")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Use of Vaping as a Smoking Cessation Aid: A Review of Clinical Trials
Authors Ashour AM
Received 4 May 2023
Accepted for publication 21 July 2023
Published 27 July 2023 Volume 2023:16 Pages 2137—2144
DOI https://doi.org/10.2147/JMDH.S419945
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ahmed M Ashour
Pharmacology and Toxicology Department, College of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia
Correspondence: Ahmed M Ashour, Pharmacology and Toxicology Department, Faculty of Pharmacy, Umm AlQura University, Makkah, 21442, Saudi Arabia, Tel +966566664464, Fax +966126066693, Email [email protected]
Purpose: Smoking is a global public health concern, with a significant negative impact on human health and healthcare spending. Vaping, or the use of electronic cigarettes (e-cigarettes), has emerged as a popular alternative to traditional nicotine replacement therapies (NRTs) for smoking cessation. While considered less harmful than combustible cigarettes, the long-term health effects of e-cigarettes (vaping) are unknown. Therefore, this study aimed to identify and provide a comprehensive overview of the performance of vaping in clinical trials.
Patients and Methods: A search was conducted in the ClinicalTrials.gov database on April 14th, 2023, using the search term “smoking cessation, e-cigarettes, NRTs, and vaping”. Inclusion and exclusion criteria were defined to identify relevant clinical trials. Randomized controlled trials (RCTs) and non-randomized clinical trials that evaluated vaping as a therapeutic approach to smoking cessation were included.
Results: A total of 87 clinical trials were identified, of which only seven were related to smoking cessation through vaping as a form of treatment. The primary endpoint was the effect of vaping as smoking cessation, and the secondary endpoints were patients’ abstinence rate, withdrawal symptoms, and adverse events of e-cigarettes. Most of the trials used e-cigarettes as an intervention, with some trials including a combination of e-cigarettes and other NRTs. The trials lasted from 4 weeks to 12 months. The overall results of the trials indicated that vaping was effective in helping smokers to quit. It was also associated with a lower risk of adverse events than combustible cigarettes.
Conclusion: Vaping appears to be an effective method for smoking cessation, and it is associated with a lower risk of adverse events than combustible cigarettes.
Keywords: vaping, e-cigarettes, nicotine, smoking cessation, smoking aid
Introduction
Smoking refers to the act of inhaling and exhaling the fumes of a burning plant, such as tobacco,1 which is the prepared form of tobacco leaves cultivated for smoking. Smoking is considered to be among the leading risk factors for a number of severe diseases worldwide.2,3 In addition, smoking is the second leading cause of early mortality across the globe, significantly contributing to the overall disease burden, particularly in the developing world.4 The negative impacts of smoking extend to a loss of productivity and extensive direct healthcare costs. In 2015, the global age-standardized prevalence of daily smoking was 25% in males and 5.4% in females.5 Central and Eastern Europe as well as Southeast Asia had the highest prevalence of smoking among males, whereas China, India, and Indonesia accounted for 51.4% of the total number of world smokers.6 On the other hand, 27.3% of all female smokers were residents of the United States, China, and India.7 The number of daily male smokers was highest in countries with a middle socioeconomic index, while those with a high socioeconomic index had the highest rates of female smokers.5
Traditional cigarettes produce around 4800 different chemical compounds upon combustion.8 Smoking has been reported to cause a significant reduction in overall health. Besides increased employee absenteeism and marked increases in the utilization of health services, detrimental health effects have increased significantly over the last 50 years.9 This observation was confirmed by the Million Women study conducted in the United Kingdom, where women who had reported being current smokers at the beginning of the survey had a mortality rate approximately three times that of non-smoking women (RR = 2.76; 95% CI, 2.71–2.81) after a 12-year follow-up period.10 In the same study, around two-thirds of the total mortalities among women aged 50–69 years were attributable to smoking. In a prospective study conducted in British male doctors over 40 years of age, all-cause mortality was more than three-fold greater in current smokers than in non-smokers aged 45–64 years, during the period between 1951 and 1971. This difference continued to increase significantly in the subsequent 20 years of study.11
