Back to Journals » Advances in Medical Education and Practice » Volume 7
Using consensus methods to develop a country-specific Master of Public Health curriculum for the Republic of Maldives
Authors Robotin M, Shaheem M, Ismail AS
Received 2 September 2015
Accepted for publication 11 November 2015
Published 12 February 2016 Volume 2016:7 Pages 73—80
DOI https://doi.org/10.2147/AMEP.S95614
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Video abstract presented by Muthau Shaheem.
Views: 293
Monica C Robotin,1,2 Muthau Shaheem,3 Aishath S Ismail3
1Faculty of Medicine, School of Public Health, University of Sydney, 2Cancer Programs Division, Cancer Council New South Wales, Sydney, Australia; 3Faculty of Health Sciences, Maldives National University, Male, Maldives
Background: Over the last four decades, the health status of Maldivian people improved considerably, as reflected in child and maternal mortality indicators and the eradication or control of many communicable diseases. However, changing disease patterns are now undermining these successes, so the local public health practitioners need new skills to perform effectively in this changing environment. To address these needs, in 2013 the Faculty of Health Sciences of the Maldives National University developed the country's first Master of Public Health (MPH) program.
Methods: The process commenced with a wide scoping exercise and an analysis of the curricular structure of MPH programs of high-ranking universities. Thereafter, a stakeholder consultation using consensus methods reached agreement on overall course structure and the competencies required for local MPH graduates. Subsequently, a working group developed course descriptors and identified local public health research priorities, which could be addressed by MPH students.
Results: Ten semistructured interviews explored specific training needs of prospective MPH students, key public health competencies required by local employers and preferred MPH training models. The recommendations informed a nominal group meeting, where participants agreed on MPH core competencies, overall curricular structure and core subjects. The 17 public health electives put forward by the group were prioritized using an online Delphi process. Participants ranked them by their propensity to address local public health needs and the locally available teaching expertise. The first student cohort commenced their MPH studies in January 2014.
Conclusion: Consensus methods allowed a broad stakeholder engagement with public health curriculum development and the creation of a country-specific curriculum, informed by local realities and needs.
Keywords: public health, education, MPH, curriculum development, consensus methods
Introduction
The Republic of Maldives is a collection of 1,190 small islands situated on the southwest of Sri Lanka, in the Indian Ocean. Despite covering an area of more than 90,000 km2, the country’s land area is just 298 km2; the Maldives is the smallest Asian country and its total population is ~325,000.1 The country has an average elevation of 1.5 m above sea level, making it one of the most vulnerable countries to climate change on the planet.1 Until recently, the country’s health profile was dominated by communicable diseases, a limited access to health care, and overall poor health indicators.2 The last 40 years witnessed significant health gains, largely attributable to the successful implementation of a social goal of “Health for all”, using a Primary Health Care strategy,3 delivered by locally trained multipurpose health workers.2 Their work led to substantial reductions in child and adult mortality and morbidity and led to the eradication of malaria and significant success in controlling other communicable diseases.2 Consequently, Maldivians currently enjoy better standards of health than most other countries in the South Asian Region. These gains are being slowly eroded by the changing patterns of disease brought about by epidemiological transition, as the Maldives also have a higher noncommunicable disease burden and more noncommunicable disease risk factors than neighboring states.4–7 Some of the significant public health challenges of recent years include the reemergence of some communicable diseases, a relatively high proportion of underweight children, rising trends of substance abuse, and the health impacts of rapid urbanization and climate change.3
Consequently, new disease prevention strategies and a modern, well-trained public health workforce are required in order to address these new challenges, particularly as until recently opportunities for postgraduate public health education for midlevel health managers were quite limited. However, since 1973, the Allied Health Services Training Centre and subsequently the Faculty of Health Sciences (FHS) were established to deliver local undergraduate public health education for the country’s primary health care workforce and professional training for nurses, pharmacists, and lab technologists. To build on these foundations, in 2013, the FHS carried out a scoping exercise, to inform the development of the country’s first Master of Public Health (MPH) course. This involved the establishment of an Advisory Committee, consisting of prospective employers of MPH graduates and Heads of Departments from the Faculty of Health Sciences. They agreed on the overall process and recommended using consensus methods to guide decision making.
