")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Understanding the Experiences of Rural- and Remote-Living Patients Accessing Sub-Acute Care in Queensland: A Qualitative Descriptive Analysis
Authors Bowley JJ , Faulkner K, Finch J, Gavaghan B, Foster M
Received 5 October 2022
Accepted for publication 15 December 2022
Published 23 December 2022 Volume 2022:15 Pages 2945—2955
DOI https://doi.org/10.2147/JMDH.S391738
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jessica J Bowley,1 Kirstie Faulkner,2 Jennifer Finch,3 Belinda Gavaghan,3 Michele Foster1
1The Hopkins Centre: Research for Rehabilitation and Resilience, Griffith University, Brisbane, Queensland, Australia; 2Central Queensland Hospital and Health Service, Rockhampton, Queensland, Australia; 3Allied Health Professions’ Office of Queensland, Clinical Excellence Queensland, Brisbane, Queensland, Australia
Correspondence: Jessica J Bowley, The Hopkins Centre, Griffith University, 170 Kessels Road, Brisbane, Queensland, Australia, Tel +61 3735 8136, Email [email protected]
Introduction: The challenges associated with equitable healthcare access are often more pronounced for individuals living in rural and remote locations, compared to those in metropolitan locations. This study examined the health care transitions of rural- and remote-living patients with on-going sub-acute needs, following acute hospital discharge. This was done with the aim of exploring these patients’ experiences of client-centeredness and continuity of care, and identifying common challenges faced by rural and remote sub-acute patients accessing and transitioning to and through sub-acute care in a non-metropolitan context.
Materials and Methods: Semi-structured interviews were conducted with 37 sub-acute patients. A qualitative descriptive approach was used to analyze the interview data and explore key emergent themes in relation to client-centeredness, continuity of care, and sub-acute transition challenges.
Results: Interview participants’ average length of stay in sub-acute care was 31.6 days (range = 8– 86 days), with most transitioning from larger regional and metropolitan hospitals to on-going rural or remote sub-acute care (n = 19; 53%). Client-centeredness was primarily characterized by the quality of interpersonal experiences with staff, patient and familial involvement in care planning, and the degree to which patients felt their wishes were respected and advocated for. Continuity of care was characterized by access to and participation in rehabilitation services, and access to family and social supports. Challenges associated with sub-acute transitions were explored.
Discussion: The findings suggest important implications for health care providers, including the need to implement earlier and more frequent opportunities for patient involvement throughout the sub-acute journey. The results offer a unique perspective on the way that continuity of care is experienced and conceptualized by rural and remote patients, suggesting a revision of what is required to achieve equitable care continuity for rural and remote residents receiving care far from home.
Conclusion: It is pertinent for health care providers to consider the unique complexities associated with accessing on-going health care as a rural or remote Australian resident, and to develop mechanisms that support equitable access and continuity and facilitate continuity of care closer to home.
Keywords: care transitions, equitable access, health care access, non-metropolitan, patient discharge, rehabilitation
Introduction
Sub-acute care is an important transition of care for many people following an acute injury or illness, and the need for effective and reliable transition protocols – both into, out of, and through sub-acute care – is a critical component of effective and equitable healthcare provision.1,2 Sub-acute care has been shown to support greater functional outcomes for patients through access to rehabilitation services, regular follow-ups and support networking, multi-disciplinary engagement, and individualized care planning, beyond the point of acute hospital discharge.2 Despite these benefits, there are persistent challenges associated with enabling effective sub-acute transitions which, in the context of rural and remote health care, are often characterised by geographical isolation, proximity constraints, and poorer access to specialized care close to home. Sub-acute transition challenges are further precipitated and perpetuated by system constraints,3 inconsistent accessibility and availability of services,1,4 insufficient patient and familial involvement,3 and breakdowns in continuity of care, communication transference, and patient information sharing.3,5
The challenges associated with equitable healthcare access are often considered to be more pronounced for individuals living in rural locations.6–8 Previous studies have acknowledged inequities in the number of available services9–11 as well as the number of primary health and specialized physicians available in metropolitan compared to rural areas.9,12,13 As well, the provision of rehabilitation services – both in an inpatient and an outpatient capacity – is often more limited in rural areas, with considerably greater variability in the number, type, and availability of nursing and other allied health services, which often perpetuates the need for non-metropolitan residents to travel further from home to receive necessary care.11,13,14 Inequities in service access and provision are even further exacerbated for those living in remote communities.15
The Transition to Sub-Acute (T2SA)16 initiative was developed with the aim of delivering client-centered and seamless care for patients residing outside of metropolitan areas, receiving sub-acute and rehabilitation care in regional centers. The primary aim of this initiative, led by allied health professionals, is to facilitate the equitable and accessible provision of sub-acute services and expedite care closer to home. In the initial phase, a qualitative evaluation of the implementation and impact of the T2SA project was undertaken, focusing on the perspectives of allied health practitioners and managers, and other stakeholders, across Central Queensland Hospital and Health Service (HHS), Central West HHS, Townsville HHS, and North-West HHS.16 These findings highlighted multiple professional, procedural, organisational, and patient-related benefits associated with the T2SA initiative, as well as several structural, governance, and professional culture barriers, and the need for on-going procedural and practical supports to sustain its continuation. In the second phase, a second evaluation was undertaken, this time exploring patients’ sub-acute transition journeys following acute hospitalization, through semi-structured interviews with a sample of patients with on-going sub-acute care requirements.
