")
Back to Journals » Integrated Blood Pressure Control » Volume 16
Undiagnosed Hypertension Among Market Salespersons in Kitgum Central Market, Northern Uganda
Authors Kilama D , Ayella DO, Asiimwe I, Nakibuuka B, Laker F, Bongomin F
Received 29 March 2023
Accepted for publication 15 July 2023
Published 18 July 2023 Volume 2023:16 Pages 37—46
DOI https://doi.org/10.2147/IBPC.S402988
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Turgay Celik
Denish Kilama,1 Daniel Okumu Ayella,1 Isaac Asiimwe,1 Betty Nakibuuka,1 Florence Laker,1 Felix Bongomin2
1Department of Public Health, Faculty of Medicine, Gulu University, Gulu, Uganda; 2Department of Medical Microbiology and Immunology, Faculty of Medicine, Gulu University, Gulu, Uganda
Correspondence: Felix Bongomin, Faculty of Medicine, Gulu University, P.O. Box 166, Gulu, Uganda, Tel +256 784523395, Email [email protected]
Introduction: Hypertension may be common among market salespersons who are mostly physically inactive throughout the day. However, the burden of hypertension in this population remains unknown. In this study, we determined the prevalence of undiagnosed hypertension and associated factors among market salesperson in Kitgum central market, Kitgum district, Northern Uganda.
Methods: A cross-sectional study, recruiting market salespersons aged 18 years or older without a prior diagnosis of hypertension or currently on anti-hypertensive therapy was conducted. A standardized questionnaire was administered, and body mass index (BMI) estimated. Hypertension was defined as two consistent measurements of systolic blood pressure ≥ 140mmHg and/or diastolic blood pressure ≥ 90mmHg measured 4 hours apart. Multivariable logistic regression analysis was performed to determine factors independently associated with undiagnosed hypertension. P< 0.05 was considered statistically significant.
Results: We enrolled 240 participants. The mean age was 39.4 ± 12.8 years. Most (83.3%, n=199) participants were female and urban dwellers (88.3%, n=212). The prevalence of undiagnosed hypertension was 16.7% (n=40). Of the 40 participants with hypertension, 16 (40%) were younger than 40 years. Factors associated with undiagnosed hypertension were, age > 50 years (adjusted odds ratio (aOR): 7.0, 95% confidence interval (CI): 1.9– 25.6, p=0.003), male gender (aOR: 4.2, 95CI: 1.5– 11.1, p=0.005), alcohol consumption (aOR: 2.6, 95CI: 1.1– 6.0, p=0.021), and being overweight (aOR: 3.6, 95CI: 1.5– 8.8, p=0.005).
Conclusion: About one in six of market salespersons had undiagnosed hypertension, with a disproportionately high burden among those younger than 40 years. A larger multi-centric study is recommended to confirm our findings.
Keywords: hypertension, market salespersons, physical activity, alcohol, Uganda
Introduction
Between 1975 and 2015, the burden of hypertension among adults rose from about 594 million cases to over a billion cases globally.1 Hypertension and other non-communicable diseases (NCD) are the leading causes of premature deaths in both high- and low-income countries.2 NCDs contribute to over 70% of annual mortality, translating to over 41 million death cases globally, with between 75% and 80% these deaths occurring in low- and middle-income countries (LMIC).2 Hypertension is the leading cardiovascular risk factor for stroke and ischaemic heart diseases in the world.3 According to the recent World Health Organization report, about 27% of the adults in sub-Saharan Africa have hypertension higher than the global average of 22%.2
Hypertension accounts for approximately 7% of the global disability adjusted life years, and about 45% of global cardiovascular morbidity and mortality.4 Hypertension contributes to about 9.4 million deaths and about 17% of the total deaths globally.1 The burden of hypertension has increased exponentially over the past few decades. However, a large proportion of those with hypertension remain undiagnosed, untreated or inadequately treated predisposing to higher risk of hypertension-related complications such as stroke and myocardial infarction.5
In Africa, the estimated number of people with hypertension has increased steadily from 54.6 million in 1990 to 92.3 million in 2000 (70% rise) and 130.2 million in 2010 (41% increase from the year 2000). This number is projected to rise to 216.8 million by the year 2030 (66% rise from the year 2010).6 In sub-Saharan Africa, the total number of individuals with hypertension was estimated to be 75 million in 2008 and projected to be at 125.5 million by 2025.7 There is a high burden of hypertension in Africa; however, over three-quarters of the cases are unaware they have hypertension.8
In Uganda, according to the findings from the National NCDs Risk Factor Survey, the overall prevalence of hypertension was 26.4%, with the northern region of the country contributing 23.3% of the individuals having hypertension.9 This study also found out that the prevalence of hypertension is high in urban area yet only 7.7% of the people with hypertension were aware of their elevated blood pressure status. Hypertension is a silent killer; therefore, early identification of subjects with undiagnosed hypertension may prevent or reduce progression of many of its serious complications. Therefore, we aimed to determine the prevalence and factors associated with undiagnosed hypertension among market salespersons operating in Kitgum central market, Kitgum district, Uganda.
