Back to Journals » Infection and Drug Resistance » Volume 16
Unmet Needs in Complicated Urinary Tract Infections: Challenges, Recommendations, and Emerging Treatment Pathways
Authors Marantidis J, Sussman RD
Received 16 December 2022
Accepted for publication 24 February 2023
Published 11 March 2023 Volume 2023:16 Pages 1391—1405
DOI https://doi.org/10.2147/IDR.S382617
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Joanna Marantidis, Rachael D Sussman
Department of Urology, MedStar Georgetown University Hospital, Washington, DC, USA
Correspondence: Joanna Marantidis, 3800 Reservoir Road NW, Washington, DC, 20007, USA, Tel +1 202 444 9922, Fax +1 458 203 5006, Email [email protected]
Abstract: While urinary tract infections (UTIs) are one of the most common types of infections globally, the wide variety of presentations and of severity of disease can make it difficult to manage. The definition for uncomplicated UTIs (uUTIs) is generally regarded as UTIs in healthy, non-pregnant women whereas all other UTIs are considered complicated. There is, however, a lack of consensus definition of complicated UTIs (cUTIs), leading to global differences in management. In addition, the patients who develop complicated UTIs generally have other comorbidities that warrant more urgent intervention. One of the biggest challenges in treating cUTIs is the rise of antimicrobial resistance (AMR). While there have been recent drug approvals for new antibiotic to treat these resistant organisms, a multidisciplinary approach, including regulatory frameworks, provider education and public awareness campaigns, is crucial to limiting unnecessary treatments for asymptomatic bacteriuria (ASB) and uUTIs that can ultimately lead to more severe infections.
Keywords: antimicrobial resistance, regulatory frameworks, catheter-associated urinary tract infection, clinical trial
Introduction
Urinary tract infections (UTIs) are some of the most common infections in both the outpatient and in other healthcare settings. UTIs have a wide spectrum of clinical presentations, from benign with mild symptoms to life-threatening. As such, UTIs have been stratified as either uncomplicated or complicated. While there is no standard definition, uncomplicated UTIs (uUTIs) are generally classified as UTIs in healthy, non-pregnant women whereas all other UTIs are categorized as complicated.1 In 2011, UTIs accounted for over 400,000 hospital admissions with an estimated cost of $2.8 billion in the United States (US)2 An updated 2018 survey found that UTI was included as a diagnosis in over 2.8 million discharge summaries and that complicated UTIs (cUTIs) accounted for over 625,000 hospitalizations yearly in the US, comprising 1.8% of all admissions.3
While there are many contributing factors to this increase in hospitalizations, one of the most obvious and alarming is the increase in antibiotic resistance. Antibiotic resistance accounts for nearly 700,000 deaths yearly due to drug-resistant strains in all types of bacterial infection4 and costs the US healthcare system $55 billion in excess each year.5
There are many challenges with both diagnosing and treating UTIs. The lack of consensus definition, the wide variety of causative pathogens and patient populations, and the rise in antimicrobial resistance make treating these infections challenging. Through this review, we hope to better define and understand the unmet needs of complicated UTIs to help mitigate the personal and financial burden of these infections have not only on individual patients but also on the healthcare system.
Defining Complicated UTIs
UTIs were first categorized as uncomplicated and complicated in 1992 by the Infectious Disease Society of America (ISDA) and the European Society of Clinical Microbiology and Infectious Diseases, in an effort to standardize clinical trial participants. Defining cUTIs is crucial, as the categorization of the UTI often determines initial treatment regimen, which must balance patient disease and clinical status with the concern for development of antimicrobial resistance (AMR). For those with uncomplicated UTIs, Escherichia coli (E. coli) is by far the most common pathogen and as such oral treatment with trimethoprim-sulfamethoxazole (TMP-SMX), nitrofurantoin or fosfomycin are first-line therapies.6 In cUTIs, other pathogens are increasingly common, and more broad-spectrum coverage often for longer durations must be considered in treatment.1
This definition of cUTIs, however, is incredibly broad and includes a heterogenous patient population requiring varying degrees of intervention (Table 1). In 2010, the European Association of Urology (EAU) and EAU Section of Infections in Urology (ESIU) proposed an alternative classification system.7 This system classifies UTIs based on the clinical presentation of the UTI, the categorization of host risk factors and availability of appropriate antimicrobial therapy (Figure 1). The aim of this specific classification system is to appropriately prescribe empiric antibiotics, taking into consideration that those patients with cUTIs who may be at higher risk for being infected with highly resistant organisms.
 |
Table 1 Definitions of UTIs Among Various International Societies and Regulatory Agencies |
 |
Figure 1 The European section of infections in urology classification of UTIs. This classification includes the clinical presentation, the severity assessment and any host or pathogen risk factors (RF). This robust definition helps guide empiric antimicrobial treatment and duration. Note: Data from Johansen TEB, Botto H, Cek M, et al. Critical review of current definitions of urinary tract infections and proposal of an EAU/ESIU classification system. Int J Antimicrob Agents. 2011;38:64–70. doi:10.1016/j.ijantimicag.2011.09.009.7 |
Regulatory agencies internationally have similar definitions when providing guidance on drug development for cUTIs. The US Food and Drug Association’s (FDA) definition as stated in a recent guidance on drug development for cUTIs is defined as “a clinical syndrome characterized by pyuria and documented microbial pathogen on culture of urine or blood, accompanied by local systemic signs and symptoms”.8 The FDA acknowledges that there are patient factors that increase the risk of developing cUTIs, including the presence of an indwelling urinary catheter, residual urine volume of greater than 100 milliliters (mL) after voiding (neurogenic bladder), obstructive uropathy, azotemia, or urinary retention. The primary efficacy endpoint in clinical trials as defined by the FDA should include clinical response (resolution of symptoms without development of new symptoms) and/or microbiological response (reduction of bacterial pathogen in culture <103 CFU/mL).
The European Medicines Agency (EMA) defines patients with cUTIs as having at least one complicating factor, such as indwelling urethral catheter, urinary retention, urinary obstruction or neurogenic bladder.9 The EMA also sets a threshold for enrollment of different patients with different types of UTIs, such that patients with acute pyelonephritis and those with cUTIs should comprise at least 30% each of enrolled patients. Primary endpoints, similar to those in the US, include both clinical and microbiological improvement.
Challenges Associated with Diagnosing and Treating cUTIs
Common Pathogens
E. coli is the most common causative pathogen both in uncomplicated and complicated UTIs.10 In order of prevalence after E. Coli, Klebsiella pneumoniae (K. pneumoniae), Staphylococcus saprophyticus, Enterococcus faecalis, group B Streptococcus (GBS), Proteus mirabilis, Pseudomonas aeruginosa (P. aeruginosa), Staphylococcus aureus (S. aureus) and Candida spp. are common causes of uncomplicated UTIs. For complicated UTIs, the order of prevalence for causative agents, following E. Coli, is Enterococcus spp., K. pneumoniae, Candida spp., S. aureus, P. mirabilis, P. aeruginosa and GBS. Another study in hospitalized patients with cUTI found that E. coli, K. pneumoniae, P. aeruginosa, P. mirabilis, Enterococcus spp, and Enterobacter as the most common pathogens, in order of prevalence.11 One of the added challenges, however, is that these patients can also have multiple causative pathogens, making treating these infections increasingly challenging.
Antimicrobial Resistance
In addition to the challenge of defining cUTIs, one of the biggest threats to the management of cUTIs is antimicrobial resistance (AMR). AMR is increasingly common in UTIs, however rates differ based on geographic region.1 A review of worldwide antibiotic resistance found that 10 to 80% of pathogens were resistant to fluoroquinolones, 10 to 70% resistant to third-generation cephalosporins and 5 to 35% to carbapenems. Data shows that antimicrobial resistance is of high concern in gram-negative organisms.12 A multicenter retrospective cohort study in south and eastern Europe found that multidrug resistant (MDR) UTIs were more likely to develop in men, where infections were acquired in a medical care facility, those with an indwelling catheter, those who had a UTI within the last year and those with prior antibiotic treatment within 30 days.13 Resistance rates in those with urosepsis were higher than other clinical diagnoses of healthcare associated UTIs.14 Because resistance rates and patterns vary based on region and treatment population, each facility should develop its own resistance surveillance program to appropriately tailor empiric regimens.