In the current study, we present the findings of this second phase, reporting on the transition experiences of patients involved in the T2SA project across HHS locations in Central and North-West Queensland, Australia. The main objective of this qualitative descriptive study was to describe rural- and remote-based patients’ experiences of client-centeredness and continuity of care, and the common challenges faced, when accessing sub-acute health care, particularly in the context of transitioning to care closer to home.
Materials and Methods
Study Design
This study utilized a qualitative design, conducted in accordance with the consolidated criteria for reporting qualitative studies.17 The results were derived from a descriptive thematic analysis18 of 37 semi-structured interviews carried out with sub-acute patients and, in some cases, their family caregiver. Demographic information was informed by a review of patients’ hospital medical charts, collected at the time of the interview. Interviews were conducted between June 2019 and December 2020. The study was performed in accordance with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Ethics and governance approvals were attained from relevant committees to conduct the evaluation (Metro South Human Research Ethics Committee, HREC/2018/QMS/48160).
For the purposes of the analysis, client centeredness is defined as the provision of individualized care that is respectful of, and responsive to, the preferences, needs and values of patients and their decisions.19,20 Continuity of care is defined in line with Freeman’s21 definition of experienced continuity, where continuity of care is the experience of a coordinated and smooth progression of care, from the patient’s perspective, that encompasses patient satisfaction in relation to both the interpersonal aspects of their care as well as their health care coordination.
Recruitment and Sample
Participants were a convenience sample recruited from hospital and rehabilitation facilities across four Central and North-West Queensland HHS locations. Clinicians identified prospective participants, who they then approached with information about the study. If patients indicated an interest in participating in the study, the research team was notified, and a representative was sent to explain the research and consent process. Both verbal and written consent were obtained from all participants and/or a family member advocating on their behalf prior to the interview process, which included consent for the publication of their anonymized data and responses. From the point that the research team became involved, no participant drop-outs (ie withdrawals from the study) were acknowledged.
Chart audit data was collected from the time of hospitalization. Information collected included patients’ age, impairment type, acute length of stay (LOS), sub-acute in-patient LOS (including LOS at each location of care for patients who transitioned through multiple in-patient care settings), and transition destination/s. For patients who transitioned from hospital to other in-patient sub-acute and/or rehabilitation care facilities, chart audit data was recorded at each subsequent transition following the initial hospital discharge.
Interview Procedure
Interviews were conducted by the second author (KF), and one other senior project officer. Both interviewers were senior clinicians with relevant tertiary qualifications (ie Bachelor of Physiotherapy) and several years’ experience conducting interviews in a health care setting. Interviewers were not previously involved in any aspect of the participating patients’ care and were only known to participants within the context of the research. No relationships were established prior to conducting the interviews. Both interviewers contributed to the development of the interview questions and prompts, and to the interview approach, and these were piloted prior to commencing data collection.
Patients were interviewed in sub-acute inpatient settings at each HHS location, either during or after the receipt of sub-acute care services. Patients participated in a single semi-structured interview where they were asked a series of open-ended questions about various aspects of their sub-acute care and transition experiences (see Table 1 for interview guide). In some instances, a family member was present at the interview and contributed responses either in conjunction with or on behalf of the patient being interviewed. Responses were documented on a structured template during the interview process by the interviewer, which included recording key phrases and segments of direct responses to questions.
