Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
University Staff Insights on Interprofessional Education and Student-Led Clinic Opportunities at an Australian University
Authors Collis JM ![]() , Barradell S, Broman P
, Barradell S, Broman P ![]() , Brownie S
, Brownie S
Received 8 November 2023
Accepted for publication 28 December 2023
Published 20 January 2024 Volume 2024:17 Pages 305—315
DOI https://doi.org/10.2147/JMDH.S447690
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Julie M Collis,1 Sarah Barradell,1 Patrick Broman,1,2 Sharon Brownie1– 3
1School of Health Sciences, Swinburne University of Technology, Melbourne, VIC, Australia; 2Centre for Health and Social Practice, Waikato Institute of Technology, Hamilton, New Zealand; 3Griffith Health, Griffith University, Gold Coast, QLD, Australia
Correspondence: Julie M Collis, Email [email protected]
Purpose: Organizational and university staff buy-in and advocacy are critical considerations in planning successful interprofessional education (IPE) initiatives in healthcare, such as interprofessional student-led clinics (SLCs). This study was designed with the purpose of gaining deeper insight into current views and perspectives of academic and professional staff at an Australian university, as a precursor to planning IPE and SLC activities.
Methods: All academic and professional staff from within the School of Health Sciences were invited to participate in the study. In-depth-qualitative interviews were conducted with 16 staff to explore academic and professional staff perspectives on IPE and SLCs. Reflexive thematic analysis was used to analyse the data.
Results: Findings are grouped within five themes that incorporate broad perspectives on the tensions and possibilities of IPE and establishment of SLCs: Academic and professional staff commitment; Better/smarter IPE; Student-led clinic potential; Vision and innovation; and Strategy and resourcing. The themes reflect the high value placed on IPE by academic and professional staff and incorporate innovative ideas on how to prepare students for a rapidly changing and evolving healthcare environment. A reticence towards standard models of university based SLCs was expressed.
Conclusion: Academic and professional staff insights suggest university leaders need to develop a greater strategic focus on improving IPE. Effective engagement with staff is required to support IPE planning and implementation. If considering implementation of SLCs, contemporary fit-for-purpose models should be explored such as partnerships with primary healthcare providers, community wellness facilities, and hospital clinics rather than traditional university-based clinics.
Keywords: health occupations, interprofessional education, interdisciplinary placement, patient care team
Introduction
Education of health professionals is constantly adapting within universities to ensure that graduates are ready to practice in increasingly complex health environments.1 Current industry requirements suggest that health graduates must be ready to address complex comorbid conditions, and the burgeoning needs associated with an aging population. Interprofessional education (IPE) and practice (IPP) opportunities are globally acknowledged as an effective mechanism by which to develop the interprofessional competencies needed to address the previously mentioned challenges of contemporary health service delivery.1,2 The World Health Organisation defines IPE as occurring when students from different disciplines engage in collaborative learning and problem solving to improve health outcomes.3
One IPE strategy that has strong uptake amongst universities is the establishment of university-based student led clinics (SLCs). SLCs have been widely implemented for the purposes of providing interprofessional learning, increasing numbers of fieldwork placements, and providing healthcare to the local community and/or underserved populations.4 Although IPE and SLCs are widely reported around the world, hindrances to successful implementation of these strategies remain at the forefront of educational literature5,6 Current best-practice for IPE and SLCs, and the degree to which academic staff support establishing university-based SLCs remain unclear in the literature. Despite the longstanding recognition of the need for graduate health professionals to engage in IPE and attain interprofessional competence, progress remains frustratingly slow. For any university initiative to be successful it is essential that proposed changes be informed by current evidence, ‘what works’, and faculty views and perspectives. It is well documented that without the support and buy-in of staff and appropriate resourcing from university administration, IPE or SLC innovations are unlikely to be successful.7–9 We therefore set out to canvas academic and professional staff perspectives to inform cohesive, staff-supported directions at Swinburne University of Technology.
The aim of this study was to explore academic and professional staff perspectives on interprofessional education and SLC opportunities. The intent was to assess the level of faculty and staff understanding, buy-in and readiness for interprofessional learning and SLC development as a precursor to planning an implementation.
Methods
Study Design
This research is part of a larger case-based mixed methods study. The initial study involved a whole of school and faculty survey inviting both Likert scale and short answer responses related to IPE and SLCs. Participants were then provided with a voluntary opportunity to participate in an in-depth qualitative interview. This article reports findings of the follow-on interviews designed for qualitative exploration of the perspectives of academic and professional staff about interprofessional education and SLCs.
