Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Unilateral Spatial Neglect After Stroke: Current Insights
Authors Gammeri R, Iacono C, Ricci R ![]() , Salatino A
, Salatino A ![]()
Received 10 August 2019
Accepted for publication 24 December 2019
Published 10 January 2020 Volume 2020:16 Pages 131—152
DOI https://doi.org/10.2147/NDT.S171461
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Roberto Gammeri, 1 Claudio Iacono, 1 Raffaella Ricci, 1, 2 Adriana Salatino 1
1Department of Psychology, SAMBA (SpAtial, Motor and Bodily Awareness) Research Group, University of Turin, Turin, Italy; 2Neuroscience Institute of Turin (NIT), University of Turin, Turin, Italy
Correspondence: Raffaella Ricci; Adriana Salatino
Department of Psychology, Via Verdi, 10, Turin 10124, Italy
Tel +39 0116702057
Email [email protected]; [email protected]
Introduction: Unilateral spatial neglect (USN) is a disorder of contralesional space awareness which often follows unilateral brain lesion. Since USN impairs awareness of contralesional space/body and often of concomitant motor disorders, its presence represents a negative prognostic factor of functional recovery. Thus, the disorder needs to be carefully diagnosed and treated. Here, we attempted to present a clear and concise picture of current insights in the comprehension and rehabilitation of USN.
Methods: We first provided an updated overview of USN clinical and neuroanatomical features and then highlighted recent progresses in the diagnosis and rehabilitation of the disease. In relation to USN rehabilitation, we conducted a MEDLINE literature research on three of the most promising interventions for USN rehabilitation: prismatic adaptation (PA), non-invasive brain stimulation (NIBS), and virtual reality (VR). The identified studies were classified according to the strength of their methods.
Results: The last years have witnessed a relative decrement of interest in the study of neuropsychological disorders of spatial awareness in USN, but a relative increase in the study of potential interventions for its rehabilitation. Although optimal protocols still need to be defined, high-quality studies have demonstrated the efficacy of PA, TMS and tDCS interventions for the treatment of USN. In addition, preliminary investigations are suggesting the potentials of GVS and VR approaches for USN rehabilitation.
Conclusion: Advancing neuropsychological and neuroscience tools to investigate USN pathophysiology is a necessary step to identify effective rehabilitation treatments and to foster our understanding of neurofunctional bases of spatial cognition in the healthy brain.
Keywords: unilateral spatial neglect, rehabilitation, spatial attention, stroke
Introduction
The first attempt to define Unilateral Spatial Neglect (USN), a neuropsychological disorder of spatial awareness that often follows unilateral brain lesion, was made in the second half of the 19th century.1 A remarkable number of studies of USN have been published towards the end of the 20th century and the beginning of the current century. However, the last 10–15 years have witnessed a relative decrement in the number of neuropsychological papers investigating this syndrome. The reason might be twofold. Firstly, the advancement of neuroimaging and, more recently, brain stimulation methodologies has driven the interest (and preference) of cognitive neuroscientists toward the use of these innovative techniques to investigate the neurofunctional bases of spatial cognition in the healthy brain. Secondly, medical advances in the treatment of acute stroke have significantly improved individuals’ clinical and neuropsychological conditions. Nonetheless, USN is quite frequent since it occurs in about 25–30% of all stroke individuals and over 90% of people with USN have right-hemisphere lesions.2 In the acute phase, USN occurs in 43% of individuals with right-hemisphere lesion (RHL) and 20% of those with left-hemisphere lesions (LHL). At 3 months, it is still present in 17% and 5% of RHL and LHL individuals, respectively.3 Neglect per se, rather than overall stroke severity, predicts poor outcome in functional recovery.4 It may indeed entail longer hospitalization, functional dependency, long-term disabilities in activities of daily living and increased risk of falls.5,6
Thus, USN is an important neuropsychological condition that needs to be carefully diagnosed and treated. Here, we attempt to provide a clear and concise picture of current insights in the comprehension and rehabilitation of USN. We briefly overview USN clinical and neuroanatomical features and then highlight recent progresses in the diagnosis and rehabilitation of USN. In relation to the latter topic, we review recent findings on three of the most promising interventions for USN rehabilitation: prismatic adaptation (PA), non-invasive brain stimulation (NIBS), and virtual reality (VR).
Clinical Manifestations
Individuals affected by USN fail to explore, orient or respond to contents of the contralesional side of somatic and extrasomatic space.7,8 In the acute phase, they show an ipsilesional deviation of the head and the eyes and may respond to stimuli presented in the contralesional side as if they were in the “intact” side. During everyday activities, they may eat food only from the ipsilesional side of the plate, bump into objects located in the contralesional side when walking, and wash, shave, or apply cosmetics only to the ipsilesional side of the face/body.1
USN Is a Complex Syndrome
There is a broad consensus among researchers on the heterogeneity of USN symptoms that is thought to reflect the complexity of neural correlates of spatial attention/representation. Building a coherent representation of space entails a complex integration of different sensory inputs and output-related factors, in relation to different portions of space and coordinates systems. Coherently with this assumption, USN symptoms can dissociate across sensory modalities,9 sectors of space (i.e., personal, peri-personal and extra-personal space10–14), reference frames (egocentric vs allocentric neglect15–17), and tasks.18 An often neglected dissociation concerns symptoms affecting perceptual and output stages of spatial processing.19–23 Some USN individuals are affected by a perceptual bias reflecting lateralized impairments in spatial representation/attention. However, in other individuals, USN reflects a “reluctance” to orient the response contralesionally.19,24 This type of neglect that has been called directional hypokinesia or intentional neglect,25,26 response bias19,20 or premotor neglect24 is rarely assessed, likely because it can only be detected by using few specific tasks, the most well-known being the landmark task.19,21 Another symptom affecting output stages of stimulus processing is motor neglect, whereby a dramatic reduction in the spontaneous use of contralesional limbs is not explained by motor impairment.27 Finally, not only the type of task18 but also task demands28–31 have been found to affect neglect severity.
Given the complexity of USN symptomatology, there is the need to use comprehensive assessment tools that minimize the risk to overlook its presence. The most reliable and commonly used assessment tests are two “paper and pencil” tasks: the line bisection32 and cancellation28 tasks. On these tasks, individuals with USN are asked to bisect a horizontal line or to search for spatially distributed targets. They mark the center of the line ipsilesionally and/or search exclusively for ipsilesional targets. Administration of both tasks is critical because USN can dissociate across them.18 Furthermore, other variables need to be kept into account when using these tasks. For example, line bisection performance is affected by the length of the line and by contextual factors.32 Lines of at least 18 or 20 degree of visual angle are necessary to reliably assess neglect. Short lines and very short lines produce a contralesional bisection bias that may even overshoot the end of the line (i.e., the crossover effect;32 see also Chatterjee et al33 for crossover effects in non-spatial tasks). Cancellation tasks are significantly affected by stimuli characteristics34 and task demands.29,30 USN tests or batteries (e.g., the Behavioral Inattention Test35) often include also reading, copying and drawing tasks. In all these tests, individuals with USN omit (or may also “confabulate”) contents of contralesional space. However, canonical tests may not be sensitive enough to detect contralesional space disorders in subacute and chronic stages of the disease and more appropriate (and demanding) tasks are necessary to reveal their presence.30,36 For example, computerized methods may be more effective in detecting subtle symptoms than static paper-and-pencil tests.22,37–41 In addition, conventional evaluation tests might not provide conditions consistent with real-life situations.
An accurate diagnosis of the specific symptoms that affect individuals with USN is fundamental to design tailored rehabilitation programs that may effectively overcome the limits posited by disrupted spatial awareness to functional recovery.
Theoretical Models
USN is not caused by elementary sensory or motor deficits and dissociates from deficits of intermediate vision.22,42–44 It is thought to derive from disruption of higher level spatial attention/representational processes.7,8 Attentional theories propose that USN is accounted for by a rightward lateralized bias in the orientation of spatial attention. Kinsbourne’s hemispheric rivalry account45 posits mutual transcallosal inhibition between hemispheres in the normal brain and disruption of this balance in USN. It assumes the existence of two antagonist attentional vectors directed by each hemisphere toward the contralateral hemispace. In physiological conditions, the left-hemisphere vector is stronger than the right-hemisphere one. A brain lesion would disrupt interhemispheric balance and symptoms would be explained not only by the inactivity of the lesioned area but also by the increased activity of homologous regions of the opposite hemisphere that are released by contralateral inhibition. Given the asymmetric strength of the attentional vectors, only a right-hemisphere lesion would produce a dramatic, lateralized ipsilateral bias in attentional orienting. Heilman and colleagues8 propose a complementary model, according to which the right hemisphere would direct attention to both hemispaces, while the left hemisphere exclusively to the right one. As a consequence, a right-hemisphere lesion would more frequently cause USN.8 Representational accounts of neglect instead propose that USN is a disorder of mental space representation,46 consisting in a left–right pathological anisometry of the medium for space representation: the left-side would be more relaxed and the right-side would be more contracted/compacted.46 The contralesional relaxation of the medium might still sustain “conscious” representation of contents in space, albeit with a horizontal size distortion. Beyond a critical point, the overrelaxed medium no longer sustains conscious representations. Bisiach’s theory46 also foresees that in some individuals, the disorder affects response level of stimulus processing (i.e., response bias). Another account referring to altered mechanisms of space representations is the transformational hypothesis.47,48 It suggests that USN is due to a failure of the transformation of sensory input into motor output, which is generally based on different reference frames. Since such coordinate transformation mainly occurs in the parietal cortex,49,50 a parietal lesion might impair this process.47 As a result, the egocentric representation of the surrounding environment would be deflected towards the ipsilesional side.
Neural Correlates
Early clinical observations pointed to damage to the right posterior parietal cortex (PPC), as the most likely correlate of USN symptoms.51 Anatomo-clinical correlation studies, based on CT or MRI, confirm a predominant role of the right inferior parietal lobule in association with USN symptoms,52,53 particularly of the angular gyrus (AG). Other findings suggest the right superior temporal gyrus (STG) as the main neural correlate for USN symptoms.54 Finally, USN is also observed after lesions to frontal and subcortical structures that are functionally connected to the posterior parietal lobe.55 Recently, neuroscientists have shifted their interest from trying to identify a single brain area to investigations of brain areas that are involved as sub-components of a more complex network, responsible for space attention and representation (see Hillis et al55 for a review). Studies using advanced neuroimaging techniques have concluded that USN symptoms heterogeneity can be explained by differences in the structures or circuit affected by the lesion. For instance, using PWI and DWI, Medina and colleagues56 found that functional inactivation of the right-supramarginal gyrus was most predictive of egocentric neglect, inactivation of posterior inferior temporal and lateral occipital areas was most predictive of stimulus-centered neglect, and, posterior middle/inferior temporal regions of object-centered neglect. Damage to intraparietal sulcus (IPS) and the temporoparietal junction (TPJ) have been further associated with egocentric and allocentric neglect, respectively.57 Finally, motor-intentional USN correlates to lesions of basal ganglia.19,23 Breakdown of functional connectivity between parietal and frontal regions linked by the superior longitudinal fasciculus (SLF) has been shown to play a critical role in the occurrence, severity and chronicity of egocentric USN symptoms.2,57–62
Rehabilitation Methods
It is possible to distinguish between two types of neglect treatments: top-down and bottom-up approaches.63 The main difference between them concerns the extent of an individual’s awareness and active involvement. The former approach aims to improve perceptual and behavioural bias by acting on disrupted awareness, thus on higher-level cognitive processes. Given USN features, this approach might be difficult to be applied in individuals with severe neglect. The latter is a physiological approach that aims to affect the sensory-motor level through passive sensorial manipulations or visuomotor adaptation. In this way, it is possible to override central awareness deficit and reach higher cognitive levels of spatial and action representation.64 Given that USN is a disorder of spatial awareness, bottom-up approaches have more frequently been proposed and investigated.