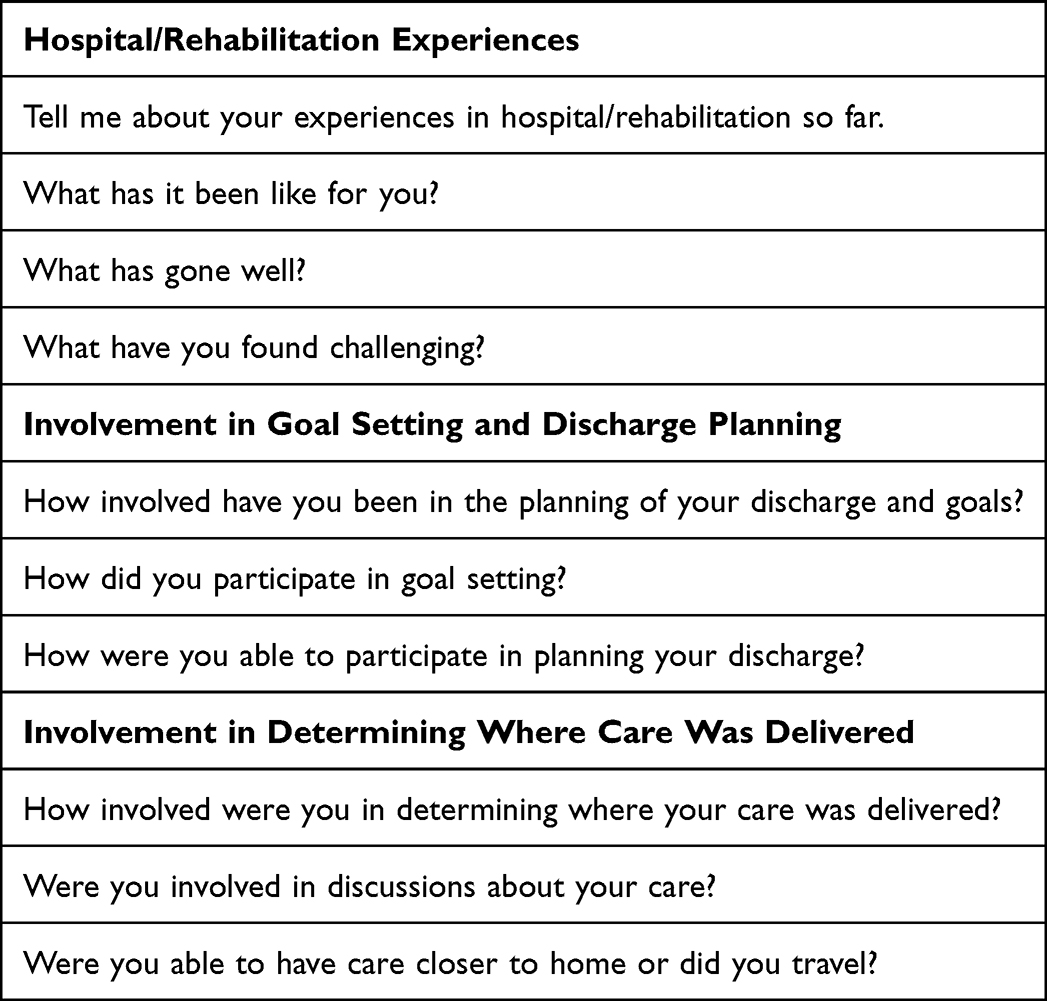 |
Table 1 Interview Guide |
The average interview duration was 30–40 minutes. Due to the pragmatic nature of the interview process, audio and visual recordings were not obtained. At the conclusion of each interview, interviewers reviewed their interview notes with participants’ (and/or their participating family member) to ensure an accurate reflection of interview content and confirm the validity and credibility of the collected data. Data saturation was achieved in some health facilities more than others, and interview data collected across different facilities were subsequently compiled into a larger dataset to achieve adequate saturation. Due to emergent participation and location constraints, member checking was not possible following analysis of the full data set.
Data Analysis
Data was analyzed using a qualitative descriptive approach, and a thematic summary of the main patient experiences was derived from the data. A descriptive approach allows the subjective and individual experiences of patients within the sub-acute environment to be captured, and provides a rich description of these findings, whilst accommodating the sampling and methodological limitations involved with collecting data via health care professionals operating on the ground.18 This approach was deemed appropriate given the primary aim of the study in describing the individual experiences of sub-acute patients.
Using a deductive approach, all phases and segments were initially organised by one researcher into the main areas of interest. Two researchers then independently read each category of data looking to identify and summaries the main sub-plots and indicate exemplar extracts. The researchers then met to discuss and agree the final construction of three descriptive themes: (1) client centeredness; (2) continuity of care and (3) sub-acute transition challenges. Demographic data collected from patients’ medical charts was used to provide a descriptive context of patients’ average length of stay, transition outcomes, and impairment types.