Resistance to pathogens often starts in the community with the treatment of ASB and uUTIs. A recent study of all antibiotic prescriptions in the US found an annual antibiotic prescription rate per 1000 population of 506, but only 353 were appropriate, demonstrating a need for improved stewardship in the outpatient setting.15 A 2021 retrospective observational study analyzed visits from 2015 to 2019 where antibiotics were prescribed for women with uUTIs.16 They found that only 58.4% (26.2 million of 44.9 million visits) were concordant with ISDA guidelines and that fluoroquinolones, which have high resistance rates and are no longer recommended as a first-line therapy, were the most commonly prescribed, though there was decreased use over the four year analysis. In addition, they found that obstetricians and gynecologists and urologists had a statistically significant likelihood of prescribing concordant antibiotics as compared to all other specialties combined.
Clinician behavior also has a significant impact on antibiotic prescription in the outpatient setting. One study found that clinicians are motivated by risk aversion, where the imminent risk of infection outweighs the long-term risk of antibiotic resistance, action bias, where there is a tendency to take action even if not appropriate and patient satisfaction, where physicians feel compelled to prescribe antibiotics by patients.17 Interventions using a multimodal approach, including engaging a quality improvement team, providing education to both prescribers and nurses, measuring performance data and providing feedback and adopting clinical decision tools and protocols, have been shown to decrease the treatment of ASB.18 Another 2008 study found a 21% reduction in treatment of ASB in a geriatric university-affiliated hospital after education session with ward physicians.19
Another challenge is the decline of discovery of new antibiotics and one of the major barriers to development of antibiotics is the lack of investment. A guidance published by the FDA discussed how pharmaceutical companies are not incentivized to create antibiotics as these drugs have relatively low return as compared to other markets, such as oncology.4 As such, there has been relatively little investment into creating novel antibiotics to tackle resistance, with less than 5% of venture capital investment in pharmaceuticals towards antimicrobial development.20
Special Patient Populations
While considering the virulence of the pathogen is important, often it is host factors that determines severity of disease. When diagnosing and treating cUTIs, it is critical to first underly the unique situations that may be present and impacting the clinical scenario.
Catheter-Associated UTIs
One of the most challenging groups of patients to treat for UTIs are those with indwelling catheters. Catheter-associated UTIs (CAUTIs) are the most common nosocomial infections both in the hospital and in long-term health facilities.10 Short-term catheterization increases CAUTI risk by 3–7% with each day of placement and the risk of complications during hospitalization increases up to 80%. For those with long-term catheterization, risk of complication is nearly 100%.21 CAUTIs are associated with increased morbidity and mortality and are the most common cause of secondary bacteremia.10 The urinary catheter bypasses the normal host immune defense along the urethra, giving microorganisms that colonize the groin and perineum direct access to the bladder. In addition, the persistent irritation causes inflammation of the catheter in the bladder and the prevention of normal bladder contraction and micturition, which compounds the susceptibility for infection.21
The challenge with these patients is distinguishing asymptomatic bacteriuria (ASB) to a symptomatic CAUTI. A 2020 study found that biofilms on the catheters were found within several hours of catheterization and biofilms progressed as a function of indwelling time.22 ISDA guidelines define CAUTI as “the presence of symptoms or signs compatible with UTI with no other identified source of infection along with ≥103 CFU/mL of ≥1 bacterial species in a single catheter urine specimen or in a midstream voided urine specimen from a patient whose urethral, suprapubic or condom catheter has been removed within the previous 48 hours”.23 Signs and symptoms of infection include new onset fevers, rigors, altered mental status, malaise, lethargy, costovertebral angle (CVA) tenderness, acute hematuria, and/or suprapubic or pelvic pain or discomfort. In addition, the ISDA states that the “presence, absence or degree of pyuria should not be used to differentiate between ASB from CAUTI.”23 The Loeb criteria were created in 2001 to minimize overtreatment of ASB in long-term facilities.24 These criteria recommend initiating treatment if at least one of the following are present: fever, new CVA tenderness, new onset of delirium or rigors. Although these criteria were published over 20 years ago, overtreatment of ASB continues to be a challenge.
Multiple studies have employed education programs to both nurses and physicians on the appropriateness of treating ASB in these patients. One study tested 169 medical residents and staff providers on the guidelines for treatment of ASB in patients with catheter, with an average knowledge score of 57.5%.25 Another study from a long-term care facility of the Cleveland Department of Veterans Affairs educated nurses to discourage the collection of urine cultures in the absence of symptoms.26 They found a sustained reduction in overall diagnoses and a reduction in total antimicrobial days of therapy that was maintained for 30-months after the education session. Interestingly, this study illustrated that many of the ordering physicians were unaware of the ISDA guidelines for treatment of CAUTIs.
These patients specifically have high rates of colonization and of symptomatic infections with multidrug resistant (MDR) pathogens. Patients with catheters are often elderly, reside in a long-term care facility and have been widely exposed to multiple antibiotics.12 This ultimately increases the risk of formation of biofilms with MDR pathogens. Although there have been many attempts to minimize the formation of these biofilms, including hydrophilic catheters, antibiotic-coated catheters and catheter irrigations, there has been mixed efficacy and the ISDA does not recommend their use.23 In the event of a CAUTI, it is important to exchange the catheter quickly, as continuing treatment with the same catheter in place increases the risk of MDR colonization.27 Recommendations remain to reduce the duration of catheterization with close attention to aseptic technique and good hand hygiene are critical to minimizing CAUTIs.28
Ureteral Dysfunction
Impaired ureteral function as seen in those patients with high intravesical pressure or vesicoureteral function predispose patients to upper UTIs. This is commonly seen in children with reflux and puts these patients at a high risk for renal scarring and recurrent UTIs. Antimicrobial prophylaxis has been found to reduce the risk of recurrent infection, but has not consistently been shown to reduce the risk of renal scarring.29 Renal scarring in and of itself may put patients at additional risk for developing UTIs and thus mitigating the development of scarring is crucial to prevent future infections.
