Back to Journals » Journal of Pain Research » Volume 14
Unilateral Acupuncture Reduces Postoperative Pain Scores in Children Undergoing Adenotonsillectomy: A Randomized Controlled Trial
Authors Ismail SA, Atef HM, Abuelnaga ME ![]() , Midan HM
, Midan HM
Received 6 October 2020
Accepted for publication 12 January 2021
Published 2 February 2021 Volume 2021:14 Pages 273—283
DOI https://doi.org/10.2147/JPR.S285322
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Michael Überall
Salah A Ismail, Hossam M Atef, Mohamed E Abuelnaga, Haddier M Midan
Department of Anesthesia, Intensive Care and Pain Management, Faculty of Medicine, Suez Canal University, Ismailia, Egypt
Correspondence: Mohamed E Abuelnaga
Department of Anesthesia, Intensive Care and Pain Management, Faculty of Medicine, Suez Canal University, The Ring Road, P.O. Box: 41522, Ismailia City, Egypt
Tel +201004150671
Fax +20643208543
Email [email protected]
Purpose: Acupuncture ameliorates several pain disorders including postoperative pain. This can help to decrease the need for postoperative analgesics. We aimed to evaluate the effectiveness of acupuncture as an adjuvant scheme reduce both intraoperative and postoperative analgesia needs in children undergoing adenotonsillectomy.
Methods: This was a randomized controlled single-blinded trial that was performed over sixty children scheduled for adenotonsillectomy. They were randomly allocated to either an intervention group that received general anesthesia plus acupuncture or a control group which received general anesthesia alone. The primary outcome was the measurement of postoperative pain scores. Secondary outcomes included measurement of time to the first request of postoperative analgesia, the number of children requesting postoperative analgesics in the first 2 hours, the incidence of postoperative complications including postoperative nausea and/or vomiting (PONV), and emergence agitation (EA).
Results: AThe Wong-Baker FACES pain scores at rest and on swallowing were significantly lower in the intervention group than in the control group postoperatively. The time to the first request of postoperative analgesia was delayed in the intervention group versus the control group, with less number of patients who have requested additional analgesia during the first 2 hours postoperatively. Postoperative agitation was lower in the intervention group versus the control group patients. However, the incidence of PONV was not statistically different between study groups.
Conclusion: Combined acupuncture with general anesthesia in children undergoing adenotonsillectomy provided better postoperative pain control with no adverse effects.
Keywords: acupuncture, adenotonsillectomy, postoperative pain
Plain Language Summary
What is already known about the topic: acupuncture is a well-known modality for both acute and chronic pain disorders. Several studies showed the efficacy of acupuncture in children undergoing adenotonsillectomy regarding postoperative analgesia, vomiting, and agitation.
What new information this study adds: in our study, we used combined preoperative unilateral different body and ear acupuncture points targeting several beneficial effects like perioperative analgesia, reducing PONV, and EA. We used manual stimulation for the body acupuncture needles. Acupuncture needles were left in place till the end of surgery.
What we found in our study: we found that acupuncture is a beneficial adjuvant to general anesthesia. It provides good perioperative pain control in children undergoing adenotonsillectomy under general anesthesia. Acupuncture can be used safely in children.
Introduction
Traditional Chinese Medicine hypothesizes that human bodies have an energy force called “Qi”. This energy is continuously flowing throughout the body in pathways called “meridians”.1,2 It is thought that disorders in the flow of Qi can cause pain and sickness. Acupuncture is believed to restore the balance of the flow of Qi when particular points “acupoints” along the meridians are stimulated.1,2
Major postoperative pain in children can slow recovery, reduce oral intake, induce disturbed sleep, and behavioral changes.3 Tonsillectomy is one of the most frequently practiced surgical operations in the ear, nose, and throat with a high occurrence of postoperative pain despite several postoperative analgesic options.4–6
Postoperative swallowing pain was found to continue for three days in children following tonsillectomy7 and can extend up to two weeks in children undergoing tonsillectomy and adenoidectomy.8 Dorkham et al9 have reported several barriers to postoperative pain management in children. The most important of these factors are parental inability to diagnose or assess pain, paternal false beliefs about analgesic drugs,10 child refusal to receive medications, low analgesic drug efficacy, insufficient dose or formulation;11 and poor discharge instructions.8,10
Opioid analgesics should be used with caution especially in children with obstructive sleep apnea.12 Although non-steroidal anti-inflammatory drugs are effective in pain management without an increased incidence of postoperative bleeding, the possibility of severe bleeding is questionable.12 Acupuncture may be used effectively as the adjunctive or principal form of alternative care.13
Several systematic reviews of studies done on untoward effects of needle acupuncture in several medical disorders concluded that it will be safe when practiced by skilled professionals.1,14,15
Acupuncture is believed to reduce pain intensity, allowing for decreased analgesic doses.16 The mechanism behind acupuncture analgesia is not precisely known. However, it may reduce pain by activating different neurotransmitters or modulators as opioid peptides, norepinephrine, serotonin, and adenosine, or through stimulation of endogenous pain inhibitory pathway.17
Several previous studies were done to evaluate the effectiveness of acupuncture as adjuvant analgesia in children undergoing tonsillectomy with or without adenoidectomy. One study used combined body and auricular acupuncture with electro-stimulation,18 while others used body acupuncture alone without needle stimulation.4,19–21
This study was conducted to evaluate the effectiveness of preoperative unilateral combined body and auricular acupuncture with manual stimulation of body acupuncture needles as an adjuvant for pain relief following adenotonsillectomy aiming to reduce postoperative pain in the pediatric age group. The primary objective was to assess the effect of acupuncture on postoperative pain scores for the first two hours after surgery following adenotonsillectomy. The secondary outcomes were the effect of acupuncture on time to the first request of postoperative analgesia for the first 24 hours, the number of patients requesting postoperative analgesia in the first 2 hours, postoperative complications including EA and PONV. We hypothesized that acupuncture will reduce postoperative pain scores in the pediatric age group following adenotonsillectomy.
