Back to Journals » Psychology Research and Behavior Management » Volume 16
Unveiling Gender Dysphoria Experiences in Turkish Young Adults: Challenges, Perspectives, and Implications in Health Care Settings
Authors Çarkaxhiu Bulut G, Yorguner N
Received 20 September 2023
Accepted for publication 21 October 2023
Published 25 October 2023 Volume 2023:16 Pages 4315—4327
DOI https://doi.org/10.2147/PRBM.S437197
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Gresa Çarkaxhiu Bulut,1 Nese Yorguner2
1Department of Psychology, Galata University, Istanbul, Turkey; 2Department of Psychiatry, Marmara University Medical School, Istanbul, Turkey
Correspondence: Gresa Çarkaxhiu Bulut, Department of Psychology, Galata University, Evliya Çelebi Mahallesi, Meşrutiyet Caddesi No: 62, Tepebaşı/Beyoğlu, Istanbul, 34421, Turkey, Tel +905337489381, Fax +905370135982, Email [email protected]
Purpose: Gender dysphoria (GD) emerged as a focal area in child and adolescent development research. While the intricacies of diagnosis and interventions for GD intertwine with diverse socio-cultural challenges, a notable dearth of knowledge exists about the experiences of transgender (TG) individuals during their formative years in Turkey. This study aims to unveil these experiences, shedding light on the challenges, perspectives, and implications in health care settings.
Patients and Methods: Our study encompassed 125 participants: 62 TGs under clinical follow-up, and a control group of 63 cisgender individuals. Surveys tailored to TG participants addressed early GD experiences, gender-typed activity participation, and psychosocial challenges from childhood through adolescence. Additionally, both cohorts contributed to a survey on attitudes towards community-based interventions, allowing for a comparative analysis of their perspectives.
Results: TGs identified their GD around age 10.77. Female-to-male TGs showed more involvement in traditionally male-associated activities, whereas male-to-female engaged more in female-associated domestic role-plays (p< 0.001). Over a third (37.09%) faced ostracization or bullying due to GD, 45.16% encountered verbal abuse, and 12.90% reported physical violence. Additionally, 40.32% had undergone treatment for depression and anxiety disorders. Most participants supported awareness initiatives, advocating for open gender expression, and normalizing the experiences of TG youth. Furthermore, 88.71% of TGs emphasized the importance of enhancing the expertise of professional groups, such as medical and mental health practitioners, in GD matters, a sentiment echoed by 68.25% of cisgender participants (p=0.030). While medical interventions were the least favored strategy at 32.80% overall, 46.78% of TGs supported it, compared to 19.05% of controls (p=0.010).
Conclusion: Our study underscores the challenges faced by TG individuals during development. Early recognition, societal awareness, enhanced training in professional healthcare environments, and comprehensive support are crucial for fostering acceptance and reducing adversity among children and adolescents navigating GD.
Keywords: gender dysphoria, mental health, health care, childhood play behaviors, psychosocial challenges, early interventions
Introduction
Gender dysphoria (GD), characterized by an incongruence between an individual’s experienced or expressed gender and their assigned gender, has become a focal point in recent research, particularly within the framework of child and adolescent development. Though once obscured by societal prejudices and medical misunderstandings, contemporary standpoints now emphasize the nuances associated with GD, thereby advocating for an in-depth analysis of this phenomenon.
Recent studies emphasize the early onset of GD.1 As the foundation for gender identity takes shape during early childhood, numerous findings suggest that feelings of incongruence arise during these foundational years, often carrying forward into adolescence.2 Consequently, early interventions become a contentious topic of discussion. The debate surrounding the diagnosis of GD during childhood and adolescence, followed by subsequent interventions, embodies a diverse mix of social, political, cultural, and moral issues. While biological findings have enriched our knowledge, they do not paint the full picture. Sociocultural determinants weigh in heavily.3,4 This debate also extends to early therapeutic interventions, which range from psychosocial interventions to hormone replacement therapies and surgical procedures. Traditionally, such interventions have been reserved for adults due to their irreversible and significant consequences. On the other hand, it is advocated that the postponement of these potential interventions may bring about the risk of augmenting the difficulties faced by adolescents with GD during their developmental phases.5 Evidence indicates that children and adolescents with GD grapple with a plethora of developmental challenges. Beyond academic underperformance and disrupted psychosocial development, their general functionality is often compromised.6 Societal biases intensify their challenges, with non-adherence to traditional gender norms often leading to discrimination, bullying, and exclusion. The larger environment often subjects transgender (TG) youth to rejection and other forms of victimization, thereby heightening their susceptibility to mental health challenges.7,8 These negative experiences can escalate into psychiatric conditions like depression and anxiety, rooted in deep-seated feelings of guilt and self-worth diminishment. Compounding these challenges, emerging data reveals that gender dysphoric adolescents exhibit higher rates of self-harm behaviors and suicidal attempts compared to their cisgender counterparts.9,10
In the context of GD, the sociocultural landscape and legal framework of a nation play a pivotal role in influencing its approach and interventions. Varied global perspectives, policies, and practices related to GD underscore the importance of localized research.11 Within the Turkish context, as observed in numerous other countries, a fervent discourse persists concerning the medical, legal, and ethical dimensions of GD. To devise multifaceted early interventions addressing the tribulations faced by gender dysphoric youth, contemporary evidence and scholarly contributions are imperative. Hence, this research endeavors to delve into the childhood and adolescent experiences of TG individuals in Turkey. Our objectives are to delve into the psychosocial, developmental, and behavioral nuances specific to Turkish TG individuals during their formative years; to identify the specific challenges they encountered in academic settings, within family dynamics, and in daily interactions; and to solicit their feedback on targeted community-based interventions and treatment strategies addressing these challenges. Through this focused exploration, we aim to deepen the understanding of TG experiences in Turkey, aspiring to guide tailored interventions for early support and the holistic well-being of young individuals.
Materials and Methods
Settings and Participants
The study was conducted within a specialized transgender care unit in a university hospital dedicated to individuals diagnosed with GD. The diagnosis of GD for the TG individuals was established by experienced specialists through elaborate and longitudinal clinical assessments. This comprehensive diagnostic process was supported by family interviews, psychometric tests, and other pertinent clinical tools to ensure accurate and robust diagnosis. Individuals under 18 years of age, those with severe psychiatric disorders, intellectual disabilities, or illiteracy were excluded from the sample. Eligible individuals were fully informed about the study’s purpose and protocol by the researchers in person, and detailed informed consent was obtained from those who volunteered to participate. In total, the study included 62 TG individuals (15 male-to-female, MTF and 47 female-to-male, FTM) who were undergoing clinical follow-up. The mean age of the transgender group was 25.69 (SD=4.49, range=19–37). Specifically, the FTMs had a mean age of 25.13 (SD=4.06) while the MTFs had a mean age of 25.87 (SD=4.65). Additionally, a control group of 63 cisgender participants (34 females and 29 males) was included to enable a comparative analysis of attitudes towards interventions addressing challenges faced by gender dysphoric individuals. Controls were primarily recruited from student groups and their relatives using the snowball sampling method. They fell within the same age range as the TG participants, and identical exclusion criteria were applied. The mean age for the cisgender group was 25.14 (SD=4.14, range=20–38), with females having a mean age of 25.52 (SD=4.65) and males a mean age of 24.67 (SD=4.12). Notably, the average ages of the groups were not significantly different (p=0.498).
