Back to Journals » Clinical Ophthalmology » Volume 20
US Retina Specialists’ Preferences for Geographic Atrophy Treatment
Authors Csaky K, Pepio AM, Thomas C ![]() , Levitan B
, Levitan B ![]() , Garg S, Tran N, Irony I, Krucien N, Doldos A, Whitty JA
, Garg S, Tran N, Irony I, Krucien N, Doldos A, Whitty JA ![]()
Received 9 January 2026
Accepted for publication 26 May 2026
Published 9 June 2026 Volume 2026:20 594882
DOI https://doi.org/10.2147/OPTH.S594882
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yousef Fouad
Karl Csaky,1 Anthony M Pepio,2 Caitlin Thomas,3 Bennett Levitan,4 Seema Garg,5 Nguyet Tran,4 Ilan Irony,6 Nicolas Krucien,3 Anastasia Doldos,3 Jennifer A Whitty3
1Ophthalmology Department, Retina Foundation of the Southwest, Dallas, TX, USA; 2Research & Development, Johnson & Johnson, Vancouver, British Columbia, Canada; 3PPD Evidera Patient-Centered Research, Thermo Fisher Scientific, London, UK; 4Global Epidemiology, Johnson & Johnson, Titusville, NJ, USA; 5Research and Development; Johnson & Johnson, Durham, NC, USA; 6Global Regulatory Affairs, Johnson & Johnson, Raritan, NJ, USA
Correspondence: Bennett Levitan, Global Epidemiology, Johnson & Johnson, Titusville, NJ, USA, Email [email protected]
Purpose: Two complement inhibitors are US-approved for geographic atrophy (GA) and other treatments are in development. We present the first quantitative assessment of retina specialists’ (RS) preferences for GA treatment. We explored how GA treatment characteristics affect RS’ preferences, the trade-offs RS are willing to make between them, and whether this varies across patient profiles.
Methods: US-based RS with ≥ 7 years of clinical experience and ≥ 50 patients with GA in the previous year selected their best and second-best treatment recommendations for specific patient profiles in 12 tasks showing two hypothetical treatment options and no treatment (best-best discrete choice experiment, BB-DCE). Treatment characteristics comprised lesion growth rate reduction, three treatment risks (mild-to-moderate uveitis, progression to wet age-related macular degeneration [AMD], and retinal vasculitis), and intravitreal injection frequency (every month, every other month, and one-time [gene therapy]). Patient profiles were defined by GA lesion location and visual acuity. Preferences were evaluated using a mixed-logit model. Relative importance of each characteristic and trade-offs were analyzed.
Results: Of 166 RS, 83.1% had experience treating GA with complement inhibitors. Improving lesion growth rate reduction from 10% to 50% had the greatest impact (almost half of decision-making). Among risks, reducing the chance of progressing to wet AMD from 15% to 1% had the greatest impact (~20% of decision-making). All else equal, RS preferred a one-time over monthly injection(s). Risk tolerance increased with higher lesion growth rate reduction and, to a lesser extent, with less frequent injections; risk tolerance was highest when considering patients with foveal-threatening GA lesions.
Conclusion: Across patient profiles, RS prioritized lesion growth rate reduction over risks; intravitreal injection frequency was the least important. However, RS were more risk-tolerant with patients with foveal-threatening lesions. RS would tolerate slightly higher risks for a one-time over monthly injection(s) if lesion growth rate reduction was comparable.
Keywords: geographic atrophy, acute macular degeneration, retina specialists, preferences, discrete choice experiment
Introduction
Geographic atrophy (GA) is an advanced form of dry age-related macular degeneration (AMD) characterized by the development of atrophic lesions in the macula, resulting in retinal cell loss.1,2 GA often starts in the perifoveal region and may include the fovea, which would cause central vision loss.1,2 GA is estimated to affect approximately five million people globally and one million in the US.3,4 People with GA often have difficulties reading, recognizing faces, or performing daily activities that require central vision, and they may experience fear, frustration, and anxiety.5–7
Dysregulation of the complement cascade is a leading contributor to GA pathogenesis.2,8 GA treatments are currently available in the US (pegcetacoplan and avacincaptad pegol9,10) and Australia (pegcetacoplan only11) as intravitreal injections: pegcetacoplan is a complement C3 inhibitor approved for dosing every 25–60 days12 and avacincaptad pegol is a complement C5 inhibitor approved for monthly dosing.10 Trials supporting approval of pegcetacoplan showed a GA lesion growth rate reduction at 24 months by 16–18% with injections every other month and by 19–22% with monthly injections.13 Avacincaptad pegol monthly injections reduced lesion growth rate by 14–27% at 12 months.14,15 However, both treatments are associated with an increased risk of progression to neovascular (wet) AMD and real-world use of pegcetacoplan identified cases of occlusive retinal vasculitis and irreversible vision loss.16,17 Further, each intravitreal injection has a risk of endophthalmitis,9,10 and the requirement for lifelong injections may compromise long-term adherence,18 potentially impacting efficacy.
Potential GA therapies differ in key characteristics, such as level of efficacy, adverse reaction risks, and injection frequency (eg., ocular gene therapies are being investigated as one-time injections18–21). Differences may impact retina specialists’ (RS) treatment preferences and the trade-offs they are willing to make when prescribing treatment for GA. Such insights can inform the acceptability of GA treatments to RS and identify factors that might impact risk tolerance and the benefit-risk balance. Since not all patients may be offered GA treatments despite approvals, this study aimed to understand drivers of clinicians’ treatment preferences and decision-making. To our knowledge, no study of RS preferences exists. We describe the results of a preference study evaluating how GA treatment-related characteristics impact RS’ preferences and the trade-offs RS are willing to make during treatment decisions, as well as whether these vary depending on patient characteristics.
Methods
Overall Study Design
RS completed a best-best discrete choice experiment (BB-DCE) survey, a type of survey increasingly used to assess the relative importance of treatment benefits and risks to patients, physicians, and other stakeholders.22,23 In BB-DCEs, participants indicate their most preferred and second most preferred treatment options from >2 alternatives. To ensure the study accounted for all key patient and treatment characteristics that RS consider during treatment decision-making, its design was informed by a targeted literature review (TLR) and clinical data review, qualitative interviews, a workshop with internal and external experts, cognitive pilot interviews, and guidance from RS (including KC) involved in study design and throughout the study process (Supplemental Figure 1).
Institutional Review Board (IRB)/Ethics Committee approval was obtained (Salus IRB, study number: 23201). The study adhered to the tenets of the Declaration of Helsinki and was conducted in accordance with International Council on Harmonisation guidelines, the Health Insurance Portability and Accountability Act, and all local laws and regulations. The survey was self-administered online with no time limit for completion (estimated duration ≈ 30 min).
Participants
Eligible participants were RS practicing in the US with ≥7 years of clinical experience with ≥50 patients with GA in the previous year. Participants were recruited by a third-party vendor (Global Perspectives) via physician panels and databases. To reach a minimum target sample size (n = 150) consistent with previous healthcare discrete choice experiments,24,25 n = 200 RS were targeted for recruitment to allow for subsequent exclusions based on predefined data quality criteria (Supplemental Methods). RS who participated in qualitative/cognitive pilot interviews were not eligible for the BB-DCE. All participants provided informed consent and received compensation for their time.