Materials and Methods
This study is a single-blinded randomized controlled clinical trial. It was conducted on 60 patients scheduled for adenotonsillectomy due to recurrent infection as an outpatient procedure (Figure 1). Children and their guardians were blind to the study group. This manuscript adheres to the applicable Equator guidelines (Consort guidelines for clinical trials with STRICTA extension) (www.consort-statement.org). This study was approved by Suez Canal University’s Institutional Review Board (research #2234) on 27 September 2017 and informed written consent was done for all patients participating in the study. Of note, the trial was registered before enrolment of the first patient at the PACTR (www.pactr.org) database (PACTR201806003339337, Date of registration: 21 April 2018). The principal investigator is Haddier M. Midan, MBBch. Patients were randomized into two equal groups using simple random tables generated from a computer software program (http://www.randomizer.org). The allocation sequence was concealed in opaque numbered envelopes. Randomization, concealment, and opening envelopes at the end of the research work were carried out by a colleague anesthesiologist who did not participate in the research work. Inclusion criteria included children from both sexes, aged between 3 and 12 years, and scheduled for elective adenotonsillectomy. Children complaining of skin lesions near acupuncture sites, psychiatric disorders, coagulopathy, chronic use of analgesic or sedative therapy, or whom guardians refused to participate in the study were excluded.
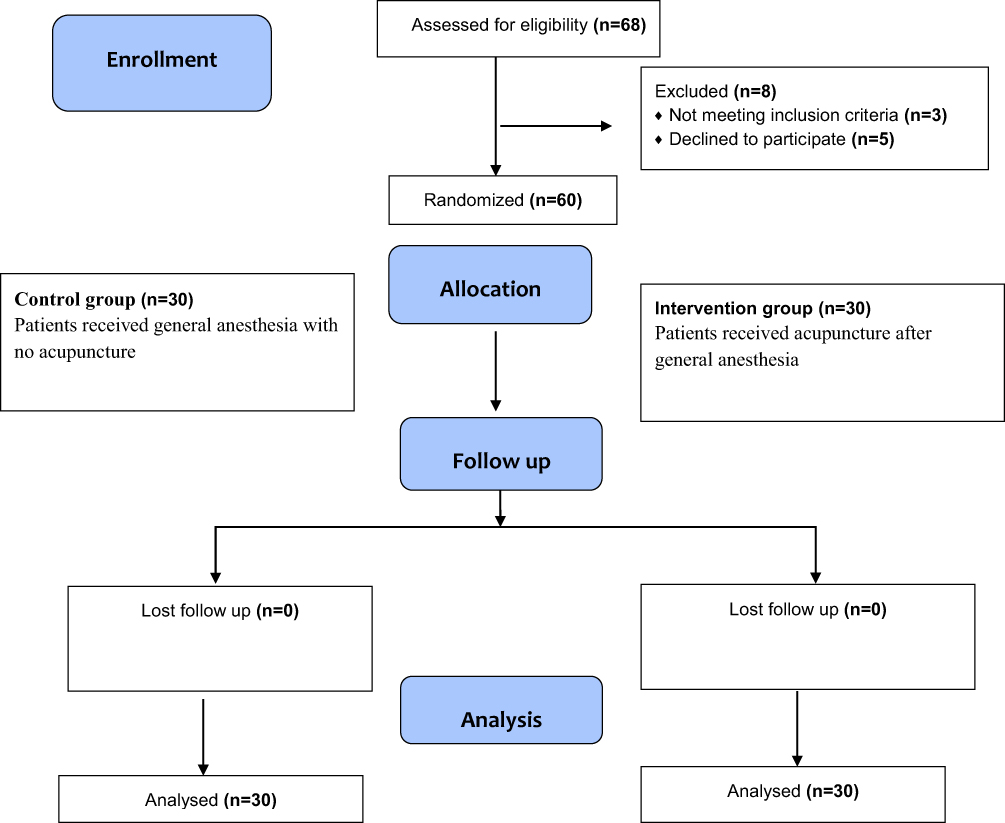 |
Figure 1 Flowchart of patient’s participation progress throughout the study. |
Patients Were Randomized into Two Equal Groups
Intervention Group (30 Children)
Where patients received general anesthesia with standard perioperative analgesics plus acupuncture.
Control Group (30 Children)
Where patients received general anesthesia with standard perioperative analgesics.
Intraoperative Technique
No pre-medications were given. Anesthesia was induced by intravenous propofol 2–3 mg/kg, and fentanyl 1mcg/kg, without muscle relaxants, and then patients were orally intubated with a suitable size endotracheal tube. Anesthesia was maintained using Isoflurane at 1 MAC in 50% oxygen in air. Mechanical ventilation started with tidal volume 8 mL/Kg, respiratory rate according to age and to keep end-tidal CO2 30–35 mmHg. Heart rate (HR), systolic blood pressure (SBP), and diastolic blood pressure (DBP) were recorded and analyzed at these time parts: (baseline, after induction of anesthesia, every 5 minutes throughout the surgery, after extubation, and every 30 minutes postoperative for 2 hours. Tramadol, 0.5 mg/kg was given intravenously as a rescue analgesic if HR increased more than 10% of baseline. All surgeries were performed by the same surgeon. Tonsillectomy was performed using blunt and sharp knife dissection, with the use of bipolar electrocautery if needed to achieve Hemostasis, while adenoidectomy was performed using the classic curettage technique.
Acupuncture Technique
Acupuncture was performed after induction of anesthesia by faculty with greater than 20 years’ experience with different acupuncture modalities. Acupuncture needles were removed before the extubation of patients.
