Back to Journals » Infection and Drug Resistance » Volume 17
Using Tocilizumab in Hematologic Malignant Patients with Severe COVID-19 Infection – Case Series Report
Authors Fu C ![]() , Zhu Y, Huang W, Luo Y, Hu Y
, Zhu Y, Huang W, Luo Y, Hu Y ![]() , Huang H, Sun J
, Huang H, Sun J
Received 7 September 2023
Accepted for publication 27 December 2023
Published 5 January 2024 Volume 2024:17 Pages 31—39
DOI https://doi.org/10.2147/IDR.S435160
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Chunlan Fu,1 Yuanyuan Zhu,2 Weijia Huang,2 Yi Luo,2 Yongxian Hu,2 He Huang,2 Jie Sun2
1Department of Hematology, Zhuji Affiliated Hospital of Wenzhou Medical University, Zhuji, Zhejiang, 311800, People’s Republic of China; 2Transplantation Center, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, 310058, People’s Republic of China
Correspondence: Jie Sun; He Huang, Email [email protected]; [email protected]
Background: Patients with hematologic malignancies usually have severe immunodeficiency and are much more likely to be severe after COVID-19 infection. Tocilizumab is a monoclonal antibody of interleukin-6 (IL-6) and is recommended for treating severe conditions in the latest COVID-19 treatment guidelines. However, the efficacy and safety of tocilizumab in hematologic malignancy patients have yet to be clarified. We report five hematologic malignancy patients with severe COVID-19 infection who were all successfully recovered with tocilizumab treatment.
Methods: We reported five hematologic malignant patients who developed severe COVID-19 infection and received tocilizumab at the First Affiliated Hospital of Zhejiang University School of Medicine during the COVID-19 pandemic in China from Dec 2022 to Mar 2023. We observed the effect of tocilizumab on COVID-19 infection and evaluated its safety.
Results: Five hematologic malignancy patients with severe COVID-19 infection were retrospectively enrolled. The dosage of tocilizumab was 400– 480mg once; one patient used a second dose of tocilizumab on the third day of medication. After receiving tocilizumab treatment, all five patients experienced a rapid decrease in body temperature and C-reactive protein (CRP) within 24 hours and improved oxygen requirement within one to three days (one patient did not experience hypoxia). Chest CT scans after one week showed absorption of lung infection. The serum IL-6 levels of three patients showed an initial increase followed by a decrease. None of the patients experienced grade 3– 4 hematologic or non-hematologic toxicity.
Conclusion: Tocilizumab can improve the outcome of severe COVID-19 infection in hematologic malignancy patients with severe immunodeficiency without severe adverse reactions.
Keywords: COVID-19, hematologic malignancy, tocilizumab
Introduction
Hematologic malignancy patients usually have severe immunodeficiency due to the underlying disease and chemotherapy.1 Some patients also receive treatments such as chimeric antigen receptor T cell (CAR-T) therapy and hematopoietic stem cell transplantation, contributing to their unique immunological status compared to non-hematologic malignancy patients.2 Those patients are much more likely to develop severe situations after COVID-19 infection. The 30-day mortality rate for malignancy patients with COVID-19 has been reported as 13–33%.3–5 A cohort study by He et al6 showed that the mortality rate of hematologic malignancy patients after COVID-19 infection is much higher compared to non-hematologic malignancy patients (62% vs 8%). A survey by the European Hematology Association7 revealed that the rate of severe or critical illness after COVID-19 infection in hematologic malignancy patients is 63.8%, with 13.8% progressing to the intensive care unit (ICU). Excessive inflammation causes widespread organ damage, multiple organ failure, and even death.8–10 Corticosteroids are recommended for severe and critical COVID-19 infection patients.11 However, it was reported that high doses and long-term use of corticosteroids would lead to adverse reactions11 and do not reduce mortality or improve outcomes for patients receiving mechanical ventilation.12,13 Nirmatrelvir/ritonavir is recommended as a standard treatment for mild, moderate, and severe COVID-19 infection.11 However, a retrospective study by Wang et al14 found that nirmatrelvir/ ritonavir does not adequately clear the virus in patients with underlying conditions such as malignant tumors, and some patients still progress to severe illness. Elevated serum IL-6 levels have been identified as a risk factor for poor prognosis in COVID-19 infection.15,16 The 10th Edition of the Chinese National Guideline for COVID-19 infection: Diagnosis and Treatment Protocol for COVID-19 infection recommends the use of IL-6 receptor antagonists like tocilizumab for severe/critical COVID-19 infection or patients with elevated serum IL-6 levels.11 A series of controlled studies17,18 showed that patients infected with severe COVID-19 received tocilizumab treatment to prevent further disease deterioration but could not improve the survival rate. The Society for Immunotherapy of Cancer suggests the use tocilizumab in severe COVID-19 infection.19 There is no universally accepted experience in managing severe COVID-19 infection, nor experience in immunosuppressive patients such as hematologic malignancy patients.