Development of Treatment Characteristics and Levels
Targeted Literature Review and Clinical Data Review
The TLR synthesized existing qualitative and quantitative evidence on preferences related to vision disorder treatments to identify potentially relevant characteristics.7,26–44 TLR insights informed the design of a semi-structured interview guide for qualitative interviews and of the BB-DCE (Supplemental Table 1 and Supplemental Methods).
Qualitative Interviews
Qualitative interviews (lasting approximately 60 minutes) were conducted with n = 15 RS between January and February 2023 to explore key treatment characteristics and other aspects of therapies suitable for inclusion in the BB-DCE (Supplemental Methods).
Treatment Characteristic Selection and Refinement
Initial characteristics were selected based on the TLR and qualitative interviews, then refined based on 60-minute cognitive pilot interviews conducted with five RS to test the relevance, completeness, and tradability of draft characteristics and their levels.26
The primary efficacy endpoint used in GA trials, lesion growth rate reduction, was selected as a benefit characteristic. Functional changes in vision were not used since currently available evidence for RS decision-making is based on structural endpoints.
Treatment risks of mild-to-moderate uveitis, progression to wet AMD, and retinal vasculitis were the key risks identified from the clinical evidence review and interviews, and intravitreal injection frequency was included to account for currently approved vs. gene therapy treatments. A timeframe of 18 months was used for these characteristics to align with the duration of current and the earliest realistic point that lesion growth rate signals a change in the patient’s trajectory.
Treatment characteristic levels, chosen to cover clinically relevant ranges for current and near-future treatments, were based on Phase 3 clinical trial data of pegcetacoplan and avacincaptad pegol and potential outcomes for gene therapies in development.14,25 Levels of retinal vasculitis risk were initially 0%, 0.001%, 0.01%, and 0.1%; this range was informed by real-world occurrences of retinal vasculitis with a complement inhibitor (~0.01%). After analyzing data from the first 40 RS, the 0.001% level was removed and a 0.02% level was added, since RS did not significantly differentiate between the levels of 0% and 0.001%.
Given the importance of lesion location and visual acuity (Snellen VA) in both eyes during the interviews, these patient characteristics were also incorporated. To avoid an excessive burden on RS, VA in the affected eye and lesion location were defined in fixed combinations (hereinafter referred to by lesion location), while VA in the non-treated eye varied independently. Lesion location levels were foveal threatening (FT), non-foveal threatening (NFT), or extrafoveal (EF). Based on clinical input, we selected two levels of VA for the untreated eye to represent good (20/20) and poor (20/200) vision. These choices provided the ability to assess the impact of key patient characteristics on RS preferences with six diverse patient profiles, rather than the single “typical” patient often used in physician preference studies (Supplemental Table 2).
The final characteristics and levels are shown in Table 1, and full definitions are given in Supplemental Table 3.
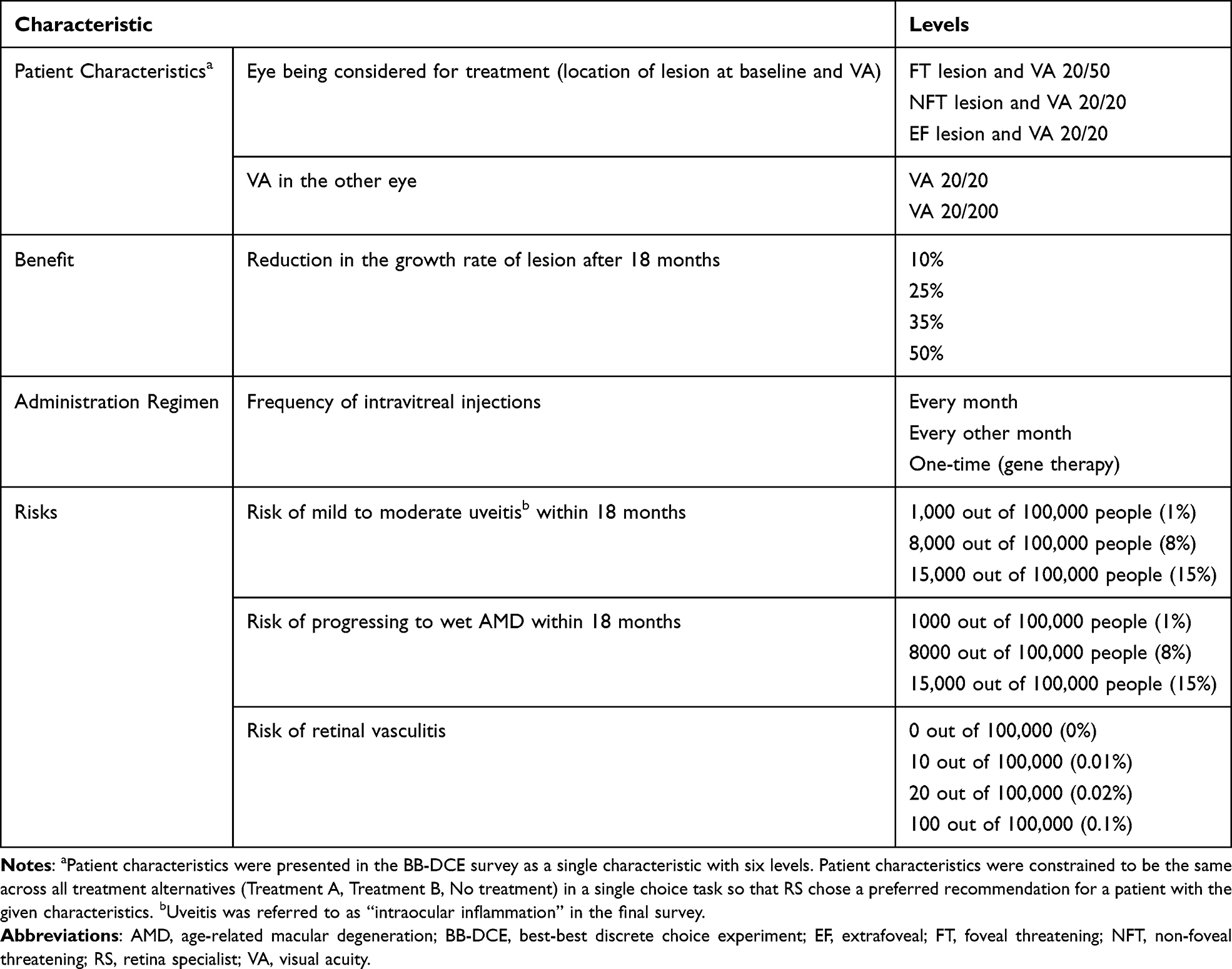 |
Table 1 Treatment Characteristics and Levels Included in the BB-DCE |
Survey Design
Survey design followed published good practice.45 At the start of the survey, RS reviewed information about the six patient profiles and characteristics, then they were oriented to the survey choice tasks. Within each task, RS were asked to select their best and second-best recommendation between two hypothetical treatment options (“Treatment A” or “Treatment B”) and “No treatment”, with the characteristic levels varying between tasks (Figure 1). A BB-DCE design46,47 was used because it captures more information per choice task than the more common single-best DCE,23 which would generate no trade-off insights if RS often selected “No treatment” (opt-out). A BB-DCE allows RS to select no treatment while generating trade-off insights for their second-best choice. As a constraint, 10% and 50% lesion growth rate reduction were not presented in the same task to avoid this characteristic dominating decision-making.