Body Acupuncture (Figure 2)
Sterile single-use acupuncture needles (Cloud and Dragon®, 10mm x 30gauge) penetrated the skin to a depth of 1 cm for the following points unilaterally; needle stimulation was done manually by anticlockwise rotation every 5 minutes till the end of surgery in the following acupoints:
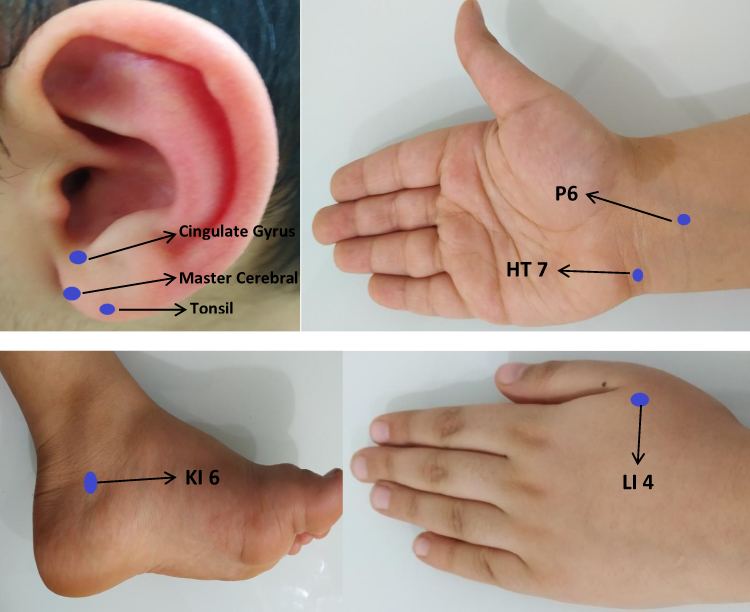 |
Figure 2 Body and ear acupoints used. |
The former, on the dorsum of the hand between 1st and 2nd metacarpal bones, the latter, in a depression 1cun (Chinese inches, equivalent to the width of the interphalangeal joint of the thumb of the patient) below the tip of the medial malleolus. These points were used for their relationship to analgesia at the throat and head and neck.18
Two cun above the transverse crease of the wrist: for its antiemetic properties.22
On the ulnar end of the transverse crease of the wrist to decrease postoperative agitation.22
Ear Acupuncture (Figure 2)
Sterile press needles (shen long pai®, 0.22X1.5) were placed at the following unilateral auricular points over ear lobule: (master cerebral, cingulate gyrus and tonsil) till the end of surgery.22
Postoperative Care
A survey form was completed at PACU by the anesthesiologist with recording and analysis of vital signs (HR, SBP, and DBP were recorded and analyzed every 30 minutes postoperative for 2 hours), pain scores at rest, and on swallowing (every 30 minutes for 2 hours) using the Wong-Baker FACES Pain Scale23 after being explained before anesthesia to the children with the help of their guardians. The time to the first request of postoperative analgesia for the first 24 hours and the number of children requesting postoperative analgesics in the first 2 hours were recorded. The incidence of postoperative nausea and/or vomiting was recorded. Postoperative emergence agitation was assessed and recorded using the PAED (Post Anesthetic Emergence Delirium) scale.24 Intravenous (IV) paracetamol 15 mg/kg was given postoperatively if the pain scores at rest ≥4. According to our hospital policy, patients were discharged home after 2 hours of surgery as long as being fully awake, have intact protective airway reflexes, controlled pain, and free of any major complications as bleeding, vomiting, or any cardiovascular events. Analgesia at home was conducted with a protocol of paracetamol 15 mg/kg oral syrup to be repeated every 6 hours; no postoperative opioids were prescribed for use at home. After the patient’s discharge, parents were contacted by phone to ask about the time of the first request of analgesia if it was not during hours of hospital stay. Parents were asked to encourage cold fluid administration as long as the child can tolerate, stay in contact with the main researcher by phone if pain or vomiting is not controlled, or in case of any event necessitating returning to the hospital.
Statistical Analysis
The statistical analysis was performed using IBM SPSS Statistics® 22 for Windows 10 operating system. Normality was assessed using the Shapiro–Wilk test and visual inspection of histograms. For demographic and baseline comparison, the standardized difference was calculated using a web-based effect-size calculator.25 Two-tailed t-test was used to analyze the continuous variables (hemodynamic parameters, pain score, 1st request of analgesia, total analgesic consumption) between the two studied groups while the chi-square test was used for categorical and dichotomous variables (incidence of nausea, vomiting, and postoperative agitation). Values were expressed as mean ± standard deviation (continuous variables) or as a percentage of the group from which they were derived (categorical variables). P-value < 0.05 was considered significant. Presentation of the statistical outcomes in the form of tables and graphs was performed using the “Microsoft Office Excel® 2010” program. Due to the unavailability of scientific publications with clear results about the efficacy of acupuncture in reducing postoperative pain in children, a sample size of 27 patients per group was required to detect 1.5 differences between the means of postoperative pain score in patients undergoing elective cardiac surgery between acupuncture group and control group at a standard deviation of 2.026 with 80% power and a 5% level of significance. Considering a 10% dropout rate, the sample size required was 60 patients (30 patients per group).
Results
Sixty patients were randomly assigned into two equal groups, intervention group, and control group (Figure 1).
Study groups were matched regarding sex, age, weight, and duration of surgery. All patients in both groups were ASA1. However, the duration of anesthesia was significantly longer in the interventional group versus the control group, mean (SD) was 58.67 (6.69) and 51.87 (5.64) minutes, respectively (p-value =0.0001) (Table 1).
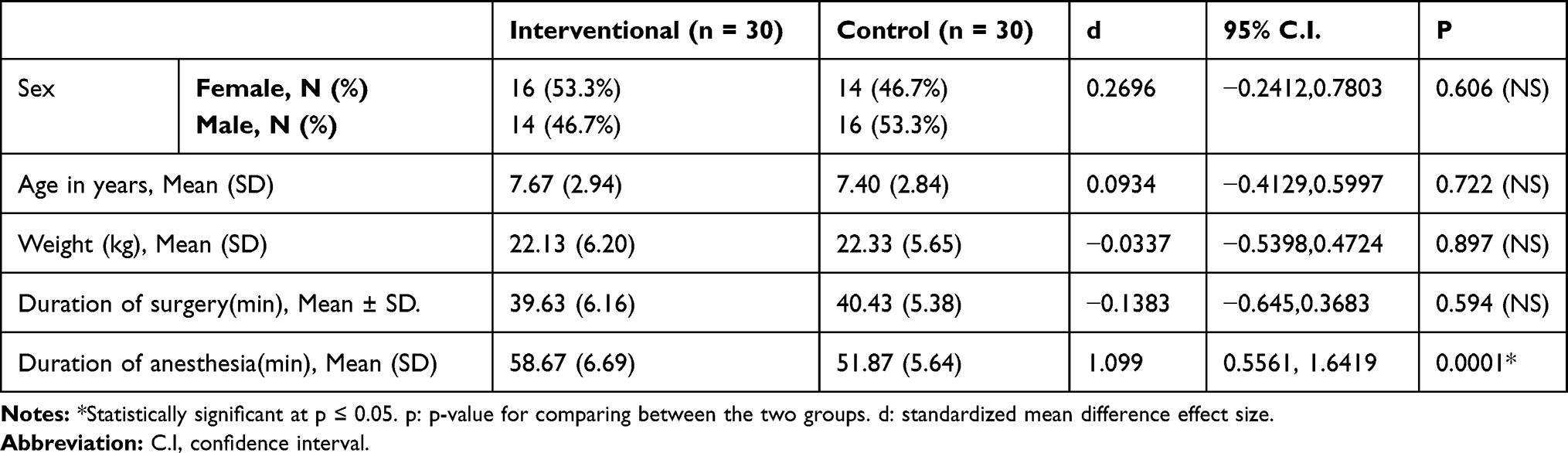 |
Table 1 Demographic Data in Both Groups of the Study |
Wong-Baker FACES pain scores every 30 minutes at rest and during swallowing were significantly lower in the intervention group than in the control group at all points after surgery (p-value =0.0001) (Table 2).