Impaired Host Response
One of the most challenging populations with cUTIs to manage are those who have impaired immune responses, including those with diabetes mellitus (DM), end-stage renal disease (ESRD), and solid organ transplantation, especially kidney transplant patients.30 DM has an independent risk factor for UTIs in women.31 There are no additional challenges in diagnosing patients with DM with UTIs, however clinicians should be vigilant about their timely diagnosis, as these patients rapidly progress to more severe illness as compared to the general population. In patients with diabetes, age above 60 years, chronic use of antibiotics, more than 6 physician contacts in the previous year, hospitalization in the previous year, and urinary incontinence were independently associated with severe UTIs.32 Another study found that the higher morbidity associated with patients with DM and cUTIs were explained by the increased prevalence of cardiovascular morbidity and higher age.33 In these patients, selection of empiric antibiotics and duration of treatment is the same as the general population. Of note, patients who are taking sodium/glucose co-transporter 2 (SGLT2) inhibitors for DM are at an increased risk of urinary tract infections as well as mycotic genital infections, likely due to increased glucose in the urine.34
Chronic kidney disease (CKD) has also been shown to place patients at higher risk for developing UTIs, likely due to the loss of antimicrobial properties in the urine, mild immunosuppression in anemia, and the inhibition of protective mucosal production in the urothelium.30 This is most strongly correlated in patients with autosomal dominant polycystic kidney disease (ADPKD), where 21–75% of patients develop a UTI over their lifetime. These patients may develop pyonephrosis and pyocysts, where the cysts become infected, as this may exist without growth of urine cultures. In these specific patients, fluoroquinolones or TMP-SMX are recommended as they have better penetration for the cysts than standard antibiotics, such as beta-lactams and aminoglycosides. In addition, a population-based cohort study of nearly 80,000 patients with DM and CKD found that having higher frailty scores put patients at a higher risk of developing UTI, and that more severe frailty exhibited a trend of having higher rates of sepsis.35
Infections in kidney transplant recipients are associated with higher morbidity and mortality. There has been a significant reduction in mortality associated with UTI after kidney transplantation, now less than 5%.30 UTIs, however, still account for about 40–50% of all infectious complications in these patients.36 There has been mixed data on if age is independently associated with UTIs in this patient population, however the association of other comorbidities as patients age is likely thought to contribute to these infections. In addition, the type of immunosuppression has been shown to increase risk of UTIs. Azathioprine, mycophenolate mofetil, and anti-thymocyte globulin are all associated with higher rate of UTI, whereas other drugs such as calcineurin inhibitors and everolimus are not.37 Many authors believe that infections are more likely to occur in the early post-transplant period, with reported rates of infection <30% in the first 3 months.38,39
Although now less fatal, acute pyelonephritis has been shown to be a risk factor for decline of renal function in renal transplant recipients,40 thus rapid diagnosis and treatment is key to preserving graft function. In order to prevent this decline in graft function, many transplant centers screen for ASB and use antimicrobial prophylaxis in the first 6 months of transplant.41 This long-term prophylaxis has been shown to reduce the risk of sepsis and bacteremia with TMP-SMX use, however there is no consensus on the regimen.42,87,88 In an already vulnerable population, this prophylaxis can lead to antimicrobial resistance. Nearly 10% of patients are thought to be colonized pre-transplant with methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococcus (VRE),43 and this poses a challenge for treatment if patients then become septic in the intensive care unit post-transplant.
Pregnancy is one of the few clinical situations where ASB is treated, as untreated infections are associated with low birthweight and preterm delivery.44 Antibiotic exposure in pregnancy can lead to both short and long-term complications, including congenital abnormalities, changes in gut microbiome and asthma, however only 10% of antibiotics have adequate data related to pregnancy.45 Beta-lactams, vancomycin, nitrofurantoin, metronidazole and fosfomycin are generally considered safe, whereas fluoroquinolones and tetracyclines should be avoided.
Emerging Treatments
Fosfomycin
Although fosfomycin is indicated as a first-line therapy for treatment of uUTIs,6 fosfomycin is not widely used for the treatment of cUTIs. Fosfomycin has extremely broad coverage against most uropathogens and is also active against extended-spectrum beta-lactamase (ESBL)/carbapenemase-producing enterobacteria, and bacteria resistant to quinolones.46 Multiple studies have shown high rates of clinical cure for oral fosfomycin in patient with cUTIs47 and MDR cUTIs.48,49 There have also been promising studies comparing intravenous fosfomycin to piperacillin-tazobactam (PTZ) for acute pyelonephritis.50 One limiting factor of fosfomycin use is the United States is cost, where fosfomycin has been documented as $67.49 per dose as compared to $0.52 per dose for nitrofurantoin and $0.06 per dose of TMP-SMX.51 A recent cost analysis, however, shows that if taking into account local resistance, need for multiple courses of antibiotics and risk of progression to more serious effective, fosfomycin could be considered a cost-effective alternative to other treatments.52 In Europe, fosfomycin is still more expensive than other first-line treatments, however this difference is much less pronounced and a cost-analysis found that when accounting for resistance rates, fosfomycin is the most cost-effective antibiotic.53 As more manufacturers continue to make generic versions of fosfomycin, the cost will continue to decrease, making fosfomycin an increasingly viable alternative to current antibiotic regimens.
Intravesical Instillations
In a recent systematic review, aminoglycosides alone and aminoglycoside/polymyxin intravesical instillation has been shown to reduction of UTI and/or reduce the sensitivity of oral antibiotic therapy.54 Many of the patients included in the reviewed studies were administering the instillation themselves, further reducing the need for hospitalization for treatment administration. Although the data provided is limited in long-term follow-up, there were no systemic side effects seen in intravesical instillation, such as ototoxicity and nephrotoxicity, that are usually seen with high-dose IV administration. Another systematic review included studies with gentamicin, neomycin/polymyxin, neomycin and colistin with similar results.55 A 2017 retrospective study examined 22 patients with neurogenic bladder who performed clean intermittent catheterization who underwent prophylactic intravesical gentamicin irrigation.56 These patients had fewer symptomatic UTIs and underwent fewer courses of oral antibiotics. In addition, the proportion of MDR organisms in urine cultures decreased and the rate of gentamicin resistance did not increase, with rare and mild adverse effects. Most studies, however, were only performed in a small cohort of patients and large-scale randomized controlled trials are still needed.57
Non-antibiotic instillations have also shown to be effective in preventing recurrent UTIs. A recent retrospective cohort study including 7 European institutions found that patients with recurrent UTIs who received 50mL hyaluronic acid and 2% chondroitin sulfate instillations had a decrease in the number of UTIs at 12 months and an increase in time between UTIs.58 These non-antibiotic instillations are thought to restore the glycosaminoglycan layer in the bladder, which is a key component of host defense. Although data is limited, both antibiotic and non-antibiotic intravesical instillations show promise in mitigating the impact of recurrent UTIs both on patients and on antibiotic resistance.
Clinical Trials for cUTIs
When treating cUTIs and pyelonephritis, source control and appropriate selection of antibiotics are key for treatment.59 Generally, gram-negative pathogens are susceptible to new antimicrobials but there is limited treatment options for resistant enterococci.1 Many new antibiotics are tested in patients with cUTI and acute pyelonephritis due to the high incidence and easy recruitment of participants. Because of the lack of consensus definition cUTI, there is variability in the inclusion criteria for the studies included in this review.60 In addition, systemic symptoms, inflammatory markers such as C-reactive protein or procalcitonin, as well as detailed culture data make testing new antibiotics in cUTIs an ideal disease group. There have been many Phase 2 and 3 clinical trials for new antibiotics in the last few decades due to antibiotic resistance, but for the purposes of the review, we will focus on significant clinical trials from the last 5 years (Table 2). Much of the research is examining the effectiveness of new antibiotics against otherwise resistant pathogens, with great promise shown for those antibiotics that treat carbapenem-resistant infections.