Ethics
Ethics approval was obtained from the Human Research Ethics Committee of Swinburne University of Technology (reference 20237061–14174).
Context
The School of Health Sciences at Swinburne University of Technology comprises three organisational departments (Department of Health Sciences and Biostatistics, Department of Nursing and Allied Health and Department of Psychological Sciences), three research centres, the Swinburne Psychology Clinic, and the Wellbeing Clinic for Older Adults. A range of entry-level (Bachelor and Graduate Masters) and postgraduate health and health professional courses are offered each year in the areas of biomedical science, statistics, nursing, dietetics, nutrition, occupational therapy, physiotherapy, psychology, health promotion, public and environmental health, and exercise and sports science.
The school is almost a decade old and is in a period of growth related to both course enrolments and expansion of health programs. Forward planning activities are exploring various strengths, facilitators, barriers, and strategies especially related to partnerships, placement models and other forms of work integrated learning.
Theoretical and Researcher Positionality
The research team were academics from the Swinburne University of Technology. All were experienced researchers familiar with qualitative methodologies. The research team had varied experience of interprofessional education and/or student led clinics and were from different disciplines (occupational therapy, physiotherapy, demography, and nursing) thereby bringing a richness of knowledge and perspective to the research question. None of the researchers interviewed staff from their own discipline to ensure any existing relationships did not influence data generation. Reflexivity throughout the study was maintained through use of field notes, challenging of assumptions and prior knowledge, and robust dialogue within the research team. Quality of analysis was promoted through a collaborative process of dialogue and debate to promote shared understandings and interpretation of the data. The study was underpinned by a constructivist paradigm. Constructivism emphasises subjectivity in the acquisition of knowledge where participant narratives of experiences and beliefs are core to the research process.10 The researcher is not an independent observer in the research, rather the relationship between researcher, participant and context is emphasized and used to construct and elucidate knowledge about the phenomena under investigation.10
Participants
We used convenience sampling to recruit participants. All academic or professional staff within the University School of Health Sciences were invited to complete an online survey regarding IPE and SLCs. At the completion of the survey participants were invited to participate in an interview to explore perspectives about IPE and SLCs in greater depth than could be achieved from a survey. Of 187 staff, 60 completed the survey. Twenty staff indicated interest in participating in the interviews and 16 consented to and proceeded to interview. Participants provided consent for publication of their anonymized responses/quotes in a range of research outputs.
Data Collection
Individual semi structured interviews were conducted with consenting participants using a prepared interview guide. Questions were structured around four areas: role within the health science school with respect to clinical education; perceptions of workforce needs within the participant’s discipline; understandings and challenges of IPE; and opportunities and directions for a potential interprofessional SLC. Interviews were conducted either face-to-face or online using Microsoft Teams according to the preference of the participant. The researchers and each participant mutually agreed the time and location of interview. Three members of the research team (JC, SBa and PB) completed the interviews but did not interview individuals from their own discipline or for whom a supervisory relationship existed. The interviews typically lasted between 45 and 60 minutes and were video and/or audiotaped. All interviews were transcribed in real time using the transcription function on Microsoft Teams. Subsequently a transcriber listened to the audio recording and corrected the transcription to provide an accurate verbatim record of the interview. Recordings were then deleted.
Data Analysis
Data were analysed according to the six steps of reflexive thematic analysis.11 Reflexive thematic analysis is a structured approach that promotes a thick description of the data.12 The researcher is recognised as an active, participatory voice in the analysis, while simultaneously remaining reflexive to and critical of the inherent knowledge, values, and beliefs they bring to the research.11 Two researchers (JC and PB) familiarised themselves with the transcripts, then inductively coded the data in NVivo 14. To ensure a consistent analytic approach, the researchers independently coded one transcript then met to compare and develop a shared understanding of the data. The remaining 15 transcripts were coded independently by JC (9) and PB (6) with frequent meetings to compare and discuss coding. A Miro board (Miro.com) was used to aid with theming. Candidate themes were firstly developed by JC and PB and then collaboratively confirmed and named by all authors.
Results
A total of 16 staff participated from end of May 2023 to 12 July 2023 as detailed in Table 1. Participants represented various disciplines across the three departments. Given the small size of the respective departments, we have elected not to provide specific disciplinary data or use pseudonyms so as not to potentially identify participants.
