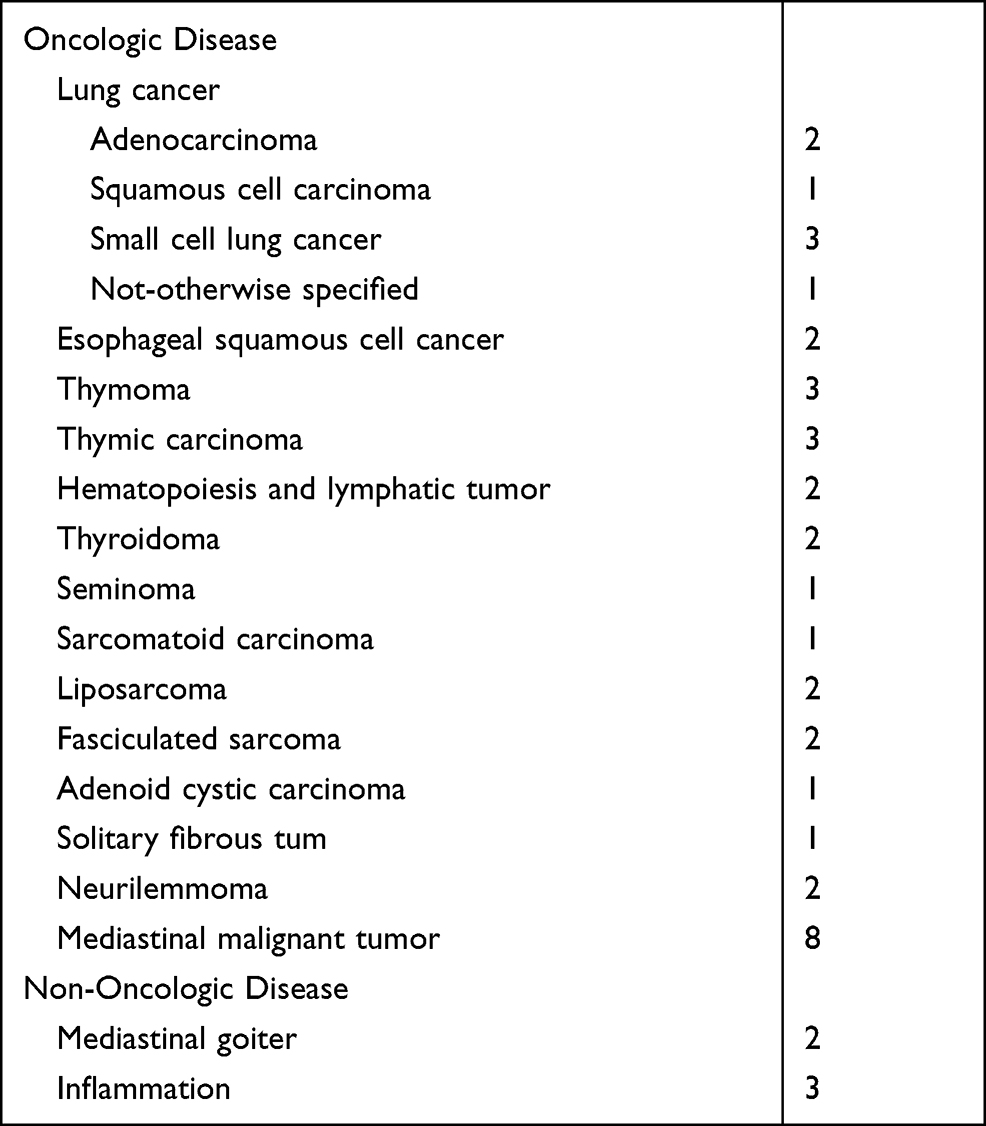 |
Table 2 Final Diagnosis |
The study flow chart is shown in Figure 1. Malignant cells were found in 21 EBUS-TBNA specimens, and 3 additional malignancies were diagnosed following additional invasive examination. The other 25 EBUS-TBNA specimens showed no evidence of malignant cells. Of the 25 patients with negative EBUS-TBNA results, 4 were censored, 3 did not undergo any additional examinations and are still alive, and 1 did not undergo any further examination and died. One patient underwent a supraclavicular lymph node biopsy and was diagnosed with squamous cell carcinoma of the lung. Two patients underwent a transthoracic biopsy and were diagnosed with sarcomatoid carcinoma and a thyroidoma, respectively. Fifteen patients received their final diagnosis based on surgical pathology. Three patients received antibiotics and their masses disappeared on subsequent imaging.