Methods
Study Design and Setting
We conducted a community-based, cross-sectional study among market salespersons (venders) in Kitgum central market, Kitgum municipality, Kitgum district in Northern Uganda. The central market has an estimated 500 salespersons. There are several items sold in the market including foods and non-food items. The market does not have a health wellness facility and all medical services are sought from either nearby clinics or Kitgum General Hospital, which is located about 2 kilometers from the market.
Study Population
We included market salespersons aged 18 years or older operating in Kitgum central market, Kitgum municipality, who provided written informed consent. We excluded pregnant women and individual with known diagnosis of hypertension or receiving anti-hypertensive medicines prescribed by a qualified physician.
Sampling Technique and Procedure
A systematic sampling method was used whereby every individual had a chance of being selected, however, if a participant was selected and found to have a known diagnosis of hypertension or were on anti-hypertensive medications, had any known heart disease, was pregnant or below 18 years, she or he was excluded from the study and the next participant was moved on to. This helped the researcher obtain samples that are representative of the population and also prevented bias as well as saved time.
Sample Size Determination
The sample size was estimated by the Kish–Leslie formula (1965). At a level of statistical significance at 95% confidence interval (standard value 1.96), prevalence of undiagnosed hypertension assumed to be 50% (since no previous study), maximum acceptable marginal error of 5% (0.05) and power of 80% gave a minimum sample size of 385 participants. Using the finite population factor for a finite population of market salesperson currently estimated at 500 in Kitgum central market, a final sample size of 240 participants was reached at, inclusive of a 10% non-response rate.
Data Collection
A semi-structured pre-tested, questionnaire was used to collect demographic and behavioral information, anthropometric and blood pressure measurements of all eligible study participants.
Data were collected on a daily basis, and all respondents were interviewed on a one-on-one basis to ensure privacy. Two different blood pressure readings were taken 4 hours apart using manual blood pressure machines with the respondent sitting upright on a firm chair and their arms at the level of the heart after resting for 5 minutes before commencement of blood pressure measurements. Average blood pressure was calculated to determine the overall blood pressure of each participant. Using a calibrated stand-on weighing scale, the weights of the participants was measured with each participant standing in an upright position on the weighing scale with feet wear off and no additional weight in the hands and pockets. Their weight was then read and recorded. The heights of the participants were obtained using a height board with the participants standing on the height meter bare footed, standing upright with the head forward and arms hanging at the side. Their maximum height was then read and recorded in meters. The BMI was then calculated by dividing weight in kilograms by height in meter squared to ascertain whether the respondent was obese or not.
Operational Definition
- Obesity: BMI >30kg/m2
- Overweight: BMI between 25 and 29.9kg/m2.
- Hypertension: A systolic blood pressure (SBP) of at least 140mmHg and/or diastolic blood pressure (DBP) of at least 90mmHg measured 4 hours apart.
Data Analysis Plan
The data was first cleaned and prepared in Microsoft Excel 2016 and then imported into STATA Software Version 17.0 for analysis. Continuous variables, such as age and blood pressure, were re-categorized into categorical outcomes using established guidelines. A bi-variable logistic regression analysis was conducted to assess the association between undiagnosed hypertension and the sociodemographic characteristics and other risk factors, and the results were presented as crude odds ratios (cOR) with their 95% confidence intervals (CI) and p-values. Independent variables that showed some evidence of association with the dependent variable at the bi-variable analysis level (p< 0.2) were included in the multi-variable logistic regression model, along with known risk factors of hypertension with borderline outcomes. Step-wise logistic regression analysis was performed adjusting for all known confounders. The results of the multi-variable logistic regression are presented as adjusted odds ratios (aOR) with their 95% CI and p-values. A p < 0.05 was considered strong evidence of an association between the independent and dependent variables. Variables with fewer than five outcomes were not included in the multi-variable regression due to data sparseness, and all variables in the model were assessed for collinearity, which was considered present if the variables had a variance inflation factor (VIF) greater than 3.
Ethical Considerations
In this study, all ethical principles related to the protection of human subjects in research were followed, as outlined in the Declaration of Helsinki. The study protocol was approved by the Gulu University Research and Ethics Committee (Approval number: GUREC-2022-378) and all study participants provided written informed consent. Permission to conduct the study was obtained from the Office of the Town Clerk of Kitgum Municipal Council, the District Health Officer for Kitgum district (DHO), and the Market Superintendent for Kitgum central market.
