Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Untangling the Professional Web: Understanding the Impact of Work-Related Factors on the Mental Health of Healthcare Professionals During the Late Stages of Covid-19 Pandemic
Authors Laza R, Lustrea A ![]() , Lazureanu VE, Marinescu AR, Nicolescu N, Herlo A
, Lazureanu VE, Marinescu AR, Nicolescu N, Herlo A ![]() , Cut TG
, Cut TG ![]() , Porosnicu TM
, Porosnicu TM ![]() , Papava I
, Papava I ![]() , Romosan RS
, Romosan RS ![]() , Romosan AM, Bondrescu M
, Romosan AM, Bondrescu M ![]() , Dimeny CZ, Nica-Bacaiteanu CB, Andor M
, Dimeny CZ, Nica-Bacaiteanu CB, Andor M ![]() , Dehelean L
, Dehelean L ![]()
Received 12 July 2023
Accepted for publication 9 August 2023
Published 17 August 2023 Volume 2023:16 Pages 2391—2404
DOI https://doi.org/10.2147/JMDH.S424563
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ruxandra Laza,1 Anca Lustrea,2 Voichita Elena Lazureanu,1 Adelina Raluca Marinescu,1 Narcisa Nicolescu,1 Alexandra Herlo,1 Talida Georgiana Cut,1,3,4 Tamara Mirela Porosnicu,3,5 Ion Papava,6 Radu Stefan Romosan,6 Ana-Maria Romosan,6 Mariana Bondrescu,3,6 Cristian Zoltan Dimeny,7 Cristina Bianca Nica-Bacaiteanu,7 Minodora Andor,8,9 Liana Dehelean6
1Department of Infectious Diseases, Victor Babes University of Medicine and Pharmacy Timisoara, Timisoara, Romania; 2Department of Educational Sciences, University Clinic of Therapies and Psycho-Pedagogical Counseling, West University of Timisoara, Timisoara, Romania; 3Doctoral School Victor Babes University of Medicine and Pharmacy Timisoara, Timisoara, Romania; 4Center for Ethics in Human Genetic Identifications, Victor Babes University of Medicine and Pharmacy Timisoara, Timisoara, Romania; 5Intensive Care Unit, Victor Babes Clinical Hospital of Infectious Diseases and Pneumophtisiology Timisoara, Timisoara, Romania; 6Department of Neurosciences-Psychiatry, Victor Babes University of Medicine and Pharmacy, Timisoara, Romania; 7Department of Psychiatry, Timis County Emergency Clinical Hospital Pius Brinzeu, Timisoara, Romania; 8Department of Medical Semiology II, Victor Babes University of Medicine and Pharmacy, Timisoara, Romania; 9Multidisciplinary Heart Research Center, Victor Babes University of Medicine and Pharmacy, Timisoara, Romania
Correspondence: Anca Lustrea, Department of Educational Sciences, University Clinic of Therapies and Psycho-Pedagogical Counseling, West University of Timisoara, Bd. Vasile Parvan 4, Timisoara, 300223, Romania, Email [email protected]
Purpose: The COVID-19 pandemic has determined an extraordinary challenge to healthcare systems worldwide. The extraordinary circumstances, characterized by elevated stress levels, prolonged working hours, new medical procedures, media attention, and high population expectations, have created an extremely stressful situation for healthcare professionals. This period has offered a unique opportunity to examine the medical system and the responses of healthcare practitioners to stress. This research aimed to identify the work-related factors that significantly impact the mental health of healthcare professionals.
Patients and Methods: Three mental health variables were assessed: anxiety, depression and stress. The work-related factors considered were professional degree, type of medical unit (COVID or non-COVID), the number of hours spent at work in a single shift, type of shifts, monthly on-call frequency, and number of COVID-19 treated patients per month. In the spring of 2022, three inventories and a demographic survey were distributed and completed online by 300 healthcare professionals from Timisoara’s public hospitals in Romania.
Results: Among the respondents, 47.7% reported mild symptoms of anxiety, 65.3% reported moderate levels of stress, and 33% of the participants reported mild symptoms of depression. The intensity of anxious, depressive, and stress symptoms varied significantly depending on the professional degree, number of on-calls per month, the type of medical unit where the participants worked, and the number of SARS CoV-2 patients treated in the previous month.
Conclusion: Current data underlines the urgency of implementing effective strategies to reduce the stress and anxiety of medical practitioners who work with COVID-19 patients. Possible interventions encompass a variety of approaches, such as improving working conditions, reducing working hours where possible, increasing access to mental health services, and promoting team-building activities to enhance social support among colleagues. Digital mental health interventions, including online counseling and stress management programs, have also shown promise in these challenging times. Sustaining the mental health of medical practitioners is vital to support the continued provision of first-rate care to patients and to build a resilient healthcare workforce capable of navigating future health crises.
Keywords: healthcare professionals, SARS-CoV-2, stress, anxiety, depression
Introduction
The COVID-19 pandemic has provoked heightened levels of stress and anxiety among healthcare personnel. These adverse effects arise from various factors, including the danger of contracting and dying from COVID-19, the potential for loved ones to be infected, self-imposed quarantine, extended work shifts, social isolation, the absence of well-defined COVID-19 protocols, insufficient access to personal protective equipment, reduced opportunities for leisure time, the erosion of doctor-patient relationships resulting from the practice of telemedicine, concerns about being tasked with caring for patients in more critical conditions than their training allows, and the limited availability of current scientific data.1 In addition to the aforementioned factors, the enduring consequences of COVID-19, the ambiguity surrounding the persistent effects of the virus, the doubt and fear accompanying each successive wave, fueled by emergent variants, and the ramifications stemming from critical staff shortages caused by the illness and subsequent absence of colleagues, have exerted a profound impact.2,3
Stress can be defined as a physiological response, triggered by the perception of a threat. Inherent in stress responses is the presence of accompanying emotional reactions, wherein anxiety emerges as a dominant and pervasive emotion.4 Anxiety has been categorized by researchers into two discernible types, distinguished by their temporal attributes: state anxiety, pertains to a transient and acute reaction triggered by the anticipation of potential threats and trait anxiety. A persistent and enduring disposition exhibited consistently throughout an individual’s lifespan, while also being interconnected with their personality traits.5 Increased trait anxiety among healthcare professionals has numerous implications. Beyond the direct impact on the individual’s mental and physical health, heightened anxiety can affect job performance, potentially leading to increased medical errors, decreased patient satisfaction, and a lower quality of care.6
Frontline healthcare practitioners have experienced divergent outcomes in terms of their mental well-being throughout various phases of the pandemic.1 By the conclusion of October 2021, as the Delta variant precipitated a surge in cases, Romania attained the unenviable distinction of occupying the top spot worldwide in terms of daily new COVID-19 fatalities per million population.
Simultaneously, the manifestation of “pandemic fatigue”, as explained by the World Health Organization was already evident. This condition refers to a diminished inclination to adhere to prescribed protective measures, which evolves progressively and is impacted by a variety of beliefs, emotions, and experiences.7,8 The responsibility of managing patients dealing with pandemic fatigue, exacerbated by their individual social and economic challenges, has intensified the emotional strain experienced by healthcare professionals directly involved in patient care.
