Back to Journals » Nature and Science of Sleep » Volume 13
Understanding the Relationship Between Sleep Problems in Early Childhood and Borderline Personality Disorder: A Narrative Review
Authors Morales-Muñoz I ![]() , Durdurak BB, Bilgin A, Marwaha S, Winsper C
, Durdurak BB, Bilgin A, Marwaha S, Winsper C
Received 23 August 2021
Accepted for publication 6 December 2021
Published 20 December 2021 Volume 2021:13 Pages 2175—2202
DOI https://doi.org/10.2147/NSS.S311672
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Isabel Morales-Muñoz,1,2 Buse Beril Durdurak,1 Ayten Bilgin,3 Steven Marwaha,1,4 Catherine Winsper5
1Institute for Mental Health, School of Psychology, University of Birmingham, Birmingham, UK; 2Department of Public Health Solutions, Finnish Institute for Health and Welfare, Helsinki, Finland; 3School of Psychology, University of Kent, Canterbury, UK; 4The Barberry National Centre for Mental Health, Birmingham and Solihull Mental Health Trust, Birmingham, UK; 5Coventry and Warwickshire Partnership NHS Trust, Research and Innovation, Coventry, UK
Correspondence: Isabel Morales-Muñoz
Institute for Mental Health, School of Psychology, University of Birmingham, 52 Pritchatts Road, Birmingham, B15 2TT, UK
Email [email protected]
Objective: Recent research indicates that sleep problems in childhood precede the development of borderline personality disorder (BPD) symptoms, but the mechanisms by which sleep problems associate with BPD are still unknown. This narrative review aims to provide some potential explanations for how early sleep problems might associate with BPD.
Methods: We used the biosocial developmental model of BPD as a framework to discuss how sleep problems may associate with BPD. Articles were identified via PubMed and Embase, and papers published between January 1991 and April 2021 were extracted. Authors made a series of literature searches using the following keywords: Sleep problems, Insomnia, Nightmares, Hypothalamic–Pituitary–Adrenal Axis (HPA), Prefrontal Cortex, Family Psychopathology, Disrupted Attachment, Child Maltreatment, Impulsivity, Emotion Regulation, Internalizing, Externalizing, Rumination, Childhood, Adolescence, Young people. The inclusion criteria were published in peer-reviewed journals; human studies or reviews; published in English. The exclusion criteria were commentaries; abstracts from conferences; studies with animal samples. A total of 96 articles were included for the purpose of this review.
Results: The evidence from this review suggests that some biological factors and core features of BPD act as potential mechanisms mediating the associations between early sleep and subsequent BPD, while some family-related factors might constitute common risk factors for sleep problems and BPD.
Conclusion: The biosocial developmental model of BPD provides a plausible characterization of how sleep disruption might lead to subsequent BPD. Further research on new developmental and early intervention approaches to understand how sleep in early stages associates with BPD could have significant clinical impact on these patients and could inform targeted therapeutic interventions.
Keywords: sleep, borderline personality disorder, biosocial developmental model, childhood, adolescence, mechanisms
Introduction
Borderline Personality Disorder (BPD) is characterized by emotional instability, impulsivity, disturbed cognition, sleeplessness and states of high inner tension. Sleep problems are common in BPD and exacerbate some core symptoms, such as emotional dysregulation (ie, the inability to flexibly respond to and manage emotions).1 However, the nature of the associations between sleep problems and BPD needs exploration and is also characterized by lack of specificity (eg, sleep also associates with other mental disorders, such as depression).2 Therefore, further research is required to understand the specific role of sleep in the development and exacerbation of BPD.
It is possible that sleep problems may precede the development of BPD. Findings from two recent longitudinal studies have provided support for the existence of prospective associations between sleep problems in childhood and subsequent BPD symptoms in adolescence. First, it was shown that persistent nightmares in childhood (ie, at 2.5, 3.5, 4.8 and 6.8 years of age) were associated with more BPD symptoms in adolescence.3 Second, shorter sleep duration at 3.5 years was prospectively associated with the development of BPD symptoms in adolescence.4 Therefore, emerging evidence suggests that nightmares and specific sleep problems occurring in early childhood are prospectively associated with the development of BPD symptoms in adolescence, at least in the general population. However, the potential mechanisms/factors underlying the associations between early sleep problems and BPD are still unknown.
The biosocial developmental model of borderline personality5 provides a framework, which helps to understand the development of BPD. In this model, the authors suggest one probable pathway that leads to BPD, which begins with early vulnerability, expressed initially as impulsivity and followed by heightened emotional sensitivity. These vulnerabilities are then potentiated across development by environmental risk factors that give rise to more significant and functionally damaging emotional, behavioral, and cognitive dysregulation. In this model, several biological correlates, psychosocial risk factors and etiological hypotheses are presented. Therefore, we will use this model as a framework to discuss how sleep problems might associate with the development of BPD. More specifically, we will focus on the factors (ie, biological, psychosocial and core features) from the model with the strongest evidence for the development of BPD and that also have links with early sleep problems. Therefore, among the biological correlates, we will focus on the hypothalamic–pituitary–adrenal axis (HPA) and prefrontal cortex. Among the psychosocial risk factors, we will focus on family psychopathology, disrupted attachment and childhood maltreatment. Finally, among the core features of BPD, we will focus on impulsivity, emotion regulation, and internalizing (eg, sadness, anxiety or loneliness) and externalizing (eg, aggression or hyperactivity) symptoms. Thus, this article reviews the links between early sleep and each of these factors, as potential mechanisms and/or contributing factors explaining the association between sleep problems and subsequent BPD, and aims to answer the following research questions:
(1) What is the association between sleep and HPA in adolescence and childhood?
(2) What is the impact of sleep on the prefrontal cortex in young adulthood, adolescence and childhood?
(3) What is the association between sleep and family psychopathology in early childhood?
(4) How do sleep and disrupted attached interact in early childhood?
(5) What is the impact of childhood maltreatment on sleep in childhood, adolescence and young adulthood?
(6) What is the link between sleep and impulsivity in young adulthood, adolescence and childhood?
(7) What is the association between sleep and emotional regulation in young adulthood, adolescence and childhood?
(8) How do sleep and internalizing/externalizing symptoms associate in adolescence and childhood?
Method
A literature search was conducted via PubMed and Embase for studies published between January 1991 and April 2021. IMM and BD conducted a series of literature searches, using the following keywords in indexed fields: ‘Sleep problems’, “Insomnia”, “Nightmares”, “HPA”, “prefrontal cortex”, “family psychopathology”, “disrupted attachment”, “child maltreatment”, “impulsivity”, “emotion regulation”, “internalizing”, “externalizing” and “rumination”, together with “childhood”, “adolescence”, “young people”. The keywords of sleep problems OR insomnia OR nightmares AND childhood OR adolescence OR young people, together with one of the correlates, separately, were used in all possible permutations, and abstracts from the results of searches were assessed. Selected papers had to meet the following criteria: (1) published in peer-reviewed journals; (2) human studies or reviews on the related topic; (3) published in English. The exclusion criteria were (1) commentaries; (2) abstracts from conferences; (3) studies with animal samples. In the next step, the full text of eligible articles was obtained and assessed. After a full-text assessment of all articles by the research team, their inclusion was subjected to open discussion by the research team. Finally, a total of 96 articles were included for the purpose of this review. See Figure 1 for details of the search and selection strategy.
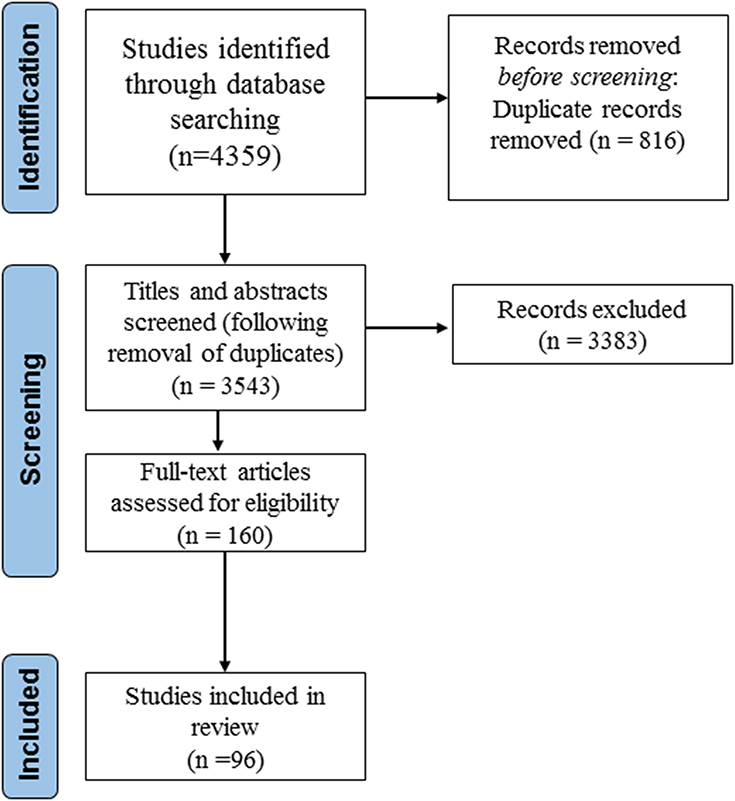 |
Figure 1 Flowchart outlining the search and selection strategy. This figure describes the search and selection for strategy for the studies included in this narrative review. Initially, 4359 studies were identified through database searching; then, 3543 studies out of them were screened for titles and abstracts; and out of these 3543 studies, 160 full-text articles were assessed for eligibility. Finally, 96 studies were included in this narrative review. |
Overlapping Biological Correlates of BPD and Sleep
Sleep and Hypothalamic–Pituitary–Adrenal Axis
The HPA axis represents a key stress response system, and growing evidence suggests that it is dysfunctional in the BPD population.6 Further, sleep, and in particular deep sleep, has an inhibitory influence on the HPA axis, whereas activation of the HPA can lead to sleeplessness.7
What is the Association Between Sleep and HPA in Adolescence and Childhood?
In adolescents, the existing studies on the topic have focused on actigraphy-based measures. For instance, in a cross-sectional study with 19-year-old healthy adolescents (N = 119), longer sleep duration was related to steeper decline in cortisol.8 Another study conducted in 265 participants with a mean age of 12.3 years old reported that actigraph-based sleep duration and sleep quality were both related to diurnal cortisol levels in boys, but not in girls.9 Further, a recent actigraphy-based cross-sectional study conducted with 55 healthy individuals aged 8–16 years found that increased HPA activity was associated with longer duration of staying awake as well as poorer sleep efficiency and greater number of awakenings.10
Further cross-sectional research has been conducted in younger ages, using both objective and subjective sleep measures. In an actigraphy-based study in eight-year-old children (N = 282), shorter average sleep duration and lower sleep efficiency were both associated with higher levels of salivary cortisol.11 Another study using sleep-electroencephalography in 113 children aged 6–10 years found that morning cortisol secretion was negatively associated with sleep duration and slow wave sleep and positively associated with the relative amount of Stage 2 sleep during the preceding night.12 Further, El-Sheikh et al reported in a study where they combined actigraphy and self-reported sleep measures in a group of nine-year-old children (N = 64) that higher levels of cortisol were related to increased subjective sleep problems and objective shorter sleep duration and poorer sleep quality.13 Pesonen et al14 examined 284 eight-year-old children and found that boys with parent-reported sleep problems (eg, difficulties in initiating and maintaining sleep, excessive somnolence, or nightmares) had lower levels of diurnal salivary cortisol. But these findings were unrelated to actual sleep duration measured by actigraphy. Finally, another study combining parent‐reported insomnia symptoms with polysomnography-based sleep duration in 327 children aged 5–12 years old showed that parent‐reported insomnia with objective short sleep duration was associated with higher cortisol levels.15
The existing studies in preschoolers have mainly used objective sleep measures. The first of these studies was done using polysomnography-based sleep recordings in 67 preschool-children aged 5.34 years and showed that the level of cortisol secretion was significantly lower in good sleepers,16 while poor sleepers16 displayed a significantly increased cortisol secretion.17 Another cross-sectional study conducted with 82 preschoolers (mean age = 4.91 years) using actigraphy showed that children with high cortisol secretion had extended sleep-onset latency and decreased sleep efficiency.18
Finally, few longitudinal studies have been conducted in infants and toddlers using parent-reported sleep measures. In a study of 322 infants aged 12–20 months, infants with a flatter diurnal cortisol slope, which is considered maladaptive, and those with a more marked morning cortisol rise had shorter nighttime sleep duration.19 Further, a longitudinal study in 51 mothers and their 18–20-month-old toddlers showed that blunted cortisol secretion patterns predicted risk for early emerging sleep problems.20
Therefore, the existing evidence suggests that associations between sleep problems and HPA axis dysfunction are evident in young ages, from adolescence to infancy. And this evidence has been supported using both subjective and objective sleep measures. More specifically, it seems that sleep difficulties are associated with increased cortisol levels, and consequently with increased HPA axis activity, in early stages of the development. However, further longitudinal studies are still needed and there is still some inconsistency concerning the associations between objective sleep duration and cortisol levels. In addition, little is known yet about the directionality of these associations. Within the context of the associations between early sleep problems and subsequent BPD symptoms, which is the focus of this review, sleep difficulties in early childhood might increase HPA axis activity, which would consequently lead to BPD symptomatology. However, further specific studies on this topic are required to test this pathway.
Sleep and Prefrontal Cortex
A number of studies have described abnormal prefrontal cortex in individuals with BPD.21 For example, reduced glucose metabolism in the prefrontal cortex has been reported in BPD patients (mean age = 34.2 years old).22 Further, BPD patients (aged 20–43 years old) demonstrated decreased metabolism in anterior cingulate and prefrontal cortex.23 In addition, some adolescents with BPD had structural alterations in frontolimbic regions.24 Concerning the role that sleep problems may have in the prefrontal cortex, there is evidence that the prefrontal cortex is particularly sensitive to sleep deprivation and benefits from good sleep practices.25 However, most of the existing evidence comes from studies in adults with a limited number of studies focusing on young people.
What is the Impact of Sleep on the Prefrontal Cortex in Young Adulthood, Adolescence and Childhood?