During the COVID-19 pandemic in China from Dec. 2022 to Mar. 2023, we successfully treated five cases of hematologic malignancy patients with severe COVID-19 infection using tocilizumab. This article presents a retrospective analysis of these five patients to evaluate tocilizumab’s clinical efficacy and safety, providing our center’s experience for severe COVID-19 infection treatment.
Diagnosis of severe COVID-19 infection refers to the Diagnostic and Treatment Protocol for Novel Coronavirus Infection (Trial Version 10): In adults, any of the following criteria can be used for diagnosis, and the symptoms cannot be explained by reasons other than COVID-19 infection: 1. Presence of dyspnea with a respiratory rate (RR) ≥ 30 breaths per minute; 2. Resting oxygen saturation (SpO2) ≤ 93% while breathing ambient air; 3. The arterial partial pressure of oxygen (PaO2) to the fraction of inspired oxygen (FiO2) ratio ≤ 300 mmHg (1 mmHg = 0.133 kPa); 4. Progressive worsening of clinical symptoms, with lung imaging showing >50% lesion progression within 24–48 hours. Diagnosis criteria for critical COVID-19: Shock occurs; Respiratory failure requires mechanical ventilation; If combined with other organ failures, ICU monitoring and treatment are required. According to the Diagnostic and Treatment Protocol for Novel Coronavirus Infection (Trial Version 10), IL-6 receptor antagonists like tocilizumab are recommended when the patient is diagnosed with severe and critical COVID-19, and the laboratory detection of IL-6 significantly increased.11 The recommended initial dose of tocilizumab is 4–8 mg/kg; the maximum cumulative doses should not exceed 800 mg. The definition and grading criteria for clinical adverse reactions are according to the Common Terminology Criteria for Adverse Events (CTCAE) 5.0.20
Cases Presentation
Case 1
This patient was female, 71 years old, diagnosed with chronic myeloid leukemia for over 20 years, receiving long-term treatment of dasatinib. On December 20, 2022, she was diagnosed with diffuse large B-cell lymphoma. On December 30, she received a ZR2 (Ibrutinib+Lenalidomide+Rituximab) regimen for treatment. On December 31, the patient developed a fever with a maximum temperature of 39.7°C. On January 2, 2023, she tested nucleic acid positive for SARS-CoV-2 on a nasopharyngeal swab, and a chest CT showed pneumonia. Her blood routine showed white blood cells were 1.15×10^9/L, neutrophils 0.74×10^9/L, hemoglobin 84g/L, and platelets 61×10^9/L. The patient experienced dyspnea, with the lowest arterial oxygen pressure (PaO2) at 65.1mmHg. Oxygen was administered at 10L/min, and methylprednisolone 40mg qd was added. On January 7, chest CT showed progression of bilateral lung inflammation. IL-6 was 193.69pg/mL, and CRP was 20.4mg/L. The patient was diagnosed with severe COVID-19 infection, and 320mg of tocilizumab was given immediately on January 7. On January 8, the patient’s body temperature decreased to normal, and the chest tightness and dyspnea improved. CRP also decreased. The serum IL-6 initially increased, peaking at 688.27pg/mL, then gradually decreasing. On January 13, her chest CT showed absorption of inflammation. On January 19, the patient met the discharge criteria and was discharged.