In recent years, vaping (e-cigarettes) has received significant attention.12 E-cigarettes are battery-operated devices that heat liquid in order to produce an aerosol that is then inhaled.13 As the popularity of vaping grows, especially among adolescents and young adults, substantial concerns have been raised regarding its effects on public health.14 Vaping has grown in popularity as a result of the perception that e-cigarettes are less harmful than combustible cigarettes.15 The burning of tobacco in combustible cigarettes emits toxic chemicals that contribute to preventable diseases, such as lung cancer, heart disease, and respiratory disease.16 E-cigarettes, on the other hand, do not burn tobacco but instead heat a liquid that contains nicotine, flavors, and other additives.17 Compared to traditional cigarettes, e-cigarettes do not produce tobacco smoke nor contain tar, so they may come with a lower risk of adverse effects.17 Nevertheless, data on the long-term health effects of e-cigarettes are not yet available, so whether or not they pose a significant health risk when compared to combustible cigarettes remains undetermined.18
Governments strive to control tobacco use by implementing comprehensive control policies and specific strategies, such as the taxation of tobacco products,19 establishing smoke-free areas, banning smoking in public areas,20,21 as well as conducting smoking cessation interventions in the community and on a nation level.22,23 Medically assisted smoking cessation involves the use of a clinically approved approach to relieve nicotine withdrawal symptoms and reduce the cravings caused by nicotine addiction.24,25 Over the past few years, vaping has gained considerable attention as an approach for quitting smoking. Nicotine replacement therapies (NRTs), such as nicotine gum, patches, and lozenges, have long been used to assist smokers in quitting.26 However, e-cigarettes have emerged as an alternative to traditional NRTs.27 Vaping can be an effective approach for the treatment of nicotine addiction as its administration reverses withdrawal symptoms and takes away the urge to smoke during the first days of abstinence.
The vape is an Electronic Nicotine Delivery System (ENDS) manufactured to mimic the satisfactory senses of traditional smoking.28 Recent studies have shown that the use of e-cigarettes may increase smoking cessation rates. A US study with 161,054 respondents reported a higher smoking cessation rate in smokers who went on to use e-cigarette users than in those who did not (5.6% vs 4.5%).29 In addition, the WHO considers e-cigarettes to be less toxic than tobacco cigarettes, and the former may thus be proposed as a less harmful alternative.28 This study aims to compile clinical trials on vaping and summarize their findings, including the primary endpoints and treatment outcomes.
Materials and Methods
Search Strategy
The ClinicalTrials.gov database was searched on April 14th, 2023 for all relevant trials. Our aim was to identify all studies examining the use of vaping as a therapeutic approach for the cessation of smoking. Using the website’s search engine as a search tool, a search for clinical trials on “smoking cessation, e-cigarettes, NRTs, and vaping” was conducted.
Review of Search Results
In order to identify relevant clinical trials, inclusion and exclusion criteria defined in the research interest were used. Clinical trials that evaluated vaping as a treatment for smoking cessation were included. Studies were excluded if they were not completed or had no results, and they were included if they were completed clinical trials from Phase I to Phase IV that evaluated vaping as a treatment for smoking cessation. The title of the study, study status, type of study, type of intervention, and outcome data were extracted from the relevant trials, and this information is presented in Table 1.