Assessments
Sociodemographic data and pertinent information regarding past psychiatric treatment history were collected using a sociodemographic form. Furthermore, participants engaged in responding to four distinct sub-surveys, each tailored to gather specific information. These sub-surveys were developed by the researchers, drawing inspiration from questionnaires employed in similar studies within this field.
First Experiences Questionnaire: This is a 6-item questionnaire composed of open-ended questions. It aimed to gain insights into experiences such as the age at which participants first recognized their GD, the first time they shared their feelings of dysphoria with others, and when they began to exhibit behaviors associated with their identified gender.
Types of Games and Activities Questionnaire: This 6-item, Likert-type questionnaire evaluated participation and interest levels in games and activities that traditionally have a gender-specific association in childhood and adolescence. The items were adapted from Pre-school Activities Inventory (PSAI) and questionnaires from previous studies assessing gender-typed toy and activity preferences of children.12,13 Examples of these games and activities include house playing, guns and model cars, individual and team sports, and lego-chess.
Early Life Difficulties in GD Questionnaire: Comprising 8 Likert-type items, this questionnaire sought to understand the challenges – both direct and indirect – that participants faced in their childhood and adolescence because of GD. It also aimed to gauge frequent negative experiences and their perceived levels of social support.
Attitudes Towards Early Interventions in GD Questionnaire: This 5-item Likert-type questionnaire was designed to assess participants’ viewpoints and attitudes concerning proposed interventions. The suggested interventions were drawn from previous work in the field and are believed to help alleviate the challenges faced by individuals with GD during their childhood and adolescence.3,14,15
The research protocol and all associated materials were reviewed and approved by the Ethics Committee of Marmara University Medical School (approval number: 092019-1088).
Statistical Analysis
Statistical analyses were conducted using SPSS, version 24.0. Descriptive statistics were presented as counts, percentages, means, standard deviations, medians, and ranges. The Pearson Chi Square test was utilized to compare the distribution of categorical variables between the two independent groups. Mann–Whitney U-test was employed for non-normally distributed continuous variables. Given the multiple comparisons made within each category, we applied the Bonferroni correction to control the familywise error rate. The original significance threshold was set at α=0.05, but with the Bonferroni correction applied, the adjusted α varied depending on the number of tests in the respective category.
Results
First Experiences with GD
Participants reported recognizing their GD at an average age of 10.77 (SD=4.58) (Table 1). The average age for first disclosing their GD was 16.67 (SD=3.91). No statistically significant differences were observed between FTMs and MTFs in these ages (p=0.974 and p=0.736, respectively). The average age participants adopted a name that aligned with their felt gender was 14.80 (SD=7.51). While FTMs adopted a name that aligned with their felt gender at an earlier average age of 13.66 (SD=7.63) compared to MTFs, who averaged at 18.21 (SD=6.16), this difference was not statistically significant after applying the Bonferroni correction (p=0.014). On the other hand, FTMs began dressing in alignment with their felt gender at an earlier average age of 12.02 (SD=4.75) compared to MTFs’s 18.57 (SD=4.38) (p<0.001). The majority (53.22%) of participants first disclosed their GD to friends, while a mere 4.83% first shared it with their parents. No difference was noted in the disclosure preference between FTMs and MTFs (p=0.881). A minority (8%, n=5) had not informed their family of their GD; all of these were FTMs.
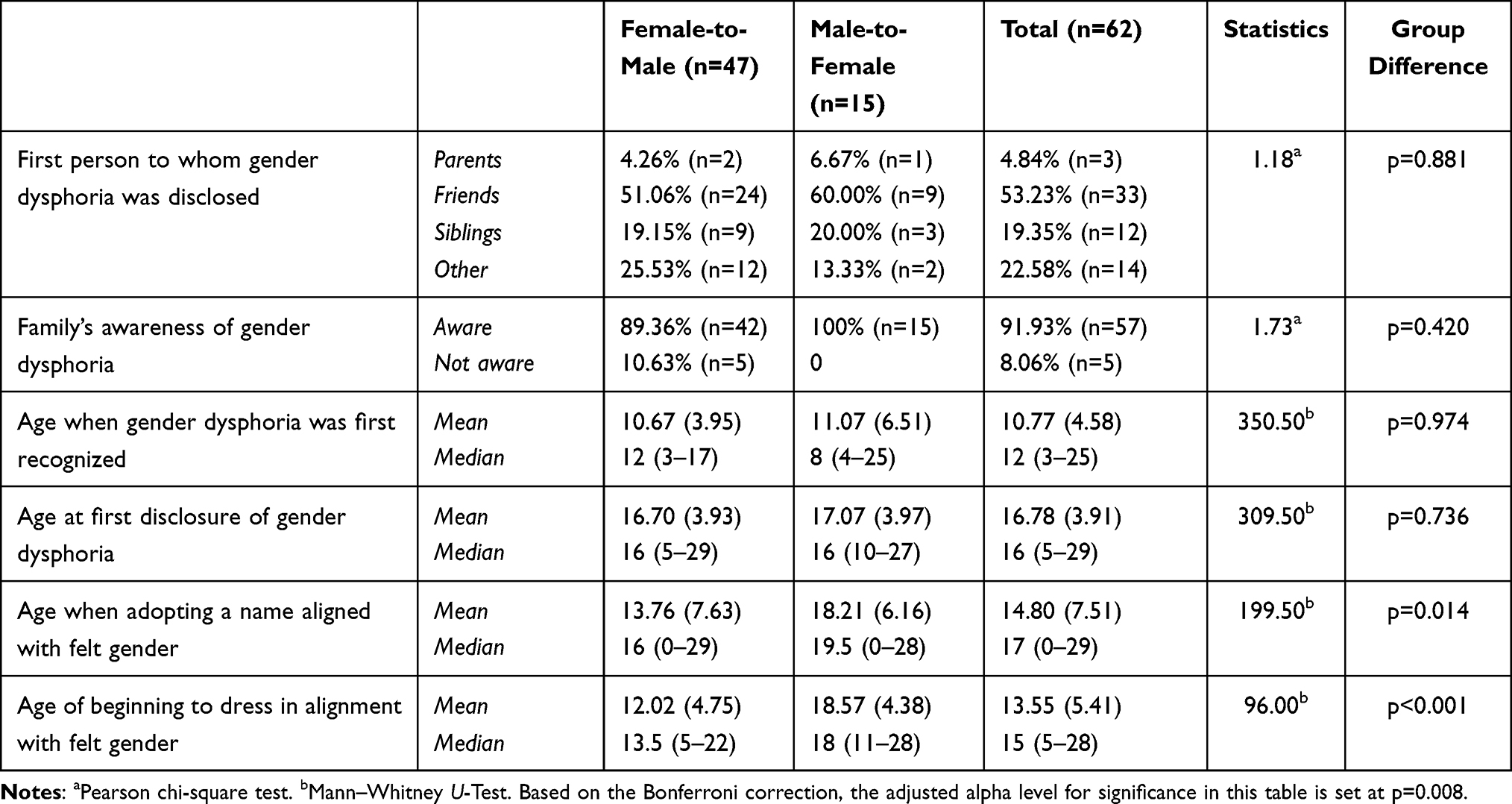 |
Table 1 Early Life Experiences with Gender Dysphoria |
Gender-Specific Activity Involvement During Childhood
Table 2 presents the engagement level in traditionally gender-specific activities and broader appeal activities during early childhood and adolescence for FTMs and MTFs. FTMs reported significantly higher rates of interest and participation in traditionally male-associated team sports like football and basketball (82.97% vs 13.33%; p<0.001) and male-associated toys like toy cars and action figures (72.34% vs 13.33%, p<0.001). They also showed more interest in constructive and creative activities such as model airplanes and Legos (48.93% vs 6.66%), although this difference did not reach statistical significance after applying the Bonferroni correction (p=0.025). Conversely, MTFs had significantly higher engagement rates in traditionally female-associated domestic role-play games (73.33% vs 2.12%, p<0.001). Notably, no differences were observed between FTMs and MTFs in involvement in neutral or broadly appealing individual sports or digital games and activities (p=0.252 and p=0.328, respectively).