Case 2
This patient was female and 67 years old. She was diagnosed with multiple myeloma. On November 25, 2022, she received BCMA-CAR-T therapy. On December 30, the patient developed a fever with a maximum temperature of 39.5°C. On January 6, 2023, she tested nucleic acid positive for SARS-CoV-2 on a nasopharyngeal swab, and her chest CT showed bilateral lung inflammation. Blood routine showed the white blood cells were 5.2×10^9/L, neutrophils 4.28×10^9/L, hemoglobin 105g/L, and platelets 176×10^9/L. The patient experienced significant chest tightness, with the lowest oxygen saturation at 86%. Oxygen was administered at 15L/min, and dexamethasone 10mg qd was added. On January 10, a chest CT showed that lung inflammation had progressed. The serum IL-6 level was 287.74pg/mL, and CRP was 34.71mg/L then. The patient was diagnosed with severe COVID-19 infection. The patient received dexamethasone at 10mg Q12h and nirmatrelvir/ritonavir 3# Q12h on January 10, 400mg tocilizumab was administrated on the same day. On January 11, the patient’s body temperature rapidly decreased, and chest tightness and dyspnea improved. On January 12, the auscultation of her lungs revealed coarse and moist rales, and the patient was considered to have a progression of infection. Then, tocilizumab was administered again with one dose of 400mg.11 Subsequently, CRP and IL-6 decreased progressively. On January 17, the chest CT showed absorption of lung infections compared to previous scans. On January 24, the patient had chest tightness and dyspnea again, with oxygen saturation dropping to 70–80%. The SARS-CoV-2 nucleic acid was tested again and was still positive. The chest CT showed progression of bilateral lung inflammation. Sputum culture revealed the presence of moderate amounts of white candida, suggesting secondary pulmonary fungal infection. On January 30, the patient developed significant chest tightness and dyspnea. Her family refused further treatments and left the hospital on January 31.
Case 3
This patient was female, 53 years old. She was diagnosed with acute myeloid leukemia. The most recent chemotherapy was administered on November 9, 2022, with FLAG regimen (Fludarabine 50mg/m2 on days 1–5, Cytarabine 2.0/m2 on days 1–5, G-CSF 150ug q12h on days 0–5). On January 13, 2023, the patient developed a fever with a maximum temperature of 40°C, and SARS-CoV-2 on nasopharyngeal swab nucleic acid tested positive. Chest CT showed bilateral lung inflammation. Blood routine revealed the white blood cells were 1.22×10^9/L, neutrophils 0.69×10^9/L, hemoglobin 43g/L, and platelets 82×10^9/L. Dexamethasone 10mg Q12h and nirmatrelvir/ritonavir 3# Q12h were added on January 13. On January 17, the patient’s oxygen saturation dropped to 88%, and oxygen was administered at 9L/min. By that time, she was diagnosed with severe COVID-19 infection. Tocilizumab treatment was initiated on the same day with a dose of 480mg. Within 24 hours, the patient’s body temperature decreased, and respiratory distress and hypoxemia improved significantly. C-reactive protein decreased progressively. The chest CT on January 20 and January 26 showed absorption of inflammatory lesions in both lungs. On January 20, the SARS-CoV-2 nucleic acid test was negative. On February 6, the patient met the discharge criteria and was discharged.
Case 4
This patient was female and 68 years old. She was diagnosed with acute myeloid leukemia. On December 9, 2022, the patient received chemotherapy with decitabine 20mg/m2 d1-5 plus IA 3+7 regimen, followed by HLA mismatched donor stem cell transplantation (micro-transplant). On December 30, the patient developed a fever with a maximum temperature of 39.4°C. On January 4, 2023, the patient tested positive for SARS-CoV-2 on a nasopharyngeal swab, and nirmatrelvir/ritonavir 3# Q12h was administered. On January 12, Her chest CT showed bilateral lung inflammation. On January 17, the serum IL-6 level was 133.48pg/mL, CRP was 143.72mg/L, and the blood routing showed the white blood cells were 0.3×10^9/L, neutrophils 0.03×10^9/L, hemoglobin 46g/L, and platelets 41×10^9/L. She was diagnosed with severe COVID-19 pneumonia. 400mg of tocilizumab was administrated to her immediately. On January 18, the patient’s body temperature quickly returned to normal, and CRP decreased. The serum IL-6 levels gradually increased to 362.85pg/mL and then decreased. The chest CT on January 18 showed reduced bilateral lung inflammation. On January 30, the patient met the discharge criteria and was discharged.