This study aimed to identify the work-related factors that significantly impact the mental health of the medical practitioners who provide care for COVID-19 patients, following two years into the pandemic. Through the identification of these factors, healthcare organizations and medical systems stakeholders can adopt evidence-based measures to enhance the quality of medical practice. Initiating interventions that could include managing working conditions, offering support services like psychological counseling, and fostering the development of resilient professionals from the early stages of university training can be viable strategies to implement, within a cost-effective approach.
Materials and Methods
A quantitative, non-experimental, comparative design was proposed. The mental health variables (anxiety, depression, and stress) were assessed with dedicated psychometric scales. The data were processed using version 20 of the IBM SPSS Statistics program. The Shapiro–Wilk normality test revealed that the data did not have a Gaussian distribution. Therefore, non-parametric analyses (the Mann–Whitney U-test, the Kruskal–Wallis test, and Dunn-Bonferroni’s post hoc tests) were used to evaluate group differences. The chi-square test was employed to analyze significant associations among variables. Using logistic regressions, the effects of several parameters on the likelihood that participants exhibit anxiety, depression, and stress were determined. For all findings, a two-tailed analysis was conducted, using a predetermined level of 0.05 for statistical significance.
Participants
The present study involved a cohort of 300 healthcare professionals recruited from four distinct hospitals situated in Timisoara, Romania, as presented in Table 1. These participants were evenly distributed between two groups, with half of them serving in medical units specifically designated for patients infected with SARS-CoV-2 (herein referred to as the “COVID section”), while the remaining half operated in non-COVID departments, encompassing a broad spectrum of 27 medical specialties.
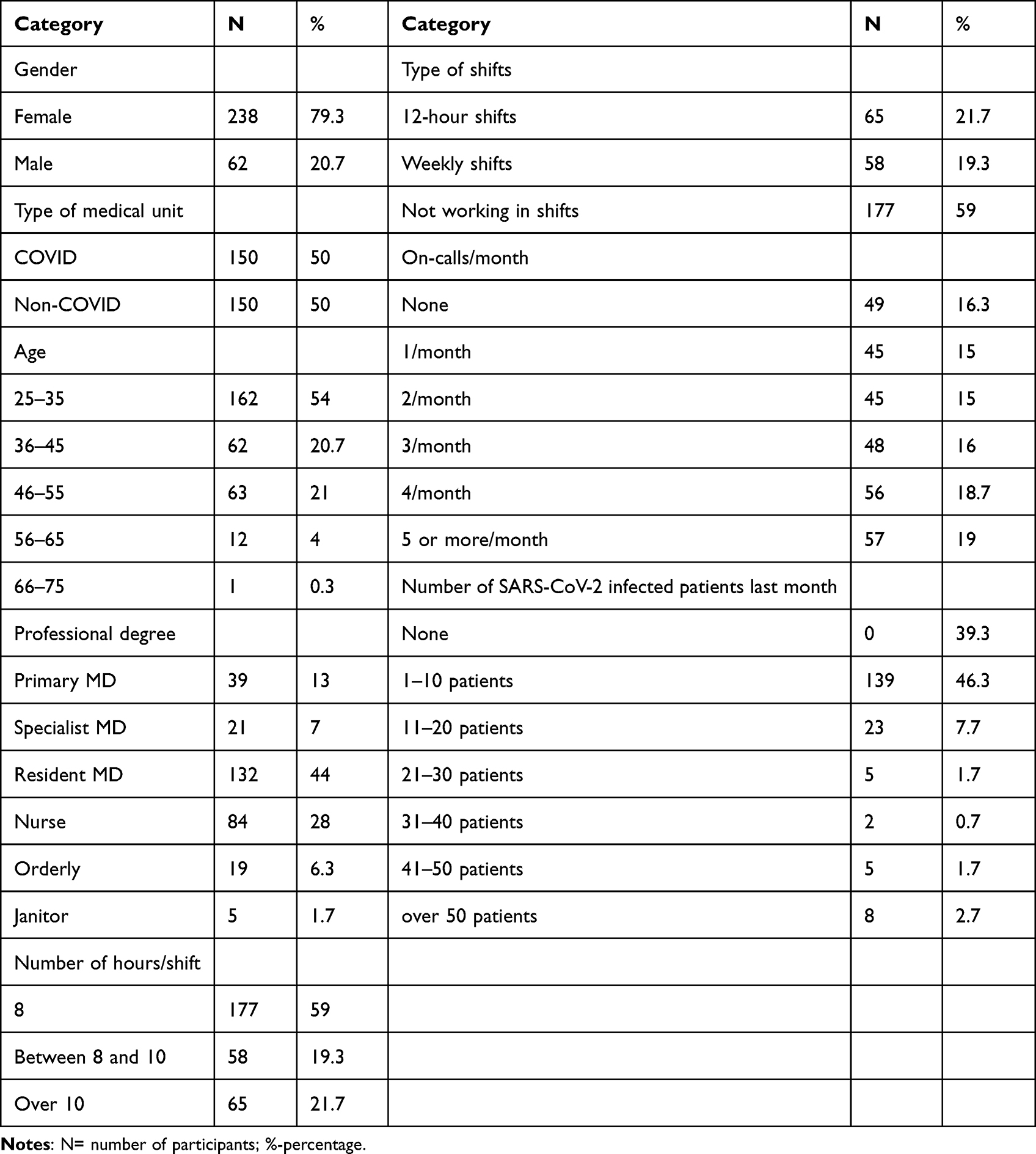 |
Table 1 Descriptive Summary of the Participants |
Regarding the demographic composition of the sample, it is noteworthy that a substantial majority of participants were female, accounting for approximately 79.3% of the total cohort. Furthermore, doctors were predominantly represented, constituting 92% of the participants. Among doctors, residents were the most prevalent, comprising 44% of the sample. In terms of age distribution, the age group ranging from 46 to 55 years exhibited the highest prevalence, comprising 21% of the overall participants.
The investigation also considered various work-related factors in its analysis, which are presented in Table 1. These factors encompassed the following variables: shift work patterns, number of hours worked per day, frequency of monthly shifts, and the extent of contact with SARS-CoV-2-infected patients treated within the preceding month.
Instruments
The assessment of the mental health of the healthcare professionals was carried out on three distinct variables, namely anxiety, depression, and stress. Three distinct assessment tools were employed to quantify each of the three variables in this study.
The assessment of anxiety levels amidst the participants was performed with the “Beck Anxiety Inventory (BAI)”, a widely recognized and psychometrically validated instrument.9 The BAI is designed to comprehensively measure the presence and severity of anxiety symptoms by employing a set of 21 items. Each item is specifically designed to measure various somatic and cognitive symptoms associated with anxiety. To assess the magnitude of anxiety symptoms, a 4-point Likert scale was utilized. The BAI score ranges from 0 to 63, encompassing the entire spectrum of anxiety symptom severity. To facilitate the interpretation of anxiety levels, the BAI provides a classification system that categorizes scores into five different anxiety levels.
The assessment of depressive symptoms among healthcare professionals was conducted using the “Beck Depression Inventory (BDI)”.10 The BDI is a 21-item instrument developed to evaluate the frequency of depressive symptoms encountered in the preceding week. Participants were asked to express the intensity of their depressive symptoms, on four levels, from “absence of sadness “to” overwhelming sadness or unhappiness”. The BDI classifies depressive symptom severity into six distinct levels, the BDI’s total score permits the classification of depressive symptom severity based on predetermined ranges.