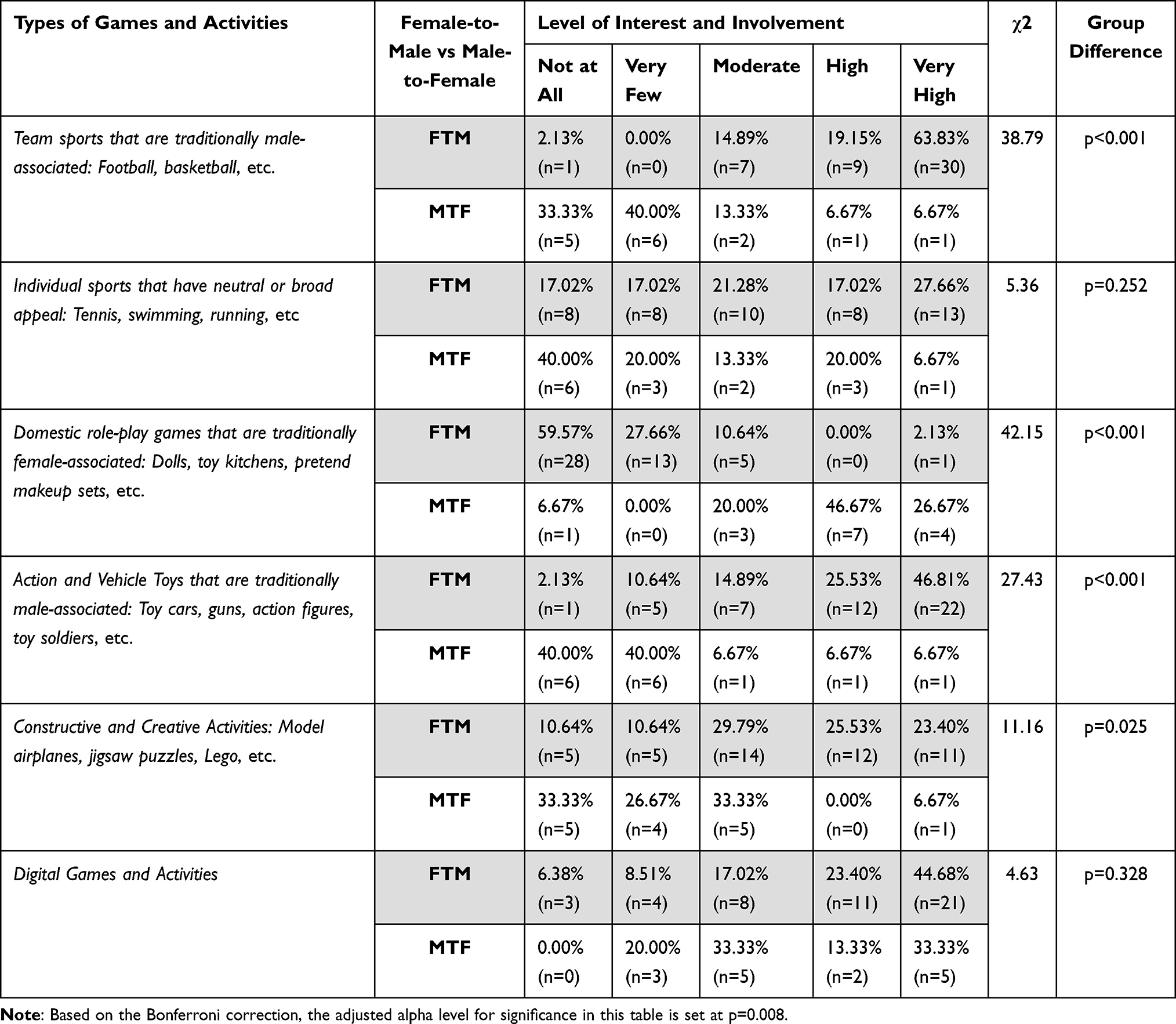 |
Table 2 Engagement Levels in Gender-Specific Games and Activities During Childhood and Adolescence |
Negative Experiences and Challenges
16.12% of participants reported seeking child psychiatry services during childhood or adolescence directly due to GD, while 20.96% sought these services due to indirect complications arising from GD, such as peer bullying and adjustment issues (Table 3). FTMs and MTFs displayed comparable rates of childhood psychiatric referrals (p=0.514). Excluding ongoing GD treatments, 40.32% of participants indicated that they received treatment for depression and anxiety disorder cluster diagnoses. Another 14.51% were treated for other psychiatric diagnoses such as OCD, eating disorders, and neurodevelopmental disorders.