Case 5
This patient is male, 32 years old. He was diagnosed with myelodysplastic syndrome (IPSS-R: high-risk). The patient’s last chemotherapy was administered on November 6, 2022, with azacitidine 75mg/m2 d1-7 plus IA 3+7 regimen. On February 2, 2023, the patient developed a fever with a maximum temperature of 40°C and tested positive for SARS-CoV-2 on a nasopharyngeal swab, and nirmatrelvir/ritonavir 3# Q12h was given. After that, the patient experienced shortness of breath. Blood gas analysis showed a partial pressure of oxygen (PaO2) of 57.3mmHg. Oxygen was administered at 15L/min, and methylprednisolone was added at 40mg every 8 hours. On February 13, the blood routine showed white blood cells were 17.82×10^9/L, neutrophils 4.28×10^9/L, hemoglobin 48g/L, and platelets 15×10^9/L, the serum IL-6 level was 56.38pg/mL, CRP was 172.78mg/L. His chest CT revealed bilateral multiple infiltrates. He was then diagnosed with severe COVID-19 infection. Tocilizumab was treated at 480mg at once. On February 14, the patient’s body temperature decreased to 38°C, and CRP decreased. The serum IL-6 levels sharply increased to 2778.07pg/mL and then decreased. The chest CT on February 17 showed a lung reduction. However, due to disease progression to acute leukemia, upon the request of the patient’s family, the patient was transferred to a local hospital for further treatment on March 14, 2023.
Results
This study included five cases of hematologic tumor patients with severe COVID-19 infection. A summary of the patient’s clinical characteristics and other medication information before tocilizumab administration can be found in Table 1. The clinical changes and laboratory examination