")
Back to Journals » Nature and Science of Sleep » Volume 15
Use of Insomnia Treatments and Discussions About Sleep with Health Professionals Among Australian Adults with Mental Health Conditions
Authors Russell DI , Reynolds AC, Appleton SL , Adams RJ , Correia H , Bowman JA, Gill TK , Metse AP
Received 24 March 2023
Accepted for publication 20 July 2023
Published 7 August 2023 Volume 2023:15 Pages 623—637
DOI https://doi.org/10.2147/NSS.S412468
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Daniel I Russell,1 Amy C Reynolds,2 Sarah L Appleton,2,3 Robert J Adams,2,3 Helen Correia,4 Jenny A Bowman,5,6 Tiffany K Gill,7 Alexandra P Metse5,6,8
1College of Science, Health, Engineering and Education (SHEE), Murdoch University, Murdoch, Western Australia, 6150, Australia; 2Flinders Health and Medical Research Institute (Sleep Health), College of Medicine and Public Health, Flinders University, Adelaide, South Australia, Australia; 3The Freemasons Centre for Male Health & Wellbeing, The University of Adelaide, Adelaide, South Australia, 5005, Australia; 4Psychological Sciences, Australian College of Applied Professions Perth, Northbridge, Western Australia, 6003, Australia; 5School of Psychological Sciences, University of Newcastle, Callaghan, New South Wales, 2308, Australia; 6Hunter Medical Research Institute (HMRI), New Lambton Heights, NSW, 2305, Australia; 7Adelaide Medical School, The University of Adelaide, Adelaide, South Australia, 5005, Australia; 8School of Health, University of the Sunshine Coast, Sippy Downs, Queensland, 4556, Australia
Correspondence: Daniel I Russell, Murdoch University, 90 South Street, Murdoch, Western Australia, 6150, Australia, Email [email protected]
Background: Insomnia is a common issue among individuals with mental health conditions, yet the frequency of insomnia treatment remains unclear. The purpose of this study was to investigate the prevalence of probable insomnia, discussions regarding sleep with health professionals, and the utilisation of commonly delivered insomnia treatments in Australian adults diagnosed with mental health conditions.
Methods: This study represents a secondary analysis of data collected through a cross-sectional, national online survey conducted in 2019. A subset included participants (n = 624, age 18– 85y) who self-reported a diagnosis of depression, bipolar disorder, anxiety, panic disorder, or post-traumatic stress disorder. Participants were classed as having probable insomnia based on self-reported symptoms and a minimum availability of 7.5 hours in bed.
Results: Among individuals with probable insomnia (n = 296, 47.4%), 64.5% (n = 191) reported discussing sleep with one or more health professionals, predominantly with general practitioners (n = 160, 83.8%). However, 35.4% (n = 105) of people with probable insomnia had not discussed their sleep with a health professional. Additionally, 35.1% (n = 104) used prescribed medication for sleep, while only 15.9% (n = 47) had used the first line recommended treatment of cognitive-behavioral therapy for insomnia in the last 12 months.
Conclusion: Although most participants who met the criteria for probable insomnia had engaged in discussions about sleep with health professionals, utilisation of first line recommended treatment was low. Interventions that promote routine assessment of sleep and first line treatment for insomnia by health professionals would likely benefit people with mental health conditions.
Keywords: sleep, insomnia, help seeking, assessment, treatment, care, mental health
Plain Language Summary
Insomnia is a prevalent issue among individuals with mental health conditions. However, the extent to which individuals with mental health conditions and insomnia engage in discussions about sleep with health professionals remains unclear. This study was a secondary analysis of a national survey conducted in Australia in 2019, revealing that nearly half (47.4%) of participants with mental health conditions met the criteria for probable insomnia.
Among those with probable insomnia, approximately 64.5% reported having discussions about sleep with a health professional. However, only 16% of individuals with probable insomnia used the recommended first line treatment of cognitive-behavioral therapy for insomnia techniques. Barriers such as cost and lack of a referral by a general practitioner were commonly cited as reasons for not accessing psychological interventions.
Additionally, the type of treatment used was associated with daytime symptoms of insomnia. This finding suggests the importance of investigating health professionals’ perceptions of daytime insomnia symptoms, as these perceptions may influence treatment decisions. Overall, this study highlights that probable insomnia is highly prevalent among individuals with mental health conditions. While discussing sleep with health professionals appears relatively common within this population, generally discussions do not translate to first line treatment. Further research and interventions focusing on improving sleep assessment and access to appropriate treatments are warranted.
Introduction
Insomnia is prevalent worldwide with estimates of 6–25% among adults,1 including in high-income countries, such as Australia,2 the United States,3 and Canada.4 The prevalence of insomnia is notably higher among people with mental health conditions.5 Within this population, approximately 50% are reported to experience symptoms associated with insomnia.6 In a 2018 study by Seow et al,7 45% of adults with depression and 33% of adults with anxiety met the criteria for insomnia disorder according to the DSM-V classification.
The extent to which sleep is discussed with health professionals has been reported for certain populations, such as children.8 However, despite the high prevalence of insomnia in adults with mental health conditions,6,7 there has been limited research on the frequency of discussions about sleep with health professionals for this group. Existing studies indicate a low proportion of individuals engaging in such discussions.9–11 For example, a study conducted in the US reported that approximately one third of adults self-reported ever discussing sleep with a health professional. This study also explored factors associated with discussing sleep and found those with symptoms of insomnia, depression, anxiety, and who had used sleep medication were more likely to have had a conversation with a health professional.9 Furthermore, a cross-sectional study conducted in Australia among adults who self-reported a diagnosis or treatment for a mental health condition within the last 12 months reported that only 38% were asked about the duration or quality of their sleep by a health professional during that period.10 A study conducted in the UK, which involved the assessment of clinical notes among community mental health service users, reported that while 71% of new users were asked about their sleep, sleep discussions occurred in only 30% of all contacts.11 However, these studies do not provide information on the proportion of individuals with insomnia symptoms within this population who engaged in discussions about sleep or received treatment from health professionals. Furthermore, there is limited knowledge regarding other factors associated with sleep discussions, the specific health professionals involved in these discussions, or the frequency at which such discussions take place for individuals with mental health conditions.
Community-based studies indicate that among individuals with mental health conditions, the use of medication for insomnia is more prevalent compared to the recommended first line treatment of cognitive-behavioral therapy for insomnia (CBTi).10–12 In a study conducted in the UK among outpatients with a nonaffective psychotic disorder who reported discussing sleep with a health professional, approximately 56% received some form of treatment. Within this subset, 61% received prescribed sleep medication, while 27% received CBTi.12 Another survey involving clients of community mental health services in the UK reported that 61% of participants experiencing insomnia symptoms had not been offered any form of treatment. Among those who did receive treatment, 31.5% received prescribed sleep medication, while only 5.5% received CBTi.11 Additionally, a recent telephone survey conducted in Australia among community-dwelling adults with self-reported mental health conditions assessed the rates of treatment received for symptoms associated with insomnia. The study reported that 30% of participants received some form of treatment, with prescribed sleep medication being the most common treatment option (57%), while CBTi was received by a smaller proportion (9%).10 These studies collectively suggest that the utilisation of first line treatment for insomnia is low among individuals living with mental health conditions. However, there is limited knowledge about how different sleep treatments are accessed and what barriers hinder access to first line treatments.