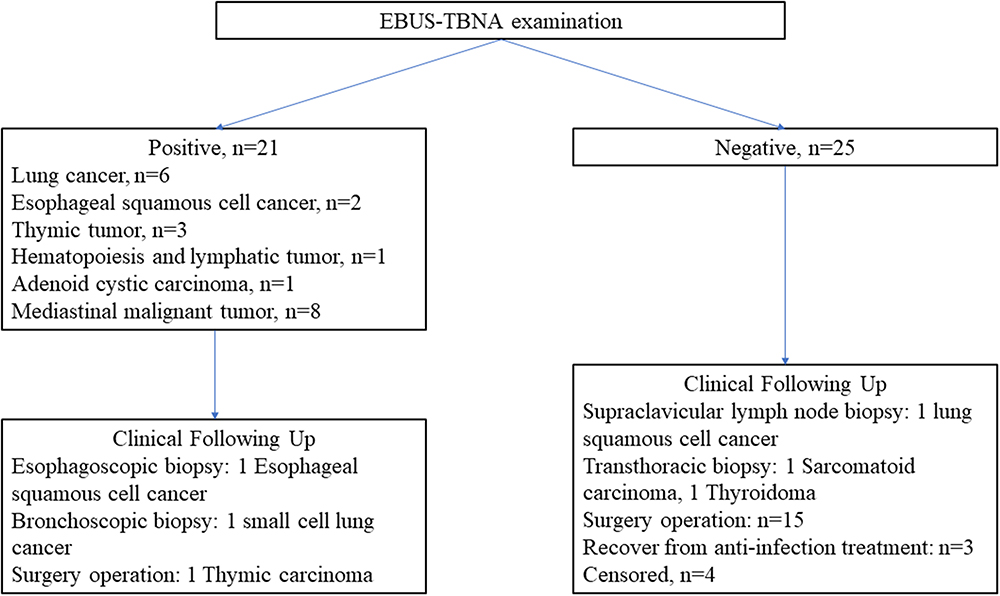 |
Figure 1 The flow chart of study. |
Four patients were censored in this study, so only 42 were included for future analysis. The overall sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic yield of EBUS-TBNA was 63.6%, 100%, 100%, 42.9%, and 71.4%. The diagnostic yield of EBUS-TBNA for different diseases varied. The yield of EBUS-TBNA for common tumors of the chest, such as lung or esophageal cancer, reached 100%. However, the yield fell to 0% for rare diseases such as a reproductive system or mesenchymal tumor (Table 3).
 |
Table 3 Diagnostic Accuracy of EBUS-TBNA for Mediastinal Masses |
Discussion
Mediastinal diseases can originate from different tissues and therefore require different treatments. For example, thymomas are often treated with surgery, lymphoma or reproductive system tumors are always managed with chemotherapy and/or radiotherapy, and metastatic disease often requires systemic treatment.6–10 A diagnosis is therefore required to appropriately plan treatment. Over the last few years many diagnostic methods for mediastinal masses have been used in clinical practice. One invasive examination is mediastinoscopy, but mediastinoscopy requires general anesthesia and can result in significant trauma. CT-guided percutaneous transthoracic biopsy is less invasive but exposes patients to large doses of radiation.12,20
EBUS-TBNA is a recently developed method for diagnosing thoracic disease. It has been widely applied in clinical practice due to its safety and high degree of accuracy. It has a lower complication rate.21,22 EBUS-TBNA has a high sensitivity and nearly 100% specificity. It was therefore recommended by the NCCN for the diagnosis and staging of lung cancer.4 As mediastinal disease is rare, up until now few studies have focused on the diagnostic value of EBUS-TBNA for mediastinal masses.13,14,23 As a large center for thoracic disease we track mediastinal disease for future analysis.24 EBUS-TBNA has been routinely performed at our center for nearly 10 years. Sun et al25 reported that the diagnostic yield of EBUS-TBNA in lung cancer approaches 90%. The work by Yang et al18 performed at our institution reported that EBUS-TBNA in the diagnosis of non-lymph node thoracic lesions was 95.1% accurate. With respect to benign disease, our group has reported diagnostic yields of 90% and 94.17%, in the diagnosis of intrathoracic tuberculosis and pulmonary sarcoidosis with EBUS-TBNA, respectively.26,27 However, the clinical value of EBUS-TBNA in the diagnosis of mediastinal masses has rarely been reported.
