")
Back to Journals » OncoTargets and Therapy » Volume 12
Update on elotuzumab for the treatment of relapsed/refractory multiple myeloma: patients’ selection and perspective
Authors Trudel S, Moreau P, Touzeau C
Received 22 March 2019
Accepted for publication 31 May 2019
Published 18 July 2019 Volume 2019:12 Pages 5813—5822
DOI https://doi.org/10.2147/OTT.S174640
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sanjeev K. Srivastava
Sabrina Trudel,1 Philippe Moreau,1–3 Cyrille Touzeau1–3
1Hematology Department, University Hospital, Nantes, France; 2Centre de Recherche en Cancérologie et Immunologie Nantes-Angers (CRCINA), Institut National de la Santé et de la Recherche Médicale (INSERM), Centre National de la Recherche Scientifique (CNRS), Université d’Angers, Université de Nantes, Nantes, France; 3Site de Recherche Intégrée sur le Cancer (SIRIC), Imaging and Longitudinal Investigations to Ameliorate Decision-making (ILIAD), Nantes, France
Abstract: Monoclonal antibodies (mAbs) targeting antigens expressed by plasma cells demonstrated major clinical activity in multiple myeloma patients and therefore became a new major class of drug for these patients. Elotuzumab is a humanized mAb targeting the cell surface signaling lymphocytic activation molecule family member 7, a glycoprotein highly expressed on plasma cells, that is the second mAb approved for the treatment of myeloma patients. The mechanism of action of elotuzumab includes natural killer cell (NK) mediated antibody-dependent cellular cytotoxicity and direct activation of NK-cells. Elotuzumab has been approved in combination with lenalidomide and dexamethasone (Elo-Rd) and pomalidomide and dexamethasone (Elo-Pd) for the treatment of relapsed myeloma patients. The present review will focus on elotuzumab, providing a summary of the mechanism of action, efficacy and safety and taking into consideration patients’ selection.
Keywords: CS1, SLAMF7, elotuzumab, monoclonal antibody, multiple myeloma
Introduction
Multiple myeloma (MM) is a mature B-cell neoplasm characterized by the neoplastic proliferation of clonal bone marrow plasma cells producing a monoclonal immunoglobulin. MM accounts for approximately 2% of all new cancer cases and nearly 15% of hematologic malignancies.1 MM primarily affects older individuals with a median age at the time of diagnosis of nearly 70 years.2 The life expectancy of myeloma patients has doubled over the past decades.3 This outstanding improvement is predominantly due to the widespread use of proteasome inhibitor (PI) (ie, bortezomib, carfilzomib) and immunomodulatory drugs (IMiDs) (ie, thalidomide, lenalidomide, pomalidomide), the major cornerstones of myeloma therapy. However, the outcome of patients whose disease became refractory to PI and IMiDs remains poor, with a median overall survival (OS) of nearly 1 year.4 Therefore, improving the myeloma armamentarium with effective novel agents is warranted.
More recently, monoclonal antibodies (mAbs) targeting antigens expressed by plasma cells demonstrated major clinical activity in MM and therefore became a new major class of drug for the treatment of MM patients.5 In 2015, the mAbs elotuzumab and daratumumab have been approved for the treatment of MM patients. Daratumumab is a fully humanized immunoglobulin G1 (IgG1) mAb targeting CD38, a cell surface glycoprotein widely expressed on myeloma cells. The results of the large Phase II study SIRIUS led to the approval of daratumumab single agent for the treatment of relapsed MM patients who have received at least three prior therapies, including bortezomib, lenalidomide and pomalidomide.6 In 2016, daratumumab in combination with lenalidomide and dexamethasone, or bortezomib and dexamethasone was approved for the treatment of patients with MM who have received at least one prior therapy.7,8 In 2017, daratumumab in combination with pomalidomide and dexamethasone was approved for the treatment of relapsed and refractory MM previously treated with lenalidomide and a PI.9 In 2018, daratumumab has also been approved, in combination with bortezomib melphalan and prednisone, in transplant ineligible newly diagnosed MM patients.10 Daratumumab displays an excellent safety profile with low-grade infusion-related reactions (IRR) occurring mostly during the first infusion as the main treatment-emergent adverse event.11
Elotuzumab, a humanized mAb targeting the cell surface protein SLAMF7, is the second mAb approved for the treatment of myeloma patients.
The present review will focus on elotuzumab, providing a summary of the mechanism of action and of the evidence regarding clinical results and safety profile of the elotuzumab-based treatment of MM. Taking into consideration patients’ perspectives and quality of life, we will explore the evidence behind elotuzumab therapy in terms of improving patients’ outcome and satisfaction.
Mechanism of action of elotuzumab
Elotuzumab (Elo) is a humanized IgG1 mAb directed against SLAMF7, also called CS1 (cell surface glycoprotein CD2 subset 1).12,13 SLAMF7 is a glycoprotein highly expressed on most normal and abnormal plasma cells, and natural killer cells, but not on hematopoietic stem cells and other normal tissues.14 More than 95% of bone marrow myeloma cells express SLAMF7.14 The primary mechanism of action of elotuzumab is via NK cell-mediated antibody-dependent cellular cytotoxicity.13,14 Elotuzumab also directly activates NK cells through both SLAMF7 pathway and Fc receptors (CD16).15 Expression of SLAMF7 is maintained in all subgroups of MM patients, regardless of cytogenetics or previous lines of therapy.14 With little to no expression of SLAMF7 protein in normal tissue, elotuzumab selectively kills myeloma cells with minimal off-target effects.14 Elotuzumab indeed allows a highly targeted therapy with minimal undesirable side effects to the patient. In contrast to elotuzumab, daratumumab is a humanized mAb directed against CD38. Daratumumab binds to CD38 expressing tumor cells and therefore induce apoptosis directly through Fc mediated cross-linking as well as by immune-mediated tumor cell lysis through ADCC and antibody-dependent cellular phagocytosis).16 Daratumumab has also been shown to deplete T- and B-regulatory cells thereby stimulating clonal expansion of helper and cytotoxic T cells, which has not been demonstrated with elotuzumab.16
Mechanisms involved in resistance to elotuzumab are still unclear. Recently, serum level of soluble SLAMF7 has been shown to inhibit elotuzumab ADCC cytotoxicity in vitro.17
Current treatment options with elotuzumab in relapsed refractory myeloma
Elotuzumab single agent
Clinical trials evaluating elotuzumab in MM patients are summarized in Table 1. Elotuzumab monotherapy at doses ranging from 0.5 to 20 mg/kg demonstrated no single agent activity in a Phase I dose-escalating trial (n=35).18 In this study, only 26% of patients with relapsed refractory multiple myeloma (RRMM) achieved stable disease as best response. Elotuzumab monotherapy was however associated with a minimal toxicity, mostly related to IRR.