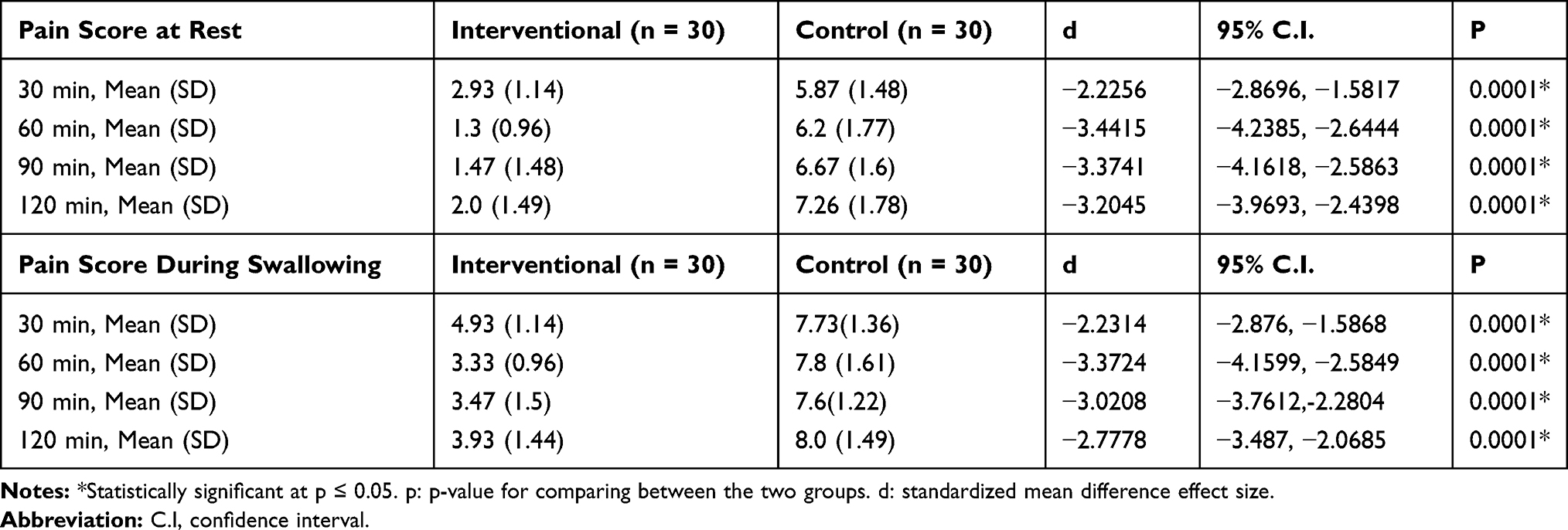 |
Table 2 Postoperative Wong-Baker FACES Pain Scores at Rest and During Swallowing |
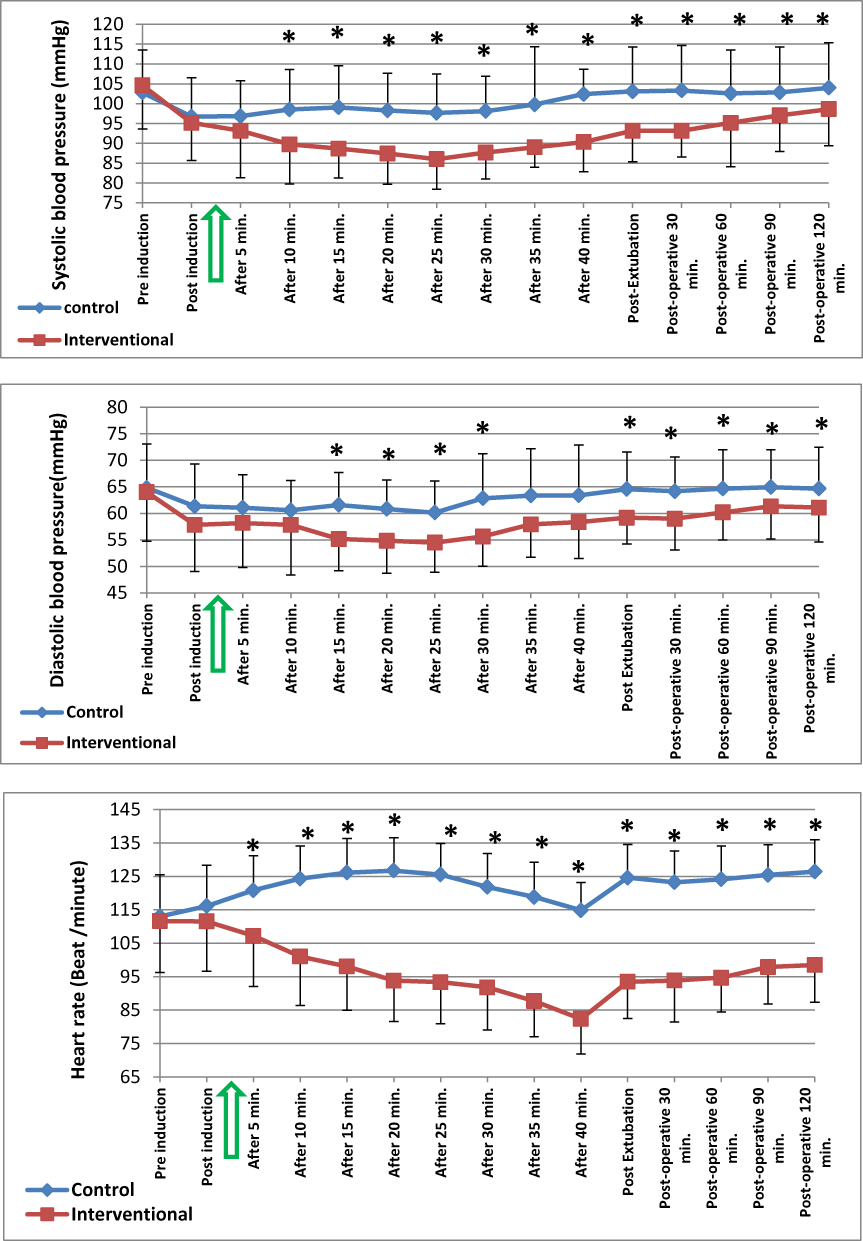
Our results showed that the mean SBP (range: 86.03 −104.6 mm Hg), DBP (range: 54.48–61.33 mm Hg) and HR (range: 82.33 −111.6 beat/min) were lower at most intraoperative and postoperative time points in the intervention group versus the control group where SBP, DBP, and HR means ranged from (96.73 −104 mm Hg), (60.14–64.93mm Hg) and (113–126.7 beat/min) respectively (Figure 3).


