")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 15
Untimely Initiation of Whole Cow Milk, Stunting, and Related Factors in South Gondar, Ethiopia
Authors Yisak H , Gedamu D, Ewunetei A
Received 17 January 2024
Accepted for publication 22 March 2024
Published 3 April 2024 Volume 2024:15 Pages 159—170
DOI https://doi.org/10.2147/PHMT.S454615
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Hiwot Yisak,1 Dejen Gedamu,2 Amien Ewunetei3
1Department of Nutrition, Debre Tabor University, Debre Tabor, Ethiopia; 2Department of Statistics, Debre Tabor University, Debre Tabor, Ethiopia; 3Department of Pharmacy, Debre Tabor University, Debre Tabor, Ethiopia
Correspondence: Hiwot Yisak, Email [email protected]
Introduction: Despite being an excellent source of essential nutrients, whole cow’s milk poses risks for young children. This is mainly due to its association with adverse effects, including growth inhibition, delayed brain and motor development, and increased morbidity and mortality. The current study aimed to evaluate the occurrence of untimely introduction of whole cow milk, stunting and related factors among children below the age of 5 years.
Methods: A community-centered survey was implemented on 806 mother–child matches. Expressive statistics such as frequency, magnitude, mean and standard deviation were computed. Multivariable logistic regression was done to discover independent determinants of the dependent variables. A p-value of < 0.05 was used to affirm significant association.
Results: From the survey participant children 311 (39.2%) of them were stunted. About 453 (57.1%) of children were fed whole cow milk earlier than the age of one year. Mothers who are able to read and write were 49% less likely to initiate cow milk earlier than the age of one year with AOR = 0.51, 95% CI 0.33– 0.78. Not attending the growth monitoring and promotion service is a risk for untimely introduction of whole cow milk (AOR = 3.47, 95% CI 2.43– 4.94). Children who did not start consuming whole cow milk earlier than the age of one year were 54% less likely to be stunted than those who started consuming whole cow milk before the age of one year (AOR = 0.46, 95% CI 0.33– 0.65).
Conclusion: More than half of the study participant children started consuming whole cow milk before the age of one year. Children who did not start consuming whole cow milk early were less likely to be stunted.
Keywords: untimely initiation, whole cow milk, stunting, Ethiopia
Introduction
A lot of whole cow milk is consumed by young children. Even though whole whole cow milk is generally recognized to be not good for young children due to its low iron content, it is an excellent provider of important nutrients. The first mechanism is that whole cow milk makes it difficult for the baby to receive the iron levels required for growth. A second mechanism is through intestinal blood loss that occurs when healthy neonates are fed whole cow milk and affects about 40% of them. The third factor is that whole cow milk’s high calcium and casein content inhibits the absorption of dietary non-heme iron. Babies that drink whole cow milk receive significantly more protein and minerals than they need which is a burden to their body. Whole cow milk has a higher renal solute load, which results in higher urine concentrations when compared with breast milk or formula milk. The kidney’s ability in infants might not be enough to keep the water balance stable. In the event that the water balance becomes negative, severe dehydration may ensue.1–4
According to recent studies, consuming whole cow milk has a harmful effect on physical body growth, mainly on weight speeding up and the occurrence of juvenile obesity. A few further reasons are listed for avoiding giving newborns full cow milk, such as allergy to milk proteins and high renal solute loads. Also. whole cow milk may affect linear growth and raises levels of the growth hormone ‘insulin-like growth factor1’.5,6
According to Rolland premature adiposity bounce back and associations with measures of adiposity, later on, are seen when average protein intakes are particularly high at young ages (15% energy). The link is with overall protein intake from whole cow milk.7 Untimely initiation of whole cow milk proteins upgrades the risk of occurrence of a milk protein allergy. Given the possible correlation between early exposure to whole cow milk proteins and the development of type 1 diabetes mellitus, it is powerfully suggested in children with a strong family history of insulin-dependent diabetes mellitus that infants be breastfed and not taking commercially available whole cow milk or products containing intact whole cow milk protein during the first year of life.