The objective of the current study was to examine the prevalence of discussions about sleep and receipt of treatment for insomnia among Australian adults with a mental health condition. Specifically, we aimed to explore:
- Discussions with a health professional about sleep, specifically in terms of the proportion who had discussed sleep with a health professional on one or more occasions in the past 12 months, as well as the number of discussions, and
- Self-reported use of sleep treatments according to the proportion of individuals who used prescribed sleep medication and/or cognitive behaviour therapy for insomnia in the past 12 months.
Method
Design
This is a secondary analysis of the Australian 2019 Sleep Health Foundation insomnia survey, as previously described.1,13 The survey comprised self-reported items assessing sleep quality, sleep disorders, and health service use, along with clinical and demographic information. This secondary analysis only included participants with a mental health condition (henceforth referred to as “ever-diagnosed mental health condition”). Participants self-reported receiving at least one diagnosis of depression/bipolar disorder, anxiety/panic disorder, or post-traumatic stress disorder from a doctor. This study was approved by the ethics committee at the University of Adelaide (H-2018-214), with reciprocal approval at Murdoch University (2020/099).
Sample and Recruitment Procedure
Recruitment and data collection were conducted between March and April 2019, by Dynata (previously Research Now Survey Sampling International – SSI), the largest first-party data company internationally, including a panel of over 500,000 Australian survey takers. Potential participants were initially screened for broad inclusion criteria: at least 18 years of age, an Australian citizen or permanent resident, and able to access the online survey. The final sample (n = 2044) was selected via a three-stage process to minimize the risk of sample bias: (1) randomly selected participants completed a demographic profiling survey, (2) demographic information was then used to identify appropriate participants for the sleep survey; and (3) selected participants were invited via the Dynata participant interface to complete the web-based sleep survey. Participants were blind to the content of the survey prior to participation to reduce risk of bias associated with self-selection. All participants confirmed consent to continue to the survey. Sample recruitment methods have previously been reported in detail using the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) (see Supplementary Material). Six hundred and twenty-four adults (30.5%) from the complete sample reported at least one ever-diagnosed mental health condition and adequate information to determine probable insomnia status.
Measures
Participant Demographic and Clinical Information
Participant demographic information included: age (years), gender (male, female, other), postcode, education (still at school, left school at 16 years or less, left school after age of 16, left school after age of 16 but still studying, trade/apprenticeship, certificate/diploma, bachelor degree or higher, refused), marital status (married, living with a partner, separated, divorced, widowed, never married, refused), and country of birth.
For regression analyses, the following variables were reduced into fewer levels as follows: Age (18–34, 35–49, 50–85); postcode data was used to determine region (metro, regional/rural) and coded to the Australian Bureau of Statistics standard Socio-Economic Index for Areas Index of Relative Socio-Economic Disadvantage14 and grouped into advantaged (highest 40%), mid-level (middle 20%), and disadvantaged (lowest 40%) of socio-economic status postcodes;15 education (higher education (post-secondary school), high school or less); country of birth (Australia, rest of the world); and marital status (with partner, without partner).
Probable Insomnia
Probable insomnia was determined using criteria specified in the DSM-5 and ICSD-3.16,17 Items relating to difficulties initiating and maintaining sleep (DIMS) asked participants to report how frequently (rarely or never, a few nights a month, a few nights a week, every or almost every night) in the past month they (1) experienced difficulty falling asleep; (2) waking a lot during the night; and (3) waking up too early and not able to get back to sleep. Daytime symptoms included participant reported frequency (rarely or never, a few nights a month, a few nights a week, every or almost every night) in the past month of experiencing (1) felt fatigue or exhaustion; (2) sleepiness that interfered with daily activities; and (3) felt sleepy when sitting quietly during the day or early evening.
For analyses, probable insomnia was determined (yes/no) in participants who reported at least one DIMS symptom together with at least one daytime symptom at a frequency of “a few nights/times a week” or “every or almost every night/day” over the last month, with at least a nightly average (across weekdays and weekends) availability of 7.5 hours in bed.1 This is consistent with ICSD-3 defined insomnia. Participants meeting probable insomnia status would meet ICSD-3 diagnostic criteria for short-term insomnia. In the original sample, most participants (n = 1031, 50.4%) who reported high-frequency symptoms (“a few nights/times a week” or “every or almost every night/day”) also reported that symptoms were chronic (experienced for ≥3 months).2 Therefore, findings can be generalised to chronic and short-term insomnia populations. Participants with insufficient information to calculate average time in bed (TIB), or who provided improbable values (ie <3h habitual TIB), were excluded from analyses.
Current Mental Health Difficulties
Current mental health difficulties were assessed using an item from the EuroQol (European quality of life) five dimension scale (EQ-5D-5L),18 a standardised measure of health status. Current mental health difficulties were determined (yes/no) according to participants being asked “Please tick the one response that best describes your health today”. Under anxiety/depression, response options included: I am not anxious or depressed, I am slightly anxious or depressed, I am moderately anxious or depressed, I am severely anxious or depressed, I am extremely anxious or depressed, and Do not know. Participants were deemed to be experiencing current mental health difficulties if they reported feeling moderately, severely, or extremely anxious or depressed.
Discussions with a Health Professional About Sleep
All participants were asked: “During the last 12 months have you discussed your sleep with any of the following health professionals?” Response options included: general practitioner, physiotherapist, chiropractor, specialist in private practice, hospital physician, other physician, psychologist, psychiatrist, other, or none of these (multiple responses were permitted). The number of different health professionals with which the participants discussed sleep were grouped as none, one, or more than one. Participants reporting at least one discussion were asked additional questions, which included: “How many times in total would you say you have discussed your sleep with a doctor or medical professional in the past year?” Response options included: Never, once, 2 times, 3 times, 4 times, 5 times, and over 5 times, and were categorised as none, one or two, and three or more.
Participants were also asked “What prompted you to discuss your sleep with a health professional?” Response options included: I felt unwell physically; I felt unwell emotionally; I was aware of feeling sleepy/unfocussed; I was worried about my ability to do my job; I was worried about my ability to do other non-work tasks; in comparison to other people’s sleep patterns, I was worried about my sleep although I was not tired during the day; I did not feel safe driving; a family member suggested I needed to speak to a professional; a friend suggested I needed to speak to a professional; I went to my health professional with another concern/issue but sleep was discussed; the health professional raised the issue of my sleep; and other.