results, including CRP (Figure 1), body temperature (Figure 2), oxygen requirements (Figure 3), and serum IL-6 concentrations (Figure 4), after tocilizumab treatment in the five cases are summarized. After tocilizumab treatment, two patients experienced Grade 1 liver function abnormalities with elevated alanine aminotransferase levels (one patient increased from 53 U/L to 101 U/L, and another patient increased from 75 U/L to 157 U/L). Both patients received hepatoprotective treatment, and their liver function recovered to normal within one week. None of the patients experienced Grade 3–4 hematological, cardiac, or renal toxicity during treatment.
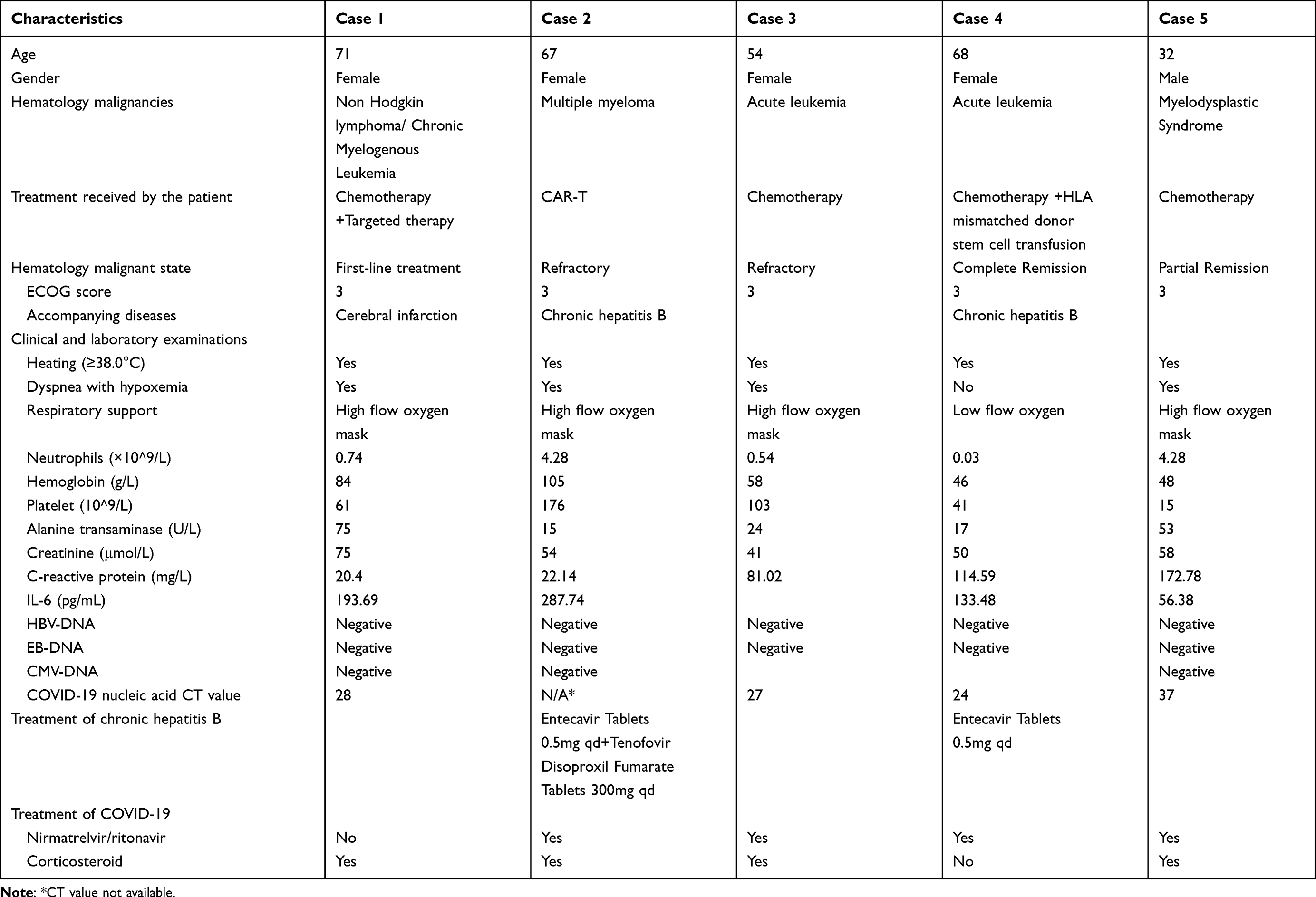 |
Table 1 The Clinical Characteristics of Patients Before Tocilizumab Administration |
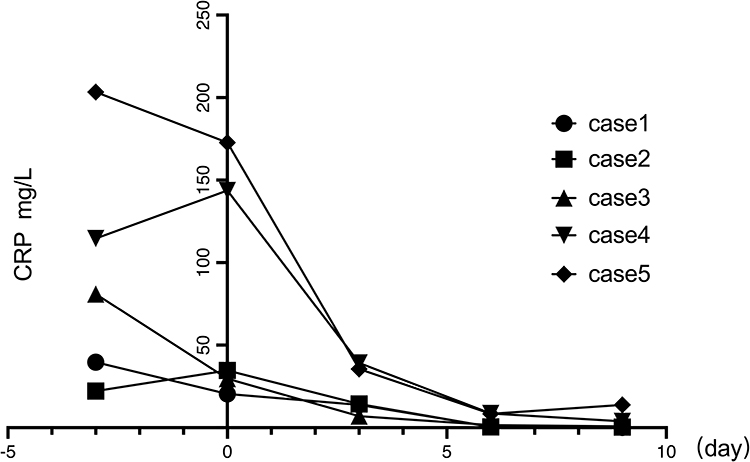 |
Figure 1 Changes of CRP before and after tocilizumab treatment. Before tocilizumab treatment, all patients had higher than normal CRP values, and the first test after tocilizumab treatment showed that CRP values decreased significantly, and the median CRP value decreased from 34.71mg/L (20.4mg/L −172.78mg/L) before treatment to 13.88 mg/L (7mg/L −39.21mg/L). Day 0 is when the first dose of tocilizumab was given. Abbreviation: CRP, C-reactive protein. |
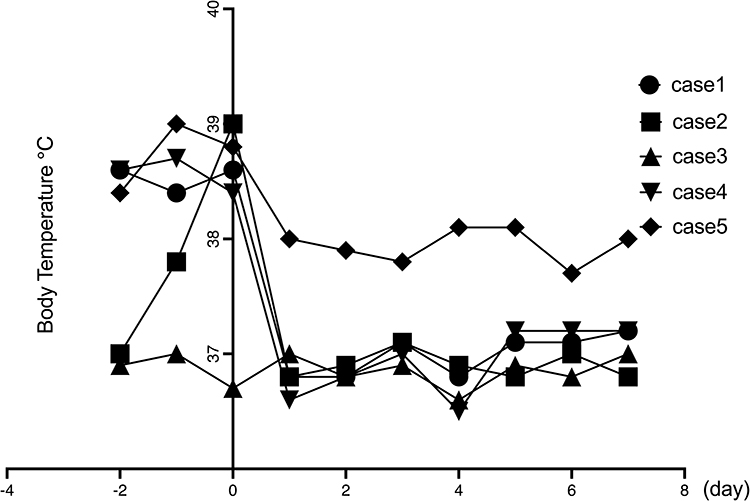 |
Figure 2 Changes in Body Temperature of patients before and after tocilizumab treatment. Before treatment with tocilizumab, all patients had fever (Tmax > 39°C), and after treatment with tocilizumab, body temperature decreased significantly within 24 hours, and the median Tmax decreased from 38.5°C (36.7°C-39°C) to 36.8°C (36.6°C-37.9°C). Day 0 is when the first dose of tocilizumab was given. Abbreviation: T, Temperature. |