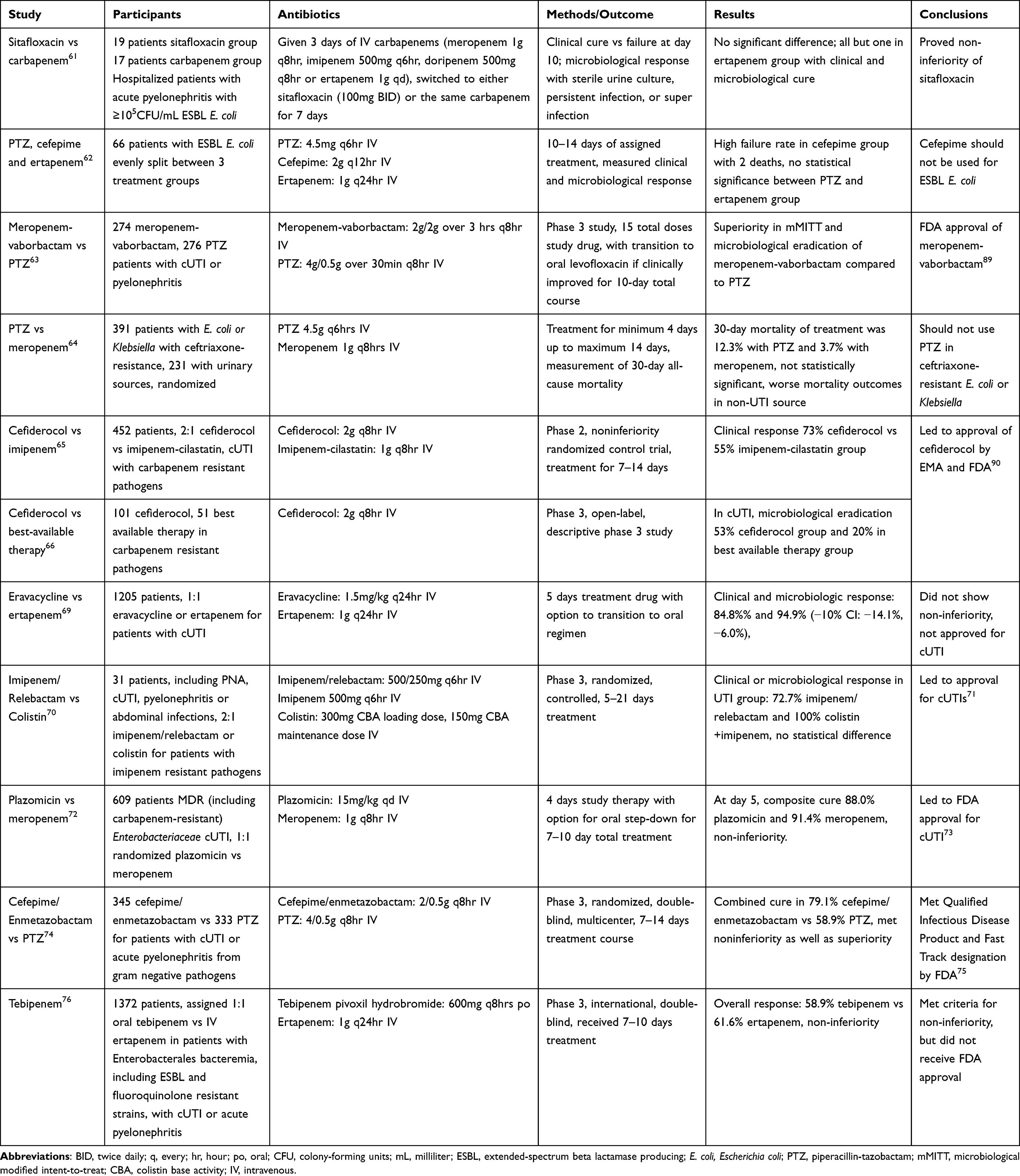 |
Table 2 Summary of Recent Clinical Trials for Antibiotics Treating Multidrug Resistant Organisms. Dosages Documented are for Those with Normal Renal Function and All Studies Adjusted Doses for Creatinine Clearance |
Sitafloxacin versus Ertapenem
In 2017, a pilot study compared the use of oral sitafloxacin to ertapenem in patients with ESBL E. coli with non-bacteremic acute pyelonephritis.61 Nineteen patients were enrolled in the sitafloxacin group with 17 in the ertapenem group. All patients were given 3 days of intravenous carbapenem and then switched for 7 days to either oral sitafloxacin or intravenous ertapenem. Baseline characteristics were similar between the two groups, except there was a lower proportion of previous urinary catheter insertion in the sitafloxacin group. At day 10, all but one patient in the ertapenem group had clinical cure and microbiological eradication was comparable between both groups, without significant side effects.
PTZ, Cefepime and Ertapenem
Seo et al conducted a prospective, randomized open-label study comparison of the therapeutic efficacy of PTZ, cefepime and ertapenem in patients with febrile nosocomial UTI with ESBL E. coli.62 A total of 66 participants were evenly assigned to the PTZ and ertapenem group. Enrollment into the cefepime group was stopped after recruitment of 6 participants due to high failure rate, including 2 deaths. The clinical and microbiological response was 93.9% with PTZ and 97.0% with ertapenem, but the rates were not statistically different. Based on this study, patients with cUTI with ESBL-producing pathogens should not be treated with cefepime.
TANGO I: Meropenem-Vaborbactam versus PTZ
Kaye et al conducted a Phase 3 multicenter, multinational randomized clinical trial for patients with cUTI or acute pyelonephritis with 274 patients receiving meropenem-vaborbactam and 276 receiving PTZ.63 After 15 total doses, patients could be transitioned to oral levofloxacin if met criteria for clinical improvement for 10 day total course. Primary endpoint for FDA criteria was overall success (clinical cure or improvement and microbial eradication composite) at end of intravenous treatment in the modified intent-to-treat (mITT) population. Primary endpoint for the EMA criteria was microbial eradication at test-of-cure (TOC) visit in the mITT and microbiologic evaluable populations. Superiority of meropenem-vaborbactam over PTZ was concluded for the overall success rate, at the lower limit of the 95% confidence interval.
PTZ versus Meropenem
This noninferiority randomized clinical trial in 391 patients with E. coli or Klebsiella pneumoniae bloodstream infection and ceftriaxone resistance sought to determine if PTZ could be used as a carbapenem-sparing therapy.64 Of these patients, 231 had infections from urinary tract source. Thirty-day mortality rate of patients treated with PTZ compared with meropenem was 12.3% and 3.7%, respectively, which did not meet the noninferiority margin and does not support the use of PTZ in these patients. Of note, mortality was higher in those with non-UTI infection source (12.8% vs 4.8%), however this was not statistically significant on multivariate analysis.
Cefiderocol
In this phase 2 multicenter, double-blind, parallel-group, noninferiority trial, 452 patients with cUTI with or without pyelonephritis were randomly assigned 2:1 to receive infusions of cefiderocol or imipenem-cilastatin.65 The primary endpoint was a composite of clinical response and microbiological response at TOC for the mITT population. At TOC, clinical response was achieved by 73% of the cefiderocol group and 55% of patients in the imipenem-cilastatin group (p = 0.0004), establishing non-inferiority. Observed treatment differences were high for cefiderocol group, especially in those infected with resistant pathogens, thus clinical benefit for cefiderocol may be present.
A phase 3 open-label study was also conducted with patients admitted to the hospital with evidence of nosocomial pneumonia, blood stream infections, sepsis or cUTI and carbapenem-resistant gram-negative pathogen.66 Participants were assigned 2:1 to either cefiderocol or best available therapy for 7–14 day treatment course. In patients with complicated UTI, primary endpoint was microbiological cure in mITT population, which was achieved in 53% of the cefiderocol group and 20% in best available therapy group, which proved similar clinical and microbiological efficacy. Both these trials led to the FDA and EMA approval of cefiderocol.67
IGNITE3: Eravacycline vs Ertapenem
Eravacycline is a tetracycline that has been approved for use in complicated intra-abdominal infections.68 In a study of the use of eravacycline in cUTIs, Tetraphase Pharmaceuticals enrolled 1205 patients randomized 1:1 to receive either eravacycline or ertapenem for 5 days and then were eligible for transition to an oral agent.69 Primary endpoints included both clinical and microbiological response. Responder rates in the mITT group were 84.8% and 94.8% for eravacycline and ertapenem, respectively (−10% CI: −14.1%, −6.0%), which did not show non-inferiority. Thus, eravacycline has not been approved for the use of cUTIs in the US.