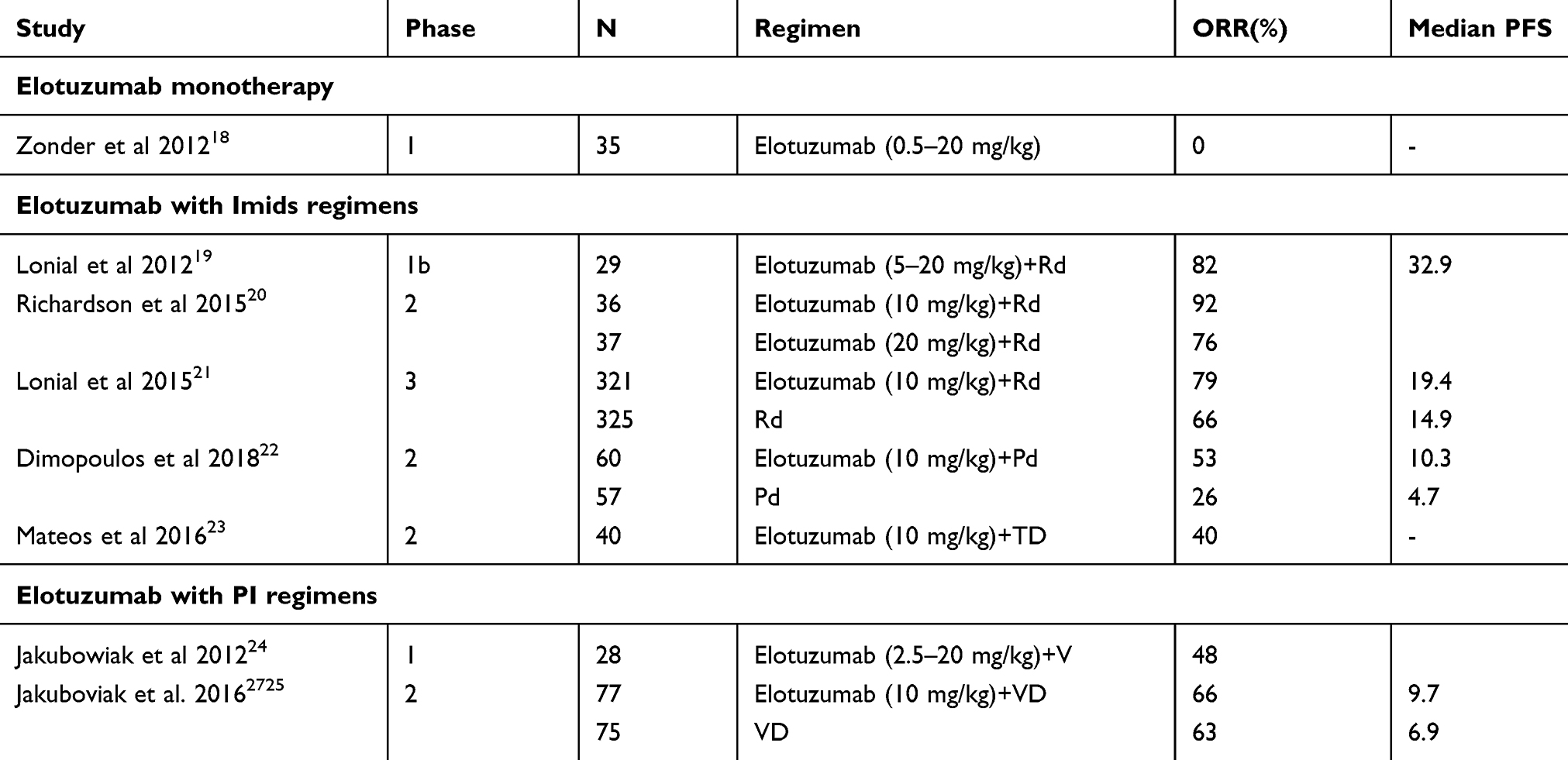 |
Table 1 Elotuzumab for the treatment of multiple myeloma: Phase I–III clinical trials |
Elotuzumab in combination with IMIDS
Lenalidomide
A Phase I study evaluated elotuzumab dose-escalation (5, 10 or 20 mg/kg) in combination with lenalidomide and dexamethasone (n=29).19 Majority (79%) of these patients were lenalidomide naïve. Only one patient was refractory to lenalidomide. The scheme of elotuzumab administration in combination with IMiDs is reported in Table 2. The overall response rate (ORR) was 82%, with 9 patients achieving at least a very good partial response (VGPR). The ORR among patients prior exposed to lenalidomide was 33%. The median progression-free survival (PFS) was 32.9 months.