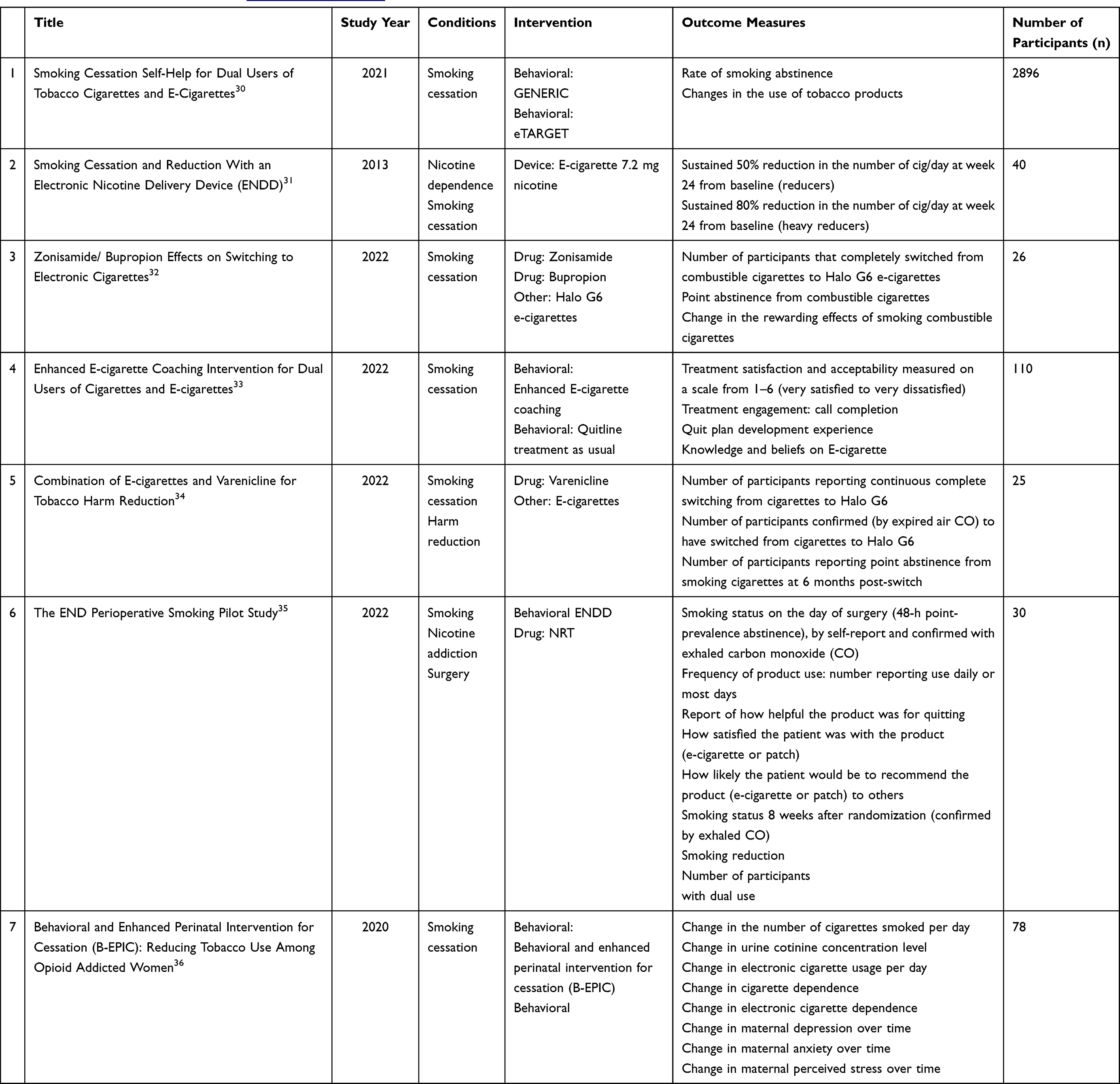 |
Table 1 List of the Clinical Trials from https://clinicaltrials.gov, Updated on 14-04-2023 |
Results
Number of Relevant Clinical Trials
As of April 14th, 2023, a total of 87 clinical trials registered on ClinicalTrials.gov were related to smoking cessation through vaping as a form of treatment. Out of these, only seven clinical trials focused on studying the effects of vaping. All seven studies have been completed, and detailed information—the study title, status, condition, intervention, outcome measures, and cohort size—is provided in Table 1. The primary endpoint was the effect of vaping as smoking cessation, and the secondary endpoints were patients’ abstinence rate, withdrawal symptoms, and adverse events of e-cigarettes. Most of the trials used e-cigarettes as an intervention, with some trials including a combination of e-cigarettes and other NRTs and/or behavioral intervention. The trials lasted from 4 weeks to 12 months. The overall results of the trials showed that vaping was effective in helping smokers to quit, reducing the number of cigarettes/day, and increasing the rate of smoking abstinence, with gradually reducing nicotine levels. In addition, the use of vaping was associated with a lower risk of adverse events than combustible cigarettes.