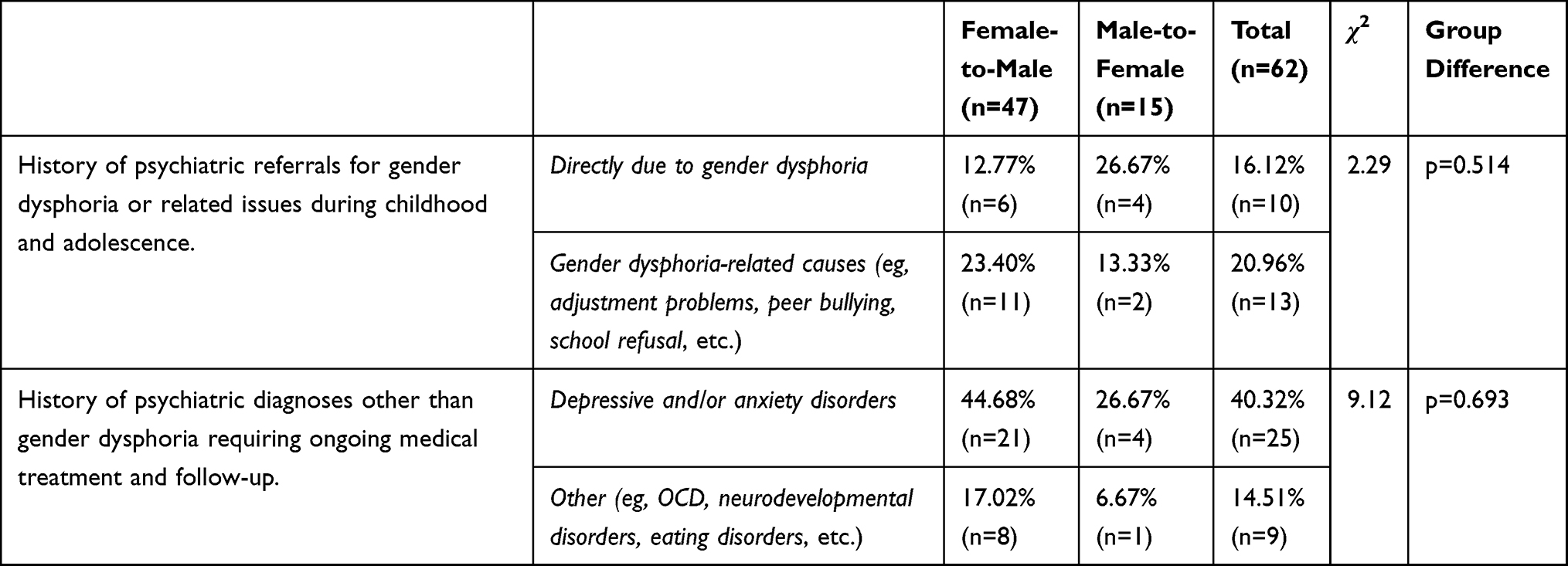 |
Table 3 Psychiatric Referrals and Diagnoses Related to Gender Dysphoria |
Table 4 illustrates the various adversities participants faced during their childhood due to GD. A significant 77.42% of participants acknowledged feelings of guilt or perceived defectiveness stemming from their GD. Alarmingly, 83.87% withheld their GD from family members during the early periods of their lives out of fear of receiving a harsh response. Peer ostracization or bullying because of their GD was reported by 37.09% of participants, and 27.42% faced educational discrimination attributed to their GD. On a positive note, 41.94% stated that their family’s reaction to their GD was supportive. However, nearly half, 48.39%, believed that challenges related to their GD adversely affected their academic performance. Furthermore, 45.16% suffered verbal abuse from acquaintances due to their GD, and 12.90% endured physical violence. MTFs experienced more verbal abuse than FTMs, although the group difference lacked statistical significance (p=0.043).
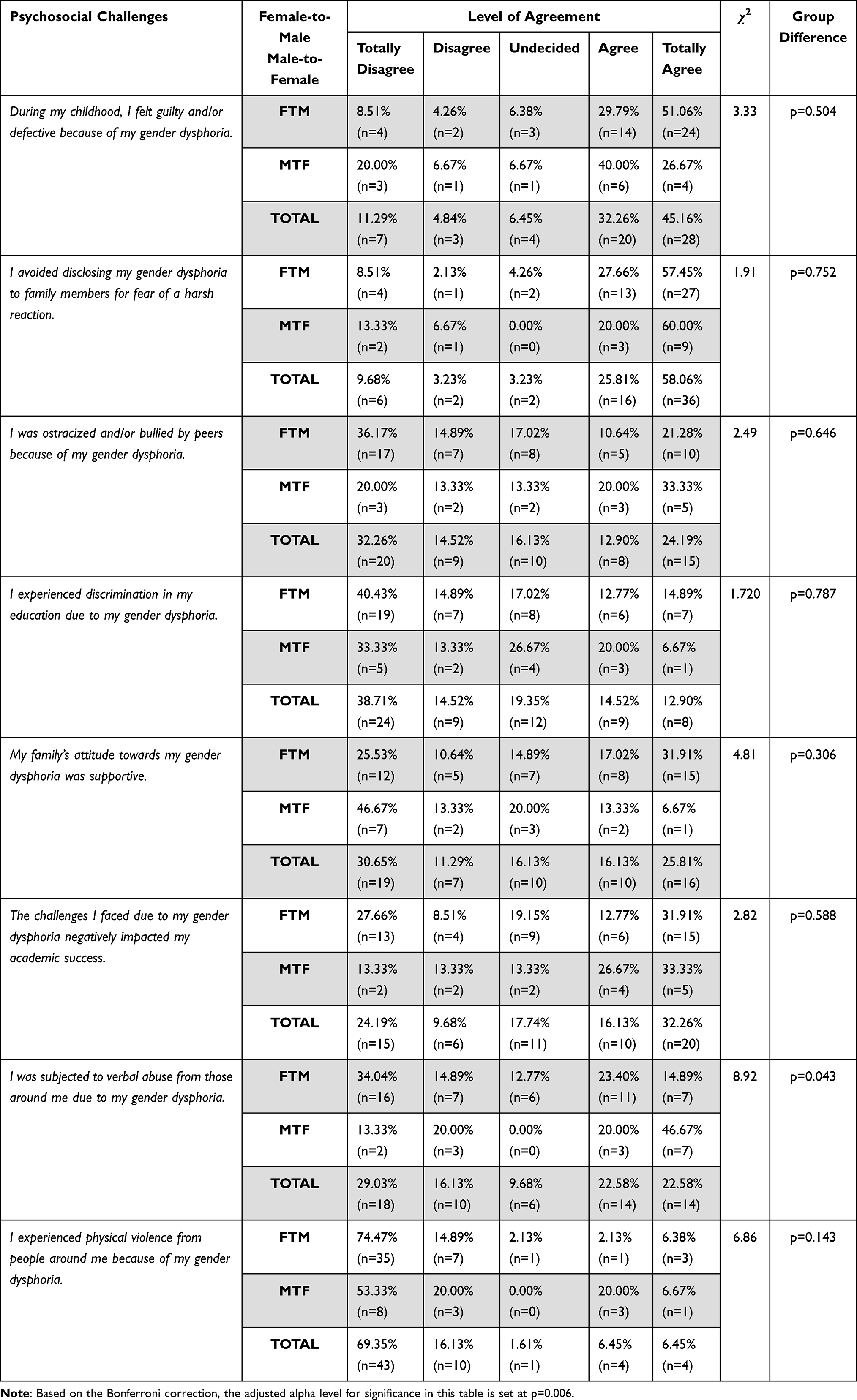 |
Table 4 Psychosocial Challenges Due to Gender Dysphoria During Childhood and Adolescence |
Attitudes Towards Early Intervention Strategies
Table 5 and Figure 1 delve into the perspectives of TG participants and cisgender controls regarding the potential significance of interventions designed to alleviate the challenges faced by individuals with GD during their formative years. An overwhelming 95.16% of TG participants underscored the importance of raising awareness through educational endeavors, such as organizing programs and campaigns on GD in educational settings and wider society. This sentiment was more prevalent among TG respondents compared to cisgender controls, with 76.19% echoing this sentiment, although the difference just fell short of statistical significance (p=0.013). Both groups predominantly supported initiatives to encourage children and adolescents to freely express their gender identity and to normalize their experiences by assuring them that their feelings are natural and shared by others. These initiatives were backed by 95.16% vs 84.13% and 90.32% vs 79.36% of TG and cisgender participants, respectively, with no statistically significant difference. Controversially, the consideration of medical interventions, such as hormone therapy to delay puberty for young individuals with GD, was the least endorsed strategy, receiving the nod from just 32.80% of respondents. However, a more substantial portion of TG participants (46.78%) favored this approach compared to only 19.05% of cisgender controls (p=0.010). Lastly, a significant disparity emerged in views on enhancing professional competence. As many as 88.71% of TG participants deemed it vital to augment the expertise of professional groups—including medical and mental health practitioners—in relation to GD, a view shared by 68.25% of cisgender participants (p=0.030).
