")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Usage of Glucagon-Like Peptide-1 for Obesity in Children; Updated Review of Clinicaltrials.gov
Authors Alorfi NM , Alshehri FS
Received 16 May 2023
Accepted for publication 7 July 2023
Published 31 July 2023 Volume 2023:16 Pages 2179—2187
DOI https://doi.org/10.2147/JMDH.S419245
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Nasser M Alorfi, Fahad S Alshehri
Pharmacology and Toxicology Department, College of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia
Correspondence: Nasser M Alorfi, Pharmacology and Toxicology Department, Faculty of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia, Tel +966 500644261, Email [email protected]
Background: Obesity in both adults and children is a primary health concern that can lead to many complications at a young age, including insulin resistance, type 2 diabetes, and other diseases. Glucagon-like peptide-1 receptor agonists (GLP-1) are drugs utilized to treat diabetes, but they are also approved as an adjunct to a low-calorie diet to reduce body weight and to enhance the metabolic profile readings for diabetic and non-diabetic patients. However, their efficacy and safety in children have not been extensively examined.
Aim: To identify glucagon-like peptide-1 medications for obesity in pediatric participants (aged up to 17 years old).
Methods: Analysis of all clinical trials registered on ClinicalTrials.gov for obesity using GLP-1 as a treatment for children.
Results: As of January 26th, 2023, 10,828 clinical trials were found. The search included childhood obesity using GLP-1. The number of trials on the use of GLP-1 to treat childhood obesity is limited. The final number of analyzed trials was 19. GLP-1 has been shown to result in the effective management of body gain among children.
Conclusion: Exenatide, semaglutide, and liraglutide were the only GLP-1 medications used as the pharmacotherapy option. It has been studied in many circumstances eg, to treat children with severe obesity, PCOS, hypothalamic obesity, glucose tolerance, and as a complementary treatment alongside behavior-lifestyle change and surgery for obesity.
Keywords: obesity, GLP-1, clinical trials, exenatide, semaglutide, liraglutide
Introduction
Obesity in both adults and children is a primary health concern and a number of complications can arise from the condition at a young age, such as insulin resistance, type 2 diabetes mellitus (DM), and other diseases.1 Obese children are more likely to experience hypertension, hyperlipidemia, liver and kidney diseases, cardiovascular disease, asthma, sleep apnea, and bone and joint problems.2,3 Obesity in pediatrics not only affects physical health, but mental health is also affected.4–6 Obese and overweight children are also more likely to experience bullying, depression, social isolation, and struggles with self-esteem than children of normal weight.7,8 The prevalence of obesity has been linked to low levels of physical activity, a poor diet and a generally sedentary way of life.9–11 Additionally, many pre-packaged and processed foods are high in calories and low in nutrients, making it easier for people to consume excess calories and gain weight.12,13
Therapeutically, glucagon-like peptide-1 receptor agonists (GLP-1) are employed to treat diabetes but they have also been approved as an adjunct to a lower calorie diet to reduce total body weight, and to enhance the metabolic profile readings for diabetic and non-diabetic patients.14–16 Their mechanism of action is that they act like GLP-1 by binding GLP-1 receptors in several tissues, for example, pancreatic beta cells, pancreatic ducts and gastric mucosa.15 Their main effect is the stimulation of the release of glucose-dependent insulin from pancreatic islets decreasing glucagon secretion in a glucose-dependent manner.17 As they slow down gastric emptying, they promote satiety, thereby reducing the number of calories consumed.18,19 They also increase the activity of lipolysis in adipocytes, leading to increased fat metabolism and reduced fat storage in the body.20,21 This can lead to weight loss, improved insulin sensitivity, and improved metabolic profile readings.22,23
However, the efficacy and safety of this drug for children have not been extensively examined. Turning to the situation of pediatrics and obesity, the World Health Organization (WHO) reported that around 39 million children aged less than 5 years old were overweight or obese in 2020. Furthermore, in 2016, among the global population of children and adolescents (aged between 5 and 19 years old), more than 340 million were obese or overweight.24
Human studies have been performed to assess the effects of GLP-1 drugs on obesity, a consequence of engaging in obesity-related behaviors or being obese. A few clinical trials have been performed with children, and this paper analyzes the usage of GLP-1 with obese children.
Methods
Clinical Trials Data
The search process involved conducting a comprehensive exploration of clinical trials registered on the ClinicalTrials.gov database up to and including the date of 26th January 2023. To identify relevant studies, we utilized the keyword “Obesity” as the criterion for the “condition and disease” category within the search engine.
Data Screening and Extraction
The studies related to GLP-1 usage in obese children were screened by using database filters. “Child (birth-17)” was used as an eligibility criterion to select only the trials conducted with children. Then, “Glucagon-Like Peptide 1” was selected for the next step for the drug intervention, located on the topic tab. Exclusion criteria were used to continue the screening. Non-GLP-1 agonist drug usage and “no-results shown” were used as exclusion criteria. Eight studies passed the screening as they involved children and the use of a GLP-1 agonist. Prisma flow diagram of search identified from Clinicaltrials.gov bases presented in Figure 1.