Formal consensus methods have been extensively used to facilitate decision making in medicine and in health research,8 leading to agreement in situations where the evidence is limited or unclear, or where the position of the key stakeholders may be divergent.9 The anonymous answers can allow participants to express their “true” opinions,10 eschewing a “groupthink” mentality. The Delphi process allows a structured interaction of a diverse stakeholder group,11 keeping the interaction on topic and on time.
This paper describes the overall priority setting process and the methodologies used to reach consensus and develop a Maldivian MPH course, informed by local realities and needs.
Methods
The formal process commenced with a wide consultation involving a survey of local academics, health care providers, and organizations engaged in the delivery of primary health care in the country. The FHS convened a curriculum steering group, comprising two academic leads from the Faculty of Health Sciences (its Dean and the Head of the Public Health Department) and a visiting Australian Public Health academic. The FHS conducted a local market analysis of prospective employers to gauge the demand for alumni with postgraduate public health qualifications, and help determine MPH class sizes in the short to medium term.
The steering group agreed on a framework and intermediate stages for the MPH curriculum development. The key steps in the process are summarized in Figure 1.
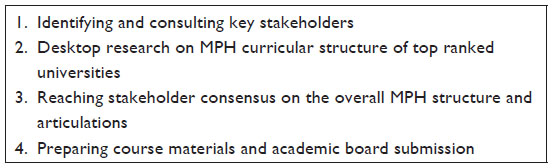 | Figure 1 Steps used in the Maldivian curriculum development process. |
Identifying and consulting key stakeholders
The steering group developed a list of local stakeholders in the MPH development process. They included Maldives National University (MNU) academics and senior administrative staff, potential employers and funders of public health research, representatives from the Ministry of Health, the Health Protection Agency, the World Health Organization, and a local nongovernment organization working on health and development. An interview template was developed by the curriculum steering group and utilized to guide the semistructured interviews (Figure S1). This format was deemed optimal for eliciting relevant information from local experts expeditiously and facilitating an open exchange of ideas about public health educational needs. Interview questions sought to identify stakeholders’ views on the salient local public health needs, the training needs of the existing public health workforce, organizational capacity to support MPH course development, preferred MPH training models and core competencies of the local MPH graduates.
Desktop research on MPH curricular structure of top ranked universities
To gain a better understanding of the range of MPH programs offered internationally, we conducted desktop research on MPH curricular structure of high-ranking MPH programs listed in the QS Stars system, the World Universities, and the Times Higher Education, and/or personally suggested by local stakeholders, as graduates of those programs. We researched publicly available data on MPH course structure, duration, prerequisites, and core and elective subjects on offer.
Reaching consensus on MPH structure and articulations
Given the diversity of the stakeholder group, their different roles, and levels of experience and seniority, the steering group decided to use consensus methods to reach agreement on curricular structure. A nominal group consultation reviewed the information collected through in-depth interviews and the results of desktop research on curricular structure, discussed local MPH core competencies, and agreed on the overall MPH structure, its core subjects, and suggested possible elective subjects relevant for the Maldives. Participants included FHS academic staff, MPH graduates from other universities, prospective students and other representatives from previously identified stakeholder groups. The process was finalized through an online Delphi process, which invited participants to rank the proposed elective subjects by their ability to meet local public health needs and the availability of local teaching expertise to deliver them.
Preparing course materials and academic board submission
After reaching consensus on course structure, the Australian academic worked in collaboration with local academics to write course descriptors for all subjects and prepared the submission for the new course to be approved by the MNU Committee on courses.