To measure the intensity of perceived stress among healthcare professionals, “The Perceived Stress Scale (PSS-10)” was used.11 The PSS-10 is a 10-item validated instrument aimed to assess the degree to which individuals perceived commonplace circumstances to be unpredictable, uncontrollable, or overwhelming in the last month. Participants were requested to score the frequency of the perceived stress on a five-level scale, with higher scores denoting higher stress levels.
In addition to the measures of mental health, a supplementary section comprising 11 demographic questions was included at the outset of the questionnaires. These questions aimed to gather information regarding various demographic characteristics of the participants. Specifically, the demographic questionnaire sought information about the participants’ age, gender, the specific hospital and medical unit in which they were employed, whether their department treated COVID-19 patients or not, professional degree, the number of working hours per shift, the frequency of on-calls per month, and the number of patients treated for SARS-CoV-2 infection within the preceding month. The inclusion of these demographic questions allowed for a comprehensive characterization of the participants and provided important needed information for the work-related factors analyses.
Results
To ensure the statistical validity of the findings, a preliminary assessment was conducted to examine the normality of the data distribution before conducting any inferential analyses. The obtained results from the psychometric tests (for anxiety, depression, and stress) did not exhibit a Gaussian distribution, as determined by the Shapiro–Wilk test (p<0.05). Consequently, non-parametric tests were employed for the assessment of these results.
To ascertain the severity of mental health issues experienced by healthcare professionals, a frequency analysis of anxiety, depression, and stress symptoms was conducted (Table 2).
 |
Table 2 Intensity of Symptoms Frequency Distribution |
The results revealed that the majority of healthcare professionals reported experiencing mild symptoms of anxiety, accounting for 47.7% of the participants. In terms of stress levels, a significant percent of the participants (65.3%) reported moderate levels of stress. Furthermore, the analysis indicated that a substantial percent of the healthcare professionals (67%) did not exhibit any depressive symptoms, while 33% of the participants reported mild symptoms of depression.
Professional Degree
An important professional factor that was considered in this study is the participants’ professional degree. A Kruskal–Wallis test was conducted to assess the variations in symptoms among distinct professional degrees. The results revealed statistically significant differences in anxiety (p = 0.02), depression (p < 0.0001), and stress (p = 0.04) across the various professional degrees (Table 3).
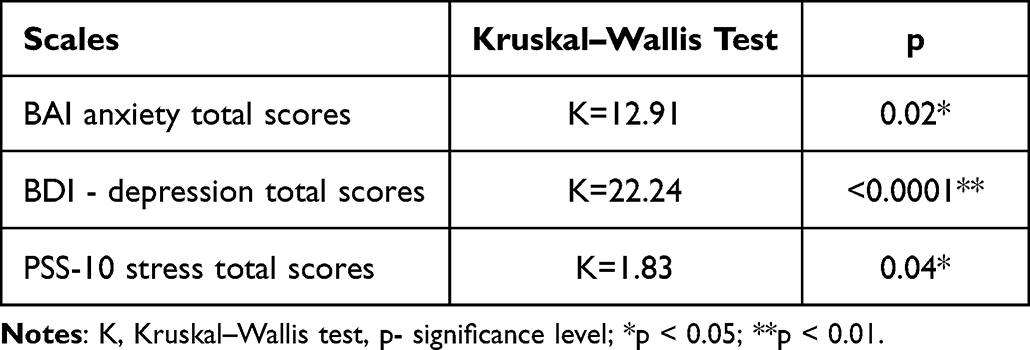 |
Table 3 Kruskal–Wallis Test for Differences Between Symptoms for Various Professionals Degrees |
To further investigate the differences in symptoms among different professional degrees, Dunn’s post hoc analysis with Bonferroni correction was conducted for BAI, BDI, and PSS-10 scores. Pairwise post-hoc Dunn tests revealed significant differences in anxiety. Specifically, significant differences were found between specialists MD (N=21) and orderly (N=19) (p=0.035), as well as between specialists MD (N=21) and residents MD (N=132) (p=0.034).
For depression, significant differences were observed between specialists MD (N=21) and orderly (N=19) (p=0.03), between specialists MD (N=21) and nurses (N=84) (p=0.009), and between primary MD (N=39) and nurses (N=84) (p=0.04). After the application of the Bonferroni correction, the post hoc did not uncover any statistically significant variances in stress levels.
A chi-square test was carried out to explore the differences in symptom intensity for anxiety, depression, and stress, based on professional degree. The results demonstrated that there was a significant association between professional degree and the intensity of depressive symptoms (χ2 = 26.4, p = 0.003). However, no significant associations were found between professional degree and the intensity of anxiety (χ²=20.26, p=0.16) or stress symptoms (χ²=16.85, p=0.78). These findings suggest that the professional degree of participants plays a role specifically in the intensity of depressive symptoms, but not in the intensity of anxiety or stress symptoms. Professionals with higher qualifications, such as specialists MD, may experience increased symptoms of anxiety and depression in comparison to professionals with lower qualifications.
Type of Medical Unit (COVID Vs Non-COVID)
To evaluate the differences between healthcare specialists from COVID and non-COVID medical units in terms of anxiety, depression, and stress, a Mann–Whitney U-test was conducted (Table 4). Significant differences in anxiety symptoms were observed between participants working in COVID units (Mdn = 13, n = 150) and non-COVID units (Mdn = 8.5, n = 150), with a Mann–Whitney U value of 8511.5, z = −3.64, p < 0.001. Similarly, significant differences in depressive symptoms were found between participants working in COVID units (Mdn = 0.38, n = 150) and non-COVID units (Mdn = 0.28, n = 150), with a Mann–Whitney U value of 9462, z = −2.38, p = 0.01. These findings demonstrate that healthcare professionals working in COVID units reported notably higher scores for anxiety and depressive symptoms compared to their colleagues working in non-COVID units.
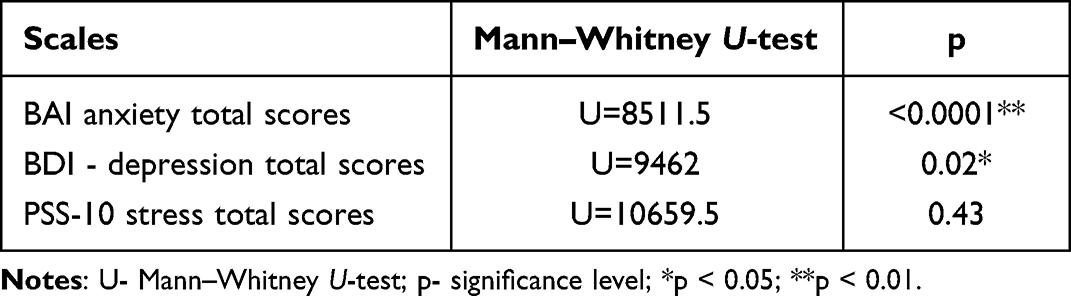 |
Table 4 Mann–Whitney U-Test for Anxiety, Depression, and Stress by COVID and Non-COVID Medical Units |
A chi-square test was carried out to explore the differences in intensity of symptoms based on the type of medical unit. The results indicated that there was a significant association between the type of medical unit and the intensity of anxiety symptoms (χ²=12.21, p=0.007). However, no significant associations were found between the type of medical unit and the intensity of depressive symptoms (χ²=2.78, p=0.24) or stress symptoms (χ²=0.63, p=0.72). These findings suggest that the type of medical unit in which participants work (COVID or non-COVID) plays a role specifically in the intensity of anxiety symptoms, but not in the intensity of depressive or stress symptoms.