Results
Thirty-seven participants were included in the final sample. Demographic data collected from patients’ hospital charts were only obtainable for 36 participants. Sample characteristics are detailed in Table 2. Patients’ average length of stay in sub-acute care was 31.6 days (range = 8–86 days). Multiple trauma, stroke, orthopedic, and neurological patients had the longest sub-acute lengths of stay on average. Reconditioning (ie rehabilitation to improve physical capacity following significant medical illness or surgery) and fractured neck of femur (NOF) patients had considerably shorter lengths of stay on average, and amputation patients had the shortest average length of stay. The average length of stay for sub-acute patients who discharged directly home from a regional facility was considerably shorter compared to patients who transitioned to on-going rural care. Despite this, transitioning to on-going rural care was the most common transition type (n = 19; 53%), followed by direct discharge from a regional site (n = 17; 47%), indicating a shift towards more sub-acute patients accessing care closer to home.
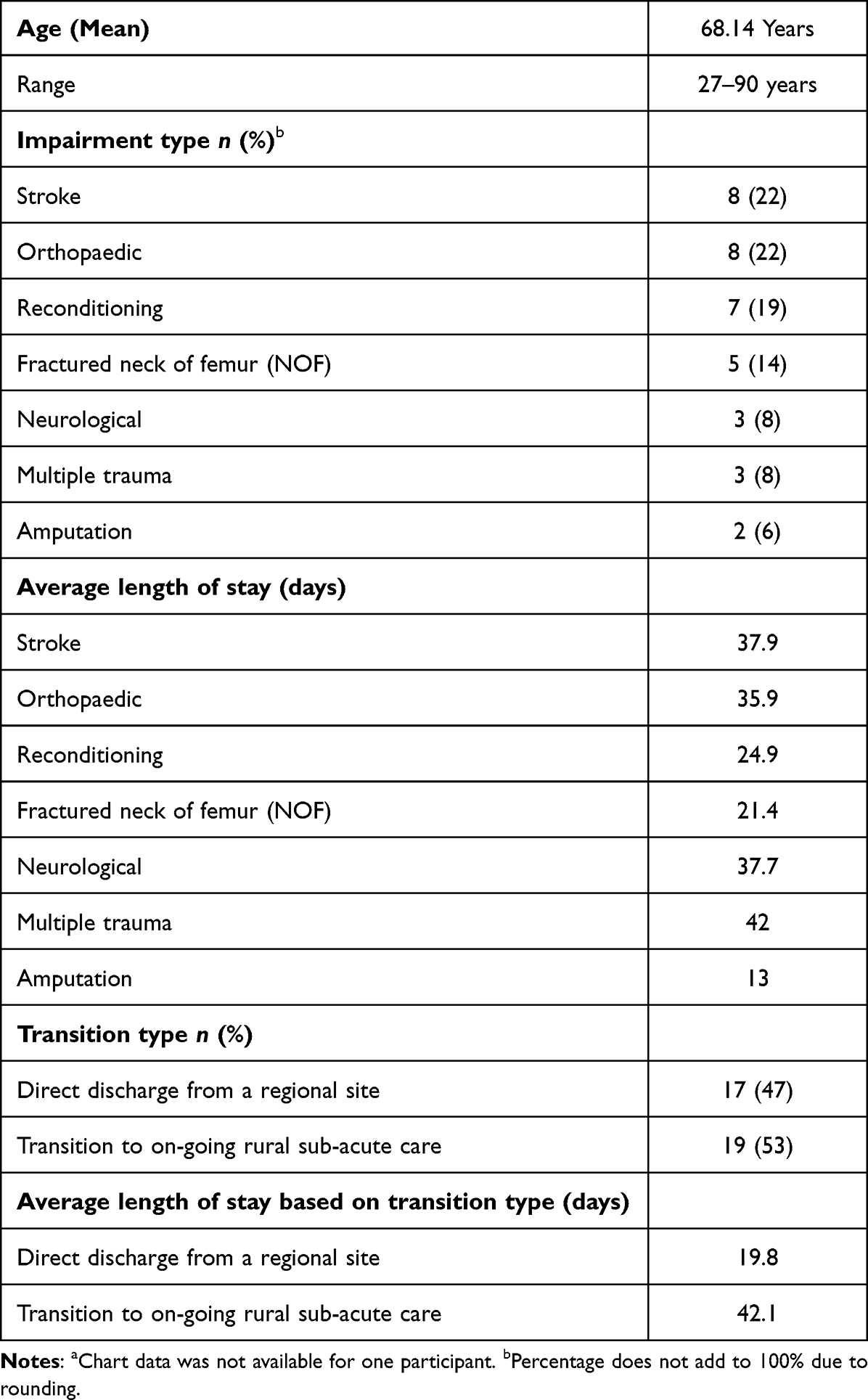 |
Table 2 Patient Characteristics (N = 36)a |
Client Centeredness
Indicators of client-centered care expressed by participants during their interviews related to the interpersonal qualities and adaptability of staff, experiences of being involved and informed in goal setting and decision-making, a sense of being listened to and having wishes heard, and the extent to which transition preferences were respected and advocated for. In every case, positive experiences, and active involvement in each of these areas was generally associated with better transition experiences overall.