Results
Demographic Characteristics
We enrolled a total of 240 respondents. The mean age of all study participants was 39.4 ± 12.8 years. Most (83.3%, n=199) of the participants were female and were married (63.8%, n=153). The residence of the participants was distributed as follows: 11.67% lived in rural areas and 88.33% lived in urban areas (Table 1).
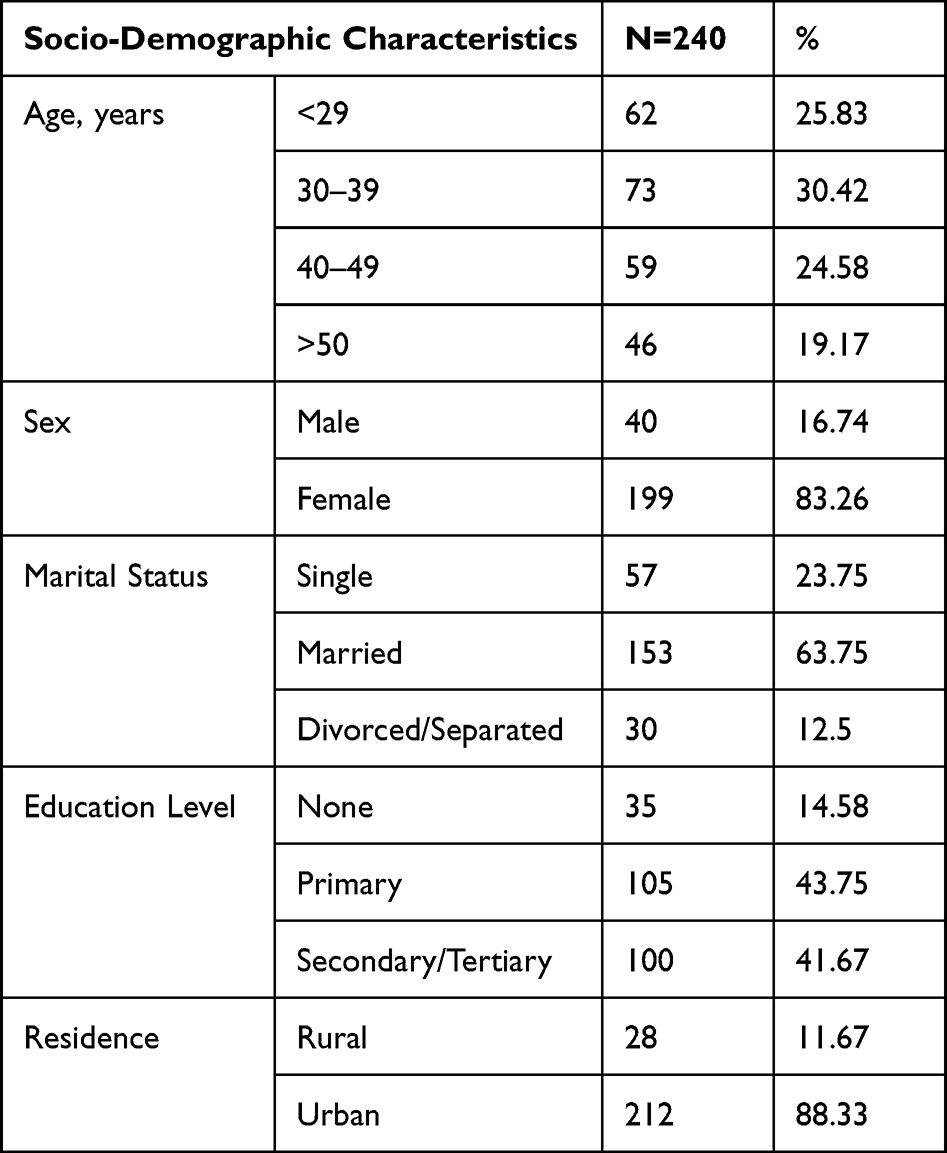 |
Table 1 Demographic Characteristics of the Study Participants |
Behavioural and Socio-Economic Characteristics of the Participants
More than half (57.5%, n=138) of the study participants had larger household size. Seventy-four (30.8%) participants practiced agriculture in addition to market sales. Overall, 181 (75.4%) participants had no history of alcohol use and 2 (0.8%) smoked cigarette. Family history of hypertension was positive for 68 (28.3%) participants and that of diabetes mellitus in 10 (4.2%) participants (Table 2).