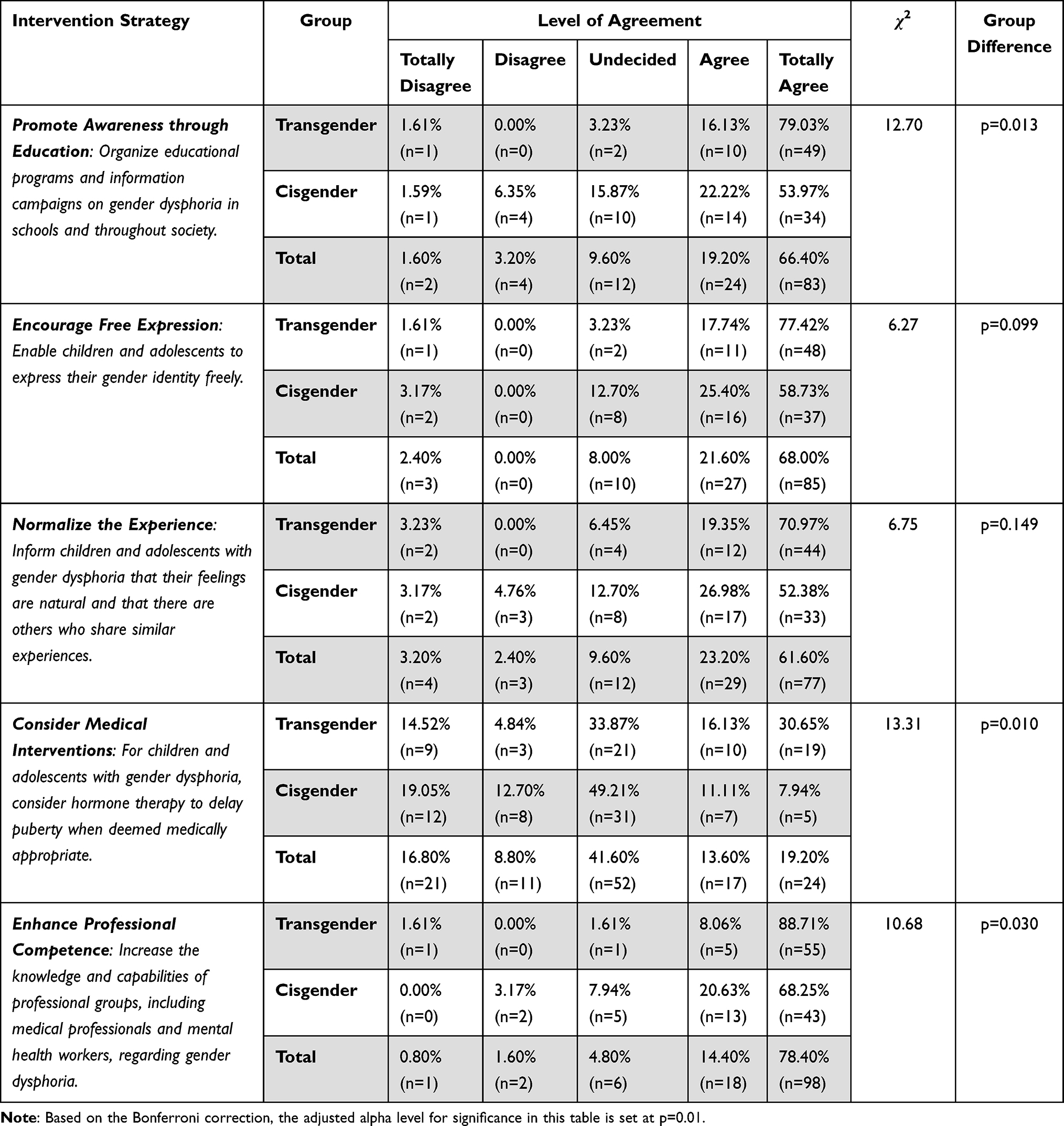 |
Table 5 Participants’ Perspectives on Interventions for Childhood/Adolescence Gender Dysphoria Challenges |
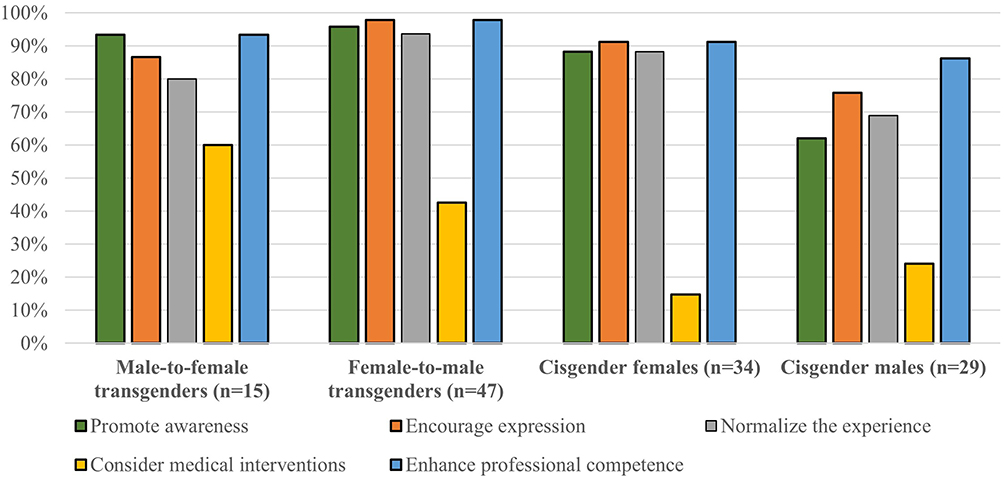 |
Figure 1 Support percentages for different interventions among male-to-female transgender individuals, female-to-male transgender individuals, cisgender females, and cisgender males. |
Discussion
This study aimed to examine the psychosocial, developmental, and early behavioral characteristics of Turkish TG individuals, explore the challenges they faced across different contexts during childhood and adolescence, and gain insight into their perspectives on early interventions.