There was no statistically significant difference between study groups regarding the intraoperative need for rescue analgesia, only 30.0% of patients in the interventional group received intraoperative extra-analgesia versus 53.3% of patients in the control group (RR=0.5625, 95% CI=0.2963 to 1.0678, P-value = 0.067) (Table 3).
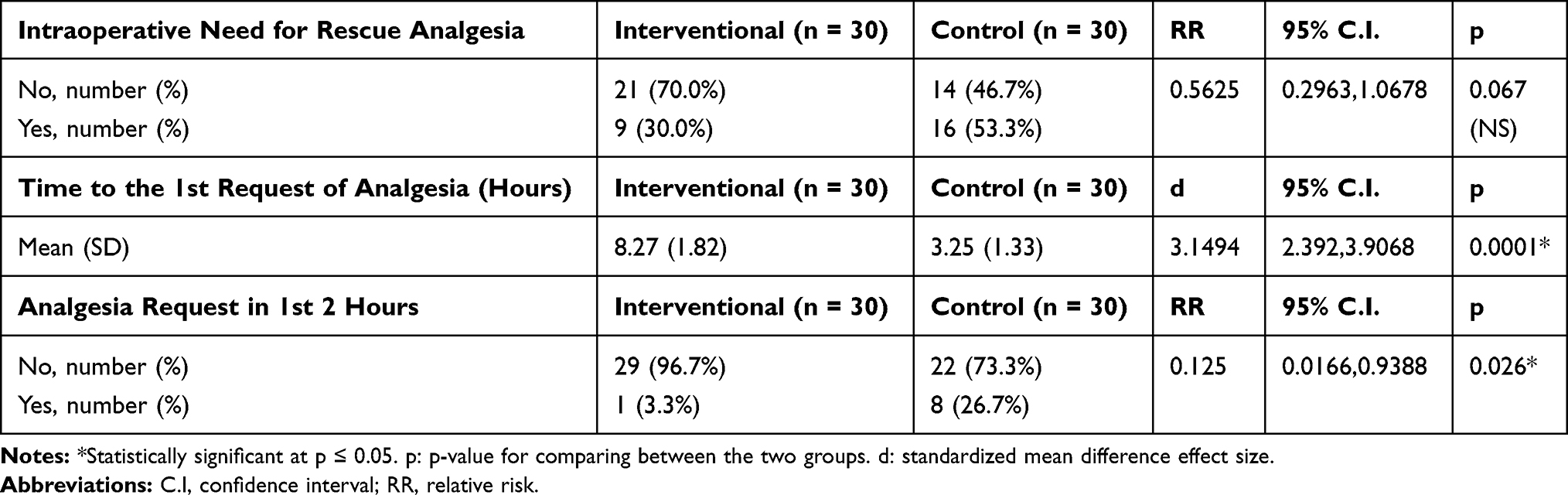 |
Table 3 Intraoperative Need for Rescue Analgesia, Time to the First Request of Postoperative Analgesia in Hours and Number of Patients Requesting Analgesia in the 1st Two Hours |
The first request of postoperative analgesia was significantly delayed in the intervention group than in the control group, mean (SD) was 8.27 (1.82) and 3.25 (1.33) hours, respectively, standardized mean difference (d=3.1494), (95% CI=2.392 to 3.9068), p value=0.0001. Patients requesting additional analgesia during the first 2 hours postoperatively were significantly lower in the interventional group (3.3%) versus the control group (26.7%), (RR=0.125, 95% CI=0.0166 to 0.9388, p-value =0.026) (Table 3).
There was no statistically significant difference between study groups regarding the incidence of postoperative nausea and vomiting. 36.7% and 53.3% of patients in the intervention and control groups, respectively, had nausea (RR=0.6875, 95% CI=0.386 to 1.2245, P-value=0.194) while 26.7% and 43.3% in the intervention and control groups, respectively, had vomiting (RR=0.6154, 95% CI=0.2993 to 1.2653, P-value=0.176) (Table 4).