Sleep Treatment
All participants were asked “Over the last 12 months, how frequently have you used the following specifically to help you sleep?” Response order was randomised in the survey and multiple responses were permitted. The current analysis focused on the use of clinician-delivered evidence-based treatments only, with relevant response options including: sleep medication prescribed by a doctor (eg, temazepam or Valium), melatonin prescribed by a doctor, and cognitive behaviour therapy techniques for insomnia from a health professional. Responses on the frequency of treatment included: Every night or almost every night, a few nights a week, a few nights a month, rarely, never, refused, or do not know.
Participants who reported use of “cognitive-behaviour therapy techniques from a health professional” or “sleep medication prescribed by a doctor” and/or “melatonin prescribed by a doctor” at least a few nights a month, were coded as having used the specific treatment. Participants who reported “never/rarely/refused/don’t know” for CBTi or sleep medication were coded as having not used the specified treatment.
Reasons for Not Accessing Consultation and/or Treatment from a Psychologist or Psychiatrist
Participants who did not report discussing sleep with either a psychologist or psychiatrist in the last 12 months were asked “Why didn’t you receive treatment from a psychologist or psychiatrist for your sleep problem?” Response options included no private health insurance; cost concerns/too expensive; general practitioner not referred/raised me as a possibility; concern about needing a mental health treatment plan to access psychologist; my sleep problem did not bother me enough; and other reason (specify).
Analyses
Analyses were conducted using jamovi Version 1.6. (The jamovi project) and Microsoft Excel (2018). Descriptive statistics (percentages, means, and standard deviations) were used to summarise sociodemographic information, insomnia status, insomnia associated symptoms, current mental health difficulties, discussions with health professionals, and sleep treatment usage. Differences in distribution were determined using chi squared analyses according to probable insomnia status and current mental health difficulties as appropriate. Adjusted models were determined using binomial logistic regressions and ordinal logistic regressions as appropriate, and covariates were included in models if their univariate association with the dependent variable was p ≥ 0.25. The assumption of proportional odds for the ordinal logistic regression analyses were tested via parallel lines tests and conducted using IBM Statistical Package for the Social Sciences (SPSS®) version 25.0 (IBM Corp., Armonk, NY, USA). Sensitivity analyses were conducted to control for daytime symptoms by considering insomnia as only DIMS with average TIB ≥7.5 hours (see Supplementary Content for Detail).
Results
Participant Characteristics
Table 1 summarises participant demographic information overall. A further breakdown according to the type of ever-diagnosed mental health condition is provided in Supplementary Table S1. Included participants were mostly female (62.2%), living in a metropolitan area (65.4%), and born in Australia (85.4%). The mean age of the sample was 43.6 years (standard deviation [SD] = 15.9). Regarding socioeconomic status, the sample contained similar proportions of disadvantaged (39.7%) and advantaged (38.6%) participants. Current mental health difficulties were reported by 55.3% of participants, with 85.3% of participants reported feeling at least slightly anxious or depressed.
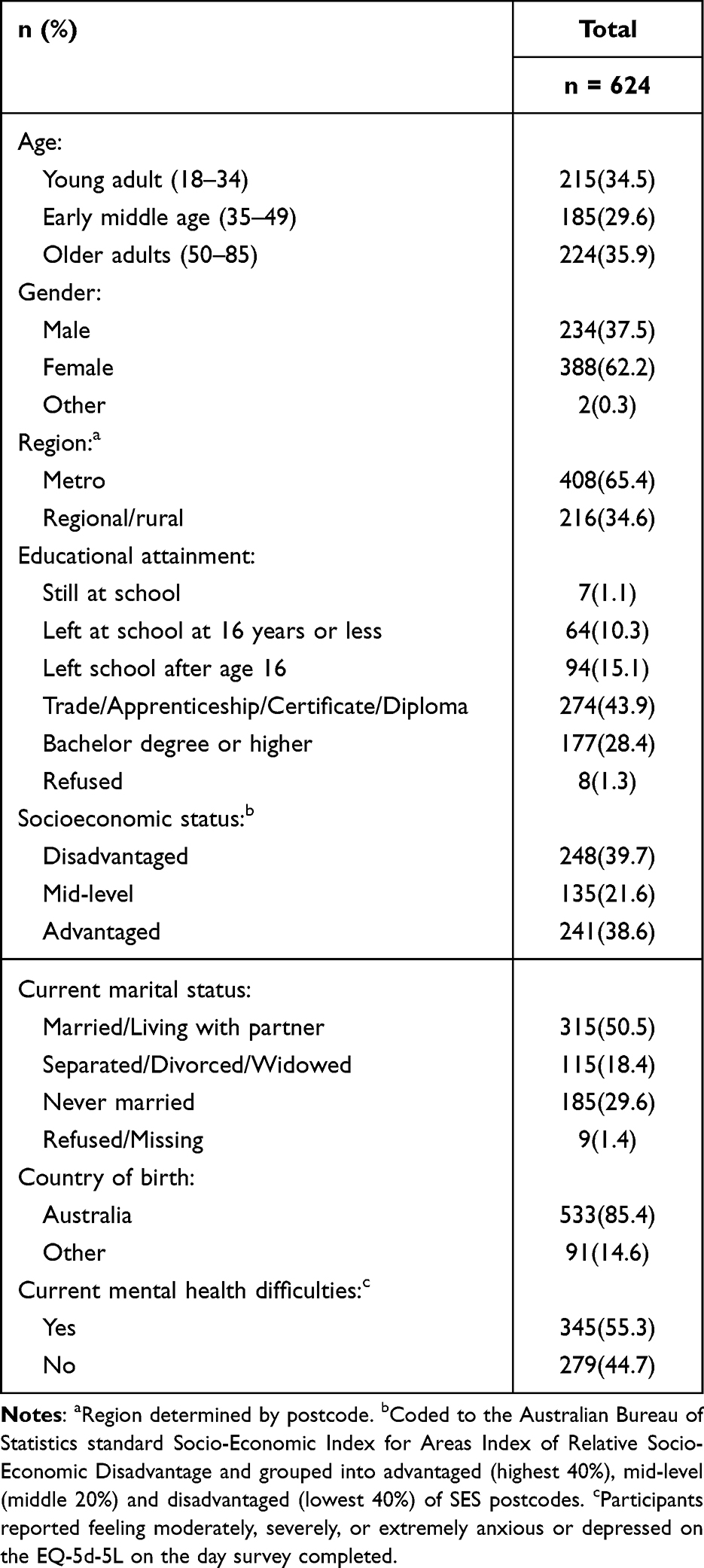 |
Table 1 Demographic and Clinical Information of Participants with an Ever-Diagnosed Mental Health Condition |
Prevalence of Probable Insomnia in the Sample
Almost half (47.4%) of participants in the sample met criteria for probable insomnia (Table 2), with 60.7% reported feeling sleepy during the day or early evening, 60.1% felt fatigued or exhausted, 52.4% reported difficulty falling asleep, and 60.3% reported waking during the night. Probable insomnia was more common in those with current mental health difficulties (53.9%) than those without (39.4%).