A cross-sectional study of 20 young subjects (age range 17–23) using functional magnetic resonance imaging (fMRI) showed that sleep deprivation associated with deficits in the bilateral inferior frontal gyrus, left subthalamic nucleus and left lingual gyrus.24 Further, a recent cross-sectional study with 25 healthy young adults and adolescents (age range = 12–22) using actigraphy and resting-state fMRI showed that irregular sleep patterns are associated with increased network connectivity in the default mode network– specifically in the right and left lateral parietal lobule.26 In adolescents, three studies have examined the associations between sleep and brain structure. In one of these studies using structural MRI, the brain areas in which higher volume was correlated with longer sleep duration included the orbitofrontal cortex, prefrontal and temporal cortex, precuneus, and supramarginal gyrus.27 Another cross-sectional study conducted in 177 adolescents (mean age 14.4 years), the medial prefrontal cortex correlated both with bedtime and wake-up times.28 A third study conducted in forty-six adolescents using a functional MRI scan during which they completed a cognitive control and risk taking task found that adolescents who reported poorer sleep also exhibited less recruitment of the dorsolateral prefrontal cortex during cognitive control.29
So far, only two studies have examined the associations between sleep and brain areas in children. In a cross-sectional study in 15 male children (ages 7–11 years), shorter sleep duration contributed to neural alterations of brain regions involved in the regulation of emotion and reward processing (including prefrontal areas).30 In a longitudinal study from the Generation R cohort, mothers reported sleep disturbances in 720 children at ages 2 months, 1.5, 2, 3, and 6 years and T1-weighted MRI images were used to assess brain structure at 7 years. The authors reported that more adverse developmental course of childhood sleep disturbances was associated with smaller grey matter volumes and thinner dorsolateral prefrontal cortex.31 Therefore, there is still limited research examining the specific effects of sleep in prefrontal brain areas in young ages. Among the existing evidence, the studies support those findings from adult research and suggest that sleep problems have an impact on the prefrontal cortex. However, further studies in this area are still needed and especially longitudinal studies and manipulation studies in young children and infants. The current evidence, and specially the one that comes from sleep deprivation studies, supports the notion that early sleep problems might have an impact in prefrontal areas, and subsequently, impairments at this cortical level might underlie the development of BPD symptoms.
Overlapping Psychosocial Risk Factors for BPD and Sleep
Sleep and Family Psychopathology
There is convincing evidence that the families of patients with BPD have greater rates of psychopathology (eg, depressive, substance abuse, or antisocial disorders) than the families of healthy controls.32 This may be due to the familial risk and heritability observed in BPD patients33 or due to the maladaptive parenting strategies frequently experienced by BPD patients.34 Research investigating the links between offspring sleep and parental psychopathology has been limited. Most studies in this area are related to maternal depression, and more specifically in the perinatal and postnatal period. Further, all these studies have mainly focused on the effects of parental mental health on their offspring’s sleep during childhood or infancy, and thus for this specific section, we will focus here on these stages.
What is the Association Between Sleep and Family Psychopathology in Early Childhood?
Concerning the effect that parental mental health has in sleep development in early childhood, and in relation to the perinatal period, depressed pregnant women seem to have newborns exhibiting higher levels of disrupted sleep.35 Similarly, prenatal maternal anxiety and depression predict more sleep problems in toddlers aged 18–30 months,36 and mothers with prenatal depression report more night awakenings in their one-year-old infants.37 There is also evidence that both mother’s prenatal and early postpartum depression symptoms associate with the emergence of infant’s sleep problems.38 With respect to postpartum depression only, depressed mothers report more infants’ sleep difficulties in the first weeks,39 and in the first year.40 Further, maternal report of infant sleep problem can be considered a significant predictor of maternal postnatal depression.41 Beyond the infancy period, in a clinical sample of mothers with mood disorders,42 sleep problems are more frequent, severe and persistent in infants of depressed mothers. Similarly, maternal symptoms of anxiety and depression during the first year of the child’s life are associated with nocturnal awakening at six and 18 months.43 Finally, infant sleeping problems relate to maternal depressive (and comorbid anxiety) disorders irrespective of maternal parity.44
Among the effects that maternal depression has in toddlers’ and/or children’s sleep functioning, most evidence supports the negative effect of maternal depression. In a large cross-sectional study using a large representative sample of 2–3 years old children, self-reported mother depressive symptomatology contributed to parent-reported sleep problems in toddlers.45 Similarly, in another cross-sectional study in 6000+ 3-to-4 years old twin pairs, maternal depression was associated with sleep problems.46 Another cross-sectional study conducted in 4–9 years old children (N=1391) corroborated the associations between maternal depression and children’s sleep disturbances also in preschoolers and school-aged children.47 Only one study, so far, has examined the effects of maternal depression in their offspring sleep using polysomnography in 64 healthy infants and showed that altered sleep structure was observed in children born from depressed mothers.48
Few studies have also examined other maternal mental health problems, rather than maternal depression. Previous research suggests that infant sleep problems are associated with poorer health in both parents.49 In a study conducted by Warren et al,50 the authors examined four- and 14-month-old infants of mothers with panic disorder (PD) and showed that infants from the four-month cohort with PD mothers had more fragmented sleep at eight months. In another study, in a sample of cocaine-exposed seven-month-old infants,51 the findings showed that exposed infants who had mothers with higher levels of anxiety showed higher levels of sleep problems. Finally, a recent study reported that several maternal risk factors during pregnancy were related to sleep difficulties in infants.52 In relation to children, in a study conducted including 182 families, bedtime behavior and daytime sleepiness seemed to be greatly affected in those children of mothers with mental health problems.53
To sum up, the existing literature has been mainly focused on maternal depression, especially perinatal and postnatal depression and mostly in children and infants. Also, most of these studies have been conducted using parent-reported sleep measures and scarce research has used objective-based sleep measures. Further, some attempts have been made to investigate the role of other maternal mental disorders on infants’ sleep. The existing evidence suggests that mother mental health problems may lead to subsequent sleep problems in their children, although there is also some evidence suggesting the opposite effect (ie, the impact of sleep on parent’s psychopathology). In the context of the development of BPD and the role of sleep, this evidence suggests that parental mental health problems could be a common risk factor for sleep problems and BPD symptoms.
Sleep and Disrupted Attachment
Problems in secure attachment formation are associated with both BPD psychopathology54 and child sleeping problems.55 Considering that attachment has been mainly studied in infancy and childhood, the studies reported in this section will cover these stages.
How Do Sleep and Disrupted Attached Interact in Early Childhood?
In a meta-analysis study conducted in 2017, the authors reported positive associations between secure infant-mother attachment and sleep efficiency and insecure-resistant attachment and sleep problems.56 Most of the studies on the topic have been conducted using a longitudinal approach. For instance, in a study using objective measures of sleep and attachment in 62 middle-class families, children with secure attachment subsequently slept more and had higher sleep efficiency than those with insecure attachment.57 In another longitudinal study using parent-reported sleep measures in 134 mother–child dyads between six and 36 months,58 it was shown that children with disorganized attachment had prospectively shorter sleep duration, later bedtime, and more awakenings. In another longitudinal study where attachment at 18 months and children’s actigraph-based and parent-reported sleep quality at 24 months were examined in 55 families,59 higher resistance predicted longer wake duration at night.
Longitudinal studies in infants have also reported the association between attachment and sleep.60 For instance, information on night wakings in 93 infants showed that attachment at 12 months was related to infant night waking patterns in the first six months of life. In another longitudinal study where attachment and sleep were measured from seven to 14 months of child’s life, infants with a secure attachment had lower number of night wakings over time.61 Further, there is also evidence of the impact of sleep difficulties in subsequent disruption of attachment in early childhood. For instance, infants with insecure-resistant attachments at 15 months have greater numbers of night wakings and longer night-waking episodes at six and 15 months.62 Similarly, sleep problems in infants at three months were associated with disorganized attachment at 18 months.63
In whole, the existing evidence suggests that disruptive attachment leads to sleep difficulties in infancy and childhood, but there is also evidence that early sleep problems might impact later attachment styles, suggesting a bidirectional association between sleep and attachment. In relation to the associations between early sleep and BPD, one explanation could be that disrupted attachment may be a common risk factor for both sleep problems and BPD. But also, other potential explanation could be that early sleep problems would lead to disrupted attachment, which consequently leads to the development of BPD symptoms. Further longitudinal research on how disrupted attachment, early sleep difficulties and BPD symptoms interact with each other is still needed.
Sleep and Childhood Maltreatment
BPD associates with history of maltreatment in childhood.64 Further, childhood abuse could be also a risk factor for sleep difficulties. Although the effects of childhood maltreatment can also lead to sleep problems in adulthood,65 for this review, we will only focus on those relevant studies investigating the associations between childhood maltreatment and sleep in childhood, adolescence and young adults.
What is the Impact of Childhood Maltreatment on Sleep in Childhood, Adolescence and Young Adulthood?
In a recent study conducted in 18–22 years old young adults, childhood emotional neglect predicted insomnia symptoms.66 Further, in a recent study conducted including 181 college students, those who reported more childhood maltreatment also reported significantly lower quality sleep and felt less rested upon awakening.67 In adolescence, a study conducted in 73 subjects found that more severe childhood maltreatment was related to increased sleep disturbances.68 In another longitudinal study using 2910 adolescents aged 14–17 years old, sexual abuse, physical abuse, intimate partner violence, emotional maltreatment and physical neglect in childhood were all associated with several sleep problems in adolescence.69 Another recent study conducted in 153,547 adolescents found that physical abuse, emotional abuse, sexual abuse, physical neglect or emotional neglect associated with increased risk of sleep disturbance.70 In 1997, a study using 44 pre-pubertal children found that abused children had prolonged actigraphy-based sleep latency and decreased sleep efficiency.71
In a large population-based sample of adolescents (N = 9582), youth exposed to childhood adversity were more likely to have insomnia, with a larger risk for those exposed to interpersonal violence during early childhood or adolescence, and a clear dose–response relationship between exposure to multiple types of adversity and risk for insomnia.72 Another longitudinal study in 147 female adolescents showed that sexually abused participants reported greater rates of sleep disturbances.73 Finally, in a recent longitudinal cohort study of 2491 children at 5–9 and 10–16 years old, having an accumulation of childhood adversities significantly associated with sleep disturbances in youth 10–16 years, but not in younger children.74
Therefore, the existing evidence suggests that childhood maltreatment may lead to sleep difficulties in young adulthood, adolescence and childhood. However, most of this research has been conducted using subjective sleep measures and further research using objective-based sleep measures is needed. Within the context of the associations between early sleep and BPD, childhood maltreatment could be a common risk factor for sleep and BPD symptoms.
Core Features of BPD
Sleep and Impulsivity
Impulsivity in BPD is a central symptom.75 Further, although inadequate sleep has been linked to poor impulse control in adults, little research has investigated the role of sleep on impulsive behaviors in younger ages.
What is the Link Between Sleep and Impulsivity in Young Adulthood, Adolescence and Childhood?
In relation to the associations in young adults, one study conducted in 373 young adults (18–29 years) found that higher levels of sleepiness associated with several types of impulsivity.76 Another recent study in 13‐ to-19-year‐olds diagnosed with bipolar disorder (BD; n = 33, 16.2 years), the change in sleep duration between school days and weekends was associated with increased impulsivity.77 Further, one study conducted in 19 young adults showed that acute sleep restriction caused deregulation of cognitive control that may manifest in increased impulsivity.78
In children and adolescents, there is also some research on the associations between sleep and impulsivity. In one study conducted in 87 healthy participants (8.6 to 15.8 years),79 sleepiness following acute sleep restriction was not sufficient to produce deficits in impulsivity and sustained attention. Further, another study conducted in 1180 children (7–10 years) showed that children with sleep disorders had greater predisposition to impulsivity.80 A randomized trial using a sample of 34 typically developing children aged 7 to 11 years reported that a cumulative restriction of sleep of 54.04 minutes was associated with detectable deterioration in restless-impulsive behavior scores.81
Therefore, the existing scarce evidence from studies in young people and adolescents suggests that sleep might play a causal role in the development of impulsive behaviours, while further research is still needed to confirm whether this is also true in children. However, with the existing evidence we can hypothesize that impulsivity could be considered a mediating factor in the associations between early sleep and BPD symptoms; however, further research is still needed.
Sleep and Emotion Regulation
Emotion dysregulation is often considered a core characteristic of BPD.82 Further, there is also evidence about the associations between emotion regulation and sleep, such as the developmental cascade model in which sleep problems have a persistent negative effect on emotional regulation, which in turn contributes to ongoing sleep problems and poorer attentional regulation in children over time.83 In recent years, there has been also an increasing research interest in understanding the bidirectional relationship between emotion and sleep. The relationship between inadequate sleep and mood has been well established in adults. However, further studies are still needed in younger ages, and especially to investigate the potential role of sleep in emotion regulation.
What is the Association Between Sleep and Emotion Regulation in Young Adulthood, Adolescence and Childhood?
In a recent cross-sectional study conducted in young people (20 years old), distraction and reappraisal (ie, two emotion regulation strategies) were impaired by sleep deprivation.84 Another sleep deprivation study with 50 healthy adolescents, aged 14–17, confirmed that several nights of sleep restriction adversely affects adolescents’ ability to regulate their emotions.85 In another manipulation study, but this time in 32 children (8–12 years), modest differences in sleep duration, accumulated over few days, affected critical emotional functions in children.85 Further, a recent study showed that after two nights of sleep restriction conducted in a sample of 53 children aged 7–11 years old alterations in children’s affect, emotional arousal, facial expressions, and emotion regulation appeared.86 In young children, in a sleep restriction study conducted in 10 healthy toddlers (30–36 months),87 sleep restriction resulted in an increase in negative emotional responses.
This relationship between sleep and emotion regulation has been also tested in large representative samples of adolescents. For instance, in a nationally representative sample (N = 10,148; 13–18 years), differential relations between sleep problems and certain regulation strategies were found.88 Finally, some attempts have been conducted to specifically investigate the role of sleep problems and emotion regulation in BPD. In a study conducted in 450 undergraduates (23 years old), BPD characteristics capturing emotional dysregulation showed the strongest correlations with poor sleep quality.89 Further, a recent study conducted in 217 adolescent inpatients with self-reported measures of sleep disturbance, emotional dysregulation and BPD symptoms showed that BPD features and emotion dysregulation were significantly related to indices of sleep disturbance, but there was no empirical support for the mediating role of emotion regulation in the relation between sleep and BPD.90 Also in relation to sleep problems and emotion regulation in BPD, one study examined the level of dream disturbances (ie, nightmares) in connection with measures of emotional instability in 23 subjects diagnosed with BPD and 23 controls, and found an association between dream disturbances and levels of emotional instability in BPD patients.91
Therefore, the existing evidence supports the notion that sleep problems might have a role in the development of emotional dysregulation. In relation to the topic of this review, sleep problems in early childhood might lead to emotional dysregulation, which subsequently would lead to BPD symptoms. Therefore, emotional dysregulation could be treated as a mediating factor in the associations between early sleep and subsequent BPD. However, the potential mediation role of emotion dysregulation in the association between sleep and BPD should be further investigated, preferably using longitudinal approaches for large sample size of individuals.
Sleep and Internalizing/Externalizing Problems
BPD is highly comorbid with internalizing and externalizing psychopathology.92 Concerning sleep in childhood, one common finding is the links with internalizing and externalizing difficulties. Some studies have focused on internalizing and externalizing problems separately, while others have included both constructs together.
How Do Sleep and Internalizing/Externalizing Symptoms Associate in Adolescence and Childhood?