Results
Identifying and consulting key stakeholders
During July–August 2013, we conducted semistructured interviews with a total of nine stakeholders, comprising two FHS academics, three representatives from the Maldivian Ministry of Health, two from the Health Protection Agency, and one each from the World Health Organization and the International Center for Environment, Development and Operational Research (ENDEVOR). Participants were invited to comment on the salient issues and concerns in local health care delivery and related public health learning needs for the Maldivian health workforce. Data were analyzed inductively and the main training needs identified are briefly summarized in Figure 2.
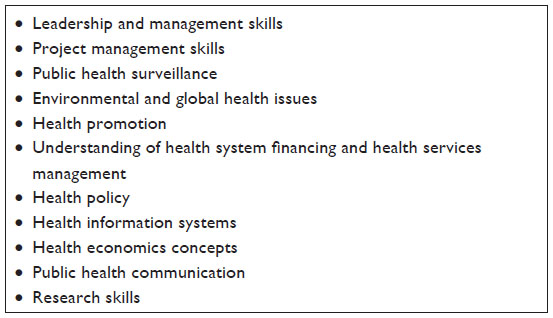 | Figure 2 Public health training needs identified by Maldivian stakeholders. |
As many prospective students were already engaged in health care delivery or administration, participants recommended that the MPH program should strengthen students’ leadership, management, and research skills. They recommended the inclusion of research in the core subjects. In their view, students had to be involved in all steps of the research process, from defining research questions, writing research proposals, preparing an Ethics application, collecting and analyzing data, and producing research reports and academic publications. They suggested that work placements could offer students direct experience in policy development and on the evaluation, planning, costing, and implementation of public health interventions.
Desktop research on MPH curricular structure of top ranked universities
The Australian academic researched the curricular structure of 20 MPH programs from different world regions, including five universities each from Australia, North America, the UK, and the Asian region. The selection of these regions was also prompted by the fact that universities from these regions represent the most common Alma Maters of most Maldivian stakeholders who completed or were intending to enroll in public health degrees. While the majority of the programs were of 12 months’ duration, six programs offered full time courses of 2 years’ duration.
The majority of the courses included core and elective subjects and enabled streaming or specialization. The most common core subjects included epidemiology, biostatistics, research methods, and Public Health Foundations. Some programs also included environmental health, health promotion, and health administration as core subjects. To provide a practical component, many courses stipulated the completion of a research project and/or a Professional Practice Unit (Australian universities) or a practicum and capstone or culminating experience (US universities) or a dissertation (UK universities).
One program offered an integrated curriculum, combining content from discipline-specific courses in biostatistics, environmental health, epidemiology, health administration, and social and behavioral sciences, delivered through a modular course offering cross-disciplinary topics, reinforced through skills-building sessions.12
Reaching consensus on MPH structure and articulations
The 14 attendees (representatives of designated stakeholder groups) included FHS academic staff, MPH graduates of overseas universities, prospective students, and representatives of stakeholder groups. The workshop commenced with a review of the findings of in-depth interviews and those of the desktop research and went on to seek agreement on the key competencies expected of Maldivian MPH graduates and on overall course structure.
Participants worked in small groups to generate recommendations for the knowledge and skills required by Maldivian Public Health practitioners. They included understanding of health economics, health financing, public health leadership and management, communication skills, and facility to use electronic media.
Finally, participants worked together as one group to define core and elective MPH subjects. Using a round robin strategy, each participant suggested his or her top three priorities for MPH core subjects. All suggestions were recorded on a flip chart by the workshop facilitator and the number of “votes” for each subject was tallied. The group reached agreement on the titles of core subjects, the content area they covered, and their interrelationships. Participants concurred that some subjects would cover more than one content area (eg, “Public Health Leadership and Management”), but that mergers were not appropriate for other subjects (eg, epidemiology and biostatistics would be stand-alone subjects).