The interpersonal qualities and adaptability of staff were key factors influencing overall sub-acute experience. Most patients reported positive experiences with sub-acute staff and enjoyed interacting with staff. Overall, patients reported that staff were attentive, and valued the ability of staff members to adapt care based on their individual needs.
76-year-old patient admitted for reconditioning: They are impeccable down there; the girls are 100%. more people around brightens my day
41-year-old patient with multiple trauma: I’ve been blown away by staff and the level of care… Within the first week, I have the social worker support, psychologist, dietitians, all the services I needed were available and working for you. I didn’t have to ask for help
Two opposing experiences were evident in relation to patients’ experiences of being involved and informed in goal setting and decision-making. Many patients highlighted the value of being well informed about their care and appreciated being asked questions that allowed them to have input into their care planning.
63-year-old patient with fractured NOF: Everyone treated me like an individual and listened to me… Doctors talked to me a few times about discharge to make sure things are in place and keep me up to date. I’ve definitely felt involved and had a say…
In contrast to the many patients and families who reported positive experiences of being heard and involved in the planning process, others reported limited involvement and inconsistent information from care teams. In these cases, patients reported a desire to be more involved in planning and decision-making highlighting the importance of patient involvement in achieving client-centered care.
27-year-old patient with multiple trauma: Never really said when I was going… I would set myself goals like the stairs and showed them I could do it so they could let me go
58-year-old patient with fractured NOF: Wife spoke to the team to help push getting home ASAP [as soon as possible] … had to give them a shove to get home sooner
More patients felt involved in goal setting than they did in discharge planning, and many expressed a desire to be more actively involved in their discharge planning.
Husband speaking on behalf of 74-year-old patient with orthopedic injury: Weren’t really involved in the discharge planning discussions… it was 50/50
68-year-old patient with neurological impairment: I would have wanted to be more involved with my discharge planning… it would have been better to have one more step
Wife speaking on behalf of 80-year-old patient admitted following stroke: There has not been much talk about his discharge yet… they’ve been focusing on the ‘now’… would like to discuss it further
A contrast was also evident in relation to experiences of respect and advocacy for patients’ wishes. In many cases, patients were appreciative of efforts made by staff to advocate for their transition preferences and reported positive experiences with staff who worked hard to respect and adapt transition plans to accommodate their patients’ individual needs and wishes.
76-year-old patient admitted for reconditioning: Yesterday [the doctor] asked, ‘Do you think it is better to be here or [closer to home]?’… I feel better now that I’ve said my mind, I want to go back…
50-year-old patient with orthopedic injury: They tried to tell me what was going on… Can’t get there [home] quick enough!
In contrast, a small number of patients reported negative experiences, primarily characterized by feelings that patients were not consulted about changes and subsequent transitions were not aligned with patient needs. As well, some patients reported that they needed to advocate for themselves to achieve desired transition outcomes.
Daughter speaking on behalf of 76-year-old patient admitted for reconditioning: If I don’t ring and ask, they don’t tell me anything
53-year-old patient admitted following an amputation: I’ve been quite vocal… I told them upstairs to get me into rehab [rehabilitation] or I’m going home!
Continuity of Care
Access to and involvement in rehabilitation services, continuity of staff and the communication of patient information, and a desire to be closer to family and support systems were the most common factors influencing continuity of care.
Patients valued having access to rehabilitation services, and generally reported a strong desire to be actively involved in rehabilitation programs. Several patients expressed a desire to be more heavily involved in rehabilitation programs, and generally did not want this aspect of their care to be neglected. While several patients reported rehabilitation to be a challenging aspect of their hospital experience, most patients still viewed rehabilitation as valuable and enjoyed the benefits gained by participating in rehabilitation programs.
63-year-old patient with fractured NOF: I have no complaints about rehab – it has been marvelous… They got me up walking and doing things I never thought I could do
75-year-old patient with multiple trauma: Good how they get you going
Some patients also highlighted a preference for continuity of staff, and several acknowledged the importance of maintaining continuity in relation to the communication and transference of patient information. Given the positive interpersonal relationships many patients developed with sub-acute staff, separation from these relationships when transitioned to new care environments was often viewed as a challenge. In some cases, staffing changes also led to breakdowns in the transfer or communication of patient information, either between different members of staff, or between different care facilities, which was a source of frustration for patients and the family members advocating on their behalf.