RESTORE-IMI 1: Imipenem/Relebactam vs Colistin Plus Imipenem
Relebactam is a beta-lactamase inhibitor that can restore imipenem activity against imipenem non-susceptible pathogens.70 In their phase 3 randomized, controlled, double-blind trial, hospitalized patients with hospital acquired or ventilator-associated pneumonia, complicated intraabdominal infection or cUTI caused by imipenem non-susceptible (but colistin and imipenem/relebactam susceptible) were randomized 2:1 to 5–21 days imipenem/relebactam or colistin+imipenem.70 Sixteen patients had cUTI or pyelonephritis. Primary endpoint for patients with cUTI or pyelonephritis was a composite clinical and microbiological response at early follow-up, 5–9 days following end of therapy in mITT population. Overall response in the UTI group was observed in 72.7% imipenem/relebactam and 100% colistin+imipenem patients, with no statistical difference in overall response, day 28 favorable clinical response, 28-day mortality, or serious adverse events. This led to FDA approval for the treatment for cUTIs.71
Plazomicin vs Meropenem
In a multicenter, multinational, randomized, double-blind phase 3 trial, once-daily plazomicin was tested against meropenem for the treatment of cUTIs.72 Plazomicin is an aminoglycoside with bactericidal activity against MDR (including carbapenem-resistant) Enterobacteriaceae. This noninferiority study randomly assigned 609 patients with cUTIs, including pyelonephritis, in a 1:1 ratio to receive plazomicin or meropenem with option for oral step-down therapy after receiving at least 4 days of study therapy for a total of 7 to 10 days of therapy. The primary endpoints were composite cure at day 5 and at the test-of-cure visit (15 to 19 days after initiation of therapy) in the mMITT population. At day 5, composite cure was 88.0% for plazomicin and 91.4% for meropenem, confirming noninferiority of plazomicin (95% CI −10.0 to 3.1). Superiority of plazomicin was exhibited at TOC visit, with composite cure of 81.7% for plazomicin and 70.1% meropenem (95% CI 2.7 to 20.3). This ultimately led to the approval of plazomicin for treatment of cUTI.73
Cefepime/Enmetazobactam vs PTZ
In a phase 3, randomized, double-blind, active-controlled, multicenter, noninferiority clinical trial, Kaye et al compared the efficacy of cefepime/enmetazobactam vs PTZ in patients with cUTI.74 The primary outcome was combined clinical cure and microbiological eradication. After randomization, 79.1% (273/345) patients receiving cefepime/enmetazobactam achieved combined cure as compared to 58.9% (196/333) receiving PTZ (between-group difference 21.2% [95% CI, 14.3% to 27.9%]). This met criteria for noninferiority as well as superiority for the primary outcome, which met criteria for Qualified Infectious Disease Product and Fast-Track Designation by the FDA.75
Tebipenem
Tebipenem pivoxil hydrobromide, an orally bioavailable carbapenem with activity against MDR Enterobacterales, was compared to intravenous ertapenem in a phase 3, international, double-blind, double-dummy trial.76 A total of 1372 hospitalized patients were enrolled, in which 868 were included in the microbiologic intention-to-treat population. An overall response was seen in 58.9% of patients who received tebipenem pivoxil hydrobromide as compared with 61.6% who received ertapenem (95% CI −9.7 to 3.2). Clinical cure at TOC visit was observed in 93.1% of patients who received tebipenem pivoxil hydrobromide and 93.6% of patients who received ertapenem (CI −4.0 to 2.8). Although tebipenem pivoxil hydrobromide was noninferior to intravenous ertapenem, it did not meet the FDA criteria for noninferiority margin of −12.5%, and further studies are needed prior to approval.77
Recommendations
Global participation in both an antibiotic stewardship program and regulatory frameworks are necessary to mitigate the impact of antimicrobial resistance and promote the discovery of new drugs. In 2013, Rex et al proposed a regulatory framework with tiered approach based on the clinical need and data available.78 The European Union (EU) launched New Drugs for Bad Bugs (ND4BB), a € 650 million program partnering industry, academia and biotech organizations to combat antimicrobial resistance in Europe.79 The US also incentivized pharmaceutical companies to prioritize antibiotics by passing the Generating Antibiotic Incentives Now (GAIN) Act of 2011, which extended the exclusivity period for new infectious disease drug products by 5 years.80 In 2016, the FDA announced the Limited Population Pathway for Antibacterial and Antifungal Drugs, which facilitated the approval of antimicrobial and antifungal drugs to treat serious and life-threatening infections in a limited population of patient with unmet needs.81 In addition, the Joint Commission released a new and revised antibiotic stewardship program which outlined the current expectations for antibiotic stewardship nationwide.67
Improvements in diagnosing infections can also help meet the unmet needs for treating cUTIs. More rapid diagnostics can not only help provide more accurate care to patients in addition to reducing the risk of antibiotic resistance.4 For example, a recent study found that in a model of point-of-care testing for Neisseria gonorrhea for strains that are not resistant to previous first-line therapies could reduce the total treatment time and reduce cost by using older more cost-effective antibiotics.82 In addition, using older antibiotics could reduce resistance to newer, more expensive antibiotics and allow those to remain viable treatment options in the future. While urine culture remains the gold standard for diagnosing a UTI, PCR has been shown to be non-inferior to urine culture in patients with acute cystitis.83 In their study, Wojno et al found that PCR exhibited greater accuracy than culture for pathogen detection and identification of bacteria in 36% with negative traditional culture. In addition, they found that PCR was much more sensitive in detecting polymicrobial infections than urine culture. To counter, however, PCR may be detecting bacteria that are not clinically significant, which may lead to increased use of antibiotics when not clinically indicated.
While bedside diagnostics are still in development, there have been validated tools to predict antibiotic resistance. Zilberberg et al developed a model assigning weighted points for the following characteristics: admission from an extended care facility (1), history of weight loss (1), early mechanical ventilation (1), age <50 years (2), male gender (3), catheter-associated UTI (4) or prior antibiotic treatment (4), and prior carbapenem-resistant infection (8). This tool had a high negative-predictive value. In patients who scored below 3, which accounted for approximately 30% of the cohort, there was a ~1% risk of cUTI caused by carbapenem-resistant organism. In addition, individualized multivariate predictive models used in combination with existing resistance-prediction models can predict the probability of susceptibility gram-negative bacteremia with the commonly prescribed antibiotics.84 Patients who underwent intervention by applying these models to their care were more likely to have their therapy de-escalated. This study also found there was an increased proportion of patients who were on the narrowest adequate therapy at time of culture finalization. These tools can continue to be implemented until more rapid diagnostics are developed.
Conclusion
Complicated UTIs are an enormous burden on not only patients but also on the healthcare system. The lack of consensus definition has driven variability both in treatment options and in clinical trials. Special populations, especially those with catheters in place and those who have impaired immune response mechanisms make treating and diagnosing cUTIs a continued challenge. Antimicrobial resistance, especially in the context of treating cUTIs, continues to be one of the largest threats to our healthcare system globally. Regulatory frameworks in place have helped new drugs enter the pipeline for the treatment of resistant bacteria. Antibiotic stewardship programs will need to be prioritized moving forward to mitigate resistance in the future.
Abbreviations
UTI, urinary tract infection; uUTI, uncomplicated UTI; US, United States; cUTI, complicated UTI; ISDA, Infectious Disease Society of America; E. coli, Escherichia coli; TMP-SMX, trimethoprim-sulfamethoxazole; EAU, European Association of Urology; ESIU, European Association of Urology Section of Infections in Urology; FDA, Food and Drug Association; mL, milliliters; CFU, colony forming units; EMA, European Medicines Agency; AUA, American Urological Association; AMR, antimicrobial resistance; CAUTI, catheter-associated urinary tract infection; ASB, asymptomatic bacteriuria; CVA, costovertebral angle; MDR, multi-drug resistant; DM, diabetes mellitus; ESRD, end-stage renal disease; SGLT2, sodium/glucose co-transporter 2; CKD, chronic kidney disease; ADPKD, autosomal polycystic kidney disease; MRSA, methicillin-resistant Staphylococcus aureus; VRE, vancomycin-resistant Enterococcus; PTZ, piperacillin-tazobactam; PCR, polymerase chain reaction; mITT, modified intent-to-treat; TOC, test of cure.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wagenlehner FME, Bjerklund Johansen TE, Cai T, et al. Epidemiology, definition and treatment of complicated urinary tract infections. Nat Rev Urol. 2020;17(10):586–600. doi:10.1038/s41585-020-0362-4
2. Simmering JE, Tang F, Cavanaugh JE, Polgreen LA, Polgreen PM. The increase in hospitalizations for urinary tract infections and the associated costs in the United States, 1998–2011. Open Forum Infect Dis. 2017;4(1):ofw281. doi:10.1093/ofid/ofw281
3. Zilberberg MD, Nathanson BH, Sulham K, Shorr AF. Descriptive epidemiology and outcomes of hospitalizations with complicated urinary tract infections in the United States, 2018. Open Forum Infect Dis. 2022;9(1):ofab591. doi:10.1093/ofid/ofab591
4. Tackling drug-resistant infections globally: final report and recommendations / the review on antimicrobial resistance chaired by Jim O’Neill. Wellcome Collection. Available from: https://wellcomecollection.org/works/thvwsuba.
