Back to Journals » International Journal of General Medicine » Volume 19
Using the Systemic Inflammatory Response Index and the Prognostic Nutritional Index in Predicting Subsequent Bone Metastases in Patients with Non-Small Cell Lung Cancer
Authors Wang P, Yan X, Yan G, Li D, Ma L ![]()
Received 29 December 2025
Accepted for publication 24 March 2026
Published 1 April 2026 Volume 2026:19 592374
DOI https://doi.org/10.2147/IJGM.S592374
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ching-Hsien Chen
Peng Wang,1 Xiaojing Yan,2 Guangxuan Yan,3 Dan Li,4 Li Ma2,5
1Department of Orthopaedics, Beijing Luhe Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Medical Affairs, Beijing Chest Hospital, Capital Medical University & Beijing Tuberculosis and Thoracic Tumor Research Institute, Beijing, People’s Republic of China; 3Department of Orthopaedics, Beijing Chest Hospital, Capital Medical University & Beijing Tuberculosis and Thoracic Tumor Research Institute, Beijing, People’s Republic of China; 4Functional Examination Section, Cancer Hospital Chinese Academy of Medical Sciences, Beijing, People’s Republic of China; 5Department of Medical Oncology, Beijing Chest Hospital, Capital Medical University & Beijing Tuberculosis and Thoracic Tumor Research Institute, Beijing, People’s Republic of China
Correspondence: Li Ma, Email [email protected]
Objective: This study aimed to identify the risk factors for Bone Metastases (BM) in patients with non-small cell lung cancer (NSCLC) and develop a scoring system combining the systemic inflammatory response index (SIRI) and prognostic nutritional index (PNI) to predict subsequent bone metastases in patients with NSCLC.
Methods: A retrospective analysis of patients with NSCLC treated at our hospital between February 2019 and January 2025 was conducted. Based on the occurrence of BM during follow-up, patients were stratified into the BM or the non-BM group. After their preoperative SIRI and PNI values were calculated, receiver operating characteristic (ROC) curve analysis was used to determine the optimal cut-off values for SIRI and PNI, which were used to establish the SIRI–PNI scoring system. The SIRI–PNI scores were compared between the groups, and univariate and multivariate logistic regression analyses were performed to identify factors influencing BM development.
Results: Among the 418 patients included with a mean follow-up of 11.91 ± 0.88 months (range: 9– 14 months), 142 were diagnosed with BM (33.97%). ROC analysis determined an optimal threshold of 539.0 for the SIRI (area under the curve [AUC] = 0.877; 95% confidence interval [CI]: 0.807– 0.947) and 44.8 for the PNI (AUC = 0.801; 95% CI: 0.689– 0.912). An SIRI–PNI scoring system was established, with scores ranging from 0 to 2. Clinical stage, lymph node metastasis, and SIRI–PNI score significantly differed between the BM and non-BM groups (P < 0.05). Multivariate analysis identified clinical stage IV (odds ratio = 11.91, P < 0.0001) and a SIRI–PNI score of 2 (P < 0.0001) as independent risk factors for BM.
Conclusion: Advanced clinical stage (IV) and a high SIRI–PNI score (2 points) are significant prognostic indicators for BM development in patients with NSCLC. The preoperative SIRI–PNI scoring system may facilitate early identification of high-risk patients.
Plain Language Summary: Bone Metastases (BM) are a frequent and debilitating complication of lung cancer, leading to skeletal-related events that severely compromise patient prognosis and quality of life. Early identification of high-risk individuals remains a clinical challenge, as current diagnostic methods are often resource-intensive and employed after symptomatic presentation.This study investigated the utility of a simple scoring system based on the systemic inflammatory response index (SIRI) and the prognostic nutritional index (PNI), both of which are derived from routine blood parameters, to predict the risk of subsequent BM in patients with non-small cell lung cancer (NSCLC).Analysis of 418 patients demonstrated that the combined SIRI and PNI score effectively stratified BM risk. Multivariate analysis identified advanced clinical stage (IV) and a high SIRI–PNI score as significant independent predictors of BM development.The proposed SIRI–PNI scoring system offers a readily accessible, non-invasive tool for the early risk stratification of patients with NSCLC. Its implementation could facilitate timely intervention strategies, such as enhanced surveillance or prophylactic bone-targeting therapy, to mitigate BM-related morbidity and improve clinical outcomes.