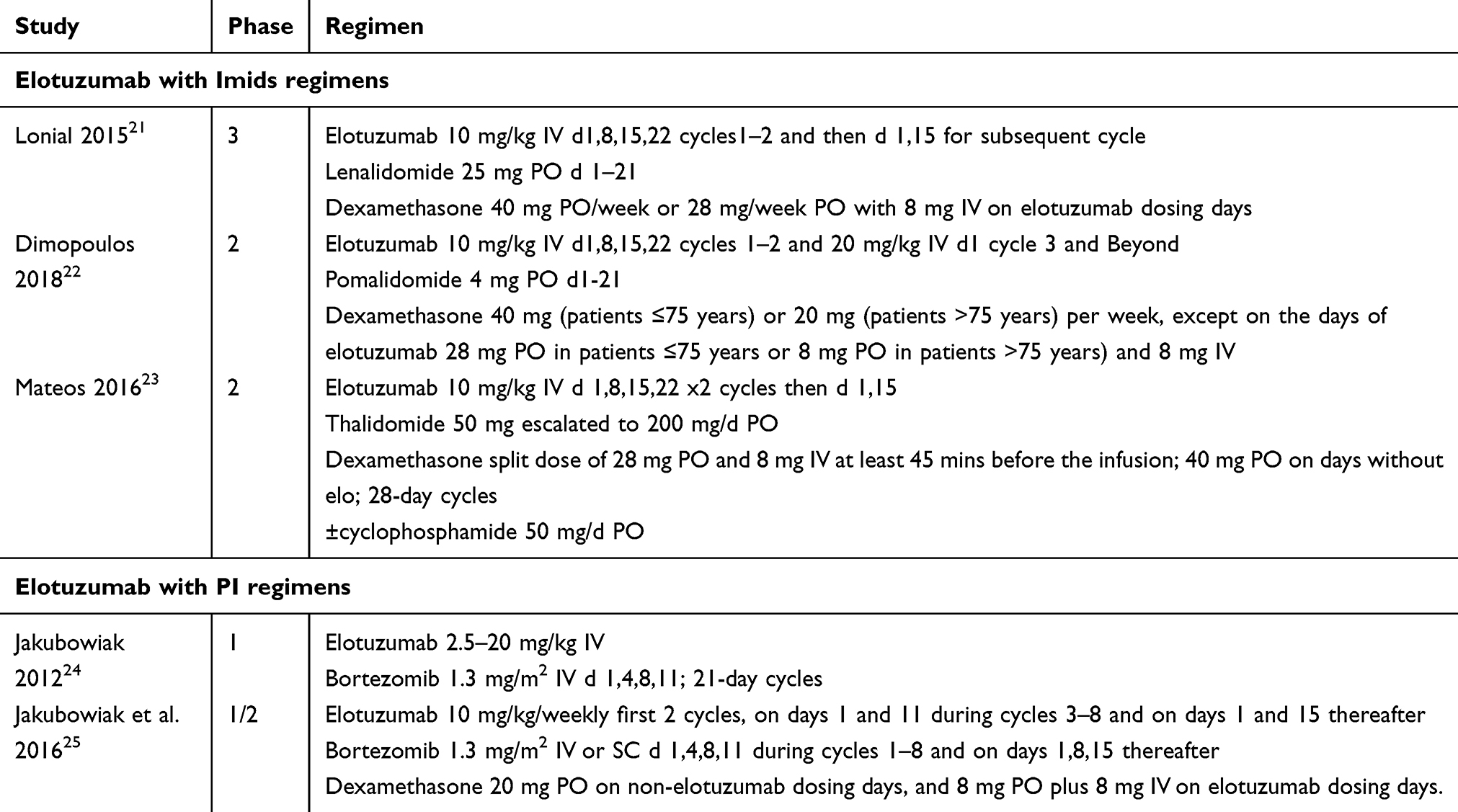 |
Table 2 Administration schemes of elotuzumab-based regimen |
A Phase 2 trial evaluated elotuzumab (10 or 20 mg/kg) in combination with lenalidomide and dexamethasone in 73 patients with RRMM.20 Of note, none of these patients were previously exposed to lenalidomide. The triplet combination elotuzumab, lenalidomide and dexamethasone (Elo-Rd) led to an ORR of 84%, including 14% of stringent complete response and 42% of VGPR. The 10 mg/kg cohort was associated with a better efficacy with a median PFS of 32 versus 25 months in the 20 mg/kg cohort. Addition of elotuzumab was not associated with an increased toxicity from those expected from the doublet lenalidomide and dexamethasone. Based on the results of these studies, the dose of 10 mg/kg was therefore identified for further studies.20
The Elo-Rd triplet was then evaluated in a large Phase III trial (ELOQUENT-2) that enrolled 646 patients with RRMM (1–4 prior lines; median of 2). Patients were assigned to receive lenalidomide and dexamethasone with or without elotuzumab (10 mg/kg) until progression or unacceptable toxicity.21,22,26 Less than 10% of patients had been previously exposed to lenalidomide and none was refractory. With a median follow-up of 33 months, Elo-Rd resulted in a higher ORR (79% versus 66% in the control group; p<0.001), including 4% of complete response (CR) and 28% of VGPR, and an improvement in median PFS of 19.4 months versus 14.9 months with lenalidomide and dexamethasone (Rd) alone (HR 0.70, 95% CI 0.60–0.89; p<0.001). Interference in estimation of the monoclonal spike in patients receiving mAbs could explain the decreased CR rates in the elotuzumab group seen in the Phase III ELOQUENT-2 study (4% in Elo-Rd vs 7% in Rd).21 Subgroup analysis demonstrated similar efficacy across age groups and disease risk groups, including del(17p) or t(4;14) abnormalities. Median OS was also improved; 43.7 months in Elo-Rd versus 39.6 months in the control group (HR 0.77, 95% CI 0.61–0.97; p=0.0257). Elotuzumab did not appear to be associated with impairment of overall health-related quality of life despite longer treatment administration due to intravenous infusion. Based on this study, elotuzumab was approved by the US Food and Drug Administration (FDA) in combination with lenalidomide and dexamethasone (Rd) for the treatment of patients with MM who have received 1 to 3 prior therapies.
Pomalidomide
ELOQUENT-3 Phase II trial enrolled 117 patients with RRMM (at least two prior lines, refractory to their last treatment and refractory to lenalidomide and a PI) assigned to receive pomalidomide and dexamethasone (Pd) with or without elotuzumab.22 Patients had previously received a median of 3 (2–8) lines of therapy. Elotuzumab, pomalidomide and dexamethasone (Elo-Pd) resulted in a higher ORR (53% versus 26%) when compared to pomalidomide and dexamethasone (Pd) cohort, including 3% CRs, 5% CR and 12% VGPR, with a median time to response of 2 months. Results of this study showed improved PFS with no incremental toxic effects, compared with lenalidomide and dexamethasone alone (median PFS 10.3 months in Elo-Pd group versus 4.7 months; HR 0.54; 95% CI 0.34–0.86). Although OS data are still immature, there is a trend favoring the elotuzumab arm (HR 0.62; 95% CI 0.30–1.28). Based on these results, elotuzumab has been approved by the US FDA for use in combination with pomalidomide and dexamethasone (Pd) in patients who have received at least two prior therapies, including lenalidomide and a PI.