Early Experiences
In our sample, TG individuals typically recognized their GD at approximately age 10.77. This observation reinforces prior research suggesting that GD often surfaces during early years and persists through adolescence.1,16 Moreover, with the rising visibility and acceptance of TG identities in media and society, younger individuals appear to be exploring and affirming their gender identities earlier than past cohorts. Evidence indicates that while not all children diagnosed with GD between ages 5 to 12 retain their diagnosis into adolescence, a substantial number of teenagers with GD recall experiencing cross-gender behavior and feelings from an early age. Furthermore, many adolescents with GD continue to experience it into adulthood.17,18
The act of disclosing GD is a significant event for many. In our dataset, individuals, on average, disclosed their GD at age 16.67. This gap between the onset of feelings and their disclosure underscores the internal struggles individuals might face, possibly due to societal challenges and biases. Disturbingly, more than 83% of our participants chose not to reveal their GD to family members, fearing negative consequences. This mirrors prior studies emphasizing the societal adversities faced by individuals with GD, including discrimination and exclusion.6
Presently, social gender transitioning—such as adopting a new name, changing physical appearance, or using different pronouns—is increasingly acknowledged as a viable step for gender-variant youth.19 Within our sample, participants, on average, adopted a gender-affirming name at 14.80 years and began dressing in line with their felt gender by 13.55 years. Yet, the literature remains somewhat inconclusive on the optimal timing and conditions under which gender dysphoric children and adolescents benefit most from such transitions. A recent UK study by Morandini et al explored the mental health implications of social transitioning. Intriguingly, their findings showed no significant impact of social transition, including name changes, on mental health.20 Notably, FTM transitions were more common than MTF transitions, both in their study and ours. Our research further revealed that FTMs embarked on social transition steps earlier on average than MTFs. This mirrors findings from Holt et al21 suggesting that prepubertal and adolescent birth-assigned females are more likely to have socially transitioned before engaging with specialized gender services than their birth-assigned male counterparts. This trend might be attributed to societal and cultural norms, wherein there is perhaps a reduced stigma attached to masculine presentation by birth-assigned females than feminine presentation by birth-assigned males.
Activities and Play Behaviors
Human children display distinct gender-based differences in pre-school activities and preferences. Typically, boys gravitate towards vehicles, weapons, and construction toys, while girls show a preference for dolls, kitchen sets, cosmetics, and dress-up items.22 These differences go beyond toy choices, encompassing behavior (eg, boys often being more physically active and engaging in rougher play) and social interactions (eg, between ages 4.5 to 6.5, children usually spend three to ten times more time with same-sex peers than with those of the opposite sex).23,24 While many studies highlight the influence of prenatal androgens on these gendered behaviors,25 others emphasize the roles of gender identity and societal stereotypes.26
In our research, FTMs reported a higher inclination towards activities traditionally associated with males during their childhood and adolescence. Conversely, MTFs showed a similar trend, favoring activities typically associated with females. However, there were no discernible differences between FTMs and MTFs in their participation in neutral activities or widely popular individual sports and digital games. Our findings reaffirm the idea that those with GD tend to align with activities corresponding to their experienced gender, echoing earlier research indicating an early gender-based divergence in interests.4,13,27,28 Importantly, gender nonconforming play behaviors can lead children to face societal challenges such as discrimination and ostracization, increasing their risk of mental health issues.29 This psychological distress, often resulting from peer rejection and teasing, is notably higher in gender-variant youth than in those with gender-stereotypical behaviors.30,31
Psychosocial Challenges
The multifaceted challenges encountered by TG participants in our study are of significant concern. Among them, 45.16% reported experiencing verbal abuse from acquaintances as a result of their GD, while 12.90% had endured physical violence. Although these figures are alarmingly high, even more striking rates were documented in a recent nationwide study conducted with gender dysphoric adolescents in the US.32 In that study, a staggering 73% of TG and gender-nonconforming adolescents reported instances of psychological abuse, 39% reported experiencing physical abuse, and 19% reported incidents of sexual abuse. It’s noteworthy to mention that the risk of psychological abuse was observed to be particularly pronounced among those who were assigned female at birth, which contrasts with the findings in our study.
Peer ostracization or bullying because of their GD was reported by 37.09% of participants, and 27.42% faced educational discrimination attributed to their GD. These rates are also in line with previous literature and require attention given that poor peer relations and rejection are strongly related to poor mental health among dysphoric adolescents.16,29 Strikingly, 20.96% of our participants had sought child and adolescent psychiatry services due to indirect complications arising from GD, such as peer bullying and adjustment issues. A staggering 77.42% of our participants reported to have grappled with feelings of guilt or perceived defectiveness; echoing earlier findings where TG individuals often endure self-devaluation, and heightened vulnerability.10 Indeed, 40.32% of our participants indicated that, aside from their clinical follow-up for GD, they were diagnosed with and received treatment for depression and anxiety disorder cluster diagnoses. In a multicentered survey conducted on gender dysphoric adolescents from Netherlands and Canada, poor peer relations was found to be the strongest predictor of behavioral and emotional problems in gender dysphoric adolescents.29 An analysis of chart reviews from clinics in the UK and US found depression in over half of the participants33,34 Similarly, a US study evaluating youths identified that a comparable proportion displayed at least mild depressive symptoms.35 Other studies, including a Canadian survey on adolescents and an assessment from a specialized Amsterdam clinic found a prevalence of depression hovering around one-third among gender dysphoric adolescents.36,37 Furthermore, a recent systematic review focusing on adolescent populations with gender dysphoria highlighted the substantially high proportions of depression and anxiety disorders, which are the most common mental health problems among this population.38
The majority of participants in our study had refrained from revealing their GD to family members during the early periods of their lives, due to fear of negative reactions. This concern is evident in the low percentage of participants who initially disclosed their GD to parents, compared to over half who first confided in friends. Notably, 11% of FTMs in our sample had not informed their families about their GD. Among the participants, 41.94% reported receiving supportive reactions from their families in response to their GD, echoing previous research that highlights lower family support for TG individuals compared to cisgenders.39 Numerous studies emphasize the pivotal role of family support in the mental well-being of TG adolescents, sometimes surpassing support from peers or significant others.7,40,41 This emphasis on family backing may stem from the requirement of parental consent for gender-affirming care sought by TG minors. While peer support remains crucial, given the higher victimization rates experienced by TG adolescents, these studies consistently underscore the profound impact of familial acceptance and understanding on the mental health of TG youth.42
Views on Interventions and Strategies
In this study, we also examined the viewpoints of TG individuals and cisgender control participants regarding a range of proposed strategies and interventions aimed at addressing the challenges faced by TG youth.3 The efficacy of these interventions has been the subject of exploration in a handful of previous studies. For instance, a study conducted in the US demonstrated the efficacy of media interventions in fostering positive attitudes towards marginalized TG groups among university students.43 Additionally, political advertisements advocating TG rights were shown to significantly improve attitudes and counter discriminatory effects against TG individuals.44 Other approaches encompass web-based interventions targeting health practitioners’ biases towards TG individuals,45 psycho-education initiatives, and family-based acceptance interventions.15
Within our sample, a significant degree of support for the suggested strategies was observed among both control and TG participants. The majority in both groups emphasized the importance of raising awareness through educational initiatives, such as organizing campaigns on GD within educational settings and the broader society. Initiatives encouraging young individuals to openly express their gender identity and assuring them of the naturalness and shared nature of their feelings were also widely endorsed. Enhancing the professional competence of medical and mental health practitioners was another focal point. However, while these attitudes were relatively consistent across the two groups, TG participants exhibited stronger enthusiasm and conviction.