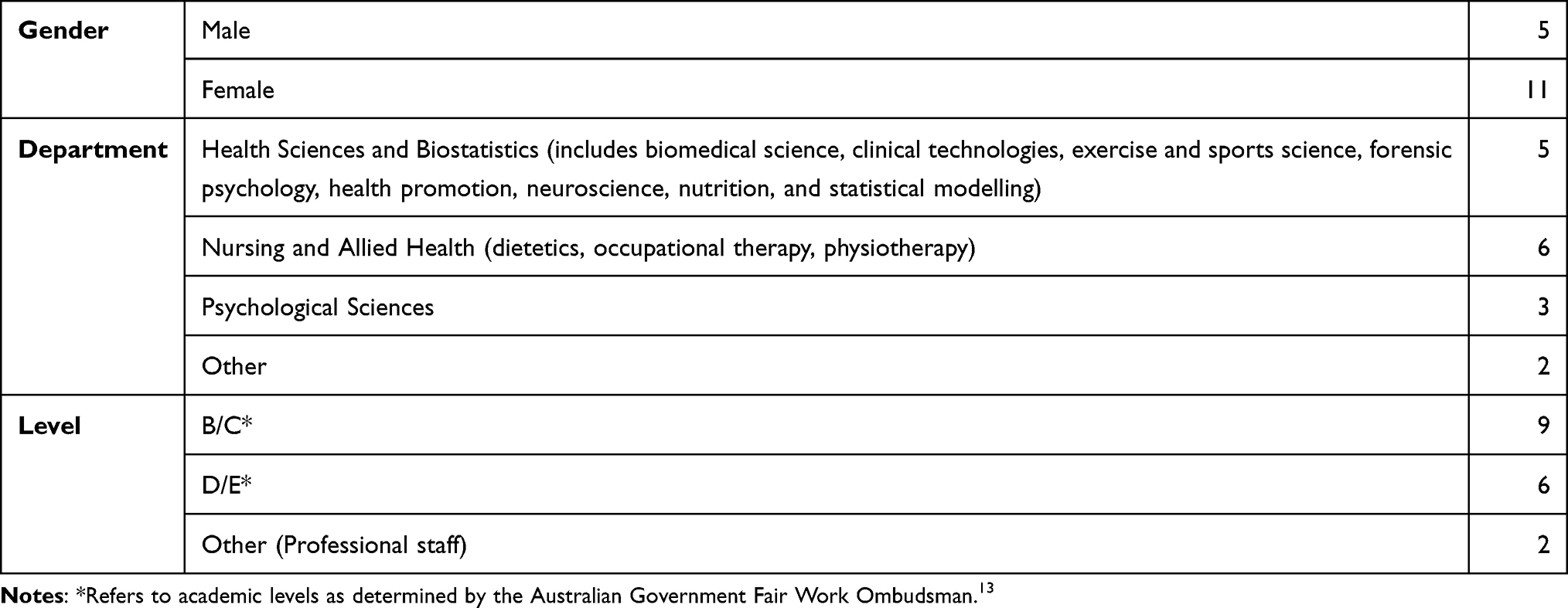 |
Table 1 Participant Characteristics |
Narratives from the interviews demonstrated the deep desire of academic and professional staff to develop students capable of working in complex environments and addressing complex health needs. Five themes were generated describing a broad spectrum of perspectives on interprofessional education and future innovation and are summarised in Table 2. The themes with illustrative quotes are detailed. Description of the themes also outline the concepts embedded within each theme. Responses provided insight regarding staff commitment to IPE with stronger more divergent views expressed in respect to the option for university based SLCs.
 |
Table 2 Themes Describing Academic and Professional Staff Perspectives on IPE and SLC Opportunities |
Theme One: Academic and Professional Staff are Highly Invested in Developing a Workforce Responsive to Mental Health, Chronic Conditions, Aged Care, and Disability
The first theme describes how academic and professional staff have a strong impetus to develop students ready to fill future workforce gaps. Narratives revealed that university academic and professional staff have a “bird’s eye” view of healthcare needs and are acutely aware of enabling health professional students to work across a broad spectrum of practice areas. Gaps in healthcare delivery were understood to be complex, far ranging and evolving. The most pressing gaps in healthcare were perceived to be in the areas of mental health, chronic conditions, aged care, and disability.
…the desperate need is in a couple of spaces, aged care and community in-home care…the aged care population are increasingly being supported to stay at home because there will never be enough aged care facilities…so being in that community aged care home visit space is critical. Disability care [is also] more and more needed in the home space, particularly for, you know, younger people who are not suited to aged care facilities. P8
Mental health was widely articulated as an area of healthcare that is under-resourced.