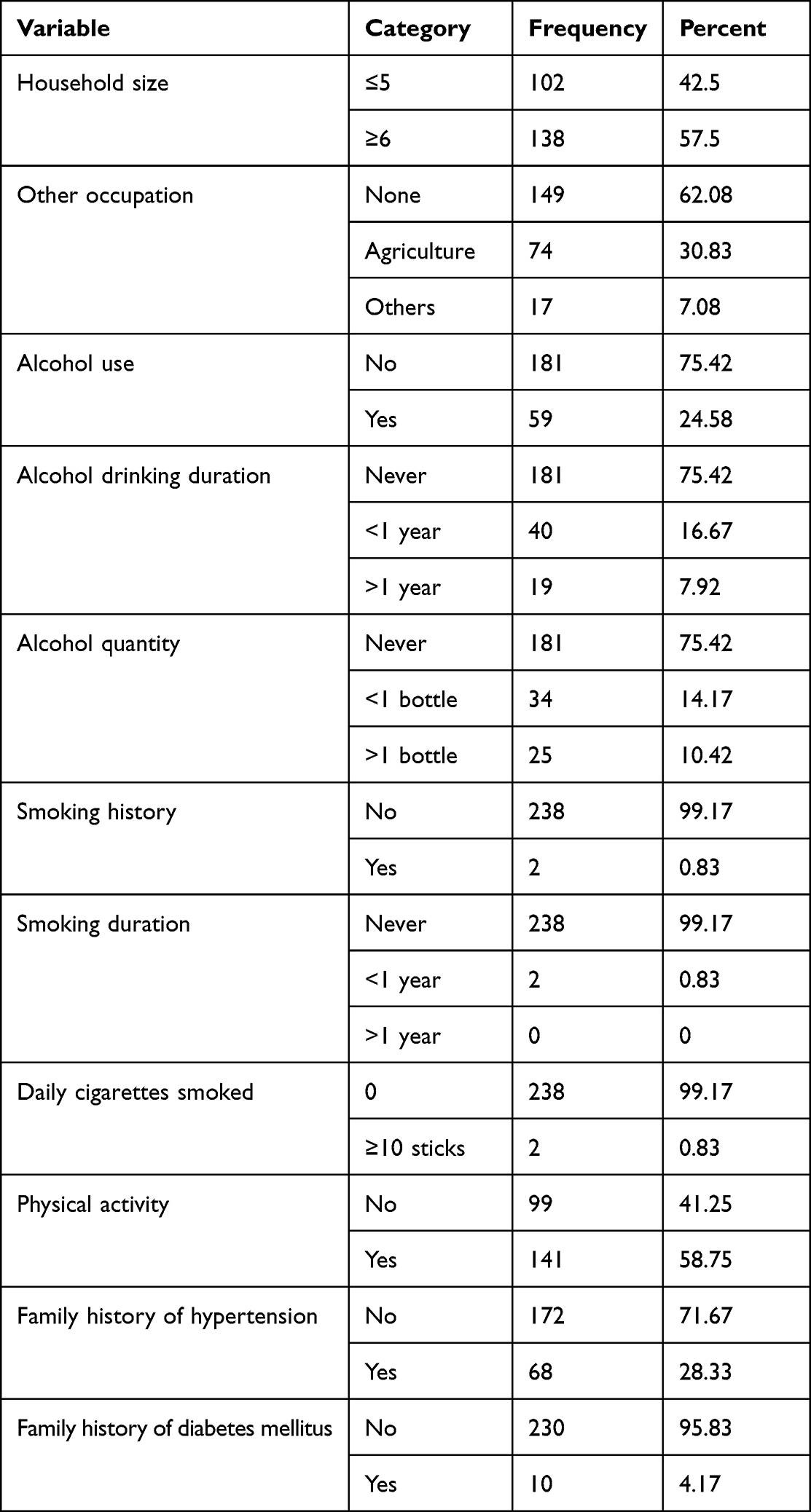 |
Table 2 Behavioural and Socio-Economic Characteristics of the Participants |
Body Mass Indices of the Participants
Of the 240 participants, 119 (49.6%) had normal BMI, 79 (32.9%) were overweight, and 42 (17.5%) were obese (Figure 1).
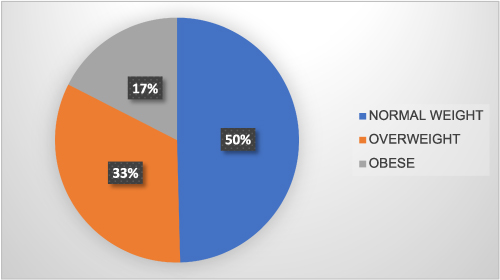 |
Figure 1 The distribution of the body mass indices of the study participants. |
Prevalence of Undiagnosed Hypertension
Overall, 40 (16.7%) participants had undiagnosed hypertension (Figure 2).
