Back to Journals » Open Access Journal of Contraception » Volume 14
Uptake and Associated Factors of Male Contraceptive Method Use: A Community-Based Cross-Sectional Study in Northern Uganda
Authors Tumwesigye R ![]() , Kigongo E
, Kigongo E ![]() , Nakiganga S, Mbyariyehe G, Nabeshya J
, Nakiganga S, Mbyariyehe G, Nabeshya J ![]() , Kabunga A, Musinguzi M, Migisha R
, Kabunga A, Musinguzi M, Migisha R ![]()
Received 26 April 2023
Accepted for publication 9 July 2023
Published 14 July 2023 Volume 2023:14 Pages 129—137
DOI https://doi.org/10.2147/OAJC.S418820
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Igal Wolman
Raymond Tumwesigye,1 Eustes Kigongo,2 Stella Nakiganga,3 Godfred Mbyariyehe,3 Joel Nabeshya,1 Amir Kabunga,4 Marvin Musinguzi,5 Richard Migisha6
1Department of Emergency Nursing and Critical Care, Faculty of Nursing and Midwifery, Lira University, Lira City, Uganda; 2Department of Environment Health and Disease Control, Faculty of Public Health, Lira University, Lira City, Uganda; 3Department of Nursing, Faculty of Nursing and Midwifery, Lira University, Lira City, Uganda; 4Department of Psychiatry, Faculty of Medicine, Lira University, Lira City, Uganda; 5Department of Community Health, Faculty of Public Health, Lira University, Lira City, Uganda; 6Department of Physiology, Mbarara University of Science and Technology, Mbarara City, Uganda
Correspondence: Raymond Tumwesigye, Department of Emergency Nursing and Critical Care, Faculty of Nursing and Midwifery, Lira University, Lira City, Uganda, Tel +256 782810567, Email [email protected]
Background: Uganda has one of the highest fertility rates in Sub-Saharan Africa (SSA). Improving contraceptive uptake in all genders, including males, may be critical to meeting family planning goals in such a setting. Yet, data on male contraception uptake and associated factors in SSA, including Uganda, are limited. We determined the uptake and associated factors of male contraception use in Lira City, Northern Uganda.
Methods: We conducted a community-based cross-sectional study from November 12, 2022, to December 12, 2022, among men aged ≥ 18 years. We used multi-stage sampling to select participants from 12 cells of Lira City divisions of East and West. Data were collected using interviewer-administered structured questionnaires. We defined uptake in males who had used any contraceptive method, including periodic abstinence, withdrawal, condoms, and vasectomy in the previous four weeks. We performed modified Poisson regression to identify associated factors of male contraception uptake.
Results: We recruited 401 participants with mean age of 30.4 (± 9.3) years. Male contraceptive uptake was 46.4%, 95% CI: 41.5– 51.3%. Ever heard about male contraception (adjusted prevalence ratio [aPR] =1.73, 95% CI: 1.172– 2.539, p=0.006), willingness to use novel methods (aPR=2.90, 95% CI: 1.337– 6.293, p=0.007), both partners being responsible for contraception (aPR: 1.53, 95% CI: 1.113– 2.119, p=0.009) were the factors associated with male contraception uptake.
Conclusion: We found that nearly half of the men surveyed had used male contraceptive methods in Lira City. Factors associated with the uptake of male contraception included having heard about male contraception, joint couple decision regarding contraception, and the use of novel methods of male contraception. We recommend comprehensive education and awareness campaigns to promote male contraception, with a particular emphasis on encouraging shared decision-making within couples and introducing innovative contraceptive options.