Child growth has been recognized as a critical indicator of development by both the Sustainable Development Goals (SDGs) and the Millennium Development Goals (MDGs).8 SDG target 2.2 aims to end malnutrition in all its forms, including stunting of children. But, under-five mortality, delayed motor development, reduced mental capacity, low academic accomplishment, and a large financial burden are all impacted by pediatric anemia.9–11 Studies have suggested that untimely whole cow milk intake may be a risk factor for low hemoglobin content in early childhood.12,13 A Brazilian study also found a link between milk consumption and baby anemia prevalence.14 A systematic review found that whole cow milk consumption in late infancy was inversely associated with iron status, but follow-on formula was positively associated. Fortified foods appear to improve iron status in late childhood.15 Furthermore, another study found that children who had whole cow milk were more likely to have low hemoglobin concentrations than infants who consumed camel milk.16
In Ethiopia, anemia and stunting co-occurred at alarmingly high rates in newborns and young children.17 The overall prevalence of anemia in Ethiopia ranges from 34.4–58.65%.18–21Poor socioeconomic position and low maternal education are two factors that contribute to the untimely introduction of unaltered cow’s milk.22 One study in Ethiopia showed that only 24% of those interviewed reported consuming iron-rich meals in the 24 hours before the interview.23 And since there is no study regarding the untimely introduction of whole cow milk and the related factors, the current study aimed to evaluate the magnitude of untimely introduction of cow’s milk, stunting, and related factors among children below the age of 5 years in South Gondar district, Northwest Ethiopia.
Methodology
Study Area
The research took place within the South Gondar Zone, situated in the Amhara Region of Ethiopia. Mount Guna, reaching 4231 meters, stands as the highest peak in South Gondar. Notable towns within this zone include Addis Zemen, Debre Tabor and Wereta. According to the 2007 Census conducted by the Central Statistical Agency of Ethiopia (CSA), South Gondar Zone accommodates a total population of 2,051,738. Of this populace, 1,041,061 are men and 1,010,677 are women. The census identified 468,238 households in the zone, averaging 4.38 individuals per household. The zone boasts 96 health centers, 7 primary hospitals and 1 general hospital.
Study Design and Period
The study employed a community-based cross-sectional quantitative study design and took place between May 15, 2023 and June 17, 2023.
Source Population
The population source comprised children aged below 5 years and their mothers or caregivers residing in the South Gondar Zone.
Study Population
The participants in this study were children under 5 years old along with their mothers or caregivers residing in kebeles that were randomly chosen for the research.
Study Subjects
Every child under 5 years old, alongside their respective mother or caregiver, was selected using a systematic random approach and included in the study.
Inclusion and Exclusion Criteria
Inclusion Criteria for Children
Children who are living in the study area for more than or equal to 6 months.
Exclusion Criteria for Children
Children who are seriously ill at the time of data collection.
Children with visible physical deformity due to the fact it may under- or overestimate anthropometric results.
Sample Size
The size of the sample was determined utilizing the formula for a single population proportion.
Where: n = sample required
Z = 95% confidence level = 1.96
P = prevalence rate =50%
D = margin of error (5%)
By considering the design effect of 2=384*2 = 768 and by adding+5% of 768 to compensate for the non-response rate makes the final sample size; is 806 children.
Sampling Methods
This research utilized a multistage cluster sampling strategy. Five districts were chosen randomly from 10 districts in the South Gondar Zone. Subsequently, one kebele was randomly selected from each district. The allocation of study subjects to selected kebeles was based on a proportional-to-population size, considering the number of children under 5 years old in each kebele. Systematic random sampling techniques were employed to select the study subjects; random start was applied to select the first child then a sampling interval of 7 was used (see Figure 1). The total number of children in the chosen kebeles was 5838.