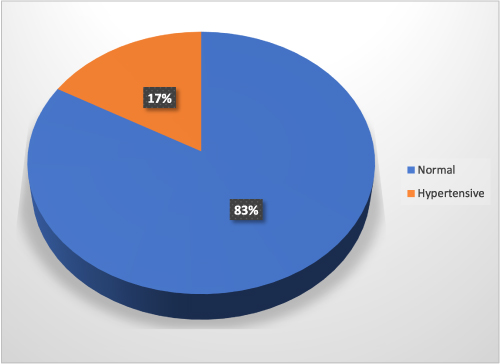 |
Figure 2 The prevalence of hypertension among the study participants. |
Factors Associated with Undiagnosed Hypertension
Factors statistically significantly associated with undiagnosed hypertension were, age >50 years (aOR: 7.0, 95CI: 1.9–25.6, p=0.003), male gender (aOR: 4.2, 95CI: 1.5–11.1, p=0.005), alcohol use (aOR: 2.6, 95CI: 1.1–6.0, p=0.021), and being overweight (aOR: 3.6, 95CI: 1.5–8.8, p=0.005), Table 3.
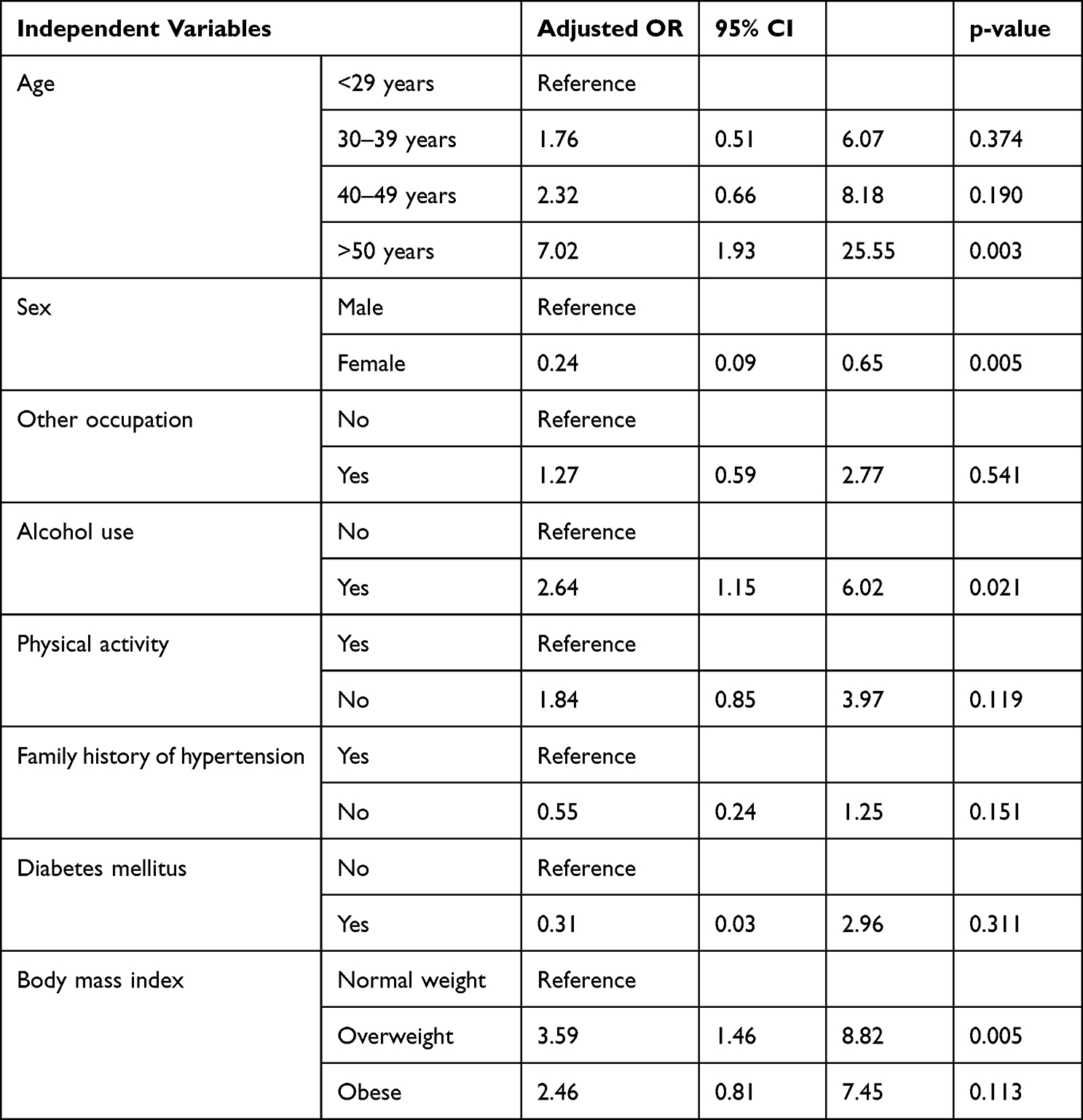 |
Table 3 Multivariable Analysis of Factors Associated with Undiagnosed Hypertension Among Market Salespersons in Kitgum, Uganda |
Discussion
In this cross-sectional study among adult market vendors in Kitgum central market, mainly consisting of urban population, the prevalence of hypertension was about 17%. Our findings show that older age, male gender, alcohol intake, and being overweight were associated with hypertension. Our findings suggest a significantly high proportion of market salesperson living with hypertension not being aware of their blood pressure status. The prevalence of hypertension of about 17% is similar to findings from previous study in western and eastern Uganda that found a prevalence of hypertension of 22%,10 This is consistent with the fact that hypertension is a silent disease with millions of people living with the disorder in the community without being diagnosed.