Participants proposed 19 MPH core subjects, ultimately consolidated into six core subjects. A similar process led to the consolidation of the 35 proposed electives into 17 subjects.
To finalize the curricular structure, we employed a modified online Delphi process, which invited nominal group participants to finalize the elective MPH subject list. Participants were invited to rank their top 8 choices among the proposed 17 electives, according to the extent to which they addressed local public health needs (in a first round) and by taking into account the availability of local teaching resources (in the second and final round). Participants were also invited to provide feedback on the priority setting process.
The consensus process was completed over a period of 2 weeks, in August 2013. The final list of MPH subjects is provided in Table 1.
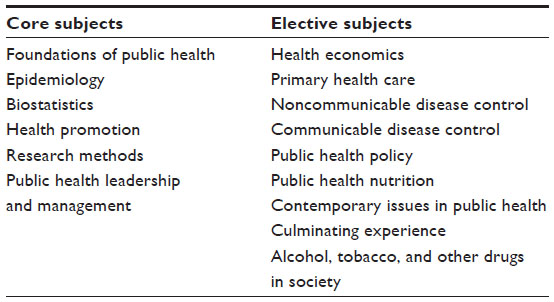 | Table 1 Core and elective subjects for the Maldives National University MPH program |
The overall MPH structure was developed in line with stakeholder recommendations and is depicted diagrammatically in Figure 3. All core subjects (six subjects of 20 credit points each) are part of the year 1 curriculum. Following successful completion of the 1st year of study, students can exit the program with a Graduate Diploma in Public Health, or go on to complete their MPH through a Professional Practice stream (involving six elective subjects and a smaller research project), or a research-based stream (involving four electives and a more substantial research project). Both streams require students to work independently, as well as to work in groups to complete some tasks.
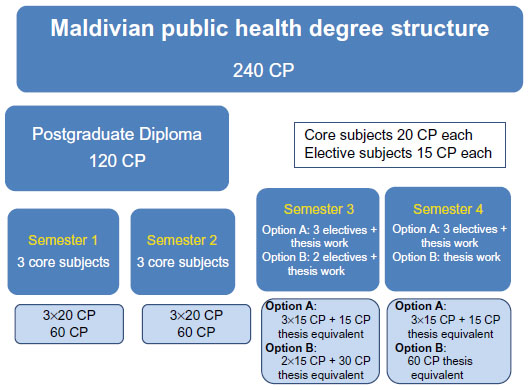 | Figure 3 A diagrammatic representation of the MPH subjects and their articulations. |
Preparing course materials and an academic board submission
Following stakeholder endorsement of the overall course structure and deliverables, we established an advisory group at faculty level, to guide the development of course descriptors, subject outlines, learning activities, and assessments for each subject.
The group recommended the inclusion of a culminating experience in the 2nd year of study. This requires students to identify and address a topical public health issue in the Maldives, research it, and prepare either an ethics application (Research stream students) or a Ministerial briefing on an emerging public health topic (Professional Practice stream).
The MNU Committee on Courses approved the MPH course in October 2013 and the first MPH student intake occurred in the 2014 academic year, enrolling eleven students. Eight students (73%) went on to complete the MPH program and will be graduating in November 2015.
