")
Back to Journals » Infection and Drug Resistance » Volume 16
Use of Contezolid for the Treatment of Refractory Infective Endocarditis in a Patient with Chronic Renal Failure: Case Report
Authors Zhao S, Zhang W, Zhang L, Zhang J, Li J , Si L, Ding Y, Li M, Song Y
Received 22 March 2023
Accepted for publication 31 May 2023
Published 13 June 2023 Volume 2023:16 Pages 3761—3765
DOI https://doi.org/10.2147/IDR.S413452
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Supplementary video of "Contezolid for infective endocarditis" [ID 413452].
Views: 245
Sheng Zhao, Wei Zhang, Linfei Zhang, Jing Zhang, Jinghang Li, Linjie Si, Yi Ding, Mingke Li, Yuanyuan Song
Department of Cardiovascular Surgery, The First Affiliated Hospital of Nanjing Medical University (Jiangsu Province Hospital), Nanjing, People’s Republic of China
Correspondence: Sheng Zhao, Department of Cardiovascular Surgery, The First Affiliated Hospital of Nanjing Medical University (Jiangsu Province Hospital), Nanjing, 210029, People’s Republic of China, Tel +86-25-83714511ext 3107, Fax +86-25-83718836, Email [email protected]
Abstract: Infective endocarditis (IE) caused by methicillin-resistant Staphylococcus aureus (MRSA) is usually life threatening and difficult to treat. Contezolid is a newly approved oxazolidinone antimicrobial agent showing potent activity against MRSA. We successfully treated a case of refractory IE caused by MRSA with contezolid in a 41-year-old male patient. The patient was admitted due to recurrent fever and chills for more than 10 days. He had chronic renal failure for more than 10 years and under ongoing hemodialysis. The diagnosis of IE was confirmed by echocardiography and positive blood culture of MRSA. Antimicrobial therapy with vancomycin combined with moxifloxacin, and daptomycin combined with cefoperazone-sulbactam failed in the first 27 days. Moreover, the patient had to take oral anticoagulant after removal of tricuspid valve vegetation and tricuspid valve replacement. Contezolid 800 mg was added orally every 12 hours, to replace vancomycin, for its anti-MRSA activity and good safety profile. Temperature normalized after the contezolid add-on treatment for 15 days. No relapse of infection or drug-related adverse reaction was reported at 3-month follow-up since the diagnosis of IE. This successful experience serves as motivation for a well-designed clinical trial to confirm the utility of contezolid in managing IE.
Keywords: infective endocarditis, methicillin-resistantStaphylococcus aureus, contezolid, chronic renal failure
Introduction
Infective endocarditis (IE) is a common life threatening cardiovascular disease associated with high incidence and fatality rate. As a result of death and illness or function impairment, IE caused the loss of 1.58 million disability-adjusted life-years in 2010 globally.1 Currently, more IE patients may have comorbidities such as chronic obstructive pulmonary disease, diabetes mellitus, cancer, and liver or kidney disease. Native valve IE still accounts for 71% to 78% of total cases even though the incidence of prosthetic valve and cardiac device-related endocarditis is increasing (13–17%) as more patients may have a history of valve surgery and the use of implanted pacemakers or defibrillators increases.1,2 Majority of IE cases are caused by Gram-positive bacteria, especially Staphylococcus species. Staphylococcus aureus remains the most common pathogen of IE, causing 20% to 68% of cases in both native and prosthetic valve infections.1 Methicillin-resistant S. aureus (MRSA) is a major cause for concern in IE treatment, especially among high-risk patients, such as chronic hemodialysis patients and injection drug users.