Keywords: systemic inflammatory response index, prognostic nutritional index, non-small cell lung cancer, bone metastases, prediction
Introduction
Lung cancer remains the leading cause of cancer-related mortality worldwide and a major global health burden. Recent epidemiological studies indicate that both the incidence and mortality of lung cancer remain high despite advances in screening and treatment strategies. Lung cancer accounts for a substantial proportion of global cancer-related deaths and imposes significant challenges on healthcare systems worldwide.1,2 In China, lung cancer has the highest incidence among all cancers, and its rate continues to rise.1,3 Among lung cancer subtypes, non-small cell lung cancer (NSCLC) accounts for approximately 85% of all cases. Patients with NSCLC often exhibit no specific symptoms in the early stages, and the risk of distant metastasis increases as the disease progresses.
Approximately 30–40% of patients with lung cancer develop bone metastases, making it one of the most frequent sites of distant spread.4 Bone Metastases (BM) is associated with a poor prognosis, with a median survival of approximately 6–10 months after diagnosis. BM frequently leads to skeletal-related events, including bone pain, pathological fractures, and impaired mobility, which significantly reduce quality of life and survival.5 Therefore, early identification of patients at high risk for BM is crucial for improving clinical management and prognosis in lung cancer.6,7
Currently, whole-body bone scintigraphy is a common clinical tool for diagnosing BM. However, its use is limited by high cost, significant radiation exposure, and limited accessibility. Consequently, there is considerable clinical value in identifying a low-cost, non-invasive predictive method or biomarker for early detection of BM in lung cancer. Peripheral blood inflammatory markers, such as neutrophil and lymphocyte counts, have established prognostic significance in various malignancies, including gastric cancer8 and gallbladder cancer.9 The systemic inflammatory response index (SIRI) is a hematological biomarker used to assess a patient’s inflammatory status, while the prognostic nutritional index (PNI) evaluates nutritional status and prognosis.10–13 Recent studies confirm that both indices are closely associated with disease progression, metastasis, and prognosis in various cancers.14,15 However, their role in predicting subsequent BM in lung cancer patients remains unexplored. To fill this research gap, this study investigated the clinical utility of a combined SIRI–PNI scoring system in predicting subsequent BM in patients with NSCLC to provide insights for BM prevention and management.
Materials and Methods
Study Design and Participants
This retrospective study enrolled patients diagnosed with NSCLC who received treatment at Beijing Chest Hospital between February 2019 and January 2025. The inclusion criteria were (1) diagnosis of NSCLC confirmed by biopsy or pathological examination, (2) initial consultation with no prior anti-tumor therapy, (3) availability of complete clinical data, and (4) ability to participate in follow-up. The exclusion criteria were (1) concomitant autoimmune diseases, (2) recent acute or chronic infectious diseases, (3) prior anti-tumor treatment, (4) presence of BM at initial diagnosis, (5) incomplete follow-up or clinical data, and (6) conditions that could significantly affect systemic inflammatory or nutritional status, such as acute infections, autoimmune diseases, or other severe inflammatory conditions. Ethical approval for this study was obtained from the Beijing Chest Hospital Ethics Committee (Ethical Approval No. BJXK-2025-KY-31). All patients provided written informed consent.
Data Collection
Demographic and clinical data, including sex, age, smoking history, histological type, clinical stage according to the 8th edition of the American Joint Committee on Cancer Staging Manual, tumor location, and lymph node metastasis status, were collected from electronic medical records. The clinical records were reviewed to identify potential conditions that could influence systemic inflammatory or nutritional indicators, such as acute infections or autoimmune diseases. Patients with one or more of these conditions identified during baseline evaluation were excluded from the study. All patients underwent imaging evaluation, including bone scintigraphy, positron emission tomography-computed tomography (PET-CT), computed tomography (CT), or magnetic resonance imaging (MRI), according to clinical guidelines to exclude pre-existing Bone Metastases.
Laboratory Measurements and Index Calculation
Within 1 week before surgery (or before initial systemic treatment for inoperable cases), peripheral venous blood was collected from all patients after an overnight fast. An automatic blood analyzer (Sysmex, Kobe, Japan) was used to measure neutrophil, lymphocyte, and platelet counts. Serum albumin level was measured using standard biochemical methods.