Concerning the associations between sleep and internalizing problems, in a study in 300 eight-year-old twin pairs, several sleep difficulties were associated with depression, and the overall association was largely influenced by genes.93 Following the research on the genetic contribution, a recent study conducted with 5111 adolescent twin pairs reported also a large genetic overlap between sleep problems and internalizing symptoms.94 Some other studies have focused on the prospective associations between sleep and internalizing symptoms. In a recent longitudinal study among 319 youth (aged 11–26 years), dysregulated sleep was bidirectionally associated with clinician-rated anxiety and depression symptom severity.95 In another recent study in 993 and 736 participants (longitudinal cohort entry age of 10/11 years), sleep duration was not longitudinally associated with internalizing problems but it was in the cross-sectional analyses.96 Further, a longitudinal study conducted in 2,510 adolescents reported the effect of sleep duration and cigarette smoking on later internalizing problems.97 Another longitudinal study conducted in 1,089 children found that bedtime but not nighttime waking problems significantly predicted adolescent internalizing problems.98 In younger ages, a recent longitudinal study conducted in 35,075 mothers of children between 1.5 and 8 years old showed a bidirectional association between subjective sleep and internalizing symptoms from toddlerhood to middle childhood.99 Further, and using actigraphy measures, a recent study conducted in 119 children assessed longitudinally at 30, 36, 42, and 54 months reported that sleep variability and late sleep timing in toddlerhood were associated with higher levels of internalizing problems.100
Regarding the research on the associations between sleep and externalizing problems, in a longitudinal study by Muratori et al in 227 children (6–10 years),101 increased sleep problems associated with worsening of inattentive and hyperactive behavioral problems one year later. Similarly, in a cross-sectional study in 8950 preschoolers, shorter nighttime sleep duration was associated with higher likelihood of parent-reported externalizing symptoms.102 Also in preschoolers, a study of 510 children aged 2 to 5 years reported that parent-reported short sleep was associated with more externalizing problems.103 Further, in a recent study conducted in 196 children aged 34–77 months externalizing problems rather than cognitive development were associated with sleep difficulties in preschool children with developmental disability.104
Most of the studies on the topic have examined the effects of sleep with both internalizing and externalizing symptoms. In adolescents, in a longitudinal study in 555 young adolescents (Mean age = 13.96), sleep problems were precursors of substance use, internalizing and externalizing problems in adolescence.105 Concerning studies in childhood, in a cohort study using data obtained every 2 years in 4983 children aged 4–5 years, bidirectional associations were found between sleep problems and externalizing but not with internalizing symptoms.106 Further, in a longitudinal study including 270 children with ADHD, aged 5–13 years, the main findings showed a weak evidence of a bidirectional relationship between sleep problems and internalizing/externalizing problems.107