The most widely used top-down approach is visual scanning training (VST), during which the therapist encourages individuals to pay attention to and explore portions of space contralateral to the brain lesion. The standard procedure consists of different training tasks, such as visual search, digit detection, figure copying, picture exploring, reading and writing. The exploratory behaviour of contralesional contents of space is systematically strengthened by visual and verbal reinforcements, as well as compensatory strategies. Despite a wide variability of response to VST, overall, significant improvement of neglect has been reported following this intervention65 (for a review see Luauté et al66). Some studies, comparing the efficacy of VST to that of bottom-up approaches, did not find any significant difference between them.67–69 Nonetheless, some RCT and single-case studies suggest that VST beneficial effects might be enhanced by the combination of this intervention with other techniques, such as, for example, left-hand somatosensory stimulation,70 limb activation71 or transcranial Direct Current Stimulation.72
Over the years, a number of different techniques have been proposed to rehabilitate neglect symptoms. A large number of studies have been published for each approach. Since this is not a systematic review of neglect treatments, we will focus on the most promising recently proposed rehabilitation methods, although other effective – but less employed – techniques have been investigated to treat the disorder, such as eye-patching,73 caloric vestibular stimulation,74 visuomotor imagery,75 mirror therapy,76 TENS,77 Optokinetic Stimulation78–80 and the Constraint-induced movement therapy.81,82 Specifically, we conducted a MEDLINE literature research on the use of prismatic adaptation, non-invasive brain stimulation and virtual reality in USN rehabilitation. To this end, we used the following combinations of words: “neglect”, “rehabilitation”, “prism adaptation”, “tDCS”, “galvanic vestibular stimulation”, “TMS”, “TBS”, “Virtual reality”. Reference lists from identified articles were also reviewed. Studies were selected according to the following exclusion criteria: nonintervention studies; theoretical, descriptive, or review papers; papers without adequate specification of interventions; subjects other than persons with stroke and USN; non-English language papers. The identified studies were classified according to the strength of their methods based on Cicerone et al83 recommendations. Specifically, three main levels of evidence were established. Studies were considered Class I evidence if they had well-designed, prospective, randomized controlled trials. Prospective studies with “quasi-randomized” assignment to treatment conditions were designed as Class Ia studies. Class II studies comprised prospective nonrandomized cohort studies, retrospective, nonrandomized case–control studies, or clinical series with well-designed controls (eg, multiple baseline across subjects). Studies were considered as Class III evidence if they consisted of clinical series without concurrent controls, or single-case studies with appropriate single-subject methods. All classifications were based on the agreement of at least two authors. The disagreement between reviewers was resolved by the evaluation of a third author.
Prismatic Adaptation
Prismatic Adaptation (PA) is one of the most widely studied and used bottom-up procedure for USN rehabilitation. Since the literature on this topic is very extensive and several reviews on this procedure have been published, here, we will present a non-exhaustive overview of recent relevant studies on PA for the treatment of USN (see Table 1). Standard PA procedure foresees that subjects wear the prismatic goggles, producing a visual shift, and perform different tasks to reach visual targets (e.g., pointing, reaching or throwing). These tasks are initially failed because of the deviation caused by the shift of the visual field that generates a mismatch between the perceptive object position and the arm movement trajectory. After a series of trials with visual feedback, the subjects adapt to optical displacement, improving their performance. After removing the prisms, movement trajectory deviates in the direction opposite to the visual shift, indicating a negative aftereffect. PA effects have been initially interpreted as due to a correction of the biased egocentric representation, in line with the transformational hypothesis. However, some studies suggested that PA may mainly affect motor-intentional “aiming” (response) neglect rather than perceptual levels of space representation.84 Finally, some authors proposed that PA improves spatial cognition by inhibiting the PPC contralateral to the prismatic deviation, restoring, as a result, interhemispheric balance,85,86 in line with USN rivalry account.45 Although it is not clear yet the exact nature of the mechanisms underlying beneficial effects of PA in USN, this non-invasive procedure has showed its effectiveness in several studies and therefore researchers are currently exploring its potentials. For example, single rightward-PA sessions can improve USN from 2 hrs87 to few days.85,88 Likewise, two daily sessions of PA-treatment for 2 weeks may produce beneficial effects persisting for 1 to 6 months.63,89 Although several Randomized Control Trials (RCTs) have been published, the evidence supporting a systematic efficacy of PA for neglect rehabilitation is still controversial. For example, three studies reported a significant improvement in 51 individuals with USN treated by PA compared to a placebo control group, both in standard neglect tests90,91 and in functional independence measures.92 Positive outcomes were also observed in studies comparing PA to VST, whereby the effectiveness of both approaches was found.67,69 However, mixed results have been reported in a brain-damaged woman suffering from USN who showed amelioration soon after 4 days of PA treatment,93 but not after 1 month at follow-up. Moreover, no beneficial effects by PA were observed in four RCT-studies treating overall 72 individuals affected by USN.94–97 A possible explanation of negative findings might be that visuomotor adaptation (ie, aftereffect) has to reach a critical threshold to affect performance in other tasks.98 Given the high intra- and interindividual variability of individuals with USN, visuomotor adaptation induced by low power prisms (i.e., shifting the visual field of 5°, 6° or 10°) – as those used in RCT studies that did not find any beneficial outcomes after PA94–97 – might be too small to produce detectable effects in all patients. The fact that the critical threshold can only be reached with prisms of high power (i.e., shifting the visual field of 10° or 12°, as those used in the above studies that found significant PA effects) might explain some negative findings. Another suggestive possibility is that, as demonstrated by Fortis and collaborators,84 PA is more effective when USN affects response level of stimulus processing. However, with the exception of few investigations,67,84 studies on PA never disentangle the two components of USN, not making possible to understand whether PA efficacy may depend on the stage (input vs output) affected by the lesion. Future investigations on PA rehabilitation (but also on other types of interventions) need to provide information on whether USN occurs at perceptual or response stages of stimulus processing. Besides the power of prismatic goggle also this variable might explain the heterogeneity of findings. In general, tailoring PA treatment to specific forms of USN may result in a more successful rate of improvement. As shown in Table 1, on the basis of Cicerone et al83 classification, 9 out of 16 of selected works on PA were classified as class I (or Ia) studies.
 | 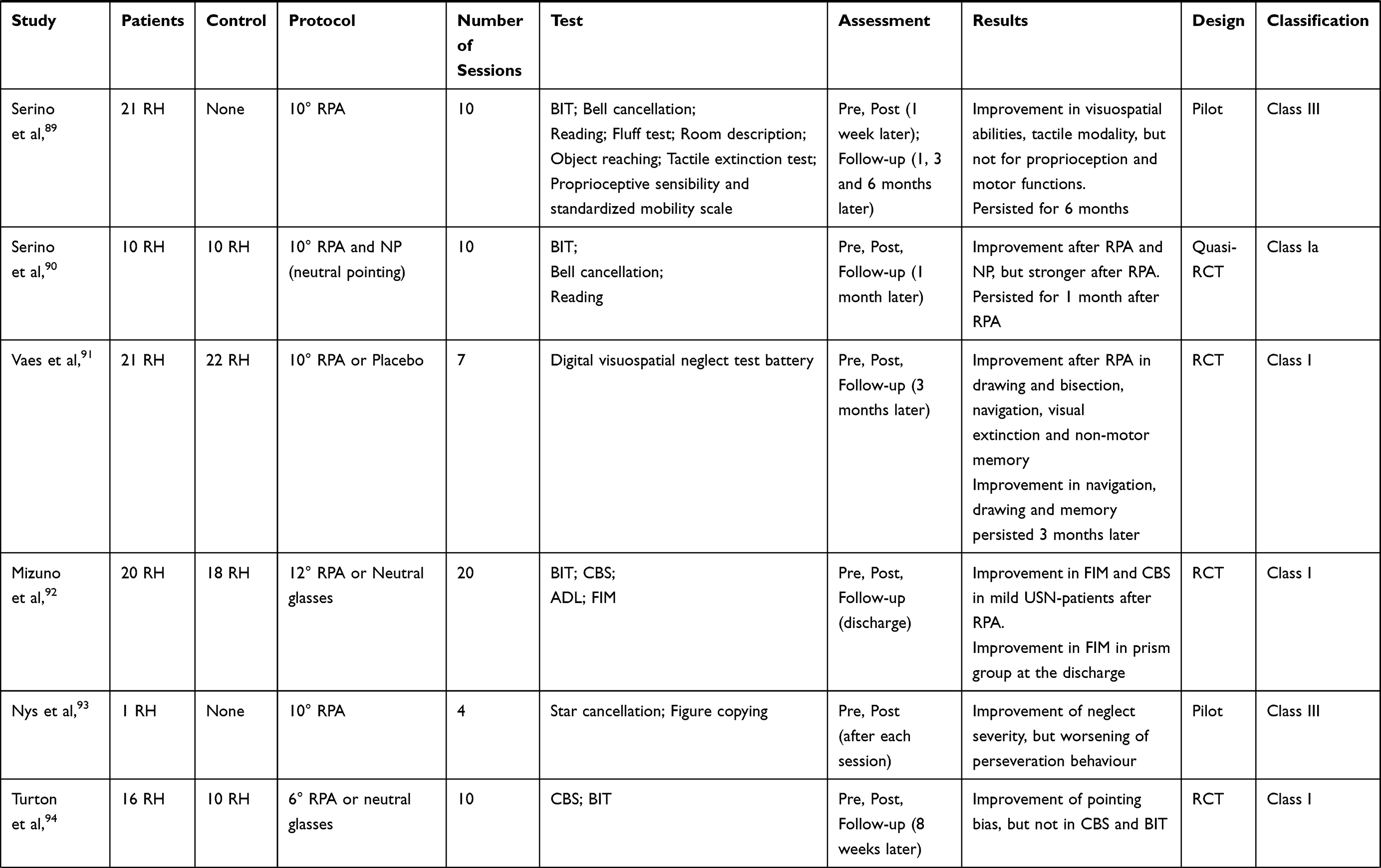 | 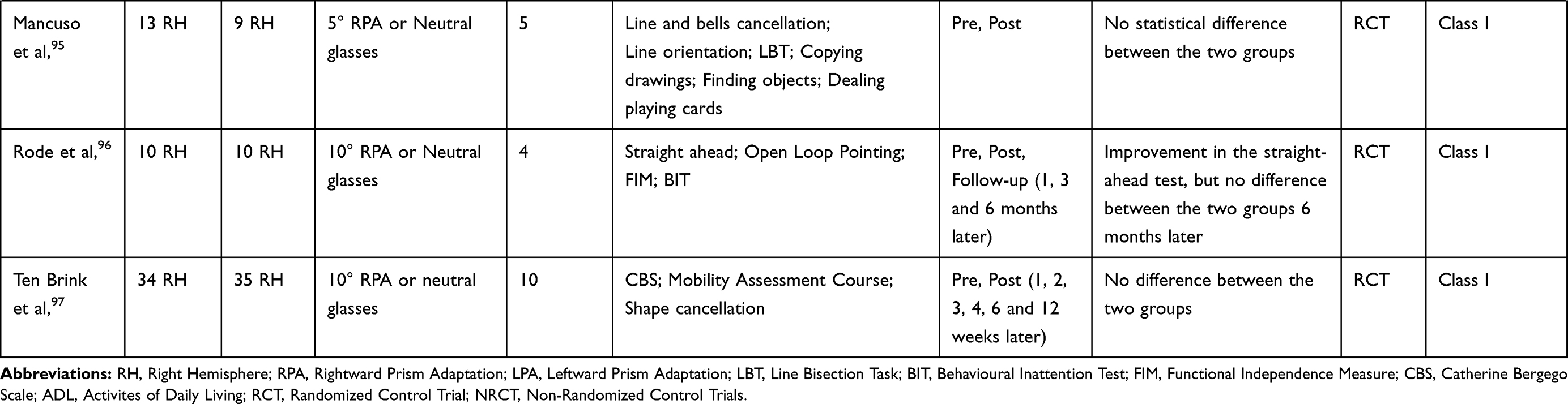 |
Table 1 Prism Adaptation Studies |
Non-Invasive Brain Stimulation
NIBS may be effective in ameliorating cognitive and motor disorders in individuals affected by stroke99,100 or by other neurological disorders.101–103 The first attempts to treat neuropsychological symptoms using NIBS were made in individuals with USN.104,105 In line with the hemispheric rivalry account of neglect,45 according to which symptoms are not solely due to inactivity of the lesioned area, but also to increased activity of homologous regions of the opposite hemisphere, therapeutic effects in USN are typically obtained by down-regulating the PPC of the intact hemisphere and/or up-regulating the PPC of the affected hemisphere. It is worth noticing that the first NIBS studies for USN rehabilitation have been published less than 20 years ago. In Tables 2 and 3 are reported studies investigating the efficacy of different Non-Invasive Brain Stimulation (NIBS) techniques and protocols for the treatment of USN. The number and quality of studies reported in these Tables index a fast-growing interest and literature on this topic.