Number of Hours Spent in a Single Shift
Based on the number of hours spent per shift, participants were divided into three independent groups: those working up to 8 hours daily, those working 8–10 hours daily, and those working over 10 hours daily. To investigate the potential differences in symptoms across these groups, the Kruskal–Wallis test was conducted.
The results of the Kruskal–Wallis test revealed no significant differences induced by the number of hours spent in a single shift, for depressive symptoms (p = 0.94), anxiety symptoms (p = 0.56), or stress symptoms (p = 0.35). Additionally, no significant associations were observed between the hours spent at work in a shift and the intensity of participants’ anxiety symptoms (χ² = 0.83, p = 0.99), depressive symptoms (χ² = 1.12, p = 0.89), or stress symptoms (χ² = 6.28, p = 0.17).
These findings suggest that the number of hours spent per shift does not appear to exert a substantial impact on the severity of symptoms experienced by medical professionals in terms of anxiety, depression, or stress.
Type of Shifts
Based on the type of shifts, participants were categorized into three independent groups: those working 12-hour shifts, those working weekly shifts, and those not working in shifts. The results of the Kruskal–Wallis test revealed no significant differences induced by the type of shifts for anxiety symptoms (p = 0.81), depressive symptoms (p = 0.45), or stress symptoms (p = 0.60). Additionally, no significant associations were observed between the type of shifts and the intensity of participants’ anxiety symptoms (χ²=3.002, p=0.81), depressive symptoms (²=1.78, p=0.77), or stress symptoms (χ²=0.33, p=0.98). The type of shift does not appear to significantly impact the intensity of mental health symptoms experienced by medical professionals.
On-Calls/Month
Six possible groups emerged: none, 1/month, 2/month, 3/month, 4/month, and 5 or more/month. The results of the Kruskal–Wallis test indicated significant differences induced by the number of on-calls/month for anxiety (p = 0.02), depression (p < 0.0001) and stress (p = 0.04) (see Table 5). To further investigate the differences in symptoms among different on-calls/month, Dunn’s post-hoc analysis with Bonferroni correction was conducted for BAI, BDI, and PSS-10 scores. For anxiety symptoms, significant differences were found between participants with 3 calls/month (N=48) and 1 call/month (N=45) (p=0.03), between those with 4 calls/month (N=56) and 1 call/month (N=45) (p=0.03), and between those with 5 calls/month (N=57) and 1 call/month (N=45) (p=0.001).
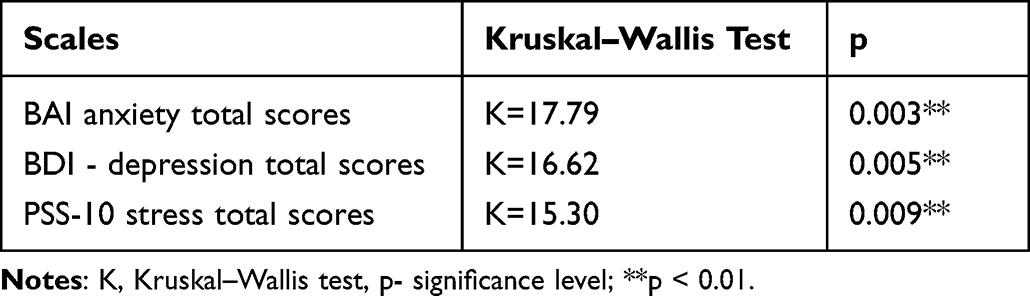 |
Table 5 Kruskal–Wallis Test for Differences Between Symptoms for Number of on-Calls/Month |
Regarding depressive symptoms, significant differences were observed between participants with no on-calls (N=49) and 1 on-call/month (N=45) (p=0.02), as well as between those with 3 calls/month (N=57) and 1 call/month (N=45) (p=0.01).
For stress symptoms, significant differences were found between participants with no on-calls (N=49) and 1 on-call/month (N=45) (p=0.02), as well as between those with 3 calls/month (N=48) and 1 call/month (N=45) (p=0.01).
These findings suggest that the number of on-calls per month is associated with significant differences in anxiety, depression, and stress symptoms. Participants with no shifts or higher numbers of on-calls per month tend to exhibit higher levels of these symptoms compared to those with fewer on-calls.
A chi-square test was conducted to investigate the differences in symptom intensity based on number of shifts/month. The results indicated that there was a significant association between the number of shifts/month and the intensity of anxiety symptoms (χ²=36.84, p=0.001). However, no significant associations were found for depression (χ²=18.20, p=0.052) or stress symptoms (χ²=17.14, p=0.07).
Number of SARS-Cov-2 Infected Patients in the Last Month with Whom Participants Had Been in Contact
Seven possible groups emerged: none, 1–10 patients, 11–20 patients, 21–30 patients, 31–40, 41–50 patients and over 50 patients. The results of the Kruskal–Wallis test indicated significant differences induced by the number of SARS-CoV-2 infected patients for anxiety (p = 0.02), depression (p < 0.0001) and stress (p = 0.04) (see Table 6).
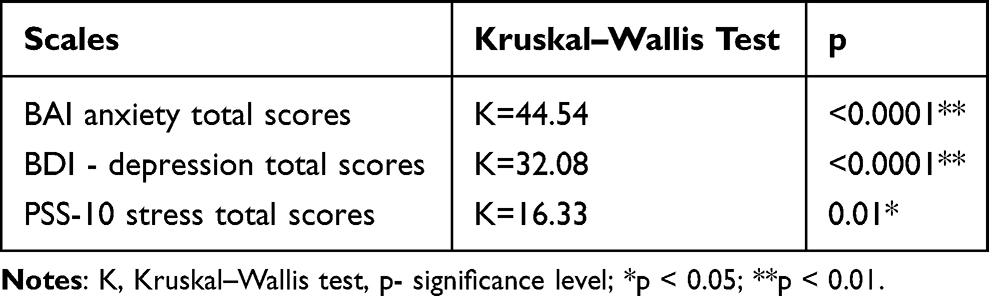 |
Table 6 Kruskal–Wallis Test for Differences Between Symptoms of Anxiety, Depression and Stress for Number of SARS-CoV-2 Infected Patients in the Last Month with Whom Participants Had Been in Contact |
To further investigate the differences in symptoms among different number of SARS-CoV-2 patients, Dunn’s post-hoc analysis with Bonferroni correction was conducted for BAI, BDI, and PSS-10 scores. For anxiety symptoms, significant differences were found between participants with contact with 1–10 patients (N=139) and with no contact (N=118) (p<0.0001), between those in contact with 41–50 patients (N=5) and no contact (N=118) (p=0.005), and between those in contact with over 50 patients (N=8) and no contact (N=118) (p=0.004). Regarding depressive symptoms, significant differences were found between participants with contact with 1–10 patients (N=139) and with no contact (N=118) (p<0.0001). For stress symptoms, significant differences were found between participants with contact with 1–10 patients (N=139) and with no contact (N=118) (p<0.008).