In younger children, in a study conducted in 297 families with 5–6-year-old preschoolers, both short sleep duration and sleeping difficulties were associated with children’s behavioral symptoms.108 Childhood sleep problems have also been related to maternal ratings of internalizing and externalizing problems during adolescence for both boys and girls in a study with 292 boys and 94 girls from a community sample of high-risk families.109 Further, a recent study conducted in 48 boys and 74 girls aged 7–11 years reported that parental reports of sleep disturbances can be used to identify children at increased risk for internalizing and externalizing problems.110 Another study conducted in a sample of 285 elementary school students found that self-reported time in bed and sleep quality was negatively associated with internalizing and externalizing symptoms.111 In a recent longitudinal study, Williamson et al examined 4517 children recruited at birth and found that children with increased middle childhood sleep problems experienced greater internalizing and externalizing symptoms at 10–11 years.112
Also, in a recent longitudinal study with more than 1000 infants and toddlers,113 short sleep duration and more night wakings in infancy were associated with internalizing symptoms at 24 months; and more night wakings and longer sleep-onset latency in infancy with externalizing problems at 24 months. Another study in 123 toddlers reported that short sleep predicted greater externalizing behaviors a year later.114 In a 2017 study, later bedtimes and less total sleep predicted social-emotional problems in infants and toddlers.115 A larger longitudinal study conducted in 32,662 children reported that short sleep duration and frequent nocturnal awakenings at 18 months significantly predicted both concurrent and later incidence of emotional and behavioral problems at 5 years.116 In a cross-sectional study among a community sample of children and adolescents (N = 175), depressive symptoms showed a greater association with sleep problems among adolescents, while anxiety symptoms were generally associated with sleep problems in all youth.117 Similarly, a longitudinal study in 1001 toddlers from 24- to 36-months found specific relations between sleep problems and internalizing and externalizing problems during toddlerhood.118
To sum up, these findings suggest that there is a robust association between sleep problems and both internalizing and externalizing problems at different stages from infancy to young adulthood. Several studies suggest the existence of a bidirectional association, but more evidence supports the notion that sleep affects internalizing/externalizing symptoms, rather than the opposite direction. However, further research is still needed. In the context of this review, we suggest that early sleep problems might underlie the development of internalizing/externalizing problems which subsequently may lead to BPD symptoms. However, another approach could be that internalizing/externalizing symptoms are a common factor of sleep and BPD symptoms, thus further investigation is required.