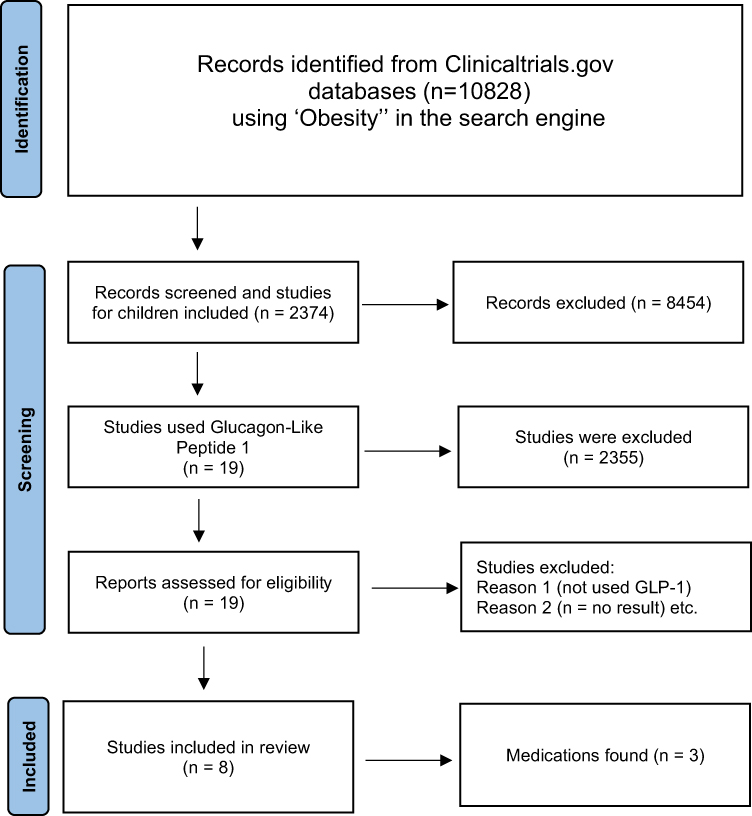 |
Figure 1 PRISMA flow chart of studies via Clinicaltrials.gov databases (Updated on 24th January 2022). Notes: Adapted from BMJ (OPEN ACCESS) Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow et al The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71.25 |
Data and information from the trials were extracted and categorized to show their trends and characteristics. The issues for categorization were title of clinical trial, drug used, condition, number of sample (n), phase of study, involvement in obesity and the rationale for GLP-1 usage were shown in Table 1. Pharmacological class, indication, and the side effects of the GLP-1 agonists used were tabulated in Table 2. Rationales for GLP-1 Usage in these trials were fully explained in Table 3.