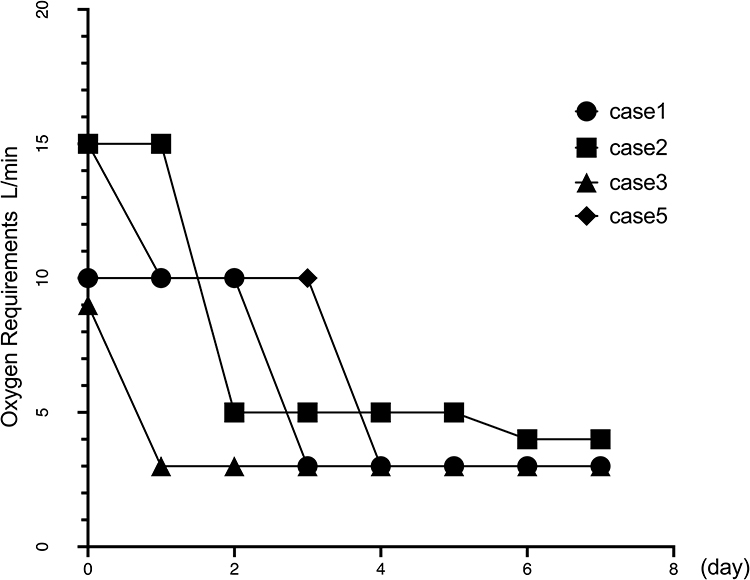 |
Figure 3 Changes in Oxygen Requirements by patients before and after tocilizumab treatment. Four patients improved their oxygen demand within 1–3 days after receiving tocilizumab (case 4 did not develop hypoxia during the course of the disease), and the median oxygen flow rate decreased from 10 L/min (9 L/min-15L/min) to 3 L/min (3L/min-10L/min). Day 0 is when the first dose of tocilizumab was given. |
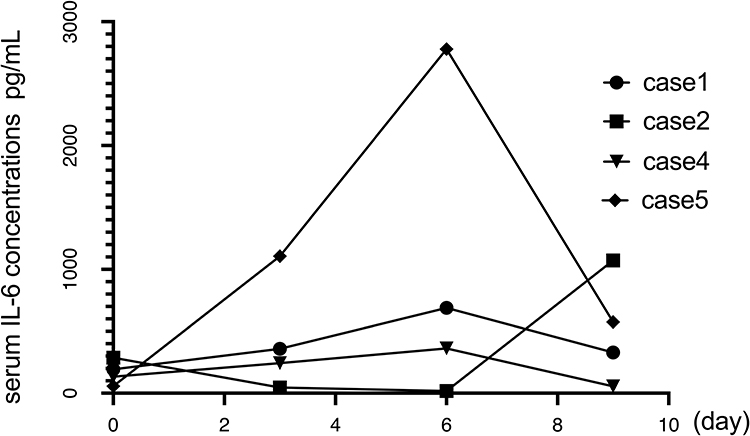 |
Figure 4 Changes of the serum IL-6 concentrations before and after tocilizumab treatment. The serum IL-6 concentrations of four patients before tocilizumab administration was 56.38–287.74pg/mL, which was higher than normal. After receiving tocilizumab, IL-6 levels first increased (362.85pg/mL −2778.07pg/mL) and then decreased (54.95pg/mL −574.37pg/mL). Case 3 did not monitor IL-6 before and after treatment. Day 0 is when the first dose of tocilizumab was given. Abbreviation: IL-6, interleukin-6. |
Discussion
In this retrospective study, all five patients received tocilizumab immediately after being diagnosed with severe COVID-19 infection. All patients showed effective disease control with rapid improvement in symptoms such as fever dyspnea and lab examinations such as CRP and CT pneumonia images without severe toxicity. One patient developed a secondary pulmonary fungal infection, and another died due to myelodysplastic syndrome progression—no deaths due to COVID-19 infection. Our experience suggests an early use of tocilizumab as soon as the patient met the diagnosis of severe COVID-19 infection and with an elevation of serum IL-6.