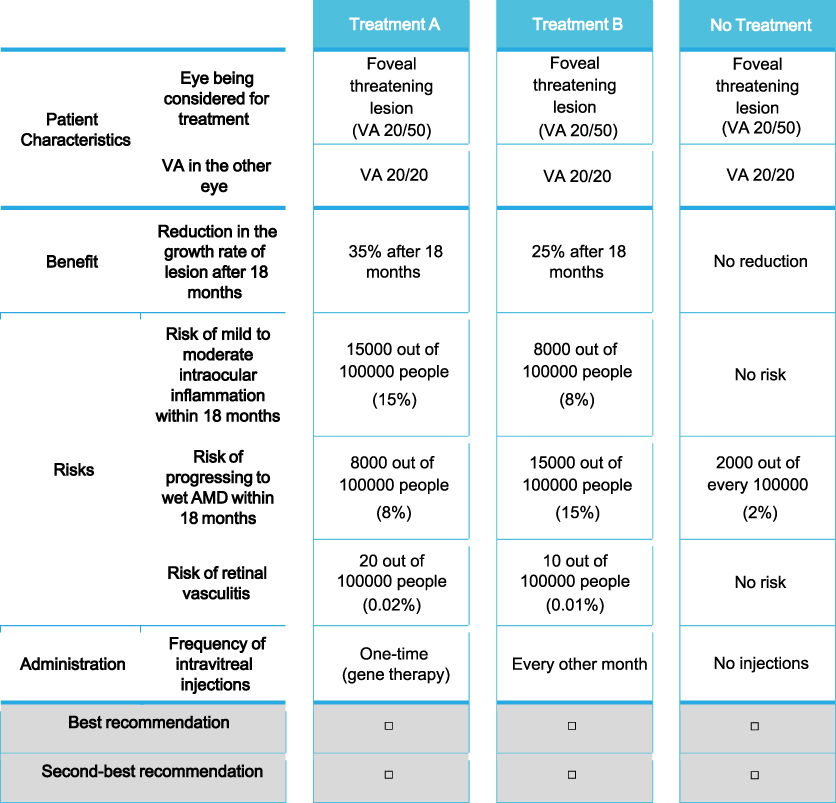 |
Figure 1 BB-DCE Choice Task. Example BB-DCE choice task used in the study. Abbreviations: AMD, age-related macular degeneration; BB-DCE, best-best discrete choice experiment; VA, visual acuity. |
Within each task, the patient profile was fixed so that RS made treatment recommendations for the defined patient profile. The levels within the “No treatment” alternative were constant for all tasks; given there is a natural risk of progression to wet AMD without treatment,13 respondents were informed that “No treatment” included a 2% risk within 18 months. Respondents were asked to only consider the selected characteristics in their decision-making.
RS also completed four non-experimental choice tasks: one practice task (where they were familiarized with the format of the choice tasks), one repeated-choice task to assess choice stability (where the third choice task they completed was repeated later), and two dominance tasks to assess engagement in the survey (where one treatment had superior lesion growth rate reduction and lower risks than the other, with the same injection frequency). These tasks were used to assess data quality/validity (Supplemental Methods). The selected characteristics and levels were combined into three blocks of 12 tasks using a D-efficient design generated with Ngene® software version 1.2.1 (ChoiceMetrix, Sydney, Australia). Order of tasks was randomized across participants to avoid potential ordering effects on decision-making.
Finally, RS were asked questions about their demographics and clinical experience, perspectives on gene therapy, potential challenges scheduling patients depending on injection frequency, and willingness to take risks.48,49
A copy of the full survey is available in the Supplemental Methods.
Data Quality Assessment
As pre-specified, RS were excluded from the analyses if they failed both dominance tasks, completed all BB-DCE choice tasks in <2 minutes (unless they systematically selected no treatment), or always selected “Treatment A” or “Treatment B” as their first-best recommendation (Supplemental Methods).
Statistical Analysis
BB-DCE data were analyzed using a mixed-logit (MXL) model that estimated how changes in each treatment characteristic affected RS’ choices, while accounting for between-subject heterogeneity in preferences.50 The MXL model was estimated using the Apollo package (version 0.3.3) in R software (version 4.4).51
Model estimates were then used to compute relative attribute importance (RAI) to assess the influence of a treatment characteristic on treatment choices, relative to all other characteristics across the included level ranges.52 Measures of minimum acceptable benefit and simultaneous maximum acceptable risk thresholds were also analyzed.53
Finally, heterogeneity in RS’ preferences associated with RS demographic and clinical experience variables was assessed using interacted MXL models. Additional details are provided in Supplemental Methods.
Results
Participants
The main survey was conducted between March and July 2024. One hundred and ninety-eight RS completed the survey and 166 were included in the analyses (mean age 48.9 [standard deviation (SD) = 9.2] years) following pre-specified data validity assessments. Most were male (n = 131, 78.9%) and either owners of a private practice (n = 80, 48.2%) or salaried employees (n = 75, 45.2%). Approximately half worked in a practice located in an urban (n = 96, 57.8%) or suburban (n = 82, 49.4%) area; six (3.6%) reported working in a rural area. RS had been practicing medicine for a median of 16 years (range: 7–40) and had managed a median of 300 patients (range: 55–1000) with GA in the previous year. Most RS reported experience prescribing pegcetacoplan (n = 127, 76.5%) or avacincaptad pegol (n = 97, 58.4%) for GA; n = 28 (16.9%) had prescribed neither. Two-thirds of the sample did not have experience being an investigator on a GA treatment trial (n = 124, 74.7%) (Supplemental Figure 2 and Supplemental Table 4).
Data Quality and Validity
Most participants passed both dominance tasks (n = 156, 94.0%) and provided consistent answers to the repeated-choice task (n = 131, 78.9%) and made choices that were not dominated by any individual treatment characteristic (n = 149, 89.8%). The median survey response time was 21.8 (interquartile range: 14.4–44.9) minutes (Supplemental Table 5).
Perceptions and Attitudes
While eight RS (4.8%) always chose no treatment in the choice tasks, 55 (33.1%) never chose no treatment; the remainder mixed decisions between treatment and no treatment based on the treatment and patient profiles presented.
Most RS reported a patient who had a FT lesion and VA of 20/200 in the other eye to be the most important to treat (n = 133, 80.1%). Willingness to prescribe differed significantly across patient profiles, with the proportion of treatment A/B selection (vs. no treatment) ranging from 56.3% to 87.1% (Supplemental Tables 5–7).
On average, on a 10-point scale (0 = “not challenging” to 10 = “very challenging”), RS rated the challenge of scheduling patients as 2.9 (SD = 2.4) for a one-time injection, 4.3 (SD = 2.6) for an injection every other month, and 5.7 (SD = 3.0) for an injection every month. Most RS reported being willing to offer gene therapy to patients with GA (n = 133, 80.1%). On average, RS rated their willingness to take risks as 5.6 (SD = 2.3) on a 10-point scale (0 = “not willing at all to take risks” and 10 = “very willing to take risks”); risk tolerance did not differ significantly with willingness to offer gene therapy (Supplemental Table 8).