The present work evaluated the clinical value in the diagnosis of mediastinal masses. The overall sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic yield was 63.6%, 100%, 100%, 42.9%, and 71.4%, respectively. The specificity and positive predictive value of EBUS-TBNA was 100%, as there were no false positive cases. The sensitivity and diagnostic yield was moderate.
The sensitivity, negative predictive value and diagnostic yield calculated in the present work are lower than those reported by other studies. To explore the reasons for this discrepancy we future divided mediastinal diseases into several groups (Table 4). With our revised classification the diagnostic value of EBUS-TBNA for esophageal tumors was 100%, but was 0% for thyroid, reproductive system, and mesenchymal tissue tumors. EBUS-TBNA had a moderate diagnostic value for thymic tumors and hematologic and lymphatic tumors. Lung, esophageal and thymic tumors are the most common diseases managed at our institution’s department of thoracic surgery. We have therefore seen the highest diagnostic value of EBUS for those diseases.28,29 One reason for this may be because lung, esophageal and thymic tumors originate from epithelial cells and are familiar to the pathologist. EBUS-TBNA yields “a long tissue core” due to acquisition of tissue with a needle. Compared with different forms of transthoracic biopsy, less lesion tissue is obtained with EBUS-TBNA. Further, less necrosis is found in lung, esophageal and thymic tumors compared with sarcoma. In our study, 2 patients were diagnosed with a hematologic and lymphatic tumor. Interestingly, one of these patients was initially diagnosed with Castleman’s disease by EBUS-TBNA and other imaging examinations. However, Reed-Sternberg cells were found in his surgery specimen, so his final diagnosis was Hodgkin’s lymphoma.30 The poor accuracy of EBUS-TBNA in the diagnosis of lymphoma has been previously reported.31,32 In the case of seminoma, only crushed small round cells are found in the background of blood clots in the EBUS-TBNA specimen. This is consistent with the pathologic features of seminoma, which always include necrosis.33 Of the 8 mesenchymal tumors biopsied in this work, a large amount of necrosis and blood clots was found in 6, while the other 2 specimens had bronchial mucosa epithelium, cartilage fragments and some fibrous tissue. Seven of these patients were diagnosed based on their surgical pathology, while the other was diagnosed with a transthoracic biopsy.34,35
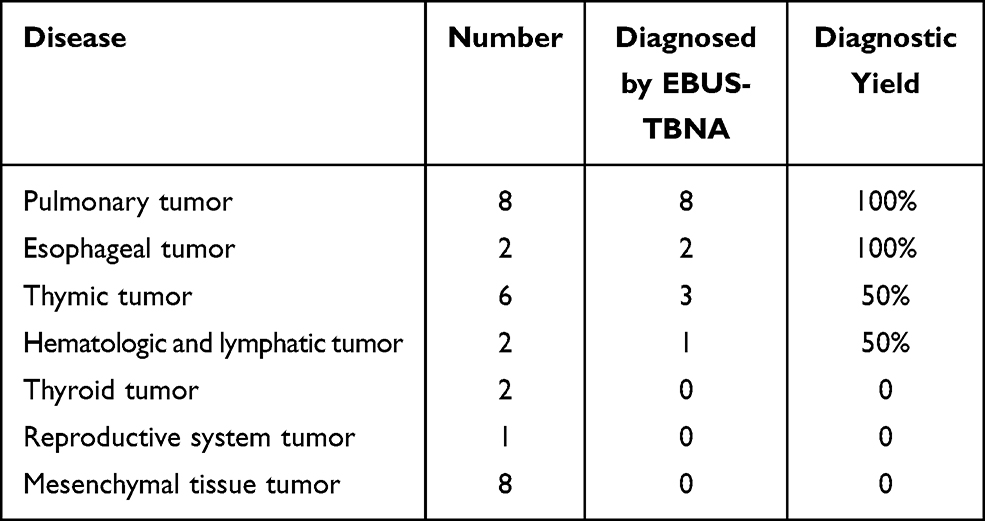 |
Table 4 Diagnostic Yield of EBUS-TBNA for Different Diseases |
Owing to the tertiary referral nature of our center, only 5 of the patients in our study were ultimately diagnosed with a non-tumor disease (88.1% malignant disease). In contrast with other studies, pulmonary, esophageal and thymic tumors were only a small part of the diseases diagnosed in this study (38%, 16/42). As this is a retrospective single center study, some bias is inevitable.
In conclusion, EBUS-TBNA is a safe and effective means for diagnosing common mediastinal masses.