The 2015 European Society of Cardiology (ESC) guidelines for the management of infective endocarditis recommend vancomycin as the first line treatment for IE caused by MRSA.2 However, nephrotoxicity has limited the use of vancomycin. MRSA isolates are usually also resistant to other alternative antimicrobial agents. Therefore, it is highly challenging to manage IE caused by MRSA in a critically ill patient with severe underlying diseases. A newly developed antimicrobial agent with a safer profile and higher anti-MRSA activity may provide an opportunity to cure such cases. We successfully treated a case of acute IE caused by MRSA with contezolid, a newly approved oxazolidinone antibiotic, in a patient under ongoing hemodialysis due to chronic renal failure. This case may help clinicians consider the potential utility of contezolid alone or in combination therapy in managing refractory infections.
Case Presentation
The patient was a 41-year-old male (body weight of 70 kg) who was admitted to the Kidney Critical Unit of Jiangsu Province Hospital due to recurrent fever for more than 10 days. The patient had a history of uremia for more than 10 years. He had been receiving continuous renal replacement therapy via hemodialysis. The patient got a fever (38.6 °C) and chills for unknown reason about 10 days prior. Oral prednisone and ibuprofen suspension were used to help control the fever of unknown origin but only contained the temperature temporarily. Echocardiography and laboratory tests confirmed the diagnosis of acute IE caused by MRSA, which was isolated from sputum and blood culture. A local hospital had used vancomycin plus moxifloxacin to treat IE which failed. The patient also had a history of restless leg syndrome for 9 years and thoracic trauma in March 2021.
At the time of admission, the patient had a clear mind in thinking. Physical examination showed body temperature of 36.8°C, respiratory frequency 25 breaths per minute, heart rate 124 beats per minute, and blood pressure 107/75 mmHg. Wet rales were heard on both lungs. Chest CT scan identified multiple patchy nodular opacities with cavities in both lungs. Systolic heart murmur was heard over the tricuspid valve area. Echocardiography revealed the presence of tricuspid valve vegetation along with left heart enlargement and abnormal ventricular wall movement. Moderate reflux of mitral valve and tricuspid valve and reduction of left ventricular contractile function were also confirmed (Supplementary Video 1). The left ventricular ejection fraction was about 20%. Initial laboratory tests showed significant leukocytosis (WBC 21.4×109/L) and neutrophils predominance (90.1%), decreased lymphocytes (1.1×109/L), anemia (hemoglobin of 6.8 g/dL), and platelet count of 260×109/L. Serum procalcitonin was elevated to 1.55 ng/mL (normal range: 0–0.5 ng/mL) and N-terminal pro-B-type natriuretic peptide (NT-proBNP) was also significantly higher (>35,000 pg/mL) than normal range (<125 pg/mL). MRSA was isolated from sputum and blood culture repeatedly (on July 8, July 17, and July 24). This clinical evidence confirmed the diagnosis of right heart IE due to MRSA (Table 1).
 |
Table 1 Antimicrobial Susceptibility Testing of the Methicillin-Resistant Staphylococcus aureus Isolated from Blood of a Patient Diagnosed with Infective Endocarditis on July 17 |
Vancomycin (1.0 g q12h) and moxifloxacin were used to control infection initially in accordance with the guideline for management of IE and the results of antimicrobial susceptibility testing.2 However, the patient had recurrent fever up to 39.0°C until admission to our hospital. After admission, moxifloxacin was switched to daptomycin (420 mg qd) plus cefoperazone-sulbactam (3.0 g q8h) empirically considering the potent activities of daptomycin against MRSA and possible Gram-negative bacterial infection. Emergency surgical procedures were carried out to remove the vegetation on the tricuspid papillary muscle and replace the tricuspid valve. Unfortunately, fever remained after the operation, which was considered partly due to bloodstream and pulmonary MRSA infection. Secondary Acinetobacter baumannii infection was also possible because a new infection was detected by chest radiography. Vancomycin was combined with daptomycin to control MRSA infection because daptomycin alone was insufficient. Considering the severe underlying disease of the patient, nephrotoxicity of vancomycin, and possible bleeding tendency due to oral anticoagulants after surgery, the anti-MRSA regimen was further adjusted. Contezolid 800 mg was administered orally twice daily to replace vancomycin to target MRSA. Tigecycline and meropenem were also used to deal with the secondary pulmonary infection caused by A. baumannii. The clinical symptoms were resolved and the temperature was normlalized 15 days after contezolid add-on therapy (Figure 1). The subsequent blood culture was negative.