Of notable significance was the lower acceptance of hormonal treatment and medical interventions during adolescence. The difference in attitudes on this issue was even more pronounced between groups, with less than half of TG participants and one-fifth of cisgender participants showing support. This attitudinal divergence towards biological interventions compared to psychosocial interventions underscores the cautious stance both groups take on medical procedures. Literature indicates that criticisms and concerns surrounding hormonal replacement and medical interventions for children and adolescents with GD are multifaceted. These concerns may stem from apprehensions about physical impacts, irreversibility, and the potential disruption of natural gender expression trajectories in developmental stages.46 The complexity extends to issues of medical competence and the potential long-term physical and psychological impacts not fully understood at a young age.47 Moreover, societal, cultural, and ethical considerations further complicate the topic.4 Collectively, the intricate nature and consequences of biological interventions, coupled with insufficient evidence on long-term effects, might contribute to heightened skepticism and uncertainty surrounding them.
Limitations
Our study possesses several notable limitations. Firstly, our participant sample was derived from individuals undergoing clinical follow-up in a specialized unit for GD. While this offers insights into those seeking clinical support, it may not comprehensively represent the entire spectrum of TG experiences in Turkey. Furthermore, our control sample primarily consisted of university students and relatives. The exact relationship of these relatives to the TG participants is not detailed, which raises concerns about the potential influence of genetic and social proximity on GD expression and, subsequently, on the validity of group comparisons. This could impede our capacity to draw robust conclusions about the broader population. Another limitation pertains to the uneven distribution of participants in our subgroups. A particular constraint here is the underrepresentation of MTF participants, reflecting a trend observed in Turkey, where MTF individuals may avoid health care settings and formal procedures more often than FTMs. This has potential implications for bias and interpreting the results. While our investigation into gender-specific activities offers valuable insights for the TG group, not collecting similar data from the control participants limits the extent of comparisons and conclusions drawn regarding gender-based behavioral tendencies. Additionally, relying on retrospective reports of childhood and adolescent experiences from TG adults introduces the risk of recall bias. Memories of past events and emotions might be influenced by current viewpoints, possibly resulting in data inaccuracies or omissions.
Conclusion
Our study underscores the multifaceted challenges and experiences of gender dysphoric individuals during their developmental years, particularly in the context of Turkey. Early recognition and supportive interventions, societal awareness, professional training, and holistic support mechanisms are of paramount importance to foster acceptance, reduce adversity, and pave the way for a more understanding and inclusive future for children and adolescents with GD.
Ethics Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Disclosure
The authors have no conflict of interest to declare for this work.
References
1. Fast AA, Olson KR. Gender development in transgender preschool children. Child Dev. 2018;89(2):620–637. doi:10.1111/cdev.12758
2. Olson J, Forbes C, Belzer M. Management of the transgender adolescent. Arch Pediatr Adolesc Med. 2011;165(2):171–176. doi:10.1001/archpediatrics.2010.275
3. Holman CW, Goldberg JM. Ethical, legal, and psychosocial issues in care of transgender adolescents. Int J Transgend. 2006;9(3–4):95–110. doi:10.1300/J485v09n03_05
4. Drescher J, Pula J. Ethical issues raised by the treatment of gender‐variant prepubescent children. Hast Center Rep. 2014;44(s4):S17–S22. doi:10.1002/hast.365
5. Hughes LD, Kidd KM, Gamarel KE, Operario D, Dowshen N. “These laws will be devastating”: provider perspectives on legislation banning gender-affirming care for transgender adolescents. J Adolesc Health. 2021;69(6):976–982. doi:10.1016/j.jadohealth.2021.08.020
6. De Vries AL, Cohen-Kettenis PT. Clinical management of gender dysphoria in children and adolescents: the Dutch approach. J Homosex. 2012;59(3):301–320. doi:10.1080/00918369.2012.653300
7. Simons L, Schrager SM, Clark LF, Belzer M, Olson J. Parental support and mental health among transgender adolescents. J Adolesc Health. 2013;53(6):791–793. doi:10.1016/j.jadohealth.2013.07.019
8. Nahata L, Quinn GP, Caltabellotta NM, Tishelman AC. Mental health concerns and insurance denials among transgender adolescents. LGBT Health. 2017;4(3):188–193. doi:10.1089/lgbt.2016.0151
9. Thoma BC, Salk RH, Choukas-Bradley S, Goldstein TR, Levine MD, Marshal MP. Suicidality disparities between transgender and cisgender adolescents. Pediatrics. 2019;144(5). doi:10.1542/peds.2019-1183
10. Reisner SL, Vetters R, Leclerc M, et al. Mental health of transgender youth in care at an adolescent urban community health center: a matched retrospective cohort study. J Adolesc Health. 2015;56(3):274–279. doi:10.1016/j.jadohealth.2014.10.264
11. Hollinsaid NL, Price MA, Hatzenbuehler ML. Transgender-specific adolescent mental health provider availability is substantially lower in states with more restrictive policies. J Clin Child Adolesc Psychol. 2022;1–12. doi:10.1080/15374416.2022.2140433
12. Golombok S, Rust J. The Pre-School Activities Inventory: a standardized assessment of gender role in children. Psychol Assess. 1993;5(2):131. doi:10.1037/1040-3590.5.2.131
13. Roshan GM, Talaei A, Sadr M, Arezoomandan S, Kazemi S, Khorashad BS. Recalled pre-school activities among adults with gender dysphoria who seek gender confirming treatment—An Iranian study. Asian J Psychiatr. 2019;42:57–61. doi:10.1016/j.ajp.2019.03.028
14. Telfer MM, Tollit MA, Pace CC, Pang KC. Australian standards of care and treatment guidelines for transgender and gender diverse children and adolescents. Med J Aust. 2018;209(3):132–136. doi:10.5694/mja17.01044
15. Malpas J, Pellicane MJ, Glaeser E. Family-based interventions with transgender and gender expansive youth: systematic review and best practice recommendations. Transgend Health. 2022;7(1):7–29. doi:10.1089/trgh.2020.0165
16. Clark TC, Lucassen MF, Bullen P, et al. The health and well-being of transgender high school students: results from the New Zealand adolescent health survey (Youth’12). J Adolesc Health. 2014;55(1):93–99. doi:10.1016/j.jadohealth.2013.11.008
17. Drummond KD, Bradley SJ, Peterson-Badali M, Zucker KJ. A follow-up study of girls with gender identity disorder. Dev Psychol. 2008;44(1):34. doi:10.1037/0012-1649.44.1.34
18. Wallien MS, Cohen-Kettenis PT. Psychosexual outcome of gender-dysphoric children. J Am Acad Child Adolesc Psychiatry. 2008;47(12):1413–1423. doi:10.1097/CHI.0b013e31818956b9
19. Ehrensaft D, Giammattei SV, Storck K, Tishelman AC, St. Amand C. Prepubertal social gender transitions: what we know; what we can learn—A view from a gender affirmative lens. Int J Transgend. 2018;19(2):251–268. doi:10.1080/15532739.2017.1414649
20. Morandini JS, Kelly A, de Graaf NM, et al. Is social gender transition associated with mental health status in children and adolescents with gender dysphoria? Arch Sex Behav. 2023;52(3):1045–1060. doi:10.1007/s10508-023-02588-5
21. Holt V, Skagerberg E, Dunsford M. Young people with features of gender dysphoria: demographics and associated difficulties. Clin Child Psychol Psychiatry. 2016;21(1):108–118. doi:10.1177/1359104514558431
22. Cohen-Bendahan CC, Van De Beek C, Berenbaum SA. Prenatal sex hormone effects on child and adult sex-typed behavior: methods and findings. Neurosci Biobehav Rev. 2005;29(2):353–384.