Keywords: knowledge, male contraception, practices, uptake, Uganda
Background
Globally, male contraceptive use stands at 12.5% and about 60.0% of males are indirectly involved in family planning through spousal communication and approval.1 There is a paucity of literature concerning male contraceptive use in Africa; however, a recent systematic review reported a low level of willingness to use novel male hormonal contraceptives of 34.0%.2 According to the Uganda Demographic and Health survey of 2016, 35.9% of men were using a modern contraceptive method, an increase from 10.4% in 1995.3 Yet, the country is grappling with the highest fertility rate in the region and it stands at 5.4.4
Male partners play a key role in family planning/contraceptive uptake and use. This is influenced by different dimensions that include personal, organizational, spiritual, cultural, and political.2 Henceforth, increasing access to and uptake of male contraceptive methods (periodic abstinence, withdrawal, condoms, and vasectomy) is paramount in reducing abortion rates and unintended pregnancies.5 Additionally, contraception helps in healthy timing and spacing of pregnancies, hence regulating fertility. This correlates with a fall in infant, child, and maternal mortality.1 A recent review reported that male contraception has the potential to shift societal gender dynamics and provide males with gender control over their production.4,6 However, recent clinical trials have reported that men are less willing to use male contraceptives with a level as low as 13.6%.2 If not addressed, this is likely to compromise the achievement of Sustainable Development Goal 3.8 which targets health for all by the year 2030.
In Lira City, there has been a recurrent resistance to family planning by men due to widespread misconceptions about the use of family planning with frequent cases of domestic violence towards their female counterparts.7 Furthermore, a recent study in Uganda found that for men, a lack of knowledge, fear of their partners experiencing side effects, and dissatisfaction with male contraceptive methods have been key barriers to their involvement in their reproductive health.8 Hence, male contraception has been underutilized due to a myriad of factors. Thus far, male contraceptive behavior has been a largely understudied area in Uganda, yet male involvement in family planning both as clients and partners remains a key focus of reproductive health programs.9 Therefore, the purpose of this study was to determine the uptake and associated factors of male contraception use in Lira, Northern Uganda.
Methods
Study Setting
The study was conducted in Lira City from November 12, 2022, to December 12, 2022. Lira city is located in the central part of northern Uganda about 343km from Kampala, well known as one of the regions in northern Uganda with a poor contraceptive non-use prevalence of 50%.10 The city comprises four major divisions, namely: Lira City West, East Division, Central, and Adyel division. The current uptake of male modern contraceptives in Lira City is unknown; however, recent studies found that the prevalence of utilization of modern contraceptives among postpartum women at two health centers in Lira City was 49.4%.11
Study Design
This was a community-based cross-sectional study.
Study Population and Eligibility Criteria
We included males aged 18 years and above, who were residing in the selected divisions of Lira City during the study period. The study excluded male health workers because they have good knowledge of male contraceptives and were likely to skew the data. Additionally, individuals who declined to consent were excluded.
Sampling Criteria
A multi-stage sampling technique was used to select the participants from the Lira City Divisions of East and West. The 12 selected cells were Bar-onger Central and Go-down, Railway Quarters, Boroboro East, Baridike, Owinyo church, Ayago (a and b) and Kirombe Central and West, Teso A and Lira Modern Primary School. The two divisions, East and West were selected. Within each of the two divisions, two sub-counties were selected by simple random sampling. From each sub-county, two parishes were selected by a simple random sampling technique. A consecutive sampling technique was used to select the participants who gave written consent. In the technique, participants meeting the inclusion criteria and willing to participate were selected for the study. Participants who at the time of data collection were emotionally or psychologically unstable or had difficulty communicating or had cognitive impairment were excluded.
Sample Size Estimation
The study estimated sample size using the Kish formula (1965), assuming a variability (p=0.13), 95% Confidence interval, 5% margin of error, and Z=1.96. In order to account for the non-response rate, the sample size was increased by 10% to 193 participants. By factoring in the design effect of 2, this doubled the calculated minimum sample size to generate a total estimate of 386.
Data Collection
Five research assistants who were social scientists and good in both English and local dialect were recruited and trained to guide participants in filling in the questionnaire. Data for the present study was collected using a researcher-formulated questionnaire. The instrument had two sections, A and B. Section A captured demographic information such as age, education, marital status, and others. Section B captured information on awareness of, knowledge of, and practices of male contraceptive use and had 15 items. Such items included, “Have you ever heard about male contraception?” It captured information on the basis of “yes” and “no.” The uptake of male contraception, or self-reported use of male contraceptives in the prior month, was the study’s outcome variable and was assessed as a yes/no response. The independent variables included sociodemographic characteristics, knowledge about, and practices regarding male contraception. Pretesting of the questionnaire was done on 10% of the respondents, giving a Cronbach's alpha of 0.89.