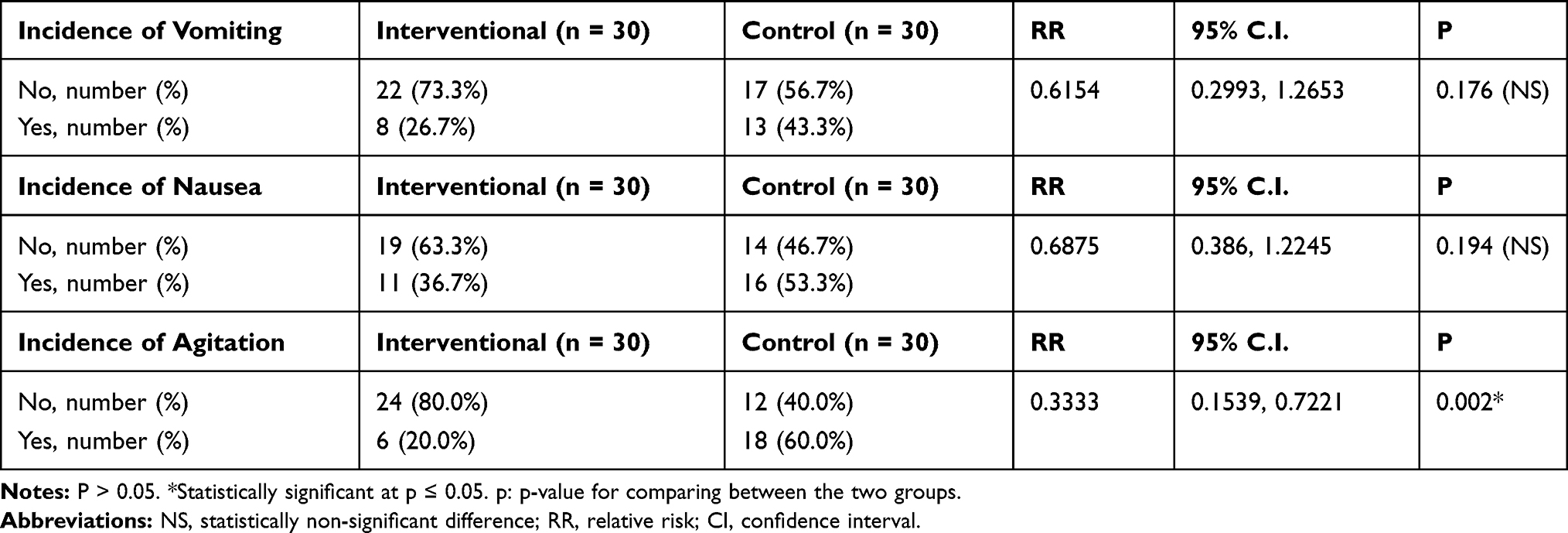 |
Table 4 Incidence of Postoperative Nausea, Vomiting, and Emergence Agitation |
Postoperative agitation was significantly lower in the intervention group (20.0% of patients) than in the control group (60.0% of patients) (RR=0.3333, 95% CI=0.1539 to 0.7221, P value =0.002) (Table 4).
No postoperative complications necessitating hospital readmission have occurred. No acupuncture-related adverse effects were noted.
Discussion
In the present study, we found that unilateral combined body and auricular acupuncture was effective in reducing pain scores at rest and on swallowing in children undergoing adenotonsillectomy. The time to the first request of postoperative analgesics was found significantly longer in the intervention group, with less number of patients in the intervention group requesting additional analgesia during the first 2 hours postoperatively. The duration of anesthesia was found to be longer in the intervention group versus the control group due to excess time spent on the insertion of acupuncture needles, as well as the better degree of analgesia found in the intervention group which may contribute to delayed recovery from anesthesia. We found better perioperative hemodynamic profile in the intervention group versus the control group. This could be attributed to better intraoperative pain relief and less stress.
Similar to our results, Ochi in 2013 performed a retrospective study over 56 patients less than 18 years old undergoing tonsillectomy and adenoidectomy. Local injection of lidocaine 1% with epinephrine 1:100,000 into both tonsillar beds was performed before starting surgery. Postoperative acupuncture was done mainly to LI4 acupoint, instead of codeine for pain relief. The mean reported pain score before acupuncture administration was 5.52 out of 10, in comparison to 1.92 out of 10 following acupuncture with no detected adverse effects.27
Correspondingly, similar results were found by Gilbey et al in 2015 when they compared ordinary postoperative analgesic treatment versus the same regimen plus acupuncture in a randomized, controlled, single-blinded study for tonsillectomy with or without adenoidectomy in 60 children aged 3–12 years. Postoperative bilateral acupuncture was done to six body acupoints (LI1, LI11, and ST44) three times, 2 hours after discharge from the recovery room, 4–8 hours after the first one, and finally 12–18 hours after the second one. Pain scores were significantly lower in the acupuncture group versus the control group mainly after the second and third sessions.20
Tsao et al in 2015, conducted a double-blind randomized controlled trial over 59 children aged 3–12 years undergoing tonsillectomy with or without adenoidectomy and tympanostomy. Patients were randomized to receive either acupuncture or sham acupuncture. Combined auricular and body acupuncture was done with electrical stimulation of body acupoints, and all needles were kept in place to the end of surgery. Pain scores according to patient-reported data were found to be significantly lower in the acupuncture group versus the sham acupuncture group, with the only tendency of improvement according to parent’s reported data.18
In 2016, 12 studies were included in a meta-analysis, addressing the efficacy of acupuncture on post-tonsillectomy pain, nausea, and vomiting. Nine studies were conducted over children, two studies on adults, and one study done over children and adolescents. Cho et al found reduced pain scores and postoperative analgesic needs during the first 48 hours in acupuncture-treated patients versus the control group. However, there were high levels of heterogeneity in multiple measured outputs; thus, acupuncture effectiveness cannot be believed to have been sufficiently evaluated.28
Similar to our results, Oates et al found improvement of self-reported pain scores as well as the associated hemodynamic changes.29
In 2020, HO et al conducted a randomized controlled trial over 251 children aged 2–10 years undergoing tonsillectomy or adenotonsillectomy under general anesthesia. Patients were assigned to either acupuncture group or control group. Acupuncture was done after induction of anesthesia for 10 body acupoints without electrical or manual stimulation. Postoperative pain scores were found significantly lower in the acupuncture group versus the control group in the first 12 hours following surgery.21
In the current study, the incidence of EA was found significantly lower in the acupuncture group versus the control group, which could be due to the effect of the HT7 acupuncture point effect and reduced postoperative pain scores.
EA in pediatrics has several risk factors including preschool age, preoperative anxiety, pain, nausea, vomiting, otolaryngology instrumentation, and inhaled anesthetic drugs specially sevoflurane.30
Similarly, Hijikata et al31 reported that electro-acupuncture of HT7 acupoint reduced the incidence of EA in children undergoing minor elective surgery. Lin et al32 also reported that acupuncture treatment at bilateral LI4 and HT7 acupoints markedly reduced postoperative pain and EA in children undergoing bilateral myringotomy and tympanostomy tube insertion.