Preferences for Treatment Characteristics
On average, RS valued increasing lesion growth rate reduction most when considering a patient with an FT lesion and 20/200 VA in the other eye (RAI 52.1%) and least when considering a patient with an EF lesion and 20/20 VA in the other eye (RAI 40.9%). The importance of lesion growth rate reduction was more influenced by GA lesion location than VA in the other eye, although both were relevant (Figures 2–3, Supplemental Table 9 and Supplemental Figure 3). These results align with the descriptive responses regarding which patients RS deemed most important to treat (Supplemental Table 6).
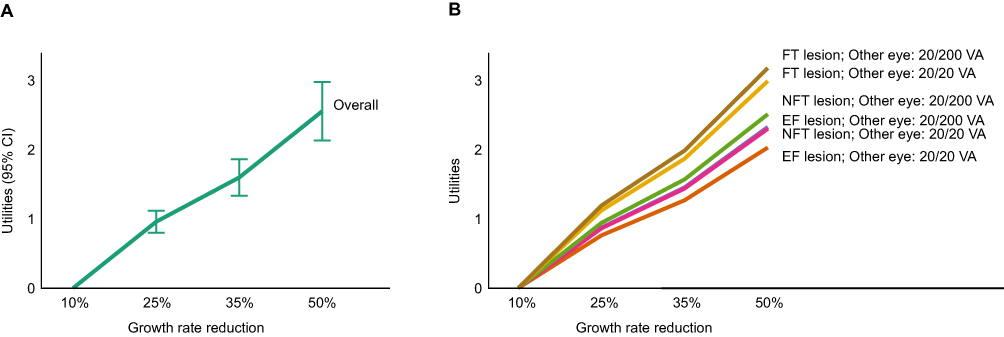 |
Figure 2 Impact of Lesion Growth Rate Reduction on RS Preferences, Overall and by Patient Profile (MXL Model). Impact of increasing lesion growth rate reduction on RS preferences overall (A) and by patient profile (B). The larger the utility (vertical distance), the more influential growth rate reduction is on decision-making. Abbreviations: CI, confidence interval; EF, extrafoveal; FT, foveal threatening; MXL, mixed-logit; NFT, non-foveal threatening; RS, retina specialist; VA, visual acuity. |
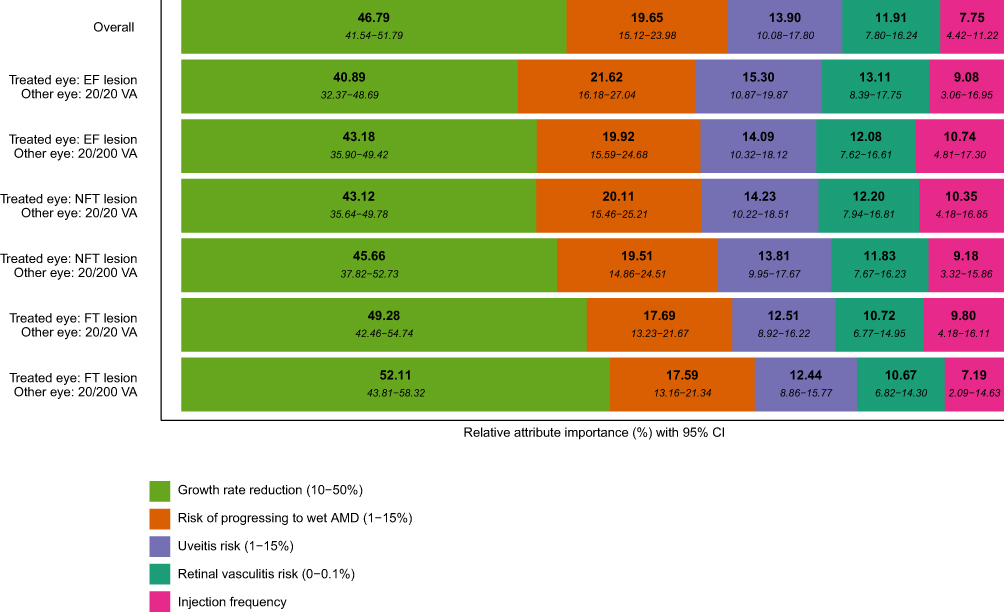 |
Figure 3 RAI (Overall and by Patient Profile). RAI values represent the relative importance that RS placed on each treatment characteristic across the level ranges included in the BB-DCE. 95% CI ranges are shown in italics under each RAI value. The level range for each characteristic is shown in the key. Higher RAI values indicate that changes in that characteristic, across the full level range, contribute a higher amount to treatment decision-making. Abbreviations: AMD, age-related macular degeneration; CI, confidence interval; EF, extrafoveal; FT, foveal threatening; NFT, non-foveal threatening; RAI, relative attribute importance; RS, retina specialists; VA, visual acuity. |
For all patient profiles, improving lesion growth rate reduction from 10% to 50% had the largest impact on RS’ treatment preferences (RAI 40.9–52.1%) (Figure 3 and Supplemental Figure 3). Among the three risks, over the ranges assessed, the risk of progressing to wet AMD had the largest impact on RS’ treatment choices (RAI 17.6–21.6%), followed by risks of mild-to-moderate uveitis (RAI 12.4–15.3%) and retinal vasculitis (RAI 10.7–13.1%). Although RS preferred to avoid retinal vasculitis, they did not significantly differentiate between a 0.1% and 0.02% retinal vasculitis risk. The higher relative importance of risks for patients with EF lesions suggests that RS were slightly more risk-averse when making treatment decisions for these patients, compared with those with FT lesions, for whom RS placed more importance on lesion growth rate (Figure 3).
Finally, injection frequency impacted RS’ treatment preferences, although this was the least important characteristic to RS regardless of patient profile (RAI 7.2–10.7%). Although RS preferred a one-time injection to an injection every month on average, preference differences were not statistically significant for all patient profiles. On average, for one profile (EF lesion and 20/200 VA in the other eye), RS preferred an injection every other month vs. one-time; however, this was not significant (p = 0.166; two-sided z-test) (Figure 3 and Supplemental Table 9).
Willingness to Trade-off Between Treatment Characteristics
Across all patient profiles, RS were willing to tolerate considerably higher side effect risks for an increase in lesion growth rate reduction, as shown by the shift in the risk tolerance curve from 10% lesion growth rate reduction in Figure 4A to 35% in Figure 4B (details in Supplemental Figure 4 and Supplemental Table 10). Each line represents the maximum acceptable combination of risks averaged over all patient profiles for a given lesion growth rate reduction and injection frequency, with retinal vasculitis risk fixed at 0.01%. Values below and to the left of a line are acceptable; values above and to the right are not. For example, on average, for a 10% reduction in lesion growth rate with a one-time injection, RS were willing to tolerate a maximum of 9.4% wet AMD risk, a 12.8% mild-to-moderate uveitis risk, or various combinations below the line. For a 35% reduction in lesion growth rate with a one-time injection, RS were willing to tolerate a 30.2% wet AMD risk, a 42.2% mild-to-moderate uveitis risk or a wider range of combinations. Since the maximum risks included in the study were 15%, maximum acceptable risks above this level should be interpreted with caution.