5. Smith R, Coast J. The true cost of antimicrobial resistance. BMJ. 2013;346:f1493. doi:10.1136/bmj.f1493
6. Anger J, Lee U, Ackerman AL, et al. Recurrent uncomplicated urinary tract infections in women: AUA/CUA/SUFU guideline. J Urol. 2019;202(2):282–289. doi:10.1097/JU.0000000000000296
7. Johansen TEB, Botto H, Cek M, et al. Critical review of current definitions of urinary tract infections and proposal of an EAU/ESIU classification system. Int J Antimicrob Agents. 2011;38:64–70. doi:10.1016/j.ijantimicag.2011.09.009
8. US Food and Drug Administration. Complicated urinary tract infections: developing drugs for treatment; 2020. Available from: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/complicated-urinary-tract-infections-developing-drugs-treatment.
9. EMA. Evaluation of medicinal products indicated for treatment bacterial infections - scientific guideline. European Medicines Agency; 2018. Available from: https://www.ema.europa.eu/en/evaluation-medicinal-products-indicated-treatment-bacterial-infections-scientific-guideline.
10. Flores-Mireles AL, Walker JN, Caparon M, Hultgren SJ. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nat Rev Microbiol. 2015;13(5):269–284. doi:10.1038/nrmicro3432
11. Zilberberg MD, Nathanson BH, Sulham K, Fan W, Shorr AF. Development and validation of a bedside instrument to predict carbapenem resistance among gram-negative pathogens in complicated urinary tract infections. Infect Control Hosp Epidemiol. 2018;39(9):1112–1114. doi:10.1017/ice.2018.166
12. Zowawi HM, Harris PNA, Roberts MJ, et al. The emerging threat of multidrug-resistant gram-negative bacteria in urology. Nat Rev Urol. 2015;12(10):570–584. doi:10.1038/nrurol.2015.199
13. Gomila A, Shaw E, Carratalà J, et al. Predictive factors for multidrug-resistant gram-negative bacteria among hospitalised patients with complicated urinary tract infections. Antimicrob Resist Infect Control. 2018;7(1):111. doi:10.1186/s13756-018-0401-6
14. Tandoğdu Z, Bartoletti R, Cai T, et al. Antimicrobial resistance in urosepsis: outcomes from the multinational, multicenter global prevalence of infections in urology (GPIU) study 2003–2013. World J Urol. 2016;34(8):1193–1200. doi:10.1007/s00345-015-1722-1
15. Fleming-Dutra KE, Hersh AL, Shapiro DJ, et al. Prevalence of inappropriate antibiotic prescriptions among US ambulatory care visits, 2010–2011. JAMA. 2016;315(17):1864–1873. doi:10.1001/jama.2016.4151
16. Langner JL, Chiang KF, Stafford RS. Current prescribing practices and guideline concordance for the treatment of uncomplicated urinary tract infections in women. Am J Obstet Gynecol. 2021;225(3):272.e1–272.e11. doi:10.1016/j.ajog.2021.04.218
17. Mohareb AM, Letourneau AR, Sánchez SM, Walensky RP, Hyle EP. Addressing antibiotic overuse in the outpatient setting: lessons from behavioral economics. Mayo Clin Proc. 2021;96(3):537–542. doi:10.1016/j.mayocp.2020.10.033
18. Daniel M, Keller S, Mozafarihashjin M, Pahwa A, Soong C. An implementation guide to reducing overtreatment of asymptomatic bacteriuria. JAMA Intern Med. 2018;178(2):271–276. doi:10.1001/jamainternmed.2017.7290
19. Bonnal C, Baune B, Mion M, et al. Bacteriuria in a geriatric hospital: impact of an antibiotic improvement program. J Am Med Dir Assoc. 2008;9(8):605–609. doi:10.1016/j.jamda.2008.04.004
20. Renwick MJ, Simpkin V, Mossialos E. Targeting innovation in antibiotic drug discovery and development: the need for a one health – one Europe – one world framework. European Observatory on Health Systems and Policies; 2016. Available from: http://www.ncbi.nlm.nih.gov/books/NBK447337/.
21. Flores-Mireles A, Hreha TN, Hunstad DA. Pathophysiology, treatment, and prevention of catheter-associated urinary tract infection. Top Spinal Cord Inj Rehabil. 2019;25(3):228–240. doi:10.1310/sci2503-228
22. Werneburg GT, Nguyen A, Henderson NS, et al. The natural history and composition of urinary catheter biofilms: early uropathogen colonization with intraluminal and distal predominance. J Urol. 2020;203(2):357–364. doi:10.1097/JU.0000000000000492
23. Hooton TM, Bradley SF, Cardenas DD, et al. Diagnosis, prevention, and treatment of catheter-associated urinary tract infection in adults: 2009 international clinical practice guidelines from the infectious diseases society of America. Clin Infect Dis. 2010;50(5):625–663. doi:10.1086/650482
24. Loeb M, Bentley DW, Bradley S, et al. Development of minimum criteria for the initiation of antibiotics in residents of long-term–care facilities: results of a consensus conference. Infect Control Hosp Epidemiol. 2001;22(2):120–124. doi:10.1086/501875
25. Trautner BW, Petersen NJ, Hysong SJ, Horwitz D, Kelly PA, Naik AD. Overtreatment of asymptomatic bacteriuria: identifying provider barriers to evidence-based care. Am J Infect Control. 2014;42(6):653–658. doi:10.1016/j.ajic.2014.02.003
26. Zabarsky TF, Sethi AK, Donskey CJ. Sustained reduction in inappropriate treatment of asymptomatic bacteriuria in a long-term care facility through an educational intervention. Am J Infect Control. 2008;36(7):476–480. doi:10.1016/j.ajic.2007.11.007
27. Morton SC, Shekelle PG, Adams JL, et al. Antimicrobial prophylaxis for urinary tract infection in persons with spinal cord dysfunction. Arch Phys Med Rehabil. 2002;83(1):129–138. doi:10.1053/apmr.2002.26605
28. Lo E, Nicolle LE, Coffin SE, et al. Strategies to prevent catheter-associated urinary tract infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35(5):464–479. doi:10.1086/675718
29. Hoberman A, Greenfield SP, et al; RIVUR Trial Investigators. Antimicrobial prophylaxis for children with vesicoureteral reflux. N Engl J Med. 2014;370(25):2367–2376. doi:10.1056/NEJMoa1401811
30. Tandogdu Z, Cai T, Koves B, Wagenlehner F, Bjerklund-Johansen TE. Urinary tract infections in immunocompromised patients with diabetes, chronic kidney disease, and kidney transplant. Eur Urol Focus. 2016;2(4):394–399. doi:10.1016/j.euf.2016.08.006
31. Geerlings SE, Meiland R, Hoepelman AIM. Pathogenesis of bacteriuria in women with diabetes mellitus. Int J Antimicrob Agents. 2002;19(6):539–545. doi:10.1016/s0924-8579(02)00090-0
32. Venmans LMAJ, Sloof M, Hak E, Gorter KJ, Rutten GEHM. Prediction of complicated urinary tract infections in patients with type 2 diabetes: a questionnaire study in primary care. Eur J Epidemiol. 2007;22(1):49. doi:10.1007/s10654-006-9077-y
33. van der Starre WE, Borgdorff H, Vollaard AM, et al. Diabetes and the course of febrile urinary tract infection. Diabetes Care. 2013;36(12):e193–e194. doi:10.2337/dc13-0903
34. Singh M, Sharma R, Kumar A. Safety of SGLT2 inhibitors in patients with diabetes mellitus. Curr Drug Saf. 2019;14(2):87–93. doi:10.2174/1574886314666190206164647
35. Chao CT, Lee SY, Wang J, Chien KL, Huang JW. Frailty increases the risk for developing urinary tract infection among 79,887 patients with diabetic mellitus and chronic kidney disease. BMC Geriatr. 2021;21(1):349. doi:10.1186/s12877-021-02299-3
36. Säemann M, Hörl WH. Urinary tract infection in renal transplant recipients. Eur J Clin Invest. 2008;38(Suppl 2):58–65. doi:10.1111/j.1365-2362.2008.02014.x
37. Fiorentino M, Pesce F, Schena A, Simone S, Castellano G, Gesualdo L. Updates on urinary tract infections in kidney transplantation. J Nephrol. 2019;32(5):751–761. doi:10.1007/s40620-019-00585-3
38. Senger SS, Arslan H, Azap OK, Timurkaynak F, Cağir U, Haberal M. Urinary tract infections in renal transplant recipients. Transplant Proc. 2007;39(4):1016–1017. doi:10.1016/j.transproceed.2007.02.060