Across all OT programs there’s been a shortage of mental health placements for a number of years, which is a huge workforce issue. And so, there’s various strategies that we’re using to try and increase those number of placements. So, I’d say mental health is the clinical area [of greatest need]. P9
Many participants also highlighted the need for students to have greater opportunities to work in Indigenous health in order to develop culturally safe competencies and knowledge.
And we haven’t even gone far enough into the indigenous health [space]. We need to push for you know, everyone needs to push further into that sphere. P15
A common concern expressed in addressing gaps in the mental health, aged care and disability sectors was the difficulty of exposing health professional students to these clinical areas via fieldwork placements. Without exposure to varied clinical populations, students do not see these sectors as a viable future employment.
That’s an area that we wanted to grow because it can become a vicious circle in terms of like a full-on effect. Like if a student doesn’t have a mental health placement, then it would be less likely that they’re interested to apply for a mental health job in the future. So then that continues. P5
Some participants described perceptions about the aged care sector that needed to be challenged due to poor perceptions or work conditions in those sectors. There was a perception that health professionals are underutilised in aged care, and that disciplines such as occupational therapy or exercise physiologists have more skills and knowledge to offer than is currently utilised.
I guess in aged care… there are not enough registered nurses to deliver the safe and quality care… they don’t stay long, you know. They have the expectation that they will go to the facility (aged care) because they couldn’t find any jobs other elsewhere. P4
Theme Two: Interprofessional Education Requires Better and Smarter Approaches
Academic and professional staff were clear that health professional students need to learn collaborative healthcare practice. IPE was highly valued but seen to be too siloed within disciplines and lacking a cohesive approach within the university. Participants expressed that students needed to have a strong sense of their own professional identity before embarking on interprofessional learning.
Overall participants perceived that IPE empowers students to approach healthcare through a diverse lens.
Yeah, I mean, you can learn a lot, you can learn in 10 minutes with what I call cross disciplinary [education]. You know when you sort of switch over and get another perspective from the person working next to you, you learn, the acceleration of learning is massive. Because you’re suddenly looking at it from a different perspective and that person is talking to you and trying things that they say 100 times a day. But to you, it’s new material. And you go well, OK, I’m gonna use that. P15
Terminology surrounding IPE was often expressed as being problematic without a unified definition. While many participants described IPE as collaborative problem-solving, others saw multi-disciplinary learning as a more appropriate and descriptive term.
I’m careful about using interprofessional because I think it confuses people and IPE is sort of the standard abbreviation… but they’re not working in an interprofessional way. If you get what I mean, it’s just that all the professions are together, working on the one thing. I’d prefer to call it multidisciplinary learning because I think people still stay in their lanes a bit and I think they need to when they’re still learning their lanes. P11
IPE was seen to be more than working with health professionals. Practicing collaboratively was also about working with disciplines such as designers, engineers, or data analysts to solve healthcare problems.
Biostats is integral to a school of health and my feeling is that it needs to be incorporated everywhere… Quite frankly, they need us as much statistics as they can get. They’ve got to be comfortable with all these different streams of data, making sense of them. P10
Many participants saw fieldwork placements as the primary vehicle for learning interprofessional practice, while others perceived this as being limited because good models of IPP are rare.
So the competency [interprofessional learning] has to be met across the [clinical] placement... we’re not working necessarily directly with other disciplines, it’s more around who’s involved with the client... you know how you work with other disciplines and that you know that that’s not something you teach in a class. So, it can maybe depend on the circumstances, the particular placements the person goes on or the supervisor they have or their own particular personal style which impacts on somebody. P3
Participants described a broad range of strategies used at our university to facilitate IPE such as simulations, case studies, group discussions, guest lectures, student volunteer projects. Simultaneously, frustrations were expressed about how poorly IPE is implemented.
Overall, there was a sense of needing to do IPE better and find more creative and innovative ways of facilitating interprofessional learning.
It’s [interprofessional learning] very limited... it’s mostly students who are coming from other programs that are in the classroom and contributing their own disciplinary knowledge. So, it’s ad hoc and it would be great if we had some shared classes across the different fields that were more structured. P7
Theme Three: University-Based Student Led Clinics Have Potential but are Limited in Scope and Vision
This theme relates to academic and professional staff perspectives around SLCs and the potential of such a model for their own programs and courses. SLCs were seen to offer possibilities for individual disciplines and for interprofessional education. Equally, SLCs were seen to be limited in their potential to address multifaceted placement demands and expose students to specific and underserved areas of healthcare (most notably, complex mental health and acute hospital care).
At Swinburne University of Technology there is a uni-professional Psychology Clinic, and its importance to the clinical psychology program and positive reputation was emphasised.