Funding
This study was supported by grants from the Medical Engineering Cross Research Foundation of Shanghai Jiao Tong University (ZH2018QNA67), Scientific Research Project of Shanghai Municipal Health Commission (20194Y0168), and the Shaoxing Bureau of Science and Technology (2018C30061).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kinsey CM, Arenberg DA. Endobronchial ultrasound-guided transbronchial needle aspiration for non-small cell lung cancer staging. Am J Respir Crit Care Med. 2014;189(6):640–649. doi:10.1164/rccm.201311-2007CI
2. Gu P, Zhao YZ, Jiang LY, Zhang W, Xin Y, Han BH. Endobronchial ultrasound-guided transbronchial needle aspiration for staging of lung cancer: a systematic review and meta-analysis. Eur J Cancer. 2009;45(8):1389–1396. doi:10.1016/j.ejca.2008.11.043
3. Vaidya PJ, Munavvar M, Leuppi JD, Mehta AC, Chhajed PN. Endobronchial ultrasound-guided transbronchial needle aspiration: safe as it sounds. Respirology. 2017;22(6):1093–1101. doi:10.1111/resp.13094
4. NCCN guidelines for NSCLC. 2021:v2.
5. Richardson JD, Wilson ME, Miller FB. The widened mediastinum. Diagnostic and therapeutic priorities. Ann Surg. 1990;211(6):731–736. doi:10.1097/00000658-199006000-00012
6. Tzankov A. Non-neoplastic lesions of the mediastinum. Pathologe. 2016;37(5):400–411. doi:10.1007/s00292-016-0197-1
7. Rieker RJ, Marx A, Agaimy A, Ströbel P. Mesenchymal tumors of the mediastinum. Pathologe. 2016;37(5):449–456. doi:10.1007/s00292-016-0190-8
8. Rascoe PA, Kucharczuk JC, Cooper JD. Surgery of the mediastinum: historical notes. Thorac Surg Clin. 2009;19(1):1–5. doi:10.1016/j.thorsurg.2008.09.007
9. Davenport E, Malthaner RA. The role of surgery in the management of thymoma: a systematic review. Ann Thorac Surg. 2008;86(2):673–684. doi:10.1016/j.athoracsur.2008.03.055
10. Sweetenham JW. Treatment of lymphoblastic lymphoma in adults. Oncology. 2009;23(12):1015–1020.
11. Raj Behl P, Hilton CJ, Holden MP. Mediastinoscope: another use. J Cardiovasc Surg. 1986;27(2):236–237.
12. Priola AM, Priola SM, Cataldi A, et al. CT-guided percutaneous transthoracic biopsy in the diagnosis of mediastinal masses: evaluation of 73 procedures. Radiol Med. 2008;113(1):3–15. doi:10.1007/s11547-008-0233-1
13. Eckardt J. Endobronchial ultrasound-guided transbronchial needle aspiration of lesions in mediastinum. J Thorac Dis. 2010;2(3):125–128.
14. Yasufuku K, Nakajima T, Fujiwara T, Yoshino I, Keshavjee S. Utility of endobronchial ultrasound-guided transbronchial needle aspiration in the diagnosis of mediastinal masses of unknown etiology. Ann Thorac Surg. 2011;91(3):831–836. doi:10.1016/j.athoracsur.2010.11.032
15. Zhu F, Ma D-C, Xu N, et al. Diagnostic value of video-assisted mediastinoscopy and endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal lymphadenectasis without pulmonary abnormalities. Med Sci Monit. 2017;23:3064–3070. doi:10.12659/MSM.900968
16. Mishra MM, Reynolds JP, Sturgis CD, Booth CN. Diagnosis of mediastinal lesions unassociated with lung carcinoma diagnosed by endobronchial ultrasound transbronchial needle aspiration (EBUS-TBNA). J Am Soc Cytopathol. 2016;5(4):189–195. doi:10.1016/j.jasc.2016.02.003
17. Gulla KM, Gunathilaka G, Jat KR, et al. Utility and safety of endobronchial ultrasound-guided transbronchial needle aspiration and endoscopic ultrasound with an echobronchoscope-guided fine needle aspiration in children with mediastinal pathology. Pediatr Pulmonol. 2019;54(6):881–885. doi:10.1002/ppul.24313
18. Yang H, Zhao H, Garfield DH, Teng J, Han B, Sun J. Endobronchial ultrasound–guided transbronchial needle aspiration (EBUS-TBNA) in the diagnosis of non-lymph node thoracic lesions. Ann Thorac Med. 2013;8(1):14–21. doi:10.4103/1817-1737.105714
19. Ben S, Akulian J, Wang K-P. Endobronchial ultrasound transbronchial needle aspiration: a hybrid method. J Thorac Dis. 2015;7(S4):S287–S291.