77-year-old patient with orthopedic injury: You have to build a relationship with staff and then as soon as you do, you move again which is challenging…
76-year-old patient admitting for reconditioning: The doctors haven’t been talking to each other. I have three different doctors and none of them know what the other is doing… frustrating
56-year-old patient admitted for reconditioning: Although the physios [physiotherapists] were good in rehab, they did change a few times… Got tired of telling the same story
A desire to be closer to home, and to family, friends, and support systems, was a very common theme amongst patients. Most patients acknowledged the importance of having access to family and friends, and a preference to receive care closer to home, and many reported the difficulties associated with being away from loved ones.
63-year-old patient with fractured NOF: Do not get to see family and friends much, they are far, far away
27-year-old patient with multiple trauma: I fought to get back here… I wanted to be closer to my family and didn’t want to be alone… I’m excited about getting home
84-year-old patient with fractured NOF: Family equals half your health
Sub-Acute Transition Challenges
Patients identified several challenges associated with their sub-acute transition experiences, including the financial and psychological impacts of receiving care far from home, the impacts for families, and patients’ perceptions about quality of care in rural versus regional facilities.
Many patients acknowledged the financial and psychological impacts of being separated from their families and communities, and the burdens placed on families while receiving care far from home.
Daughter speaking on behalf of 83-year-old patient admitted for reconditioning: [Dad] just wants to go home… Dad is like a fish out of water, he’s seeing a white wall and he’ll never get out of here
Husband speaking on behalf of 56-year-old patient admitted for reconditioning: She wanted to go home… she was sad and wanted to go home so she could be comfortable
27-year-old patient with multiple trauma: It has cost a lot of money for them. I reckon [AUD]$4000 just in Brisbane
Overwhelmingly, the greatest barrier to patients accessing care closer to home was patients’ perceptions about the quality of care available in rural and remote locations. Patients often reported feeling that services in rural facilities were sub-optimal, especially in comparison to regional facilities. Many expressed some hesitancy about transitioning to care in rural sites, and generally perceived regional facilities to provide higher quality care and services.
50-year-old patient with orthopedic injury: Closer to home is good, but there are not as many facilities rurally
82-year-old patient with orthopedic injury: It’s a better place for you [at the regional hospital], because of more specialists… they tell me that physio is not as good there
55-year-old patient admitted following stroke: Not up to standard. Not knocking [the rural therapist], but not like the ones here… There’s no reason for me to go there before going home
69-year-old-patient admitted for reconditioning: Would love to [receive care closer to home] but not possible, no systems and facilities… they need to do something about that
Interestingly, despite the hesitation commonly associated with transitioning to rural sites, patients who did transition to on-going rural care generally reported that the care they received was the same and that they were satisfied with the care offered in rural facilities.
84-year-old patient with fractured NOF: All been good… No difference in therapies
63-year-old patient with fractured NOF: [when asked about transitioning to care closer to home] There is some anxiety, anxiety about the care, but I didn’t know what to expect but was fine once I got here
Discussion
This evaluation identified several factors influencing the sub-acute transition experiences of people living in remote and rural areas accessing sub-acute care services in Queensland. Several important themes are identified in relation to how these patients characterize client-centeredness and continuity of care, as well as some of the common challenges faced by rural patients accessing sub-acute services. Overall, patients reported differing levels of satisfaction, which were heavily influenced by the nature of patients’ interpersonal experiences with allied health staff, the degree to which they had access to family and social supports, and their level of involvement in transition and discharge planning.
The nature and quality of interpersonal experiences with allied health and nursing staff heavily influenced how patients perceived their overall hospital and sub-acute/rehabilitation experience, highlighting the importance of maintaining quality staffing in sub-acute care environments. Previous studies have also emphasized the extent to which positive interpersonal experiences with health care staff influence health care satisfaction.22–24 Positive experiences with staff not only foster a greater sense of respect and involvement but are often also an important source of emotional support for patients and families across the care continuum.24,25 Based on the findings of this study, the provision of these supports appears to be especially important for rural patients receiving care away from home, particularly when access to usual family and social supports is limited by geographical or financial constraints.
Patient involvement in goal setting and discharge planning varied, which impacted on patients’ perceptions of client centeredness and quality of care. A key finding was that patients felt more involved in goal setting than they did in discharge planning, and many expressed a desire to be consulted earlier, particularly about their discharge plans. This may indicate that planning in relation to goals identified in an in-patient capacity is currently felt to be more accessible to patients, whereas care planning beyond patients’ hospital admission is felt to be less clearly developed or discussed. Inconsistencies, particularly in relation to discharge planning, is already known to be a factor contributing to poorer health care and transition experiences.26–29 To address these inconsistencies, practitioners may need to consider how to better identify opportunities for planning and enacting transition discussions earlier in the sub-acute process. A critical component of this is improving the quality and frequency of patient consultations, which may need to be addressed at the treating clinician level – that is, with allied health professionals engaging with sub-acute patients.