A chi-square test was conducted to investigate the differences in symptom intensity based on the number of SARS-Cov-2 infected patients in the last month with whom participants had been in contact. The results indicated that there was a significant association between the number of patients and the intensity of anxiety symptoms (χ²=61.09, p<0.0001). However, no significant associations were found for depression (χ ²=20.92, p=0.052) or stress symptoms (χ²=17.99, p=0.11).
Logistic Regressions
A logistic regression analysis was conducted to examine the effects of various parameters (gender, age, professional degree, number of hours worked per a single shift, type of shifts, number of on-calls/month, loss of a relative following SARS-CoV-2 infection, number of patients with SARS-CoV-2 infection treated, BDI score for depression, PSS-10 stress score) on the presence of self-assessed anxiety among the participants. The overall model was found to be statistically significant, χ2(59) = 183.73, p < 0.0001, explaining 65% of the variance (Nagelkerke R2) and accurately classifying 86.7% of the cases. Several factors were found to be significantly associated with a higher probability of experiencing anxiety:
- Participants who worked weekly shifts had a significantly higher probability of presenting anxiety compared to those who did not work shifts or worked 12-hour shifts (p = 0.03). They had a 11.99 times higher probability (95% CI [1.31; 109.54]) of developing anxiety.
- Participants who performed 1 guard per month had a significantly higher probability of developing anxiety compared to those who did not perform guards or performed more than 2 guards per month (p = 0.03). They had a 0.16 times higher probability (95% CI [0.03; 0.83]) of experiencing anxiety.
- Participants who worked between 8 and 10 hours per day had a significantly higher probability of developing anxiety compared to those who worked less than 8 hours or more than 10 hours per day (p = 0.04). They had a 10.18 times higher probability (95% CI [1.17; 88.92]) of experiencing anxiety.
- Participants with higher PSS-10 stress scores had a significantly higher probability of presenting anxiety (p = 0.001). They had a 1.07 times higher probability (95% CI [1.07, 1.29]) of experiencing anxiety for each unit increase in PSS-10 score.
- Participants with higher scores on the BECK inventory for depressive symptomatology had a significantly higher probability of presenting anxiety (p < 0.0001). They had a 358.88 times higher probability (95% CI [33.48; 3846.71]) of experiencing anxiety for each unit increase in the BECK score.
These findings suggest that factors such as working weekly shifts, performing 1 guard per month, working between 8 and 10 hours per day, higher stress and depressive scores are associated with an increased likelihood of experiencing anxiety among the participants.
A logistic regression analysis was conducted to examine the effects of several parameters age, gender, professional degree, number of hours worked per a single shift, type of shifts, number of on-calls/month, loss of a relative following SARS-CoV-2 infection, number of patients with SARS-CoV-2 infection treated, BAI score for anxiety, PSS-10 stress score) on the presence of self-assessed depressive symptoms among the participants.
The logistic regression model was found to be statistically significant, χ2(33) = 203.25, p < 0.0001, explaining 69% of the variance (Nagelkerke R2) and correctly classifying 87.7% of the cases.
Several factors were found to be significantly associated with a higher probability of experiencing depressive symptoms:
- Participants who faced the death of a family member post-SARS-Cov-2 infection had a significantly higher probability of experiencing depression compared to those who did not face such a situation (p = 0.01). They had a 0.21 times higher probability (95% CI [0.06, 0.71]) of experiencing depression.
- Participants with higher PSS-10 stress scores had a significantly higher probability of experiencing depression (p < 0.0001). They had a 1.29 times higher probability (95% CI [1.16, 1.43]) of experiencing depression for each unit increase in PSS-10 score.
- Participants with higher anxiety scores on BAI had a significantly higher probability of experiencing depression (p < 0.0001). They had a 1.14 times higher probability (95% CI [1.09, 1.21]) of experiencing depression for each unit increase in BAI score.
These findings suggest that factors such as facing the death of a family member post-SARS-CoV-2 infection, higher stress and anxious symptomatology are associated with an increased likelihood of experiencing depressive symptoms among the participants.
A logistic regression analysis was conducted to examine the effects of several parameters age, gender, professional degree, number of hours worked per a single shift, type of shifts, number of on-calls/month, loss of a relative following SARS-CoV-2 infection, number of patients with SARS-CoV-2 infection treated, BDI depression score, BAI anxiety score, on the presence of self-assessed stress-related symptoms among the participants.
The logistic regression model was found to be statistically significant, χ2(33) = 122.08, p < 0.0001, explaining 49% of the variance (Nagelkerke R2) and correctly classifying 83% of the cases.
Several factors were found to be significantly associated with a higher probability of presenting high levels of stress:
- Participants who perform 4 guards per month had a significantly higher probability of presenting high levels of stress compared to those who do not perform guards or perform below or over 4 guards per month (p = 0.049). They had a 3.67 times higher probability (95% CI [1.01, 13.41]) of presenting high levels of stress.
- Participants with higher scores on the BAI had a significantly higher probability of presenting high levels of stress (p = 0.04). They had a 1.07 times higher probability (95% CI [1.01, 1.14]) of presenting high levels of stress for each unit increase in BAI score for anxiety.
- Participants with higher scores on the BDI for depressive symptomatology had a significantly higher probability of presenting high levels of stress (p < 0.0001). They had a 136.67 times higher probability (95% CI [16.42, 1137.53]) of presenting high levels of stress for each unit increase in the BECK score for depression.
These findings suggest that factors such as performing 4 guards per month, higher scores on the anxiety and depression are associated with an increased likelihood of presenting high levels of stress among the participants.