 |
Table 2 Difficulties Initiating or Maintaining Sleep, Daytime Difficulties, and Probable Insomnia Over the Past Month by Current Mental Health Difficulties |
Discussions with a Health Professional About Sleep
The prevalence of discussions with a health professional about sleep are summarised in Table 3. Over half of the sample reported discussing sleep at least once in the last 12 months (n = 327, 52.4%), with 28% (n = 174) speaking once to a health professional, and 25% (n = 153) more than once. Sleep discussions were mostly reported with general practitioners (n = 271, 82.9%) and psychologists (n = 89, 27.2%) (Table 3). Feeling unwell emotionally (n = 173, 52.9%) and having awareness of feeling sleepy/unfocussed (n = 140, 42.8%) were the main reasons for discussing sleep.
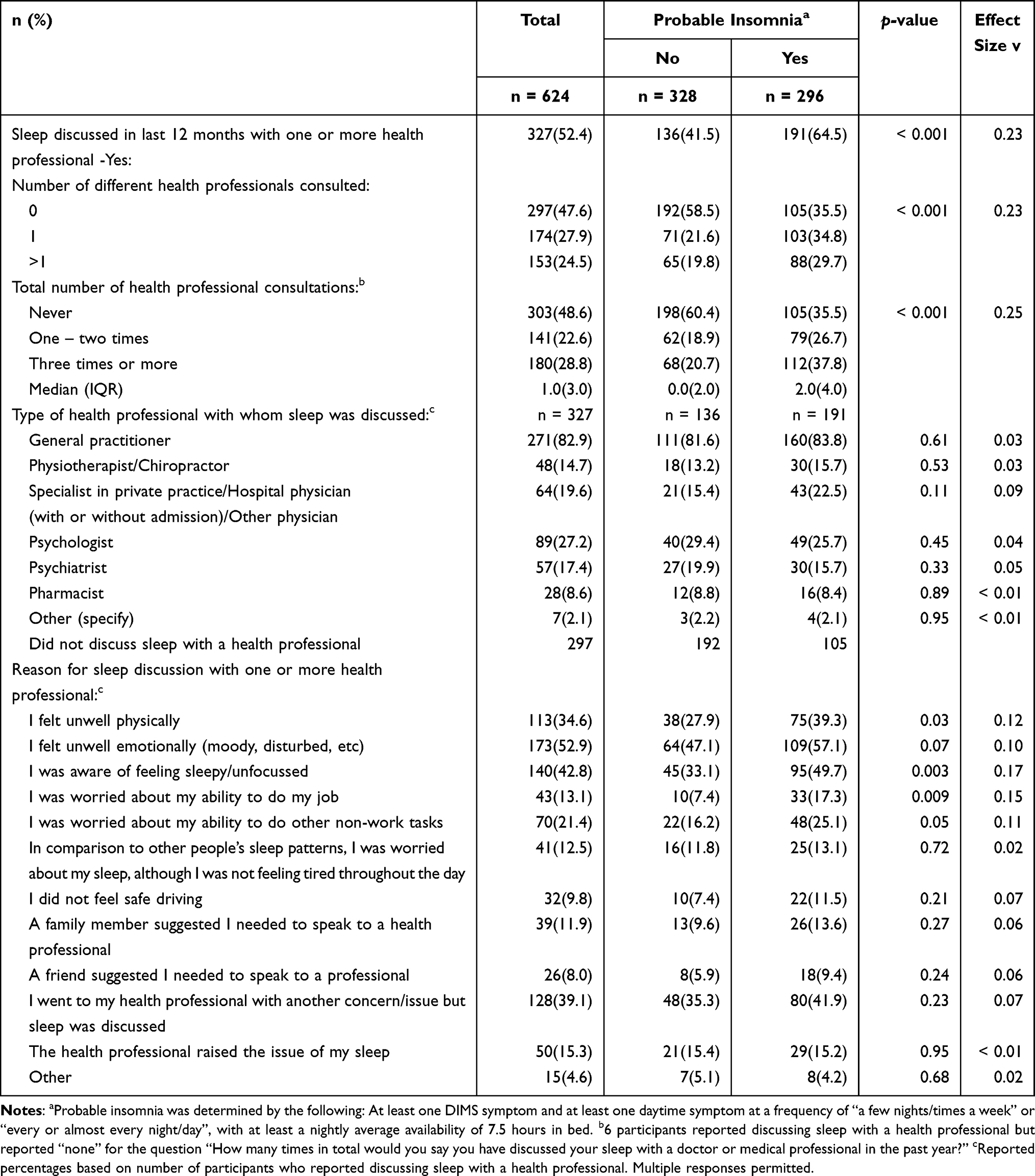 |
Table 3 Discussions About Sleep with Health Professionals in the Prior 12 Months, Overall and by Probable Insomnia Status |
Participants with probable insomnia were significantly more likely to have discussed sleep with at least one health professional (64.5% v 41.5%), had discussed sleep with a number of different health professionals (29.7% v 19.8% for more than one type of health professional) and reported more discussions (37.8% v 20.7% for three or more discussions) compared to those without probable insomnia. The type of health professional consulted was consistent between those with and without probable insomnia (Supplementary Table S2). These findings remained when probable insomnia was classified as only DIMS with average TIB ≥7.5 hours (Supplementary Table S3).
Factors associated with discussions about sleep with health professionals are summarised in Table 4. To better understand predictors of those who a) discussed sleep with a health practitioner, and b) had more discussions about sleep with health practitioners, multivariable models were conducted to explore sociodemographic predictors of discussions about sleep.
 |
Table 4 Univariate Associations Between Clinical and Sociodemographic Factors with Discussing Sleep with a Health Professional, and Total Number of Sleep Discussions in the Last 12 Months |
Any Discussion About Sleep with Health Professionals in the Past 12 Months
Participants who met criteria for probable insomnia (compared to those who did not; p < 0.001) and those who were 50–85 years old (compared to 18–34 years; p = 0.047) were more likely to have had a discussion about sleep with a health professional in the past 12 months (Table 5). In sensitivity analyses (Supplementary Table S4), a higher likelihood of discussing sleep with at least one health professional still occurred when probable insomnia was classified as only DIMS with average TIB ≥7.5 hours (compared to those without specified symptoms; p < 0.001), and among those with current mental health difficulties (compared to those without; p = 0.02).
 |
Table 5 Characteristics Associated with Discussing Sleep with a Health Professional Determined by Binary Logistic Regression, and Total Number of Discussions About Sleep in the Last 12 Months Determined by Ordinal Logistic Regression |
Number of Discussions About Sleep with Health Professionals in the Past 12 Months
A higher number of sleep discussions were associated with probable insomnia (p < 0.001), current mental health difficulties (p = 0.02), and older age (50–85 years v 18–34 years; p = 0.02) in the multivariable model (Table 5). In sensitivity analyses, where insomnia was indicated if DIMS and TIB≥ 7.5h (ie, no daytime symptoms), the same relationships persisted (Supplementary Table S4).