Crucially, most patients who wished to receive care closer to home were ultimately able to do so, indicating a successful shift towards more equitable care in rural and remote areas, which was valued highly by patients. Despite this, hesitancy about receiving care in rural locations was common. The perception that rehabilitation services are poorer in rural and remote areas is an enduring barrier to equitable access. Both in the current findings and the existing literature, there remains a significant degree of hesitancy associated with receiving care outside of metropolitan locations,30 often founded on the notion that services offered in rural sites will “fall short” compared to services offered in metropolitan facilities.31 Despite this, most patients were ultimately satisfied with their care and transition outcomes after transitioning rural. This suggests that a vital part of improving equitable access to health care in non-metropolitan regions may start with taking steps to offset patient apprehension and hesitancy about transitioning rural. To be successful in transitioning more patients to care closer to home, better education and endorsement of the quality of care available in rural and remote locations is still needed.
A key contribution of the findings is the way in which continuity of care is uniquely conceptualized by patients in the context of rural health care. For rural and remote Australians in this study, effective continuity of care was not only viewed as the continuity of physical care, but also continuity of access to family and community supports across the care continuum. Many participants expressed a desire to receive care closer to home, which was often in response to a desire to be closer to families, friends, and community. In conjunction with this, the hardships associated with separation from family and community connections were a common challenge identified by patients, particularly those receiving care away from home for extended periods. This suggests that continuity of care is characterized by patients as being more than just access to health services; continuity of access to family and social supports was decidedly as important, if not more important, to sub-acute patients in relation to effective and satisfactory continuity of care.
This dual conceptualization of continuity of care has both practical and policy implications, many of which are unique to the provision of sub-acute services for rural and remote living patients. The likelihood of being significantly displaced from home and community following an acute episode is far greater for rural and remote Australians, particularly those requiring specialized supports and treatment.32–36 Therefore, isolation from family and friends, and separation from community, is often more pronounced.35,37,38 To improve quality of care for these individuals, it is important for health providers to consider ways to better improve continuity of access to social supports, particularly among rural patients forced to relocate for care. Telehealth services have been shown to be an effective mechanism for improving access, communication, and engagement with health services,26 particularly amongst patients living in rural communities.10 In cases where direct access to family and social supports is not possible, it may be possible for sub-acute services to consider how telehealth and digital services may also be utilized to improve continuity of access to social supports for patients requiring extended stays in sub-acute facilities far from home. This may in turn alleviate some of the challenges currently impacting patient experiences in relation to home and community separation during sub-acute engagement.
From a policy perspective, policy makers may consider revising the way that continuity of care is currently characterized. The experience of continuity of care may be uniquely different for Australians living in rural and remote communities compared to those receiving sub-acute care services in metropolitan regions. For rural patients, continuity of care appears to involve continuity in the context of access to family and community, as well as continuity of health care. The introduction of new protocols to enable continuity of care in the context of both service continuity and social continuity may be the necessary next step towards optimizing equitable health service engagement for rural and remote sub-acute patients. At the very least, it seems imperative that policy makers begin reflecting on the importance of maintaining social continuity during sub-acute transitions, and what implications this may have for improving the provision of sub-acute services, and for the equitable provision of health care services more broadly.
Limitations
The T2SA initiative was developed and is led by health care professionals, and data, such as that reported in the current study, often requires collection “on the ground”, in the context of everyday health service operations. Thus, an inherent limitation of this pragmatic approach is that data was collected and recorded by health care professionals (albeit, only those unaffiliated with participants’ care), rather than dedicated researchers introduced into the health care system for the purposes of conducting the research. As such, in this study, interviews were not audio-taped, and verbatim transcripts of patient and family responses were not obtained. In turn, the resulting dataset was only analyzed at a basic descriptive level, appropriate to the quality of the available data. In the context of this study, we acknowledge the necessity of this compromise to allow for the collection of authentic patient data in coordination with the daily running of the health systems involved. However, additional qualitative analyses are required to further validate the present findings, incorporating additional measures necessary to increase reliability and validity of the data such as training for health care professionals as data collectors and interview recording and transcription protocols.