The prevalence of hypertension in the present study is consistent with previous reports from Ethiopia (12.3%),8 and North Central Nigeria (17.2%) of the participants who were hypertensive but not aware.2 However, our findings is not in agreement with a study done in Uganda which found a prevalence of hypertension of 27% and only 8% were aware of their diagnosis.11 A national survey in Uganda found that only 7.7% of the people with hypertension were aware of their blood pressure status.12 This difference might have been due to the differences in the study populations and the study design as our study was a cross sectional, but the study done by Majumdar and the team was retrospective, while the study by Gawattude and his team was a nationwide survey, while our study only investigated market salesperson. A study recruiting individuals from a rural community in Sudan found the prevalence of undiagnosed hypertension of about 38.2%,13 a similar study in Nigeria among market traders,14 and to another study, where the prevalence of undiagnosed hypertension was 42.8%.6 The variation in the study results may be due to the differences in the study population as our study was done in urban market where majority of the study participants were possibly more aware about their health status. Secondly, the low consumption of fats and sugar and high consumption of vitamins among our respondents that may explain a healthy diet which is protective for hypertension. Additionally, there has been an increasing campaign on non-communicable diseases like diabetes and hypertension which probably resulted into an increasing awareness among the people which might have resulted into some reduction in the prevalence of undiagnosed hypertension. Nevertheless, this relatively moderately low prevalence of undiagnosed hypertension with the facts that global death due to non-communicable disease being on increase compared to other causes,15 and also hypertension being a silent killer in Uganda,16 clearly point out the need for continuous campaign to create awareness about the condition to help reduce the rampant morbidity and mortality that comes as result of living with undiagnosed hypertension.
We found that the odds of having hypertension increased with age, people between the ages of 30–39 years had 76% higher odds of having hypertension as compared to those less than 29 years of age, while those 40–49 had more than twice higher odds of having hypertension compared to those <29 years. The highest odds of having hypertension were observed among participants older than 50 years. Additionally, we found that the odds of having hypertension were greater if the participant was male, had history of alcohol consumption, and was overweight which is in agreement to a study done in Wakiso district Central Uganda,17 a study done on epidemiology of hypertension in Uganda also revealed that male sex, higher BMI and advancing age were associated with hypertension12 which was in agreement with a study in sub-Saharan Africa which also revealed that older age was highly associated with hypertension.6 These findings are explained by the scientific facts that as people aged, they tend to develop hypertension as a result of increased resistance in the blood vessels.18 Therefore, the need to encourage healthy living practices among the elderly to reduce on the risks as evidence by some studies is recommended.19
The study also revealed that men are more likely to have undiagnosed hypertension compared to women which is in agreement with the finding from MEPI-CVD survey,17 to finding from another related study on hypertension which revealed that awareness about hypertension was higher among women than men;20 and results from national survey in Kenya on prevalence, awareness, treatment, and control and determinants of hypertension which showed that men were less aware of their hypertension status.1 The finding was, however, not in agreement to a related cross-sectional community-based study in Sudan which revealed a higher prevalence of undiagnosed hypertension among females (39.3%) more than among males (36.7%).13 These findings may be explained by the general poor health seeking behaviours among men unlike women. The variation in the findings above with that of South Sudan may be due to the socio-economic differences in the study population as our study involved only market vendors and male respondents were few.