 | 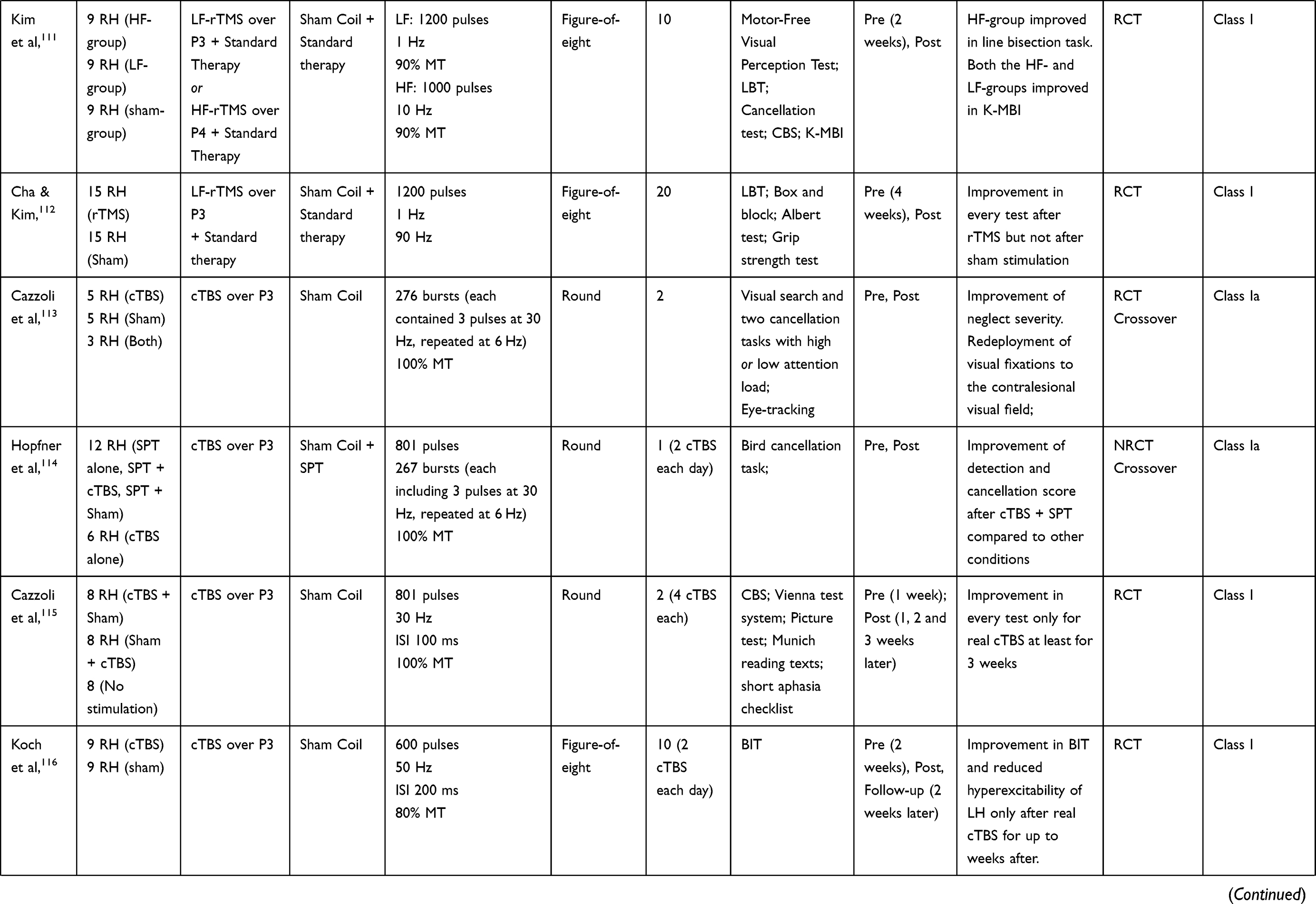 |  |
Table 2 TMS Studies |
 | 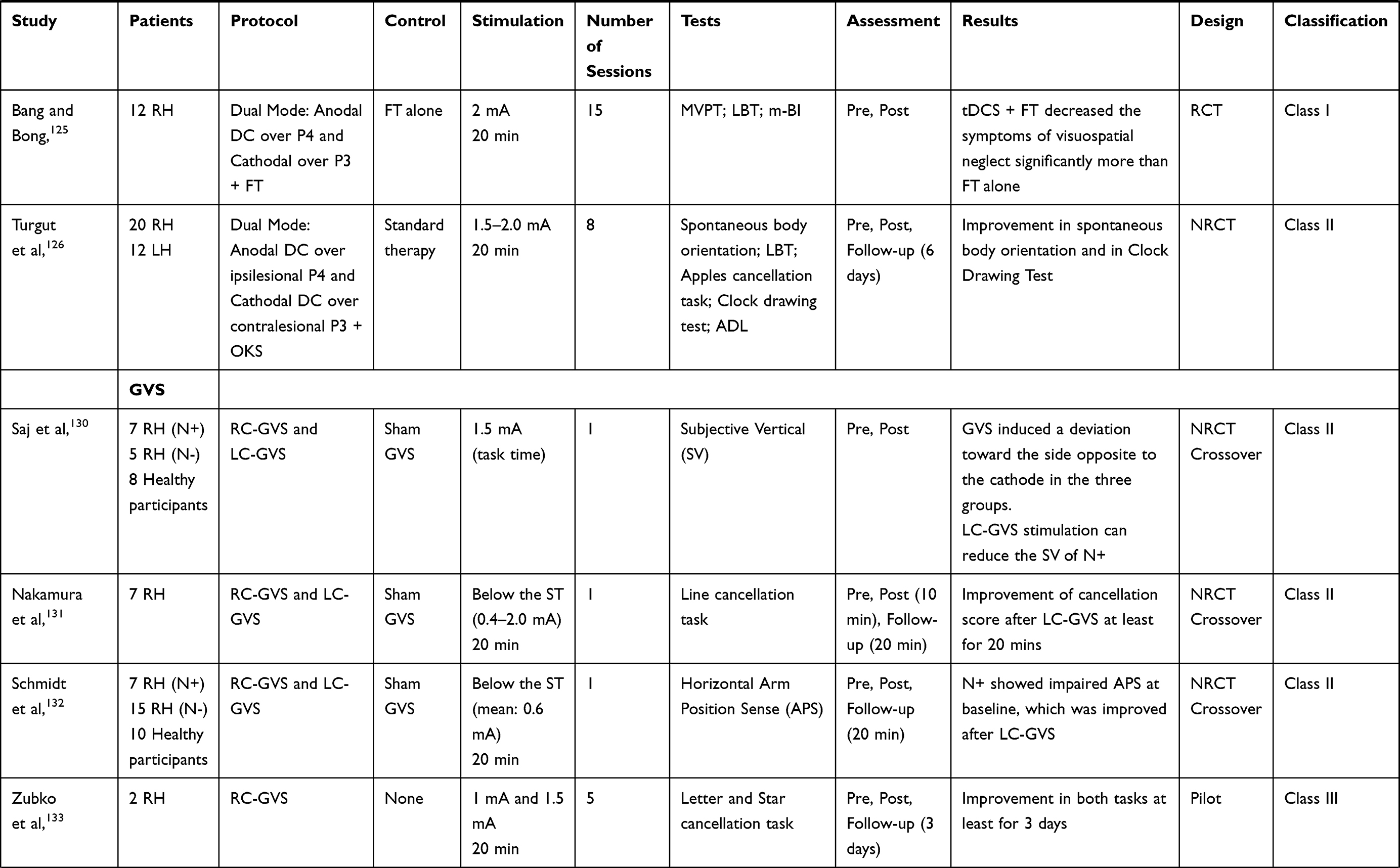 | 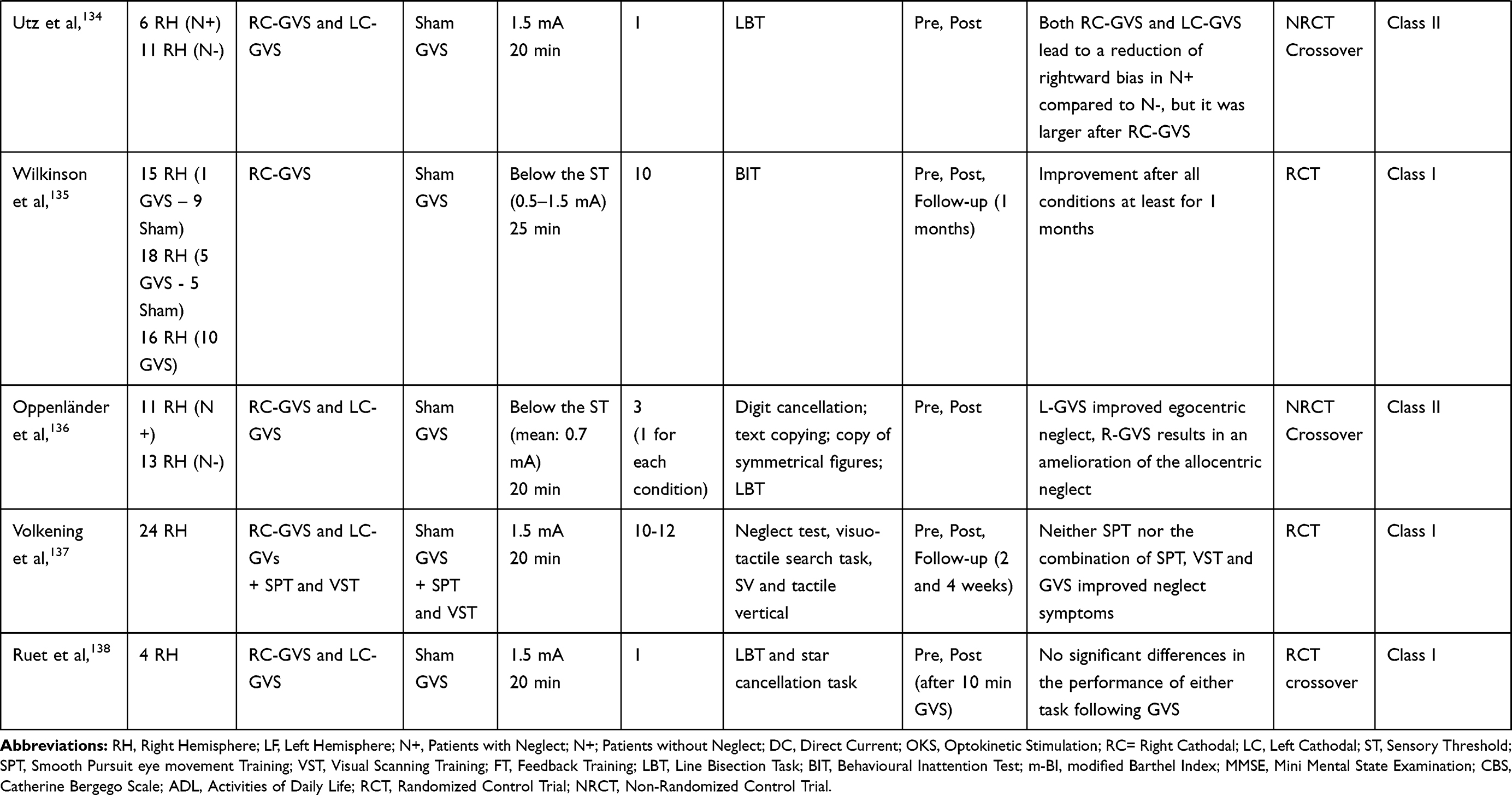 |
Table 3 tDCS and GVS Studies |
Transcranial Magnetic Stimulation (TMS)
In a proof of concept study, Brighina and collaborators were the first to apply a low-frequency (1 Hz) rTMS treatment (seven sessions over 2 weeks) to the healthy hemisphere of three individuals suffering from visuospatial neglect.104 Participants showed significant improvement on different tasks (landmark, line bisection, clock drawing) lasting up to 15 days from the intervention. Subsequent pilot105–108 and NRCT studies110 administering low-frequency rTMS to the left-hemisphere in small groups of individuals with left USN confirmed and extended preliminary findings. Furthermore, two RCT-studies corroborated the above outcomes.111,112 In recent years, researchers have also successfully applied inhibitory continuous Theta Burst Stimulation (cTBS) to the healthy hemisphere of individuals with USN in NRCT,113,114 as well as in RCT-studies115–118 observing long-lasting improved performance. Interestingly, Yang and colleagues119 conducted a RCT study to compare behavioural and brain plasticity effects in USN individuals undergoing low-frequency rTMS, high-frequency rTMS, or cTBS. The cTBS group exhibited the best outcome at 1 month after the end of treatments, followed by the low-frequency and high-frequency group. Interestingly, DTI evaluation showed a connectivity enhancement of the white matter tract network related to visual attention in the cTBS group.119 Table 2 reports TMS studies of USN treatments. On the basis of Cicerone et al83 classification, 50% of these studies (8 out of 16) were scored as high-quality studies (class I or Ia).
Transcranial Direct Current Stimulation (tDCS)
Only a few studies have been conducted using tDCS in the context of USN. Preliminary works administering a single session of excitatory stimulation (ie, anodal or a-tDCS) to the affected hemisphere120,121 or inhibitory stimulation (ie, cathodal or c-tDCS) to the intact one120 showed improved performance on line bisection and cancellation/visual search tasks. In a double-blind randomized cross-over study, Sunwoo and colleagues,122 comparing the effects of a dual-mode protocol (ie, a-tDCS of the affected hemisphere and c-tDCS of the intact hemisphere concurrently) to those of single-mode a-tDCS of the affected hemisphere, found that both single- and dual-mode tDCS were safe and effective for USN rehabilitation. Another double-blind, single-case, cross-over study,72 using a combined approach of biparietal tDCS (the anode was applied to the right PPC and the cathode to the left PPC) and cognitive training, showed greater USN improvement when using biparietal tDCS than standard therapy alone or sham. Beneficial effects were still observed at 3 months after treatment. However, a subsequent placebo-controlled study123 did not find any long-term USN improvement after parietal right-anodal and left-cathodal-tDCS of PPC. To our knowledge, only two studies used RCT designs. Yi and colleagues124 applied a-tDCS to the right-PPC and c-tDCS to the left-PPC and found beneficial effects on left-USN compared to sham-stimulation. The same protocol was applied by Bang & Bong125 in combination with Feedback Training (FT). Results showed greater improvement of symptoms after tDCS combined with FT than FT alone. In a recent NRCT study, Turgut and collaborators126 compared the efficacy of biparietal tDCS combined with optokinetic stimulation (eight sessions over 2 weeks) to that of a standard cognitive training, in 10 individuals with LHL and 6 with RHL suffering from USN. The authors showed greater efficacy of tDCS compared to standard treatment. Interestingly, RHL-participants showed improvement of allocentric symptoms, while the ones with LHL improved their egocentric symptoms. Findings from this study indicate that differences between egocentric and allocentric symptoms need to be considered in future brain stimulation studies. As shown in Table 3, 5 out of 8 tDCS studies provide class I (or Ia) evidence.83
Galvanic vestibular stimulation (GVS) is a variant of tDCS that consists in applying a weak direct percutaneous current through an anode and a cathode positioned over the right and the left mastoids. Cathodal currents induce an increase and anodal currents a decrease in the firing rate of the vestibular nerve.127–129 Some NRCT-studies applying R-GVS (ie, right anodal/left cathodal stimulation) showed beneficial effects on perceptual130,131 and arm-position symptoms132 of neglect. On the contrary, in other pilots,133 NRCT-134 and RCT-studies,135 L-GVS (ie, left anodal/right cathodal stimulation) has been found to ameliorate USN and the effects persist up to a month when stimulation was applied for several (10) sessions.135 A recent NRCT-study tested repetitive-GVS in right-brain-damaged people with neglect syndrome, by comparing the effects of R-GVS, L-GVS and sham stimulation.136 While previous studies showed vestibular stimulation effects on egocentric spatial neglect symptoms, authors interestingly reported that L-GVS significantly improved egocentric neglect (assessed by line bisection and text copying task) whereas R-GVS results in amelioration of allocentric neglect (evaluated by figure copying and digit cancellation tasks). However, two recent RCT-studies, using repeated sessions of stimulations (10–12 sessions)137 did not observe any post-treatment effects by GVS on neglect symptomatology.137,138 Future studies are necessary to better understand the specific influence of GVS on disorders of spatial awareness and its potential in neglect rehabilitation. As shown in Table 3, only 3 out of 9 studies were classified as class I investigations.