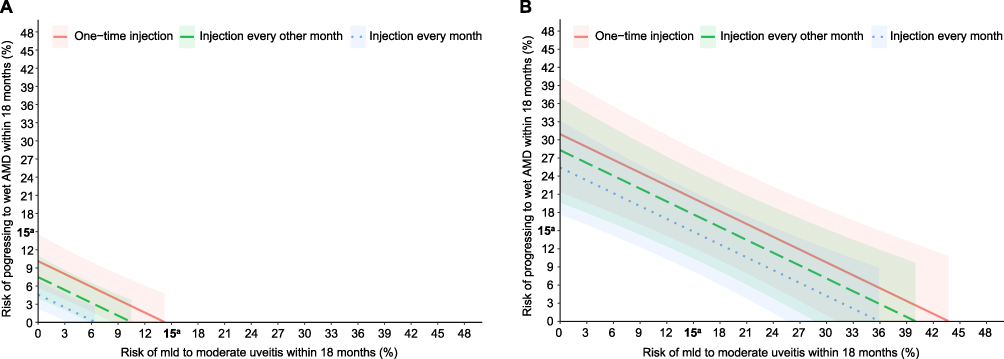 |
Figure 4 Risk Tolerance (Maximum Acceptable Risk). Curves showing RS tolerance for the combined risks of progressing to wet AMD and mild to moderate uveitis within 18 months per intravitreal injection frequency (one-time, every other month, every month), based on a 10% (A) or a 35% reduction (B) in lesion growth rate. Values to the left of each line represent acceptable combinations of risks for that injection frequency. Shaded areas represent the 95% CI for each injection frequency. Both scenarios include a 0.01% risk of retinal vasculitis. Numerical values for the x-axis and y-axis intercepts are provided in Supplemental Table 10. aMaximum value included in the study. Abbreviations: AMD, age-related macular degeneration; CI., confidence interval; RS, retina specialist. |
On average, RS were willing to tolerate higher adverse reaction risks for less frequent injections, although to a much lesser extent than for increased lesion growth rate reduction. Conversely, RS were willing to accept more frequent intravitreal injections in exchange for reduction in these risks (Figure 4, Supplemental Figure 4 and Supplemental Tables 10–11).
Although not all differences were statistically significant, the acceptable combinations of risk for mild-to-moderate uveitis and for progression to wet AMD were on average highest for a single injection and lowest for a monthly injection.
Preference Heterogeneity
Overall, RS’ treatment preferences were similar based on their demographics and clinical experience, including gender, years of experience, practice location and setting, and experience in GA clinical trials. Lesion growth rate reduction had the largest impact on treatment preferences for all RS subgroups (RAI 39.3–55.7%). While some differences in RAI were found, most notably for location of clinical practice, none reached statistical significance at the 5% level (Supplemental Figure 5).
Discussion
We assessed the characteristics that influence RS treatment preferences in GA and the trade-offs they are willing to make, considering currently available evidence on possible treatments. Over the ranges used, preferences were most influenced by lesion growth rate reduction, regardless of lesion location or VA in the other eye. By contrast, intravitreal injection frequency was the least important characteristic to RS, and less influential on RS’ treatment decision-making than other characteristics, possibly because RS consider intravitreal injections a standard office-based procedure commonly used in wet AMD. However, for comparable lesion growth rate reduction, RS preferred a one-time injection to a monthly injection, even with some additional risks.
Among the three risks and level ranges included, RS were most concerned about risk of progressing to wet AMD, followed by risks of mild-to-moderate uveitis and retinal vasculitis. While on average RS were more likely to choose a treatment with a lower vasculitis risk, they were much more sensitive to reducing the risk from 0.02% to either 0.001% or 0% than they were to reducing the risk from 0.1% to 0.02%. This may be because any risk over 0.02% was deemed to be unacceptable. The value that RS placed on safety versus other treatment characteristics varied by patient type: RS were more risk-averse, and more likely to select no treatment, for patients with an EF/NFT lesion with 20/20 VA in the other eye; by contrast, RS were more risk-tolerant when considering patients with FT lesions, for whom they placed greater value on lesion growth rate reduction and lower value on avoiding risks, regardless of the VA in the patient’s other eye.
While average RS’ risk tolerance increased with less frequent injections (assuming comparable lesion growth rate reduction), the most notable increase was for higher lesion growth rate reduction; this is consistent with lesion growth rate reduction being the most valued treatment characteristic.
Potential study limitations include the fact that, as with all stated preference methods, RS’ responses to hypothetical choice tasks may not reflect their actual decisions in a clinical setting (hypothetical bias).54 However, a published review of DCE studies suggests that carefully designed preference instruments may reasonably predict real-world choices;55 the rigorous approach taken to develop and pretest the BB-DCE survey in this study (ie., informed by a TLR, qualitative interviews [n = 15 RS], pilot-testing interviews [n = 5 RS], and internal/external RS input) mitigated potential hypothetical bias. Despite ongoing research, no new treatments have been approved since this study was conducted, and preferences are not expected to have changed over this timeframe. Sample demographics might impact preferences, and preferences among study participants may differ from the general RS population or from RS who declined to participate. Although preferences were not found to be significantly affected by RS’ characteristics (eg., experience being an investigator in a GA trial, practice location, practice setting, or employment type), other RS characteristics for which data were not collected might influence RS’ perspectives. This BB-DCE included lesion growth rate reduction as the measure of efficacy, which does not fully reflection vision functional outcomes. While anatomical/structural measures are accepted trial endpoints to the US FDA and other regulatory authorities,56 they may not be sufficient in real-world settings, and the field (including European regulators) is evolving towards functional measures. Future preference research might be able to use functional efficacy measures if GA treatments show such benefits for approval. Functional changes in vision were not used here since currently available evidence for RS decision-making is based on structural endpoints, but they are more suitable for patient preference studies. Preference research is increasingly encouraged by regulators;57–59 while regulators focus on patient preferences, understanding physician preferences supports shared decision-making by clarifying how clinicians interpret evidence and trade-offs and helps anticipate treatment patterns across patient subgroups. Considered alongside patient preferences, this enables more transparent, patient-centered decisions.
A strength of this study is that it accounted for variability in patient profiles, which is not standard practise in physician preference studies but allows for more clinically realistic and relevant results.60 However, due to methods-related limitations, and to reduce respondent burden and impact on sample size requirements, it was not possible to include a large number of patient profiles, and six key patient profiles were included. While patients may experience different VA for a given lesion location,61 here RS were asked to consider a patient with a specific VA for each lesion location. The use of fixed combinations of patient characteristics does not hinder their interpretation in the context of the study, but it may reduce generalizability to other patient profiles not assessed within the study. We assume that RS’ decision-making when asked about the most important patient to treat was based on available treatment options, so changes in the available options may impact the most important patients to treat. Additionally, since this study’s goal was to assess acceptable benefit-risk trade-offs without confounding by cost, RS were asked not to consider cost/insurance coverage. However, once a treatment is deemed to have a favorable benefit-risk profile, we recognize that cost and insurance coverage may influence physician decision-making and patient access in clinical practice. While RS were asked not to consider cost/insurance or issues related to scheduling/managing their practice due to repeated injections, we cannot confirm whether they made any such assumptions, and the study did not specify whether gene therapy may impact a patient’s ability to receive future treatments.