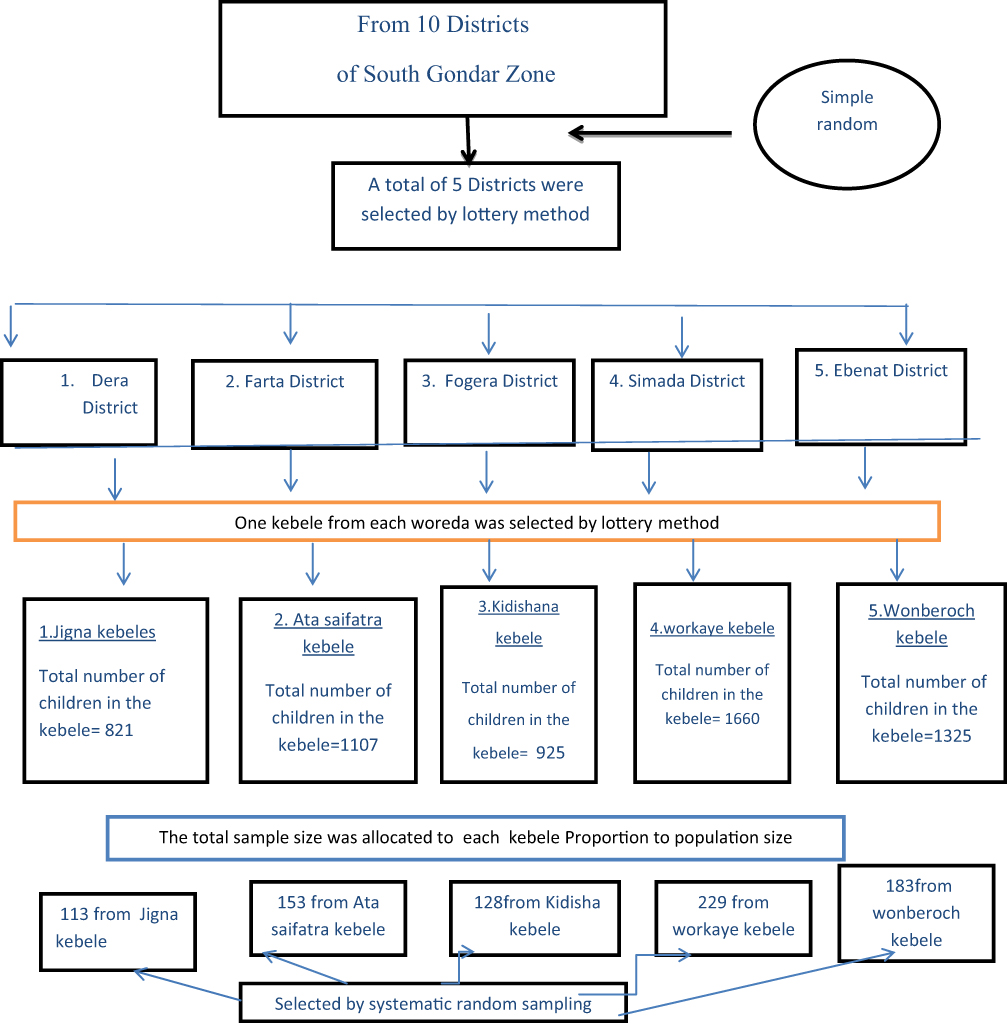 |
Figure 1 Schematic presentation of sampling techniques. |
Data Collection
Anthropometric measures were also taken, and data were gathered using a structured questionnaire (with both closed-ended and open-ended items) adapted from the Ethiopian National Nutrition Survey questionnaire. The data collection team consisted of 12 individuals, including 2 supervisors. They were chosen through the zone’s health stations and clinics. The mothers of the children participated in the interview and questionnaire. One child was chosen at random from homes with more than one child under the age of 5. Children under the age of 2 (below 85 cm) had their height (length) measured lying down using a wooden board, and children over the age of 2 had their stature measured standing up in centimeters to the nearest millimeter. The average of the two measurements was determined. All participants provided their informed consent before the interview.
Data Quality Management
For fieldwork purposes, the English-prepared questionnaire was translated into Amharic and then back into English to ensure uniformity. For three days, supervisors and interviewers received training on data collection methods, interviewing techniques, anthropometric measurements and data recording. Before the actual data collection, a pre-test was conducted on 35 mother–child pairs in Debre Tabor Kebele 6 to gauge response accuracy and determine the amount of time required. Two independent people measured the same person’s height twice, and the mean measurement was utilized for the analysis. Every day’s information was verified for accuracy, and any discrepancies were reported back to the collectors. The software EpiData version 3.2 was used to reduce errors during data entry and processing because it can identify a variety of values or errors during these processes. In order to assess the performance of the enumerators (data collectors) during the pre-testing and compare their accuracy and precision to the supervisors, a standardization test for anthropometric measurement was also carried out. For those data collectors with poor precision and accuracy, retraining was given.
Data Processing and Analysis
Initially, the data underwent checks for completeness and consistency, followed by coding and entry into EpiData version 3.2 software. Nutritional data were processed using WHO Anthro software, converting indices (such as H/A) into Z-scores while accounting for age and sex based on WHO standards. Children with height-for-age below two standard deviations from the reference population’s median were identified as stunted. Subsequently, the information was transferred to SPSS program Version 20 for analysis. Descriptive tests including frequencies, crosstabs, mean, and standard deviation were initially applied. Following this, bivariate tests utilizing crude odds ratios were employed to evaluate associations between categorical variables and the outcome. Finally, a multivariate logistic regression model was utilized to identify predictors of the outcome variables. Variables exhibiting a p-value less than 0.05 in the bivariable logistic regression were entered into the final multivariate logistic regression model. Throughout all statistical tests, a significance level of p < 0.05 was considered the cutoff point for determining statistical significance.