23. Hines M. Sex-related variation in human behavior and the brain. Trends Cogn Sci. 2010;14(10):448–456. doi:10.1016/j.tics.2010.07.005
24. Auyeung B, Baron-Cohen S, Ashwin E, et al. Fetal testosterone predicts sexually differentiated childhood behavior in girls and in boys. Psychol Sci. 2009;20(2):144–148. doi:10.1111/j.1467-9280.2009.02279.x
25. Pasterski V, Geffner ME, Brain C, Hindmarsh P, Brook C, Hines M. Prenatal hormones and childhood sex segregation: playmate and play style preferences in girls with congenital adrenal hyperplasia. Horm Behav. 2011;59(4):549–555. doi:10.1016/j.yhbeh.2011.02.007
26. Tobin DD, Menon M, Menon M, Spatta BC, Hodges EV, Perry DG. The intrapsychics of gender: a model of self-socialization. Psychol Rev. 2010;117(2):601. doi:10.1037/a0018936
27. Cardoso FL. Recalled sex-typed behavior in childhood and sports’ preferences in adulthood of heterosexual, bisexual, and homosexual men from Brazil, Turkey, and Thailand. Arch Sex Behav. 2009;38(5):726–736. doi:10.1007/s10508-008-9312-6
28. Koehler A, Richter-Appelt H, Cerwenka S, et al. Recalled gender-related play behavior and peer-group preferences in childhood and adolescence among adults applying for gender-affirming treatment. Sex Relatsh Ther. 2017;32(2):210–226. doi:10.1080/14681994.2016.1195908
29. de Vries AL, Steensma TD, Cohen-Kettenis PT, VanderLaan DP, Zucker KJ. Poor peer relations predict parent-and self-reported behavioral and emotional problems of adolescents with gender dysphoria: a cross-national, cross-clinic comparative analysis. Eur Child Adolesc Psychiatry. 2016;25(6):579–588. doi:10.1007/s00787-015-0764-7
30. Baams L, Beek T, Hille H, Zevenbergen FC, Bos HM. Gender nonconformity, perceived stigmatization, and psychological well-being in Dutch sexual minority youth and young adults: a mediation analysis. Arch Sex Behav. 2013;42(5):765–773. doi:10.1007/s10508-012-0055-z
31. Robinson JP, Espelage DL, Rivers I. Developmental trends in peer victimization and emotional distress in LGB and heterosexual youth. Pediatrics. 2013;131(3):423–430. doi:10.1542/peds.2012-2595
32. Thoma BC, Rezeppa TL, Choukas-Bradley S, Salk RH, Marshal MP. Disparities in childhood abuse between transgender and cisgender adolescents. Pediatrics. 2021;148(2). doi:10.1542/peds.2020-016907
33. Freedman D, Tasker F, Di Ceglie D. Children and adolescents with transsexual parents referred to a specialist gender identity development service: a brief report of key developmental features. Clin Child Psychol Psychiatry. 2002;7(3):423–432. doi:10.1177/1359104502007003009
34. Spack NP, Edwards-Leeper L, Feldman HA, et al. Children and adolescents with gender identity disorder referred to a pediatric medical center. Pediatrics. 2012;129(3):418–425. doi:10.1542/peds.2011-0907
35. Olson J, Schrager SM, Belzer M, Simons LK, Clark LF. Baseline physiologic and psychosocial characteristics of transgender youth seeking care for gender dysphoria. J Adolesc Health. 2015;57(4):374–380. doi:10.1016/j.jadohealth.2015.04.027
36. Khatchadourian K, Amed S, Metzger DL. Clinical management of youth with gender dysphoria in Vancouver. J Pediatr. 2014;164(4):906–911. doi:10.1016/j.jpeds.2013.10.068
37. de Vries AL, Doreleijers TA, Steensma TD, Cohen‐Kettenis PT. Psychiatric comorbidity in gender dysphoric adolescents. J Child Psychol Psychiatry. 2011;52(11):1195–1202. doi:10.1111/j.1469-7610.2011.02426.x
38. Thompson L, Sarovic D, Wilson P, Sämfjord A, Gillberg C, Chen R. A PRISMA systematic review of adolescent gender dysphoria literature: 2) mental health. PLOS Global Public Health. 2022;2(5):e0000426. doi:10.1371/journal.pgph.0000426
39. Davey A, Bouman WP, Arcelus J, Meyer C. Social support and psychological well‐being in gender dysphoria: a comparison of patients with matched controls. J Sex Med. 2014;11(12):2976–2985. doi:10.1111/jsm.12681
40. McConnell EA, Birkett M, Mustanski B. Families matter: social support and mental health trajectories among lesbian, gay, bisexual, and transgender youth. J Adolesc Health. 2016;59(6):674–680. doi:10.1016/j.jadohealth.2016.07.026
41. Puckett JA, Matsuno E, Dyar C, Mustanski B, Newcomb ME. Mental health and resilience in transgender individuals: what type of support makes a difference? J Fam Psychol. 2019;33(8):954. doi:10.1037/fam0000561
42. Olsavsky AL, Grannis C, Bricker J, et al. Associations among gender-affirming hormonal interventions, social support, and transgender adolescents’ mental health. J Adolesc Health. 2023;72(6):860–868. doi:10.1016/j.jadohealth.2023.01.031
43. Taracuk MD, Koch JM. Use of a media intervention to increase positive attitudes toward transgender and gender diverse individuals. Int J Transgend Health. 2023;24(1):86–98. doi:10.1080/26895269.2021.1878479
44. Flores AR, Haider-Markel DP, Lewis DC, Miller PR, Taylor JK. Antidiscrimination interventions, political ads on transgender rights, and public opinion: results from two survey experiments on adults in the United States. Front Psychol. 2021;12:3477. doi:10.3389/fpsyg.2021.729322
45. Costa AB, Pase PF, de Camargo ES, et al. Effectiveness of a multidimensional web-based intervention program to change Brazilian health practitioners’ attitudes toward the lesbian, gay, bisexual and transgender population. J Health Psychol. 2016;21(3):356–368. doi:10.1177/1359105316628748
46. Mahfouda S, Moore JK, Siafarikas A, Zepf FD, Lin A. Puberty suppression in transgender children and adolescents. Lancet Diabetes Endocrinol. 2017;5(10):816–826. doi:10.1016/S2213-8587(17)30099-2
47. Vrouenraets LJJJ, de Vries AL, Arnoldussen M, et al. Medical decision-making competence regarding puberty suppression: perceptions of transgender adolescents, their parents and clinicians. In: European Child and Adolescent Psychiatry. Springer. 2022:1–19.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.