Discussion
Smoking is associated with high morbidity, and results of the National Health Interview Survey (NHIS) showed that active smokers had at least one or more smoking-related conditions than non-smokers.37 The prevalence of lung cancer (4.5−9.3%) and chronic obstructive pulmonary disease (COPD), defined as having chronic bronchitis or emphysema (2−4%), is high among both current and former smokers. In particular, cigarette smoking is a major etiology of lung adenocarcinoma. However, the risk associated with smoking is strongly dependent on the specific composition of tobacco smoke, which varies between cigarette types (filtered or not) and brands.38 Despite the lack of a confirmed causative cigarette design, it has been suggested that the use of ventilated filters and higher levels of nitrosamine content are major adenocarcinoma-causing factors [HHS2]. With regard to other cancer types, smoking has been significantly associated with hepatocellular carcinoma, colorectal cancer, and general adverse health outcomes in cancer-affected smokers. On the other hand, there may be a causal relationship between active smoking and tuberculosis as well as tuberculosis-associated mortality. There is a 20−30% increased risk of stroke in individuals exposed to second-hand smoke.39
Overall, exposure to tobacco via the inhalation of smoke and oral exposure to smokeless tobacco both have significant consequences for health.39 This is attributed to the harmful constituents of tobacco products.40 For example, the exhaled breath of smokers with COPD contains significantly higher concentrations of aluminium than that of healthy non-smokers.41 Cadmium is considered one of the major toxic components of tobacco, and it has a long biological half-life. Emphysema and interstitial fibrosis are unfavorable sequelae of exposure to nebulized cadmium materials.42,43 Arsenic, present in both oral and inhaled tobacco, results in defects in the relaxation of blood vessels and subsequent cardiovascular disorders.44 In addition, exposure to barium in tobacco via oral ingestion or inhalation may lead to hypertension, an increased heart rate, and benign granulomatous pneumoconiosis.39
There are several approaches to smoking cessation, including the gradual reduction of tobacco use, NRT, and prescription medications.45 Some people may also benefit from counseling or support groups to help them quit smoking.46 As a relatively novel method for smoking cessation, vaping may be particularly attractive to current smokers.47 E-cigarettes come in a variety of flavors, which may appeal to smokers who are seeking an alternative to traditional cigarettes in their attempt to quit.48 Studies have indicated that e-cigarettes may reduce cravings for combustible cigarettes, in addition to being more satisfying and less addictive.49 Furthermore, vaping provides smokers with a viable alternative to conventional smoking, as e-cigarette can be used in indoor spaces where smoking is not allowed.50 While several studies have suggested that vaping may not be as effective as established smoking cessation methods,51–53 others have suggested e-cigarettes as more effective than NRTs, such as nicotine gum or patches.54 Nevertheless, evidence of the long-term efficacy of e-cigarettes for smoking cessation is still limited.
Thus, the effectiveness of vaping as a smoking cessation aid remains a topic of ongoing scientific research.55 Some argue that e-cigarettes offer a less harmful and potentially satisfying alternative to conventional cigarettes, conducive to cessation.56 Nevertheless, researchers are concerned about the safety of e-cigarettes57 and their potential as a gateway to smoking.58 Further research into their potential impact on public health is therefore warranted.59,60 Meanwhile, healthcare professionals should consider the available evidence and exercise caution when prescribing or recommending e-cigarettes to patients as an aid for quitting smoking. The individual characteristics, preferences, and risks of each patient should be considered.