Data Analysis
Every questionnaire was checked for completeness. Data were collected using Open Data Kit (ODK) software and thereafter exported to Microsoft excel for cleaning and editing, which was later exported to STATA version 17 (STATACorp LLC, Texas, USA). Descriptive statistics including frequencies and percentages were used to summarize the participants’ characteristics. Univariate analysis was done to generate frequencies and percentages for male contraceptive uptake variables related to knowledge and practices. Bivariate and multivariate analysis with a well-constructed regression model of predictors of male contraception was done. The outcome variable was extracted from the question, have you ever used any male contraception in the previous four weeks? Responses were Yes or No. We utilized prevalence ratios by way of a modified Poisson regression method employing a generalized linear model with Poisson as family and log link without an offset and integrating robust standard errors.12,13 Given the high prevalence (46.4%), odds ratios could have overestimated the effect size, hence they were not employed.14
Results
Socio-Demographic Characteristics
We analyzed data from 401 male participants, with an average age of 30.4 (±9.3) years with an average of 3 children. Most participants had completed tertiary education (37.7%; n=151), were married (60.6%; n=243), and were peasants (46.3%; n=155). Most of the respondents were Anglican (47.4%; n=190) and lived in an urban setting (91.5%; n=367) (Table 1).
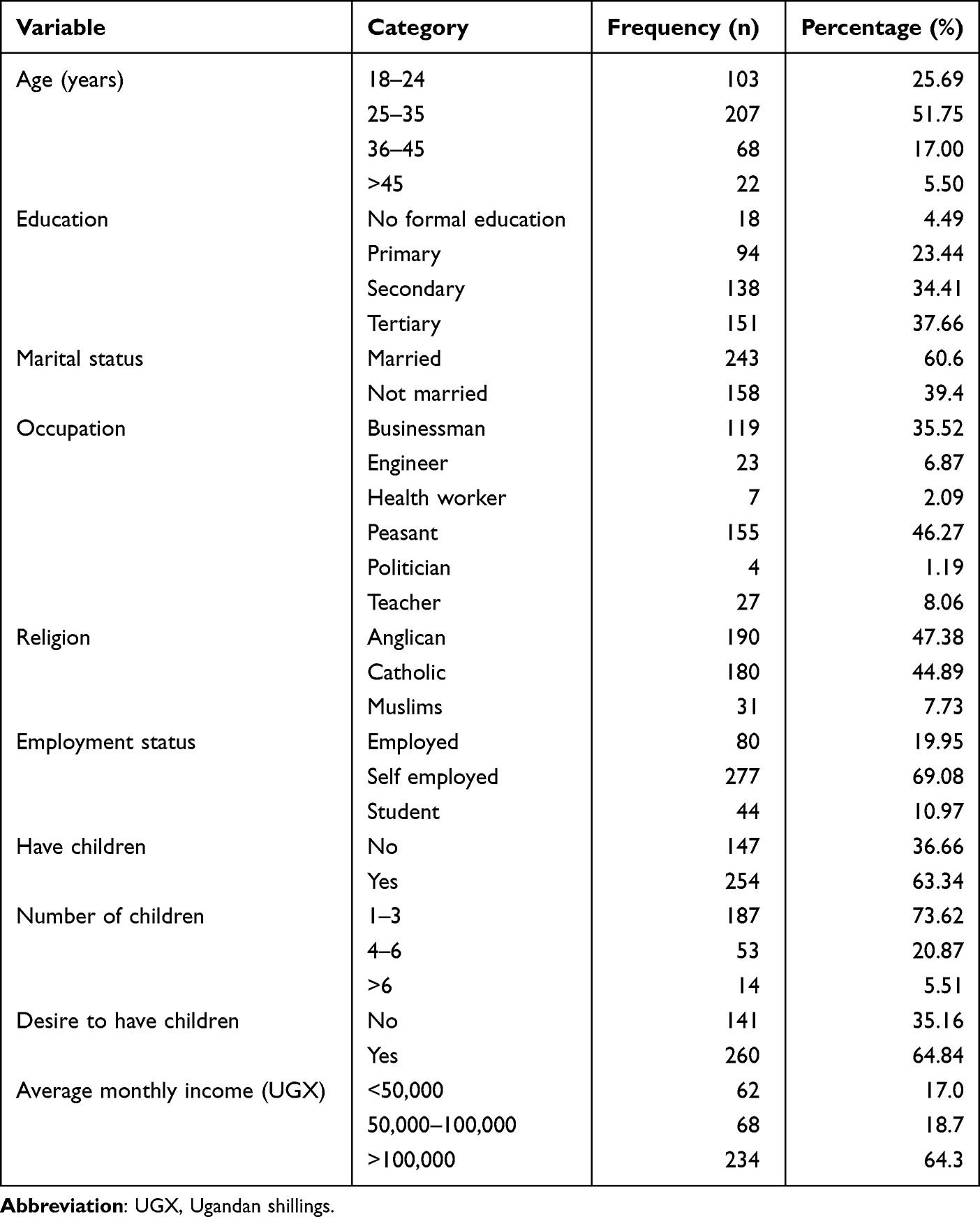 |
Table 1 Socio-Demographic Characteristics of Respondents (N=401) |
Male Contraceptive Uptake Variables Related to Knowledge and Practices