Another finding in the current study was that the incidence of postoperative nausea and vomiting was lower in the intervention group than in the control group but without a significant difference between both groups.
Similarly, Özmert et al found that acupuncture at P6 acupoint for at least 20 minutes has been associated with a lower incidence of PONV.33
Moreover, in a recent meta-analysis, Shin et al selected eight randomized controlled clinical trials out of collected 415 publications that investigated the antiemetic effect of acupuncture at a p6 point on pediatric patients after tonsillectomies. PONV was found to be significantly reduced in patients treated by acupuncture treatment in contrast to the control group.34
The clinical efficacy of acupuncture on intraoperative analgesia is still debatable. Although some studies reported that combined intraoperative acupuncture and regular anesthetic policies can reduce the required dose of opioids, other studies have demonstrated doubtful outcomes thus further research work is mandatory.35
Lastly,; there were some limitations to our study. Our study is single-blinded as the outcome assessor is the anesthesiologist who performed the intervention. The procedure study subjects stayed in the hospital for a limited postoperative time since adenotonsillectomy was performed in an ambulatory setting leading to restrict our ability to record the total analgesic consumptions in 24 hours. More multicenter large-sample and high-quality randomized controlled studies are required to evaluate the effect of acupuncture as an adjuvant to general anesthesia in other types of surgery in children and adults. A three arms study is recommended to ensure the effectiveness of acupuncture perioperative analgesia.
Conclusion and Clinical Implications
Acupuncture is a useful adjuvant to general anesthesia in children undergoing adenotonsillectomy. It reduced significantly postoperative pain scores and postoperative analgesic consumption and decreased the incidence of EA. Proper postoperative analgesia especially after oral surgery can help early return to normal diet and hence minimizing the need for hospital readmission. Acupuncture analgesia can decrease the need for perioperative opioid drugs which could be beneficial especially in patients suffering OSA. We believe that acupuncture is a cost-effective procedure that should be integrated into the routine anesthetic management for oral surgery in children.
Abbreviations
PACTR, Pan African Clinical Trial Registry; HR, heart rate; SBP, systolic blood pressure; DBP, diastolic blood pressure; PONV, postoperative nausea and vomiting; EA, emergence agitation; TCM, Traditional Chinese Medicine; LI4, Large intestine 4; KI6, kidney 6; P6, Pericardium 6; HT7, Heart 7; cun, Chinese inch.
Data Sharing Statement
The individual de-identified datasets that underlie the results reported during the current study will be made available. Other study documents that will be made available include the study protocol and informed consent form. Data will be accessible by request directed to the corresponding author at [email protected] and it will be sent by email. Data will be available beginning 3 months and ending 12 months following article publication.
Ethics Statement
This study has been performed in accordance with the principles of Helsinki Declaration on human experimentation. This study was approved by Suez Canal University’s Institutional full Board committee (research #2234) on 27th September 2017 and written informed consent was obtained from the parents of all subjects participating in the trial. The trial was registered before enrolment of the first patient at the Pan African Clinical Trial Registry (www.pactr.org) database (PACTR201806003339337, Date of registration: 21st April 2018). This manuscript adheres to the applicable CONSORT guidelines.
Acknowledgments
We would like to show thanks and gratitude to every participant patient and their parents in our work. Deep thanks to our colleagues and nursing staff in the Suez Canal university hospital operating rooms. Special thanks to our colleague Wesam Fawzy, MD for her help in statistical work.
Author Contributions
All authors made a significant contribution to the conception, study design, execution, acquisition of data, analysis, and interpretation of data. All authors took part in drafting, revising the article; gave final approval of the version to be published; have agreed to submit it to the current journal; and agreed to be responsible for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, non-commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Asher GN, Jonas DE, Coeytaux RR, et al. Auriculotherapy for pain management: a systematic review and meta-analysis of randomized controlled trials. J Altern Complement Med. 2010;16(10):1097–1108. doi:10.1089/acm.2009.0451
2. Spagrud LJ, von Baeyer CL, Ali K, et al. Pain, distress, and adult-child interaction during venipuncture in pediatric oncology: an examination of three types of venous access. J Pain Symptom Manage. 2008;36(2):173–184. doi:10.1016/j.jpainsymman.2007.10.009
3. Power NM, Howard RF, Wade AM, Franck LS. Pain and behaviour changes in children following surgery. Arch Dis Child. 2012;97:879–884. doi:10.1136/archdischild-2011-301378
4. Dingemann J, Plewig B, Baumann I, Plinkert PK, Sertel S. Acupuncture in post-tonsillectomy pain. HNO. 2017;65(S1):73–79. doi:10.1007/s00106-016-0289-5
5. Shum S, Lim J, Page T, et al. An audit of pain management following pediatric day surgery at British Columbia Children’s Hospital. Pain Res Manag. 2012;17:328–334. doi:10.1155/2012/541751
6. Stewart DW, Ragg PG, Sheppard S, Chalkiadis GA. The severity and duration of postoperative pain and analgesia requirements in children after tonsillectomy, orchidopexy, or inguinal hernia repair. Pediatr Anesth. 2012;22:136–143. doi:10.1111/j.1460-9592.2011.03713.x
7. Wilson ME, Helgadottir HL. Patterns of pain and analgesic use in 3 to 7year old children after tonsillectomy. Pain Manag Nurs. 2006;7:156–166. doi:10.1016/j.pmn.2006.09.005
8. Fortier MA, MacLaren JE, Martin SR, Perret KD, Kain ZN. Pediatric pain after ambulatory surgery: where’s the medication? Pediatrics. 2009;124:e588–e595. doi:10.1542/peds.2008-3529
9. Dorkham MC, Chalkiadis GA, von Ungern Sternberg BS, Davidson AJ, Lonnqvist P-A. Effective postoperative pain management in children after ambulatory surgery, with a focus on tonsillectomy: barriers and possible solutions. Paediatr Anaesth. 2014;24(3):239–248. doi:10.1111/pan.12327
10. Kankkunen P, Vehvilainen JK, Pietila AM, Kokki H, Halonen P. Parents’ perceptions and use of analgesics at home after children’s day surgery. Paediatr Anaesth. 2003;13:132–140. doi:10.1046/j.1460-9592.2003.00998.x
11. Sutters KA, Holdridge-Zeuner D, Paul SM, et al. A descriptive feasibility study to evaluate scheduled oral analgesic dosing at home for the management of postoperative pain in preschool children following tonsillectomy. Pain Med. 2012;13:472–483. doi:10.1111/j.1526-4637.2011.01324.x
12. Tan GX, Tunkel DE. Control of pain after tonsillectomy in children: a review. JAMA Otolaryngol. 2017;143(9):937–942. doi:10.1001/jamaoto.2017.0845
13. Kallush A, Kacker A. Is acupuncture an effective complementary tool within otolaryngological perioperative care? Laryngoscope. 2018;128(3):543–544. doi:10.1002/lary.26826
14. Yeh CH, Chiang YC, Hoffman SL, et al. Efficacy of auricular therapy for pain management: a systematic review and meta-analysis. Evid Based Complement Alternat Med. 2014;2014:1–14.