Virtual Reality
Computerized methods may provide a proper alternative approach to standard methods not only for the assessment but also for the rehabilitation of neglect.39 One of the most advanced tools recently implemented in clinical treatments is Virtual Reality (VR). In Table 4 are reported the most significant or recent studies on the use of VR for USN treatment. The VR can simulate relevant situations of everyday life and the possibility to control for head, eyes and limbs movements or postural shifts, provide a key feature for an optimal research setting.41 To our knowledge, the only RCT-study using VR on USN-rehabilitation was conducted by Kim and colleagues.139 Twelve people suffering from USN were asked to accomplish the following three tasks: 1) “Bird and Ball”, where they had to touch flying balls to turn them into a bird; 2) “Coconut”, where they had to grab a coconut falling down from a tree; and 3) the “Container”, where they had to relocate an object from one side to the other. The authors compared the outcomes of the experimental group to those of a control group undergoing standard training. Treatments were administered for 15 days over 3 weeks. Although both groups showed improvement after intervention, the VR-group had higher scores in star cancellation test and the Catherine Bergego Scale compared to controls. Another contribution to the use of VR in neglect rehabilitation is a single case study using the “Duckneglect” platform,140 in which the participant was asked to reach various targets in conditions requiring different levels of difficulty. The virtual environment was arranged in ecological settings representing everyday life situations. Authors administered the videogame-like task to a man affected by neglect, 5 days a week for a month. Results showed improvement of neglect on several standard evaluations and in daily-life activities persisting up to 5 months. A third low-cost VR-system for training street-crossing was validated by Navarro and colleagues.141 Fifteen USN individuals were recruited and compared to 17 post-stroke individuals without USN and 15 healthy participants. Interestingly, results showed that USN-group had more difficulties crossing the street avoiding accidents than the non-USN control group and healthy controls. Furthermore, a correlation between the scores of standard neuropsychological tests and those of the virtual street-crossing system was observed, suggesting the potential of the VR approach for USN rehabilitation. Another novel VR-training method is the RehAtt.142 The software consisted in visual scanning training with multi-sensory stimulation in a VR-environment. Fifteen post-stroke individuals suffering from chronic neglect were trained for 15 sessions over 5 weeks. Results showed that the VR-training improved visuospatial deficits and activities of daily living.142 Interestingly, 2 years later, authors used fMRI to evaluate changes in brain activity during Posner′s Cueing Task after RehAtt™ rehabilitation. The amelioration of neglect symptoms was associated with increased brain activity in the pre‐frontal and temporal cortex during attentional cueing,143 suggesting enhancement of top-down strategies, and increased inter-hemispheric resting-state functional connectivity of the dorsal attentional network.144 A final promising protocol was tested in a single-blind dose–response study in healthy subjects, by using VR as an alternative to real prisms.98 Authors progressively induced a displacement of the visual field following the virtual PA procedure, making difficult for the subject to become aware of the experimental manipulation. Results showed that large rightward deviations may affect sensorimotor performance in healthy participants similarly to neglect patients without generating discomfort linked to the large visual shift. However, results need to be replicated in stroke individuals with USN. Taken together, these studies suggest that VR-systems may represent a suitable alternative to standard rehabilitation techniques. By involving multisensory online feedbacks in real-like situations, virtual approaches may provide novel powerful tools for neglect rehabilitation.145 As shown in Table 4, only one out of five studies was classified as class I investigation. However, VR is one of the most recent and innovative approaches of USN rehabilitation and, up to now, its potentials have been only minimally explored.