The SIRI was calculated as SIRI = NEUT (×109/L) × PLT (×109/L) / LY (×109/L).16
The PNI was calculated as PNI = ALB (g/L) + 5 × LY (×109/L).17
Follow-up and Definition of Bone Metastases
All patients were followed up via outpatient visits and telephone interviews. The follow-up cut-off date was October 1, 2025, and the endpoint was the first diagnosis of BM during follow-up. BM was diagnosed according to relevant guidelines18 if any of the following criteria were met: (1) positive findings on bone imaging (bone scan, PET-CT, or CT); (2) pathological confirmation of BM via bone biopsy; or (3) suggestive findings of bone destruction on CT or MRI with exclusion of other benign bone diseases.
Establishment of the SIRI–PNI Scoring System
Receiver operating characteristic (ROC) curve analysis was performed to determine the optimal cut-off values for SIRI and PNI. Based on these cut-offs, a composite SIRI–PNI scoring system ranging from 0 to 2 was established to indicate the following:
0 points: SIRI below the cut-off AND PNI above the cut-off.
1 point: SIRI above the cut-off OR PNI below the cut-off.
2 points: SIRI above the cut-off AND PNI below the cut-off.
Statistical Analysis
The sample size was considered sufficient according to the events-per-variable principle for logistic regression analysis. Data were analyzed using SPSS statistical software (version 21.0, IBM Corp., Armonk, NY, USA). Normally distributed quantitative data are presented as the mean ± standard deviation and were compared using the independent samples t-test. Categorical and ordinal data are presented as the frequency (percentage) and were compared using the chi-square test or Fisher’s exact test, as appropriate. Univariate and multivariate logistic regression analyses (backward stepwise method, with entry and removal criteria set at P < 0.10 and P < 0.05, respectively) were performed to identify independent risk factors for BM, with the results expressed as odds ratios (ORs) and 95% confidence intervals (CIs). The predictive performance of the SIRI-PNI model was assessed using ROC curves, and the results were reported as the area under the curve (AUC), sensitivity, and specificity. Pearson’s correlation coefficient was used to analyze the relationship between SIRI and PNI. The multicollinearity among variables included in the regression model was evaluated using the variance inflation factor (VIF), with VIF < 5 was considered acceptable. A two-tailed P-value < 0.05 was considered statistically significant. To evaluate potential overfitting and assess the stability of the predictive model, internal validation was performed using bootstrap resampling with 1000 iterations.
Results
Patient Characteristics
A total of 418 patients with NSCLC were included in the final analysis. Their demographic and clinical characteristics are summarized in Table 1. Further analyses exploring the association between the SIRI–PNI score and clinicopathological characteristics revealed that the SIRI–PNI score was significantly associated with clinical stage (P < 0.001) but not histological subtype (P > 0.05).
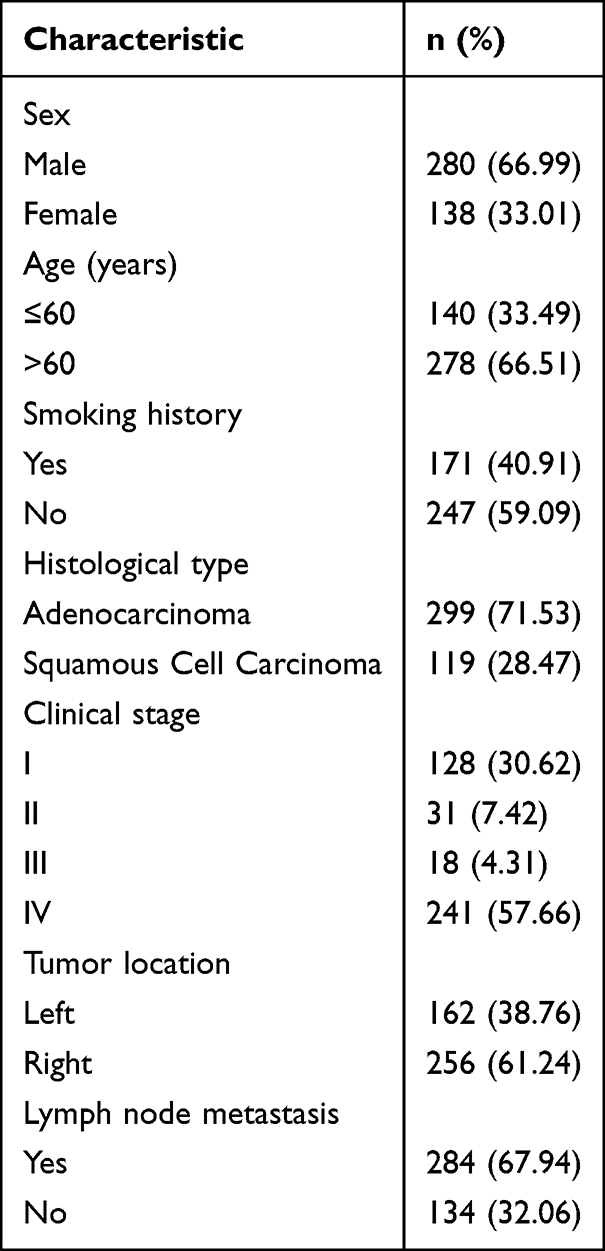 |
Table 1 Baseline Demographic and Clinical Characteristics of Patients with NSCLC (n = 418) |
SIRI-PNI Cut-off Values and Predictive Performance
ROC curve analysis (Figure 1) revealed that the optimal cut-off value for the SIRI was 539.0, with an AUC of 0.877 (95% CI: 0.807–0.947), a sensitivity of 86.36%, and a specificity of 72.73%. The optimal cut-off for the PNI was 44.8, with an AUC of 0.801 (95% CI: 0.689–0.912), a sensitivity of 81.40%, and a specificity of 74.42%. A significantly negative correlation was observed between the SIRI and PNI (r = –0.711, P < 0.001). Using these thresholds, the SIRI–PNI scoring system was developed as described in the Methods section.