In three cases, there was an initial progressive increase followed by a subsequent decrease in serum IL-6 level after tocilizumab administration, which returned to normal within ten days. This clinical phenomenon is consistent with the findings of other reports.21–23 Zhao et al21 proposed that during COVID-19 infection, there is a rapid synthesis of IL-6, leading to a rapid increase in serum IL-6 levels in the body. By binding to the IL-6 receptor, tocilizumab does not affect the continuous synthesis of IL-6, resulting in the transient elevation of serum IL-6 levels. However, tocilizumab blocks the downstream effects of IL-6, preventing the inflammatory damage caused by IL-6. In this study, patients with elevated serum IL-6 levels after receiving tocilizumab did not experience worsened clinical symptoms.
According to the Diagnosis and Treatment Plan for Pneumonia Infected by Novel Coronavirus (10th Edition),11 antiviral treatment is recommended for COVID-19 in moderate and minor patients. Tocilizumab treatment is recommended first for COVID-19 severe/critical patients with elevated serum IL-6 levels. Tocilizumab combined with corticosteroid treatment is recommended for patients with hypoxemia. The number of cases in this clinical report is small, which is insufficient to conclude the true efficacy and safety of tocilizumab use in patients with hematologic tumors under severe COVID-19 infection. Some questions, such as whether tocilizumab can become a first-line recommended treatment for patients with blood tumors infected with COVID-19 and how to balance anti-tumor and antiviral treatment, require further investigations. However, the current clinical treatment findings can lay the foundation for future research.
In summary, tocilizumab can suppress the cytokine storm induced by COVID-19 and appears to be an effective treatment strategy for severe COVID-19 infection in hematologic malignant tumor patients with abnormal immune response abilities and minimal adverse events. However, the conclusions still need sufficient case numbers for further research and validation.
Data Sharing Statement
All available information is contained within the manuscript. Further inquiries can be directed to the corresponding author.
Ethics Statement and Consent for Publication
The patients have signed informed consent to publish the case details. The First Affiliated Hospital of Zhejiang University School of Medicine approves the publication of the case details.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and publication of this article: This study was supported by the National Nature and Science Foundation of China (Grant Numbers:82070200) and Zhuji Medical and Health Technology Plan Projiect (Grant Numbers:2023YW095).
Disclosure
The authors declare no potential conflicts of interest.