Table 1 describes the key features of each of the studies included in this narrative review.
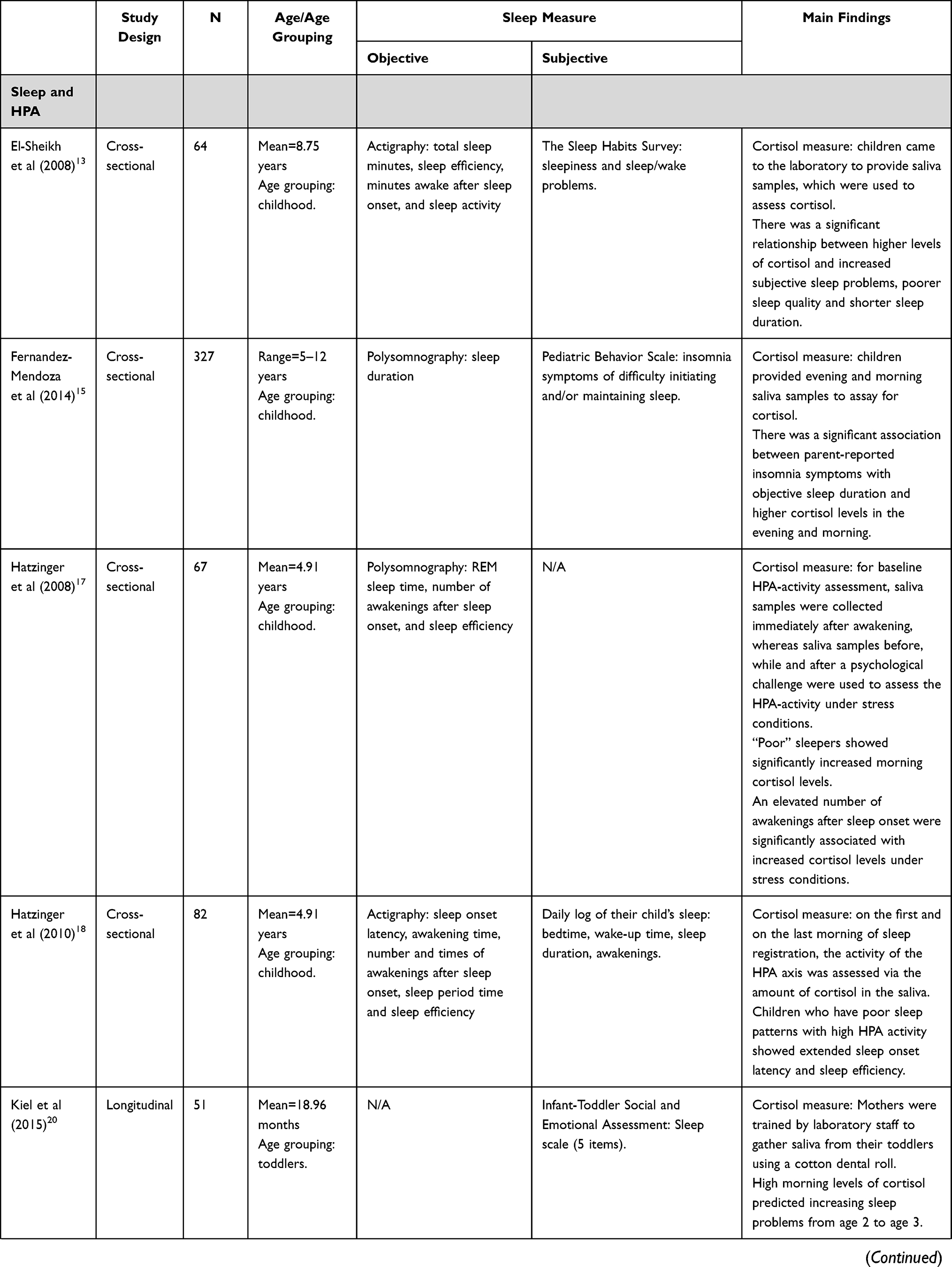 | 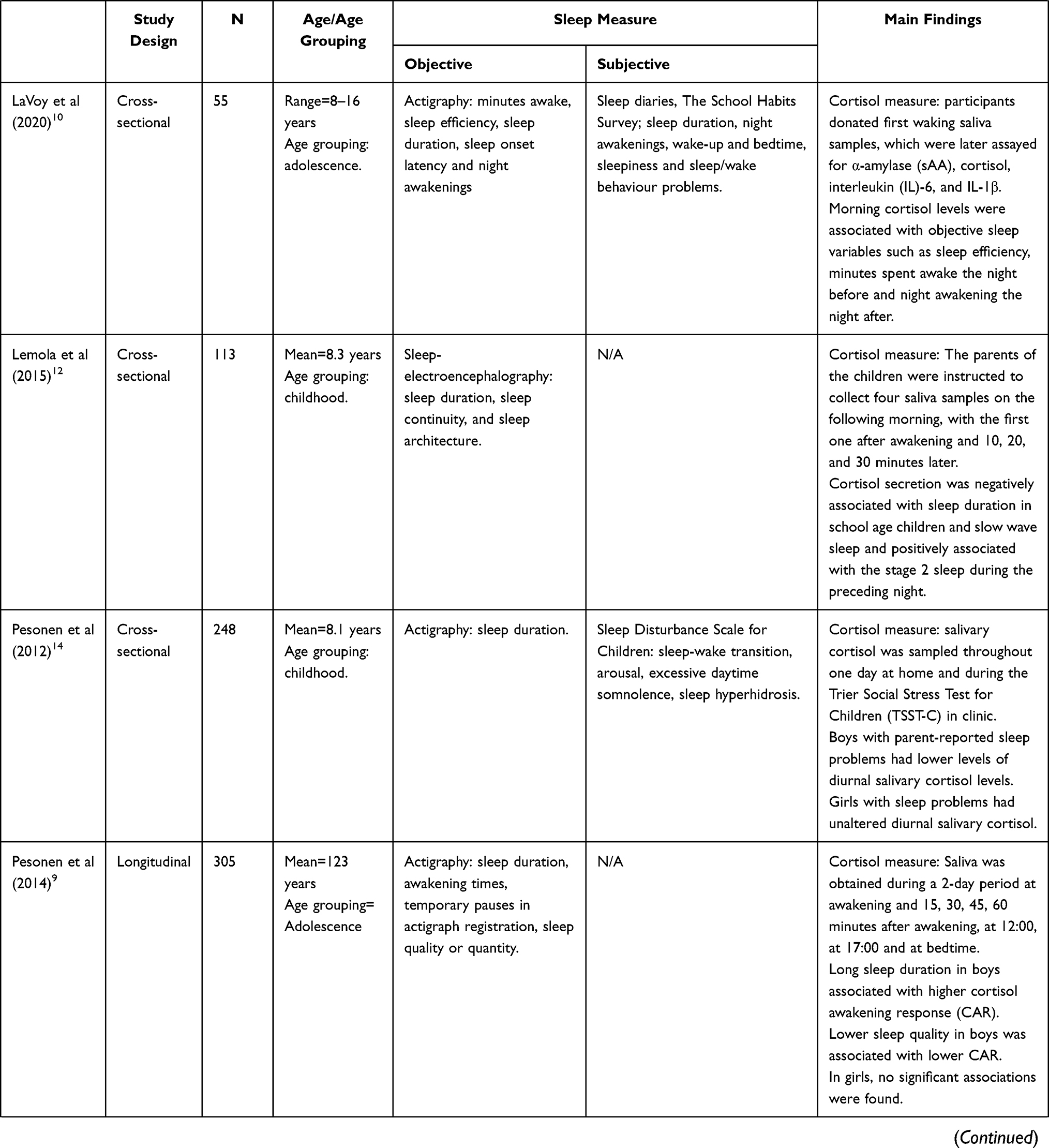 | 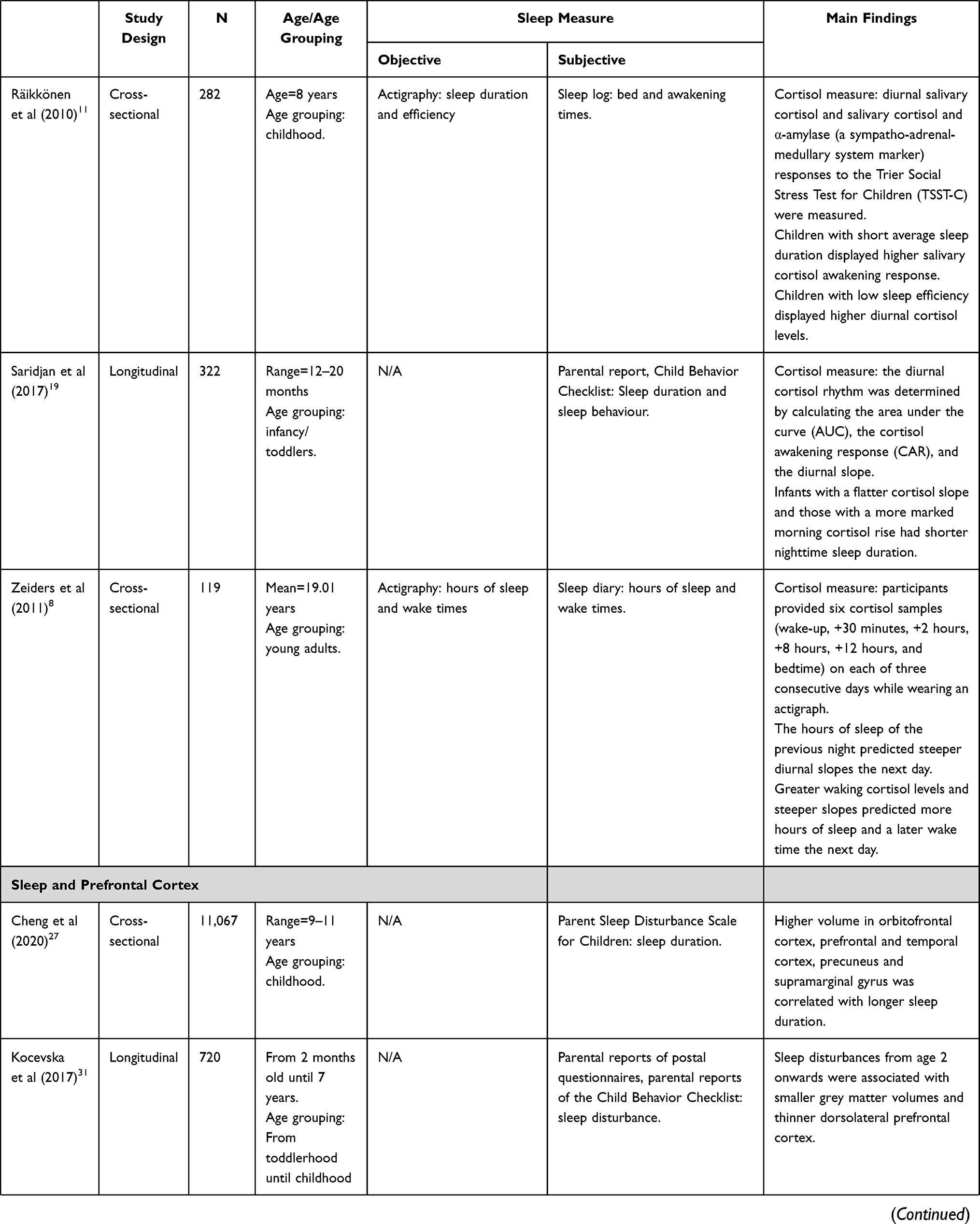 | 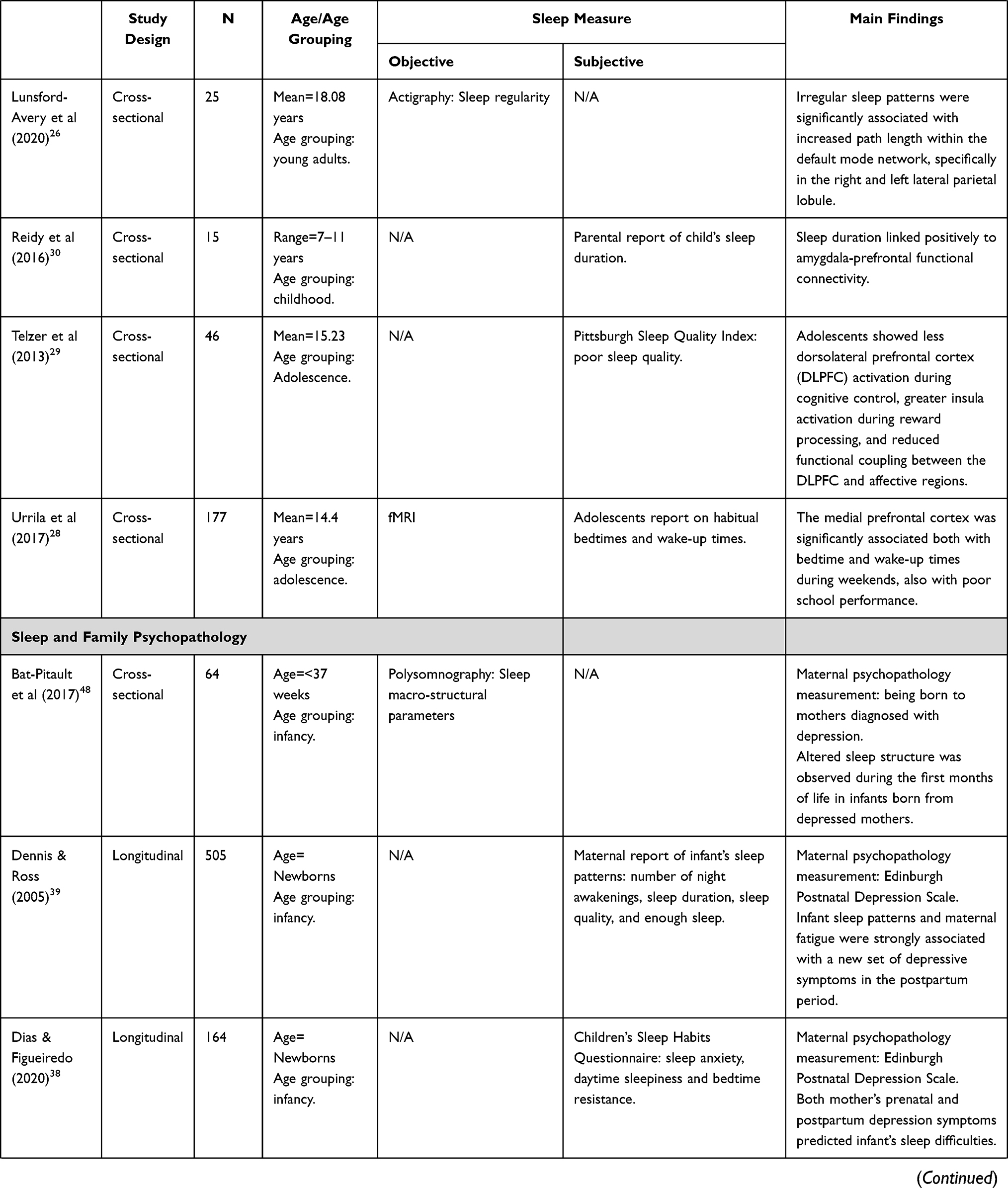 | 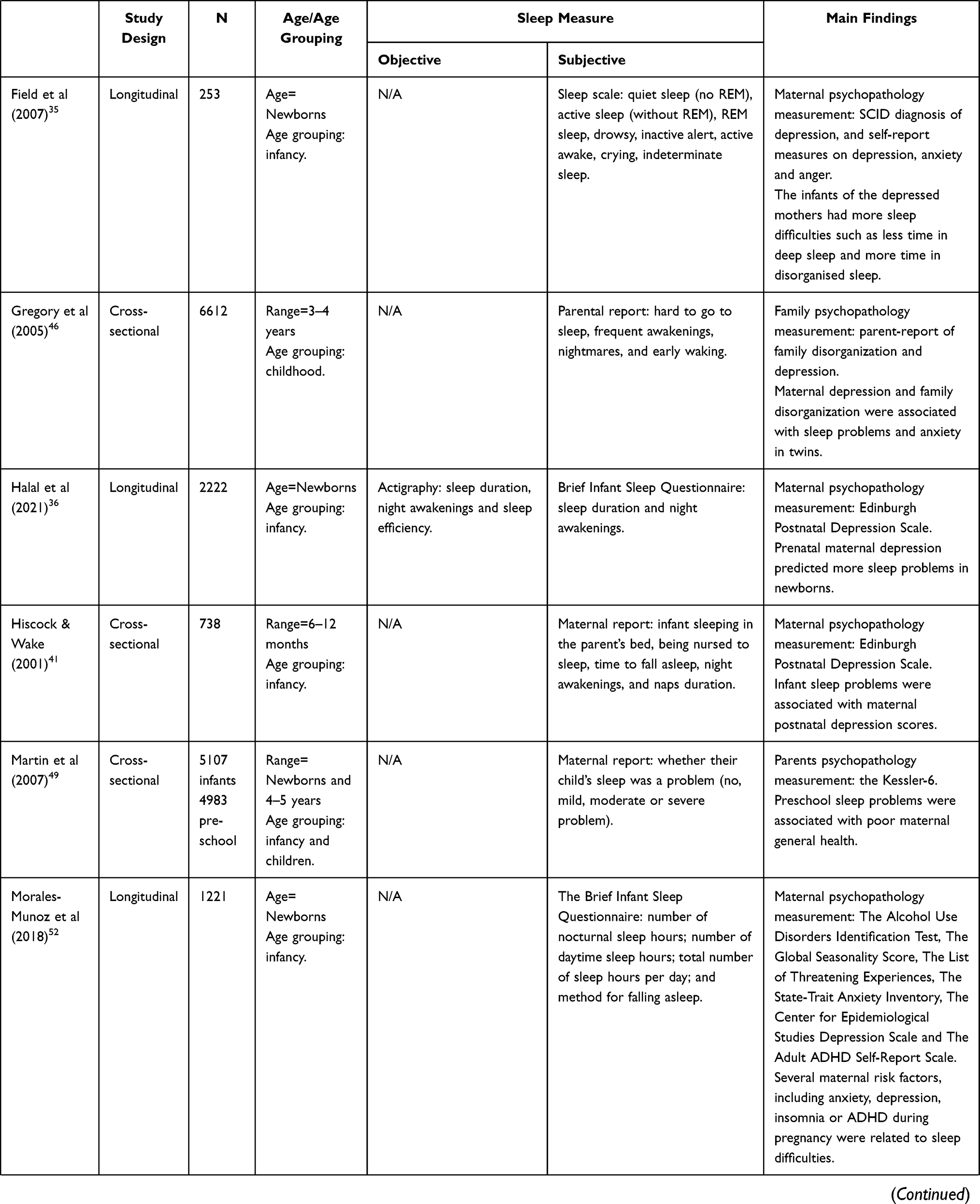 | 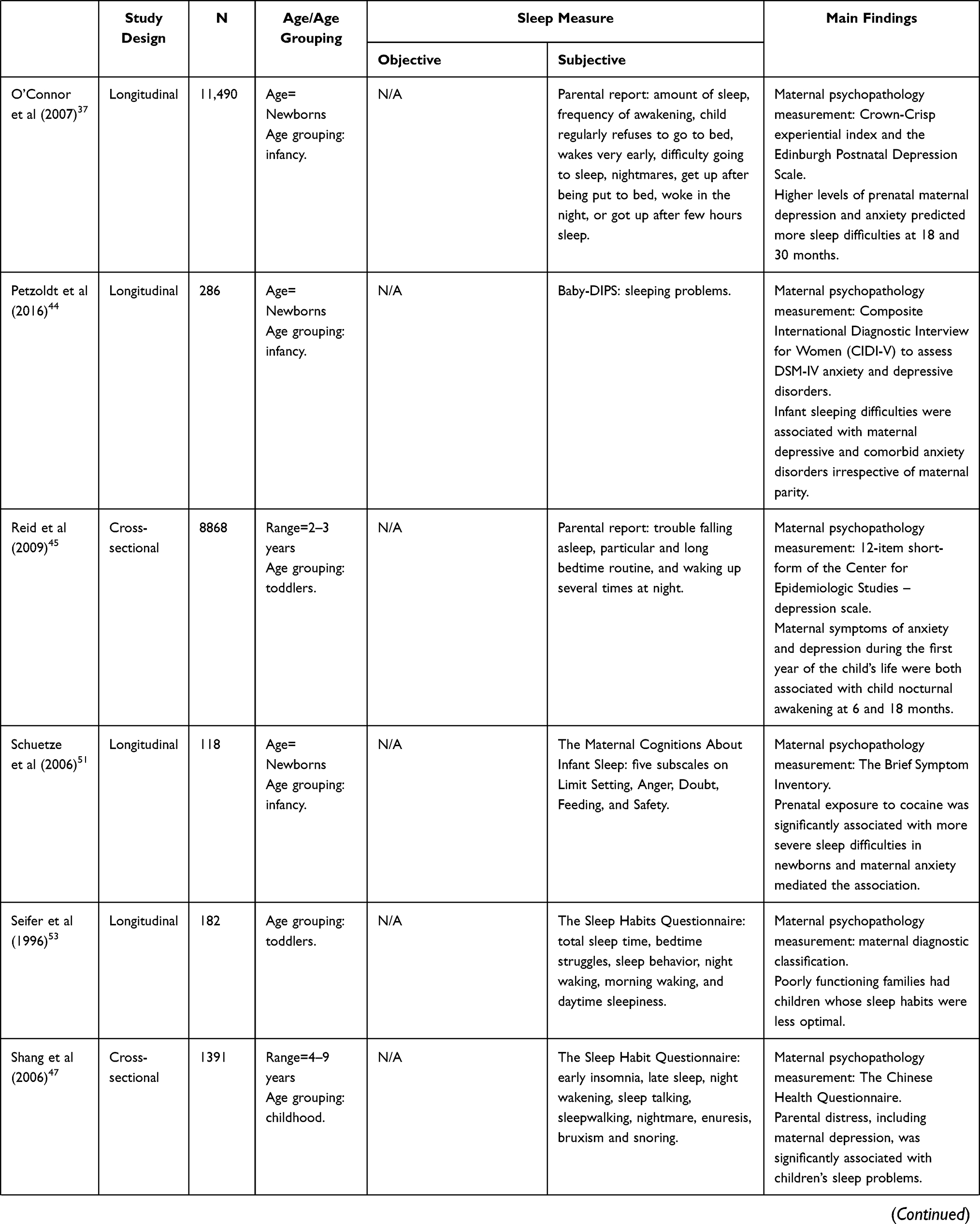 | 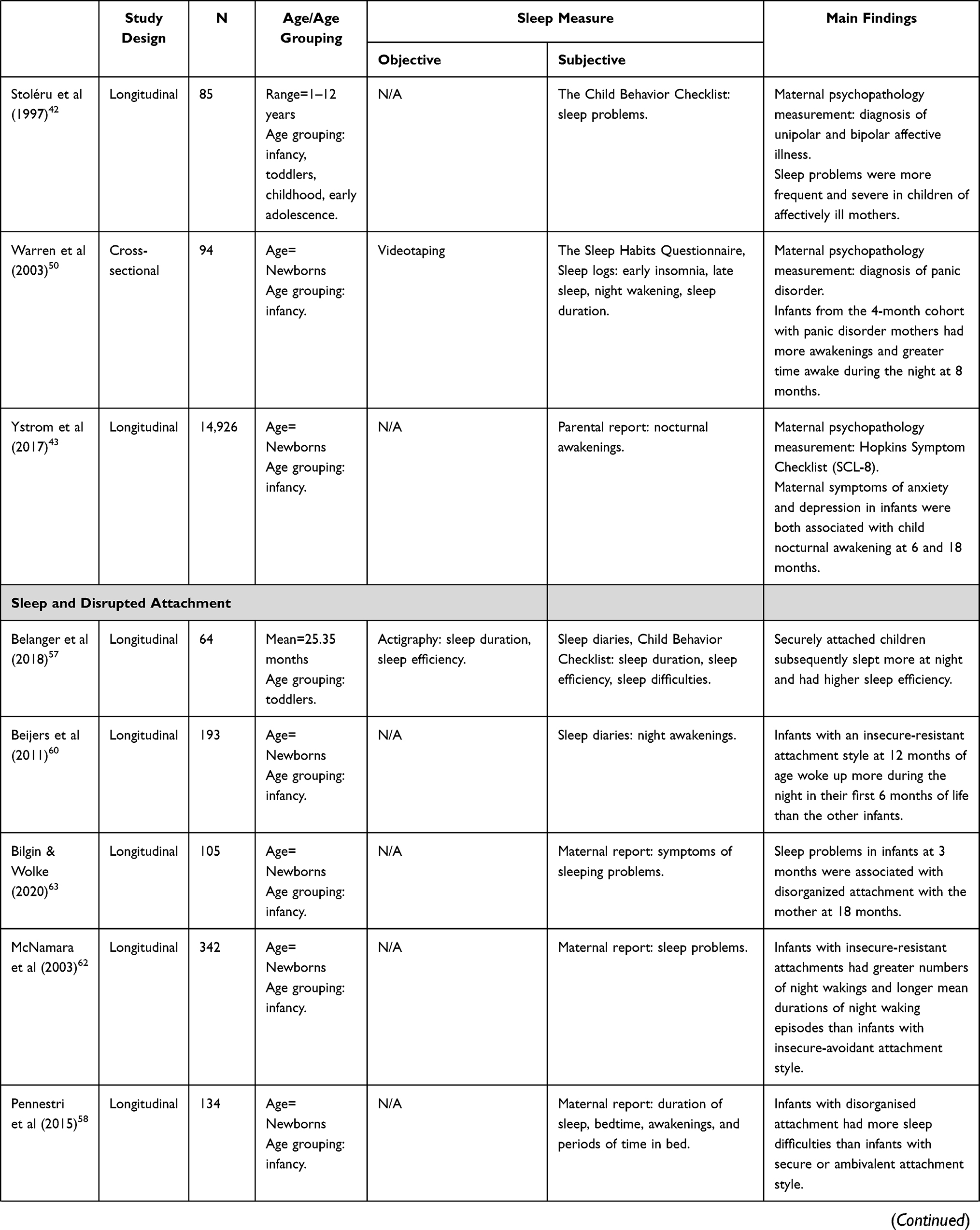 | 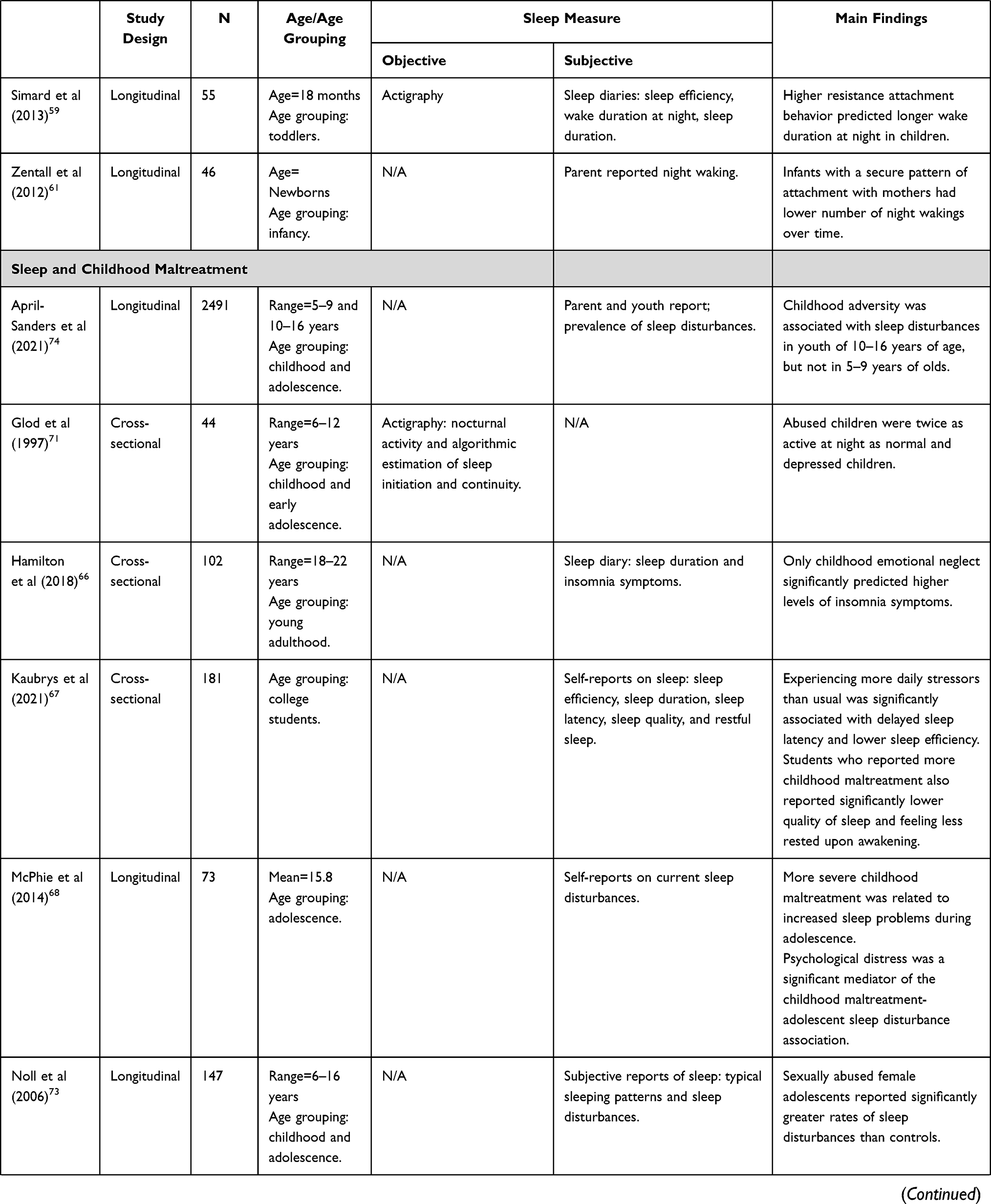 | 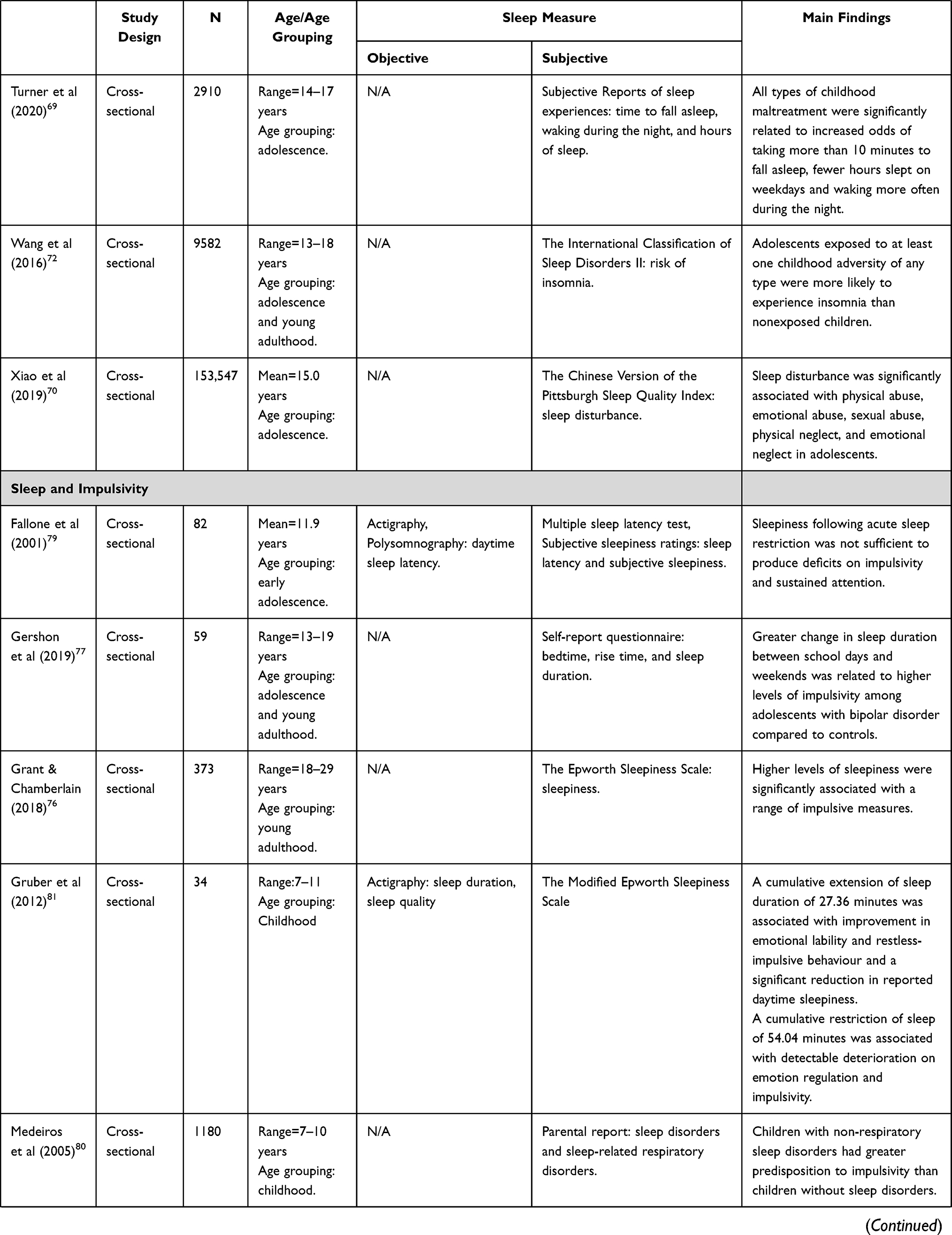 | 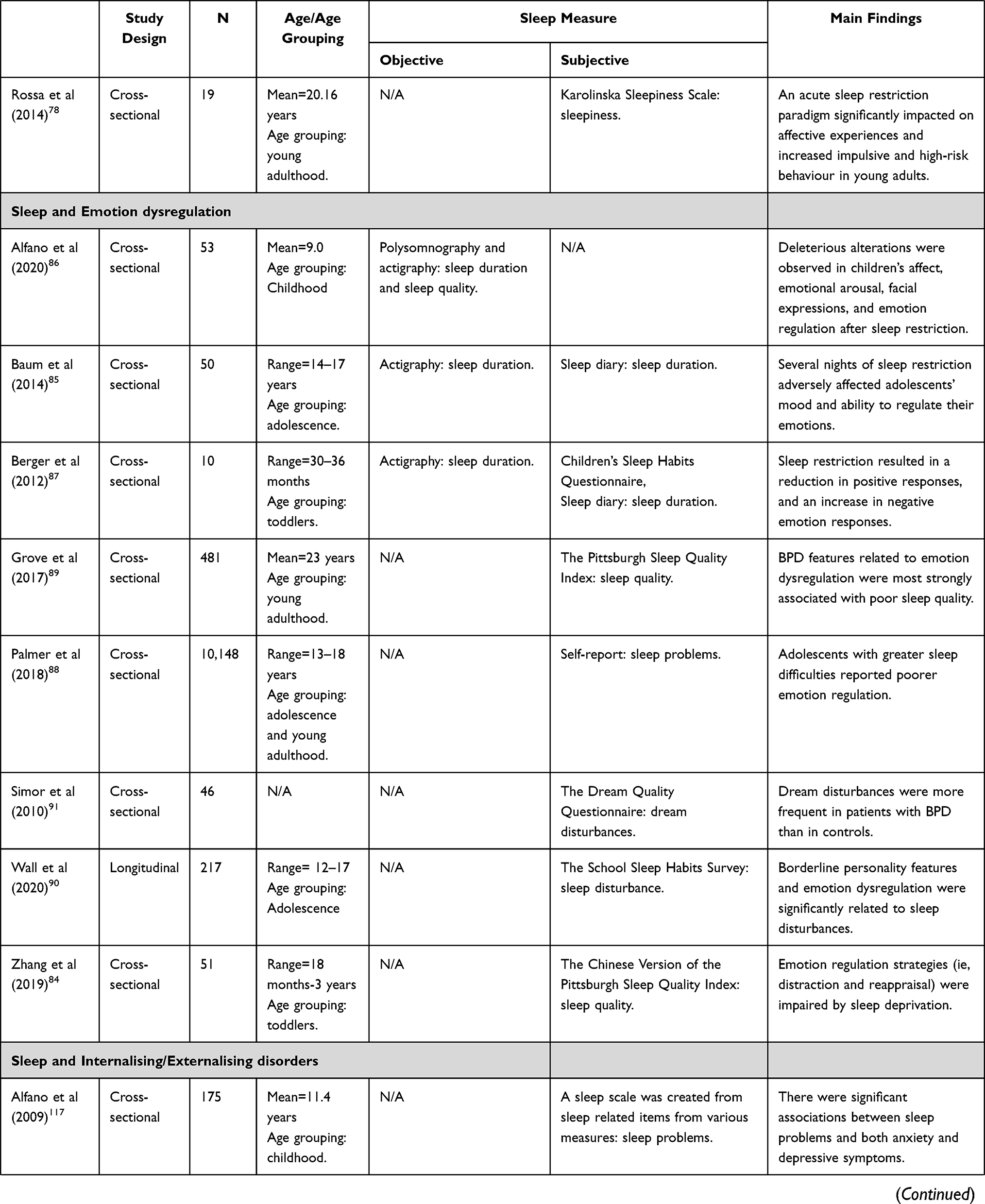 | 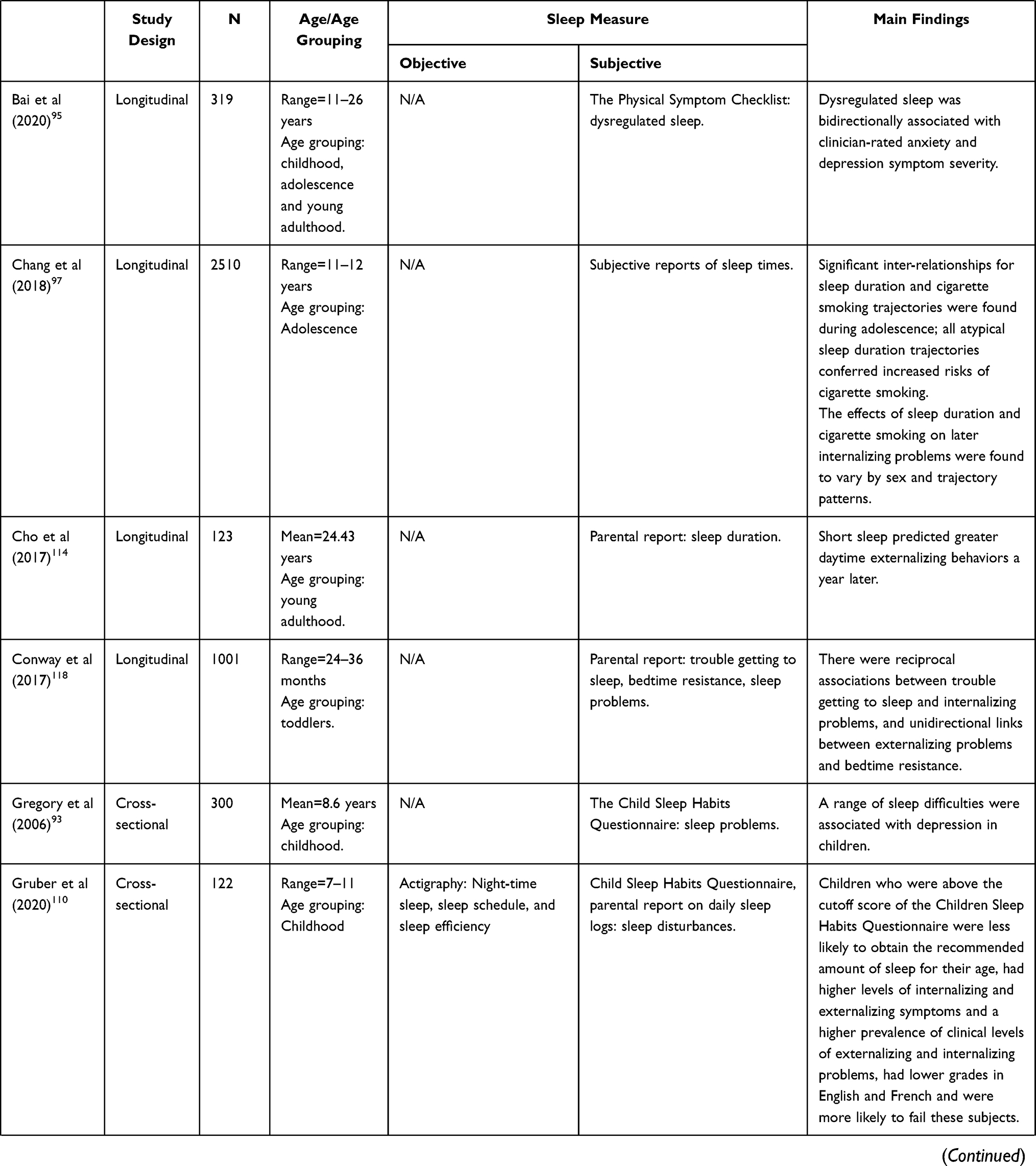 | 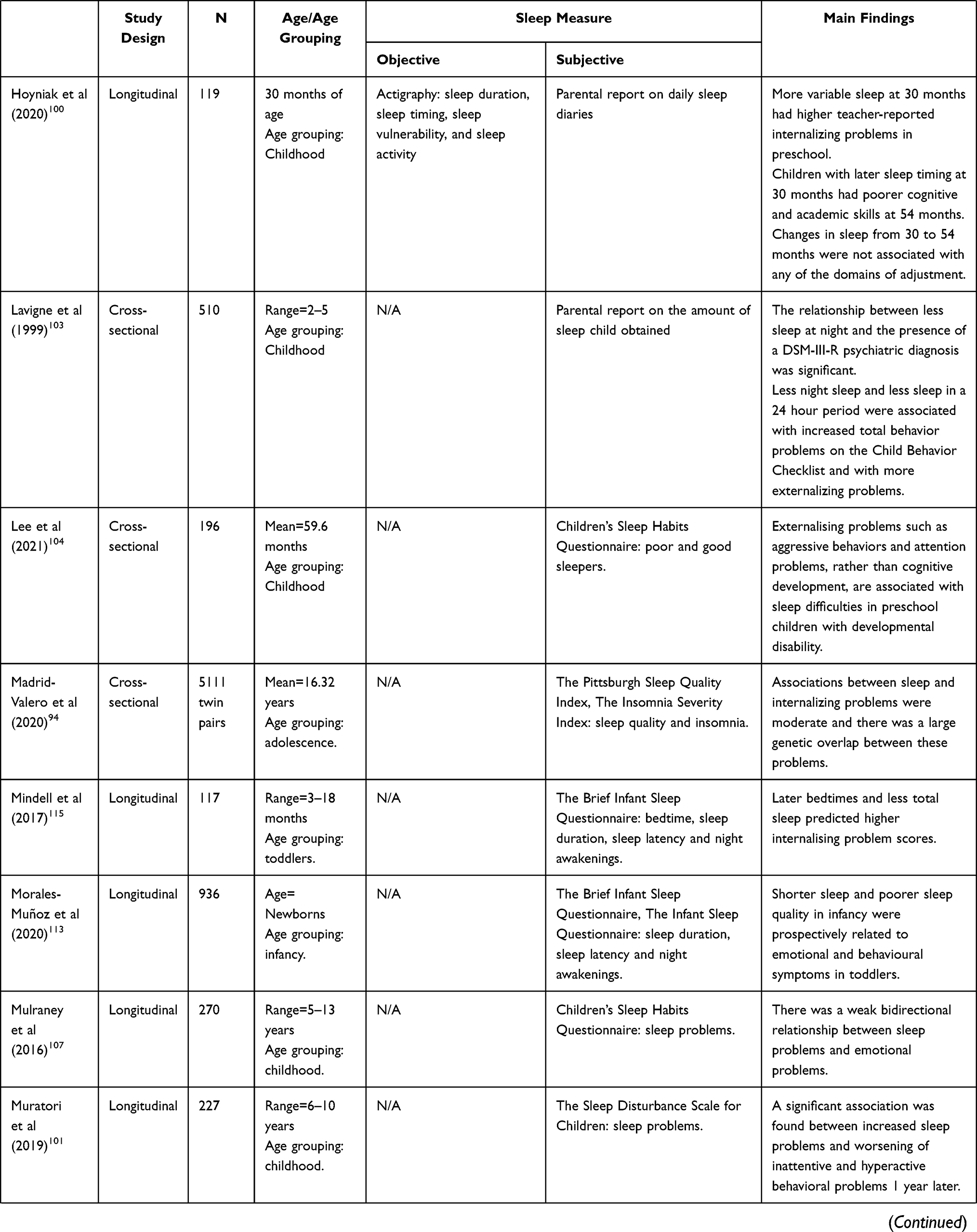 | 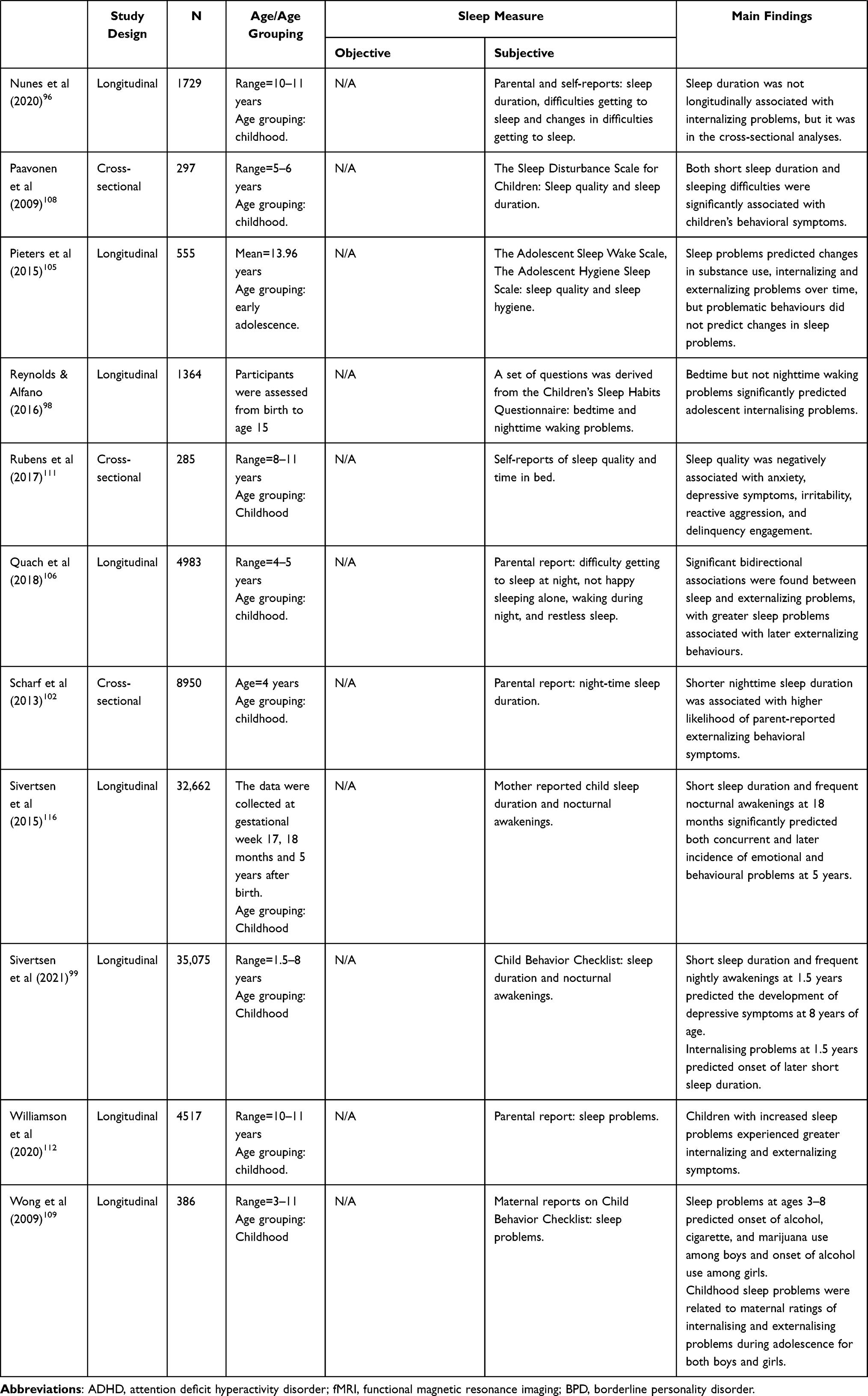 |
Table 1 Description of the Studies Included in the Narrative Review |
Conclusion
There are several pathways that could explain why sleep problems and subsequent BPD symptoms associate (see Figure 2). In this review, we used the biosocial developmental model of BPD as a framework to discuss how sleep problems might associate with the development of BPD including some of the correlates, risk and/or etiological factors described in this model. For instance, here we present evidence that supports the link between early sleep and some of the most relevant features that characterize BPD (ie, dysfunction of the HPA axis and prefrontal cortex, family psychopathology, disrupted attachment, childhood maltreatment, impulsivity, emotion regulation, and internalizing/externalizing symptoms). Therefore, this suggests that some of these factors could act as mediating factors in the associations between sleep and subsequent BPD symptoms (ie, HPA, prefrontal functioning, emotional dysregulation, impulsivity and internalizing/externalizing symptoms), while some other factors might constitute a common risk factor (ie, family psychopathology, disrupted attachment and childhood maltreatment). Other potential explanations using the biosocial developmental model of BPD could relate to the fact that early sleep problems could be an indicator of early difficulties with regulation, which in turn would predict higher levels of co-developing internalizing and externalizing symptoms which subsequently lead to the development of BPD psychopathology in adolescence.119 In addition, there is some evidence which suggests that sleep disturbance might play a causal role in some of these processes. To ascertain this causal role of sleep, experimental designs such as sleep manipulation are required.120 For instance, there is evidence for a causal link between sleep deprivation and deficits at the level of the prefrontal cortex, as well as increased impulsivity and/or dysregulation problems, using cross-sectional studies. Further, longitudinal studies partially support the fact that early sleep problems might potentially cause disruptions in the development of secure infant-mother attachment and externalizing and internalizing symptoms in childhood. These studies report that sleep problems precede the development