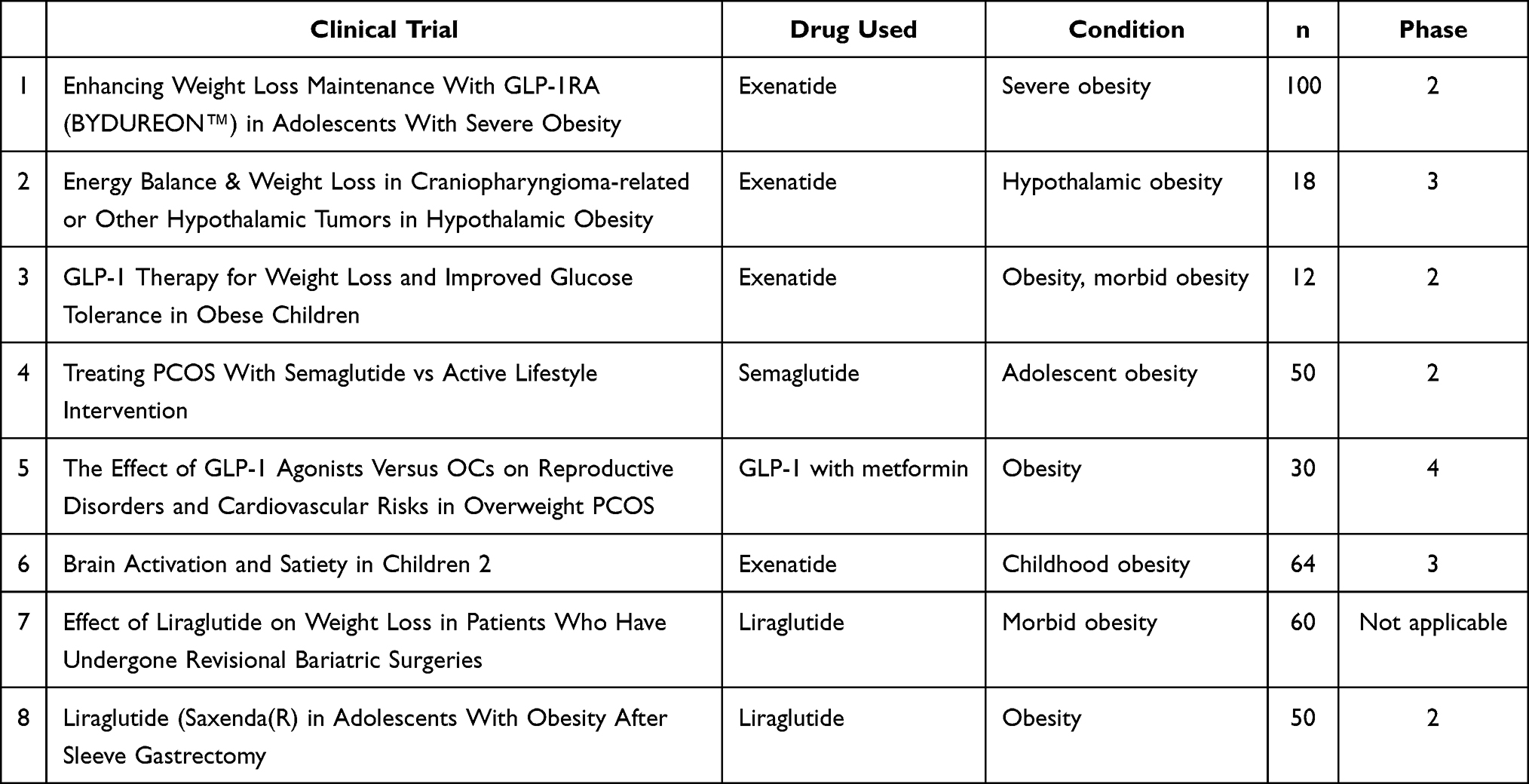 |
Table 1 Clinical Trials, Drug Used, Condition, Enrolment Size and Clinical Phase |
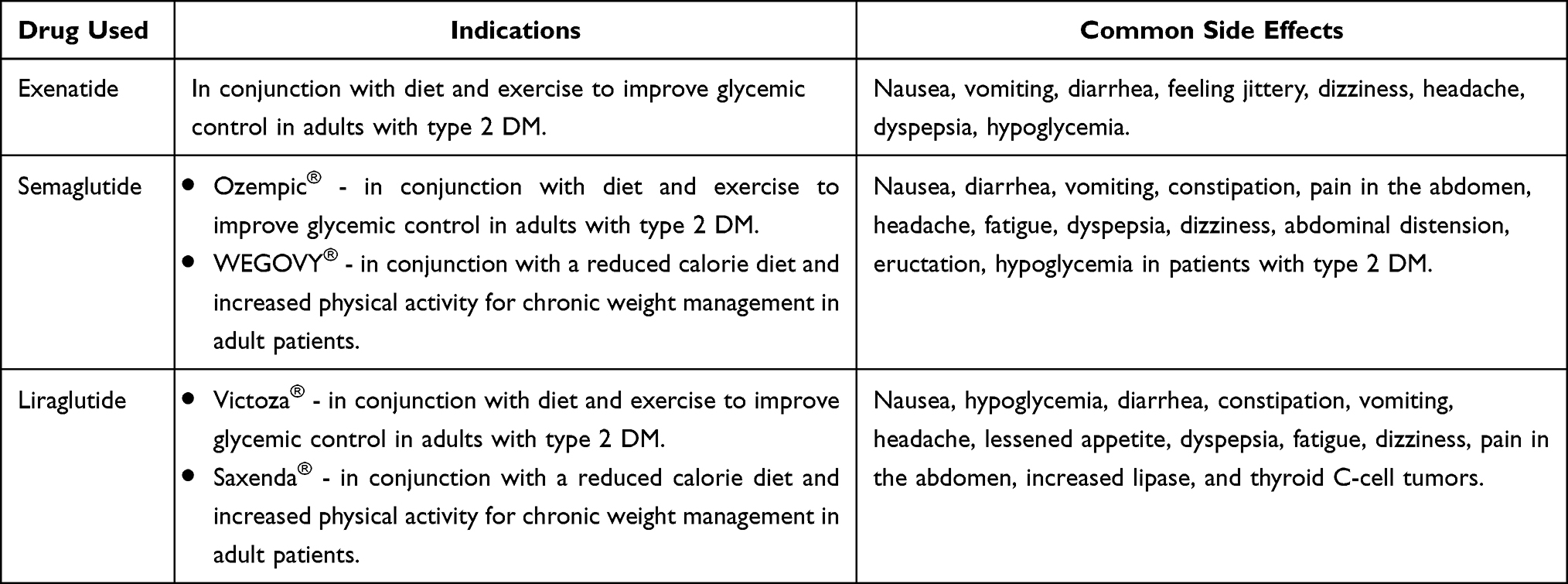 |
Table 2 Main GLP-1 Drugs Used, Indication, and Common Side Effects |
 |
Table 3 Rationale for GLP-1 Usage |
Results
The clinical trials registered up to and including 26th January 2023 on the ClinicalTrials.gov database was searched, using “Obesity” as the keyword for “condition and disease” in the search engine. In total, 10,828 studies related to obesity were found. This effectively located the relevant clinical trials and allowed the researchers to quickly identify studies on the topic of interest.