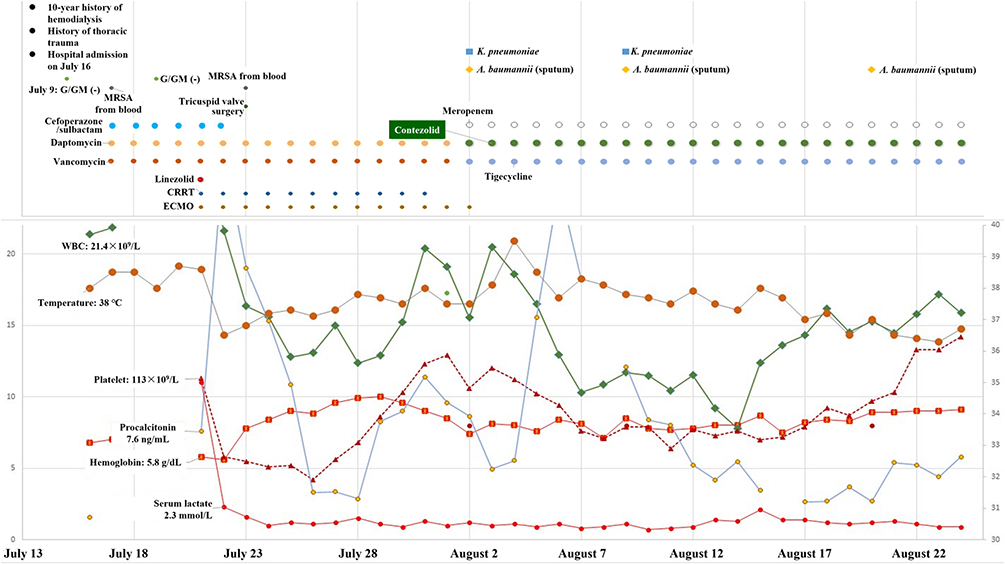 |
Figure 1 Antimicrobial therapies and the changing patterns of clinical variables in a patient with acute infective endocarditis. Antimicrobial dosing regimens: contezolid 800 mg q12h; daptomycin 420 mg once daily; cefoperazone/sulbactam 3.0 g q8h; vancomycin 1.0 g q12h; meropenem 2g q12h; tigecycline 100mg q12h; linezolid 600mg q12h. Abbreviations: CRRT, continuous renal replacement therapy; ECMO, extracorporeal membrane oxygenation; G/GM(-), negative result of serum (1,3)-β-D glucan (G-test) and galactomannan (GM-test) for fungal infections; MRSA, methicillin-resistantStaphylococcus aureus; WBC, white blood cell count. |
At the 3-month follow-up since the diagnosis of IE, no relapse of infection or drug-related adverse reaction was reported. The latest follow-up laboratory tests on February 14, 2022 (6 months after discharge from hospital) did not show any symptoms or signs of IE. The liver function and coagulation tests were generally normal except slight bleeding tendency, evidenced by prothrombin time of 15.9 seconds (normal range: 10.2–12.9) and international normalized ratio of 1.35 (normal range: 0.87–1.16). Overall, the refractory IE caused by MRSA was successfully treated with oral contezolid 800 mg every 12 hours (twice daily) for 45 days.
Discussion
Aging population and increasing use of prosthetic valve and cardiac devices have led to a large number of IE.2 Antimicrobial treatment is essential because bacterial pathogens are the fundamental cause of IE. Chronic renal failure and multidrug-resistant pathogens are always factors interfering with the choice of appropriate antimicrobial agents, just like in this case. Even after surgical treatment to remove the vegetation and replace the tricuspid valve, it should not be taken for granted or assumed that the IE would be cured easily.