of subsequent child and family-related difficulties, and although longitudinal designs cannot fully determine causality, their analyses meet some of the Bradford Hill criteria for causation, such as temporality and plausibility.121 However, there is still a lack of studies investigating the potential mechanisms by which sleep disturbances might lead to some of these processes. There is a need for further research on the potential underlying mechanisms such as family factors, parenting strategies, or biochemical changes in the central nervous system.
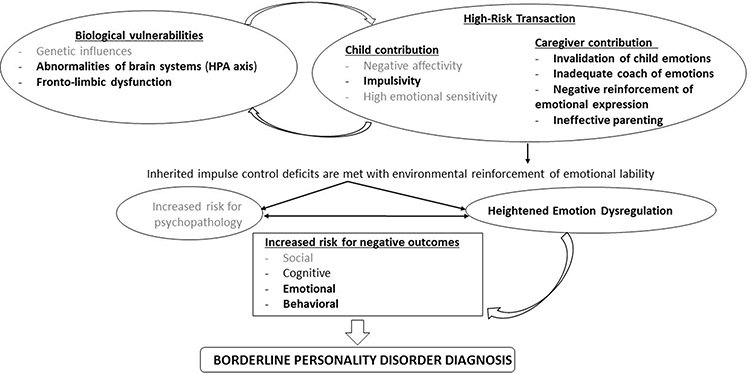 |
Figure 2 Adaptation of the biosocial developmental model of BPD. In this figure we present the pathways that could explain why sleep problems and subsequent BPD symptoms associate, using the biosocial developmental model by Crowell et al. In bold we have highlighted the processes that could have potential interaction with sleep problems and thus could explain the potential associations between sleep and BPD. These are HPA, prefrontal cortex, impulsivity, family psychopathology, disrupted attachment, childhood maltreatment, emotional dysregulation and internalizing/externalizing symptoms. |
A strength of the literature included in this review is the inclusion of a variety of processes potentially associated with sleep and which could explain the link between sleep and BPD. Therefore, this provides evidence of a number of potential mechanisms underlying these associations and allows us to advance on the current knowledge of the topic. Further, to do so, this narrative review uses as a framework the biosocial development model of BPD, which is a well-tested model of BPD. Other strength of this narrative review is the inclusion of both subjective and objective sleep measures. Further, we also included not only cross-sectional studies but also longitudinal and sleep manipulation studies, which allows to decipher the potential causal role of sleep in some of these processes. However, we only focused here on some of the processes presented in the biosocial development model of BPD, while some other potentially relevant mechanisms are not discussed in this narrative review, which constituted a disadvantage of the present work. Further, other limitations of the current review of the literature are (i) the small sample size used in some of the studies; (ii) many of the studies were cross-sectional and thus causality cannot be inferred; and (iii) a relatively short follow-up period in most of the longitudinal studies included. In addition, due to the nature of the current review (ie, narrative review), this was limited by the subjective nature of its methodology, rather than presenting the operationalization of the variables, the magnitude of effect sizes, and/or the sample sizes, which is characteristic of a systematic review. Further, we only included two databases as search engines and there was no critical appraisal of the included studies. Future studies should consider conducting a systematic review and/or meta-analysis to reveal patterns in the current literature that could not be detected through a narrative review.