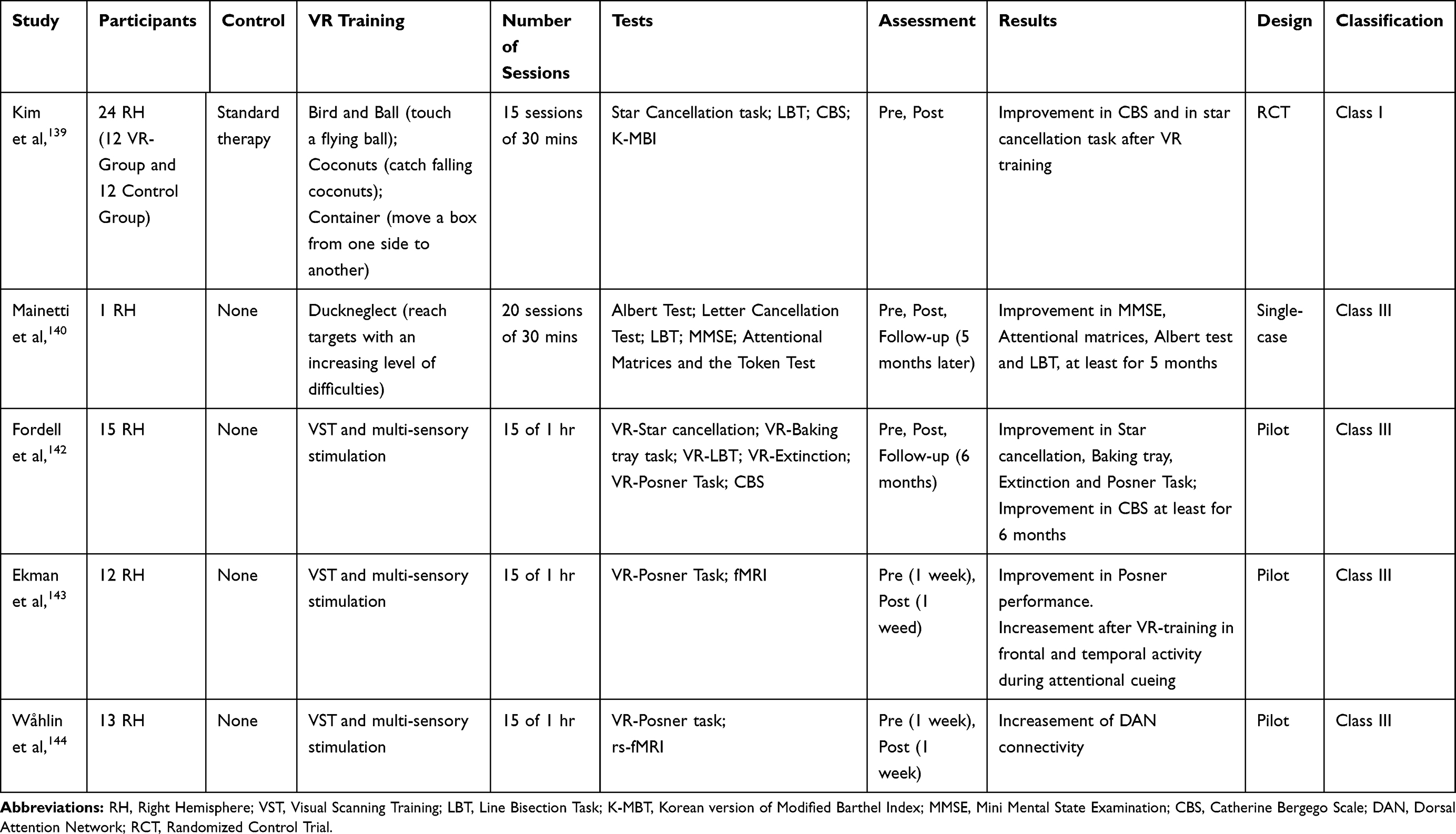 |
Table 4 Virtual Reality (VR) Studies |
Conclusions and Future Directions
Investigations of USN have provided most of the knowledge we currently have on the neural mechanisms of spatial attention and representation and their interaction with the response system. Nonetheless, correlating brain lesion localization with behavioral impairment presents a series of limitations (i.e., the extent of natural lesions which often involve more than one structure, the effects of the diaschisis and brain reorganization). Moreover, individuals’ clinical and cognitive conditions may posit practical constraints on recruitment and testing. In the last 20 years, cognitive neuroscientists have used TMS to induce neglect-like behaviors in healthy volunteers and overcome the above limits. These studies have disentangled previous controversies on neglect neuroanatomy, confirming a causal role of the right PPC in visuospatial attention during performance of stimulus detection146 and line bisection/landmark 60,147–153 tasks, and a role of superior temporal cortex in the performance of visual conjunction search task.18 These findings, in line with the observation that USN may dissociate across tasks, further highlight the importance of using diverse types of assessment tools to reliable evaluate neglect symptomatology for both clinical and experimental purposes. Consistent with recent studies on neglect neuroanatomy,58,154 single-pulse TMS applied to the right PPC inside the scanner, shows that neglect-like bias on the landmark task is associated with decreased activity of right parieto-frontal areas corresponding to those connected by SLFII.60 In contrast to the rivalry account of USN45 and in line with Heilmann’s hypothesis,8 these TMS/fMRI findings also show decreased activity of contralateral PPC (see Bagattini et al155 for similar findings), suggesting that unbalanced inter-hemispheric activity might worsen neglect symptomatology but not be necessary for its emergence. Future TMS and neuroimaging studies in the healthy brain may help to clarify the nature of neglect symptoms and the possibilities offered by brain stimulation, PA and other techniques to modulate them. As described in the present paper, high-quality studies have already demonstrated the efficacy of PA, TMS and tDCS interventions for the treatment of USN. In addition, preliminary investigations are suggesting the potentials of GVS and VR approaches for UNS rehabilitation. However, optimal protocols for USN rehabilitation still need to be defined.
To sum up, the application of advanced neuroimaging and brain stimulation techniques in healthy individuals and in individuals with USN may help to overcome parts of the limits posit by classical neuropsychological studies. On the other hand, only high-quality neuropsychological investigations of individuals with USN may provide unique insights into the syndrome and, consequently, into the mechanisms underpinning conscious space representations in the healthy brain.
Disclosure
The authors declare no conflicts of interest.
References
1. Bisiach E. Unilateral neglect and related disorders. In: Denes G, editor. Handbook of Clinical and Experimental Neuropsychology. Hove, East Sussex: Psychology Press; 1999:479–496.
2. Corbetta M, Kincade M, Lewis C, Snyder AZ, Sapir A. Neural basis and recovery of spatial attention deficits in spatial neglect. Nat Neurosci. 2005;8:1603–1610. doi:10.1038/nn1574
3. Ringman JM, Saver JL, Woolson RF, Clarke W, Adams JH. Frequency, risk factors, anatomy, and course of unilateral neglect in an acute stroke cohort. Neurology. 2004;63(3):468–474. doi:10.1212/01.WNL.0000133011.10689.CE.
4. Di Monaco M, Schintu S, Dotta M, Barba S, Tappero R, Gindri P. Severity of unilateral spatial neglect is an independent predictor of functional outcome after acute inpatient rehabilitation in individuals with right hemispheric stroke. Arch Phys Med Rehabil. 2011;92(8):1250–1256. doi:10.1016/j.apmr.2011.03.018
5. Czernuszenko A, Członkowska A. Risk factors for falls in stroke patients during inpatient rehabilitation. Clin Rehabil. 2009;23(2):176–188. doi:10.1177/0269215508098894
6. Nijboer T, van de Port I, Schepers V, Post M, Visser-Meily A. Predicting functional outcome after stroke: the influence of neglect on basic activities in daily living. Front Hum Neurosci. 2013;7:182. doi:10.3389/fnhum.2013.00182
7. Bisiach E, Berti A. Consciousness in dyschiria. In: Gazzniga M, editor. The Cognitive Neurosciences. MIT Press; 1995.
8. Heilman KM, Valenstein E, Watson RT. Neglect and related disorders. Semin Neurol. 2000;20(4):463–470. doi:10.1055/s-2000-13179
9. Jacobs S, Brozzoli C, Farnè A. Neglect: a multisensory deficit? Neuropsychologia. 2012;50(6):1029–1044. doi:10.1016/j.neuropsychologia.2012.03.018
10. Berti A, Frassinetti F. When Far Becomes Near: remapping of Space. J Cogn Neurosci. 2000;12(3):415–420. doi:10.1162/089892900562237
11. Neppi-Modona M, Rabuffetti M, Folegatti A, Ricci R, Berti A. Bisecting lines with different tools in right brain damaged patients: the role of action programming and sensory feedback in modulating spatial remapping. Cortex. 2007;43:397–410. doi:10.1016/S0010-9452(08)70465-9
12. Aimola L, Schindler I, Simone AM, Venneri A. Near and far space neglect: task sensitivity and anatomical substrates. Neuropsychologia. 2012;50(6):1115–1123. doi:10.1016/j.neuropsychologia.2012.01.022
13. Karnath HO, Rorden C. The anatomy of spatial neglect. Neuropsychologia. 2012;50(6):1010–1017. doi:10.1016/j.neuropsychologia.2011.06.027
14. Spaccavento S, Cellamare F, Falcone R, Loverre A, Nardulli R. Effect of subtypes of neglect on functional outcome in stroke patients. Ann Phys Rehabil Med. 2017;60(6):376–381. doi:10.1016/j.rehab.2017.07.245
15. Caggiano P, Jehkonen M. The ‘Neglected’ personal neglect. Neuropsychol Rev. 2018;28(4):417–435. doi:10.1007/s11065-018-9394-4
16. Chatterjee A. Picturing unilateral spatial neglect: viewer versus object centred reference frames. J Neurol Neurosurg Psychiatry. 1994;57(10):1236–1240. doi:10.1136/jnnp.57.10.1236
17. Marsh EB, Hillis AE. Dissociation between egocentric and allocentric visuospatial and tactile neglect in acute stroke. Cortex. 2008;44(9):1215–1220. doi:10.1016/j.cortex.2006.02.002
18. Ellison A, Schindler I, Pattison LL, Kinsbourne AD. An exploration of the role of the superior temporal gyrus in visual search and spatial perception using TMS. Brain. 2004;127(10):2307–2315. doi:10.1093/brain/awh244
19. Bisiach E, Ricci R, Lualdi M, Colombo MR. Perceptual and response bias in unilateral neglect. Brain Cogn. 1998;37(3):369–386. doi:10.1006/brcg.1998.1003
20. Bisiach E, Ricci R, Berruti G, Genero R, Pepi R, Fumelli T. Two-dimensional distortion of space representation in unilateral neglect: perceptual and response-related factors. Neuropsychologia. 1999;37:1491–1498. doi:10.1016/S0028-3932(99)00046-9
21. Milner AD, Harvey M, Roberts RC, Forster SV. Line bisection errors in visual neglect: misguided action or size distortion? Neuropsychologia. 1993;31:39–49. doi:10.1016/0028-3932%2893%2990079-F
22. Ricci R, Chatterjee A. Sensory and response contributions to visual awareness in extinction. Exp Brain Res. 2004;157(1):85–93. doi:10.1007/s00221-003-1823-8
23. Vossel S, Eschenbeck P, Weiss PH, Fink GR. The neural basis of perceptual bias and response bias in the Landmark task. Neuropsychologia. 2010;48(13):3949–3954. doi:10.1016/j.neuropsychologia.2010.09.022
24. Saevarsson S, Eger S, Gutierrez-Herrera M. Neglected premotor neglect. Front Hum Neurosci. 2014;8(October):8–11. doi:10.3389/fnhum.2014.00778
25. Watson RT, Miller BD, Heilman KM. Nonsensory neglect. Ann Neurol. 1978;3(6):505–508. doi:10.1002/ana.410030609
26. Heilman KM, Bowers D, Coslett HB, Whelan H, Watson RT. Directional hypokinesia: prolonged reaction times for leftward movements in patients with right hemisphere lesions and neglect. Neurology. 1985;35(6):855–859. doi:10.1212/WNL.35.6.855
27. Sampanis DS, Riddoch J. Motor Neglect and Future Directions for Research. Front Hum Neurosci. 2013;7(March):1–2. doi:10.3389/fnhum.2013.00110
28. Chatterjee A, Mennemeier M, Heilman KM. A stimulus-response relationship in unilateral neglect: the power function. Neuropsychologia. 1992;30(12):1101–1108. doi:10.1016/0028-3932(92)90101-Q
29. Sarri M, Greenwood R, Kalra L, Driver J. Task-related modulation of visual neglect in cancellation tasks. Neuropsychologia. 2009;47(1):91–103. doi:10.1016/j.neuropsychologia.2008.08.020
30. Ricci R, Salatino A, Garbarini F, et al. Effects of attentional and cognitive variables on unilateral spatial neglect. Neuropsychologia. 2016;92:158–166. doi:10.1016/j.neuropsychologia.2016.05.004
31. Blini E, Tilikete C, Farnè A, Hadj-Bouziane F. Probing the role of the vestibular system in motivation and reward-based attention. Cortex. 2018;103:82–99. doi:10.1016/j.cortex.2018.02.009
32. Ricci R, Chatterjee A. Context and crossover in unilateral neglect. Neuropsychologia. 2001;39(11):1138–1143. doi:10.1016/S0028-3932%2801%2900054-9
33. Chatterjee A, Ricci R, Calhoun J. Weighing the evidence for cross over in neglect. Neuropsychologia. 2000;38:1390–1397. doi:10.1016/S0028-3932%2800%2900042-7
34. Chatterjee A, Thompson KA, Ricci R. Quantitative analysis of cancellation tasks in neglect. Cortex. 1999;35:253–262. doi:10.1016/S0010-9452%2808%2970798-6
35. Wilson BM, Cockburn J, Halligan P. Development of a behavioral test of visuospatial neglect. Arch Phys Med Rehabil. 1987;68(2):98–102.