This study found out that the odds of developing undiagnosed hypertension was higher in those who drink alcohol. This is in agreement with a study done on alcohol consumption, hypertension and obesity, a relationship pattern along different age groups in Uganda, which found out that hypertension prevalence ratios were higher with higher age groups, among moderate and non-drinkers but not among frequent drinkers.21 Long-term alcohol use can contribute to the pathophysiology of hypertension through multiple mechanisms, including activation of the renin-angiotensin-aldosterone system, increased sympathetic nervous system activity, oxidative stress, endothelial dysfunction, and impaired nitric oxide bioavailability, all of which promote vasoconstriction, sodium retention, volume expansion, and vascular remodelling, ultimately leading to elevated blood pressure levels. Our finding is also in agreement with that of a study carried out in Kenya in which 4485 participants were recruited, and, which revealed that, harmful use of alcohol among other factors like older age, higher body mass index were factors associated with hypertension,1 another study in Ethiopia.22 Furthermore, this finding was in agreement with the results from a country-wide survey on socio-demographic and lifestyle factors associated with hypertension in Nigeria which found out that alcohol consumption was associated with hypertension23 and a cross-sectional national population-based survey which showed that past month binge drinking was associated with hypertension.24
This study found out that overweight of the respondents had almost fourfold higher odds of developing undiagnosed hypertension compared to normal weight respondents, followed by obese respondents who had 2.5-fold higher odds of developing undiagnosed hypertension. This finding was in agreement with findings from other studies done in Uganda,21 a 2015 study on determinants of hypertension in a young adult Ugandan population in epidemiological transition-The MEPI-CVD survey found out that Hypertension was significantly associated with obesity, male sex, and older age-group among other factors,17 A sub-Saharan Africa study,12 a cross-sectional study carried out among 6538 male partners of pregnant women participating in the healthy initiative program in north central Nigeria that noted that being overweight and obese, was associated with undiagnosed hypertension.2 This relation was also noted in a study on prevalence of hypertension and its associated risk factors in rural black population of Mthatha town, south Africa which found out that overweight/obese status among other factors was positively associated with the risk of developing hypertension.25 The findings were further noted in a study carried out at the U.N. Mehta Institute of Cardiology and Research Centre in India, where obesity was one of the major risk factors for un-diagnosed hypertension.26 This clearly shows the universality of positive association of overweight to hypertension. Therefore, a lot of effort need to be geared towards controlling weight as part of the healthy living practices to prevent hypertension.19
This study has some limitations. We were unable to investigate other laboratory factors such as cholesterol level which are known risk factors for hypertension. However, the study sample size was large enough and our study focused on a population with limited literature as most previous studies included both those who were hypertensive and those who did not know their blood pressure level.
Conclusions
In this study, we found that about one in six of market salespersons in Kitgum district had undiagnosed hypertension. Our findings are confirmatory of the fact that age, weight, sex, and alcohol intakes are highly associated with hypertension. The highest odds of having hypertension were observed among participants older than 50 years. We recommend enhanced awareness among both rural and urban population about hypertension to reduce the prevalence of undiagnosed hypertension and prevent complications.
Data Sharing Statement
All supporting data are included within the manuscript.
Ethical Approval
The study received ethical approval from the Gulu University Research and Ethics Committee (Approval number: GUREC-2022-378). All study participants provided written informed consent, and Declaration of Helsinki was observed.
Informed Consent
The participating students provided both written and verbal consent.
Acknowledgments
The authors would like to acknowledge the study participants for this study.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mohamed SF, Mutua MK, Wamai R, et al. Prevalence, awareness, treatment and control of hypertension and their determinants: results from a national survey in Kenya. BMC Public Health. 2018;18(Suppl 3). doi:10.1186/s12889-018-6052-y
2. Banigbe BF, Itanyi IU, Ofili EO, Ogidi AG, Patel D, Ezeanolue EE. High prevalence of undiagnosed hypertension among men in North Central Nigeria: results from the Healthy Beginning Initiative. PLoS One. 2020;15(11):26–37. doi:10.1371/journal.pone.0242870
3. Undavalli VK, Mp H. Prevalence of undiagnosed hypertension: a public health challenge. Int J Commun Med Public Health. 2018;5:1366. doi:10.18203/2394-6040.ijcmph20180974
4. Zeng Z, Chen J, Xiao C, Chen W. A global view on prevalence of hypertension and human develop index. Ann Glob Health. 2020;86(1):1–6.
5. Ataklte F, Erqou S, Kaptoge S, Taye B. Burden of undiagnosed hypertension in sub-saharan Africa: a systematic review and meta-analysis; 2015. Available from: https://pubmed.ncbi.nlm.nih.gov/25385758/.
6. Okello S, Muhihi A, Mohamed SF, Ameh S, Ochimana C. Hypertension prevalence, awareness, treatment, and control and predicted 10- year CVD risk: a cross-sectional study of seven communities in East and West Africa (SevenCEWA). BMC Public Health. 2020;20:1–13.