Out of the total sample of 401 male participants, the uptake of male contraceptives was 46.4% (n=186) with a 95% confidence interval of 41.5% to 51.3%. The majority of the respondents had heard about male contraceptives (61.9%; n=248) and knew condoms as a male contraceptive method (68.8%; n=275). Most of the respondents had obtained this information from friends (48.9%; n=108) and had talked to their spouses about using male contraceptives (53.1%; n=213). However, most of the respondents were not willing to use novel contraceptives (61.6%; n=247) and their spouses had not approved of the use of male contraceptives (51.4%; n=206) (Table 2).
 |
Table 2 Knowledge and Practices Regarding Male Contraceptive Use Among Respondents (N=401) |
Factors Associated with Male Contraceptive Use
At Multivariate analysis (Table 3), ever hearing about male contraception (adjusted prevalence ratio [aPR]=1.73, 95% CI: 1.172–2.539, p=0.006), willingness to use novel methods (aPR=2.90, 95% CI: 1.337–6.293, p=0.007), both partners responsible for contraception (aPR: 1.53, 95% CI: 1.113–2.119, p=0.009) were significantly associated with uptake of male contraceptives. Participants who had heard about male contraceptives were 1.73 times more likely to use male contraceptives compared to those who had not heard of male contraceptives. Respondents who were willing to use novel methods of male contraceptives were 2.9 times more likely to use male contraceptives compared to those who were not willing to use novel methods. Males who reported that both partners are responsible for contraceptive use were 1.53% more likely to use male contraceptives (Table 3).