Variables
Dependent Variable
Early initiation of whole cow milk
Stunting
Predictor variables
Family size, Income, Educational levels of both mother and father, Maternal employment status, Head of household, Child’s age, Mother’s age, Child’s gender, Birth order of the child, Child’s health status, Feeding and care-giving practices, Water supply source, Environmental sanitation, and Presence of latrine facilities.
Operational Definitions
Early Initiation of cows milk – introduction of whole cow milk before one year of age
Stunting - H/A that is less than −2 SD below the
International media NCHS/WHO reference values
Results
The mean age of study participant mothers is 29.41±8.3 SD. Most of the mothers are in the age group of 21–35 which accounts for 604 (76.1%) of study participant mothers. About 729 (91.8%) of children live in the households having a family size of less or equal to five. 127 (16%) of study participant mothers have two under-5 children while 131 (16.5%) mothers did not attend any formal education (Table 1).
 |
Table 1 Socio Demographic Characteristics of the Mothers |
Environmental and Sanitation Conditions
The source of water for 273 (34.4%) of the households was protected spring. Disposal method of children’s feces was directly into latrine for 253 (31.9%) of households (Table 2).
 |
Table 2 Environmental and Sanitation Condition |
Children’s Nutrition
About 757 (95.3%) of mothers start breastfeeding immediately after giving birth. 498 (62.7%) of children were given a pre-lacteal feed rather than breast milk within the first three days after birth. 198 (24.9%) of mothers use food combinations to enhance micronutrient absorption. 63 (7.9%) of mothers did not feed colostrum for their last child. 316 (39.8%) of children were fed by bottle. About 517 (65.0%) of mothers switches or takes away the breast before the baby finishes feeding. From the total study participant children 761 (95.8%) of them had vitamin A supplementation every 6 months. 743 (93.6%) of children have completed vaccination. 653 (82.2%) uses iodized salt for complementary food preparation. Of the total study participant mothers 713 (89.8%) of them give tea or coffee with meal for their children. From the total index children studies 311 (39.2%) of them are stunted. About 453 (57.1%) of children were given whole cow milk earlier than the age of one year (Table 3).
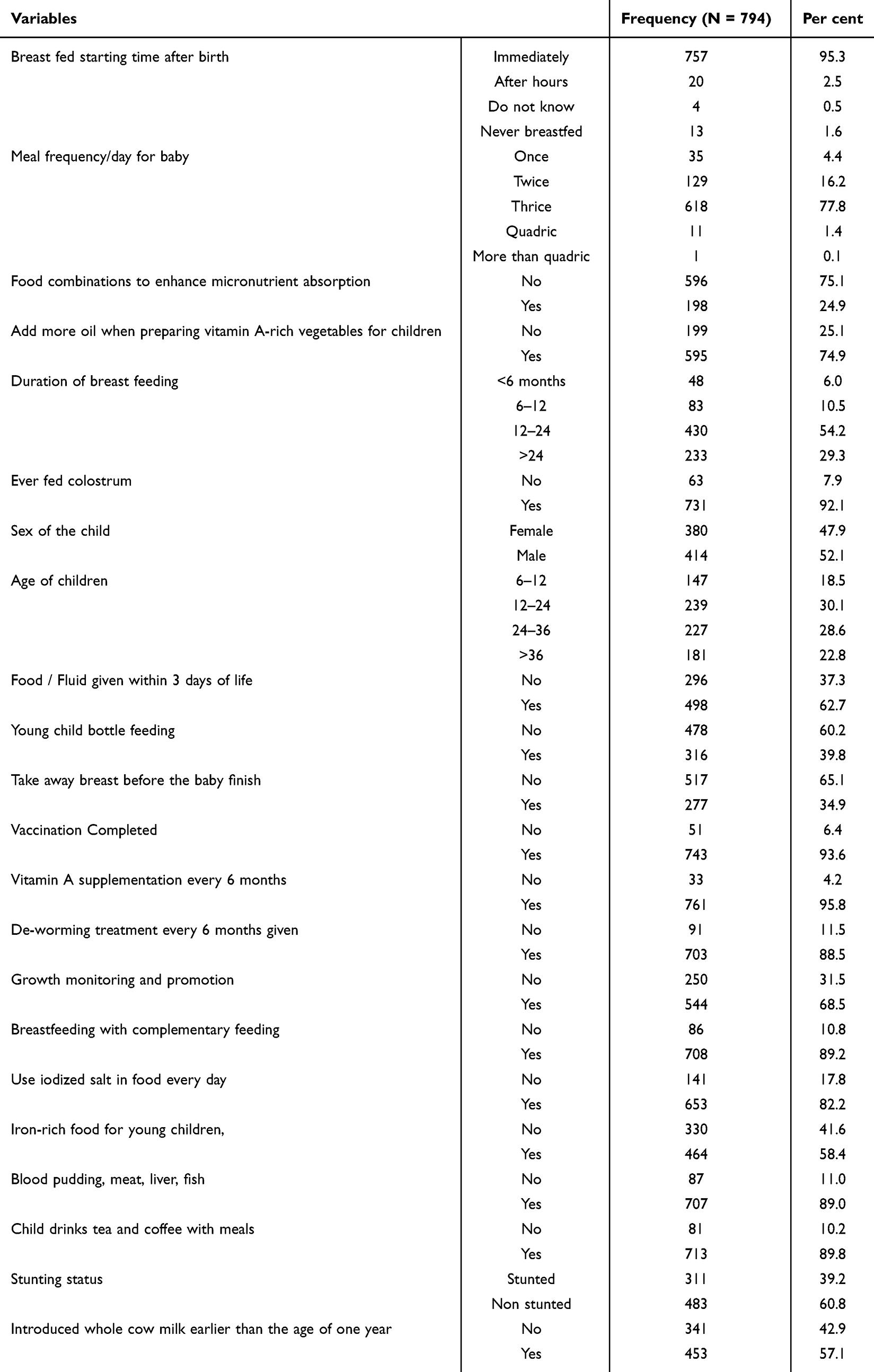 |
Table 3 Feeding Practices of Children |
Predictors of Untimely Initiation of Whole Cow Milk