7. Twagirumukiza M, De Bacquer D, Kips JG, De Backer G, Stichele R, Van Bortel LM. Current and projected prevalence of arterial hypertension in sub-Saharan Africa by sex, age and habitat: an estimate from population studies. J Hypertens. 2011;29(7):1243–1252. doi:10.1097/HJH.0b013e328346995d
8. Wachamo D, Geleta D, Woldesemayat EM. Undiagnosed hypertension and associated factors among adults in Hawela Tula sub-city, Hawassa, Southern Ethiopia: a community-based cross-sectional study. Risk Manag Healthc Policy. 2020;13:2169–2177. doi:10.2147/RMHP.S276955
9. Guwatudde D, Mutungi G, Wesonga R, Kajjura R. The epidemiology of hypertension in Uganda: findings from the national non-communicable diseases risk factor survey. PLoS One. 2015. doi:10.1371/journal.pone.0138991
10. Lunyera J, Kirenga B, Stanifer JW, et al. Geographic differences in the prevalence of hypertension in Uganda: results of a national epidemiological study. PLoS One. 2018;13(8):1–12. doi:10.1371/journal.pone.0201001
11. Majumdar U, Nanyonga Clarke R, Moran AE, et al. Hypertension screening, prevalence, treatment, and control at a large private hospital in Kampala, Uganda: a retrospective analysis. PLOS Glob Public Health. 2022;2(5):e0000386. doi:10.1371/journal.pgph.0000386
12. Guwatudde D, Mutungi G, Wesonga R, et al. The epidemiology of hypertension in Uganda: findings from the national non-communicable diseases risk factor survey. PLoS One. 2015;10(9):1–13. doi:10.1371/journal.pone.0138991
13. Bushara SO, Noor SK, Elmadhoun WM, Sulaiman AA, Ahmed MH. Undiagnosed hypertension in a rural community in Sudan and association with some features of the metabolic syndrome: how serious is the situation? Ren Fail. 2015;37(6):1022–1026. doi:10.3109/0886022X.2015.1052951
14. Vincent GO, Adaji JO, Umeonwuka CI. Prevalence of undiagnosed hypertension among traders at a regional market in Nigeria. Ann Med Heal Serv Res. 2017;7(2):97–101.
15. Roth GA, Abate D, Abate KH, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1736–1788.
16. WHO. Hypertension Emerges as Silent Killer in Uganda. WHO; 2021.
17. Kayima J, Nankabirwa J, Sinabulya I, et al. Determinants of hypertension in a young adult Ugandan population in epidemiological transition — the MEPI-CVD survey. BMC Public Health. 2015;15:1–9.
18. Kasper D, Fauci A, Hauser S, et al. Harrison’s Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2) 20th Edition.
19. WHO. Adherence to lifestyle modification among hypertensive clients: a descriptive cross-sectional study; 2013. Available from: https://www.scirp.org/(S(vtj3fa45qm1ean45vvffcz55))/journal/paperinformation.aspx?paperid=82696.
20. Reckelhoff JF. Gender differences in hypertension; 2018. Available from: https://pubmed.ncbi.nlm.nih.gov/29406364/.
21. Tumwesigye NM, Mutungi G, Bahendeka S, et al. Alcohol consumption, hypertension and obesity: relationship patterns along different age groups in Uganda. Prev Med Rep. 2020;19:101141. doi:10.1016/j.pmedr.2020.101141
22. Policy H. Undiagnosed hypertension and associated factors among adults in Hawela Tula Sub-City, Hawassa, Southern Ethiopia: a community-based cross-sectional study. Risk Manag Healthc Policy. 2020;15:2169–2177.
23. Adeke AS, Chori BS, Neupane D, Sharman JE, Odili AN. Socio-demographic and lifestyle factors associated with hypertension in Nigeria: results from a country-wide survey. J Hum Hypertens. 2022. doi:10.1038/s41371-022-00673-1
24. Pengpid S, Peltzer K. Prevalence, awareness, treatment and control of hypertension among adults in Kenya: cross-sectional national population-based survey. East Mediter Health J. 2020;26(8):923–932.
25. Sharma JR, Mabhida SE, Myers B, et al. Prevalence of hypertension and its associated risk factors in a rural black population of Mthatha Town, South Africa. Int J Environ Res Public Health. 2021;18:1215. doi:10.3390/ijerph18031215
26. Shukla AN, Madan T, Thakkar BM, Parmar MM, Shah KH. Prevalence and predictors of undiagnosed hypertension in an apparently healthy western Indian population. Adv Epidemiol. 2015;2015:1–5. doi:10.1155/2015/649184
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.