20. Petranovic M, Gilman MD, Muniappan A, et al. Diagnostic yield of CT-guided percutaneous transthoracic needle biopsy for diagnosis of anterior mediastinal masses. Am J Roentgenol. 2015;205(4):774–779. doi:10.2214/AJR.15.14442
21. Sehgal IS, Dhooria S, Aggarwal AN, Agarwal R. Training and proficiency in endobronchial ultrasound-guided transbronchial needle aspiration: a systematic review. Respirology. 2017;22(8):1547–1557. doi:10.1111/resp.13121
22. Wahidi MM, Herth F, Yasufuku K, et al. Technical aspects of endobronchial ultrasound-guided transbronchial needle aspiration: CHEST guideline and expert panel report. Chest. 2016;149(3):816–835. doi:10.1378/chest.15-1216
23. Zhao H, Wang J, Zhou Z-L, et al. Application of endobronchial ultrasound-guided transbronchial needle aspiration in the diagnosis of mediastinal lesions. Chin Med J. 2011;124(23):3988–3992.
24. Li GS, Liu K, Publishing Company AME. Professor changqing pan: build Shanghai chest hospital as an international brand. Shanghai Chest. 2017;1(1):2. doi:10.21037/shc.2017.05.02
25. Sun J, Zhang J, Zhao H, Shen J, Gu A, Han B. Role of endobronchial ultrasound-guided transbronchial needle aspiration in the diagnosis of bronchogenic carcinoma: experience of a single institution in China. Thorac Cancer. 2010;1(1):28–34. doi:10.1111/j.1759-7714.2010.00010.x
26. Sun J, Teng J, Yang H, et al. Endobronchial ultrasound-guided transbronchial needle aspiration in diagnosing intrathoracic tuberculosis. Ann Thorac Surg. 2013;96(6):2021–2027. doi:10.1016/j.athoracsur.2013.07.005
27. Sun J, Yang H, Teng J, et al. Determining factors in diagnosing pulmonary sarcoidosis by endobronchial ultrasound-guided transbronchial needle aspiration. Ann Thorac Surg. 2015;99(2):441–445. doi:10.1016/j.athoracsur.2014.09.029
28. Moonim MT, Breen R, Gill-Barman B, Santis G. Diagnosis and subclassification of thymoma by minimally invasive fine needle aspiration directed by endobronchial ultrasound: a review and discussion of four cases. Cytopathology. 2012;23(4):220–228. doi:10.1111/j.1365-2303.2012.01007.x
29. Yoshida Y, Singyoji M, Ashinuma H, et al. Successful diagnosis of a thymoma by endobronchial ultrasound-guided transbronchial needle aspiration: a report of two cases. Intern Med. 2015;54(21):2735–2739. doi:10.2169/internalmedicine.54.3486
30. Fajgenbaum DC, Shilling D. Castleman disease pathogenesis. Hematol Oncol Clin North Am. 2018;32(1):11–21. doi:10.1016/j.hoc.2017.09.002
31. Erer OF, Erol S, Anar C, Aydoğdu Z, Özkan SA. Diagnostic yield of EBUS-TBNA for lymphoma and review of the literature. Endosc Ultrasound. 2017;6(5):317–322. doi:10.4103/2303-9027.180762
32. Velu PP, Reid PA, Wallace WA, Skwarski KM. Isolated mediastinal lymphadenopathy - performance of EBUS-TBNA in clinical practice. J R Coll Physicians Edinb. 2017;47(1):52–56. doi:10.4997/JRCPE.2017.111
33. Mégevand R, Etienne T, Spiliopoulos A. Germ cell tumors of the mediastinum. Cancer. 2015;80(4):699–707.
34. Borden EC, Baker LH, Bell RS, et al. Soft tissue sarcomas of adults: state of the translational science. Clin Cancer Res. 2003;9(6):1941–1956.
35. Tian Q, Chen L-A, Wang R-T, Yang Z, An Y. The reasons of false negative results of endobronchial ultrasound-guided transbronchial needle aspiration in the diagnosis of intrapulmonary and mediastinal malignancy. Thorac Cancer. 2013;4(2):186–190. doi:10.1111/1759-7714.12010
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.