39. Abbott KC, Swanson SJ, Richter ER, et al. Late urinary tract infection after renal transplantation in the United States. Am J Kidney Dis. 2004;44(2):353–362. doi:10.1053/j.ajkd.2004.04.040
40. Pellé G, Vimont S, Levy PP, et al. Acute pyelonephritis represents a risk factor impairing long-term kidney graft function. Am J Transplant. 2007;7(4):899–907. doi:10.1111/j.1600-6143.2006.01700.x
41. El Amari EB, Hadaya K, Bühler L, et al. Outcome of treated and untreated asymptomatic bacteriuria in renal transplant recipients. Nephrol Dial Transplant. 2011;26(12):4109–4114. doi:10.1093/ndt/gfr198
42. Green H, Rahamimov R, Gafter U, Leibovitci L, Paul M. Antibiotic prophylaxis for urinary tract infections in renal transplant recipients: a systematic review and meta-analysis. Transpl Infect Dis. 2011;13(5):441–447. doi:10.1111/j.1399-3062.2011.00644.x
43. Ziakas PD, Pliakos EE, Zervou FN, Knoll BM, Rice LB, Mylonakis E. MRSA and VRE colonization in solid organ transplantation: a meta-analysis of published studies. Am J Transplant. 2014;14(8):1887–1894. doi:10.1111/ajt.12784
44. Köves B, Cai T, Veeratterapillay R, et al. Benefits and harms of treatment of asymptomatic bacteriuria: a systematic review and meta-analysis by the European Association of urology urological infection guidelines panel. Eur Urol. 2017;72(6):865–868. doi:10.1016/j.eururo.2017.07.014
45. Bookstaver PB, Bland CM, Griffin B, Stover KR, Eiland LS, McLaughlin M. A review of antibiotic use in pregnancy. Pharmacotherapy. 2015;35(11):1052–1062. doi:10.1002/phar.1649
46. López-Montesinos I, Horcajada JP. Oral and intravenous fosfomycin in complicated urinary tract infections. Rev Esp Quimioter. 2019;32(Suppl 1):37–44.
47. Qiao LD, Zheng B, Chen S, et al. Evaluation of three-dose fosfomycin tromethamine in the treatment of patients with urinary tract infections: an uncontrolled, open-label, multicentre study. BMJ Open. 2013;3(12):e004157. doi:10.1136/bmjopen-2013-004157
48. Senol S, Tasbakan M, Pullukcu H, et al. Carbapenem versus fosfomycin tromethanol in the treatment of extended-spectrum beta-lactamase-producing Escherichia coli-related complicated lower urinary tract infection. J Chemother. 2010;22(5):355–357. doi:10.1179/joc.2010.22.5.355
49. Pullukcu H, Tasbakan M, Sipahi OR, Yamazhan T, Aydemir S, Ulusoy S. Fosfomycin in the treatment of extended spectrum beta-lactamase-producing Escherichia coli-related lower urinary tract infections. Int J Antimicrob Agents. 2007;29(1):62–65. doi:10.1016/j.ijantimicag.2006.08.039
50. Kaye KS, Rice LB, Dane AL, et al. Fosfomycin for injection (ZTI-01) versus piperacillin-tazobactam for the treatment of complicated urinary tract infection including acute pyelonephritis: ZEUS, a phase 2/3 randomized trial. Clin Infect Dis. 2019;69(12):2045–2056. doi:10.1093/cid/ciz181
51. NADAC (National Average Drug Acquisition Cost); 2022. Available from: https://data.medicaid.gov/dataset/dfa2ab14-06c2-457a-9e36-5cb6d80f8d93.
52. Kassabian M, Calderwood MS, Ohsfeldt R. A cost-effectiveness analysis of fosfomycin: a single-dose antibiotic therapy for treatment of uncomplicated urinary tract infection. Health Serv Insights. 2022;15:11786329221126340. doi:10.1177/11786329221126340
53. Sadler S, Holmes M, Ren S, Holden S, Jha S, Thokala P. Cost-effectiveness of antibiotic treatment of uncomplicated urinary tract infection in women: a comparison of four antibiotics. BJGP Open. 2017;1(3). doi:10.3399/bjgpopen17X101097
54. Ong A, Pietropaolo A, Brown G, Somani BK. Are intravesical aminoglycosides the new gold standard in the management of refractory urinary tract infection: a systematic review of literature. J Clin Med. 2022;11(19):5703. doi:10.3390/jcm11195703
55. Pietropaolo A, Jones P, Moors M, Birch B, Somani BK. Use and effectiveness of antimicrobial intravesical treatment for prophylaxis and treatment of recurrent Urinary Tract Infections (UTIs): a systematic review. Curr Urol Rep. 2018;19(10):78. doi:10.1007/s11934-018-0834-8
56. Cox L, He C, Bevins J, Clemens JQ, Stoffel JT, Cameron AP. Gentamicin bladder instillations decrease symptomatic urinary tract infections in neurogenic bladder patients on intermittent catheterization. Can Urol Assoc J. 2017;11(9):E350–E354. doi:10.5489/cuaj.4434
57. Andretta E, Longo R, Balladelli M, Sgarabotto C, Sgarabotto D. Intravesical gentamicin: an option for therapy and prophylaxis against recurrent UTIs and resistant bacteria in neurogenic bladder patients on intermittent catheterization. Antibiotics. 2022;11(10):1335. doi:10.3390/antibiotics11101335
58. Cicione A, Cantiello F, Ucciero G, et al. Intravesical treatment with highly-concentrated hyaluronic acid and chondroitin sulphate in patients with recurrent urinary tract infections: results from a multicentre survey. Can Urol Assoc J. 2014;8(9–10):E721–E727. doi:10.5489/cuaj.1989
59. Wagenlehner FME, Tandogdu Z, Bjerklund Johansen TE. An update on classification and management of urosepsis. Curr Opin Urol. 2017;27(2):133–137. doi:10.1097/MOU.0000000000000364
60. Portsmouth S, Bass A, Echols R, Tillotson G. Heterogeneity of recent phase 3 complicated urinary tract infection clinical trials. Open Forum Infect Dis. 2021;8(3):ofab045. doi:10.1093/ofid/ofab045
61. Malaisri C, Phuphuakrat A, Wibulpolprasert A, Santanirand P, Kiertiburanakul S. A randomized controlled trial of sitafloxacin vs. ertapenem as a switch therapy after treatment for acute pyelonephritis caused by extended-spectrum β-lactamase-producing Escherichia coli: a pilot study. J Infect Chemother. 2017;23(8):556–562. doi:10.1016/j.jiac.2017.05.005
62. Seo YB, Lee J, Kim YK, et al. Randomized controlled trial of piperacillin-tazobactam, cefepime and ertapenem for the treatment of urinary tract infection caused by extended-spectrum beta-lactamase-producing Escherichia coli. BMC Infect Dis. 2017;17(1):404. doi:10.1186/s12879-017-2502-x
63. Kaye KS, Bhowmick T, Metallidis S, et al. Effect of meropenem-vaborbactam vs piperacillin-tazobactam on clinical cure or improvement and microbial eradication in complicated urinary tract infection: the TANGO I randomized clinical trial. JAMA. 2018;319(8):788–799. doi:10.1001/jama.2018.0438
64. Harris PNA, Tambyah PA, Lye DC, et al. Effect of piperacillin-tazobactam vs meropenem on 30-day mortality for patients with E coli or Klebsiella pneumoniae bloodstream infection and ceftriaxone resistance: a randomized clinical trial. JAMA. 2018;320(10):984–994. doi:10.1001/jama.2018.12163
65. Portsmouth S, Veenhuyzen D, Echols R, et al. Cefiderocol versus imipenem-cilastatin for the treatment of complicated urinary tract infections caused by gram-negative uropathogens: a phase 2, randomised, double-blind, non-inferiority trial. Lancet Infect Dis. 2018;18(12):1319–1328. doi:10.1016/S1473-3099(18)30554-1
66. Bassetti M, Echols R, Matsunaga Y, et al. Efficacy and safety of cefiderocol or best available therapy for the treatment of serious infections caused by carbapenem-resistant gram-negative bacteria (CREDIBLE-CR): a randomised, open-label, multicentre, pathogen-focused, descriptive, phase 3 trial. Lancet Infect Dis. 2021;21(2):226–240. doi:10.1016/S1473-3099(20)30796-9
67. The Joint Commission. New and revised requirements addressing antibiotic stewardship for the hospital and critical access hospital programs. Available from: https://www.jointcommission.org/standards/prepublication-standards/new-and-revised-requirements-addressing-antibiotic-stewardship-for-hospital/.