Vancomycin is the first-line treatment for IE because most cases are caused by Staphylococcus species, especially S. aureus.1,2 In the cases of MRSA infection, vancomycin is always the first choice of clinicians. However, bone marrow suppression, neuropathy, nephrotoxicity, and other side effects of intravenous administration have reminded doctors to curtail vancomycin dose.3,4 In this case, vancomycin was used initially according to the guidelines for management of IE caused by MRSA which lasted 27 days. But the clinical efficacy was not satisfactory. Daptomycin add-on therapy also failed to control MRSA infection. Vancomycin and daptomycin failed even after the removal of vegetation and replacement of the tricuspid valve. Successive cultures and antimicrobial susceptibility testing showed the MICs of vancomycin against MRSA strains were 1, 1, and ≤0.5 mg/L (all susceptible). Inadequate vancomycin concentration at the site of infection may be the main cause of treatment failure. The clinical outcome is not always consistent with the laboratory findings.
Contezolid is a newly developed oxazolidinone antibiotic which was approved by the National Medical Products Administration of China in June 2021 for the treatment of complicated skin and soft tissue infections caused by Gram-positive pathogens. It is an ideal alternative choice to vancomycin. The off-label use of contezolid for treating refractory IE caused by MRSA achieved satisfactory result in this case. The unique molecular structure allows contezolid to bind more tightly to bacterial targets to exert higher antibacterial activity and to reduce the probability of developing resistance.5 Before contezolid add-on therapy, various antimicrobial agents did not lead to the resolution of clinical infection (eg, WBC, temperature, and procalcitonin) in nearly one month. Contezolid therapy helped the patient recover from IE, but did not produce any of the adverse effects (eg, thrombocytopenia, skin rashes) commonly observed with other antibiotics.6,7 Both in vitro and in vivo studies5 have indicated that, unlike other oxazolidinone drugs, contezolid has no significant monoamine oxidase inhibition effect, so oral administration of contezolid is unlikely to induce the drug-drug interaction related to monoamine oxidase inhibition.
Our preliminary experience suggests that in addition to vancomycin, novel anti-MRSA antibiotics such as contezolid and daptomycin may be considered for patients with severe kidney disease, which may probably limit the use of vancomycin. This consideration is based on the etiological features of IE, namely, most pathogens are Gram-positive bacteria.8,9 Oral contezolid has another advantage in longer duration of treatment, which can avoid the side effects of intravenous administration. Some authors have reported that early sequential oral administration of linezolid is a good choice to enhance long-term health and economic outcomes.10 In a systematic review of published case reports, 63.6% (21/33) of IE patients were cured after linezolid therapy, but thrombocytopenia developed in 30.8% (8/26) of the patients with relevant laboratory data.3 Another systematic review compared the effectiveness and safety of linezolid versus vancomycin, teicoplanin, or daptomycin against MRSA bacteremia, which indicated that the four drugs were comparable in the primary effectiveness outcome (all-cause mortality) and secondary effectiveness outcomes (including clinical and microbiological cure, hospital length of stay, recurrence, and 90-day readmission rates), and drug-related adverse effects.11 The authors suggest that linezolid could be a potential first-line drug against MRSA bacteremia. As a newer member of oxazolidinones, oral contezolid may be more appropriate than linezolid in the treatment of IE due to its better safety profile and satisfactory antibacterial activity.12 Recently, it was reported that MRSA-associated sepsis was treated with contezolid successfully in an elderly patient.13
There are some limitations in this case report, which may affect the judgement of the effect of contezolid treatment. Firstly, the new drug contezolid was not tested in antimicrobial susceptibility testing because it is a newly approved antibiotic and no standards or disk were available for clinical laboratory to use. Secondly, the patient had not only IE, but also secondary pulmonary infection caused by Gram-negative bacteria. The antimicrobial regimens covered both Gram-positive and Gram-negative pathogens. It is impossible to separately evaluate the efficacy of contezolid on MRSA alone because other antibiotics in the combination therapy such as tigecycline may also have activity against MRSA. In summary, the successful experience in this case serves as motivation for a well-designed clinical trial to confirm the utility of contezolid in managing IE.