Discussion
This study applied a non-experimental comparative design to examine the impact of various work-related factors on the mental health of healthcare professionals. We aimed to assess the workplace factors documented in specialized literature that are known to influence mental health: professional degree, type of medical unit (COVID or non-COVID), number of hours worked per shift, type of shifts, monthly on-call frequency, and the number of SARS CoV-2 patients treated in the previous month.12–16 Anxiety, depression and stress were assessed as mental health most relevant measures, as reported in scientific literature.17 The main goal was to evaluate how these factors influence the levels of anxiety, depression, and stress among healthcare professionals. Non-parametric tests were employed to examine the data and determine the significance of the differences induced by these factors and mental health outcomes. The findings revealed that a significant percentage of healthcare professionals reported experiencing mild symptoms of anxiety, while a substantial percentage reported moderate levels of stress with only a third experiencing mild depressive symptoms (similar with Sun et al, 2021).18 These findings underscore the psychological consequences of the pandemic on healthcare professionals, emphasizing the necessity for targeted interventions and support systems to attend to their mental health needs.19 It is crucial for healthcare organizations to recognize and prioritize the mental well-being of their employees to guarantee the provision of high-quality healthcare and prevent burnout.20
In our study, the findings indicate that doctors exhibit higher levels of anxiety, depression, and stress compared to professionals with lower qualifications, such as nurses, orderlies, or janitors. Moreover, the degree and qualification of the professionals appear to influence the intensity of depressive symptoms but not anxiety or stress symptoms. Specifically, a higher level of qualification is associated with a greater reporting of depressive symptoms. Among the primary MDs, higher levels of depressive symptoms were reported compared to specialists or residents.These results contradict previous studies that reported nurses as having higher depressive symptoms.21 The divergent findings observed in this study may be attributed to the influence of cultural disparities inherent in the training system of medical personnel and the prevailing system of professional hierarchies within hospitals. Cultural factors play a significant role in shaping the norms, values, and expectations within a given society, including the medical profession.22,23 The training system for medical personnel differs across countries and regions, encompassing variations in educational curricula, clinical rotations, and supervision practices.24 These dissimilarities may lead to differences in exposure to stressors, the development of coping mechanisms, and the overall resilience of healthcare professionals. Consequently, the varying levels of anxiety, depression, and stress observed amidst medical personnel in this study could be attributed to the cultural variations in training programs and the unique challenges they entail. Furthermore, the hierarchical structure within hospitals, which assigns varying levels of authority and responsibility to different professional roles differ across organizational cultures, can also contribute to the divergent findings.24 In some cultural contexts, there may be a strong emphasis on hierarchy and deference to seniority within the medical profession. This hierarchical system may result in increased pressure and expectations placed on healthcare professionals occupying higher positions, such as specialists or senior physicians, leading to heightened anxiety and depression in comparison to their counterparts in lower positions.25 Conversely, healthcare professionals in lower positions may experience different stressors associated with their roles and responsibilities, leading to variations in mental health outcomes.
Throughout the COVID-19 pandemic, specific medical units have been designated either for the care of patients infected with SARS-CoV-2 or for handling non-COVID cases, with the primary objective of minimizing the risk of contamination. It is widely recognized that healthcare professionals working in COVID units experience significant impacts on their well-being and mental health.26 The inherent nature of their work in these high-risk environments, combined with the unique challenges and stressors associated with managing a highly contagious and potentially life-threatening virus, can have profound effects on their psychological and emotional states.27
The findings of the current study offer additional evidence that supports the idea that healthcare professionals employed in COVID units exhibit significantly higher levels of anxiety and depressive symptoms compared to their counterparts in non-COVID units.11 This suggests that the specific type of medical unit in which healthcare professionals work plays a role specifically in the intensity of anxiety symptoms, while not significantly affecting the intensity of depressive or stress symptoms.
These findings are consistent with prior research, elucidating work-related factors that contribute to heightened levels of anxiety among healthcare practitioners in COVID units. Specifically, these factors include increased exposure to critically ill patients, constant fear of acquiring the virus and transmitting it to family members, and the overwhelming workload.28 The demanding nature of providing care in COVID units, with its associated risks and uncertainties, can lead to a heightened sense of anxiety among healthcare professionals.29
It is crucial to recognize the necessity of introducing interventions to promote the well-being and psychological health of healthcare professionals.30 Institutions and healthcare organizations should prioritize allocating resources for mental health support systems to meet the specific needs of individuals working in COVID units.31 These resources may include access to mental health counseling, regular check-ins with healthcare professionals to assess their well-being, and the implementation of strategies to mitigate stress and promote resilience.32 Additionally, fostering a supportive and empathetic work environment, where healthcare professionals feel valued and supported, can contribute to reducing the impact of anxiety symptoms and enhancing their overall well-being.33
The number of hours spent at work has been consistently acknowledged as a significant work-related factor in relation to occupational well-being in the medical profession.34 In the present research, the number of hours spent at work was operationalized using three variables: the number of hours spent at work in a single shift, the type of shifts, and the monthly on-call frequency. Prior research has demonstrated that an increase in the duration of work hours can have adverse effects on the well-being and mental health of medical personnel.13 However, the findings of the study did not reveal significant results for two of the variables: the number of hours spent per shift and the type of shifts. These variables did not show statistically significant differences in symptoms of anxiety, depression, or stress among the healthcare professionals. In contrast, the number of on-calls per month was determined to have an effect on mental health outcomes, as previous studies.35 Participants who had no shifts or a higher number of on-calls per month tended to demonstrate elevated levels of symptoms related to anxiety, depression, and stress in contrast to those with fewer on-calls. This finding indicates that the frequency of on-calls, rather than the duration of a single shift or the type of shift, is a more influential factor in determining the mental health outcomes of healthcare professionals. These results align with previous research highlighting the adverse consequences of extended working hours and increased work demands on the mental health of medical personnel.36,37 Healthcare organizations must take into account the impact of on-call frequency on the well-being of their employees and implement strategies that promote a healthy work-life balance. These strategies may include workload management, appropriate staffing levels, and providing support and resources for healthcare professionals to cope with the demands associated with on-call duties.38
The impact of contact with and providing care for individuals affected by SARS-CoV-2 has been a topic of frequent investigation throughout the pandemic.39 Previous research has shown that providing care to this patient population can lead to a range of mental health issues (such as anxiety, depression) (Guo et al, 2020) or increased stress (Roy et al, 2020).40,41
In the present study, we aimed to assess the impact of contact with SARS-CoV-2 patients by quantifying the number of cases with which the medical staff had direct contact. The range of contact varied from no cases to over 50 cases. Our findings revealed significant differences in mental health symptoms based on the number of patients encountered. Specifically, there was a notable difference between healthcare practitioners who directly interacted with patients infected with SARS-CoV-2 compared to those who did not, indicating that the presence of any patient with SARS-CoV-2 increased the anxiety levels of heathcare professionals.42 Moreover, as the number of patients with whom the medical staff came into contact increased, the symptoms became more pronounced.
These results align with previous research highlighting the possible adverse consequences of delivering care to individuals infected with SARS-CoV-2 (similar to Buselli et al, 2020).43 The nature of working closely with individuals who have a highly contagious and potentially life-threatening virus can induce a various mental health challenges among healthcare professionals. The cumulative impact of caring for a larger number of patients further exacerbates these symptoms.
Significant differences in all three measured variables, anxiety, depression, and tension, were determined by professional degree, number of on-calls per month, and interactions with patients who have contracted SARS-CoV-2. Working in a COVID unit was significant only for anxious and depressive symptoms.
Factors such as working weekly shifts, performing 1 guard per month, working between 8 and 10 hours per day, and higher stress and depressive symptoms are linked to a higher probability of experiencing anxiety among the participants. Factors such as facing the death of a family member post-SARS-CoV-2 infection, higher stress and anxious symptomatology relate to an increased likelihood of experiencing depressive symptoms. Factors such as performing 4 on-calls per month, higher scores on anxiety and depression are linked to a higher probability of presenting high levels of stress.
Anxiety, depression, and stress are interconnected dimensions of mental health that often coexist and have significant implications for overall well-being.44 These psychological states can mutually influence and exacerbate one another, leading to detrimental effects on an individual’s ability to perform their work effectively. It is therefore crucial to recognize the impact of these mental health challenges, particularly among medical personnel who treat patients who have been infected with SARS-CoV-2, and to provide appropriate counseling and support services.44
Several Limitations
Several limitations should be acknowledged in this study. First, the sample of healthcare workers enrolled in this study did not accurately represent the entire population of medical personnel. The study was conducted within a particular setting and geographical region, potentially restricting the generalizability of the findings to different healthcare settings or populations. To enhance the generalizability of the findings, future research could consider conducting comparative studies on medical systems from diverse countries. Second, the study focused on specific work-related factors, such as professional degree, type of medical unit, duration of each working shift, type of shifts, monthly on-call frequency, and number of SARS-CoV-2 patients treated. Other potentially relevant organizational factors such as supervision, responsibilities, and recognition were not included in the analysis. Future studies could consider a more comprehensive approach by incorporating a wider range of work-related and individual factors.