Thalidomide
A Phase II study investigated elotuzumab in combination with thalidomide and dexamethasone with/without addition of cyclophosphamide according to response.23 Forty patients with RRMM were included (median of three prior therapies), including 98% and 73% of patients previously exposed to bortezomib and lenalidomide, respectively. The ORR was 38%, including 18% achieving VGPR or better. The median PFS was 3.9 months and the median OS was 16.3 months. Overall, no increased toxicity was observed with addition of elotuzumab. These efficacy results are clearly inferior to those achieved with Elo-Rd or Elo-Pd. Moreover, thalidomide was associated with peripheral neuropathy mostly of grades 1–2 in 20% of patients and grades 3–4 in 3% of patients.
Elotuzumab in combination with bortezomib
Combination with elotuzumab and bortezomib (Elo-V) was evaluated in a Phase I study that enrolled 28 RRMM patients (median of two prior therapies), including 39% of patients that were previously exposed to bortezomib. The scheme of elotuzumab administration in combination with PIs is reported in Table 2. The ORR was 48%, including 7% of complete response (CR).24 The median time to progression was 9.46 months. These favorable efficacy results were confirmed in a randomized Phase II study that compared elotuzumab (10 mg/kg), bortezomib and dexamethasone (Elo-Vd) over bortezomib and dexamethasone (Vd) in 152 patients with RRMM (1–3 prior therapies).25 Half of the patients (49%) were previously exposed, but not refractory to bortezomib. In both arms, treatment was given until disease progression or unacceptable toxicity. Despite similar ORR between the two cohorts (66% versus 63%), the addition of elotuzumab demonstrated an improvement in PFS in patients with RRMM that did not however reach statistical significance (median 9.7 versus 6.9 months; HR 0.72, 95% CI 0.49–1.06; p=0.09).
Safety and practical considerations
Infusion-related reactions
Initial Phase I study of single-agent elotuzumab was associated with IRR in 58.8% of patients. IRR consisted mostly on chills, fatigue, pyrexia, nausea and back pain.18 In the Phase III trial ELOQUENT-2 (Elo-Rd), IRR were reported in 33 (10%) of patients in the elotuzumab arm. Again, IRR were mostly grade 1/2 with only 4 patients with grade 3 reactions (no grade 4 or 5). Most (70%) of these reactions occurred during the first infusion. Only two patients (1%) discontinued treatment because of the infusion reaction. Very similar IRR rates and grade were observed in the randomized ELOQUENT-3 trial (Elo-Pd). These reactions might be related to the direct effects of elotuzumab on immune-effector cells and increase in pro-inflammatory cytokines.28
Premedication with steroids, acetaminophen and antihistamines within 30–60 mins prior to elotuzumab infusion is recommended and strongly diminished the frequency of these reactions.28 Prevention and prompt management of infusion reactions is then important to avoid drug discontinuation which may affect treatment efficacy. Close monitoring of patients, especially during the first infusion, is thus recommended.
Other adverse events
Overall, except from IRR, the addition of elotuzumab to standard regimens including IMiDs or PI is not associated with increased toxicity from those expected with these regimens without elotuzumab.
Hematologic toxicities
Based on the ELOQUENT 2 (Elo-Rd) and 3 (Elo-Pd) trials, rates of anemia, thrombocytopenia and neutropenia were similar in the elotuzumab and control groups.21,27 Rates of grades 3 and 4 lymphocytopenia were however significantly higher rate (77% vs 49%) with elotuzumab in the ELOQUENT 2 trial.21 However, in the ELOQUENT 3 trial, grades 3–4 lymphocytopenia were not significantly different (8% vs 2%).22 Since elotuzumab has no expression of SLAMF7 protein in hematopoietic progenitor cells, it has a lower myelosuppressive profile than daratumumab.14
Infections
Overall rate of infections was not increased with the addition of elotuzumab. However, rate of viral infections with herpes zoster (grade 1/2) was greater in the elotuzumab group than in the control group in both ELOQUENT 2 trial (4.1% vs 2.2%) and ELOQUENT 3 trial (5% vs 2%).21,23 Initiation of prophylaxis against herpes zoster reactivation, such as acyclovir or valacyclovir, is recommended.28 Except for herpes zoster, there was no increase in the incidence of opportunistic infections.
Quality of life
Importantly, quality of life and pain evaluation were assessed using the Brief Pain Inventory-Short Form and the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30 module (QLQ-C30) and myeloma-specific module (QLQ-MY20). Baseline pain and quality of life scores did not change substantially throughout treatment with both regimens, which supports the tolerability and safety of the mAb.29
Practical considerations
Dose adaptation and drug interaction
Analysis of elotuzumab pharmacokinetic properties according to renal impairment, hepatic impairment and age support its use in patients with those conditions without dose adjustment.30 The clearance of elotuzumab increased according to body weight, supporting weight-based dosing. Since formal drug to drug interaction studies are missing, no drug interaction is identified with elotuzumab.
Interference with response monitoring
Unlike CD38 mAbs, elotuzumab does not interfere with blood compatibility tests because SLAMF7 is not expressed on red blood cells.14 However, elotuzumab is a humanized IgG kappa mAb potentially doing comigration with the patient’s monoclonal protein which is often detected on routine serum protein electrophoresis and immunofixation for monitoring disease response. This interference can lead to a small overestimation of the monoclonal spike and affects assessment of response according to International Myeloma Working Group (IMWG) criteria.31 Strategies to overcome this interference based on shifting the therapeutic antibody band have been developed, but, unfortunately, none is currently available. Dosing soluble levels of SLAMF7 as an indicator of disease burden in MM could be a potential option for determining response to elotuzumab therapy.32
How to integrate elotuzumab in the treatment of relapsed myeloma
The therapeutic landscape for RRMM who received 1–3 prior lines of therapy has dramatically evolved in the past years. Several Phase III randomized trials lead to the approval by the FDA and European Medicines Agency of new combination therapies for these patients. These new options include IMiDs-based combinations (ie, carfilzomib, lenalidomide and dexamethasone [KRd], ixazomib, lenalidomide and dexamethasone [IRd], EloRd and daratumumab, lenalidomide and dexamethasone [DaraRd])8,21,33,34,35 and PI-based combinations (ie, carfilzomid and dexamethasone [Kd], panobinostat, bortezomib and dexamethasone [PanoVd], daratumumab, bortezomib and dexamethasone [DaraVd]).7,36,37,38 Approved options for RRMM who received at least one prior therapy are summarized in Table 3. The choice of the best therapy, including elotuzumab, depends on the patient and disease characteristics, previous lines of therapy and the availability of these combinations.