In terms of occupation mothers who were students and house servants are more likely to introduce whole cow milk before one year with AOR = 7.21,95% CI 2.63–18.12 and 5.91 (3.52–23.23) respectively. Late introduction of breast feeding is protective against untimely introduction of whole cow milk with AOR = 0.24, 95% CI 0.06-0.90. Furthermore delayed initiation of additional food other than breast milk after the age of 6 months is also protective against untimely initiation of whole cow milk with AOR = 0 0.51, 95% CI 0.28–0.89. Mothers who did not apply a variety food combination to enrich the nutrient consumption of their child have extra probability to introduce whole cow milk early with AOR = 1.63, 95% CI 1.11–2.4 2. Mothers who are able to read and write are 49% less likely to introduce whole cow milk earlier than the age of one year with AOR = 0.51, 95% CI 0.33–0.78. Bottle feeding is positively associated with untimely introduction of whole cow milk AOR = 1.55, 95% CI 1.11–2.24. Not attending growth monitoring and promotion service is a risk for untimely introduction of whole cow milk, AOR = 3.47, 95% CI 2.43–4.94 . Early consumption of whole cow milk is 2 times more practiced among those not consuming iron-rich foods regularly with AOR = 2.57, 95% CI 1.82–3.63. Non-stunted children are less likely to start whole cow milk untimely as compared with stunted ones, AOR = 0.46, 95% CI 0.32–0.65 (Table 4).
 |
Table 4 Factors Associated with Early Initiation of Cow’s Milk |
Factors Associated with Stunting
Those from a family with monthly income of less than 3000 birr had an increased likelihood of becoming stunted children, AOR 1.68, 95% CI 1.11–2.55. Late introduction of complementary feeding is protective against stunting with AOR = 0.62, 95% CI 0.36–1.05 while use of food combination is associated with stunting, AOR = 1.53, 95% CI 1.05–2.23. Children who did not complete vaccination were more likely to be stunted than those who completed the vaccination, AOR = 1.94, 95% CI 1.04–3.61. Further more children who did not attend the growth monitoring and promotion service were more likely to be stunted than those who attended growth monitoring and promotion service, AOR = 1.51, 95% CI 1.07–2.14.Those children did not consume iron-rich foods regularly were more likely to be stunted than those who consume them regularly with AOR = 1.72, 95% CI 1.23–2.39. Children who did not start consuming whole cow milk earlier than the age of one year were 54% less likely to be stunted than those who started consuming whole cow milk earlier than one year AOR = 0.46, 95% CI 0.33–0.65 (Table 5).