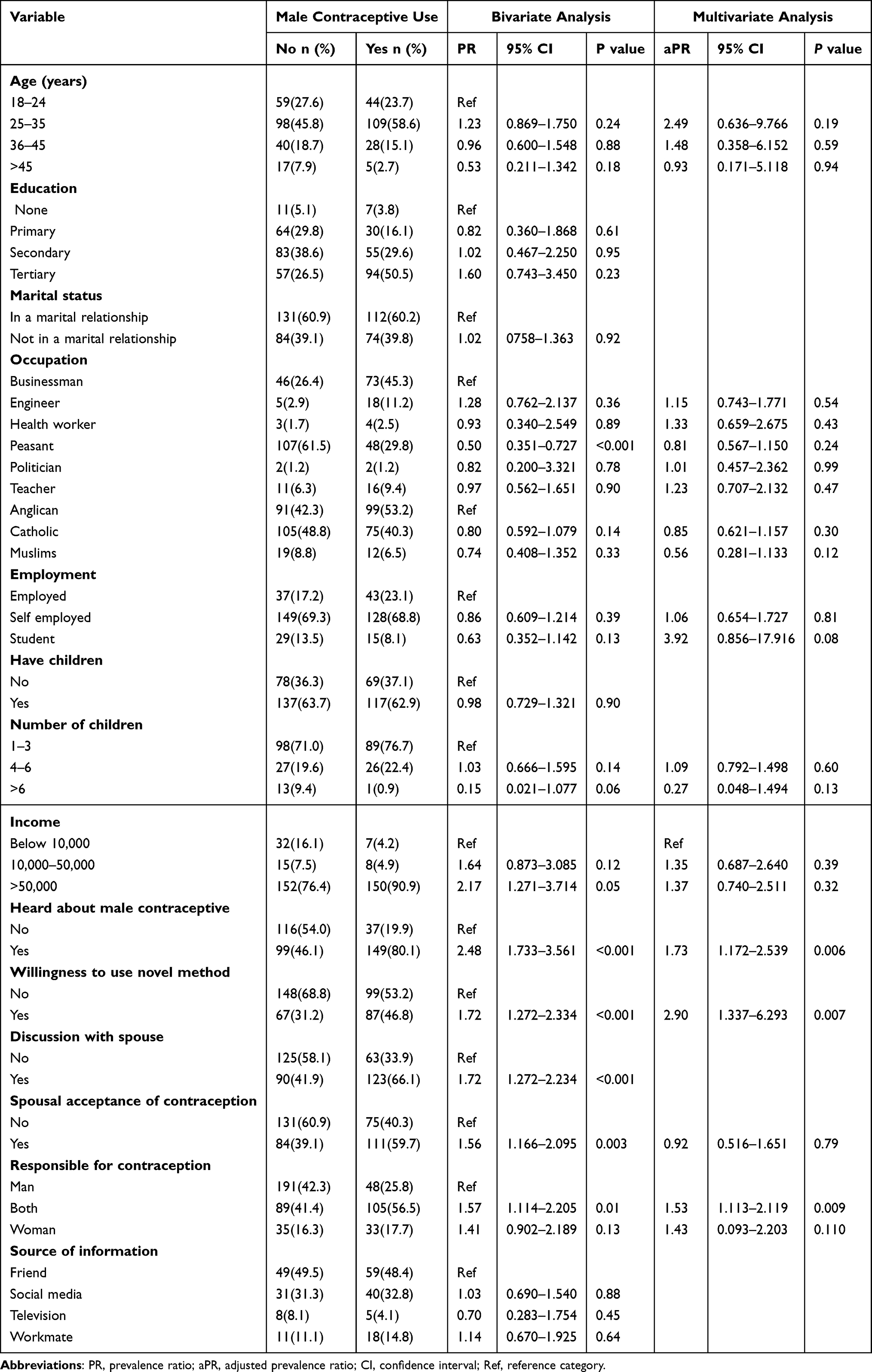 |
Table 3 Bivariate and Multivariate Analysis for Factors Associated with Male Contraceptive Use, Lira City, Uganda |
Discussion
We conducted a study to determine the uptake and associated factors of male contraceptive method use in Northern Uganda. We found the uptake of male contraceptives was 46.4%. The findings report an improvement in the uptake of modern male contraception contrary to the previously reported uptake of 35.9% by a recent cross-sectional population survey conducted in Uganda.6 This is most likely due to the increase in massive campaigns on virtual communication platforms, radios, and TVs regarding male contraception use in the study setting. Moreover, in the current study, men who had ever heard about male contraception were more likely to use male contraception compared to their counterparts who did not get any information regarding male contraception. The uptake of male contraceptives in the current study is consistent with previous reports from Cameroon and Ghana, which documented rates of 46.4% and 42.6%, respectively.15,16 However, the uptake is higher than 38.4% reported in urban Uganda.17 This discrepancy may be attributed to differences in sample size and geographic settings.