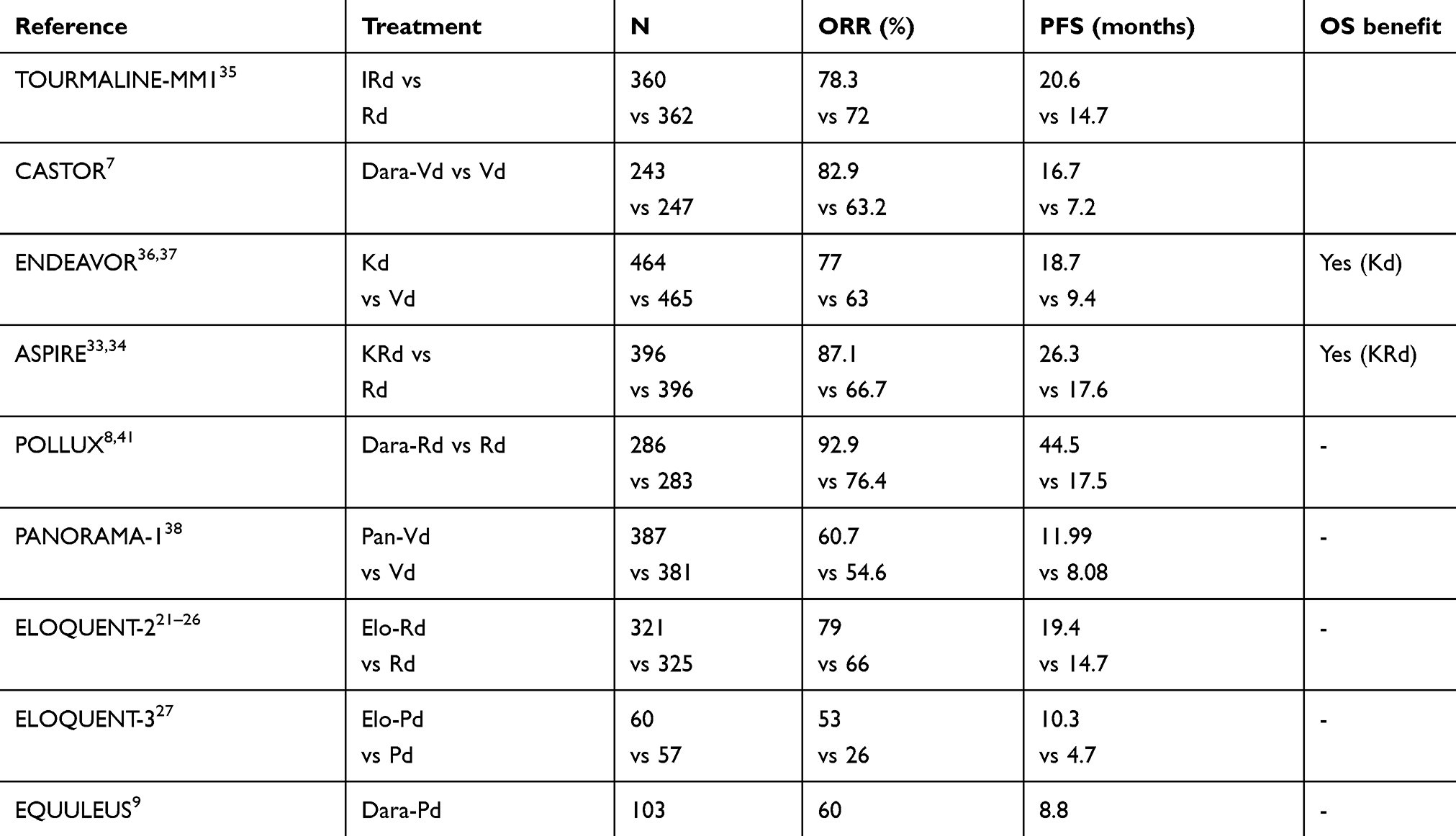 |
Table 3 Approved options for RRMM who received at least 1 prior therapy |
Elotuzumab approval and therapeutic alternatives in RRMM
Because of the paucity of clinical results obtained with elotuzumab monotherapy, elotuzumab is not a recommended option as a single agent treatment for MM patients.
Results obtained from a combination of elotuzumab with bortezomib are disappointing. Duration and depth of response with Elo-Vd are not significantly improved versus Vd.24,25 Moreover, we have other PI-based options, including Kd and DaraVd that demonstrated significant PFS benefit in comparison with Vd.7,36 The triplet combination PanoVd has also demonstrated improved PFS in comparison with Vd but is associated significant gastrointestinal and hematologic toxicities.37
On the other hand, elotuzumab demonstrated strong efficacy when combined to the IMids-based regimens Rd and Pd.21,27 The potency of these combinations might be related to the mechanism of action of IMiDs that have immunostimulatory effects that induce activation of NK cells and enhanced ADCC activity.39,40 Both randomized trials with Elo-Rd (ELOQUENT-2) and Elo-Pd (ELOQUENT-3) have demonstrated a statistically significant benefit in PFS when compared to the control arm.21,27 Based on the result of the ELOQUENT-2 trial, the FDA approved elotuzumab in combination with lenalidomide and dexamethasone (Elo-Rd) for RRMM who have received at least one prior line of therapy. For the treatment of patients with RRMM, lenalidomide has also been studied in combination with carfilzomib (KRd), ixazomib (IRd) and daratumumab (DaraRd).8,33,35 In terms of response PFS, the triplet DaraRd led to better results in comparison with Elo-Rd, with similar safety profiles. Indeed, the median PFS with DaraRd was 40 months versus 19.4 months for Elo-Rd.41 In terms of survival, only KRd demonstrated an OS advantage over Rd at this time.34
Results from the ELOQUENT-3 trial also led to FDA approval of elotuzumab in combination with pomalidomide and dexamethasone for RRMM who have received at least two prior lines of therapy and refractory to PI and lenalidomide. There are ongoing studies with combination of anti-CD38 mAbs, daratumumab and isatuximab, with pomalidomide and dexamethasone in the setting of RRMM. Association of carfilzomib with pomalidomide and dexamethasone (KPd) is difficult to compare with Elo-Pd since PFS was inferior (7,3 months) in one trial but it included a population of patients with more advance disease with a median of six prior lines of treatment.42 The other study with KPd was associated with a similar PFS of 10.3 months.43 KPd combination is not yet approved. Alternative option of treatment with pomalidomide in RRMM is pomalidomide, cyclophosphamide and dexamethasone (PCD). As published by Baz et al, PCD was associated with an ORR of 65% and a PFS of 9.5 months.44 The efficacy of PCD has been recently confirmed in the real-life setting.43,45 Elo-Pd compares favorably to PCD in term of efficacy but at a higher cost therapy and less convenient than the all-oral triplet. A large Phase Ib study reported the promising efficacy of the triplet combination of pomalidomide dexamethasone and daratumumab (Dara-Pd) in 103 patients with advanced MM (median of four prior therapies, 20% refractory to lenalidomide). The ORR was 60% and the median PFS was 8.8 months.9
When choosing the optimal regimen for a patient, profile of toxicities have also to been taken into consideration and balanced according to patients’ comorbidity. The addition of elotuzumab to IMiDs-based therapy allows a favorable safety profile.