 |
Table 5 Factors Associated with Stunting |
Discussion
In the current study the prevalence of untimely initiation of whole cow milk earlier than the age of one year is 57.1%. Similarly, 41% of infants in a 1996 study on the pattern of feeding of infants in Addis Ababa, Ethiopia, drank cow’s milk.24 Comparably 49.6% (95% CI 44.7–54.4%) of young children in Woldia Town, Northeast Ethiopia, practice adequate supplemental feeding.25 Similarly, a study in Brazil showed that 53.8% of 575 mothers of children under the age of one used whole cow milk for their children under the age of one year.26
In this study mothers who are able to read and write are 49% less likely to introduce whole cow milk earlier than the age of one year with AOR = 0.51, 95% CI 0.33–0.78. Similarly, a systematic review that evaluated the factors influencing untimely weaning and the consumption of unadulterated whole cow milk in young children found that maternal education and socioeconomic level were the factors that contributed to the untimely introduction of unadulterated whole cow milk.22 Untimely initiation of whole cow milk also exhibited a similar association with educational level, according to another study. When compared with children from mothers with an intermediate level of education, a higher proportion of children from mothers with a low level of education (12% vs 5%) were given whole cow milk at 3 months of age. Between the latter group and babies born to mothers with high levels of education, a comparable difference was seen.27 In the same way a study in Woldia town, Northeast Ethiopia illustrated that mothers’ educational status, with AOR 0.37, 95% CI 0.18–0.75, was significantly related with child feeding habit.25
In the current study children who did not start consuming whole cow milk earlier than the age of one year were 54% less likely to be stunted than who started consuming whole cow milk before the age of one year. In addition those children did not consume iron-rich foods regularly were more likely to be stunted than those who consume regularly, AOR = 1.72. These may be due to the fact that unmodified whole cow milk before one year of age and the untimely introduction of complementary foods before the age of 4–6 months are linked to a number of health risks in children, including iron deficiency anemia, elevated renal solute concentration, high loss of blood from the intestine, chronic constipation and anal fissures. Additionally, there is mounting evidence linking iron deficiency anemia to developmental delays, and that the relationship is causative.28 Moreover, different illnesses that might be caused by anemia can result in malnutrition including stunting as illnesses are the immediate causes of malnutrition as per the UNICEF’s conceptual frame work of malnutrition. Researchers found that parents of stunted children used less effective complementary and breastfeeding techniques and were less receptive to their children’s signals of hunger and satiation. The study from Ethiopia showed that feeding practice is connected with food intake and length/height of children in rural Ethiopia, (p <0.05).29
In this study early consumption of whole cow milk is more practiced among children who do not consume iron-rich foods regularly, AOR = 2.57, 95% CI 1.82–3.63, and less consumption of iron-rich foods can predispose children to anemia. A systematic review that found that infants who drink whole cow milk had a higher risk of iron deficiency anemia than those who drink formula milk (RR = 3.76; 95% CI 2.73, 5.19)30 supported the finding of the current study.
The current study showed that not attending the growth monitoring and promotion service is a risk for untimely initiation of whole cow milk, AOR = 3.47 95% CI 2.43–4.94. This may be because health-care professionals can offer advice on the best ways to feed children when mothers and childrenuse the development monitoring and promotion service. Additionally, introducing supplemental food later after 6 months protects against starting whole cow milk earlier (AOR = 0.51, 95% CI 0.28–0.89). Mothers who did not use a range of food combinations to enhance their child’s nutrient intake were more likely to start introducing whole cow milk early. These could be brought on by a lack of variety in food options; mothers might view whole cow milk as one alternative or a complementary food.
This study shows that untimely initiation of whole cow milk (AOR = 1.55, 95% CI 1.11–2.24) is positively correlated with bottle feeding. Due to their low socioeconomic condition, the majority of mothers may not be able to buy formula milk and instead choose to utilize cow’s milk, which is easier to bottle-feed children.