Drugs Used to Treat Obesity in Children
Nineteen studies were found, but only three drugs were used. These are detailed below.
- Exenatide, which is a drug that activates GLP-1 receptors, was authorized by the US Food and Drug Administration (FDA) in 2005 to help adults with type 2 DM to improve their glycemic control in combination with diet and exercise.26,27 Its mechanism is similar to that of other GLP-1 receptor agonists. By attaching to GLP-1 receptors in the pancreas, it triggers a rise in the glucose-dependent release of insulin from beta cells, inhibiting glucagon secretion, slowing down the emptying of the stomach, and decreasing food consumption.28,29 In terms of side effects, the most common is nausea; this varies with the dosage and is becomes less common with continuous use of the drug.30 Other less common side effects are vomiting, diarrhea, hypoglycemia, feeling dizzy, headaches, pruritus or nodules at the injection site, and dyspepsia.31–33 Moreover, exenatide itself is teratogen class C and cannot be used in pregnancy.26 With regard to the incidence of hypoglycemia when taking exenatide, it is lower than with other diabetic therapies, due to the glucose-dependent release of insulin.34,35
- Semaglutide is a drug that stimulates GLP-1 receptors and is recommended as a supplementary treatment along with diet and exercise to enhance glycemic regulation in adults diagnosed with type 2 DM.15 It was approved in 2017 by the US FDA under the trade name of “Ozempic”. “WEGOVY” has been granted approval as a supplementary therapy along with a decreased calorie intake and increased physical activity to promote long-term weight control among adult patients who have an initial BMI ≥30 kg/m2 (obesity) or ≥ 27 kg/m2 (overweight) in combination with at least one comorbid condition associated with weight gain (such as dyslipidemia, hypertension, or type 2 DM).36–38
Semaglutide is a GLP-1 analog with 94% sequence homology to human GLP-1.39 Similar to other GLP-1 receptor agonists, it functions by specifically attaching to and stimulating the GLP-1 receptor. This interaction prompts pancreatic beta cells to produce more insulin and reduce glucagon secretion, ultimately resulting in a decrease in blood glucose levels.40,41 The blood-glucose-lowering mechanism also lengthens gastric emptying in the early postprandial phase.42 Moreover, the drug can also activate brain GLP-1 receptors, which physiologically regulate appetite and the intake of calories.43
Common side effects of semaglutide are vomiting, nausea, diarrhea, constipation, abdominal distension, abdominal pain, headache, dizziness, fatigue, dyspepsia, eructation, hypoglycemia in patients with type 2 DM, gastroenteritis, flatulence, and gastroesophageal reflux disease.44–46 There are concerns and safeguards associated with thyroid C-cell tumors, acute pancreatitis as observed in clinical studies, sudden gallbladder disease, hypoglycemia when taken with an insulin secretagogue or insulin, sudden kidney injury, the onset of complications related to diabetic retinopathy in individuals with type 2 DM, and suicidal ideation and behavior.47
Discussion
Obesity is preventable and researchers want to explore the effects of GLP-1 in lowering body weight, body fat and improving metabolic features among pediatric participants.55 This study evaluates the efficacy of this medication as a possible treatment approach for childhood obesity. As expected, the reasons for GLP-1 usage for obesity were involved with its mechanism and GLP-1 receptor activity, especially its non-glycemic effects and its benefits regarding comorbidity related with insulin resistance.30,56,57 These have a significant impact on weight loss. Its non-glycemic effects include its impact on gastric emptying time, the suppression of inappropriate post-meal glucagon elevation, and food intake reduction; all of these directly and positively impact weight loss.58,59
Gastric emptying time has an effect on satiety. Previous studies have found a correlation between the duration of satiety and gastric emptying time for a solid meal. An increase in the gastric emptying rate might reduce the intake of satiety-enhancing food or caloric intake, and promote obesity.60,61 Therefore, the control of food or energy intake and food timing is a prominent factor in the success of weight loss therapy.62 Publications reveal that the glucagon level can induce satiety.63,64 Thus, the suppression of inappropriate post-prandial glucagon affects satiety reduction, influencing weight loss. The suppression of glucagon is the result of physiological control by insulin levels – insulin inhibits glucagon secretion.65,66 Therefore, GLP-1 which enhances insulin secretion, can lead to the effect of postprandial glucagon release and satiety.67
Turning to the insulin-related effects of GLP-1, it enhances insulin secretion and also affects insulin resistance through its effects, such as increasing the expression of glucose transporters in insulin-dependent tissues, and playing a role in lipid metabolism modulation, inflammation, and oxidative stress reduction.68–70 GLP-1 can also improve some comorbidities like polycystic ovary syndrome (PCOS).71,72 It draws attention to the study of GLP-1 and its effect on weight loss in PCOS patients, glucose tolerance, and hypothalamic obesity, as shown in the results section of this review article.
According to the results section, one main observation is that all of these studies were focused on the use of GLP-1 as a treatment for severe obesity, obesity with comorbidity, and in combination with other therapy strategies like surgery. This corresponds to the clinical recommendation in practice guidance for the treatment of childhood obesity treatment, such as the latest guidance from the American Academy of Pediatrics.