Conclusions
This is the first study to quantitatively assess RS’ preferences for treating GA and their perspectives on ocular gene therapies for GA. Although the findings should be interpreted in the context of preference research, these results may inform the acceptability of GA treatments to RS and identify factors that might impact risk tolerance and the benefit-risk balance. RS in this study were most likely to treat patients with FT lesions and poor VA in the other eye, and they would tolerate higher risks with these patients than with others, for a given improvement in lesion growth rate reduction. Over the level ranges considered, risks (particularly wet AMD) and intravitreal injection frequency had a relevant but much smaller impact on decision-making compared with lesion growth rate reduction, which was the main driver of treatment choice. Overall, RS were willing to tolerate higher side effect risks for increased lesion growth rate reduction or less frequent intravitreal injections (assuming comparable lesion growth rate reduction). Most RS would be willing to offer ocular gene therapy to patients with GA, but the advantage of less frequent intravitreal injections would only be relevant if lesion growth rate reduction was comparable to that of approved treatments. When clinical trial data for gene therapies become available, this study may support assessing whether RS consider observed reductions in the lesion growth rate to outweigh observed risks of wet AMD and uveitis and the need for a one-time intravitreal injection. Future studies could also explore patients’ preferences for GA treatment and whether they differ from RS’ preferences.
Declarations
Institutional Review Board (IRB)/Ethics Committee approval was obtained (Salus IRB, study number: 23201). The study adhered to the tenets of the Declaration of Helsinki and was conducted in accordance with International Council on Harmonisation guidelines, the Health Insurance Portability and Accountability Act, and all local laws and regulations. All participants provided informed consent and received compensation for their time.
Abbreviations
AMD, age-related macular degeneration; BB-DCE, best-best discrete choice experiment; CI, confidence interval; DCE, discrete choice experiment; EF, extrafoveal; FT, foveal threatening; GA, geographic atrophy; MXL, mixed-logit; NFT, non-foveal threatening; RAI, relative attribute importance; RS, retina specialists; SD, standard deviation; TLR, targeted literature review; VA, visual acuity.
Data Sharing Statement
The datasets analyzed during the current study will not be made publicly available as consent was not provided for third party analysis of the data.
Acknowledgments
The authors thank the RS who participated in the study and the steering committee members for their input. Medical writing was provided by Pablo Izquierdo, PhD, and Surayya Taranum, PhD, CMPP (PPD clinical research business of Thermo Fisher Scientific) in accordance with Good Publication Practice guidelines and was funded by Janssen Research & Development, LLC.
Funding
This study was funded by Janssen Research & Development, LLC. The sponsor participated in the study conceptualization, design and conduct; interpretation of the data; and preparation, review, and approval of the manuscript.
Disclosure
Parts of the work described in this paper were presented as a poster entitled “US retina specialists’ preferences for treating geographic atrophy with gene therapy and complement inhibitors” at the 2025 Association for Research in Vision and Ophthalmology annual meeting. The poster’s abstract was published in Investigative Ophthalmology & Visual Science June 2025, Vol. 66, 3773: https://iovs.arvojournals.org/article.aspx?articleid=2804077.
KC has provided data and safety monitoring for Adverum Biotechnologies and has served as a consultant for Abbvie, Annexon Biosciences, Cognition Therapeutics, EyeBio, F. Hoffman-La Roche AG, Genentech Inc., Astellas, Johnson & Johnson Health Care Systems Inc., Merck, NGM Biopharmaceuticals, Novartis, Regeneron Pharmaceuticals Inc., and Boehringer Ingelheim Pharmaceuticals. AP, BL, SG, NT, and II are employed by Janssen Research & Development, LLC. BL and NT are stockholders in Johnson & Johnson; BL is also a stockholder in a portfolio that at times includes other pharmaceutical and healthcare-related companies. CT, NK, AD, and JAW are employed by PPD Evidera Patient-Centered Research (part of Thermo Fisher Scientific), which was funded by Janssen Research & Development, LLC to undertake the study. CT, NK and JAW are minor shareholders of Thermo Fisher Scientific.
The authors report no other conflicts of interest in this work.
References
1. Fleckenstein M, Mitchell P, Freund KB, et al. The progression of geographic atrophy secondary to age-related macular degeneration. Ophthalmology. 2018;125(3):369–13. doi:10.1016/j.ophtha.2017.08.038
2. Bakri SJ, Bektas M, Sharp D, Luo R, Sarda SP, Khan S. Geographic atrophy: mechanism of disease, pathophysiology, and role of the complement system. J Manag Care Spec Pharm. 2023;29(5–a Suppl):S2–s11. doi:10.18553/jmcp.2023.29.5-a.s2
3. Liao DS, Grossi FV, El Mehdi D, et al. Complement C3 inhibitor pegcetacoplan for geographic atrophy secondary to age-related macular degeneration: a randomized Phase 2 trial. Ophthalmology. 2020;127(2):186–195. doi:10.1016/j.ophtha.2019.07.011
4. Chakravarthy U, Bailey CC, Johnston RL, et al. Characterizing disease burden and progression of geographic atrophy secondary to age-related macular degeneration. Ophthalmology. 2018;125(6):842–849. doi:10.1016/j.ophtha.2017.11.036
5. Krogh Nielsen M, Hinnerskov JMV, Sørensen TL. Geographic atrophy - Signs, symptoms, and quality of life. Acta Ophthalmol. 2023;101(8):896–902. doi:10.1111/aos.15794
6. Morga A, Chamberlain CX, Meyers O, Roberts C, Gaspar L, Su J. Content validity and cognitive debriefing of a patient-reported outcome instrument evaluating symptoms and disease impact in patients with geographic atrophy. Ophthalmol Ther. 2023;12(2):1181–1193. doi:10.1007/s40123-023-00667-3
7. Carlton J, Barnes S, Haywood A. Patient perspectives in geographic atrophy (GA): exploratory qualitative research to understand the impact of GA for patients and their families. Br Ir Orthopt J. 2019;15(1):133–141. doi:10.22599/bioj.137
8. Boyer DS, Schmidt-Erfurth U, van Lookeren Campagne M, Henry EC, Brittain C. The pathophysiology of geographic atropy secondary to age-related macular degeneration and the complement pathway as a therapeutic target. Retina. 2017;37(5):819–835. doi:10.1097/iae.0000000000001392
9. US Food and Drug Administration. SYFOVRE™ (pegcetacoplan injection). Highlights of prescribing information. 2021. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/217171s002lbl.pdf.
10. US Food and Drug Administration.IZERVAY™ (avacincaptad pegol intravitreal solution). Highlights of prescribing information. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/217225s000lbl.pdf.