Conclusion
In this study more than half of children were fed whole cow milk earlier than the age of one year. Late introduction of breast feeding and complementary feeding is protective against untimely introduction of whole cow milk. Mothers who did not apply a variety food combination to enrich the nutrient consumption of their child were more likely to start whole cow milk early. Mothers that are able to read and write are less likely to introduce whole cow milk earlier than the age of one year. Not attending the growth monitoring and promotion service is a risk for untimely introduction of whole cow milk. Untimely intake of whole cow milk is more likely to be practiced among children who do not consume iron-rich foods regularly. Children who did not start consuming whole cow milk earlier than the age of one year were less likely to be stunted than those who started consuming whole cow milk earlier than the age of one year.
Strengths and Limitations
Weaknesses include potential recall bias and the likelihood of inaccurate reporting regarding the ages of the children. Strength lies in the study’s community-oriented approach, conducting interviews directly within households, enhancing its representation of the community.
Abbreviations
AOR, Adjusted Odds Ratio; CI, Confidence Interval; COR, Crude Odds Ratio; CSA, Central Statistical Agency of Ethiopia; H/A, Height for Age; MDGs, Millennium Development Goals; NCHS, National Center for Health Statistics; SD, Standard Deviation; SDGs, Sustainable Development Goals; SPSS, Statistical Package for Social Science; WHO, World Health Organization.
Data Sharing Statement
The corresponding author can provide the datasets utilized or analyzed during the present study upon reasonable request.
Ethical Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki. Ethical approval was secured from the Institutional Research Ethics Review Board at Debre Tabor University, bearing the reference number (CHS/4231/2023). Formal letters were sent to all relevant authorities in the Zone, district, and kebeles, requesting their cooperation in facilitating the study. Prior to data collection, interviewers elucidated the study’s objectives, potential benefits, and risks of the study to the study participants, to ensure informed written consent. All the respondents of this study were above the age of 18. Respondents were informed of their absolute right to decline participation at any point without facing any consequences. Furthermore, participants were assured of confidentiality, emphasizing that the information provided would solely be used for the study’s purposes. Any data collected did not include their names, their child’s names, or any other identifying information linking back to them.
Acknowledgment
The authors wish to express their gratitude to the South Gondar Health Office, as well as to the data collectors and respondents involved in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Leung AK, Sauve RS. Whole cow’s milk in infancy. Paediatrics Child Health. 2003;8(7):419–421. doi:10.1093/pch/8.7.419
2. Kibangou IB, Bouhallab S, Henry G, et al. Milk proteins and iron absorption: contrasting effects of different caseinophosphopeptides. Pediatr Res. 2005;58(4):731–734. doi:10.1203/01.PDR.0000180555.27710.46
3. Roughead ZK, Zito CA, Hunt JR. Inhibitory effects of dietary calcium on the initial uptake and subsequent retention of heme and nonheme iron in humans: comparisons using an intestinal lavage method–. Am J Clin Nutrit. 2005;82(3):589–597. doi:10.1093/ajcn/82.3.589
4. Ziegler EE. Adverse effects of cow’s milk in infants. Issu Complement Feed. 2007;60:185–199
5. Thorsdottir I, Thorisdottir AV. Whole cow’s milk in early life. Milk Produ Hum Nutrit. 2011;67:29–40
6. Agostoni C, Turck D. Is cow’s milk harmful to a child’s health? J Pediatr Gastroenterol Nutr. 2011;53(6):594–600. doi:10.1097/MPG.0b013e318235b23e
7. Rolland-Cachera MF, Deheeger M, Akrout M, Bellisle F. Influence of macronutrients on adiposity development: a follow up study of nutrition and growth from 10 months to 8 years of age. Int J Obes Relat Metab Disord. 1995;19(8):573–578
8. Lu Y, Nakicenovic N, Visbeck M, Stevance A-S. Policy: five priorities for the UN sustainable development goals. Nature. 2015;520(7548):432 3. doi:10.1038/520432a