The Swinburne clinic is very respected. I think people know that they get good training, lots of very hands-on supervision. Quality of supervision can vary a bit, so the fact that they know that our students have been through our clinic and have been supervised by our staff, I think really does help. P13
Academic and professional staff expressed a range of views around the potential for expanded or interprofessional SLCs. Some were very enthusiastic about such clinics and what they might offer, suggesting that that they could provide much-needed placement opportunities, aid in the development of key skills and knowledge for students, and also contribute to filling healthcare gaps and improving health outcomes in the community.
I’m really excited about this opportunity…I really like the concept about the student led interprofessional clinic because we can solve many problems with this approach... students can get expertise. We can deliver services to the community or placement. I really like this concept…I have not directly led any student led interprofessional clinic, but I’m fascinated with this idea. P4
Other staff were more circumspect, emphasizing the challenges that an SLC would face, including in supervision (several noted tensions between academic teaching and clinical supervisory roles that may be blurred in a university-based SLC), logistics (such as timetabling, locating physical space, and liability issues), the likely cost and the lack of infrastructure (such as ability to refer for an x-ray or medical support). SLCs were noted by some staff to be very resource intensive and difficult to fund.
that’s obviously one, you need funding. Someone who’s gonna run and manage it, and you’d probably need administrative staff. That would be liaising with all of the different areas within the university, depending on the target student population that could be utilized to benefit the programs, the holistic programs, for each of the different target populations.And space, I guess. Funding and space. Knowing how big you should make it, who then has access to it? Is it just for Community service and research or is it blended them with teaching as well? P1
Several staff suggested that continuity of care is a challenge for SLCs, given students are only on placement for part of a year. Staff thought that this meant such a clinic would need to operate narrowly, in terms of the level of care of services offered, or perhaps require paying staff, at considerable cost, to provide appropriate care.
I think the on-campus model might turn into a white elephant because there’ll be times where it will just be dead. There’ll be no one around like as you know, there are times when the campus is busy and the times of the campus is there’s no one here. So economically it just, I just don’t know that it would be viable. P15
Staff also challenged student led as a term. This related to the level of supervision required, ethically and/or legally, for students engaged in healthcare delivery. Given that the provision of care in an SLC would always require intensive levels of supervision from registered professionals, staff queried the framing of services as “student-led”.
So, student-led is... I mean, it’s hard to know unless everybody has a consistent definition of what’s meant by student led. For me it would be hard to have something that was completely student-led just because of the needs for supervision for our accreditation purposes. P13
Some academics, particularly those who were more experienced, expressed doubts around the potential of any SLC to provide the type of learning or placement opportunities that their programs are currently lacking. Staff suggested that the scope of practice for an on-campus SLC would be inherently limited, and unlikely to provide sufficient scope for a full placement:
So yes, the students could absolutely engage, but it wouldn’t meet this the you know the proof test for the accreditation board. There would still be many other things that they would need to do outside that project to demonstrate that they’ve met clinical competency. P8
Theme Four: Expansive, Innovative Solutions are Envisioned by Academic and Professional Staff
This theme encompasses the innovative and expansive thinking of participants about new directions for IPE and student-delivered healthcare. While staff were cautious about a university SLC there were a plethora of ideas around developing SLCs in partnership with community or hospital health services. Staff also perceived opportunities to expand into areas such as management of neurodiverse populations, increasing numbers of undergraduate and post graduate students and expanding the range of programmes offered. Some staff offered ideas about working with community facilities.
We have some partners [who] do amazing things that specialize in the over 60 population, which I think is pretty young … and this setup … it’s not a gym. It’s set up like a health club. They have EPs (exercise physiologists). They have, you know, a range of other health professionals, physios, EPs, but others as well. So, they have those sorts of clinics, and they also provide in home care. P8
Other staff offered ideas about partnering with existing healthcare providers.
One of the things that we’re working on with. is a student led clinic that is actually housed at [the hospital]… So that that clinic is for elective hand surgery wait list patients … it would be an interesting model in that it’s gonna be collaborative with other universities. So, our placements are at different times to [another university] … we can sort of stagger it so that their students are on in a block. Then our students are on in a block and that way they’ve got coverage for most of the year. P11
A blended face-to-face and telehealth clinic was another suggestion for developing interprofessional competencies in an SLC setting.