The consensus recommendation suggests that obesity weight loss pharmacotherapy can be provided to children aged 8–11 in combination with healthy behavior and lifestyle. The selection of which drug to utilize for childhood obesity may be based on medications’ indications, risks, and benefits.73 Although intensive health behavior and lifestyle (IHBLT) has the largest amount of supporting evidence and is the first-line recommendation, pharmacotherapy is employed for children and young people who require an extra treatment option to manage their obesity – especially children with life-threatening or simultaneous medical conditions, and those who are dealing with more pronounced obesity.73
According to the guidance, the evidence on the drugs used for childhood obesity treatment is limited. However, GLP-1s, such as liraglutide, exenatide, dulaglutide, and semaglutide, are mentioned in the guidance. The weight loss effects of GLP-1 are related to its mechanism of reducing appetite by decreasing the rate at which the stomach empties and by affecting specific areas in the central nervous system. Two small studies on exenatide (by weekly injection) in 8-year-old children demonstrated a lowering of BMI by 0.9 to 1.18, but there were significant negative side effects. Exenatide is currently approved in children 10 to 17 years of age with type 2 DM. In a recent randomized controlled study, administering liraglutide injections once a day was proven to be more efficient than a placebo in reducing the weight of children aged 12 or above with obesity who had not responded to lifestyle interventions. Nonetheless, the primary drawbacks were feelings of nausea and vomiting. Also, for individuals with a family history of multiple endocrine neoplasia, there is a slightly heightened risk of developing medullary thyroid cancer.73 It is obvious that pharmacotherapy can be an adjunct when behavior and lifestyle changes do not work, and drug treatment should be selected based on the cause of obesity, the presence of comorbidity, the severity of the disease and individual risk-benefit of use.
Limitations
It is important to note that the presented analysis has some limitations since the data came only from registered trials on ClinicalTrials.gov.
Conclusion
From the ClinicalTrial.gov data, it was found that GLP-1 drugs such as exenatide, semaglutide, and liraglutide were used as the pharmacotherapy option for childhood obesity. However, there is limited evidence as only eight clinical trials were conducted with a pharmacotherapy treatment for childhood obesity. It can be concluded that GLP-1 is the most common drug used for this case. The severity, comorbidity, and causes of disease are the main rationale for drug use, and drugs are usually combined with another treatment strategy such as lifestyle changes and/or surgery. The usage of GLP-1 in obesity with comorbidity and with some causes of obesity such as PCOS, hypothalamic obesity, and insulin tolerance were studied. The reason for choosing GLP-1 to treat obesity in this group is the benefit gained from the pathology related to the GLP-1 mechanism and activity.
Future Considerations
GLP-1 therapies should be used as an adjunct to lifestyle modifications, and healthcare professionals should be aware of the available GLP-1 therapies, their mechanisms of action, dosing regimens, and safety profiles. Long-term safety and efficacy data are limited, emphasizing the need for cautious monitoring and further research in this area. Future studies should focus on optimal dosages, treatment duration, and potential effects on growth and development. These guidelines aim to assist healthcare professionals in making informed decisions while considering the unique characteristics of each patient.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bays HE, Bindlish S, Clayton TL. Obesity, diabetes mellitus, and cardiometabolic risk: an Obesity Medicine Association (OMA) Clinical Practice Statement (CPS) 2023. Pillars. 2023;5:100056. doi:10.1016/J.OBPILL.2023.100056
2. Xu S, Xue Y. Pediatric obesity: causes, symptoms, prevention and treatment (review). Exp Ther Med. 2016;11:15–20. doi:10.3892/ETM.2015.2853/HTML
3. Chung ST, Onuzuruike AU, Magge SN. Cardiometabolic risk in obese children. Ann N Y Acad Sci. 2018;1411:166–183. doi:10.1111/NYAS.13602
4. Strauss RS. Childhood obesity and self-esteem. Pediatrics. 2000;105:e15–e15. doi:10.1542/PEDS.105.1.E15
5. Wardle J, Cooke L. The impact obesity on psychological well-being. Best Pract Res Clin Endocrinol Metab. 2005;19:421–440. doi:10.1016/J.BEEM.2005.04.006
6. Russell-Mayhew S, McVey G, Bardick A, Ireland A. Mental health, wellness, and childhood overweight/obesity. J Obes. 2012;2012:1–9. doi:10.1155/2012/281801
7. Lumeng JC, Gannon K, Cabral HJ, Frank DA, Zuckerman B. Association between clinically meaningful behavior problems and overweight in children. Pediatrics. 2003;112:1138–1145. doi:10.1542/PEDS.112.5.1138
8. Stice E, Presnell K, Shaw H, Rhode P. Psychological and behavioral risk factors for obesity onset in adolescent girls: a prospective study. J Consult Clin Psychol. 2005;73:195–202. doi:10.1037/0022-006X.73.2.195
9. Jezewska-Zychowicz M, Gębski J, Plichta M, Guzek D, Kosicka-Gębska M. Diet-related factors, physical activity, and weight status in Polish adults. Nutrients. 2019;12:11. doi:10.3390/NU11102532
10. Mushtaq MU, Gull S, Mushtaq K, Shahid U, Shad MA, Akram J. Dietary behaviors, physical activity and sedentary lifestyle associated with overweight and obesity, and their socio-demographic correlates, among Pakistani primary school children. Int J Behav Nutr Phys Act. 2011;8:8. doi:10.1186/1479-5868-8-130
11. Hartung D, Stadeler M, Grieshaber R, Keller S, Jahreis G. Work and diet-related risk factors of cardiovascular diseases: comparison of two occupational groups. J Occup Med Toxicol. 2010;5:1–8. doi:10.1186/1745-6673-5-4/TABLES/2
12. Costa CS, Del-Ponte B, Assunção MCF, Santos IS. Consumption of ultra-processed foods and body fat during childhood and adolescence: a systematic review. Public Health Nutr. 2018;21:148–159. doi:10.1017/S1368980017001331
13. Harb AA, Shechter A, Koch PA, St-Onge MP. Ultra-processed foods and the development of obesity in adults. Eur J Clin Nutr. 2022;2022:1–9. doi:10.1038/s41430-022-01225-z