Prescribed Sleep Medication and Cognitive-Behavioural Therapy for Insomnia (CBTi) Usage in the Past 12 Months
A greater proportion of participants reported using prescribed medication (n = 168, 26.9%) in comparison to CBTi techniques (n = 72, 11.5%). More participants with probable insomnia reported the use of prescribed sleep medication (p < 0.001) and CBTi (p = 0.001) than participants who did not meet the criteria for probable insomnia (Table 6). Within those who met criteria for probable insomnia, 35.1% (n = 104) indicated they had been prescribed sleep medication. Only 15.9% (n = 47) had used CBTi.
 |
Table 6 Univariate Associations Between Probable Insomnia Status and Prescribed Sleep Medication Usage and Cognitive-Behaviour Therapy Techniques for Insomnia Administered by a Health Care Professional in the Last 12 Months |
Predictors of Using Prescribed Sleep Medication and Cognitive-Behavioural Therapy for Insomnia (CBTi) in the Past 12 Months
Factors associated with prescribed sleep medication and cognitive-behavioural therapy for insomnia (CBTi) usage are summarised in Supplementary Table S5. Use of prescribed medication was associated with probable insomnia (p < 0.001), current mental health difficulties (p = 0.02), and male sex (p = 0.02) (Table 7). In sensitivity analyses, associations with DIMS and TIB ≥7.5 hours (p = 0.03), current mental health difficulties (p < 0.01), and male sex (p = 0.04) persisted (Supplementary Table S6).
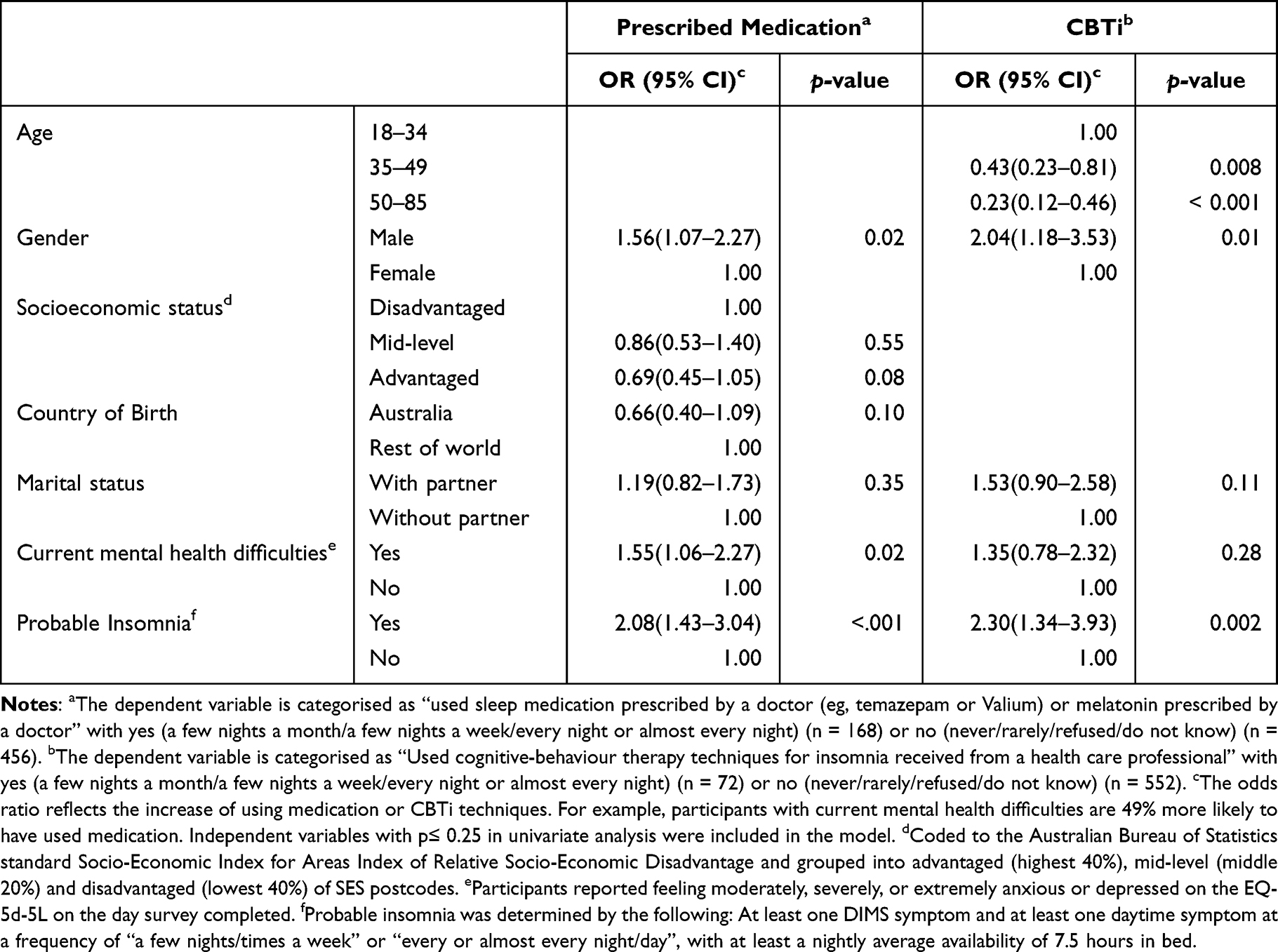 |
Table 7 Characteristics Associated with Using Sleep Medication Prescribed by a Doctor (eg, Temazepam or Valium, or Melatonin) and Using Cognitive-Behaviour Therapy for Insomnia (CBTi) in the Last 12 Months Determined by Binary Logistic Regression |
Use of CBTi in the overall sample was associated with probable insomnia (p = 0.002), younger age (18–34 years) (compared to older age 50–85 years; p < 0.001; early middle age 35–49; p = 0.008), and male sex (p = 0.01). In the sensitivity analysis using DIMS and TIB ≥7.5 hours, only the association with younger age (18–34 years) (compared to older age 50–85 years; p < 0.001; early middle age 35–49; p = 0.008), and male sex (p = 0.02), persisted (Supplementary Table S6).
Reasons for Not Accessing Consultation and/or Treatment from a Psychologist or Psychiatrist
Of the participants who did not receive consultation from a psychologist or psychiatrist but met criteria for probable insomnia (n = 232), 127 (54.7%) provided an indication of reasons for non-engagement. Reasons are summarised in Table 8. Cost concerns were the most common reason for not accessing such consultations, closely followed by general practitioners not raising psychological treatment as a possibility. Specified “other” reasons included sleep problems attributed to medical conditions, difficulties accessing services due to time constraints, and poor experiences with psychologists in the past.