 |
Figure 1 Receiver operating characteristic (ROC) curves of SIRI and PNI for predicting bone metastases in NSCLC. The AUC values were 0.877 for SIRI and 0.801 for PNI. Abbreviations: SIRI, systemic inflammatory response index; PNI, prognostic nutritional index; AUC, area under the curve; NSCLC, non-small cell lung cancers. |
Univariate Analysis of Factors Associated with Bone Metastases
During a mean follow-up of 11.91 ± 0.88 months (range: 9–14 months), 142 patients (33.97%) developed BM (BM group), while 276 did not (non-BM group). Univariate analysis (Table 2) revealed statistically significant differences between the two groups in clinical stage, lymph node metastasis status, and SIRI–PNI score (all P < 0.05) but not in sex, age, smoking history, histological type, or tumor location (all P > 0.05). Notably, 92.96% of patients in the BM group were at clinical stage IV, and 58.45% had a SIRI–PNI score of 2; in contrast, no patients in the non-BM group had a score of 2.
 |
Table 2 Univariate Analysis of Factors Associated with Bone Metastases in Patients with NSCLC |
Multivariate Logistic Regression Analysis for Bone Metastases
When variables with P < 0.10 in the univariate analysis (clinical stage, lymph node metastasis, and SIRI–PNI score) were entered into the multivariate logistic regression model, clinical stage IV (OR = 11.91, 95% CI: 5.29–26.78, P < 0.0001) and a SIRI–PNI score of 2 emerged as significant independent predictors of BM (Table 3). Notably, no patients in the non-BM group had a SIRI–PNI score of 2. Consequently, the estimated OR was extremely large, reflecting a very strong association between a high SIRI–PNI score and the occurrence of BM.
 |
Table 3 Multivariate Logistic Regression Analysis of Risk Factors for Bone Metastases in Patients with NSCLC |
Discussion
The findings of this study demonstrate that a preoperative scoring system combining the SIRI and the PNI effectively predicts the risk of subsequent BM in patients with primary NSCLC. Accordingly, a high SIRI–PNI score (2 points) and advanced clinical stage (IV) were found to be strong independent risk factors for BM development.
Occurring in 20–40% of patients with NSCLC, BM signifies disease progression often leading to skeletal-related events that severely compromise quality of life and survival.5 Although bone scintigraphy remains a key diagnostic tool, its limitations necessitate the identification of accessible, non-invasive biomarkers for early risk stratification.6,7 Inflammation and nutritional status are increasingly recognized as critical determinants of cancer progression and metastasis.10,12 Integrating neutrophil, platelet, and lymphocyte counts, the SIRI reflects systemic inflammation,16,19 whereas the PNI, based on albumin and lymphocyte counts, assesses nutritional and immune status.17,20
Both indices have shown prognostic value in various cancers, including lung cancer,12,13,21 but their combined role in predicting BM has, until now, been unclear. The ROC analysis conducted in this study demonstrated the robust predictive ability of both indices for BM, with the SIRI showing slightly higher discriminatory power (AUC 0.877) than the PNI (AUC 0.801). The significantly negative correlation between the SIRI and PNI underscores the interplay between inflammation and malnutrition in advanced cancer. The SIRI–PNI scoring system developed in this study effectively stratified the participants into distinct risk categories. The stark contrast between the study groups—58.45% of the BM group had a SIRI–PNI score of 2 compared with 0% of the non-BM group—highlights its potential clinical utility.