If we had a student led clinic that actually taught students how to deliver telehealth in an interprofessional way, it could be pretty amazing.But I also think it needs to be a hybrid model. So, I think we actually…need to go out. We need to touch base. Do a face to face in the community. Then we deliver telehealth for a number of weeks…then we go back out. So there’s a blended or a hybrid model where we are seeing you face to face, but maybe you know I don’t know once a month or once every two months or something like that because I also strongly believe that you know we need to be out there and actually assessing people’s performance in their home. You know, are they actually coping? P8
Participants also suggested setting up a SLC within a medical practice or a community facility such as a leisure centre.
It’s a little bit of a different it’s sort of, an alternative placement if you know what I mean rather than a student led clinic is a sort of a different idea. You might have a student led clinic and you might have a satellite. You know where that student may spend some time in the satellite, in [a] GP Super Clinic or something like that. P15
Theme Five: Implementing IPE Innovations Requires Strategic, Focused Resourcing
Our final theme focuses on the efforts needed to action changes envisioned by participants. Our university has big thinkers, and many different ideas and directions were expressed. A unified direction or solution was not articulated, and it was evident that ongoing consultation and strategic investment of resources into interprofessional learning or student -delivered services is needed.
It’s [IPE] probably a bit siloed and I think now that I’m reflecting on it would be really good to enhance that interprofessional learning. I’m not entirely sure how that would work. But doesn’t mean it shouldn’t work, doesn’t mean we shouldn’t do it. P16
When asked about the challenges to interprofessional education and practice, participants expressed the need for greater resourcing.
Most of it is time and resource based. Everybody is trying to do more and more with less time and fewer resources, and I think in practice what that means is that the hierarchies and the power dynamics that exist within the health system are exacerbated. So, people feel like they’re not entitled to ask questions of people that might be higher up in the administration than them or from a specialty that has more prestige or more esteem than they perceive their own as being. And so, these barriers, that kind of shouldn’t exist between professionals. P13
There were frequent concerns about appropriate staffing, supervision, and ensuring a sustainable model is implemented.
But I’m just thinking about promoting the clinic and having all the links and permits and having the recognition within the area and having the procedures and policies in place, having the infrastructure. So that might take a while. I’d say to have that established and get that up and working as something that we can count on as a sustainable placement opportunity. Well yeah, I think so. I think risk management and referrals and continuity of care. P5
When asked about factors that would facilitate implementation of innovations such as SLCs, community partnerships or interprofessional learning, there were commonly expressed ideas about the need for careful planning, consultation with faculty, adequate staffing and funding, and having a clear vision.
I think if we had the right human resources, if we had enough staff, I don’t believe it is doable at the moment. Right now, it is incredibly difficult because I’m the only one. So, I think if we had the right staffing, I think it’s definitely a possibility. P16
Discussion
This case-based study set out to investigate academic and professional staff perspectives about directions for interprofessional education and potential establishment of university-based SLCs. University staff hold a wealth of perspectives that help university leaders plan initiatives supported and informed by academic and professional staff knowledge. Without faculty buy-in, IPE initiatives are highly unlikely to succeed.7 This study identified five themes that reveal both tensions and possibilities around IPE and establishment of SLCs. Participant narratives revealed an urgent need to develop graduates who are industry-ready to work in mental health, chronic conditions, aged care, and disability. Our participants perceived IPE as essential for preparing students to manage complex health needs but described enduring challenges with the execution of interprofessional activities. Moreover, while university-based student led clinics were perceived to have a role in health profession education, existing models were not perceived to be broad enough in scope. Expansive innovations were envisioned that included partnerships with existing and community health providers. Appropriate resourcing and strategic planning were highlighted as essential ingredients to action such innovations.
The study was conducted as part of our university’s health expansion planning processes with a view to the establishment of an SLC. An unexpected finding was the tension expressed around establishing a university-based student led clinic. Student-led clinics are widely implemented in Australia and worldwide,14,15 yet participants in our study, some with extensive SLC experience, did not see a SLC situated on the university campuses as an innovative way forward. Reasons for this included, but extended beyond, the well-recognised challenges of staffing, timetabling, and financial sustainability.4,5,16 One perspective was that SLCs do not serve clinical populations broad enough in scope to meet the fieldwork needs of health professional students most notably in acute hospital settings, mental health, chronic conditions, and aged cared. Participants saw potential for a university-based clinic with non-acute populations for providing health promotion or wellness interventions however this may not be supported by all disciplines. Student-led clinics were not perceived to be a one-size fits all solution and academic staff were reluctant to engage in a project that would not meet the most urgent needs of their discipline.