14. Collins L, Costello RA. Glucagon-Like Peptide-1 Receptor Agonists. StatPearls; 2022.
15. Alorfi NM, Algarni AS. Clinical impact of semaglutide, a glucagon-like peptide-1 receptor agonist, on obesity management: a review. Clin Pharmacol. 2022;14:61–67. doi:10.2147/CPAA.S374741
16. Isaacs D, Prasad-Reddy L, Srivastava SB. Role of glucagon-like peptide 1 receptor agonists in management of obesity. Am J Heal Pharm. 2016;73:1493–1507. doi:10.2146/AJHP150990
17. Janez A, Muzurovic E, Stoian AP, et al. Translating results from the cardiovascular outcomes trials with glucagon-like peptide-1 receptor agonists into clinical practice: recommendations from a Eastern and Southern Europe diabetes expert group. Int J Cardiol. 2022;365:8–18. doi:10.1016/J.IJCARD.2022.07.017
18. Van Can J, Sloth B, Jensen CB, Flint A, Blaak EE, Saris WHM. Effects of the once-daily GLP-1 analog liraglutide on gastric emptying, glycemic parameters, appetite and energy metabolism in obese, non-diabetic adults. Int J Obes. 2013;38:784–793. doi:10.1038/ijo.2013.162
19. Krieger JP. Intestinal glucagon-like peptide-1 effects on food intake: physiological relevance and emerging mechanisms. Peptides. 2020;131:170342. doi:10.1016/J.PEPTIDES.2020.170342
20. Armstrong MJ, Hull D, Guo K, et al. Glucagon-like peptide 1 decreases lipotoxicity in non-alcoholic steatohepatitis. J Hepatol. 2016;64:399–408. doi:10.1016/J.JHEP.2015.08.038
21. González-García I, Milbank E, Diéguez C, López M, Contreras C. Glucagon, GLP-1 and Thermogenesis. Int J Mol Sci. 2019;20:3445. doi:10.3390/IJMS20143445
22. Jiang Y, Wang Z, Ma B, et al. GLP-1 improves adipocyte insulin sensitivity following induction of endoplasmic reticulum stress. Front Pharmacol. 2018;9:1168. doi:10.3389/FPHAR.2018.01168/BIBTEX
23. Zhang F, Chen Z, Wu D, et al. Recombinant human GLP-1 beinaglutide regulates lipid metabolism of adipose tissues in diet-induced obese mice. IScience. 2021;10:24. doi:10.1016/J.ISCI.2021.103382
24. World Health Organization. Obesity and overweight; 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
25. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
26. Bridges A, Bistas KG, Jacobs TF. Exenatide. In: StatPearls. StatPearls Publishing; 2021.
27. Latif W, Lambrinos KJ, Rodriguez R. Compare and Contrast the Glucagon-Like Peptide-1 Receptor Agonists (GLP1RAs). StatPearls; 2022.