Finally, the study did not explore the effectiveness of specific interventions or support systems in mitigating the effect of work-related factors on mental health outcomes. Future research could investigate the efficacy of other programs directed toward addressing the mental health needs of healthcare professionals and examine the factors that contribute to their success.
Conclusion
This non-experimental comparative study aimed to explore the impact of work-related factors on the mental health of healthcare professionals during the COVID-19 pandemic. The results revealed a significant psychological burden experienced by healthcare workers. Those working in COVID units reported elevated levels of anxiety and depressive symptoms in contrast to those in non-COVID units, emphasizing the need for targeted interventions and support systems in high-risk environments.
The professional degree of participants also played a role in the intensity of mental health-related issues. Doctors reported higher levels of these symptoms than other healthcare professionals. This finding suggests the existence of unique stressors and challenges faced by doctors that warrant further investigation.
Furthermore, the frequency of on-call duties impacted mental health outcomes. Healthcare professionals with either no on-call duties or a higher number of on-calls per month experienced elevated levels of anxiety, depression, and stress symptoms. To mitigate these effects, healthcare organizations should prioritize workload management and implement strategies to support the mental well-being of their employees.
Additionally, contact with COVID-19 patients was associated with increased symptomatology across all three variables. Healthcare professionals who had contact with a higher number of SARS-CoV-2 patients reported more significant levels of anxiety, depression, and stress. This highlights the psychological impact of caring for individuals with the virus and emphasizes the importance of implementing measures to protect healthcare professionals’ well-being.
In conclusion, this study contributes to the understanding of work-related factors that significantly affect the mental health of healthcare professionals during the pandemic. It stresses the importance of prioritizing the mental well-being of healthcare workers, providing comprehensive mental health resources, and fostering a supportive work environment. By addressing these factors, healthcare organizations can better support their staff, deliver quality care, and prevent burnout. Further research is necessary to deepen our knowledge of these factors and develop targeted interventions to support healthcare professionals in their crucial roles.
Ethics and Consent Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Infectious Diseases and Pneumophtisiology Victor Babes Hospital, Nr.5059 from 28 May 2021. Data was collected online via a link sent by email. All gathered information was confidential; the participation was entirely voluntary and written informed consent was obtained from all the participants.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bradley M, Chahar P. Burnout of healthcare providers during COVID-19. CCJM. 2020;2020:1.
2. Shanafelt T, Ripp J, Trockel M. Understanding and addressing sources of anxiety among health care professionals during the COVID-19 pandemic. JAMA. 2020;323(21):2133. doi:10.1001/jama.2020.5893
3. Briciu V, Leucuta DC, Tőkés GE, Colcear D. Burnout, depression, and job stress factors in healthcare workers of a romanian COVID-19 dedicated hospital, after two pandemic years. IJERPH. 2023;20(5):4118. doi:10.3390/ijerph20054118
4. Daviu N, Bruchas MR, Moghaddam B, Sandi C, Beyeler A. Neurobiological links between stress and anxiety. Neurobiol Stress. 2019;11:100191. doi:10.1016/j.ynstr.2019.100191
5. Dehelean L, Papava I, Musat MI, et al. Coping strategies and stress related disorders in patients with COVID-19. Brain Sci. 2021;11(10):1287. doi:10.3390/brainsci11101287
6. Yip YC, Yip KH, Tsui WK. The transformational experience of junior nurses resulting from providing care to COVID-19 patients: from facing hurdles to achieving psychological growth. IJERPH. 2021;18(14):7383. doi:10.3390/ijerph18147383
7. Our World in Data. Romania: coronavirus Pandemic Country Profile; 2022. Available from: https://ourworldindata.org/corona-virus/country/romania#daily-confirmed-deaths-how-do-they-compare-to-other-countries.
8. Pandemic fatigue—reinvigorating the public to prevent COVID-19. policy framework for supporting pandemic prevention and management. WHO Regional Office for Europe: Copenhagen, Denmark; 2020. Available from: https://apps.who.int/iris/bitstream/handle/10665/335820/WHO-EURO-2020-1160-40906-55390-eng.pdf.
9. Beck AT, Epstein N, Brown G, Steer R. Beck Anxiety Inventory. J Consult Clin Psychol. 2012;2012:1. doi:10.1037/t02025-000
10. Amagasa T, Nakayama T. Relationship between long working hours and depression: a 3-year longitudinal study of clerical workers. J Occup Environ Med. 2013;55(8):863–872. doi:10.1097/JOM.0b013e31829b27fa
11. Al-Amer R, Malak Malakeh Z, Aburumman G, et al. Prevalence and correlates of psychological reactions among jordanian nurses during the coronavirus disease 2019 pandemic; 2020. Available from: https://www.researchsquare.com/article/rs-35820/v1.
12. Heponiemi T, Kouvonen A, Vänskä J, et al. Effects of active on-call hours on physicians’ turnover intentions and well-being. Scand J Work Environ Health. 2008;34(5):356–363.
13. Spoorthy MS, Pratapa SK, Mahant S. Mental health problems faced by healthcare workers due to the COVID-19 pandemic–A review. Asian J Psychiatr. 2020;51:102119. doi:10.1016/j.ajp.2020.102119
14. Cohen S, Kamarck T, Mermelstein R. Perceived Stress Scale. Measuring Stress. 2014;2014:1. doi:10.1037/t02889-000
15. Braquehais MD, Vargas-Cáceres S, Gómez-Durán E, et al. The impact of the COVID-19 pandemic on the mental health of healthcare professionals. QJM. 2020;113(9):613–617. doi:10.1093/qjmed/hcaa207
16. Chutiyami M, Cheong AMY, Salihu D, et al. COVID-19 pandemic and overall mental health of healthcare professionals globally: a meta-review of systematic reviews. Front Psychiatry. 2022;12:804525. doi:10.3389/fpsyt.2021.804525
17. Sun P, Wang M, Song T, et al. The psychological impact of COVID-19 pandemic on health care workers: a systematic review and meta-analysis. Front Psychol. 2021;12:626547. doi:10.3389/fpsyg.2021.626547
18. Vizheh M, Qorbani M, Arzaghi SM, Muhidin S, Javanmard Z, Esmaeili M. The mental health of healthcare workers in the COVID-19 pandemic: a systematic review. J Diabetes Metab Disord. 2020;19(2):1967–1978. doi:10.1007/s40200-020-00643-9
19. Liu Z, Wu J, Shi X, et al. Mental health status of healthcare workers in China for COVID-19 Epidemic. Ann Glob Health. 2020;86(1):128. doi:10.5334/aogh.3005
20. Kunz M, Strasser M, Hasan A. Impact of the coronavirus disease 2019 pandemic on healthcare workers: systematic comparison between nurses and medical doctors. Curr Opin Psychiatry. 2021;34(4):413–419. doi:10.1097/YCO.0000000000000721
21. Dragioti E, Tsartsalis D, Mentis M, Mantzoukas S, Gouva M. Impact of the COVID-19 pandemic on the mental health of hospital staff: an umbrella review of 44 meta-analyses. Int J Nurs Stud. 2022;131:104272. doi:10.1016/j.ijnurstu.2022.104272
22. Meeuwesen L, van den Brink-Muinen A, Hofstede G. Can dimensions of national culture predict cross-national differences in medical communication? Patient Educ Couns. 2009;75(1):58–66. doi:10.1016/j.pec.2008.09.015
23. World Health Organization. Education and Training: Technical Series on Safer Primary Care. Geneva: World Health Organization; 2016.