Limitations
There are limited long-term data on the safety and effectiveness of vaping as a smoking cessation aid. Most clinical trials conducted in this field have relatively short follow-up periods, typically ranging from a few weeks to a few months. As a result, the long-term effects of vaping on smoking cessation rates, relapse rates, and overall health outcomes may not be fully captured, which could limit our ability to draw definitive conclusions about the sustained effectiveness and safety of vaping as a smoking cessation aid. Additionally, the heterogeneity in design, methodology, and sample size of the clinical trials included in this review may introduce variability into the findings. There is considerable variation in the types of e-cigarettes and vaping products used, the dosages and duration of use, as well as the characteristics of the study populations, which may impact the outcomes observed. This heterogeneity may make it challenging for researchers to compare and synthesize the findings across studies. Furthermore, the rapidly changing landscape of e-cigarettes and vaping products represents another limitation. The regulatory environment, marketing strategies, and product formulations of e-cigarettes are continuously evolving, and these changes may impact the generalizability of findings over time.
Conclusion
The current review suggests that vaping appears to be an effective method for motivating smokers to quit, and it is associated with a lower risk of adverse events than combustible cigarettes. However, there is limited long-term data on the safety and effectiveness of vaping as a smoking cessation aid. Future trials based on longer study periods and the evaluation of other smoking cessation interventions are warranted.
Disclosure
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Chiba M, Masironi R. Toxic and trace elements in tobacco and tobacco smoke. Bull World Health Organ. 1992;70(2):269–275.
2. United States Department of Health Human Services. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. Atlanta, GA: United States Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2014.
3. Chang JT, Anic GM, Rostron BL, et al. Cigarette smoking reduction and health risks: a systematic review and meta-analysis. Nicotine Tob Res. 2021;23(4):635–642. doi:10.1093/ntr/ntaa156
4. Jha P. The hazards of smoking and the benefits of cessation: a critical summation of the epidemiological evidence in high-income countries. eLife. 2020;9:e49979. doi:10.7554/eLife.49979
5. Reitsma MB, Fullman N, Ng M; GBD 2015 Tobacco Collaborators. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990–2015: a systematic analysis from the Global Burden of Disease Study 2015. Lancet. 2017;389(10082):1885–1906. doi:10.1016/S0140-6736(17)30819-X
6. Husain MJ, Datta BK, Nargis N, et al. Revisiting the association between worldwide implementation of the MPOWER package and smoking prevalence, 2008–2017. Tob Control. 2021;30(6):630–637. doi:10.1136/tobaccocontrol-2020-055758
7. World Health Organization. WHO Global Report on Trends in Prevalence of Tobacco Use 2000–2025. World Health Organization; 2019.
8. Hoffmann D, Hoffmann I, El-Bayoumy K. The less harmful cigarette: a controversial issue. A tribute to Ernst L. Wynder. Chem Res Toxicol. 2001;14(7):767–790. doi:10.1021/tx000260u
9. Akiyama Y, Sherwood N. Systematic review of biomarker findings from clinical studies of electronic cigarettes and heated tobacco products. Toxicol Rep. 2021;8:282–294. doi:10.1016/j.toxrep.2021.01.014
10. Pirie K, Peto R, Reeves GK, et al. The 21st century hazards of smoking and benefits of stopping: a prospective study of one million women in the UK. Lancet. 2013;381(9861):133–141. doi:10.1016/S0140-6736(12)61720-6
11. Doll R, Peto R, Wheatley K, et al. Mortality in relation to smoking: 40 years’ observations on male British doctors. BMJ. 1994;309(6959):901–911. doi:10.1136/bmj.309.6959.901
12. Huerta TR, Walker DM, Mullen D, et al. Trends in e-cigarette awareness and perceived harmfulness in the US. Am J Prev Med. 2017;52(3):339–346. doi:10.1016/j.amepre.2016.10.017