28. Drucker DJ. Mechanisms of action and therapeutic application of glucagon-like peptide-1. Cell Metab. 2018;27:740–756. doi:10.1016/J.CMET.2018.03.001
29. Andreozzi F, Raciti GA, Nigro C, et al. The GLP-1 receptor agonists exenatide and liraglutide activate Glucose transport by an AMPK-dependent mechanism. J Transl Med. 2016;14:1–13. doi:10.1186/S12967-016-0985-7/FIGURES/8
30. Filippatos TD, Panagiotopoulou TV, Elisaf MS. Adverse effects of GLP-1 receptor agonists. Rev Diabet Stud. 2014;11:202. doi:10.1900/RDS.2014.11.202
31. Consoli A, Formoso G. Potential side effects to GLP-1 agonists: understanding their safety and tolerability. Expert Opin Drug Saf. 2015;14:207–218. doi:10.1517/14740338.2015.987122
32. Thakur U, Bhansali A, Gupta R, Rastogi A. Liraglutide augments weight loss after laparoscopic sleeve gastrectomy: a randomised, double-blind, placebo-control study. Obes Surg. 2021;31:84–92. doi:10.1007/s11695-020-04850-4
33. Meier JJ. GLP-1 receptor agonists for individualized treatment of type 2 diabetes mellitus. Nat Rev Endocrinol. 2012;8:728–742. doi:10.1038/nrendo.2012.140
34. Gentilella R, Bianchi C, Rossi A, Rotella CM. Exenatide: a review from pharmacology to clinical practice. Diabet Obes Metab. 2009;11:544–556. doi:10.1111/J.1463-1326.2008.01018.X
35. Davies MJ, Donnelly R, Barnett AH, Jones S, Nicolay C, Kilcoyne A. Exenatide compared with long-acting insulin to achieve glycaemic control with minimal weight gain in patients with type 2 diabetes: results of the helping evaluate exenatide in patients with diabetes compared with long-acting insulin (HEELA) study. Diabet Obes Metab. 2009;11:1153–1162. doi:10.1111/J.1463-1326.2009.01154.X
36. Singh G, Krauthamer M, Bjalme-Evans M. Wegovy (semaglutide): a new weight loss drug for chronic weight management. J Investig Med. 2022;70:5–13. doi:10.1136/jim-2021-001952
37. Villela R, Correa R. Semaglutide 2.4 mg: the latest GLP-1RA approved for obesity. J Investig Med. 2022;70:3–4. doi:10.1136/JIM-2021-002227
38. Sharma A, Parachuri N, Kumar N, et al. Semaglutide and the risk of diabetic retinopathy—current perspective. Eye. 2021;36(36):10–11. doi:10.1038/s41433-021-01741-5
39. Jensen L, Helleberg H, Roffel A, et al. Absorption, metabolism and excretion of the GLP-1 analogue semaglutide in humans and nonclinical species. Eur J Pharm Sci. 2017;104:31–41. doi:10.1016/J.EJPS.2017.03.020
40. Kim HS, Jung CH. Oral semaglutide, the first ingestible glucagon-like peptide-1 receptor agonist: could it be a magic bullet for type 2 diabetes? Int J Mol Sci. 2021;22:9936. doi:10.3390/IJMS22189936
41. Mahapatra MK, Karuppasamy M, Sahoo BM. Semaglutide, a glucagon like peptide-1 receptor agonist with cardiovascular benefits for management of type 2 diabetes. Rev Endocr Metab Disord. 2022;23:521–539. doi:10.1007/S11154-021-09699-1/TABLES/5
42. Dahl K, Brooks A, Almazedi F, Hoff ST, Boschini C, Bækdal TA. Oral semaglutide improves postprandial glucose and lipid metabolism, and delays gastric emptying, in subjects with type 2 diabetes. Diabet Obes Metab. 2021;23:1594–1603. doi:10.1111/DOM.14373
43. Phillips A, Clements JN. Clinical review of subcutaneous semaglutide for obesity. J Clin Pharm Ther. 2022;47:184–193. doi:10.1111/JCPT.13574
44. Holst JJ, Madsbad S. Semaglutide seems to be more effective the other GLP-1Ras. Ann Transl Med. 2017;5:251–260. doi:10.21037/ATM.2017.11.10
45. Wilding JPH, Batterham RL, Calanna S, et al. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384:989–1002. doi:10.1056/NEJMOA2032183/SUPPL_FILE/NEJMOA2032183_DATA-SHARING.PDF
46. Hepprich M, Zillig D, Florian-Reynoso MA, Donath MY, Rudofsky G. Switch-to-Semaglutide Study (STS-Study): a retrospective cohort study. Diabetes Ther. 2021;12:943–954. doi:10.1007/S13300-021-01016-Y/FIGURES/3
47. Smits MM, Van Raalte DH. Safety of semaglutide. Front Endocrinol. 2021;12:496. doi:10.3389/FENDO.2021.645563/BIBTEX
48. Bacha F. FDA approval of GLP-1 receptor agonist (liraglutide) for use in children. Lancet Child Adolesc Heal. 2019;3:595–597. doi:10.1016/S2352-4642(19)30236-6
49. Scott LJ. Liraglutide: a review of its use in the management of obesity. Drugs. 2015;75:899–910. doi:10.1007/S40265-015-0408-8/FIGURES/1
50. Jacobsen LV, Flint A, Olsen AK, Ingwersen SH. Liraglutide in type 2 diabetes mellitus: clinical pharmacokinetics and pharmacodynamics. Clin Pharmacokinet. 2016;55:657–672. doi:10.1007/S40262-015-0343-6/FIGURES/11
51. Sjöholm Å. Liraglutide therapy for type 2 diabetes: overcoming unmet needs. Pharm. 2010;3:764–781. doi:10.3390/PH3030764
52. Drucker DJ, Dritselis A, Kirkpatrick P. Liraglutide. Nat Rev Drug Discov. 2010;9:267–268. doi:10.1038/NRD3148
53. Montanya E, Sesti G. A review of efficacy and safety data regarding the use of liraglutide, a once-daily human glucagon-like peptide 1 analogue, in the treatment of type 2 diabetes mellitus. Clin Ther. 2009;31:2472–2488. doi:10.1016/j.clinthera.2009.11.034
54. Ponzani P. Long-term effectiveness and safety of liraglutide in clinical practice. Minerva Endocrinol. 2013;38:103–112.