Patients selection: elotuzumab-based therapy in specific subgroups of patients?
The addition of elotuzumab to Rd resulted in improved PFS over control arms for patients with high-risk cytogenetic, including t(4;14) and 17p deletion.21 Subgroups analysis of the ELOQUENT-2 trial shown a PFS benefit of the addition of elotuzumab for patients with deletion 17p (HR 0,65; 95% CI, 0,45–0,94), 1q21 gain (HR 0,75; 95% CI, 0,56–0,99) and t(4,14) (HR 0,53; 95% CI, 0,29–0,95). In the ELOQUENT-3 trial, a trend to a better PFS was also seen for patients with high-risk cytogenetic, as defined by the IMWG, in the Elo-Pd arm.27 However, analysis of each subgroup of patients deletion 17 p, 1q21 and t(4,14) failed to demonstrate a benefit in PFS from the addition of elotuzumab. In ELOQUENT-2 trial, the PFS benefit of elo-Rd was consistent across different subgroups of patients, including those older than 65 years (HR 0,65; 95% CI, 0,50–0,85), ISS I (HR 0,13; 95% CI, 0,46–0,87) and those with creatinine clearance inferior to 60 mL/min (HR 0,56; 95% CI, 0,31–0,88). Although there was not benefit in PFS for the subgroup of patients older than 65 years in the ELOQUENT-3 trial, those with ISS I-II (HR 0,54; 95% CI, 033–0,90) and those with disease refractory to lenalidomide and a PI (HR 0,56; 95% CI, 0,33–0,97) did benefit from the addition of elotuzumab to Pd. For patients with extra-medullary disease, the impact of elotuzumab is not known.
Biomarkers predicting response to targeted therapy are needed. Some factors have been hypothesized to further help to predict response to elotuzumab therapy, such as dosing soluble SLAMF7 in serum or identification of Fc RIIIA V allele homozygous status. These factors are however not validated for current use in practice. The majority of the patients who do respond eventually develop resistance and antibodies against mAbs eventually develop and reduce their biological activity, as documented in 15% of patients in the Phase III trial in combination with lenalidomide and dexamethasone.21
Elotuzumab-based therapy: an option for patients refractory to CD38 mAbs?
To date, there are no data available about retreatment with a mAb in MM patients refractory to another mAb. Patients previously treated with a mAb are usually excluded from clinical trials testing other mAbs in RRMM. Since mAbs are now approved until progression in previously untreated MM patients based on the results of the Phase III ALCYONE and MAIA trials, most patients with RRMM will be daratumumab refractory in the next future.10,46 Since daratumumab and elotuzumab have different mechanisms of action, one targeting CD38 and the other SLAMF7, combination treatment with elotuzumab could be likewise an option treatment for anti-CD38 refractory RRMM. However, studies are needed to confirm the efficacy and safety of elotuzumab in patients that are refractory to anti-CD38 mAbs.
Ongoing studies
Multiple of other mAbs are now been tested in RRMM. Combination of elotuzumab, carfilzomib, pomalidomide and dexamethasone in RRMM is actually under investigation in a Phase II trial (NCT03155100). Phase II trial elotuzumab, pomalidomide, bortezomib and dexamethasone in RRMM (Elo-PVd) is also recruiting (NCT02718833). A Phase III study of lenalidomide and dexamethasone with or without elotuzumab in newly diagnosed patients with MM (ELOQUENT-1) is underway (NCT01335399). Elotuzumab is also investigated in combination with bortezomib, lenalidomide and dexamethasone (VRd) in newly diagnosed myeloma (NDMM) eligible for transplant in Phase II trials (NCT02375555, NCT02495922). Elotuzumab combined with carfilzomib, lenalidomide and dexamethasone is investigated in NDMM (NCT02969837). A Phase II trial with combination of elotuzumab plus lenalidomide/dexamethasone is under investigation for high-risk SMM (NCT02279394).
Conclusion
Elotuzumab demonstrated a significant clinical activity in combination with IMiDs and is approved in combination with lenalidomide and dexamethasone (Elo-Rd) and pomalidomide and dexamethasone (Elo-Pd) in RRMM patients. Elotuzumab displays a safe profile with lower rate of IRR (<10%) compared to daratumumab. Elotuzumab in combination with IMiDs is an approved option for the treatment of RRMM. Taking into consideration that most patients will be treated with anti-CD38 mAbs in first line of treatment, it may be hypothesized that elotuzumab in combination could be a future option treatment for RRMM patients with anti-CD38 refractory disease.