13. Rigotti N, Kalkhoran S. Vaping and e-Cigarettes. Waltham (MA): UpToDate; 2021.
14. Levy DT, Warner KE, Cummings KM, et al. Examining the relationship of vaping to smoking initiation among US youth and young adults: a reality check. Tob Control. 2019;28(6):629–635. doi:10.1136/tobaccocontrol-2018-054446
15. Boakye E, Obisesan OH, Osei AD, et al. The promise and peril of vaping. Curr Cardiol Rep. 2020;22(12):155. doi:10.1007/s11886-020-01414-x
16. Fernández E, Ballbè M, Sureda X, et al. Particulate matter from electronic cigarettes and conventional cigarettes: a systematic review and observational study. Curr Environ Health Rep. 2015;2(4):423–429. doi:10.1007/s40572-015-0072-x
17. Farsalinos KE, Yannovits N, Sarri T, et al. Carbonyl emissions from a novel heated tobacco product (IQOS): comparison with an e-cigarette and a tobacco cigarette. Addiction. 2018;113(11):2099–2106. doi:10.1111/add.14365
18. Kaisar MA, Prasad S, Liles T, et al. A decade of e-cigarettes: limited research and unresolved safety concerns. Toxicology. 2016;365:67–75. doi:10.1016/j.tox.2016.07.020
19. Chaloupka FJ, Yurekli A, Fong GT. Tobacco taxes as a tobacco control strategy. Tob Control. 2012;21(2):172–180. doi:10.1136/tobaccocontrol-2011-050417
20. International Agency for Research on Cancer. Evaluating the Effectiveness of Smoke-Free Policies. IARC Press, International Agency for Research on Cancer; 2009.
21. Hopkins DP, Razi S, Leeks KD, et al. Smokefree policies to reduce tobacco use. A systematic review. Am J Prev Med. 2010;38(2):S275–S289. doi:10.1016/j.amepre.2009.10.029
22. Goldberg DN, Krantz AJ, Semal S, et al. Outcomes for a public hospital tobacco cessation program: the Cook County health and hospitals system experience. J Community Health. 2016;41(6):1130–1139. doi:10.1007/s10900-016-0215-5
23. Çelik İ, Yüce D, Hayran M, et al. Nationwide smoking cessation treatment support program—Turkey project. Health Policy (New York). 2015;119(1):50–56. doi:10.1016/j.healthpol.2014.11.017
24. Burton SL, Gitchell JG, Shiffman S; Centers for Disease Control and Prevention (CDC). Use of FDA-approved pharmacologic treatments for tobacco dependence—United States, 1984–1998. MMWR Morb Mortal Wkly Rep. 2000;49(29):665–668.
25. Prochaska JJ, Benowitz NL. The past, present, and future of nicotine addiction therapy. Annu Rev Med. 2016;67:467–486. doi:10.1146/annurev-med-111314-033712
26. Hajek P, Phillips-Waller A, Przulj D, et al. A Randomized trial of e-cigarettes versus nicotine-replacement therapy. N Engl J Med. 2019;380(7):629–637. doi:10.1056/NEJMoa1808779
27. Barbeau AM, Burda J, Siegel M. Perceived efficacy of e-cigarettes versus nicotine replacement therapy among successful e-cigarette users: a qualitative approach. Addict Sci Clin Pract. 2013;8(1):5. doi:10.1186/1940-0640-8-5
28. World Health Organization. Electronic Nicotine Delivery Systems and Electronic Non-nicotine Delivery Systems (ENDS/ENNDS); 2016. Available from: www.who.int/fctc/cop/cop7/FCTC_COP_7_11_EN.pdf.