Further research should specifically investigate sleep in childhood and subsequent BPD symptoms in combination with some of the relevant features described in this review. Future research should also examine whether this pathway and potential factors described here are specific to BPD or whether this could also apply to other mental health problems, such as psychosis or depression. One hypothesis could be that under the combination of specific core features of BPD, such as the ones described in this model, impairment of sleep at specific stages of the development could lead to the development of subsequent BPD symptoms, instead of other mental health problems. However, further research is still required. This will help us to better understand how early sleep associates with BPD symptoms. This would lead to a better characterization of the potential underlying mechanisms of BPD symptoms and to a better understanding of how sleep disruption in early stages might lead to the development of subsequent BPD symptoms. In addition, further studies should focus on investigating whether sleep in early childhood might play a causal role in the development of BPD symptoms. Investigation of new developmental and early intervention approaches to understand how sleep in early childhood associates with subsequent BPD symptoms could have significant clinical impact on these patients and would aid to design better targeted therapeutic interventions.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Carpenter RW, Trull TJ. Components of emotion dysregulation in borderline personality disorder: a review. Curr Psychiatry Rep. 2013;15(1):335. doi:10.1007/s11920-012-0335-2
2. Winsper C, Tang NKY, Marwaha S, et al. The sleep phenotype of borderline personality disorder: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2017;73:48–67. doi:10.1016/j.neubiorev.2016.12.008
3. Lereya ST, Winsper C, Tang NKY, Wolke D. Sleep problems in childhood and borderline personality disorder symptoms in early adolescence. J Abnorm Child Psychol. 2017;45(1):193–206. doi:10.1007/s10802-016-0158-4
4. Morales-Muñoz I, Broome MR, Marwaha S. Association of parent-reported sleep problems in early childhood with psychotic and borderline personality disorder symptoms in adolescence. JAMA Psychiatry. 2020;77(12):1256. doi:10.1001/jamapsychiatry.2020.1875
5. Crowell SE, Beauchaine TP, Linehan MM. A biosocial developmental model of borderline personality: elaborating and extending Linehan’s theory. Psychol Bull. 2009;135(3):495–510. doi:10.1037/a0015616
6. Thomas N, Gurvich C, Kulkarni J. Borderline personality disorder, trauma, and the hypothalamus-pituitary-adrenal axis. Neuropsychiatr Dis Treat. 2019;15:2601–2612. doi:10.2147/NDT.S198804
7. Nicolaides NC, Vgontzas A, Kritikou I, Chrousos G. HPA Axis and Sleep. South Dartmouth (MA): MDText.com, Inc.; 2020.
8. Zeiders KH, Doane LD, Adam EK. Reciprocal relations between objectively measured sleep patterns and diurnal cortisol rhythms in late adolescence. J Adolesc Health. 2011;48(6):566–571. doi:10.1016/j.jadohealth.2010.08.012
9. Pesonen A-K, Martikainen S, Kajantie E, et al. The associations between adolescent sleep, diurnal cortisol patterns and cortisol reactivity to dexamethasone suppression test. Psychoneuroendocrinology. 2014;49:150–160. doi:10.1016/j.psyneuen.2014.07.005
10. LaVoy EC, Palmer CA, So C, Alfano CA. Bidirectional relationships between sleep and biomarkers of stress and immunity in youth. Int J Psychophysiol. 2020;158:331–339. doi:10.1016/j.ijpsycho.2020.10.010
11. Räikkönen K, Matthews KA, Pesonen A-K, et al. Poor sleep and altered hypothalamic-pituitary-adrenocortical and sympatho-adrenal-medullary system activity in children. J Clin Endocrinol Metab. 2010;95(5):2254–2261. doi:10.1210/jc.2009-0943
12. Lemola S, Perkinson-Gloor N, Hagmann-von Arx P, et al. Morning cortisol secretion in school-age children is related to the sleep pattern of the preceding night. Psychoneuroendocrinology. 2015;52:297–301. doi:10.1016/j.psyneuen.2014.12.007
13. El-Sheikh M, Buckhalt JA, Keller PS, Granger DA. Children’s objective and subjective sleep disruptions: links with afternoon cortisol levels. Health Psychol. 2008;27(1):26–33. doi:10.1037/0278-6133.27.1.26
14. Pesonen A-K, Kajantie E, Heinonen K, et al. Sex-specific associations between sleep problems and hypothalamic-pituitary-adrenocortical axis activity in children. Psychoneuroendocrinology. 2012;37(2):238–248. doi:10.1016/j.psyneuen.2011.06.008
15. Fernandez-Mendoza J, Vgontzas AN, Calhoun SL, et al. Insomnia symptoms, objective sleep duration and hypothalamic-pituitary-adrenal activity in children. Eur J Clin Invest. 2014;44(5):493–500. doi:10.1111/eci.12263
16. Sadeh A, Raviv A, Gruber R. Sleep patterns and sleep disruptions in school-age children. Dev Psychol. 2000;36(3):291–301. doi:10.1037//0012-1649.36.3.291
17. Hatzinger M, Brand S, Perren S, et al. Electroencephalographic sleep profiles and hypothalamic-pituitary-adrenocortical (HPA)-activity in kindergarten children: early indication of poor sleep quality associated with increased cortisol secretion. J Psychiatr Res. 2008;42(7):532–543. doi:10.1016/j.jpsychires.2007.05.010
18. Hatzinger M, Brand S, Perren S, et al. Sleep actigraphy pattern and behavioral/emotional difficulties in kindergarten children: association with hypothalamic-pituitary-adrenocortical (HPA) activity. J Psychiatr Res. 2010;44(4):253–261. doi:10.1016/j.jpsychires.2009.08.012
19. Saridjan NS, Kocevska D, Luijk MPCM, Jaddoe VW, Verhulst FC, Tiemeier H. The prospective association of the diurnal cortisol rhythm with sleep duration and perceived sleeping problems in preschoolers: the generation R study. Psychosom Med. 2017;79(5):557–564. doi:10.1097/PSY.0000000000000440
20. Kiel EJ, Hummel AC, Luebbe AM. Cortisol secretion and change in sleep problems in early childhood: moderation by maternal overcontrol. Biol Psychol. 2015;107:52–60. doi:10.1016/j.biopsycho.2015.03.001
21. New AS, Hazlett EA, Buchsbaum MS, et al. Amygdala–prefrontal disconnection in borderline personality disorder. Neuropsychopharmacology. 2007;32(7):1629–1640. doi:10.1038/sj.npp.1301283
22. De La Fuente JM, Goldman S, Stanus E, et al. Brain glucose metabolism in borderline personality disorder. J Psychiatr Res. 1997;31(5):531–541. doi:10.1016/s0022-3956(97)00001-0
23. New AS, Hazlett EA, Buchsbaum MS, et al. Blunted prefrontal cortical 18fluorodeoxyglucose positron emission tomography response to meta-chlorophenylpiperazine in impulsive aggression. Arch Gen Psychiatry. 2002;59(7):621–629. doi:10.1001/archpsyc.59.7.621
24. Winsper C, Marwaha S, Lereya ST, Thompson A, Eyden J, Singh SP. A systematic review of the neurobiological underpinnings of borderline personality disorder (BPD) in childhood and adolescence. Rev Neurosci. 2016;27(8):827–847. doi:10.1515/revneuro-2016-0026
25. Muzur A, Pace-Schott EF, Hobson JA. The prefrontal cortex in sleep. Trends Cogn Sci. 2002;6(11):475–481. doi:10.1016/s1364-6613(02)01992-7
26. Lunsford-Avery JR, Damme KSF, Engelhard MM, Kollins SH, Mittal VA. Sleep/wake regularity associated with default mode network structure among healthy adolescents and young adults. Sci Rep. 2020;10(1):509. doi:10.1038/s41598-019-57024-3
27. Cheng W, Rolls E, Gong W, et al. Sleep duration, brain structure, and psychiatric and cognitive problems in children. Mol Psychiatry. 2021;26(8):3992–4003. doi:10.1038/s41380-020-0663-2
28. Urrila AS, Artiges E, Massicotte J, et al. Sleep habits, academic performance, and the adolescent brain structure. Sci Rep. 2017;7:41678. doi:10.1038/srep41678
29. Telzer EH, Fuligni AJ, Lieberman MD, Galván A. The effects of poor quality sleep on brain function and risk taking in adolescence. Neuroimage. 2013;71:275–283. doi:10.1016/j.neuroimage.2013.01.025
30. Reidy BL, Hamann S, Inman C, Johnson KC, Brennan PA. Decreased sleep duration is associated with increased fMRI responses to emotional faces in children. Neuropsychologia. 2016;84:54–62. doi:10.1016/j.neuropsychologia.2016.01.028
31. Kocevska D, Muetzel RL, Luik AI, et al. The developmental course of sleep disturbances across childhood relates to brain morphology at age 7: the generation R study. Sleep. 2017;40(1). doi:10.1093/sleep/zsw022
32. Goldman S, D’Angelo E, DeMaso D. Psychopathology in the families of children and adolescents with borderline personality disorder. Am J Psychiatry. 1993;150(12):1832–1835. doi:10.1176/ajp.150.12.1832
33. Skoglund C, Tiger A, Rück C, et al. Familial risk and heritability of diagnosed borderline personality disorder: a register study of the Swedish population. Mol Psychiatry. 2021;26(3):999–1008. doi:10.1038/s41380-019-0442-0
34. Eyden J, Winsper C, Wolke D, Broome MR, MacCallum F. A systematic review of the parenting and outcomes experienced by offspring of mothers with borderline personality pathology: potential mechanisms and clinical implications. Clin Psychol Rev. 2016;47:85–105. doi:10.1016/j.cpr.2016.04.002
35. Field T, Diego M, Hernandez-Reif M, Figueiredo B, Schanberg S, Kuhn C. Sleep disturbances in depressed pregnant women and their newborns. Infant Behav Dev. 2007;30(1):127–133. doi:10.1016/j.infbeh.2006.08.002
36. Halal CS, Bassani DG, Santos IS, et al. Maternal perinatal depression and infant sleep problems at 1 year of age: subjective and actigraphy data from a population-based birth cohort study. J Sleep Res. 2021;30(2):e13047. doi:10.1111/jsr.13047
37. O’Connor TG, Caprariello P, Blackmore ER, Gregory AM, Glover V, Fleming P. Prenatal mood disturbance predicts sleep problems in infancy and toddlerhood. Early Hum Dev. 2007;83(7):451–458. doi:10.1016/j.earlhumdev.2006.08.006
38. Dias CC, Figueiredo B. Mother’s prenatal and postpartum depression symptoms and infant’s sleep problems at 6 months. Infant Ment Health J. 2020;41(5):614–627. doi:10.1002/imhj.21869
39. Dennis C-L, Ross L. Relationships among infant sleep patterns, maternal fatigue, and development of depressive symptomatology. Birth. 2005;32(3):187–193. doi:10.1111/j.0730-7659.2005.00368.x
40. Murray L. The impact of postnatal depression on infant development. J Child Psychol Psychiatry. 1992;33(3):543–561. doi:10.1111/j.1469-7610.1992.tb00890.x
41. Hiscock H, Wake M. Infant sleep problems and postnatal depression: a community-based study. Pediatrics. 2001;107(6):1317–1322. doi:10.1542/peds.107.6.1317
42. Stoléru S, Nottelmann ED, Belmont B, Ronsaville D. Sleep problems in children of affectively ill mothers. J Child Psychol Psychiatry. 1997;38(7):831–841. doi:10.1111/j.1469-7610.1997.tb01601.x
43. Ystrom E, Hysing M, Torgersen L, Ystrom H, Reichborn-Kjennerud T, Sivertsen B. Maternal symptoms of anxiety and depression and child nocturnal awakenings at 6 and 18 months. J Pediatr Psychol. 2017;42(10):1156–1164. doi:10.1093/jpepsy/jsx066
44. Petzoldt J, Wittchen H-U, Einsle F, Martini J. Maternal anxiety versus depressive disorders: specific relations to infants’ crying, feeding and sleeping problems. Child Care Health Dev. 2016;42(2):231–245. doi:10.1111/cch.12292
45. Reid GJ, Hong RY, Wade TJ. The relation between common sleep problems and emotional and behavioral problems among 2- and 3-year-olds in the context of known risk factors for psychopathology. J Sleep Res. 2009;18(1):49–59. doi:10.1111/j.1365-2869.2008.00692.x
46. Gregory AM, Eley TC, O’Connor TG, Rijsdijk FV, Plomin R. Family influences on the association between sleep problems and anxiety in a large sample of pre-school aged twins. Pers Individ Dif. 2005;39(8):1337–1348. doi:10.1016/j.paid.2005.06.008
47. Shang C-Y, Gau SS-F, Soong W-T. Association between childhood sleep problems and perinatal factors, parental mental distress and behavioral problems. J Sleep Res. 2006;15(1):63–73. doi:10.1111/j.1365-2869.2006.00492.x
48. Bat-Pitault F, Sesso G, Deruelle C, et al. Altered sleep architecture during the first months of life in infants born to depressed mothers. Sleep Med. 2017;30:195–203. doi:10.1016/j.sleep.2016.11.018
49. Martin J, Hiscock H, Hardy P, Davey B, Wake M. Adverse associations of infant and child sleep problems and parent health: an Australian population study. Pediatrics. 2007;119(5):947–955. doi:10.1542/peds.2006-2569
50. Warren SL, Gunnar MR, Kagan J, et al. Maternal panic disorder: infant temperament, neurophysiology, and parenting behaviors. J Am Acad Child Adolesc Psychiatry. 2003;42(7):814–825. doi:10.1097/01.CHI.0000046872.56865.02
51. Schuetze P, Lawton D, Eiden RD. Prenatal cocaine exposure and infant sleep at 7 months of age: the influence of the caregiving environment. Infant Ment Health J. 2006;27(4):383–404. doi:10.1002/imhj.20097
52. Morales-Munoz I, Saarenpaa-Heikkila O, Kylliainen A, et al. The effects of maternal risk factors during pregnancy on the onset of sleep difficulties in infants at 3 months old. J Sleep Res. 2018;27(5):e12696. doi:10.1111/jsr.12696
53. Seifer R, Sameroff AJ, Dickstein S, Hayden LC. Parental psychopathology and sleep variation in children. Child Adolesc Psychiatr Clin N Am. 1996;5(3):715–727. doi:10.1016/S1056-4993(18)30358-4
54. Agrawal HR, Gunderson J, Holmes BM, Lyons-Ruth K. Attachment studies with borderline patients: a review. Harv Rev Psychiatry. 2004;12(2):94–104. doi:10.1080/10673220490447218
55. Benoit D, Zeanah CH, Boucher C, Minde KK. Sleep disorders in early childhood: association with insecure maternal attachment. J Am Acad Child Adolesc Psychiatry. 1992;31(1):86–93. doi:10.1097/00004583-199201000-00013
56. Simard V, Chevalier V, Bédard -M-M. Sleep and attachment in early childhood: a series of meta-analyses. Attach Hum Dev. 2017;19(3):298–321. doi:10.1080/14616734.2017.1293703
57. Belanger M-E, Bernier A, Simard V, Desrosiers K, Carrier J. Sleeping toward behavioral regulation: relations between sleep and externalizing symptoms in toddlers and preschoolers. J Clin Child Adolesc Psychol. 2018;47(3):366–373. doi:10.1080/15374416.2015.1079782
58. Pennestri M-H, Moss E, O’Donnell K, et al. Establishment and consolidation of the sleep-wake cycle as a function of attachment pattern. Attach Hum Dev. 2015;17(1):23–42. doi:10.1080/14616734.2014.953963
59. Simard V, Bernier A, Bélanger M-È, Carrier J. Infant attachment and toddlers’ sleep assessed by maternal reports and actigraphy: different measurement methods yield different relations. J Pediatr Psychol. 2013;38(5):473–483. doi:10.1093/jpepsy/jst001
60. Beijers R, Jansen J, Riksen-Walraven M, de Weerth C. Attachment and infant night waking: a longitudinal study from birth through the first year of life. J Dev Behav Pediatr. 2011;32(9):635–643. doi:10.1097/DBP.0b013e318228888d
61. Zentall SR, Braungart-Rieker JM, Ekas NV, Lickenbrock DM. Longitudinal assessment of sleep–wake regulation and attachment security with parents. Infant Child Dev. 2012;21(5):443–457. doi:10.1002/icd.1752
62. McNamara P, Belsky J, Fearon P. Infant sleep disorders and attachment: sleep problems in infants with insecure-resistant versus insecure-avoidant attachments to mother. Sleep Hypn. 2003;5(1):17–26.