The biological plausibility of the findings is supported by the roles performed by the cellular components represented in the SIRI-PNI. A high SIRI reflects elevated neutrophils and/or platelets alongside relative lymphopenia. Neutrophils can promote tumor angiogenesis and invasion by releasing proteases and pro-angiogenic factors.14 Platelets facilitate tumor cell adhesion and extravasation during hematogenous dissemination, potentially promoting metastasis to bone marrow sinusoids.22 Conversely, lymphocytes are crucial for anti-tumor immune surveillance; lymphopenia may indicate impaired immune defense against metastatic spread. Low serum albumin level, a component of the PNI, is a marker of both nutritional depletion and systemic inflammatory response, which can foster a pro-tumor microenvironment.15 Thus, a patient with a high SIRI–PNI score is likely in a profound pro-inflammatory, pro-tumor, and nutritionally compromised state, which creates a biological milieu conducive to bone metastases.
Emerging evidence suggests that systemic inflammatory indicators are closely linked to the tumor immune microenvironment and may influence metastatic progression. Chronic inflammatory conditions can reshape the immune landscape, promoting tumor immune escape and facilitating tumor dissemination. Recent studies have emphasized the importance of interactions among systemic inflammation, immune infiltration, and tumor progression in lung cancer. For example, dysregulation of immune-related signaling pathways and chronic inflammatory states may alter immune cell recruitment and remodeling of the tumor microenvironment, thereby contributing to tumor metastasis and disease progression.23 In addition, specific molecular biomarkers associated with immune regulation have been identified as potential prognostic indicators in lung cancer. For example, TTC21A has been associated with immune cell infiltration patterns and clinical outcomes in lung adenocarcinoma, highlighting the relevance of immune-related molecular markers in tumor progression.24 Furthermore, certain microRNAs, such as miR-4271, have been shown to regulate receptor expression and drug sensitivity in NSCLC through modulation of intracellular signaling pathways.25 These findings suggest that inflammatory and nutritional indices, such as the SIRI-PNI, serve as integrative biomarkers reflecting both systemic inflammatory status and immune microenvironment alterations, providing biological evidence for their association with metastatic risk.
Unsurprisingly, advanced clinical stage (IV) was a major risk factor, consistent with the biology of metastatic disease. Lymph node metastasis was significant in the univariate analysis but failed to remain an independent predictor in the multivariate model, likely due to its collinearity with advanced stage and the overwhelming predictive strength of the SIRI–PNI score. Because none of the patients in the non-BM group had an SIRI–PNI score of 2, the logistic regression estimate was extremely large, reflecting the strong discriminatory ability of this score.
Despite its development of a promising clinical scoring system and identification of risk factors, this study has several limitations. First, its retrospective, single-center design may have introduced selection bias. Second, although the sample size was adequate for the primary analyses, the relatively small cohort limited the ability to perform more detailed subgroup analyses. Third, the median follow-up period was approximately 12 months. Although baseline imaging examinations were performed to exclude existing BM at diagnosis, longer follow-up may be required to capture late-occurring bone metastases. Because the primary aim of this study was to identify risk factors for the occurrence of bone metastasis and to develop a predictive scoring system rather than to analyze time-to-event outcomes, logistic regression analysis was used. Future studies with longer follow-up durations may further explore time-to-event analyses using Cox proportional hazards models. Finally, the extremely large OR observed for the SIRI–PNI score of 2 likely reflects the absence of this score in the non-BM group, which may have resulted in unstable estimates in the logistic regression model. Future prospective multicenter studies with larger cohorts and longer follow-up durations are needed to validate these findings and refine the cut-off values.