11. TGA. SYFOVRE™ (Apellis Australia Pty Ltd). 2025. Available from: https://www.tga.gov.au/resources/prescription-medicines-registrations/syfovre-apellis-australia-pty-ltdhttps://pi.apellis.com/files/PI_SYFOVRE.pdf.
12. US Food and Drug Administration. SYFOVRE™ (pegcetacoplan injection), for intravitreal use. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/217171s002lbl.pdf.
13. Heier JS, Lad EM, Holz FG, et al. Pegcetacoplan for the treatment of geographic atrophy secondary to age-related macular degeneration (OAKS and DERBY): two multicentre, randomised, double-masked, sham-controlled, phase 3 trials. Lancet. 2023;402(10411):1434–1448. doi:10.1016/s0140-6736(23)01520-9
14. Jaffe GJ, Westby K, Csaky KG, et al. C5 inhibitor avacincaptad pegol for geographic atrophy due to age-related macular degeneration: a randomized pivotal phase 2/3 trial. Ophthalmology. 2021;128(4):576–586. doi:10.1016/j.ophtha.2020.08.027
15. Iveric Bio receives U.S. FDA approval for IZERVAY™ (avacincaptad pegol intravitreal solution), a new treatment for geographic atrophy. 2023. Available from: https://www.prnewswire.com/news-releases/iveric-bio-receives-us-fda-approval-for-izervay-avacincaptad-pegol-intravitreal-solution-a-new-treatment-for-geographic-atrophy-301894042.html.
16. Becker Z. Experts flag eye inflammation reports tied to Apellis’ geographic atrophy med Syfovre. 2024. Available from: https://www.fiercepharma.com/pharma/experts-flag-eye-inflammation-reports-tied-apellis-geographic-atrophy-med-syfovre.
17. Witkin AJ, Jaffe GJ, Srivastava SK, Davis JL, Kim JE. Retinal vasculitis after intravitreal pegcetacoplan: report from the ASRS Research and Safety in Therapeutics (ReST) committee. J Vitreoretin Dis. 2024;8(1):9–20. doi:10.1177/24741264231220224
18. Heier JS, Cohen MN, Chao DL, et al. Phase 1 study of JNJ-81201887 gene therapy in geographic atrophy secondary to age-related macular degeneration. Ophthalmology. 2024. doi:10.1016/j.ophtha.2024.06.013
19. ClinicalTrials.gov. A study to evaluate intravitreal JNJ-81201887 (AAVCAGsCD59) compared to sham procedure for the treatment of geographic atrophy (GA) secondary to age-related macular degeneration (AMD). 2024. Available from: https://clinicaltrials.gov/study/NCT05811351.
20. Trivizki O, Loewenstein A, Zur D. The roadmap to geographic atrophy treatment: a journey of trials and promise. Acta Ophthalmol. 2023;101(8):891–895. doi:10.1111/aos.15801
21. Ghoraba HH, Akhavanrezayat A, Karaca I, et al. Ocular gene therapy: a literature review with special focus on immune and inflammatory responses. Clin Ophthalmol. 2022;16:1753–1771. doi:10.2147/opth.S364200
22. Soekhai V, Whichello C, Levitan B, et al. Methods for exploring and eliciting patient preferences in the medical product lifecycle: a literature review. Drug Discov Today. 2019;24(7):1324–1331. doi:10.1016/j.drudis.2019.05.001
23. Huls SPI, Lancsar E, Donkers B, Ride J. Two for the price of one: if moving beyond traditional single-best discrete choice experiments, should we use best-worst, best-best or ranking for preference elicitation? Health Econ. 2022;31(12):2630–2647. doi:10.1002/hec.4599
24. Bridges JF, Hauber AB, Marshall D, et al. Conjoint analysis applications in health - a checklist: a report of the ISPOR Good Research Practices for Conjoint Analysis Task Force. Value Health. 2011;14(4):403–413. doi:10.1016/j.jval.2010.11.013
25. Soekhai V, de Bekker-Grob EW, Ellis AR, Vass CM. Discrete choice experiments in health economics: past, present and future. Pharmacoeconomics. 2019;37(2):201–226. doi:10.1007/s40273-018-0734-2
26. McCloud C, Khadka J, Gilhotra JS, Pesudovs K. Divergence in the lived experience of people with macular degeneration. Optom Vis Sci. 2014;91(8):966–974. doi:10.1097/OPX.0000000000000320
27. Danner M, Vennedey V, Hiligsmann M, Fauser S, Gross C, Stock S. How well can analytic hierarchy process be used to elicit individual preferences? Insights from a survey in patients suffering from age-related macular degeneration. Patient. 2016;9(5):481–492. doi:10.1007/s40271-016-0179-7
28. Gallego-Pinazo R, Pina-Marin B, Comellas M, et al. Patient and retina specialists’ preferences in neovascular age-related macular degeneration treatment. A discrete choice experiment. PLoS One. 2021;16(12):e0261955. doi:10.1371/journal.pone.0261955
29. Droege KM, Caramoy A, Kersten A, et al. Patient preference of ranibizumab treatment regimen for neovascular age-related macular degeneration - monthly injections versus pro re nata. Graefes Arch Clin Exp Ophthalmol. 2014;252(1):31–34. doi:10.1007/s00417-013-2412-6
30. Bhagat D, Kirby B, Bhatt H, Jager R, George M, Sheth V. Patient preferences associated with anti-vascular endothelial growth factor therapies for neovascular age-related macular degeneration and diabetic macular edema. Clin Ophthalmol. 2020;14:2975–2982. doi:10.2147/OPTH.S273564
31. Jacobs B, Palmer N, Shetty T, et al. Patient preferences in retinal drug delivery. Sci Rep. 2021;11(1):18996. doi:10.1038/s41598-021-98568-7
32. Fenwick EK, Ozdemir S, Man REK, et al. Development and validation of a preference-based glaucoma utility instrument using discrete choice experiment. JAMA Ophthalmol. 2021;139(8):866–874. doi:10.1001/jamaophthalmol.2021.1874
33. Aspinall PA, Johnson ZK, Azuara-Blanco A, Montarzino A, Brice R, Vickers A. Evaluation of quality of life and priorities of patients with glaucoma. Invest Ophthalmol Vis Sci. 2008;49(5):1907–1915. doi:10.1167/iovs.07-0559
34. Yu T, Holbrook JT, Thorne JE, Flynn TN, Van Natta ML, Puhan MA. Outcome preferences in patients with noninfectious uveitis: results of a best-worst scaling study. Invest Ophthalmol Vis Sci. 2015;56(11):6864–6872. doi:10.1167/iovs.15-16705
35. Li T, Le JT, Hays RD, et al. Patient-reported outcomes measures and patient preferences for minimally invasive glaucoma surgical devices. Eye. 2020;34(1):205–210. doi:10.1038/s41433-019-0676-8
36. Le JT, Bicket AK, Janssen EM, et al. Prioritizing outcome preferences in patients with ocular hypertension and open-angle glaucoma using best-worst scaling. Ophthalmol Glaucoma. 2019;2(6):367–373. doi:10.1016/j.ogla.2019.08.007
37. Fenwick EK, Bansback N, Gan ATL, et al. Validation of a novel diabetic retinopathy utility index using discrete choice experiments. Br J Ophthalmol. 2020;104(2):188–193. doi:10.1136/bjophthalmol-2019-313899