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
CT and PM are members of Site de Recherche Intégrée sur le Cancer (SIRIC) ILIAD (INCA-DGOS-Inserm_12558). CT and PM are advisory board members and have received honoraria from Celgene. PM reports personal fees from Celgene, Janssen, Amgen, Takeda and AbbVie, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7–30. doi:10.3322/caac.21442
2. Moreau P, San Miguel J, Sonneveld P, et al. Multiple myeloma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017;28(suppl_4):iv52–iv61. doi:10.1093/annonc/mdx096
3. Kumar SK, Rajkumar SV, Dispenzieri A, et al. Improved survival in multiple myeloma and the impact of novel therapies. Blood. 2008;111(5):2516–2520. doi:10.1182/blood-2007-10-116129
4. Kumar SK, Dimopoulos MA, Kastritis E, et al. Natural history of relapsed myeloma, refractory to immunomodulatory drugs and proteasome inhibitors: a multicenter IMWG study. Leukemia. 2017;31(11):2443–2448. doi:10.1038/leu.2017.138
5. Touzeau C, Moreau P, Dumontet C. Monoclonal antibody therapy in multiple myeloma. Leukemia. 2017;31(5):1039–1047. doi:10.1038/leu.2017.60
6. Lonial S, Weiss BM, Usmani SZ, et al. Daratumumab monotherapy in patients with treatment-refractory multiple myeloma (SIRIUS): an open-label, randomised, phase 2 trial. Lancet. 2016;387(10027):1551–1560. doi:10.1016/S0140-6736(15)01120-4
7. Palumbo A, Chanan-Khan A, Weisel K, et al. Daratumumab, bortezomib, and dexamethasone for multiple myeloma. N Engl J Med. 2016;375(8):754–766. doi:10.1056/NEJMoa1606038
8. Dimopoulos MA, Oriol A, Nahi H, et al. Daratumumab, lenalidomide, and dexamethasone for multiple myeloma. N Engl J Med. 2016;375(14):1319–1331. doi:10.1056/NEJMoa1607751
9. Chari A, Lonial S, Suvannasankha A, et al. Open-label, multicenter, phase 1b study of daratumumab in combination with pomalidomide and dexamethasone in patients with at least 2 lines of prior therapy and relapsed or relapsed and refractory multiple myeloma. Blood. 2015;126:5085.
10. Mateos M-V, Dimopoulos MA, Cavo M, et al. Daratumumab plus bortezomib, melphalan, and prednisone for untreated myeloma. N Engl J Med. 2017. doi:10.1056/NEJMoa1714678
11. Touzeau C, Moreau P. Daratumumab for the treatment of multiple myeloma. Expert Opin Biol Ther. 2017;17(7):887–893. doi:10.1080/14712598.2017.1322578
12. Kumaresan PR, Lai WC, Chuang SS, Bennett M, Mathew PA. CS1, a novel member of the CD2 family, is homophilic and regulates NK cell function. Mol Immunol. 2002;39(1–2):1–8.
13. Tai Y-T, Dillon M, Song W, et al. Anti-CS1 humanized monoclonal antibody HuLuc63 inhibits myeloma cell adhesion and induces antibody-dependent cellular cytotoxicity in the bone marrow milieu. Blood. 2008;112(4):1329–1337. doi:10.1182/blood-2007-08-107292
14. Hsi ED, Steinle R, Balasa B, et al. CS1, a potential new therapeutic antibody target for the treatment of multiple myeloma. Clin Cancer Res. 2008;14(9):2775–2784. doi:10.1158/1078-0432.CCR-07-4246
15. Pazina T, James AM, MacFarlane AW, et al. The anti-SLAMF7 antibody elotuzumab mediates NK cell activation through both CD16-dependent and -independent mechanisms. Oncoimmunology. 2017;6(9):e1339853. doi:10.1080/2162402X.2017.1339853
16. Krejcik J, Casneuf T, Nijhof IS, et al. Daratumumab depletes CD38+ immune regulatory cells, promotes T-cell expansion, and skews T-cell repertoire in multiple myeloma. Blood. 2016;128(3):384–394. doi:10.1182/blood-2015-12-687749
17. Ishibashi M, Soeda S, Sasaki M, et al. Clinical impact of serum soluble SLAMF7 in multiple myeloma. Oncotarget. 2018;9(78):34784–34793. doi:10.18632/oncotarget.26196
18. Zonder JA, Mohrbacher AF, Singhal S, et al. A phase 1, multicenter, open-label, dose escalation study of elotuzumab in patients with advanced multiple myeloma. Blood. 2012;120(3):552–559. doi:10.1182/blood-2011-06-360552
19. Lonial S, Vij R, Harousseau J-L, et al. Elotuzumab in combination with lenalidomide and low-dose dexamethasone in relapsed or refractory multiple myeloma. J Clin Oncol. 2012;30(16):1953–1959. doi:10.1200/JCO.2011.37.2649
20. Richardson PG, Jagannath S, Moreau P, et al. Elotuzumab in combination with lenalidomide and dexamethasone in patients with relapsed multiple myeloma: final phase 2 results from the randomised, open-label, phase 1b-2 dose-escalation study. Lancet Haematol. 2015;2(12):e516–e527. doi:10.1016/S2352-3026(15)00197-0
21. Lonial S, Dimopoulos M, Palumbo A, et al. Elotuzumab therapy for relapsed or refractory multiple myeloma. N Engl J Med. 2015;373(7):621–631. doi:10.1056/NEJMoa1505654
22. Dimopoulos MA, Lonial S, Betts KA, et al. Elotuzumab plus lenalidomide and dexamethasone in relapsed/refractory multiple myeloma: extended 4-year follow-up and analysis of relative progression-free survival from the randomized ELOQUENT-2 trial. Cancer. 2018;124(20):4032–4043. doi:10.1002/cncr.31680
23. Mateos M-V, Granell M, Oriol A, et al. Elotuzumab in combination with thalidomide and low-dose dexamethasone: a phase 2 single-arm safety study in patients with relapsed/refractory multiple myeloma. Br J Haematol. 2016;175(3):448–456. doi:10.1111/bjh.14263
24. Jakubowiak AJ, Benson DM, Bensinger W, et al. Phase I trial of anti-CS1 monoclonal antibody elotuzumab in combination with bortezomib in the treatment of relapsed/refractory multiple myeloma. J Clin Oncol. 2012;30(16):1960–1965. doi:10.1200/JCO.2011.37.7069