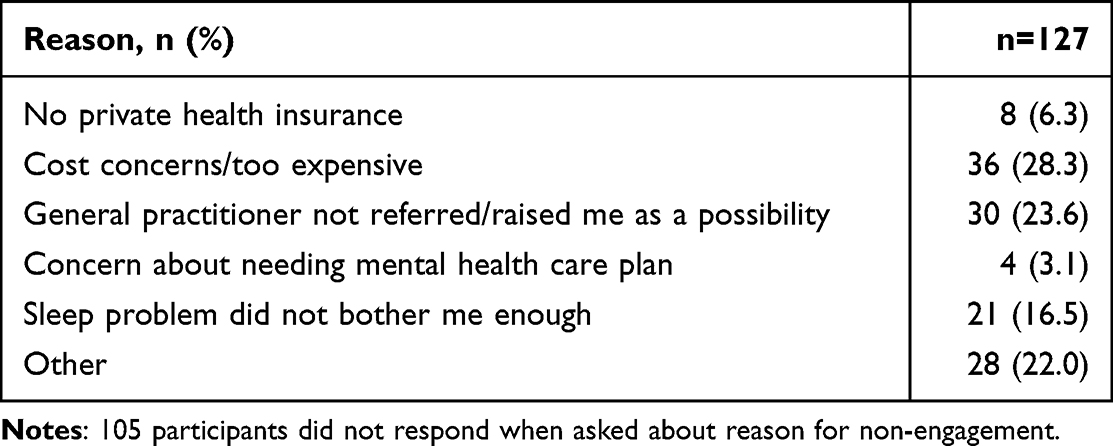 |
Table 8 Reasons for Not Accessing Consultation and/or Treatment from a Psychologist or Psychiatrist for a Sleep Problem in Participants with Probable Insomnia |
Discussion
The objective of this study was to examine the prevalence and predictors of discussions about sleep with health professionals and the utilisation of sleep treatments among a sample of Australian adults with mental health conditions. Out of the 624 participants who reported ever being diagnosed with a mental health condition, nearly half (47.4%) met the criteria for probable insomnia, with 53.9% currently experiencing mental health difficulties. Participants with probable insomnia were more likely to have discussed sleep with a health professional in the last 12 months and more likely to have engaged in multiple discussions on the topic. Among those with probable insomnia, 64.5% had discussed sleep with a health professional within the past 12 months, primarily with a general practitioner. However, despite the relatively high rates of discussions about sleep, a discrepancy was evident between these discussions and self-reported sleep treatment utilisation within the past 12 months. Approximately one-third of participants with probable insomnia (35.1%) reported using sleep medication, while only 15.9% reported using cognitive-behavioral therapy for insomnia (CBTi) techniques. This finding indicates a notable gap between discussing sleep and receiving appropriate treatment among individuals with mental health conditions who meet the criteria for probable insomnia.
A higher percentage of individuals with probable insomnia engaged in discussions about sleep with health professionals compared to the general population (64.5% vs 30.0%).2 While this is an encouraging finding, a significant proportion of individuals with probable insomnia reported that they did not discuss their sleep with a health professional within the past 12 months. This suggests that there is still room for improvement in terms of rates of discussions about sleep among individuals with probable insomnia. Treatment for insomnia has been shown to improve various mental health symptoms, regardless of whether insomnia is the primary complaint, implying that addressing sleep-related issues can have beneficial effects on both sleep and other mental health presentations.19,20 Therefore, increasing the rates of discussions about sleep and ensuring appropriate treatment for insomnia among individuals with mental health conditions may offer benefits for both sleep quality and mental health outcomes. In the present study, difficulties initiating and maintaining sleep were a primary driver for discussing sleep. Therefore, those with night-time insomnia symptoms but no daytime symptoms may still seek to improve their sleep by discussing it with a health professional. However, sensitivity analysis revealed that daytime symptoms, some of which overlap with current mental health difficulties, were also a driver for discussing sleep.
Despite two-thirds of individuals meeting the criteria for probable insomnia reporting discussing sleep with health professionals, few reported using CBTi techniques, which is the recommended first line treatment for insomnia symptoms. More than 50% of those who met the criteria for probable insomnia but did not access psychological or psychiatric services provided reasons for this. While general practitioners often manage insomnia symptoms through sleep hygiene education and prescribing medication, the provision of comprehensive sleep care can be challenging when patients present with other mental and physical health conditions due to time constraints and limited funding. Additionally, research has shown that general practitioners may have limited knowledge of CBTi and referral pathways, which can contribute to the underutilisation of this effective treatment option.21 Moreover, it has been reported that Australian health professionals receive limited training in providing sleep care.22 For example, a study conducted in 2021 among postgraduate psychology students in Australia (n = 138) reported that students received a median of only one hour of sleep education training, with almost half (47%) receiving no training at all.23 In summary, our study indicates that discussions about sleep are frequently initiated with health professionals, but this does not necessarily translate to the utilisation of first line treatment (CBTi). The lack of translation to treatment may be attributed to multiple factors, including constraints in time and funding for individual general practitioners, insufficient referral pathways,22 and the complexities associated with co-occurring mental health issues.21 Health professionals face various barriers in providing sleep care and referring patients for CBTi, particularly among individuals with mental health conditions.21 However, it is important to note that consumers also encounter barriers when accessing and receiving sleep care provision and CBTi.
Among participants who did not discuss their sleep with a psychologist or psychiatrist, cost concerns emerged as the most commonly reported reason. In Australia, general practitioners can prescribe sleep medication and, through the Better Access initiative, issue a Mental Health Treatment Plan, which provides access to and rebates for an initial ten sessions of treatment with a psychologist.24 CBTi incurs an initial higher cost, however improvements last over time, with prescribed sleep medication incurring higher costs over the long term.13 Further insight is needed to identify both clinician and consumer perceptions regarding the cost and access pathways to psychological treatment for insomnia. This is particularly salient for people with mental health conditions, who are more likely to be engaging with health services25 and have a low income.26
Individuals with probable insomnia and current mental health difficulties were more likely to report using sleep medication, regardless of the presence of daytime symptoms. People with probable insomnia were also more likely to have used CBTi techniques, albeit at much lower rates (15.9%). However, people with DIMS and TIB ≥7.5 hours only and current mental health difficulties were not more likely to use CBTi techniques. Therefore, the presence of daytime symptoms may have influenced the likelihood of receiving first line psychological treatment. The presence of overlapping daytime symptoms between insomnia and other mental health conditions, such as depression and anxiety,17 may influence health professionals’ decisions to provide or refer for psychological treatment. It is plausible that sleep difficulties are often perceived consequently or secondary to underlying mental health issues.19 Therefore, the perception and interpretation of daytime sleep symptoms by health professionals are crucial in determining assessment and treatment decisions. This aspect requires further exploration beyond the scope of the current cross-sectional study. It is evident that ongoing training and education for health professionals regarding evidence-based treatments for probable insomnia, including CBTi, is necessary. Knowledge and perceptions surrounding the efficacy of psychological treatments for insomnia may be limited.27 Improving health professionals’ understanding and awareness of these treatments can help bridge the gap between the prevalence of insomnia and the utilisation of appropriate interventions.