Discussion
We described herein the process of developing the first Maldivian MPH program, designed to address the specific needs of a developing country with a small and widely dispersed population, facing a broad range of public health challenges.3
We believe that this experience is relevant not only for newly established public health programs, but its recommendations may also be relevant for well-established MPH programs, as a changed educational environment and evolving teaching and learning needs are driving a process of “curriculum renewal”, at many established MPH programs at some American Universities,12,13 as well as in other world regions. For example, following the collapse of the old Soviet Union, the Central Asian Republic of Kyrgyzstan developed a new public health curriculum, to equip Kyrgyz students with the knowledge and skills that can ensure the maintenance of basic standards of public health.14
A recent review of Italian Public Health teaching sought to ascertain the extent to which the local postgraduate medical schools delivered the expected standards of education stipulated by the local Ministry of Health. The great majority of schools delivered on the prescribed milestones for MPH teaching, but more flexibility was deemed necessary to enable optimal resource utilization and to enable the contextualization of public health training to better address local needs.15 The review recommended a revision of the length of public health training (which in Italy involves 5 years of postgraduate training), better integration with other postgraduate training programs, and the involvement of students in the reform of public health teaching.15,16 Notably, the Maldivian curriculum development process included input from prospective students. Using consensus methods offered a level playing field, ensuring that all participants could express their opinions, addressing some of the limitations of traditional group decision making, where more senior or domineering participants may exert undue influence over the process and can limit the contribution of other group members.8,17
To equip graduates with the knowledge and skills to become effective public health practitioners, the FHS sought to develop a course informed by local public health realities, as identified by local stakeholders. Given the anticipated wide range of views among the very diverse stakeholder group, the use of consensus-building methods facilitated agreement on curricular structure. Conducting an online Delphi process made possible the participation of a larger pool of experts, despite their large workloads and travel commitments.
The need for change in educational practices across the health professions has been the subject of much research over the last decade,18 spearheading the process of reform in health professional education, training, and professional development. A Delphi process was used by the Association of Schools of Public Health to develop public health core competencies for American Universities. Fourteen universities and over 400 individuals contributed or provided input into the process, with ten working groups using a Delphi process to select and develop different sets of competencies. These articulate in an overarching model, which reflects the full range of knowledge, skills, and other attributes required for current and future public health leaders.18
The Australian Public Health Education and Research Program used a Delphi process to define core competencies for Australian MPH graduates. They included health monitoring and surveillance, disease prevention and control, health protection, health promotion, and health policy and management. All core areas are unified through a shared domain of professional population health practice, emphasizing the role of research in MPH formation.19
The Maldivian MPH includes Research Methods as part of core subjects, while applied research is a prerequisite for both the Professional Practice and the Research-based streams. To strengthen students’ research skills, in 2014, the steering group worked with local public health agencies to identify public health research priorities for the Maldives. The consultation identified a list of projects that could boost local health research capacity, support MPH trainees’ research capacity, provide “early wins” in public health, and which can be completed during 1 year of academic study. MPH students commencing their 2nd year of study and their supervisors can use this list to match a research topic with students’ interests and skills, enabling them to round off their public health portfolio, while contributing toward answering research questions of national relevance.
Many local experts identified a need to improve leadership capacity among local public health professionals. To address this gap, the consensus building process recommended the inclusion of Public Health Management and Leadership as a core MPH subject. A review of the most influential reports shaping public health education over the last century found that capacity to train future public health leaders as agents of change was a common denominator.20,21 Recently the “Leaders for European Public Health” project developed a leadership competency framework, using a Delphi survey to reach consensus.22
Good public health education relies on collaborations to help solve complex problems,20 so teamwork is critical in the training of future public health professionals. The majority of the core subjects (four out of six) in the Maldivian MPH and half of its elective subjects require students to carry out some assignment as part of a team, enhancing their effectiveness both as team members and leaders.20
The small size of the population in the Maldives poses significant challenges to program sustainability and constrains the availability of the local faculty to offer a full complement of elective subjects. Therefore, the scoping exercise conducted by the FHS staff was critical to ascertain the size of the student intake and the future local demand for public health graduates. Of the eleven students enrolled in the first MPH intake, eight are on track to complete their degree at the end of 2015. They completed an anonymous evaluation at the completion of their 1st year of study, as part of a formative evaluation process. A comprehensive evaluation of the course will take place after the first cohort graduates, to shape the MPH program into the future and to ascertain future directions and explore the possible role of online education in course delivery for elective subjects with small class numbers.