68. XERAVA (eravacycline) for injection [package insert]. Tetraphase Pharm. Waltham, MA; 2018.
69. GlobeNewswire News Room. Tetraphase announces top-line results from IGNITE3 phase 3 clinical trial of eravacycline in complicated Urinary Tract Infections (cUTI); 2018. Available from: https://www.globenewswire.com/news-release/2018/02/13/1340188/34757/en/Tetraphase-Announces-Top-Line-Results-from-IGNITE3-Phase-3-Clinical-Trial-of-Eravacycline-in-Complicated-Urinary-Tract-Infections-cUTI.html.
70. Motsch J, Murta de Oliveira C, Stus V, et al. RESTORE-IMI 1: a multicenter, randomized, double-blind trial comparing efficacy and safety of imipenem/relebactam vs colistin plus imipenem in patients with imipenem-nonsusceptible bacterial infections. Clin Infect Dis. 2020;70(9):1799–1808. doi:10.1093/cid/ciz530
71. George Sakoulas MD. FDA approves imipenem-cilastatin/relebactam (recarbrio) for complicated intra-abdominal or urinary tract infections. NEJM J Watch. 2019;2019. doi:10.1056/nejm-jw.NA49571
72. Wagenlehner FME, Cloutier DJ, Komirenko AS, et al. Once-daily plazomicin for complicated urinary tract infections. N Engl J Med. 2019;380(8):729–740. doi:10.1056/NEJMoa1801467
73. Inc A. ZEMDRITM (plazomicin) approved by FDA for the treatment of adults with complicated Urinary Tract Infections (cUTI). GlobeNewswire News Room; 2018. Available from: https://www.globenewswire.com/news-release/2018/06/26/1529573/30133/en/ZEMDRITM-plazomicin-Approved-by-FDA-for-the-Treatment-of-Adults-with-Complicated-Urinary-Tract-Infections-cUTI.html.
74. Kaye KS, Belley A, Barth P, et al. Effect of cefepime/enmetazobactam vs piperacillin/tazobactam on clinical cure and microbiological eradication in patients with complicated urinary tract infection or acute pyelonephritis: a randomized clinical trial. JAMA. 2022;328(13):1304–1314. doi:10.1001/jama.2022.17034
75. Allecra therapeutics publishes final phase 3 ALLIUM data in JAMA: cefepime/enmetazobactam met criteria for superiority; 2022. Available from: https://www.businesswire.com/news/home/20221005005413/en/Allecra-Therapeutics-Publishes-Final-Phase-3-ALLIUM-Data-in-JAMA-CefepimeEnmetazobactam-Met-Criteria-for-Superiority.
76. Eckburg PB, Muir L, Critchley IA, et al. Oral tebipenem pivoxil hydrobromide in complicated urinary tract infection. N Engl J Med. 2022;386(14):1327–1338. doi:10.1056/NEJMoa2105462
77. Duffy S. FDA needs more data on tebipenem HBr for complicated UTI. MPR; 2022. Available from: https://www.empr.com/home/news/drugs-in-the-pipeline/fda-needs-more-data-on-tebipenem-hbr-for-complicated-uti/.
78. Rex JH, Eisenstein BI, Alder J, et al. A comprehensive regulatory framework to address the unmet need for new antibacterial treatments. Lancet Infect Dis. 2013;13(3):269–275. doi:10.1016/S1473-3099(12)70293-1
79. IMI Innovative Medicines Initiative. ND4BB | new drugs for bad bugs. IMI Innovative Medicines Initiative. Available from: http://www.imi.europa.eu/projects-results/project-factsheets/nd4bb.
80. Gingrey P. H.R.2182-112th congress (2011–2012): generating antibiotic incentives now act of 2011; 2011. Available from: http://www.congress.gov/.
81. FDA. Limited population pathway for antibacterial and antifungal drugs – the LPAD pathway; 2020. Available from: https://www.fda.gov/drugs/development-resources/limited-population-pathway-antibacterial-and-antifungal-drugs-lpad-pathway.
82. Turner KM, Christensen H, Adams EJ, et al. Analysis of the potential for point-of-care test to enable individualised treatment of infections caused by antimicrobial-resistant and susceptible strains of Neisseria gonorrhoeae: a modelling study. BMJ Open. 2017;7(6):e015447. doi:10.1136/bmjopen-2016-015447
83. Wojno KJ, Baunoch D, Luke N, et al. Multiplex PCR based Urinary Tract Infection (UTI) analysis compared to traditional urine culture in identifying significant pathogens in symptomatic patients. Urology. 2020;136:119–126. doi:10.1016/j.urology.2019.10.018
84. Elligsen M, Pinto R, Leis JA, Walker SAN, Daneman N, MacFadden DR. Improving Decision Making in Empiric Antibiotic Selection (IDEAS) for gram-negative bacteremia: a prospective clinical implementation study. Clin Infect Dis. 2021;73(2):e417–e425. doi:10.1093/cid/ciaa921
85. Gupta K, Hooton TM, Naber KG, et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the infectious diseases society of America and the European society for microbiology and infectious diseases. Clin Infect Dis. 2011;52(5):e103–e120. doi:10.1093/cid/ciq257
86. Medical student curriculum: adult UTI - American Urological Association. Available from: https://www.auanet.org/meetings-and-education/for-medical-students/medical-students-curriculum/adult-uti.
87. Kidney Disease: Improving Global Outcomes (KDIGO) Transplant Work Group. KDIGO clinical practice guideline for the care of kidney transplant recipients. Am J Transplant. 2009;9(Suppl 3):S1–S155. doi:10.1111/j.1600-6143.2009.02834.x
88. Al Midani A, Elands S, Collier S, Harber M, Shendi AM. Impact of urinary tract infections in kidney transplant recipients: a 4-year single-center experience. Transplant Proc. 2018;50(10):3351–3355. doi:10.1016/j.transproceed.2018.08.022
89. VABOMERE (meropenem and vaborbactam) for injection [package insert]. Melinta Ther. Parisppany New Jersey; 2017.
90. FDA. FDA approves new antibacterial drug to treat complicated urinary tract infections as part of ongoing efforts to address antimicrobial resistance; 2020. Available from: https://www.fda.gov/news-events/press-announcements/fda-approves-new-antibacterial-drug-treat-complicated-urinary-tract-infections-part-ongoing-efforts.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.