The findings of the current study should be interpreted considering several limitations. Firstly, the data collected in this study relied on self-report measures, which may introduce potential biases. Research has shown that individuals may not always accurately estimate variables related to sleep, such as sleep latency and duration.28,29 Additionally, the accuracy of recall regarding health utilisation can be influenced by factors, such as the design of the questionnaire30 and the length of the recall period.31 Secondly, the study assessed variables related to an ever-diagnosed mental health condition, sleep symptoms over the past month, and sleep discussions and treatment over the past 12 months. The use of different time periods for different variables may introduce some inconsistency in the data and limit the ability to draw causal conclusions. Such time frames may account for notable proportion of participants without probable insomnia who reported discussing sleep and receiving treatment in the last 12 months, as sleep issues may have been resolved at the time of completing the survey. Thirdly, it is important to acknowledge that the survey was conducted online, which may have resulted in the underrepresentation of individuals who have limited internet access, such as those from remote areas32 or with severe and chronic mental health symptoms.33 Fourthly, it is important to note that this study did not consider other conditions that could potentially affect sleep, such as chronic obstructive pulmonary disease (COPD)34 or sleep apnea.35 The focus of this study was specifically on mental health conditions and probable insomnia. Exploring the associations between probable insomnia and other medical conditions like COPD or sleep apnea was beyond the scope of this research. However, future studies should consider investigating the impact of comorbid conditions on sleep and treatment utilisation in individuals with mental health conditions, probable insomnia, and individuals not meeting criteria for probable insomnia. This would provide a more comprehensive understanding of the factors influencing sleep care provision in this population. Fifthly, it is important to consider the possibility of misreporting when participants indicated receiving cognitive-behavioral therapy (CBT) instead of CBT for insomnia (CBTi). Both CBT and CBTi can include similar therapeutic components, such as cognitive restructuring and relaxation techniques.36,37 It is possible that some participants may have mistakenly reported receiving CBTi when they received a broader form of CBT that included sleep-related elements. However, it is important to note that CBTi specifically includes additional components such as stimulus control and sleep restriction therapy, which are known to be highly effective in treating insomnia symptoms.38 Therefore, the reported percentage of participants who received CBTi from a health professional may be inflated due to potential misclassification. Lastly, it is worth mentioning that the availability of health professionals trained in CBTi can be a potential barrier for consumers seeking first line treatment.24,38 However, this specific barrier was not included as an option in the survey, and therefore, its impact on treatment access and utilisation was not directly assessed in this study.
Conclusions
This study highlights that while discussions about sleep with health professionals are relatively common among individuals with a mental health condition, the utilisation of effective sleep treatments, particularly cognitive-behavioral therapy for insomnia (CBTi), remains low. The findings indicate an unmet need for care, as a significant proportion of individuals with probable insomnia do not receive appropriate treatment. Pharmacological management, such as sleep medication, is more commonly utilized than CBTi, despite CBTi being the recommended first line treatment for insomnia. Cost concerns and the lack of referral for CBTi from general practitioners were reported as barriers to accessing this treatment. It is crucial to raise awareness of the importance of sleep and the benefits of evidence-based treatments, as well as to update clinical guidelines to highlight the need for routine sleep discussions and provide clear referral pathways.
Data Sharing Statement
Data may be available upon reasonable request to the corresponding author.
Acknowledgments
The authors would like to acknowledge all participants who completed the Sleep Health Foundation Insomnia 2019 Survey.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The insomnia survey was funded by the not-for-profit Australian Sleep Health Foundation, using an unrestricted grant from Merck, Sharp & Dohme (MSD Australia) Pty Limited. MSD Australia played no role in the study design, the collection, analysis and interpretation of data, the writing of the report, or the decision to submit the article for publication.
Disclosure
DIR is supported by a Research Training Program Stipend Scholarship provided by Murdoch University. Funder did not contribute, at any stage, to the development of this study or decision to publish. ACR is a spokesperson for the Sleep Health Foundation, conducting public and workplace presentations with the aim of increasing public awareness of sleep health. She has received funding from multiple industry sources not related to this project, and was a Chief Investigator on the Sleep Health Foundation funded project from which this analysis is drawn. SLA reports grants from Sleep Health Foundation, during the conduct of the study. RJA reports grants from Sleep Health Foundation, during the conduct of the study; grants from National Health and Medical Research Council, The Hospital Research Foundation, ResMed Foundation, Philips, and Flinders Foundation, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Appleton SL, Reynolds AC, Gill TK, Melaku YA, Adams RJ. Insomnia prevalence varies with symptom criteria used with implications for epidemiological studies: role of anthropometrics, sleep habit, and comorbidities. Nat and Sci Sleep. 2022;14:775–790. doi:10.2147/NSS.S359437
2. Reynolds AC, Appleton SL, Gill TK, Adams RJ Chronic insomnia disorder in Australia; 2019. Available from: https://www.sleephealthfoundation.org.au/news/special-reports/chronic-insomnia-disorder-in-australia.html.