Conclusions
The preoperative SIRI–PNI scoring system developed in this study is a simple, non-invasive, clinically accessible tool for identifying patients with NSCLC at high risk of developing BM and predicting the risk of BM in patients with primary lung cancer. Combining readily available laboratory parameters, the score reflects the interplay of systemic inflammation and nutritional status. Identifying patients with a high SIRI–PNI score, particularly those with stage IV disease, enables clinicians to perform more vigilant monitoring, consider early bone-modifying agents, and tailor personalized treatment strategies to mitigate the morbidity associated with bone metastases.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available due to patient privacy regulations but are available from the corresponding author on reasonable request.
Ethics Statement
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of the Beijing Chest Hospital affiliated with Capital Medical University (Approval No. BJXK-2025-KY-31).
Acknowledgments
The authors thank all patients who participated in this study and the clinical staff involved in patient care and data collection. The authors would like to thank the professional editing service for English language editing.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article was submitted; and agreed to be accountable for all aspects of the work.
Funding
This study was funded by the Beijing Municipal Health Commission’s Diversified Cultivation Program for Medical Social Workers (YG239002, L.M.), the Beijing Municipal Science and Technology Commission Application Scenario Project (20230470104, L.M.), and the 2024 Annual Excellent Clinical Research Program Project of Research-Oriented Wards (BRWEP2024W042160105, L.M.).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Siegel RL, Kratzer TB, Wagle NS, et al. Cancer statistics, 2026. CA Cancer J Clin. 2026;76(1):e70043. doi:10.3322/caac.70043
2. Lu ZM, Xu SS, Ye M, et al. Comparison of pembrolizumab plus chemotherapy versus concurrent or sequential radiochemotherapy in patients with driver mutation-lacking lung adenocarcinoma presenting with recurrent laryngeal nerve invasion leading to hoarseness. J Clin. 2024;Oncol:42e14635.
3. Huang J, Deng Y, Tin MS, et al. Distribution, risk factors, and temporal trends for lung cancer incidence and mortality: a global analysis. Chest. 2022;161(4):1101–9. doi:10.1016/j.chest.2021.12.655
4. Shen H, Deng G, Chen Q, Qian J. The incidence, risk factors and predictive nomograms for early death of lung cancer with synchronous brain metastasis: a retrospective study in the SEER database. BMC Cancer. 2021;21(1):825. doi:10.1186/s12885-021-08490-4
5. Bessa CM, Silva LMD, Zamboni MM, et al. Bone metastases after stage IIIA non-small cell lung cancer: risks and prognosis. J Bras Pneumol. 2022;48(5):e20220211. doi:10.36416/1806-3756/e20220211
6. Hu X, Huang W, Sun Z, et al. Predictive factors, preventive implications, and personalized surgical strategies for bone metastases from lung cancer: population-based approach with a comprehensive cancer center-based study. EPMA J. 2022;13(1):57–75. doi:10.1007/s13167-022-00270-9
7. Miyashita H, Cruz C, Smith C. Risk factors of skeletal-related events in patients with bone metastases from non-small cell lung cancer undergoing treatment with zoledronate—a post hoc analysis of a randomized clinical trial. Support Care Cancer. 2021;29(3):1629–1633. doi:10.1007/s00520-020-05665-w
8. Aoyama T, Hara K, Kazama K, Maezawa Y. Clinical impact of nutrition and inflammation assessment tools in gastric cancer treatment. Anticancer Res. 2022;42(11):5167–5180. doi:10.21873/anticanres.16023
9. Li L, Ren T, Liu K, et al. Development and validation of a prognostic nomogram based on the systemic immune-inflammation index for resectable gallbladder cancer to predict survival and chemotherapy benefit. Front Oncol. 2021;11:692647. doi:10.3389/fonc.2021.692647
10. Song M, Zhang Q, Song C, et al. The advanced lung cancer inflammation index is the optimal inflammatory biomarker of overall survival in patients with lung cancer. J Cachexia Sarcopenia Muscle. 2022;13(5):2504–2514. doi:10.1002/jcsm.13032
11. Li W, Qu Y, Wen F, et al. Prognostic nutritional index and systemic immune-inflammation index are prognostic biomarkers for non-small-cell lung cancer brain metastases. Biomarker Med. 2021;15(13):1071–1084. doi:10.2217/bmm-2020-0786
12. Zaitsu J, Yamashita Y, Ishikawa A, et al. Systemic inflammatory score predicts response and prognosis in patients with lung cancer treated with immunotherapy. Anticancer Res. 2021;41(7):3673–3682. doi:10.21873/anticanres.15158
13. Zuo R, Zhu F, Zhang C, et al. The response prediction and prognostic values of systemic inflammation response index in patients with advanced lung adenocarcinoma. Thorac Cancer. 2023;14(16):1500–1511. doi:10.1111/1759-7714.14893
14. Lin KB, Fan FH, Cai MQ, et al. Systemic immune inflammation index and system inflammation response index are potential biomarkers of atrial fibrillation among the patients presenting with ischemic stroke. Eur. J Med Res. 2022;27(1):106.