36. Ricci R, Salatino A, Caldano M, et al. Phantom touch: how to unmask sensory unawareness after stroke. Cortex. 2019;121:253–263. doi:10.1016/j.cortex.2019.08.021
37. Ricci R, Genero R, Colombatti S, Zampieri D, Chatterjee A. Visuomotor links in awareness: evidence from extinction. Neuroreport. 2005;16(8):843–847. doi:10.1097/00001756-200505310-00013
38. Rengachary J, d’Avossa G, Sapir A, Shulman GL, Corbetta M. Is the posner reaction time test more accurate than clinical tests in detecting left neglect in acute and chronic stroke? Arch Phys Med Rehabil. 2009;90(12):2081–2088. doi:10.1016/j.apmr.2009.07.014
39. Rabuffetti M, Farina E, Alberoni M, et al. Spatio-temporal features of visual exploration in unilaterally brain-damaged subjects with or without neglect: results from a touchscreen test. PLoS One. 2012;7:2. doi:10.1371/journal.pone.0031511
40. Bonato M, Priftis K, Umilta C, Zorzi M. Computer-based attention-demanding testing unveils severe neglect in apparently intact patients. Behav Neurol. 2013;25:1–3.
41. Pedroli E, Serino S, Cipresso P, Pallavicini F, Riva G. Assessment and rehabilitation of neglect using virtual reality: a systematic review. Front Behav Neurosci. 2015;9(August):1–15. doi:10.3389/fnbeh.2015.00226
42. Ricci R, Vaishnavi S, Chatterjee A. A deficit of intermediate vision: experimental observations and theoretical implications. Neurocase. 1999;5(1):1–12. doi:10.1080/13554799908404059
43. Ricci R, Calhoun J, Chatterjee A. Orientation bias in unilateral neglect: representational contributions. Cortex. 2000;36(5):671–677. doi:10.1016/S0010-9452%2808%2970544-6
44. Bisiach E, Ricci R, Lai E, De Tanti A, Inzaghi MG. Unilateral neglect and disambiguation of the Necker cube. Brain. 1999;122(1):131–140. doi:10.1093/brain/122.1.131
45. Kinsbourne M. Hemi-neglect and hemisphere rivalry. Adv Neurol. 1977;18:41–49.
46. Bisiach E, Ricci R, Mòdona MN. Visual awareness and anisometry of space representation in unilateral neglect: a panoramic investigation by means of a line extension task. Conscious Cogn. 1998;7(3):327–355. doi:10.1006/ccog.1998.0361
47. Karnath HO. Spatial orientation and the representation of space with parietal lobe lesions. Philos Trans R Soc Lond B Biol Sci. 1997;352(1360):1411–1419. doi:10.1098/rstb.1997.0127
48. Vallar G, Guariglia C, Magnotti L, Pizzamiglio L. Optokinetic stimulation affects both vertical and horizontal deficits of position sense in unilateral neglect. Cortex. 1995;31(4):669–683. doi:10.1016/S0010-9452(13)80019-6
49. Andersen RA. Encoding of intention and spatial location in the posterior parietal cortex. Cereb Cortex. 1995;5(5):457–469. doi:10.1093/cercor/5.5.457
50. Andersen RA, Snyder LH, Bradley DC, Xing J. Multimodal representation of space in the posterior parietal cortex and its use in planning movements. Annu Rev Neurosci. 1997;20:303–330. doi:10.1146/annurev.neuro.20.1.303
51. Critchley M. The phenomenon of tactile in attention with special reference to parietal lesions. Brain. 1949;72(4):538–561. doi:10.1093/brain/72.4.538
52. Mort DJ, Malhotra P, Mannan SK, et al. The anatomy of visual neglect. Brain. 2003;126(9):1986–1997. doi:10.1093/brain/awg200
53. Vallar G. Extrapersonal visual unilateral spatial neglect and its neuroanatomy. NeuroImage. 2001;14(1 II):52–58. doi:10.1006/nimg.2001.0822
54. Karnath HO, Ferber S, Himmelbach M. Spatial awareness is a function of the temporal not the posterior parietal lobe. Nature. 2001;411(6840):950–953. doi:10.1038/35082075
55. Hillis AE. Neurobiology of unilateral spatial neglect. Neuroscientist. 2006;12(2):153–163. doi:10.1177/1073858405284257
56. Medina J, Kannan V, Pawlak MA, et al. Neural substrates of visuospatial processing in distinct reference frames: evidence from unilateral spatial neglect. J Cogn Neurosci. 2009;21:2073–2084. doi:10.1162/jocn.2008.21160.Neural
57. Chechlacz M, Rotshtein P, Bickerton WL, Hansen PC, Deb S, Humphreys GW. Separating neural correlates of allocentric and egocentric neglect: distinct cortical sites and common white matter disconnections. Cogn Neuropsychol. 2010;27(3):277–303. doi:10.1080/02643294.2010.519699
58. Bartolomeo P, Thiebaut De Schotten M, Doricchi F. Left unilateral neglect as a disconnection syndrome. Cereb. Cortex. 2007;17(11):2479–2490. doi:10.1093/cercor/bhl181
59. Doricchi F, Tomaiuolo F. The anatomy of neglect without hemianopia. NeuroReport. 2003;14(17):1–5. doi:10.1097/00001756-200312020-00021
60. Ricci R, Salatino A, Li X, et al. Imaging the neural mechanisms of TMS neglect-like bias in healthy volunteers with the interleaved TMS/fMRI technique: preliminary evidence. Front Hum Neurosci. 2012;6(December):1–13. doi:10.3389/fnhum.2012.00326
61. Molenberghs P, Sale MV, Mattingley JB. Is there a critical lesion site for unilateral spatial neglect? A meta-analysis using activation likelihood estimation. Front Hum Neurosci. 2012;6(April):1–10. doi:10.3389/fnhum.2012.00078
62. Lunven M, Bartolomeo P. Attention and spatial cognition: neural and anatomical substrates of visual neglect. Ann Phys Rehabil Med. 2017;60(3):124–129. doi:10.1016/j.rehab.2016.01.004
63. Frassinetti F, Angeli V, Meneghello F, Avanzi S, Làdavas E. Long-lasting amelioration of visuospatial neglect by prism adaptation. Brain. 2002;125(3):608–623. doi:10.1093/brain/awf056
64. Rode G, Pisella L, Rossetti Y, Farnè A, Boisson D. Bottom-up transfer of sensory-motor plasticity to recovery of spatial cognition: visuomotor adaptation and spatial neglect. Prog Brain Res. 2003;142:273–287. doi:10.1016/S0079-6123(03)42019-0
65. Antonucci G, Guariglia C, Judica A, et al. Effectiveness of neglect rehabilitation in a randomized group study. J Clin Exp Neuropsychol. 1995;17(3):383–389. doi:10.1080/01688639508405131
66. Luauté J, Halligan P, Rode G, Rossetti Y, Boisson D. Visuo-spatial neglect: a systematic review of current interventions and their effectiveness. Neurosci Biobehav Rev. 2006;30(7):961–982. doi:10.1016/j.neubiorev.2006.03.001
67. Priftis K, Passarini L, Pilosio C, Meneghello F, Pitteri M. Visual scanning training, limb activation treatment, and prism adaptation for rehabilitating left neglect: who is the winner? Front Hum Neurosci. 2013;7(July):1–12. doi:10.3389/fnhum.2013.00360
68. Salatino A, Barba S, Vigna F, et al. Prism adaptation and visual scanning training treatments in unilateral spatial neglect. Neurol Sci. 2015;36(1998):194.
69. Spaccavento S, Cellamare F, Cafforio E, Loverre A, Craca A. Efficacy of visual-scanning training and prism adaptation for neglect rehabilitation. Appl Neuropsychol Adult. 2016;23(5):313–321. doi:10.1080/23279095.2015.1038386
70. Polanowska KE, Seniów JB, Paprot E, Leśniak MM, Członkowska A. Left-hand somatosensory stimulation combined with visual scanning training in rehabilitation for post-stroke hemineglect: a randomised, double-blind study. Neuropsychol Rehabil. 2009;19(3):364–382. doi:10.1080/09602010802268856
71. Bailey MJ, Riddoch MJ, Crome P. Treatment of visual neglect in elderly patients with stroke: a single-subject series using either a scanning and cueing strategy or a left-limb activation strategy. Phys Ther. 2002;82(8):782–797. doi:10.1093/ptj%2F82.8.782
72. Brem A, Unterburger E, Speight I, Jäncke L. Treatment of visuospatial neglect with biparietal tDCS and cognitive training: a single-case study. Front Syst Neurosci. 2014;8. doi:10.3389/fnsys.2014.00180.