References
1. Bouchlarhem A, Es-saad O, Haddar L, et al. Special case of a patient in the blast phase of chronic myeloid leukemia successfully treated with tocilizumab during critical SARS-CoV-2 infection. J Int Med Res. 2022;50(3):030006052210828. doi:10.1177/03000605221082875
2. García-Suárez J, de la Cruz J, Cedillo Á. Impact of hematologic malignancy and type of cancer therapy on COVID-19 severity and mortality: lessons from a large population-based registry study. J Hematol Oncol. 2020;13(1). doi:10.1186/s13045-020-00970-7
3. Kuderer NM, Choueiri TK, Shah DP, et al. Clinical impact of COVID-19 on patients with cancer (CCC19): a cohort study. Lancet. 2020;395(10241):1907–1918. doi:10.1016/S0140-6736(20)31187-9
4. Garassino MC, Whisenant JG, Huang LC, et al. COVID-19 in patients with thoracic malignancies (TERAVOLT): first results of an international, registry-based, cohort study. Lancet Oncol. 2020;21(7):914–922. doi:10.1016/S1470-2045(20)30314-4
5. Grivas P, Khaki AR, Wise-Draper TM, et al. Association of clinical factors and recent anticancer therapy with COVID-19 severity among patients with cancer: a report from the COVID-19 and cancer consortium. Ann Oncol. 2021;32(6):787–800. doi:10.1016/j.annonc.2021.02.024
6. He W, Chen L, Chen L, et al. COVID-19 in persons with haematological cancers. Leukemia. 2020;34(6):1637–1645. doi:10.1038/s41375-020-0836-7
7. Pagano L, Salmanton-García J, Marchesi F, et al. COVID-19 infection in adult patients with hematological malignancies: a European Hematology Association Survey (EPICOVIDEHA). J Hematol Oncol. 2021;14(1):168. doi:10.1186/s13045-021-01177-0
8. Stebbing J, Phelan A, Griffin I, et al. COVID-19: combining antiviral and anti-inflammatory treatments. Lancet Infect Dis. 2020;20(4):400–402. doi:10.1016/S1473-3099(20)30132-8
9. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
10. Mahmudpour M, Roozbeh J, Keshavarz M, Farrokhi S, Nabipour I. COVID-19 cytokine storm: the anger of inflammation. Cytokine. 2020;133:155151. doi:10.1016/j.cyto.2020.155151
11. National Health Commission of the People’s Republic of China. Diagnosis and treatment plan for COVID-19(trial version 10). Int J Epidemiol Infect Dis. 2023;50:1–7. doi:10.3760/cma.j.cn331340-20230106-00004
12. Keller MJ, Kitsis EA, Arora S, et al. Effect of systemic glucocorticoids on mortality or mechanical ventilation in patients with COVID-19. J Hosp Med. 2020;15(8):489–493. doi:10.12788/jhm.3497
13. Lu S, Zhou Q, Huang L, et al; on behalf of COVID-19 Evidence and Recommendations Working Group. Effectiveness and safety of glucocorticoids to treat COVID-19: a rapid review and meta-analysis. Ann Transl Med. 2020;8(10):627. doi:10.21037/atm-20-3307
14. Wang L, Berger NA, Davis PB, Kaelber DC, Volkow ND, Xu R. COVID-19 rebound after paxlovid and molnupiravir during January-June 2022. Infect Dis. 2022. doi:10.1101/2022.06.21.22276724
15. Yang P, Ding Y, Xu Z, et al. Epidemiological and clinical features of COVID-19 patients with and without pneumonia in Beijing, China. Epidemiology. 2020. doi:10.1101/2020.02.28.20028068
16. Zhang C, Wu Z, Li JW, Zhao H, Wang GQ. Cytokine release syndrome in severe COVID-19: interleukin-6 receptor antagonist tocilizumab may be the key to reduce mortality. Int J Antimicrob Agents. 2020;55(5):105954. doi:10.1016/j.ijantimicag.2020.105954
17. Rosas IO, Bräu N, Waters M, et al. Tocilizumab in hospitalized patients with severe covid-19 pneumonia. N Engl J Med. 2021;384(16):1503–1516. doi:10.1056/NEJMoa2028700
18. Salama C, Han J, Yau L, et al. Tocilizumab in patients hospitalized with Covid-19 pneumonia. N Engl J Med. 2021;384(1):20–30. doi:10.1056/NEJMoa2030340
19. Ascierto PA, Fox BA, Urba WJ, et al. Insights from immuno-oncology: the society for immunotherapy of cancer statement on access to IL-6-targeting therapies for COVID-19. J Immunother Cancer. 2020;8(1):e000878. doi:10.1136/jitc-2020-000878
20. US Department of Health and Human Services. Common Terminology Criteria for Adverse Events (CTCAE); 2017. Available from: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf.
21. Zhao H, Zhu Q, Zhang C, et al. Tocilizumab combined with favipiravir in the treatment of COVID-19: a multicenter trial in a small sample size. Biomed Pharmacother. 2021;133:110825. doi:10.1016/j.biopha.2020.110825
22. Luo P, Liu Y, Qiu L, Liu X, Liu D, Li J. Tocilizumab treatment in COVID‐19: a single center experience. J Med Virol. 2020;92(7):814–818. doi:10.1002/jmv.25801
23. Xu X, Han M, Li T, et al. Effective treatment of severe COVID-19 patients with tocilizumab. Proc Natl Acad Sci USA. 2020;117(20):10970–10975. doi:10.1073/pnas.2005615117
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.