Data Sharing Statement
Data will be provided by the corresponding author upon reasonable request.
Informed Consent Statement
Informed consent was obtained from the patient for the publication of his medical information in this case report.
Disclosure
All authors declare no conflict of interest. The research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Yang E, Frazee BW. Infective endocarditis. Emerg Med Clin North Am. 2018;36:645–663. doi:10.1016/j.emc.2018.06.002
2. Habib G, Lancellotti P, Antunes MJ, et al; ESC Scientific Document Group. 2015 ESC guidelines for the management of infective endocarditis: the task force for the management of infective endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J. 2015;36(44):3075–3128. doi:10.1093/eurheartj/ehv319
3. Falagas ME, Manta KG, Ntziora F, Vardakas KZ. Linezolid for the treatment of patients with endocarditis: a systematic review of the published evidence. J Antimicrob Chemother. 2006;58:273–280. doi:10.1093/jac/dkl219
4. Colli A, Campodonico R, Gherli T. Early switch from vancomycin to oral linezolid for treatment of gram-positive heart valve endocarditis. Ann Thorac Surg. 2007;84:87–91. doi:10.1016/j.athoracsur
5. Gordeev MF, Yuan ZY. New potent antibacterial oxazolidinone (MRX-I) with an improved class safety profile. J Med Chem. 2014;57(11):4487–4497. doi:10.1021/jm401931e
6. Linezolid Tablets Prescribing Information. Available from: https://www.drugs.com/pro/linezolid-tablets.html. Accessed August 10, 2022.
7. Wang W, Voss KM, Liu J, Gordeev MF. Nonclinical evaluation of antibacterial oxazolidinones contezolid and contezolid acefosamil with low serotonergic neurotoxicity. Chem Res Toxicol. 2021;34(5):1348–1354. doi:10.1021/acs.chemrestox.0c00524
8. Chen X, Liu Y, Yu H, et al. Clinical characteristics, pathogenic distribution, treatment and prognosis of 300 patients with infective endocarditis hospitalized in fuwai hospital [In Chinese]. Chin Circ J. 2018;33:1102–1107.
9. Cheng J, Hu H, Zhang H, et al. Pathogen distribution and clinical characteristics analysis of 802 patients with infective endocarditis [In Chinese]. Chin Circ J. 2020;35:180–184.
10. Iversen K, Ihlemann N, Gill SU, et al. Partial oral versus intravenous antibiotic treatment of endocarditis. N Engl J Med. 2019;380:415–424. doi:10.1056/NEJMoa1808312
11. Kawasuji H, Nagaoka K, Tsuji Y, et al. Effectiveness and safety of linezolid versus vancomycin, teicoplanin, or daptomycin against methicillin-resistant Staphylococcus aureus bacteremia: a systematic review and meta-analysis. Antibiotics. 2023;12(4):697. doi:10.3390/antibiotics12040697
12. Carvalhaes CG, Duncan LR, Wang W, Sader HS. In vitro activity and potency of the novel oxazolidinone contezolid (MRX-I) tested against gram-positive clinical isolates from the United States and Europe. Antimicrob Agents Chemother. 2020;64(11):e01195–e01220. doi:10.1128/AAC.01195-20
13. Ma GH, Li XY, Li MJ, Zhu HL. A case report of MRSA-associated sepsis successfully treated with contezolid in an elderly patient [in Chinese]. Chin J Pract Intern Med. 2022;42(12):1045–1047.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.