73. Smania N, Fonte CS, Picelli A, Gandolfi M, Varalta V. Effect of eye patching in rehabilitation of hemispatial neglect. Front Hum Neurosci. 2013. doi:10.3389/fnhum.2013.00527
74. Bottini G, Gandola M. Beyond the non-specific attentional effect of caloric vestibular stimulation: evidence from healthy subjects and patients. Multisensory Res. 2015;28(5–6):591–612. doi:10.1163/22134808-00002504
75. Welfringer A, Leifert-Fiebach G, Babinsky R, Brandt T. Visuomotor imagery as a new tool in the rehabilitation of neglect: a randomised controlled study of feasibility and efficacy. Disabil Rehabil. 2011;33(21–22):2033–2043. doi:10.3109/09638288.2011.556208
76. Dohle C, Püllen J, Nakaten A, Küst J, Rietz C, Karbe H. Mirror therapy promotes recovery from severe hemiparesis: a randomized controlled trial. Neurorehabil Neural Repair. 2009;23(3):209–217. doi:10.1177/1545968308324786
77. Pitzalis S, Spinelli D, Vallar G, Russo FD. Transcutaneous electrical nerve stimulation effects on neglect: a visual-evoked potential study. Front Hum Neurosci. 2013;7. doi:10.3389/fnhum.2013.00111.
78. Kerkhoff G, Reinhart S, Ziegler W, Artinger F, Marquardt C, Keller I. Smooth pursuit eye movement training promotes recovery from auditory and visual neglect: a randomized controlled study. Neurorehabil Neural Repair. 2013;27(9):789–798. doi:10.1177/1545968313491012
79. Machner B, Könemund I, Sprenger A, Von Der Gablentz J, Helmchen C. Randomized controlled trial on hemifield eye patching and optokinetic stimulation in acute spatial neglect. Stroke. 2014;45(8):2465–2468. doi:10.1161/STROKEAHA.114.006059
80. von der Gablentz J, Könemund I, Sprenger A, et al. Brain activations during optokinetic stimulation in acute right-hemisphere stroke patients and hemispatial neglect: an fMRI study. Neurorehabil Neural Repair. 2019;33:581–592. doi:10.1177/1545968319855038
81. Kwakkel G, Veerbeek JM, Wegen EE, Wolf SL. Constraint-induced movement therapy after stroke. Lancet Neurol. 2015;14:224–234. doi:10.1016/S1474-4422(14)70160-7
82. Corbetta D, Sirtori V, Castellini G, Moja L, Gatti R. Constraint‐induced movement therapy for upper extremities in people with stroke. Cochrane Database Syst Rev. 2015;(10):
83. Cicerone KD, Dahlberg C, Kalmar K, et al. Evidence-based cognitive rehabilitation: recommendations for clinical practice. Arch Phys Med Rehabil. 2000;81(12):1596–1615. doi:10.1053/apmr.2000.19240
84. Fortis P, Chen P, Goedert KM, Barrett AM. Effects of prism adaptation on motor-intentional spatial bias in neglect. Neuroreport. 2011;22(14):700–705. doi:10.1097/WNR.0b013e32834a3e20
85. Pisella L, Rode G, Farnè A, Tilikete C, Rossetti Y. Prism adaptation in the rehabilitation of patients with visuo-spatial cognitive disorders. Curr Opin Neurol. 2006;19(6):534–542. doi:10.1097/WCO.0b013e328010924b
86. Martín-Arévalo E, Schintu S, Farnè A, Pisella L, Reilly KT. Adaptation to leftward shifting prisms alters motor interhemispheric inhibition. Cereb. Cortex. 2018;28(2):528–537. doi:10.1093/cercor/bhw386
87. Rossetti Y, Rode G, Pisella L, et al. Prism adaptation to a rightward optical deviation rehabilitates left hemispatial neglect. Nature. 1998;395(6698):166–169. doi:10.1038/25988
88. Farnè A, Rossetti Y, Toniolo S, Làdavas E. Ameliorating neglect with prism adaptation: visuo-manual and visuo-verbal measures. Neuropsychologia. 2002;40(7):718–729. doi:10.1016/S0028-3932(01)00186-5
89. Serino A, Bonifazi S, Pierfederici L, Làdavas E. Neglect treatment by prism adaptation: what recovers and for how long. Neuropsychol Rehabil. 2007;17(6):657–687. doi:10.1080/09602010601052006
90. Serino A, Barbiani M, Rinaldesi ML, Làdavas E. Effectiveness of prism adaptation in neglect rehabilitation. Stroke. 2009;40(4):1392–1398. doi:10.1161/strokeaha.108.530485
91. Vaes N, Nys G, Lafosse C, et al. Rehabilitation of visuospatial neglect by prism adaptation: effects of a mild treatment regime. A randomised controlled trial. Neuropsychol Rehabil. 2018;28(6):899–918. doi:10.1080/09602011.2016.1208617
92. Mizuno K, Tsuji T, Takebayashi T, Fujiwara T, Hase K, Liu M. Prism adaptation therapy enhances rehabilitation of stroke patients with unilateral spatial neglect: a randomized, controlled trial. Neurorehabil Neural Repair. 2011;25(8):711–720. doi:10.1177/1545968311407516
93. Nys GMS, Seurinck R, Dijkerman HC. Prism adaptation moves neglect-related perseveration to contralesional space. Cognit Behav Neurol. 2008;21(4):249–253. doi:10.1097/WNN.0b013e31818a5cc1
94. Turton AJ, O’Leary K, Gabb J, Woodward R, Gilchrist ID. A single blinded randomised controlled pilot trial of prism adaptation for improving self-care in stroke patients with neglect. Neuropsychol Rehabil. 2010;20(2):180–196. doi:10.1080/09602010903040683
95. Mancuso M, Pacini MJ, Gemignani P, et al. Clinical application of prismatic lenses in the rehabilitation of neglect patients. A randomized controlled trial a randomized controlled trial. Eur J Phys Rehabil Med. 2012;48(2):197–208.
96. Rode G, Lacour S, Jacquin-Courtois S, et al. Long-term sensorimotor and therapeutical effects of a mild regime of prism adaptation in spatial neglect. A double-blind RCT essay. Ann Phys Rehabil Med. 2015;58(2):40–53. doi:10.1016/j.rehab.2014.10.004
97. Ten Brink AF, Visser-Meily JMA, Schut MJ, Kouwenhoven M, Eijsackers ALH, Nijboer TCW. Prism adaptation in rehabilitation? No additional effects of prism adaptation on neglect recovery in the subacute phase poststroke: a randomized controlled trial. Neurorehabil Neural Repair. 2017;31(12):1017–1028. doi:10.1177/1545968317744277
98. Gammeri R, Turri F, Ricci R, Ptak R. Adaptation to virtual prisms and its relevance for neglect rehabilitation: a single-blind dose-response study with healthy participants. Neuropsychol Rehabil. 2018:1–14. doi:10.1080/09602011.2018.1502672
99. Salatino A, Berra E, Troni W, et al. Behavioral and neuroplastic effects of low-frequency rTMS of the unaffected hemisphere in a chronic stroke patient: a concomitant TMS and fMRI study. Neurocase. 2014;20(6):615–626. doi:10.1080/13554794.2013.826691
100. D’Agata F, Peila E, Cicerale A, et al. Cognitive and neurophysiological effects of non-invasive brain stimulation in stroke patients after motor rehabilitation. Front Behav Neurosci. 2016;10:135. doi:10.3389/fnbeh.2016.00135
101. Ricci R, Salatino A, Siebner HR, Mazzeo G, Nobili M. Normalizing biased spatial attention with parietal rTMS in a patient with focal hand dystonia. Brain Stimul. 2014;7(6):912–914. doi:10.1016/j.brs.2014.07.038
102. Salatino A, Momo E, Nobili M, Berti A, Ricci R. Awareness of symptoms amelioration following low-frequency repetitive transcranial magnetic stimulation in a patient with Tourette syndrome and comorbid obsessive-compulsive disorder. Brain Stimul. 2014;7(2):341–343. doi:10.1016/j.brs.2014.01.002
103. Salatino A, Boccia G, Dardanello D, et al. Acute and cumulative effects of rTMS on behavioural and EMG parameters in focal hand dystonia. Heliyon. 2019;5(11):e02770. doi:10.1016/j.heliyon.2019.e02770
104. Brighina F, Bisiach E, Oliveri M, et al. 1 Hz repetitive transcranial magnetic stimulation of the unaffected hemisphere ameliorates contralesional visuospatial neglect in humans. Neurosci Lett. 2003;336(3):131–133. doi:10.1016/s0304-3940(02)01283-1
105. Oliveri M, Bisiach E, Brighina F, et al. rTMS of the unaffected hemisphere transiently reduces contralesional visuospatial heineglect. Neurology. 2001;57(7):1338–1340. doi:10.1212/WNL.57.7.1338
106. Shindo K, Sugiyama K, Huabao L, Nishijima K, Kondo T, Izumi SI. Long-term effect of low-frequency repetitive transcranial magnetic stimulation over the unaffected posterior parietal cortex in patients with unilateral spatial neglect. J Rehabil Med. 2006;38(1):65–67. doi:10.1080/16501970500441807
107. Koch G, Oliveri M, Cheeran BJ, et al. Hyperexcitability of parietal-motor functional connections in the intact left-hemisphere of patients with neglect. Brain. 2008;131(Pt 12):3147–3155. doi:10.1093/brain/awn273
108. Song W, Du B, Xu Q, Hu J, Wang M, Luo Y. Low-frequency transcranial magnetic stimulation for visual spatial neglect: a pilot study. J Rehabil Med. 2009;41(3):162–165. doi:10.2340/16501977-0302
109. Lim JY, Kang EK, Paik NJ. Repetitive transcranial magnetic stimulation for hemispatial neglect in patients after stroke: an open-label pilot study. J Rehabil Med. 2010;42(5):447–452. doi:10.2340/16501977-0553
110. Agosta S, Herpich F, Miceli G, Ferraro F, Battelli L. Contralesional rTMS relieves visual extinction in chronic stroke. Neuropsychologia. 2014;62:269–276. doi:10.1016/j.neuropsychologia.2014.07.026
111. Kim BR, Chun MH, Kim D, Lee SJ. Effect of high- and low-frequency repetitive transcranial magnetic stimulation on visuospatial neglect in patients with acute stroke: a double-blind, sham-controlled trial. Arch Phys Med Rehabil. 2013;94(5):803–807. doi:10.1016/j.apmr.2012.12.016
112. Cha HG, Kim MK. Effects of repetitive transcranial magnetic stimulation on arm function and decreasing unilateral spatial neglect in subacute stroke: a randomized controlled trial. Clin Rehabil. 2016;30(7):649–656. doi:10.1177/0269215515598817
113. Cazzoli D, Rosenthal CR, Kennard C, Zito GA, Nyffeler T. Theta burst stimulation improves overt visual search in spatial neglect independently of attentional load. Cortex. 2015;73:317–329. doi:10.1016/j.cortex.2015.09.009