25. Jakubowiak A, Offidani M, Pégourie B, et al. Randomized phase 2 study: elotuzumab plus bortezomib/dexamethasone vs bortezomib/dexamethasone for relapsed/refractory MM. Blood. 2016;127(23):2833–2840. doi:10.1182/blood-2016-01-694604
26. Dimopoulos MA, Lonial S, White D, et al. Elotuzumab plus lenalidomide/dexamethasone for relapsed or refractory multiple myeloma: ELOQUENT-2 follow-up and post-hoc analyses on progression-free survival and tumour growth. Br J Haematol. 2017;178(6):896–905. doi:10.1111/bjh.14787
27. Dimopoulos MA, Dytfeld D, Grosicki S, et al. Elotuzumab plus pomalidomide and dexamethasone for multiple myeloma. N Engl J Med. 2018;379(19):1811–1822. doi:10.1056/NEJMoa1805762
28. Laubach JP, van de Donk N, Davies FE, Mikhael J. Practical considerations for antibodies in myeloma. Am Soc Clin Oncol Educ Book. 2018;(38):667–674. doi:10.1200/EDBK_205443
29. Cella D, McKendrick J, Kudlac A, et al. Impact of elotuzumab treatment on pain and health-related quality of life in patients with relapsed or refractory multiple myeloma: results from the ELOQUENT-2 study. Ann Hematol. 2018;97(12):2455–2463. doi:10.1007/s00277-018-3469-4
30. Berdeja J, Jagannath S, Zonder J, et al. Pharmacokinetics and safety of elotuzumab combined with lenalidomide and dexamethasone in patients with multiple myeloma and various levels of renal impairment: results of a phase Ib study. Clin Lymphoma Myeloma Leuk. 2016;16(3):129–138. doi:10.1016/j.clml.2015.12.007
31. Kumar S, Paiva B, Anderson KC, et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol. 2016;17(8):e328–e346. doi:10.1016/S1470-2045(16)30206-6
32. Postelnek J, Neely RJ, Robbins MD, Gleason CR, Peterson JE, Piccoli SP. Development and validation of electrochemiluminescence assays to measure free and total sSLAMF7 in human serum in the absence and presence of elotuzumab. AAPS J. 2016;18(4):989–999. doi:10.1208/s12248-016-9912-3
33. Stewart AK, Rajkumar SV, Dimopoulos MA, et al. Carfilzomib, lenalidomide, and dexamethasone for relapsed multiple myeloma. N Engl J Med. 2015;372(2):142–152. doi:10.1056/NEJMoa1411321
34. Siegel DS, Dimopoulos MA, Ludwig H, et al. Improvement in overall survival with carfilzomib, lenalidomide, and dexamethasone in patients with relapsed or refractory multiple myeloma. J Clin Oncol. 2018;36(8):728–734. doi:10.1200/JCO.2017.76.5032
35. Moreau P, Masszi T, Grzasko N, et al. Oral ixazomib, lenalidomide, and dexamethasone for multiple myeloma. N Engl J Med. 2016;374(17):1621–1634. doi:10.1056/NEJMoa1516282
36. Dimopoulos MA, Moreau P, Palumbo A, et al. Carfilzomib and dexamethasone versus bortezomib and dexamethasone for patients with relapsed or refractory multiple myeloma (ENDEAVOR): a randomised, phase 3, open-label, multicentre study. Lancet Oncol. 2016;17(1):27–38. doi:10.1016/S1470-2045(15)00464-7
37. San-Miguel JF, Hungria VTM, Yoon -S-S, et al. Panobinostat plus bortezomib and dexamethasone versus placebo plus bortezomib and dexamethasone in patients with relapsed or relapsed and refractory multiple myeloma: a multicentre, randomised, double-blind phase 3 trial. Lancet Oncol. 2014;15(11):1195–1206. doi:10.1016/S1470-2045(14)70440-1
38. Dimopoulos MA, Goldschmidt H, Niesvizky R, et al. Carfilzomib or bortezomib in relapsed or refractory multiple myeloma (ENDEAVOR): an interim overall survival analysis of an open-label, randomised, phase 3 trial. Lancet Oncol. 2017;18:1327–1337. doi:10.1016/S1470-2045(17)30578-8
39. Quach H, Ritchie D, Stewart AK, et al. Mechanism of action of immunomodulatory drugs (IMiDS) in multiple myeloma. Leukemia. 2010;24(1):22–32. doi:10.1038/leu.2009.236
40. Hayashi T, Hideshima T, Akiyama M, et al. Molecular mechanisms whereby immunomodulatory drugs activate natural killer cells: clinical application. Br J Haematol. 2005;128(2):192–203. doi:10.1111/j.1365-2141.2004.05286.x
41. Bahlis N, Dimopoulos M, White D. Benboubker, L. Three-Year Follow up of the Phase 3 Pollux Study of Daratumumab Plus Lenalidomide and Dexamethasone (D-Rd) versus Lenalidomide and Dexamethasone (Rd) Alone in Relapsed or Refractory Multiple Myeloma (RRMM). Blood. 2019;132(Suppl 1):1996.
42. Shah JJ, Stadtmauer EA, Abonour R, et al. Carfilzomib, pomalidomide, and dexamethasone for relapsed or refractory myeloma. Blood. 2015;126(20):2284–2290. doi:10.1182/blood-2015-05-643320
43. Bringhen S, Mina R, Cafro AM, et al. Once-weekly carfilzomib, pomalidomide, and low-dose dexamethasone for relapsed/refractory myeloma: a phase I/II study. Leukemia. 2018;32(8):1803–1807. doi:10.1038/s41375-018-0024-1
44. Baz RC, Martin TG, Lin H-Y, et al. Randomized multicenter phase II study of pomalidomide, cyclophosphamide, and dexamethasone in relapsed refractory myeloma. Blood. 2016;127:2561–2568. doi:10.1182/blood-2015-11-682518
45. Trudel S, Tessoulin B, Jullien M, et al. Pomalidomide, cyclophosphamide, and dexamethasone for relapsed/refractory multiple myeloma patients in a real-life setting: a single-center retrospective study. Ann Hematol. 2019;98:1441–1447. doi:10.1007/s00277-019-03649-3
46. Facon T, Kumar SK, Plesner T, et al. Phase 3 Randomized Study of Daratumumab Plus Lenalidomide and Dexamethasone (D-Rd) Versus Lenalidomide and Dexamethasone (Rd) in Patients with Newly Diagnosed Multiple Myeloma (NDMM) Ineligible for Transplant (MAIA). Blood. 2018;132(Suppl1):
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.