15. Yang C, Hao Z, Zhang L, Guo Q. Efficacy and safety of acupuncture in children: an overview of systematic reviews. Pediatr Res. 2015;78:112–119. doi:10.1038/pr.2015.91
16. Kemper KJ, Sarah R, Licac MPH, et al. On pins and needles? Pediatric pain patients experience with acupuncture. Pediatrics. 2000;105(Supplement 3):941–947.
17. Cho YH, Kim CK, Heo KH, et al. Acupuncture for acute postoperative pain after back surgery: a systematic review and meta-analysis of randomized controlled trials. Pain Pract. 2015;15(3):279–291. doi:10.1111/papr.12208
18. Tsao GJ, Messner AH, Seybold J, Sayyid ZN, Cheng AG, Golianu B. Intraoperative acupuncture for post-tonsillectomy pain: a randomized, double‐blind, placebo‐controlled trial. Laryngoscope. 2015;125(8):1972–1978. doi:10.1002/lary.25252
19. Sertel S, Herrmann S, Greten HJ, et al. Additional use of acupuncture to NSAID effectively reduces post-tonsillectomy pain. Eur Arch Otorhinolaryngol. 2009;266(6):919–925. doi:10.1007/s00405-008-0851-1
20. Gilbey P, Bretler S, Avraham Y, Sharabi-Nov A, Ibrgimov S, Luder A. Acupuncture for post-tonsillectomy pain in children: a randomized, controlled. Paediatr Anaesth. 2015;25(6):603–609. doi:10.1111/pan.12621
21. Ho D, Cooke K, Burns H, McCrystal D, Canty P, Bar R. Intraoperative acupuncture as complementary analgesic for post-tonsillectomy pain in children—a prospective randomised clinical trial of effects and safety. Aust J Otolaryngol. 2020;3:1–11. doi:10.21037/ajo-19-74
22. Anand KJ, Stevens BJ, McGrath PJ. Pain in Neonates and Infants. Elsevier Health Sciences; 2007.
23. Drendel AL, Kelly BT, Ali S. Pain assessment for children: overcoming challenges and optimizing care. Pediatr Emerg Care. 2011;27(8):773–781. doi:10.1097/PEC.0b013e31822877f7
24. Acar HV, Yilmaz A, Demir G, Günal Eruyar S, Dikmen B. Capsicum plasters on acupoints decrease the incidence of emergence agitation in pediatric patients. Pediatric Anesthesia. 2012;11:1105–1109. doi:10.1111/j.1460-9592.2012.03876.x
25. Wilson DB Practical meta-analysis effect size calculator; 2001. Available from: http://www.Campbellcollaboration.org/escalc/HTML/EffectSizeCalculator-SMD1.PHP.
26. Coura LEF, Manoel CHU, Poffo R, Bedin A, Westphal GA. A randomized, controlled study of preoperative electroacupuncture for postoperative pain control after cardiac surgery. Acupunct Med. 2011;29(1):16–20. doi:10.1136/aim.2010.003251
27. Ochi JW. Acupuncture instead of codeine for tonsillectomy pain in children. Int J Pediatr Otorhinolaryngol. 2013;77(12):2058–2062. doi:10.1016/j.ijporl.2013.10.008
28. Cho HK, Park IJ, Jeong YM, Lee YJ, Hwang SH. Can perioperative acupuncture reduce the pain and vomiting experienced after tonsillectomy? A meta-analysis. Laryngoscope. 2016;126(3):608–615. doi:10.1002/lary.25721
29. Oates A, Benedict KA, Sun K, Brakeman R, Lim J, Cynthia Kim C. Laser acupuncture reduces pain in pediatric kidney biopsies: a randomized controlled trial. Pain. 2017;158(1):103–109. doi:10.1097/j.pain.0000000000000734
30. Vlajkovic GP, Sindjelic RP. Emergence delirium in children: many questions, few answers. Anesth Analg. 2007;104:84–91. doi:10.1213/01.ane.0000250914.91881.a8
31. Hijikata T, Mihara T, Nakamura N, Miwa T, Ka K, Goto T. Electrical stimulation of the heart 7 acupuncture site for preventing emergence agitation in children. Eur J Anaesthesiol. 2016;33(7):535–542. doi:10.1097/EJA.0000000000000379
32. Lin YC, Tassone RF, Jahng S, et al. Acupuncture management of pain and emergence agitation in children after bilateral myringotomy and tympanostomy tube insertion. Paediatr Anaesth. 2009;19(11):1096–1101. doi:10.1111/j.1460-9592.2009.03129.x
33. Özmert S, Salman N, Sever F, et al. Acupuncture as an antiemetic in children who underwent adenoidectomy and/or tonsillectomy. Turk J Anaesthesiol Reanim. 2016;44(1):7–12. doi:10.5152/TJAR.2016.05902
34. Shin HC, Kim JS, Lee SK, et al. The effect of acupuncture on postoperative nausea and vomiting after pediatric tonsillectomy: a meta‐analysis and systematic review. Laryngoscope. 2016;126(8):1761–1767. doi:10.1002/lary.25883
35. Lu Z, Dong H, Wang Q, Xiong L. Perioperative acupuncture modulation: more than anesthesia. Br J Anaesth. 2015;115(2):183–193. doi:10.1093/bja/aev227
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.