24. Speroff T, Nwosu S, Greevy R, et al. Organisational culture: variation across hospitals and connection to patient safety climate. BMJ Qual Saf. 2010;19(6):592–596. doi:10.1136/qshc.2009.039511
25. Fernandopulle N. To what extent does hierarchical leadership affect health care outcomes? Med J Islam Republ Iran. 2021;35:117.
26. Que J, Shi L, Deng J, et al. Psychological impact of the COVID-19 pandemic on healthcare workers: a cross-sectional study in China. Gen Psych. 2020;33(3):e100259. doi:10.1136/gpsych-2020-100259
27. Xiao X, Zhu X, Fu S, Hu Y, Li X, Xiao J. Psychological impact of healthcare workers in China during COVID-19 pneumonia epidemic: a multi-center cross-sectional survey investigation. J Affect Disord. 2020;274:405–410. doi:10.1016/j.jad.2020.05.081
28. Hannemann J, Abdalrahman A, Erim Y, et al. The impact of the COVID-19 pandemic on the mental health of medical staff considering the interplay of pandemic burden and psychosocial resources—A rapid systematic review. PLoS One. 2022;17(2):e0264290. doi:10.1371/journal.pone.0264290
29. Boluarte Carbajal A, Sánchez Boluarte A, Rodríguez Boluarte A, Merino Soto C. Working conditions and emotional impact in healthcare workers during COVID-19 pandemic. J Healthc Qual Res. 2020;35(6):401–402. doi:10.1016/j.jhqr.2020.08.002
30. Perego G, Cugnata F, Brombin C, et al. Analysis of healthcare workers’ mental health during the COVID-19 pandemic: evidence from a three-wave longitudinal study. J Health Psychol;2023. 135910532311680. doi:10.1177/13591053231168040
31. Gupta N, Dhamija S, Patil J, Chaudhari B. Impact of COVID-19 pandemic on healthcare workers. Ind Psychiatry J. 2021;30(3):282. doi:10.4103/0972-6748.328830
32. Kandula UR, Wake AD. Assessment of quality of life among health professionals during COVID-19: review. JMDH. 2021;14:3571–3585. doi:10.2147/JMDH.S344055
33. Khajuria A, Tomaszewski W, Liu Z, et al. Workplace factors associated with mental health of healthcare workers during the COVID-19 pandemic: an international cross-sectional study. BMC Health Serv Res. 2021;21(1):262. doi:10.1186/s12913-021-06279-6
34. Wong K, Chan AHS, Ngan SC. The effect of long working hours and overtime on occupational health: a meta-analysis of evidence from 1998 to 2018. IJERPH. 2019;16(12):2102. doi:10.3390/ijerph16122102
35. Nicol AM, Botterill JS. On-call work and health: a review. Environ Health. 2004;3(1):15. doi:10.1186/1476-069X-3-15
36. Afonso P, Fonseca M, Pires JF. Impact of working hours on sleep and mental health. Occup Med (Chic Ill). 2017;67(5):377–382. doi:10.1093/occmed/kqx054
37. Lollis BD, Kumar M, Kaplan J, Schmelzer C, Harthcock K, Silva M. The on-call burden of physicians: discussion, recommendations and risk mitigation strategies. Clin Case Rep J. 2020;1(7):1–5.
38. Mediani HS, Adistie F, Hendrawati S, Trisyani Y. Problems facing healthcare providers when caring for COVID-19 patients: an integrative review. JMDH. 2022;15:1511–1523. doi:10.2147/JMDH.S359700
39. Roy D, Tripathy S, Kar SK, Sharma N, Verma SK, Kaushal V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J Psychiatr. 2020;51:102083. doi:10.1016/j.ajp.2020.102083
40. Guo J, Liao L, Wang B, et al. Psychological effects of COVID-19 on hospital staff: a national cross-sectional survey of China Mainland. SSRN Journal; 2020. Available from: https://www.ssrn.com/abstract=3550050.
41. Weilenmann S, Ernst J, Petry H, et al. Health care workers’ mental health during the first weeks of the SARS-CoV-2 Pandemic in Switzerland—a cross-sectional study. Front Psychiatry. 2021;12:594340. doi:10.3389/fpsyt.2021.594340
42. Buselli R, Corsi M, Baldanzi S, et al. Professional quality of life and mental health outcomes among health care workers exposed to Sars-Cov-2 (Covid-19). IJERPH. 2020;17(17):6180. doi:10.3390/ijerph17176180
43. Nowrouzi-Kia B, Sithamparanathan G, Nadesar N, Gohar B, Ott M. Factors associated with work performance and mental health of healthcare workers during pandemics: a systematic review and meta-analysis. J Public Health (Bangkok). 2022;44(4):731–739. doi:10.1093/pubmed/fdab173
44. Galbraith N, Boyda D, McFeeters D, Hassan T. The mental health of doctors during the COVID-19 pandemic. B J Psych Bull. 2021;45(2):93–97. doi:10.1192/bjb.2020.44
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Psychological Impact of Quarantine During the COVID-19 Pandemic on Quarantined Non-Healthcare Workers, Quarantined Healthcare Workers, and Medical Staff at the Quarantine Facility in Saudi Arabia
Alfaifi A, Darraj A, El-Setouhy M
Psychology Research and Behavior Management 2022, 15:1259-1270
Published Date: 17 May 2022
Spiritual Well-Being, Depression, Anxiety, and Stress in Indonesian Muslim Communities During COVID-19
Hamka, Suen MW, Ramadhan YA, Yusuf M, Wang JH
Psychology Research and Behavior Management 2022, 15:3013-3025
Published Date: 17 October 2022
Dietary Supplement Consumption and Mental Health in Indonesian Adults During Second Wave of COVID-19 Pandemic
Yusof J, d'Arqom A, Andriani AP, Nasution MZ, Fatimah N, Mustika A, Handayani S, Syed Abdul Kadir SZ
Patient Preference and Adherence 2023, 17:1799-1811
Published Date: 24 July 2023
The Association Between Cognitive Functions and Psychological Factors in Patients with Severe COPD
Hansen KK, Hilberg O, Jensen HI, Løkke A, Farver-Vestergaard I
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2065-2078
Published Date: 19 September 2023
Longitudinal Problematic Social Media Use in Students and Its Association with Negative Mental Health Outcomes
Shannon H, Bush K, Shvetz C, Paquin V, Morency J, Hellemans KGC, Guimond S
Psychology Research and Behavior Management 2024, 17:1551-1560
Published Date: 8 April 2024