Conclusion
We described the process of developing a tailored MPH curriculum for the Maldives, addressing local training needs and informed by the local public health realities. The process involved a wide consultation of stakeholders and consensus methods to define the curricular structure, allowing for an expeditious and inclusive course development process.
Acknowledgment
The MPH curriculum development process received support from the Australian government through the Australian Volunteers for International Development program and an Endeavour Executive Award.
Acknowledgments
The consensus building process was described at the International Society for Medical Decision Making (Singapore, January 5–8, 2014) in a poster presentation https://smdm.confex.com/smdm/apm2014/webprogram/Paper8113.html
The poster’s abstract was published in the Society’s journal, Medical Decision Making April 2014; vol. 34, 3: pp. E1–E38. http://mdm.sagepub.com/
An update on the MPH program will be presented in poster format at the Population Health Congress (Hobart, September 6–9, 2015).
The actual paper, however, has never been published.
Disclosure
The authors report no conflicts of interest in this work.
References
World Bank. Maldives: Clean Energy for Climate Mitigation Project. World Bank. 2014. Available from: http://www.worldbank.org/projects/P128268/maldives-clean-energy-climate-mitigation-project?lang=en. Accessed November 5, 2014. | |
Yoosuf A. Unsung Heroes: An Island Health Worker’s Journey. Male, Maldives: International Center for Environment Development and Operational Research (ENDEVOR); 2012. | |
Sulaiman AI, Abu Bakar SH, Wahab HA. Primary health care: hope and challenges for public health in Maldives. J Community Health. 2014;39(3):627–631. | |
Agyei-Mensah S, de-Graft Aikins A. Epidemiological transition and the double burden of disease in Accra, Ghana. J Urban Health. 2010;87(5):879–897. | |
Ahsan Karar Z, Alam N, Kim Streatfield P. Epidemiological transition in rural Bangladesh, 1986–2006. Glob Health Action. 2009;2. | |
Ganguly SS, Al-Lawati A, Al-Shafaee MA, Duttagupta KK. Epidemiological transition of some diseases in Oman: a situational analysis. World Hosp Health Serv. 2009;45(1):26–31. | |
World Health Organization. Maldives: Health Profile. Geneva: WHO; 2012. | |
Fink A, Kosecoff J, Chassin M, Brook RH. Consensus methods: characteristics and guidelines for use. Am J Public Health. 1984;74(9):979–983. | |
Cross H. Consensus methods: a bridge between clinical reasoning and clinical research? Int J Lepr Other Mycobact Dis. 2005;73(1):28–32. | |