The results further revealed that 53.1% had talked to their spouses about using male contraceptives and the couple jointly consented to it. The findings of this study align with recent research conducted in Malawi and Tanzania, which reported a prevalence of male involvement in family planning decisions of 53.0% and 26.6%, respectively.18 This is further supported by a study conducted in Indonesia, which found that the approval of the family planning method by spouses positively influenced the uptake of male contraception.19 This study also revealed decreased willingness for uptake in situations where only male partners were responsible for contraception. Couples need to make a joint decision regarding contraception because it involves both individuals and affects their relationship, well-being, and future plans. Making a joint decision together ensures that both partners are comfortable and in agreement with the chosen method and promotes communication, mutual trust in the relationship and overall quality of life.
Our findings show that participants who were willing to use novel methods of male contraceptives were more likely to use male contraceptives compared to those who were not willing to use novel methods. This finding aligns with the results of a recent qualitative survey conducted in Uganda and Burkina Faso, which indicated a greater level of acceptance and positive attitudes towards novel hormonal contraceptive methods in Uganda compared to Burkina Faso.20 These findings categorically indicate that there is growing awareness about men taking responsibility for contraception and will most likely accept and utilize these novel methods once available, given the fact that traditional hormonal female contraceptive methods have been associated with serious lifelong side effects in women.
Our results revealed that those who had not heard of male contraceptives and were not willing to use novel methods were less likely to use male contraceptive methods. Both of these circumstances negatively affect male contraceptive uptake rates, because men are not educated on the different options of male contraception and may not consider using them as a viable option for family planning. This can lead to deadly complications that include unintended pregnancies which can have long-term consequences for individuals, families, and communities. This result mirrors the findings of the study conducted in 2017 in Uganda.21
In a nutshell, the improved male contraceptive uptake has public health implications, as this will most likely reduce the burden of contraceptive uptake on women and potentially lower the magnitude of unintended pregnancies and the overall burden of maternal morbidity and mortality. The factors associated with male contraception such as having heard about male contraception could have been indirectly influenced by increasing male literacy levels, socioeconomic status, exposure to sexual reproductive health and rights services in schools, and media exposure. Therefore, such efforts and many others should be continuing to exist and be supported by the government of Uganda and other development partners. Lastly, joint couple decision-making around contraception use could lead to increased contraception use in general and better decision-making around family planning. The factors that could impact this decision-making process could include the level of couple communication, gender norms, power dynamics within the relationship, and individual attitudes towards contraception.
Strengths and Limitations of the Study
The study helped provide evidence of acceptability regarding further plans to roll out novel male contraception methods. However, it was limited in scope and only focused on male contraceptive uptake in Lira City Northern Uganda; hence, our findings can only be generalized to the population of men in Lira City in Northern Uganda and other similar peri-urban settings. Because the study was cross-sectional, we cannot establish causality, its limited to one point in time and does not provide information on temporal relationships. Additionally, we could not rule out under-reporting of male contraception given that it is a culturally sensitive issue that is subject to social desirability bias and the Hawthorne effect. Despite its limitations, this study produced data that will help researchers better understand the magnitude of male contraception is low and the factors associated with the uptake.
Conclusion
We found that nearly half of the men surveyed had used male contraceptive methods in Lira City. The factors associated with the uptake of male contraception included having heard about male contraception, joint couple decision regarding contraception, and use of novel methods of male contraception were significantly implicated in increasing willingness for uptake. We recommend increasing efforts to create more awareness and education around male contraceptive methods with a focus on joint decision-making between couples and the use of novel methods. This could potentially lead to an increase in the adoption of male contraceptives and ultimately contribute to more effective family planning and reproductive health outcomes.
Abbreviations
aPR, adjusted prevalence ratio; CI, confidence interval; CIRTH, Center for International Reproductive Health Training; ODK, Open Data Kit; PR, prevalence ratio; SD, standard deviation.
Data Sharing Statement
The Principal Investigator is the custodian of the datasets and other materials of this study. For confidentiality reasons, the datasets are not publicly available. However, the data sets can be availed upon reasonable request from the corresponding author.