A clear perspective that emerged was the desire to develop a new, innovative model of student-delivered services that was industry-partnership-based, across multiple sites and services. This approach was seen to be more suited to the diverse needs across disciplines and the chance to enter into areas that lack fieldwork opportunities for some disciplines such as aged care facilities or community wellness providers. Although a definitive model was not articulated by participants, it was evident that staff had expansive ideas that represent a rich untapped resource. Such ideas can be explored more deeply through strategies such as working parties or think tanks with representatives from each discipline. Universities have the opportunity to develop new models of IPE and ‘student-led-clinics’ informed by innovative thinking of health science staff that future proofs health professional education.
The frustrations expressed around IPE being too siloed, challenging to implement, and lacking university strategic direction are consistent with the literature.6,17,18 This study agrees with studies that show IPE to be highly desirable and implemented at small scale,19 but that greater efforts are required for IPE to occur in an authentic, impactful way. Equally, for faculty to engage in IPE activities in meaningful ways, there must be strong, strategic university leadership that supports and resources IPE appropriately.9,20 Solutions that have been proposed include development of a national IPE curriculum,21 institutional commitments to implementing regulatory and professional body recommendations for IPE,22,23 developing a university wide-framework for IPE,18,24 and having a dedicated IPE change-agent or ambassador at both the university lead and discipline levels.8,18
Participant definitions of interprofessional education were broadly consistent with the WHO definition of health professions learning about, from and with each other to enable collaborative healthcare that improves outcomes.3 Some participants were more cautious about using the term interprofessional education and practice as it may denote health approaches where a professional from a certain discipline is credentialled or carries out roles traditionally associated with another discipline; for example, occupational therapists prescribing mobility aids or nurses providing psychological interventions. Participants were careful to emphasise that health professional students need to be assured in their discipline-specific skills and knowledge before embarking on interprofessional learning.
Further to institutional level change this study suggests that academic and professional staff are highly innovative and keen to explore new models of interprofessional learning and fieldwork opportunities. When asked “blue-sky” thinking questions, staff were quick to suggest a breadth of innovations. Some of the ideas centred around: interprofessional student healthcare to underserved populations in settings such as community centres, gyms or neighbourhood houses; a hybrid telehealth/face-to-face service for facilitating independence and wellness in older adults; wellness coaching at local leisure centres, early childhood facilities, or retirement villages; risk screening, health promotion, and mental health interventions at GP clinics; and interprofessional healthcare for people with chronic pain, fatigue or joint conditions, neurodiverse populations, mental illness, or people who are homeless. Suggestions were made around increasing interprofessional learning opportunities between mainstream health disciplines and disciplines such as biostatisticians, computer science or data analyst students, and non-regulated health disciplines such as exercise physiology and nutrition. Innovative approaches to facilitating IPE included use of escape rooms, asynchronous activities, and expanding existing single-discipline clinics to incorporate a broader range of disciplines.
A limitation of our study is that the single university case-based methodology may not be representative of other universities. We believe, however, that results will be informative for other universities considering new directions for interprofessional education or considering the establishment of student-led services.
Conclusions
This study has highlighted current perspectives on IPE and opportunities for SLCs within an Australian university. The academic and professional staff insights gathered can be used to inform university planners within Australia and broader global contexts. The study has revealed both tensions and possibilities around IPE and establishment of SLCs. The dichotomy of perspectives indicates a need for further consultation with academic and professional staff prior to embarking on specific development initiatives. A breadth of innovative ideas for student led, interprofessional clinics, were expressed by our health science staff but opportunities to collectively explore and scrutinise such innovations are rare. Findings reinforce existing evidence of the essential need for effective engagement to support IPE planning and implementation. Practice implications emphasise the need to underpin forward planning success with continuous school-level engagement, identification of change advocates and ambassadors, strong industry partnerships and adequate resourcing.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Frenk J, Chen LC, Chandran L, et al. Challenges and opportunities for educating health professionals after the COVID-19 pandemic. Lancet. 2022;400(10362):1539–1556. doi:10.1016/s0140-6736(22)02092-x
2. Interprofessional Education Collaborative Expert Panel. Core competencies for interprofessional collaborative practice: report of an expert panel; 2011.
3. World Health Organization. Framework for action on interprofessional education & collaborative practice; 2010. Available from: https://www.who.int/publications/i/item/framework-for-action-on-interprofessional-education-collaborative-practice.