Broomfield D, Humphris GM. Using the Delphi technique to identify the cancer education requirements of general practitioners. Med Educ. 2001;35(10):928–937. | |
Jones J, Hunter D. Consensus methods for medical and health services research. BMJ. 1995;311(7001):376–380. | |
Petersen DJ, Hovinga ME, Pass MA, Kohler C, Oestenstad RK, Katholi C. Assuring public health professionals are prepared for the future: the UAB public health integrated core curriculum. Public Health Rep. 2005;120(5):496–503. | |
Begg MD, Galea S, Bayer R, Walker JR, Fried LP. MPH education for the 21st century: design of Columbia University’s new public health curriculum. Am J Public Health. 2014;104(1):30–36. | |
O’Brien V, Djusipov K, Kudaibergonova T. Public health challenges in Kyrgyzstan: developing a new curriculum. Rural Remote Health. 2005;5(4):461. | |
Garavelli E, Marcantoni C, Costantino C, et al. Education and training among Italian postgraduate medical schools in public health: a comparative analysis. Ann Ig. 2014;26(5):426–434. | |
Costantino C, Cinquetti S, Garavelli E, et al. The key role of public health medical resident education for future public health challenges. Epidemiol Prev. 2014;38(6 Suppl 2):115–119. | |
Turoff M. The policy Delphi. In: Linstone HA, Turoff M, editors. The Delphi Method: Techniques and Applications. Boston: Addison-Wesley Publishing Co; 1975:84–101. | |
Calhoun JG, Ramiah K, Weist EM, Shortell SM. Development of a core competency model for the master of public health degree. Am J Public Health. 2008;98(9):1598–1607. | |
Genat B, Robinson P. New competencies for public health graduates: a useful tool for course design. Aust N Z J Public Health. 2010;34(5):513–516. | |
Fried LP, Begg MD, Bayer R, Galea S. MPH education for the 21st century: motivation, rationale, and key principles for the new Columbia public health curriculum. Am J Public Health. 2014;104(1):23–30. | |
Smith T, Stankunas M, Czabanowska K, de Jong N, O’Connor S, Fowler Davis S. Principles of all-inclusive public health: developing a public health leadership curriculum. Public Health. 2015;129(2):182–184. | |
Czabanowska K, Smith T, Konings KD, et al. In search for a public health leadership competency framework to support leadership curriculum – a consensus study. Eur J Public Health. 2014;24(5):850–856. |
Supplementary material
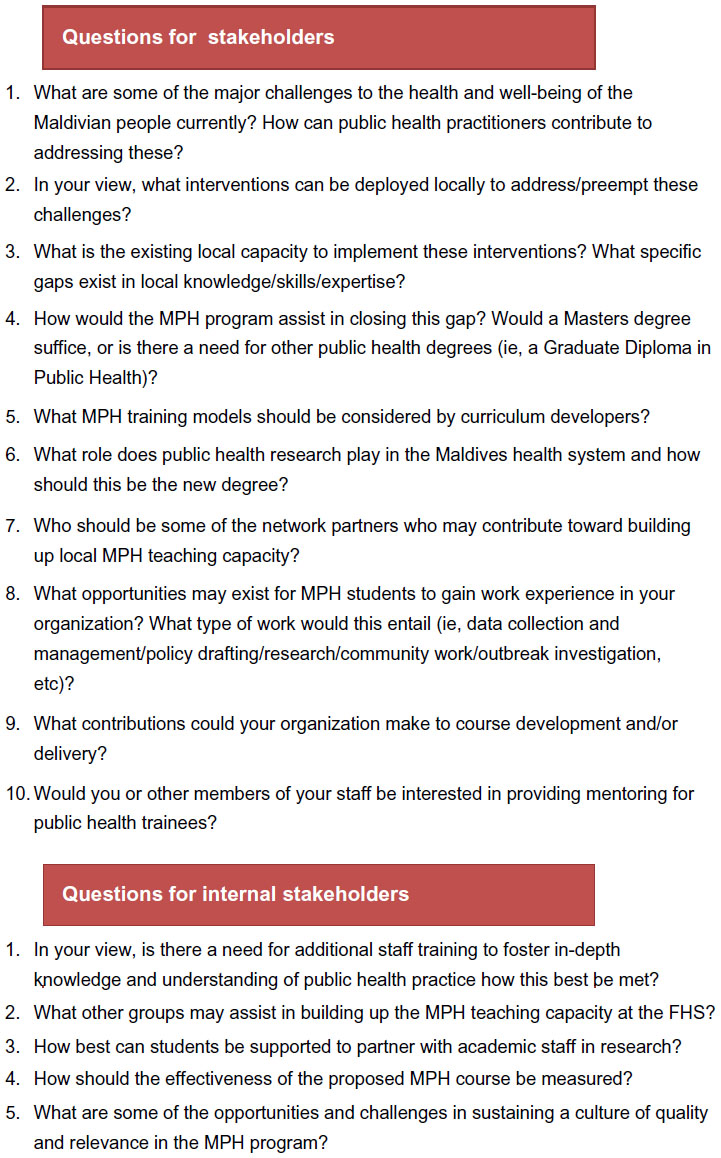 | Figure S1 Developing a MPH curriculum for the Maldives National University Semi structured interview guide. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.