38. Bhargava JS, Patel B, Foss AJ, Avery AJ, King AJ. Views of glaucoma patients on aspects of their treatment: an assessment of patient preference by conjoint analysis. Invest Ophthalmol Vis Sci. 2006;47(7):2885–2888. doi:10.1167/iovs.05-1244
39. Danner M, Vennedey V, Hiligsmann M, Fauser S, Gross C, Stock S. Comparing analytic hierarchy process and discrete-choice experiment to elicit patient preferences for treatment characteristics in age-related macular degeneration. Value Health. 2017;20(8):1166–1173. doi:10.1016/j.jval.2017.04.022
40. Baxter JM, Fotheringham AJ, Foss AJ. Determining patient preferences in the management of neovascular age-related macular degeneration: a conjoint analysis. Eye. 2016;30(5):698–704. doi:10.1038/eye.2016.18
41. Joko T, Nagai Y, Mori R, et al. Patient preferences for anti-vascular endothelial growth factor treatment for wet age-related macular degeneration in Japan: a discrete choice experiment. Patient Prefer Adherence. 2020;14:553–567. doi:10.2147/PPA.S228890
42. Vennedey V, Danner M, Evers SM, et al. Using qualitative research to facilitate the interpretation of quantitative results from a discrete choice experiment: insights from a survey in elderly ophthalmologic patients. Patient Prefer Adherence. 2016;10:993–1002. doi:10.2147/PPA.S101584
43. Bhargava JS, Bhan-Bhargava A, Foss AJ, King AJ. Views of glaucoma patients on provision of follow-up care; an assessment of patient preferences by conjoint analysis. Br J Ophthalmol. 2008;92(12):1601–1605. doi:10.1136/bjo.2008.140483
44. Mueller S, Agostini H, Ehlken C, Bauer-Steinhusen U, Hasanbasic Z, Wilke T. Patient preferences in the treatment of neovascular age-related macular degeneration: a discrete choice experiment. Ophthalmology. 2016;123(4):876–883. doi:10.1016/j.ophtha.2015.12.001
45. Reed Johnson F, Lancsar E, Marshall D, et al. Constructing experimental designs for discrete-choice experiments: report of the ISPOR Conjoint Analysis Experimental Design Good Research Practices Task Force. Value Health. 2013;16(1):3–13. doi:10.1016/j.jval.2012.08.2223
46. Postmus D, Pignatti F, Hillege HL, Tervonen T. A simulated maximum likelihood procedure for analyzing imprecise trade-off thresholds between the benefits and harms of medicines. Stat Med. 2022;41(29):5612–5621. doi:10.1002/sim.9583
47. Tervonen T, Pignatti F, Postmus D. From individual to population preferences: comparison of discrete choice and dirichlet models for treatment benefit-risk tradeoffs. Med Decis Making. 2019;39(7):879–885. doi:10.1177/0272989x19873630
48. Dohmen T, Falk A, Huffman D, Sunde U, Schupp J, Wagner GG. Individual risk attitudes: measurement, determinants, and behavioral consequences. J Eur Economic Assoc. 2011;9(3):522–550. doi:10.1111/j.1542-4774.2011.01015.x
49. Szrek H, Chao LW, Ramlagan S, Peltzer K. Predicting (un)healthy behavior: a comparison of risk-taking propensity measures. Judgm Decis Mak. 2012;7(6):716–727.
50. Hensher DA, Greene WH. The mixed logit model: the state of practice. Transportation. 2003;30(2):133–176. doi:10.1023/A:1022558715350
51. Hess S, Palma D. Apollo: a flexible, powerful and customisable freeware package for choice model estimation and application. J Choice Model. 2019;32:100170. doi:10.1016/j.jocm.2019.100170
52. Orme B. Getting Started with Conjoint Analysis: Strategies for Product Design and Pricing Research.
53. Fairchild AO, Reed SD, Gonzalez JM. Method for calculating the Simultaneous Maximum Acceptable Risk Threshold (SMART) from discrete-choice experiment benefit-risk studies. Med Decis Making. 2023;43(2):227–238. doi:10.1177/0272989x221132266
54. McFadden D, Train K. Mixed MNL models for discrete response. J Appl Econom. 2000;15(5):447–470.
55. Quaife M, Terris-Prestholt F, Di Tanna GL, Vickerman P. How well do discrete choice experiments predict health choices? A systematic review and meta-analysis of external validity. Eur J Health Econ. 2018;19(8):1053–1066. doi:10.1007/s10198-018-0954-6
56. Csaky KG, Miller JML, Martin DF, Johnson MW. Drug approval for the treatment of geographic atrophy: how we got here and where we need to go. Am J Ophthalmol. 2024;263:231–239. doi:10.1016/j.ajo.2024.02.021
57. European Medicines Agency. Qualification Opinion of IMI PREFER; 2022.
58. European Medicines Agency. ICHE22Guideline on General Considerations for Patient Preference Studies; 2025.
59. US Food and Drug Administration. Incorporating Voluntary Patient Preference Information Over the Total Product Life Cycle. Guidance for Industry, Food and Drug Administration Staff, and Other Interested Parties; 2026.
60. Zhang M, He X, Wu J, Xie F. Differences between physician and patient preferences for cancer treatments: a systematic review. BMC Cancer. 2023;23(1):1126. doi:10.1186/s12885-023-11598-4
61. The Age-Related Eye Disease Study Research Group. The Age-Related Eye Disease Study (AREDS): design implications, Control Clin Trials. 1999;20(6):573–600. AREDS report no. 1. doi:10.1016/s0197-2456(99)00031-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Preferences in the Design and Delivery of Neurodevelopmental Follow-Up Care for Children: A Systematic Review of Discrete Choice Experiments
Sharma P, Kularatna S, Abell B, Eagleson K, Vo LK, Halahakone U, Senanayake S, McPhail SM
Patient Preference and Adherence 2023, 17:2325-2341
Published Date: 19 September 2023
Medical Personnel Behavior Preferences for Providing mHealth Service in China: A Discrete Choice Experiment
Jiang S, Xiong M, Rao X, Liang J, Zhu X, Fu H, Chen J, Wang C
Risk Management and Healthcare Policy 2023, 16:2405-2418
Published Date: 10 November 2023
Preferences for Physical Examination Service in Community Health Service Center in China: A Discrete Choice Experiment
Sun H, Li F, Xu Y, Qi Q, Du Y
Patient Preference and Adherence 2024, 18:39-51
Published Date: 6 January 2024
Patients’ and Relatives’ Preferences for Outpatient and Day Care Services Within End-of-Life Care in Germany – A Discrete Choice Experiment
Apolinarski B, de Jong L, Herbst FA, Huperz C, Röwer HAA, Schneider N, Damm K, Stiel S
Patient Preference and Adherence 2024, 18:519-529
Published Date: 29 February 2024
An Empirical Comparison of Discrete Choice Experiment and Best-Worst Scaling to Estimate Patient Preferences in Infertility Treatment in China
Chen J, Qian X, Su D, Gong J, Shang J, Zhang L, Li X
Patient Preference and Adherence 2025, 19:869-882
Published Date: 30 March 2025