3. Kocevska D, Lysen TS, Dotinga A, et al. Sleep characteristics across the lifespan in 1.1 million people from the Netherlands, United Kingdom and United States: a systematic review and meta-analysis. Nat Hum Behav. 2021;5(1):113–122. doi:10.1038/s41562-020-00965-x
4. Morin CM, Jarrin DC, Ivers H, Mérette C, LeBlanc M, Savard J. Incidence, persistence, and remission rates of insomnia over 5 years. JAMA Netw Open. 2020;3(11):e2018782–e2018782. doi:10.1001/jamanetworkopen.2020.18782
5. Baglioni C, Nanovska S, Regen W, et al. Sleep and mental disorders: a meta-analysis of polysomnographic research. Psychol Bull. 2016;142(9):969–990. doi:10.1037/bul0000053
6. Roth T, Jaeger S, Jin R, Kalsekar A, Stang PE, Kessler RC. Sleep problems, comorbid mental disorders, and role functioning in the national comorbidity survey replication. Biol Psychiatry. 2006;60(12):1364–1371. doi:10.1016/j.biopsych.2006.05.039
7. Seow LSE, Verma SK, Mok YM, et al. Evaluating DSM-5 insomnia disorder and the treatment of sleep problems in a psychiatric population. J Clin Sleep Med. 2018;14(2):237. doi:10.5664/jcsm.6942
8. Mosher WA, Piccinini‐Vallis H. Assessing the frequency with which primary care providers address sleep of infants and young children. J Sleep Res. 2022;31(5):e13579. doi:10.1111/jsr.13579
9. Klingman KJ, Williams NJ, Perlis ML, Grandner MA. Doctor-patient sleep discussions for US adults: results from the SHADES study. Sleep Health. 2019;5(6):658–665. doi:10.1016/j.sleh.2019.07.004
10. Metse AP, Fehily C, Clinton-McHarg T, et al. Self-reported suboptimal sleep and receipt of sleep assessment and treatment among persons with and without a mental health condition in Australia: a cross sectional study. BMC Public Health. 2021;21(1):1–12. doi:10.1186/s12889-020-10013-y
11. O’Sullivan M, Rahim M, Hall C. The prevalence and management of poor sleep quality in a secondary care mental health population. J Clin Sleep Med. 2015;11(2):111–116. doi:10.5664/jcsm.4452
12. Reeve S, Sheaves B, Freeman D. Sleep disorders in early psychosis: incidence, severity, and association with clinical symptoms. Schizophr Bull. 2019;45(2):287–295. doi:10.1093/schbul/sby129
13. Sweetman A, Putland S, Lack L, et al. The effect of cognitive behavioural therapy for insomnia on sedative-hypnotic use: a narrative review. Sleep Med Rev. 2021;56:101404. doi:10.1016/j.smrv.2020.101404
14. Australian Bureau of Statistics. Census of Population and Housing: Socio-Economic Indexes for Areas (SEIFA); 2018. Available from: https://www.abs.gov.au/ausstats.
15. Livingston M, Callinan S, Vashishtha R, Yuen WS, Dietze P. Tracking the decline in Australian adolescent drinking into adulthood. Addiction. 2022;117(5):1273–1281. doi:10.1111/add.15720
16. American Academy of Sleep Medicine. International Classification of Sleep Disorders.
17. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5.
18. EuroQol Research Foundation. EQ-5D-5L user guide; 2019. Available from: https://euroqol.org/publications/user-guides.
19. Freeman D, Sheaves B, Waite F, Harvey AG, Harrison PJ. Sleep disturbance and psychiatric disorders. Lancet Psychiatry. 2020;7(7):628–637. doi:10.1016/S2215-0366(20)30136-X
20. Hertenstein E, Nissen C, Freeman D. CBT‐I protocols for insomnia co‐morbid with other mental disorders. In: Baglioni C, Espie CA, Riemann D, editors. Cognitive-Behavioural Therapy for Insomnia (CBT-I) Across the Life Span: Guidelines and Clinical Protocols for Health Professionals. John Wiley & Sons; 2022.
21. Haycock J, Grivell N, Redman A, et al. Primary care management of chronic insomnia: a qualitative analysis of the attitudes and experiences of Australian general practitioners. BMC Fam Pract. 2021;22(1):1–11. doi:10.1186/s12875-021-01510-z
22. Meaklim H, Jackson ML, Bartlett D, et al. Sleep education for healthcare providers: addressing deficient sleep in Australia and New Zealand. Sleep Health. 2020;6(5):636–650. doi:10.1016/j.sleh.2020.01.012
23. Meaklim H, Rehm IC, Monfries M, Junge M, Meltzer LJ, Jackson ML. Wake up psychology! Postgraduate psychology students need more sleep and insomnia education. Aust Psychol. 2021;56(6):485–498. doi:10.1080/00050067.2021.1955614
24. Department of Health. Better access initiative; 2022. Available from: https://www.health.gov.au/initiatives-and-programs/better-access-initiative.
25. Australian Institute of Health and Welfare. Mental health services in Australia: in brief 2018; 2018. Available from: https://www.aihw.gov.au.
26. Isaacs AN, Enticott J, Meadows G, Inder B. Lower income levels in Australia are strongly associated with elevated psychological distress: implications for healthcare and other policy areas. Front Psychiatry. 2018;9:536–536. doi:10.3389/fpsyt.2018.00536. doi:10.3389/fpsyt.2018.00536
27. Everitt H, McDermott L, Leydon G, Yules H, Baldwin D, Little P. GPs’ management strategies for patients with insomnia: a survey and qualitative interview study. Br J Gen Pract. 2014;64(619):e112–e119. doi:10.3399/bjgp14X677176
28. Harvey AG, Tang NKY. (Mis)perception of sleep in insomnia: a puzzle and a resolution. Psychol Bull. 2012;138(1):77–101. doi:10.1037/a0025730
29. McIntyre JPR, Ingham CM, Hutchinson BL, et al. A description of sleep behaviour in healthy late pregnancy, and the accuracy of self-reports. BMC Pregnancy Childbirth. 2016;16(1):1–8. doi:10.1186/s12884-016-0905-0
30. Bhandari A, Wagner T. Self-reported utilization of health care services: improving measurement and accuracy. Med Care Res Rev. 2006;63(2):217–235. doi:10.1177/1077558705285298
31. Dalziel K, Li J, Scott A, Clarke P. Accuracy of patient recall for self‐reported doctor visits: is shorter recall better? Health Econ. 2018;27(11):1684–1698. doi:10.1002/hec.3794
32. Australian Bureau of Statistics. Household use of information technology; 2018. Available from: https://www.abs.gov.au/statistics/industry/technology-and-innovation/household-use-information-technology/latest-release.
33. Too LS, Leach L, Butterworth P. Mental health problems and internet access: results from an Australian national household survey. JMiR Ment Health. 2020;7(5):e14825. doi:10.2196/14825
34. Chetty U, McLean G, Morrison D, Agur K, Guthrie B, Mercer SW. Chronic obstructive pulmonary disease and comorbidities: a large cross-sectional study in primary care. Br J Gen Pract. 2017;67(658):e321–e328. doi:10.3399/bjgp17X690605
35. Kaufmann CN, Susukida R, Depp CA. Sleep apnea, psychopathology, and mental health care. Sleep Health. 2017;3(4):244–249. doi:10.1016/j.sleh.2017.04.003
36. Morin CM, Bootzin RR, Buysse DJ, Edinger JD, Espie CA, Lichstein KL. Psychological and behavioral treatment of insomnia: update of the recent evidence (1998–2004). Sleep. 2006;29(11):1398–1414. doi:10.1093/sleep/29.11.1398
37. Rossman J. Cognitive-behavioral therapy for insomnia: an effective and underutilized treatment for insomnia. Am J Lifestyle Med. 2019;13(6):544–547. doi:10.1177/1559827619867677
38. Koffel E, Bramoweth AD, Ulmer CS. Increasing access to and utilization of cognitive behavioral therapy for insomnia (CBT-I): a narrative review. J Gen Intern Med. 2018;33:955–962. doi:10.1007/s11606-018-4390-1
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.