15. Wang D, Hu X, Xiao L, et al. Prognostic nutritional index and systemic immune-inflammation index predict the prognosis of patients with HCC. J Gastrointest Surg. 2021;25(2):421–427. doi:10.1007/s11605-019-04492-7
16. Xu Y, He H, Zang Y, et al. Systemic inflammation response index (SIRI) as a novel biomarker in patients with rheumatoid arthritis: a multi-center retrospective study. Clin Rheumatol. 2022;41(7):1989–2000. doi:10.1007/s10067-022-06122-1
17. Lv Y, Ji ML, Feng QY, et al. Combined test of third lumbar skeletal muscle index and prognostic nutrition index improve prognosis prediction power in resected colorectal cancer liver metastasis. Aging. 2019;11(22):10301–10315. doi:10.18632/aging.102457
18. Link H, Diel I, Ohlmann CH, et al. Guideline adherence in bone-targeted treatment of cancer patients with bone metastases in Germany. Support Care Cancer. 2020;28(5):2175–2184. doi:10.1007/s00520-019-05018-2
19. Wang C, Jin S, Xu S, Cao S. The combination of pretreatment prognostic nutritional index and neuron-specific enolase enhances prognosis predicting value of small cell lung cancer. Clin Respir J. 2021;15(3):264–271. doi:10.1111/crj.13291
20. Matsuura S, Morikawa K, Ito Y, et al. The geriatric nutritional risk index and prognostic nutritional index predict the overall survival of advanced non-small cell lung cancer patients. Nutr Cancer. 2022;74(5):1606–1613. doi:10.1080/01635581.2021.1960387
21. Zhang Q, Bao J, Zhu ZY, Jin MX. Prognostic nutritional index as a prognostic factor in lung cancer patients receiving chemotherapy: a systematic review and meta-analysis. Eur Rev Med Pharmacol Sci. 2021;25(18):5636–5652.
22. Li Y, Xu C, Yu Q. Risk factor analysis of bone metastases in patients with non-small cell lung cancer. Am J Transl Res. 2022;14(9):6696–6702.
23. Li GQ, Wan YX, Jiao A, et al. Chronic diseases and tumor immune microenvironment interactions in cancer progression. Med Res. 2025;1:62–102.
24. Wang W, Ren S, Wang Z, Zhang C, Huang J. Increased expression of TTC21A in lung adenocarcinoma infers favorable prognosis and high immune infiltrating level. Int Immunopharmacol. 2020;78:106077. doi:10.1016/j.intimp.2019.106077
25. Huang H, Han Z, Xiao L, et al. Hsa-miR-4271 downregulates the expression of constitutive androstane receptor and enhances in vivo the sensitivity of non-small cell lung cancer to gefitinib. Pharmacol Res. 2020;161:105110. doi:10.1016/j.phrs.2020.105110
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Effect of Systemic Immune-Inflammatory Index (SII) and Prognostic Nutritional Index (PNI) in Early Gastric Cancer
Jing Y, Ren M, Li X, Sun X, Xiao Y, Xue J, Liu Z
Journal of Inflammation Research 2024, 17:10273-10287
Published Date: 4 December 2024
Geriatric Nutritional Risk Index (GNRI) and Prognostic Nutritional Index (PNI) Before Treatment as the Predictive Indicators for Bone Metastasis in Prostate Cancer Patients
Chen L, Rao H, Chen N, Li R, Chen D, Jiang H
International Journal of General Medicine 2025, 18:2703-2713
Published Date: 24 May 2025
The Influence of Characteristics and Indexes (NLR, PNI, and SII) Evaluated at Admission on the Mortality Prediction of Infectious Endocarditis Patients
Sezen AI, Ozdemir YE, Borcak D, Goklu BN, Bilgin Z, Turkyilmaz G, Caglar FNT, Gedik H, Kart Yasar K
International Journal of General Medicine 2025, 18:5617-5627
Published Date: 18 September 2025