Ethics Approval and Consent to Participate
The ethical approval was granted by Gulu University Research Ethics Committee under approval number GUREC-2022-330. We sought and obtained written informed consent from respondents during data collection. The participants indicated their consent by checking an appropriate box for consent before filling out the questionnaires. Participants were told that their participation was voluntary and that there would be no negative consequences if they refused to participate (none declined). During data collection, respondents were assigned unique identifiers instead of names to protect their confidentiality. Information was stored in password-protected computers and was not shared with anyone outside the investigation team. Additionally, we obtained permission from Local council Chairpersons of the selected wards of Lira City where the study was conducted.
Acknowledgments
We thank everyone who participated in this study. We are also grateful for the support from the Center for International Reproductive Health Training (CIRTH) at the University of Michigan, United States, in conducting this study.
Author Contributions
All authors (RT, EK, SN, GM, JN, AK, MM and RM) made substantial contributions to the conception and design of the study, acquisition, analysis, and interpretation of the data. All the authors took part in drafting and revising the article critically for important intellectual content; all the authors agreed to submit the manuscript to the current journal; all authors gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Funding
This research was supported by seed funding from the Center for International Reproductive Health Training (CIRTH) at the University of Michigan, United States. This research work was supported by the Center for International Reproductive Health Training (CIRHT-UM), at the University of Michigan, it mainly supported the process of proposal development, data collection, and processing. The funder does not have any influence on the study findings or its processes.
Disclosure
The authors of this work report no conflicts of interest. However, it is important to note that Lira University had not yet established its own Research Ethics Committee at the time of our study (REC). Therefore, we sought ethical approval for our research protocol from the nearby institution, Gulu University. Initial establishment of Lira University was as a constituent college affiliated with Gulu University.
References
1. Shiferaw WS, Akalu TY, Aynalem YA. Prevalence of erectile dysfunction in patients with diabetes mellitus and its association with body mass index and Glycated hemoglobin in Africa: a systematic review and meta-analysis. Int J Endocrinol. 2020;2020:1–10. doi:10.1155/2020/5148370
2. Reynolds-Wright JJ, Cameron NJ, Anderson RA. Will men use novel male contraceptive methods and will women trust them? A systematic review. J Sex Res. 2021;58:838–849. doi:10.1080/00224499.2021.1905764
3. UDHS. Uganda Demographic and Health Survey 2016; 2016.
4. ICF&UBOS. No the DHS program—Uganda: DHS, 2018—final report title; 2018.
5. Kriel Y, Milford C, Cordero J, et al. Male partner influence on family planning and contraceptive use: perspectives from community members and healthcare providers in KwaZulu-Natal, South Africa. Reprod Health. 2019;16:1–15. doi:10.1186/s12978-019-0749-y
6. Namasivayam A, Lovell S, Namutamba S, Schluter PJ. Predictors of modern contraceptive use among women and men in Uganda: a population-level analysis. BMJ Open. 2020;10:e034675. doi:10.1136/bmjopen-2019-034675
7. The daily Monitor. Lira men reject family planning; 2021.
8. Namasivayam A Understanding unmet need for contraception in Uganda: a mixed methods study of contraceptive use among women and men; 2020.
9. Okalo P, Arach AA, Apili B, Oyat J, Halima N, Kabunga A. Predictors of unintended pregnancy among adolescent girls during the second wave of COVID-19 pandemic in Oyam District in Northern Uganda. Open Access J Contracept. 2023;Volume 14:15–21. doi:10.2147/OAJC.S399973
10. Otim J. Contraceptive nonuse among women in Uganda: a comparative assessment of predictors across regions. BMC Womens Health. 2020;20(1):1–14. doi:10.1186/s12905-020-01148-6
11. Isoke R, Kunihira I, Apili F. Prevalence, barriers and facilitators influencing modern contraceptive use among postpartum mothers at ober and barapwo health centre III, Lira City: a cross sectional design; 2022.