55. Muzurović E, Polyzos SA, Mikhailidis DP, et al. Non-alcoholic fatty liver disease in children. Curr Vasc Pharmacol. 2023;21:4–25. doi:10.2174/1570161121666221118155136
56. Friedrichsen M, Breitschaft A, Tadayon S, Wizert A, Skovgaard D. The effect of semaglutide 2.4 mg once weekly on energy intake, appetite, control of eating, and gastric emptying in adults with obesity. Diabet Obes Metab. 2021;23:754–762. doi:10.1111/DOM.14280
57. Baggio LL, Drucker DJ. Glucagon-like peptide-1 receptor co-agonists for treating metabolic disease. Mol Metab. 2021;46:101090. doi:10.1016/J.MOLMET.2020.101090
58. Paternoster S, Falasca M. Dissecting the physiology and pathophysiology of glucagon-like peptide-1. Front Endocrinol. 2018;2018:584. doi:10.3389/FENDO.2018.00584
59. Christou GA, Katsiki N, Blundell J, Fruhbeck G, Kiortsis DN. Semaglutide as a promising antiobesity drug. Obes Rev. 2019;20:805–815. doi:10.1111/OBR.12839
60. Carbannel F, Lémann M, Rambaud JC, Mundler O, Jian R. Effect of the energy density of a solid-liquid meal on gastric emptying and satiety. Am J Clin Nutr. 1994;60:307–311. doi:10.1093/AJCN/60.3.307
61. Verdich C, Madsen JL, Toubro S, Buemann B, Holst JJ, Astrup A. Effect of obesity and major weight reduction on gastric emptying. Int J Obes Relat Metab Disord. 2000;24:899–905. doi:10.1038/SJ.IJO.0801250
62. Garaulet M, Gómez-Abellán P, Alburquerque-Béjar JJ, Lee YC, Ordovás JM, Scheer FA. Timing of food intake predicts weight loss effectiveness. Int J Obes. 2013;37:604–611. doi:10.1038/IJO.2012.229
63. Al-Massadi O, Fernø J, Diéguez C, Nogueiras R, Quiñones M. Glucagon control on food intake and energy balance. Int J Mol Sci. 2019;20:3905. doi:10.3390/IJMS20163905
64. Geary N. Glucagon and the control of appetite. In: Glucagon III. Berlin, Heidelberg: Springer Berlin Heidelberg; 1996:223–238.
65. Maruyama H, Hisatomi A, Orci L, Grodsky GM, Unger RH. Insulin within islets is a physiologic glucagon release inhibitor. J Clin Invest. 1984;74:2296. doi:10.1172/JCI111658
66. Kaneko K, Shirotani T, Araki E, et al. Insulin inhibits glucagon secretion by the activation of PI3-kinase in In-R1-G9 cells. Diabetes Res Clin Pract. 1999;44:83–92. doi:10.1016/S0168-8227(99)00021-2
67. Llewellyn DC, Logan Ellis H, Aylwin SJB, et al. The efficacy of GLP-1RAs for the management of postprandial hypoglycemia following bariatric surgery: a systematic review. Obesity. 2023;31:20–30. doi:10.1002/OBY.23600
68. Sandoval D, Sisley SR. Brain GLP-1 and Insulin Sensitivity. Mol Cell Endocrinol. 2015;418(Pt 1):27. doi:10.1016/J.MCE.2015.02.017
69. Müller TD, Finan B, Bloom SR, et al. Glucagon-like peptide 1 (GLP-1). Mol Metab. 2019;30:72–130. doi:10.1016/J.MOLMET.2019.09.010
70. Kjems LL, Holst JJ, Vølund A, Madsbad S. The influence of GLP-1 on glucose-stimulated insulin secretion effects on β-cell sensitivity in type 2 and nondiabetic subjects. Diabetes. 2003;52:380–386. doi:10.2337/DIABETES.52.2.380
71. Siamashvili M, Davis SN. Update on the effects of GLP-1 receptor agonists for the treatment of polycystic ovary syndrome. Expert Rev Clin Pharmacol. 2021;14:1081–1089. doi:10.1080/17512433.2021.1933433
72. Bednarz K, Kowalczyk K, Cwynar M, et al. The role of Glp-1 receptor agonists in insulin resistance with concomitant obesity treatment in polycystic ovary syndrome. Int J Mol Sci. 2022;23:4334. doi:10.3390/IJMS23084334
73. Hampl SE, Hassink SG, Skinner AC, et al. Clinical practice guideline for the evaluation and treatment of children and adolescents with obesity. Pediatrics. 2023:151. doi:10.1542/PEDS.2022-060640/190443
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.