114. Hopfner S, Cazzoli D, Müri RM, Nef T, Nyffeler T. Enhancing treatment effects by combining continuous theta burst stimulation with smooth pursuit training. Neuropsychologia. 2015;74:145–151. doi:10.1016/j.neuropsychologia.2014.10.018
115. Cazzoli D, Müri RM, Schumacher R, et al. Theta burst stimulation reduces disability during the activities of daily living in spatial neglect. Brain. 2012;135(11):3426–3439. doi:10.1093/brain/aws182
116. Koch G, Bonnì S, Giacobbe V, et al. θ-burst stimulation of the left hemisphere accelerates recovery of hemispatial neglect. Neurology. 2012;78(1):24–30. doi:10.1212/WNL.0b013e31823ed08f
117. Fu W, Song W, Zhang Y, et al. Long-term effects of continuous theta-burst stimulation in visuospatial neglect. J Int Med Res. 2015;43(2):196–203. doi:10.1177/0300060513498663
118. Fu W, Cao L, Zhang Y, et al. Continuous theta-burst stimulation may improve visuospatial neglect via modulating the attention network: a randomized controlled study. Top Stroke Rehabil. 2017;24(4):236–241. doi:10.1080/10749357.2016.1253139
119. Yang W, Liu T, Song X, Zhang Y, Liu J. Comparison of different stimulation parameters of repetitive transcranial magnetic stimulation for unilateral spatial neglect in stroke patients. J Neurol Sci. 2015;359:219–225. doi:10.1016/j.jns.2015.08.1541
120. Ko MH, Han SH, Park SH, Seo JH, Kim YH. Improvement of visual scanning after DC brain polarization of parietal cortex in stroke patients with spatial neglect. Neurosci Lett. 2008;448(2):171–174. doi:10.1016/j.neulet.2008.10.050
121. Sparing R, Thimm M, Hesse MD, Küst J, Karbe H, Fink GR. Bidirectional alterations of interhemispheric parietal balance by non-invasive cortical stimulation. Brain. 2009;132(11):3011–3020. doi:10.1093/brain/awp154
122. Sunwoo H, Kim YH, Chang WH, Noh S, Kim EJ, Ko MH. Effects of dual transcranial direct current stimulation on post-stroke unilateral visuospatial neglect. Neurosci Lett. 2013;554:94–98. doi:10.1016/j.neulet.2013.08.064
123. Smit M, Schutter DJ, Nijboer TC, Visser-Meily JM, Dijkerman HC. Transcranial direct current stimulation to the parietal cortex in hemispatial neglect: a feasibility study. Neuropsychologia. 2015;74:152–161. doi:10.1016/j.neuropsychologia.2015.04.014
124. Yi YG, Chun MH, Do KH, Sung EJ, Kwon YG, Kim DY. The effect of transcranial direct current stimulation on neglect syndrome in stroke patients. Ann Rehabil Med. 2016;40(2):223–229. doi:10.5535/arm.2016.40.2.223
125. Bang D, Bong S. Effect of combination of transcranial direct current stimulation and feedback training on visuospatial neglect in patients with subacute stroke: a pilot randomized controlled trial. J Phys Ther Sci. 2015. doi:10.1589/jpts.27.2759
126. Turgut N, Miranda M, Kastrup A, Eling P, Hildebrandt H. tDCS combined with optokinetic drift reduces egocentric neglect in severely impaired post-acute patients. Neuropsychol Rehabil. 2018;28(4):515–526. doi:10.1080/09602011.2016.1202120
127. Utz KS, Korluss K, Schmidt L, et al. Minor adverse effects of galvanic vestibular stimulation in persons with stroke and healthy individuals. Brain Injury. 2011;25(11):1058–1069. doi:10.3109/02699052.2011.607789
128. Bense S, Stephan T, Yousry TA, Brandt T, Dieterich M. Multisensory Cortical Signal Increases and Decreases During Vestibular Galvanic Stimulation (fMRI). J Neurophysiol. 2017;85(2):886–899. doi:10.1152/jn.2001.85.2.886
129. Lopez C, Blanke O, Mast FW. The human vestibular cortex revealed by coordinate-based activation likelihood estimation meta-analysis. Neuroscience. 2012;212:159–179. doi:10.1016/j.neuroscience.2012.03.028
130. Saj A, Honoré J, Rousseaux MR. Perception of the vertical in patients with right hemispheric lesion: effect of galvanic vestibular stimulation. Neuropsychologia. 2006;44:1509–1512. doi:10.1016/j.neuropsychologia.2005.11.018
131. Nakamura J, Kita Y, Ikuno K, Kojima K, Okada Y, Shomoto K. Influence of the stimulus parameters of galvanic vestibular stimulation on unilateral spatial neglect. Neuroreport. 2015;26(8):462–466. doi:10.1097/wnr.0000000000000369
132. Schmidt LK, Utz KS, Depper L, et al. Now you feel both: galvanic vestibular stimulation induces lasting improvements in the rehabilitation of chronic tactile extinction. Front Hum Neurosci. 2013. doi:10.3389/fnhum.2013.00090
133. Zubko O, Wilkinson D, Langston D, Sakel M. The effect of repeated sessions of galvanic vestibular stimulation on target cancellation in visuo-spatial neglect: preliminary evidence from two cases. Brain Inj. 2013;27(5):613–619. doi:10.3109/02699052.2013.767938
134. Utz KS, Keller I, Kardinal M, Kerkhoff G. Galvanic vestibular stimulation reduces the pathological rightward line bisection error in neglect—A sham stimulation-controlled study. Neuropsychologia. 2011;49:1219–1225. doi:10.1016/j.neuropsychologia.2011.02.046
135. Wilkinson D, Zubko O, Sakel M, Coulton S, Higgins T, Pullicino P. Galvanic vestibular stimulation in hemi-spatial neglect. Front Integr Neurosci. 2014;8(January):1–12. doi:10.3389/fnint.2014.00004
136. Oppenländer K, Utz KS, Reinhart S, Keller I, Kerkhoff G, Schaadt AK. Subliminal galvanic-vestibular stimulation recalibrates the distorted visual and tactile subjective vertical in right-sided stroke. Neuropsychologia. 2015;74:178–183. doi:10.1016/j.neuropsychologia.2015.03.004
137. Volkening K, Kerkhoff G, Keller I. Effects of repetitive galvanic vestibular stimulation on spatial neglect and verticality perception—a randomised sham-controlled trial. Neuropsychol Rehabil. 2018;28(7):1179–1196. doi:10.1080/09602011.2016.1248446
138. Ruet A, Jokic C, Denise P, Leroy F, Azouvi P. Does galvanic vestibular stimulation reduce spatial neglect? A negative study. Ann Phys Rehabil Med. 2014;57(9–10):570–577. doi:10.1016/j.rehab.2014.09.009
139. Kim YM, Chun MH, Yun GJ, Song YJ, Young HE. The effect of virtual reality training on unilateral spatial neglect in stroke patients. Ann Rehabil Med. 2011. doi:10.5535/arm.2011.35.3.309
140. Mainetti R, Sedda A, Ronchetti M, Bottini G, Borghese NA. Duckneglect: video-games based neglect rehabilitation. Technol Health Care. 2013;21(2):97–111. doi:10.3233/THC-120712
141. Navarro M, Lloréns R, Noé E, Ferri J, Alcañiz M. Validation of a low-cost virtual reality system for training street-crossing. A comparative study in healthy, neglected and non-neglected stroke individuals. Neuropsychol Rehabil. 2013;23(4):597–618. doi:10.1080/09602011.2013.806269
142. Fordell H, Bodin K, Eklund A, Malm J. RehAtt – scanning training for neglect enhanced by multi-sensory stimulation in virtual reality. Top Stroke Rehabil. 2016;23(3):191–199. doi:10.1080/10749357.2016.1138670
143. Ekman U, Fordell H, Eriksson J, et al. Increase of frontal neuronal activity in chronic neglect after training in virtual reality. Acta Neurol Scand. 2018;138(4):284–292. doi:10.1111/ane.12955
144. Wåhlin A, Fordell H, Ekman U, Lenfeldt N, Malm J. Rehabilitation in chronic spatial neglect strengthens resting-state connectivity. Acta Neurol Scand. 2019;139(3):254–259. doi:10.1111/ane.13048
145. Rose NS, Rendell PG, Hering A, Kliegel M, Bidelman GM, Craik FIM. Cognitive and neural plasticity in older adults’ prospective memory following training with the virtual week computer game. Front Hum Neurosci. 2015;9(October):1–13. doi:10.3389/fnhum.2015.00592
146. Hilgetag CC, Théoret H, Pascual-Leone A. Enhanced visual spatial attention ipsilateral to rTMS-induced ‘virtual lesions’ of human parietal cortex. Nat Neurosci. 2001;4:953–957. doi:10.1038/nn0901-953
147. Fierro B, Brighina F, Piazza A, Oliveri M, Bisiach E. Timing of right parietal and frontal cortex activity in visuo-spatial perception: a TMS study in normal individuals. NeuroReport. 2001;12(11):2605–2607. doi:10.1097/00001756-200108080-00062
148. Giglia G, Pia L, Folegatti A, Puma AL, Brighina F. Far space remapping by tool use: a rTMS study over the right posterior parietal cortex. Brain Stimul. 2015;8:795–800. doi:10.1016/j.brs.2015.01.412
149. Giglhuber K, Maurer S, Zimmer C, Meyer B, Krieg SM. Evoking visual neglect-like deficits in healthy volunteers – an investigation by repetitive navigated transcranial magnetic stimulation. Brain Imaging Behav. 2017;11(1):17–29. doi:10.1007/s11682-016-9506-9
150. Bjoertomt O, Cowey A, Walsh V. Near space functioning of the human angular and supramarginal gyri. J Neuropsychol. 2009;3(1):31–43. doi:10.1348/174866408X394604
151. Brighina F, Bisiach E, Piazza A, et al. Perceptual and response bias in visuospatial neglect due to frontal and parietal repetitive transcranial magnetic stimulation in normal subjects. Neuroreport. 2002;13(18):2571–2575. doi:10.1097/01.wnr.0000052321.62862.7e
152. Salatino A, Poncini M, George MS, Ricci R. Hunting for right and left parietal hot spots using single-pulse TMS: modulation of visuospatial perception during line bisection judgment in the healthy brain. Front Psychol. 2014;1–7. doi:10.3389/fpsyg.2014.01238
153. Salatino A, Chillemi G, Gontero F, et al. Transcranial magnetic stimulation of posterior parietal cortex modulates line-length estimation but not illusory depth perception. Front Psychol. 2019;1–8. doi:10.3389/fpsyg.2019.01169
154. De Schotten MT, Dell’Acqua F, Forkel SJ, et al. A lateralized brain network for visuospatial attention. Nat Neurosci. 2011;14:1245–1246. doi:10.1038/nn.2905
155. Bagattini C, Mazzi C, Savazzi S. Waves of awareness for occipital and parietal phosphenes perception. Neuropsychologia. 2015;70:114–125. doi:10.1016/j.neuropsychologia.2015.02.021
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.