4. Forbes R, Beckman E, Tower M, et al. Interprofessional, student-led community health clinic: expanding service provision and clinical education capacity. Aust Health Rev. 2021;45(2):255–260. doi:10.1071/AH20021
5. Tokolahi E, Broman P, Longhurst G, et al. Student-led clinics in Aotearoa New Zealand: a scoping review with stakeholder consultation. JMDH. 2021;Volume 14:2053–2066. doi:10.2147/jmdh.s308032
6. Li JT, Chau JPC, Wong SYS, et al. Interprofessional education—situations of a university in Hong Kong and major hurdles to teachers and students. Front Educ. 2022;7. doi:10.3389/feduc.2022.653738
7. Doll J, Maio A, Potthoff M. Epic failure: lessons learned from interprofessional faculty development. Perspect Med Educ. 2018;7(6):408–411. doi:10.1007/s40037-018-0488-8
8. Najjar G, Ascione FJ. Faculty leaders’ views of successful implementation of interprofessional education: a Case Study. JIEP. 2020;21:100371. doi:10.1016/j.xjep.2020.100371
9. Olenick M, Allen LR. Faculty intent to engage in interprofessional education. JMDH. 2013;6:149–161. doi:10.2147/JMDH.S38499
10. Lee CJG. Reconsidering constructivism in qualitative research. Educ Philos Theory. 2012;44(4):403–412. doi:10.1111/j.1469-5812.2010.00720.x
11. Braun V, Clarke V, Hayfield N, Terry G. Thematic Analysis. In: Liamputtong P, editor. Handbook of Research Methods in Health Social Sciences. Springer; 2019:843–860.
12. Ponterotto JG. Brief note on the origins, evolution, and meaning of the qualitative research concept “Thick Description”. Qual Rep. 2006;11(3):538–549. doi:10.46743/2160-3715/2006.1666
13. Australian Government Fair Work Ombudsman. Higher education industry-academic staff-award 2020. Available from: https://library.fairwork.gov.au/award/?krn=MA000006#_Toc141265466.
14. Moore K, Bacon R, Bevitt T, et al. Report: the university health clinic: definition, educational practices and outcomes. FoHPE. 2018;19(2):1–13. doi:10.11157/fohpe.v19i2.213
15. Wynne D, Cooper K. Student-led rehabilitation groups and clinics in entry-level health education: a scoping review. JBI Evid Synth. 2021;19(11):2958–2992. doi:10.11124/jbies-20-00340
16. Kavannagh J, Kearns A, McGarry T. The benefits and challenges of student-led clinics within an Irish context. J Pract Teach Learn. 2014;13(2–3):58–72. doi:10.1921/jpts.v13i2-3.858
17. Lash DB, Barnett MJ, Parekh N, Shieh A, Louie MC, Tang TTL. Perceived benefits and challenges of interprofessional education based on a multidisciplinary faculty member survey. Am J Pharm Educ. 2014;78(10):180. doi:10.5688/ajpe7810180
18. Grymonpre RE, Ateah CA, Dean HJ, et al. Sustainable implementation of interprofessional education using an adoption model framework. Can J High Educ. 2016;46(4):76. doi:10.47678/cjhe.v46i4.186571
19. Wilkes M, Kennedy R. Interprofessional health sciences education: it’s time to overcome barriers and excuses. J Gen Intern Med. 2017;32(8):858–859. doi:10.1007/s11606-017-4069-z
20. Bashatah AS, Al-Ahmary KA, Al Arifi M, et al. Interprofessional cooperation: an interventional study among saudi healthcare teaching staff at King Saud University. JMDH. 2020;13:1537–1544. doi:10.2147/JMDH.S279092
21. Dunston R, Forman D, Thistlethwaite J, Steketee C, Rogers GD, Moran M. Repositioning interprofessional education from the margins to the centre of Australian health professional education – what is required? Aust Health Rev. 2019;43(2):224. doi:10.1071/ah17081
22. Bogossian F, Craven D. A review of the requirements for interprofessional education and interprofessional collaboration in accreditation and practice standards for health professionals in Australia. JIC. 2021;35(5):691–700. doi:10.1080/13561820.2020.1808601
23. Bogossian F, New K, George K, et al. The implementation of interprofessional education: a scoping review. Adv Health Sci Educ. 2023;28(1):243–277. doi:10.1007/s10459-022-10128-4
24. El-Awaisi A, Anderson E, Barr H, Wilby KJ, Wilbur K, Bainbridge L. Important steps for introducing interprofessional education into health professional education. JTUMED. 2016;11(6):546–551. doi:10.1016/j.jtumed.2016.09.004
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Do Regulatory and Curriculum Requirements for Interprofessional Practice Align?
Brownie S, Tokolahi E, Broman P, Haggie M, Andersen P
Journal of Multidisciplinary Healthcare 2023, 16:3675-3687
Published Date: 29 November 2023