63. Bilgin A, Wolke D. Infant crying problems and symptoms of sleeping problems predict attachment disorganization at 18 months. Attach Hum Dev. 2020;22(4):367–391. doi:10.1080/14616734.2019.1618882
64. Ibrahim J, Cosgrave N, Woolgar M. Childhood maltreatment and its link to borderline personality disorder features in children: a systematic review approach. Clin Child Psychol Psychiatry. 2018;23(1):57–76. doi:10.1177/1359104517712778
65. Greenfield EA, Lee C, Friedman EL, Springer KW. Childhood abuse as a risk factor for sleep problems in adulthood: evidence from a U.S. national study. Ann Behav Med. 2011;42(2):245–256. doi:10.1007/s12160-011-9285-x
66. Hamilton JL, Brindle RC, Alloy LB, Liu RT. Childhood trauma and sleep among young adults with a history of depression: a daily diary study. Front Psychiatry. 2018;9:673. doi:10.3389/fpsyt.2018.00673
67. Kaubrys M, Baker MR, Frazier PA, Nguyen-Feng VN. Relations among daily stressors, childhood maltreatment, and sleep in college students. J Couns Psychol. 2021;68(4):489–500. doi:10.1037/cou0000549
68. McPhie ML, Weiss JA, Wekerle C. Psychological distress as a mediator of the relationship between childhood maltreatment and sleep quality in adolescence: results from the Maltreatment and Adolescent Pathways (MAP) Longitudinal Study. Child Abuse Negl. 2014;38(12):2044–2052. doi:10.1016/j.chiabu.2014.07.009
69. Turner S, Menzies C, Fortier J, et al. Child maltreatment and sleep problems among adolescents in Ontario: a cross sectional study. Child Abuse Negl. 2020;99:104309. doi:10.1016/j.chiabu.2019.104309
70. Xiao D, Wang T, Huang Y, et al. Gender differences in the associations between types of childhood maltreatment and sleep disturbance among Chinese adolescents. J Affect Disord. 2020;265:595–602. doi:10.1016/j.jad.2019.11.099
71. Glod CA, Teicher MH, Hartman CR, Harakal T. Increased nocturnal activity and impaired sleep maintenance in abused children. J Am Acad Child Adolesc Psychiatry. 1997;36(9):1236–1243. doi:10.1097/00004583-199709000-00016
72. Wang Y, Raffeld MR, Slopen N, Hale L, Dunn EC. Childhood adversity and insomnia in adolescence. Sleep Med. 2016;21:12–18. doi:10.1016/j.sleep.2016.01.011
73. Noll JG, Trickett PK, Susman EJ, Putnam FW. Sleep disturbances and childhood sexual abuse. J Pediatr Psychol. 2006;31(5):469–480. doi:10.1093/jpepsy/jsj040
74. April-Sanders A, Duarte CS, Wang S, et al. Childhood adversity and sleep disturbances: longitudinal results in Puerto Rican children. Int J Behav Med. 2021;28(1):107–115. doi:10.1007/s12529-020-09873-w
75. Lieb K, Zanarini MC, Schmahl C, Linehan MM, Bohus M. Borderline personality disorder. Lancet (London, England). 2004;364(9432):453–461. doi:10.1016/S0140-6736(04)16770-6
76. Grant JE, Chamberlain SR. Sleepiness and impulsivity: findings in non-treatment seeking young adults. J Behav Addict. 2018;7(3):737–742. doi:10.1556/2006.7.2018.71
77. Gershon A, Johnson SL, Thomas L, Singh MK. Double trouble: weekend sleep changes are associated with increased impulsivity among adolescents with bipolar I disorder. Bipolar Disord. 2019;21(2):132–141. doi:10.1111/bdi.12658
78. Rossa KR, Smith SS, Allan AC, Sullivan KA. The effects of sleep restriction on executive inhibitory control and affect in young adults. J Adolesc Health. 2014;55(2):287–292. doi:10.1016/j.jadohealth.2013.12.034
79. Fallone G, Acebo C, Arnedt JT, Seifer R, Carskadon MA. Effects of acute sleep restriction on behavior, sustained attention, and response inhibition in children. Percept Mot Skills. 2001;93(1):213–229. doi:10.2466/pms.2001.93.1.213
80. Medeiros M, Carvalho LBC, Silva TA, Prado LBF, Prado GF. Sleep disorders are associated with impulsivity in school children aged 8 to 10 years. Arq Neuropsiquiatr. 2005;63(3B):761–765. doi:10.1590/s0004-282x2005000500008
81. Gruber R, Cassoff J, Frenette S, Wiebe S, Carrier J. Impact of sleep extension and restriction on children’s emotional lability and impulsivity. Pediatrics. 2012;130(5):e1155–61. doi:10.1542/peds.2012-0564
82. Daros AR, Williams GE, Meta-analysis A. Systematic review of emotion-regulation strategies in borderline personality disorder. Harv Rev Psychiatry. 2019;27(4):217–232. doi:10.1097/HRP.0000000000000212
83. Williams KE, Berthelsen D, Walker S, Nicholson JM, Developmental Cascade A. Model of behavioral sleep problems and emotional and attentional self-regulation across early childhood. Behav Sleep Med. 2017;15(1):1–21. doi:10.1080/15402002.2015.1065410
84. Zhang J, Lau EYY, Hsiao JH-W. Using emotion regulation strategies after sleep deprivation: ERP and behavioral findings. Cogn Affect Behav Neurosci. 2019;19(2):283–295. doi:10.3758/s13415-018-00667-y
85. Baum KT, Desai A, Field J, Miller LE, Rausch J, Beebe DW. Sleep restriction worsens mood and emotion regulation in adolescents. J Child Psychol Psychiatry. 2014;55(2):180–190. doi:10.1111/jcpp.12125
86. Alfano CA, Bower JL, Harvey AG, Beidel DC, Sharp C, Palmer CA. Sleep restriction alters children’s positive emotional responses, but effects are moderated by anxiety. J Child Psychol Psychiatry. 2020;61(10):1150–1159. doi:10.1111/jcpp.13287
87. Berger RH, Miller AL, Seifer R, Cares SR, LeBourgeois MK. Acute sleep restriction effects on emotion responses in 30- to 36-month-old children. J Sleep Res. 2012;21(3):235–246. doi:10.1111/j.1365-2869.2011.00962.x
88. Palmer CA, Oosterhoff B, Bower JL, Kaplow JB, Alfano CA. Associations among adolescent sleep problems, emotion regulation, and affective disorders: findings from a nationally representative sample. J Psychiatr Res. 2018;96:1–8. doi:10.1016/j.jpsychires.2017.09.015
89. Grove JL, Smith TW, Crowell SE, Ellis JH. Preliminary evidence for emotion dysregulation as a mechanism underlying poor sleep quality in borderline personality disorder. J Pers Disord. 2017;31(4):542–552. doi:10.1521/pedi_2016_30_261
90. Wall K, Vanwoerden S, Penner F, Patriquin M, Alfano CA, Sharp C. Adolescent sleep disturbance, emotion regulation and borderline features in an inpatient setting. J Clin Child Adolesc Psychol. 2020;53:1–15. doi:10.1080/15374416.2020.1772081
91. Simor P, Csóka S, Bódizs R. Nightmares and bad dreams in patients with borderline personality disorder: fantasy as a coping skill? Eur J Psychiatry. 2010;24(1):28–37. doi:10.4321/S0213-61632010000100004
92. Bailey AJ, Finn PR. Borderline personality disorder symptom comorbidity within a high externalizing sample: relationship to the internalizing-externalizing dimensional structure of psychopathology. J Pers Disord. 2020;34(6):814–826. doi:10.1521/pedi_2019_33_415
93. Gregory AM, Rijsdijk FV, Dahl RE, McGuffin P, Eley TC. Associations between sleep problems, anxiety, and depression in twins at 8 years of age. Pediatrics. 2006;118(3):1124–1132. doi:10.1542/peds.2005-3118
94. Madrid-Valero JJ, Ronald A, Shakeshaft N, Schofield K, Malanchini M, Gregory AM. Sleep quality, insomnia, and internalizing difficulties in adolescents: insights from a twin study. Sleep. 2020;43(2). doi:10.1093/sleep/zsz229
95. Bai S, Ricketts EJ, Thamrin H, et al. Longitudinal study of sleep and internalizing problems in youth treated for pediatric anxiety disorders. J Abnorm Child Psychol. 2020;48(1):67–77. doi:10.1007/s10802-019-00582-x
96. Nunes S, Campbell MK, Klar N, Reid GJ, Stranges S. Relationships between sleep and internalizing problems in early adolescence: results from Canadian National Longitudinal Survey of Children and Youth. J Psychosom Res. 2020;139:110279. doi:10.1016/j.jpsychores.2020.110279
97. Chang L-Y, Chang H-Y, Wu W-C, Lin LN, Wu -C-C, Yen -L-L. Dual trajectories of sleep duration and cigarette smoking during adolescence: relation to subsequent internalizing problems. J Abnorm Child Psychol. 2018;46(8):1651–1663. doi:10.1007/s10802-018-0414-x
98. Reynolds KC, Alfano CA. Childhood bedtime problems predict adolescent internalizing symptoms through emotional reactivity. J Pediatr Psychol. 2016;41(9):971–982. doi:10.1093/jpepsy/jsw014
99. Sivertsen B, Harvey AG, Reichborn-Kjennerud T, Ystrom E, Hysing M. Sleep problems and depressive symptoms in toddlers and 8-year-old children: a longitudinal study. J Sleep Res. 2021;30(1):e13150. doi:10.1111/jsr.13150
100. Hoyniak CP, Bates JE, McQuillan ME, et al. Sleep across early childhood: implications for internalizing and externalizing problems, socioemotional skills, and cognitive and academic abilities in preschool. J Child Psychol Psychiatry. 2020;61(10):1080–1091. doi:10.1111/jcpp.13225
101. Muratori P, Menicucci D, Lai E, et al. Linking sleep to externalizing behavioral difficulties: a longitudinal psychometric survey in a cohort of Italian school-age children. J Prim Prev. 2019;40(2):231–241. doi:10.1007/s10935-019-00547-2
102. Scharf RJ, Demmer RT, Silver EJ, Stein REK. Nighttime sleep duration and externalizing behaviors of preschool children. J Dev Behav Pediatr. 2013;34(6):384–391. doi:10.1097/DBP.0b013e31829a7a0d
103. Lavigne JV, Arend R, Rosenbaum D, et al. Sleep and behavior problems among preschoolers. J Dev Behav Pediatr. 1999;20(3):164–169. doi:10.1097/00004703-199906000-00005
104. Lee T, Kim J, Park KJ, Kim H-W. Sleep difficulties and related behavioral problems in Korean preschool children. Sleep Med. 2021;87:119–126. doi:10.1016/j.sleep.2021.09.002
105. Pieters S, Burk WJ, Van der Vorst H, Dahl RE, Wiers RW, Engels RCME. Prospective relationships between sleep problems and substance use, internalizing and externalizing problems. J Youth Adolesc. 2015;44(2):379–388. doi:10.1007/s10964-014-0213-9
106. Quach JL, Nguyen CD, Williams KE, Sciberras E. Bidirectional associations between child sleep problems and internalizing and externalizing difficulties from preschool to early adolescence. JAMA Pediatr. 2018;172(2):e174363. doi:10.1001/jamapediatrics.2017.4363
107. Mulraney M, Giallo R, Lycett K, Mensah F, Sciberras E. The bidirectional relationship between sleep problems and internalizing and externalizing problems in children with ADHD: a prospective cohort study. Sleep Med. 2016;17:45–51. doi:10.1016/j.sleep.2015.09.019
108. Paavonen EJ, Porkka-Heiskanen T, Lahikainen AR. Sleep quality, duration and behavioral symptoms among 5-6-year-old children. Eur Child Adolesc Psychiatry. 2009;18(12):747–754. doi:10.1007/s00787-009-0033-8
109. Wong MM, Brower KJ, Zucker RA. Childhood sleep problems, early onset of substance use and behavioral problems in adolescence. Sleep Med. 2009;10(7):787–796. doi:10.1016/j.sleep.2008.06.015
110. Gruber R, Somerville G, Santisteban JA. Using parental report to identify children at risk for poor sleep and daytime problems. Behav Sleep Med. 2020;18(4):460–476. doi:10.1080/15402002.2019.1613236
111. Rubens SL, Evans SC, Becker SP, Fite PJ, Tountas AM. Self-reported time in bed and sleep quality in association with internalizing and externalizing symptoms in school-age youth. Child Psychiatry Hum Dev. 2017;48(3):455–467. doi:10.1007/s10578-016-0672-1
112. Williamson AA, Mindell JA, Hiscock H, Quach J. Longitudinal sleep problem trajectories are associated with multiple impairments in child well-being. J Child Psychol Psychiatry. 2020;61(10):1092–1103. doi:10.1111/jcpp.13303
113. Morales-Muñoz I, Lemola S, Saarenpää-Heikkilä O, et al. Parent-reported early sleep problems and internalising, externalising and dysregulation symptoms in toddlers. BMJ Paediatr Open. 2020;4(1):e000622. doi:10.1136/bmjpo-2019-000622
114. Cho S, Philbrook LE, Davis EL, Buss KA. Sleep duration and RSA suppression as predictors of internalizing and externalizing behaviors. Dev Psychobiol. 2017;59(1):60–69. doi:10.1002/dev.21467
115. Mindell JA, Leichman ES, DuMond C, Sadeh A. Sleep and social-emotional development in infants and toddlers. J Clin Child Adolesc Psychol. 2017;46(2):236–246. doi:10.1080/15374416.2016.1188701
116. Sivertsen B, Harvey AG, Reichborn-Kjennerud T, Torgersen L, Ystrom E, Hysing M. Later emotional and behavioral problems associated with sleep problems in toddlers: a longitudinal study. JAMA Pediatr. 2015;169(6):575–582. doi:10.1001/jamapediatrics.2015.0187
117. Alfano CA, Zakem AH, Costa NM, Taylor LK, Weems CF. Sleep problems and their relation to cognitive factors, anxiety, and depressive symptoms in children and adolescents. Depress Anxiety. 2009;26(6):503–512. doi:10.1002/da.20443
118. Conway A, Miller AL, Modrek A. Testing reciprocal links between trouble getting to sleep and internalizing behavior problems, and bedtime resistance and externalizing behavior problems in toddlers. Child Psychiatry Hum Dev. 2017;48(4):678–689. doi:10.1007/s10578-016-0692-x
119. Winsper C, Bilgin A, Wolke D. Associations between infant and toddler regulatory problems, childhood co-developing internalising and externalising trajectories, and adolescent depression, psychotic and borderline personality disorder symptoms. J Child Psychol Psychiatry. 2020;61(2):182–194. doi:10.1111/jcpp.13125
120. Reeve S, Emsley R, Sheaves B, Freeman D. Disrupting sleep: the effects of sleep loss on psychotic experiences tested in an experimental study with mediation analysis. Schizophr Bull. 2018;44(3):662–671. doi:10.1093/schbul/sbx103
121. Fedak KM, Bernal A, Capshaw ZA, Gross S. Applying the Bradford Hill criteria in the 21st century: how data integration has changed causal inference in molecular epidemiology. Emerg Themes Epidemiol. 2015;12:14. doi:10.1186/s12982-015-0037-4
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.