29. Zhu SH, Zhuang YL, Wong S, et al. E-cigarette use and associated changes in population smoking cessation: evidence from US current population surveys. BMJ. 2017;358:j3262. doi:10.1136/bmj.j3262
30. Meltzer LR, Simmons VN, Piñeiro B, et al. Development of a self-help smoking cessation intervention for dual users of tobacco cigarettes and e-cigarettes. Int J Environ Res Public Health. 2021;18(5):2328. doi:10.3390/ijerph18052328
31. Polosa P. Smoking cessation and reduction with an electronic nicotine delivery device (ENDD). NLM identifier: NCT01195597. Available from: https://classic.clinicaltrials.gov/ct2/show/NCT01195597.
32. Foundation for a Smoke Free World INC. Zonisamide/bupropion effects on switching to electronic cigarettes (BuZonE). NLM identifier: NCT04388319. Available from: https://classic.clinicaltrials.gov/ct2/show/NCT04388319.
33. Vickerman K. Enhanced E-cigarette coaching intervention for dual users of cigarettes and e-cigarettes. NLM identifier: NCT03575468. Available from: https://classic.clinicaltrials.gov/ct2/show/NCT03575468.
34. Foundation for a Smoke Free World INC. Combination of e-cigarettes and varenicline for tobacco harm reduction (EVAR). NLM identifier: NCT04210180. Available from: https://classic.clinicaltrials.gov/ct2/show/NCT04210180.
35. Lee SM. The END perioperative smoking pilot study. NLM identifier: NCT02482233. Available from: https://classic.clinicaltrials.gov/ct2/show/NCT02482233.
36. Fallin-Bennett A, Lofwall M, Waters T, et al. Behavioral and enhanced perinatal intervention (B-EPIC): a randomized trial targeting tobacco use among opioid dependent pregnant women. Contemp Clin Trials Commun. 2020;20:100657. doi:10.1016/j.conctc.2020.100657
37. Rostron BL, Chang CM, Pechacek TF. Estimation of cigarette smoking-attributable morbidity in the United States. JAMA Intern Med. 2014;174(12):1922–1928. doi:10.1001/jamainternmed.2014.5219
38. Burns DM, Dybing E, Gray N, et al. Mandated lowering of toxicants in cigarette smoke: a description of the World Health Organization TobReg proposal. Tob Control. 2008;17(2):132–141. doi:10.1136/tc.2007.024158
39. Pappas RS. Toxic elements in tobacco and in cigarette smoke: inflammation and sensitization. Metallomics. 2011;3(11):1181–1198. doi:10.1039/c1mt00066g
40. Food and Drug Administration. Harmful and potentially harmful constituents in tobacco products and tobacco smoke: established list; 2012. Available from: https://www.fda.gov/TobaccoProducts/GuidanceComplianceRegulatoryInformation/ucm297786.htm.