12. Cook TD. Advanced statistics: up with odds ratios! A case for odds ratios when outcomes are common. Acad Emerg Med. 2002;9:1430–1434. doi:10.1197/aemj.9.12.1430
13. Barros AJD, Hirakata VN. Alternatives for logistic regression in cross-sectional studies: an empirical comparison of models that directly estimate the prevalence ratio. BMC Med Res Methodol. 2003;3:1–13. doi:10.1186/1471-2288-3-21
14. Migisha R, Ario AR, Kwesiga B, et al. Risk perception and psychological state of healthcare workers in referral hospitals during the early phase of the COVID-19 pandemic, Uganda. BMC Psychol. 2021;9:195. doi:10.1186/s40359-021-00706-3
15. Tsegaye R. Family planning need of people living with HIV/AIDS in antiretroviral therapy clinics of Horro Guduru Wollega zone, Ethiopia. BMC Res Notes. 2017;10:1–6. doi:10.1186/s13104-017-2914-0
16. Melaku YA, Zeleke EG. Contraceptive utilization and associated factors among HIV positive women on chronic follow up care in Tigray Region, Northern Ethiopia: a cross sectional study. PLoS One. 2014;9:e94682. doi:10.1371/journal.pone.0094682
17. Mbabazi L, Nabaggala MS, Kiwanuka S, et al. Factors associated with uptake of contraceptives among HIV positive women on dolutegravir based anti-retroviral treatment-a cross sectional survey in urban Uganda. BMC Women's Health. 2022;22:262. doi:10.1186/s12905-022-01842-7
18. Osuafor GN, Akokuwebe ME, Idemudia ES. Male Involvement in family planning decisions in Malawi and Tanzania: what are the determinants? Int J Environ Res Public Health. 2023;20:5053. doi:10.3390/ijerph20065053
19. Irawaty DK, Pratomo H. Socio-demographic characteristics of male contraceptive use in Indonesia. Malaysian J Public Heal Med. 2019;19:152–157. doi:10.37268/mjphm/vol.19/no.1/art.47
20. Cartwright AF, Lawton A, Brunie A, Callahan RL. What about methods for men? A qualitative analysis of attitudes toward male contraception in Burkina Faso and Uganda. Int Perspect Sex Reprod Health. 2020;46:153. doi:10.1363/46e9720
21. Thummalachetty N, Mathur S, Mullinax M, et al. Contraceptive knowledge, perceptions, and concerns among men in Uganda. BMC Public Health. 2017;17:1–9. doi:10.1186/s12889-017-4815-5
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
COVID-19 and Saudi Arabia: Awareness, Attitude, and Practice
Fawzy MS, AlSadrah SA
Journal of Multidisciplinary Healthcare 2022, 15:1595-1618
Published Date: 26 July 2022
Knowledge, Attitude, Perceived Responsibilities, and Associated Factors Regarding Colostomy Care Among Nurses Working in Surgical Units at Amhara Region General and Referral Hospitals, Ethiopia: A Mixed Method Study
Tiruneh TE, Alem G, Taddele M, Tizazu ZM, Minale FK, Alemu KD
Nursing: Research and Reviews 2022, 12:191-206
Published Date: 13 October 2022
Self-Medication Prevalence and Factors Associated with Knowledge and Attitude Towards Self-Medication Among Undergraduate Health Science Students at GAMBY Medical and Business College, Bahir Dar, Ethiopia
Siraj EA, Yayehrad AT, Kassaw AT, Kassahun D, Solomon E, Abdela H, Gizachew G, Awoke E
Patient Preference and Adherence 2022, 16:3157-3172
Published Date: 5 December 2022
Prevalence and Predictors of Knowledge and Attitude on Optimal Nutrition and Health Among Pregnant Women in Their First Trimester of Pregnancy
Gebremichael MA, Lema TB
International Journal of Women's Health 2023, 15:1383-1395
Published Date: 4 September 2023
Addressing the Neglected Burden of Cancer Cachexia: A Quasi-Experimental Study at Uganda Cancer Institute
Dave D, Angucia BS, Komukama C, Kahwa A, Srikant S, Pakileto A, Anecho E, Niyonzima N
Cancer Management and Research 2026, 18:576718
Published Date: 24 March 2026