9. Kraemer K, Cordaro J, Fanzo J, et al. The economics of poor nutrition: patterns, consequences and costs. In: Good Nutrition: Perspectives for the 21st Century. Karger Publishers; 2016:81–91
10. Dewey KG, Begum K. Long‐term consequences of stunting in early life. Maternal and Child Nutrition. 2011;7:5–18. doi:10.1111/j.1740-8709.2011.00349.x
11. Ramakrishnan U, Imhoff-Kunsch B. Anemia and iron deficiency in developing countries. Handbook of Nutrit Pregn. 2008;337–354
12. Oliveira MA, Osório MM. Cow’s milk consumption and iron deficiency anemia in children. J De Pediat. 2005;81:361–367. doi:10.2223/JPED.1386
13. Elalfy MS, Hamdy AM, Maksoud SSA, Megeed RIA. Pattern of milk feeding and family size as risk factors for iron deficiency anemia among poor Egyptian infants 6 to 24 months old. Nutr Res. 2012;32(2):93–99. doi:10.1016/j.nutres.2011.12.017
14. Hadler M-C-C, Colugnati FA, Sigulem DM. Risks of anemia in infants according to dietary iron density and weight gain rate. Preventive Med. 2004;39(4):713–721. doi:10.1016/j.ypmed.2004.02.040
15. Thorisdottir AV, Ramel A, Palsson GI, Tomassson H, Thorsdottir I. Iron status of one-year-olds and association with breast milk, cow’s milk or formula in late infancy. Eur J Nutr. 2013;52:1661–1668. doi:10.1007/s00394-012-0472-8
16. Abdurahman A, Gashu D. Level of hemoglobin among whole cow milk and camel milk consuming young children: a comparative study. PLoS One. 2021;16(3):e0247572. doi:10.1371/journal.pone.0247572
17. Mohammed SH, Larijani B, Esmaillzadeh A. Concurrent anemia and stunting in young children: prevalence, dietary and non-dietary associated factors. Nutr J. 2019;18(1):1–10. doi:10.1186/s12937-019-0436-4
18. Enawgaw B, Workineh Y, Tadesse S, Mekuria E, Addisu A, Genetu M. Prevalence of anemia and associated factors among hospitalized children attending the University of Gondar Hospital, Northwest Ethiopia. EJIFCC. 2019;30(1):35
19. Gebreweld A, Ali N, Ali R, Fisha T. Prevalence of anemia and its associated factors among children under five years of age attending at Guguftu health center, South Wollo, Northeast Ethiopia. PLoS One. 2019;14(7):e0218961. doi:10.1371/journal.pone.0218961
20. Gebrie A, Alebel A. A systematic review and meta-analysis of the prevalence and predictors of anemia among children in Ethiopia. Afr Health Sci. 2020;20(4):2007–2021. doi:10.4314/ahs.v20i4.59
21. Kawo KN, Asfaw ZG, Yohannes N. Multilevel analysis of determinants of anemia prevalence among children aged 6–59 months in Ethiopia: classical and Bayesian approaches. Anemia. 2018;2018. doi:10.1155/2018/3087354
22. Wijndaele K, Lakshman R, Landsbaugh JR, Ong KK, Ogilvie D. Determinants of early weaning and use of unmodified cow’s milk in infants: a systematic review. J Am Diet Assoc. 2009;109(12):2017–2028. doi:10.1016/j.jada.2009.09.003
23. EPHI I. Ethiopian Public Health Institute (EPHI)[Ethiopia] and ICF. Ethiopia mini demographic and health survey 2019: key Indicators; 2019
24. Ketsela T. Pattern of feeding of infants in Addis Ababa, Ethiopia. Ethiop J Health Dev. 1996;10(1):57–65
25. Asmare LD, Kassaw MW, Abebe AM, Abate BB, Dagnaw Tegegne K. Prevalence and factors associated with child feeding practice among mothers of Woldia Town, Northeast Ethiopia. NutrDietary Supplements. 2020;12:205–213. doi:10.2147/NDS.S264282
26. de Góes Cavalcanti LP, Diniz RL, Araujo BQ, et al. Factors associated with early use of whole cow’s milk by infants under one year old. Revista Brasileira em Promocao da Saude. 2015;28(4):538
27. Ummarino M, Albano F, Marco GD, et al. Short duration of breastfeeding and untimely introduction of cow’s milk as a result of mothers’ low level of education. Acta Paediatrica. 2003;92:12–17. doi:10.1111/j.1651-2227.2003.tb00641.x
28. Woldu MA, Mezgebe HB, Lekisa J. Consumption of unmodified cow’s milk and the risk of iron deficiency anemia in infants and toddlers and its management. Int J Pharm Sci Res. 2013;5:51–59
29. Abebe Z, Haki GD, Baye K. Child feeding style is associated with food intake and linear growth in rural Ethiopia. Appetite. 2017;116:132–138. doi:10.1016/j.appet.2017.04.033
30. Griebler U, Bruckmüller MU, Kien C, et al. Health effects of cow’s milk consumption in infants up to 3 years of age: a systematic review and meta-analysis. Public Health Nutrition. 2015;2015:19
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.