41. Mutti A, Corradi M, Goldoni M, et al. Exhaled metallic elements and serum pneumoproteins in asymptomatic smokers and patients with COPD or asthma. Chest. 2006;129(5):1288–1297. doi:10.1378/chest.129.5.1288
42. Snider GL, Hayes JA, Korthy AL, et al. Centrilobular emphysema experimentally induced by cadmium chloride aerosol. Am Rev Respir Dis. 1973;108(1):40–48. doi:10.1164/arrd.1973.108.1.40
43. Snider GL, Lucey EC, Faris B, et al. Cadmium-chloride-induced air-space enlargement with interstitial pulmonary fibrosis is not associated with destruction of lung elastin. Implications for the pathogenesis of human emphysema. Am Rev Respir Dis. 1988;137(4):918–923. doi:10.1164/ajrccm/137.4.918
44. Lee MY, Jung BI, Chung SM, et al. Arsenic-induced dysfunction in relaxation of blood vessels. Environ Health Perspect. 2003;111(4):513–517. doi:10.1289/ehp.5916
45. Caponnetto P, Russo C, Polosa R. Smoking cessation: present status and future perspectives. Curr Opin Pharmacol. 2012;12(3):229–237. doi:10.1016/j.coph.2012.02.005
46. García-Gómez L, Hernández-Pérez A, Noé-Díaz V, et al. Smoking cessation treatments: current psychological and pharmacological options. Rev Invest Clin. 2019;71(1):7–16. doi:10.24875/RIC.18002629
47. Sanchez S, Kaufman P, Pelletier H, et al. Is vaping cessation like smoking cessation? A qualitative study exploring the responses of youth and young adults who vape e-cigarettes. Addict Behav. 2021;113:106687. doi:10.1016/j.addbeh.2020.106687
48. Ford A, MacKintosh AM, Bauld L, et al. Adolescents’ responses to the promotion and flavouring of e-cigarettes. Int J Public Health. 2016;61(2):215–224. doi:10.1007/s00038-015-0769-5
49. Perry RN, Girgulis JP, Harrison SL, et al. Dual users’ perceptions of the addictive properties of cigarettes versus E-cigarettes. Addict Behav. 2023;136:107483. doi:10.1016/j.addbeh.2022.107483
50. Kuschner WG, Reddy S, Mehrotra N, et al. Electronic cigarettes and thirdhand tobacco smoke: two emerging health care challenges for the primary care provider. Int J Gen Med. 2011;4:115–120. doi:10.2147/IJGM.S16908
51. Brown J, Beard E, Kotz D, et al. Real‐world effectiveness of e‐cigarettes when used to aid smoking cessation: a cross‐sectional population study. Addiction. 2014;109(9):1531–1540. doi:10.1111/add.12623
52. Chen R, Pierce JP, Leas EC, et al. Effectiveness of e-cigarettes as aids for smoking cessation: evidence from the PATH Study cohort, 2017–2019. Tob Control. 2022. doi:10.1136/tobaccocontrol-2021-056901
53. McDermott MS, East KA, Brose LS, et al. The effectiveness of using e‐cigarettes for quitting smoking compared to other cessation methods among adults in the United Kingdom. Addiction. 2021;116(10):2825–2836. doi:10.1111/add.15474
54. Hajek P, Phillips-Waller A, Przulj D, et al. E-cigarettes compared with nicotine replacement therapy within the UK Stop Smoking Services: the TEC RCT. Health Technol Assess. 2019;23(43):1–82. doi:10.3310/hta23430
55. Kasza KA, Hammond D, Gravely S, et al. Associations between nicotine vaping uptake and cigarette smoking cessation vary by smokers’ plans to quit: longitudinal findings from the International Tobacco Control Four Country Smoking and Vaping Surveys. Addiction. 2023;118(2):340–352. doi:10.1111/add.16050
56. Saffer H, Dench D, Grossman M, et al. E-cigarettes and adult smoking: evidence from Minnesota. J Risk Uncertain. 2020;60(3):207–228. doi:10.1007/s11166-020-09326-5
57. Esteban-Lopez M, Perry MD, Garbinski LD, et al. Health effects and known pathology associated with the use of E-cigarettes. Toxicol Rep. 2022;9:1357–1368. doi:10.1016/j.toxrep.2022.06.006
58. Chapman S, Bareham D, Maziak W. The gateway effect of E-cigarettes: reflections on main criticisms. Nicotine Tob Res. 2019;21(5):695–698. doi:10.1093/ntr/nty067
59. O’Farrell HE, Brown R, Brown Z, et al. E-cigarettes induce toxicity comparable to tobacco cigarettes in airway epithelium from patients with COPD. Toxicol in vitro. 2021;75:105204. doi:10.1016/j.tiv.2021.105204
60. Gee RE, Boles WR, Smith DG. E-cigarettes: a public health threat, not a population health intervention. Am J Public Health. 2021;111(2):224–226. doi:10.2105/AJPH.2020.306072
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.