Conclusion
By describing rural- and remote-living patients’ experiences of sub-acute and rehabilitation care, and system transitions, the objective of this T2SA initiative was to better inform the provision of these services for a vulnerable sub-acute population. This evaluation highlights several factors which may be important to improving rural- and remote-living patients’ sub-acute transition experiences. In terms of care received in in-patient facilities, the quality and personability of staff appears to have a critical influence over positive patient experiences, as well as adequate and timely access to rehabilitation and care, and client-centered involvement at each stage of the transition, goal setting, and discharge planning. Structure and transparency around discharge planning appears particularly important to sub-acute patients, many with the motivation of receiving care closer to home in a shorter time frame, or at least being aware of a timeframe for discharge, earlier in the sub-acute process. Finally, factors for optimizing continuity of care are decidedly two-fold. While access to adequate and equitable care was the first major consideration, this evaluation also highlighted the importance of maintaining continuity of access to family and social support systems throughout the sub-acute journey. Thus, sub-acute care providers may also consider revising and re-defining how continuity of care is currently characterized in the sub-acute space, to better acknowledge and accommodate the unique care requirements of rural and remote living patients.
Data Sharing Statement
The data are not available due to privacy and ethical restrictions.
Acknowledgments
The authors acknowledge the contribution of the following allied health professionals, who were involved in this research project – Ilsa Nielsen, Sandra Phillips, Leigh Burton, Ella Dunsford, Struan Ferguson, Sarah Bohan and Liza-Jane McBride. The authors also wish to thank the participants for this project, particularly the consumers who accessed the Queensland Health sub-acute services.
Funding
This project was funded by the Allied Health Professions’ Office of Queensland, Clinical Excellence Queensland. Representatives from the Allied Health Professions’ Office of Queensland were also subsequently involved in the design of the study, data collection, analysis, and interpretation, and writing of this article for submission.
Disclosure
Ms Jessica J Bowley reports grants from the Allied Health Professions’ Office of Queensland, outside the submitted work. The authors report no conflicts of interest in this work.
References
1. Allen J, Hutchinson A, Brown R, Livingston P. Communication and coordination processes supporting integrated transitional care: Australian healthcare practitioners’ perspectives. Int J Integr Care. 2020;20(2):1. doi:10.5334/ijic.4685
2. Dawda P, Russell L. Sub-acute care: an international literature review. Canberra: Australian Primary Health Care Research Institute; 2014. Available from: https://nceph.anu.edu.au/files/Sub_acute_care_intl_lit_review.pdf.
3. Stolee P, Elliott J, Byrne K, et al. A framework for supporting post-acute care transitions of older patients with Hip fracture. J Am Med Dir Assoc. 2019;20(4):414–419. doi:10.1016/j.jamda.2019.01.147
4. Strivens E, Harvey D, Foster M, Quigley R, Wilson M. Analysing sub-acute and primary health care interfaces – research in the elderly [ASPIRE study]. Canberra: Australian Primary Health Care Research Institute; 2015. Available from: https://nceph.anu.edu.au/research/centres-departments/australian-primary-health-care-research-institute.
5. Harvey D, Foster M, Quigley R, Strivens E. Care transition types across acute, sub-acute and primary care. J Integr Care. 2018;26(3):189–198. doi:10.1108/JICA-12-2017-0047
6. Jellema S, van Hees S, Zajec J, van der Sande R, Nijhuis- van der Sanden M, Steultjens E. What environmental factors influence resumption of valued activities post stroke: a systematic review of qualitative and quantitative findings. Clin Rehabil. 2016;31(7):936–947. doi:10.1177/0269215516671013
7. Jia H, Cowper D, Tang Y, Litt E, Wilson L. Postacute stroke rehabilitation utilization: are there differences between rural-urban patients and taxonomies? J Rural Health. 2011;28(3):242–247. doi:10.1111/j.1748-0361.2011.00397.x
8. Wakerman J, Humphreys J. Sustainable workforce and sustainable health systems for rural and remote Australia. Med J Aust. 2013;199(5):14–17. doi:10.5694/mja11.11639
9. Graham SK, Cameron ID. A survey of rehabilitation services in Australia. Aust Health Rev. 2008;32(3):392–399. doi:10.1071/AH080392
10. Vratsistas‐Curto A, Shiner CT, Klein L, Faux SG. Cross‐sectional survey of rehabilitation service availability for stroke and Hip fracture in Australian public hospitals. Aust J Rural Health. 2021;29(6):958–971. doi:10.1111/ajr.12803
11. Robards F, Kang M, Steinbeck K, et al. Health care equity and access for marginalised young people: a longitudinal qualitative study exploring health system navigation in Australia. Int J Equity Health. 2019;18(1):1–14. doi:10.1186/s12939-019-0941-2
12. Verdon S, Wilson L, Smith-Tamaray M, McAllister L. An investigation of equity of rural speech-language pathology services for children: a geographic perspective. Int J Speech Lang Pathol. 2011;13(3):239–250. doi:10.3109/17549507.2011.573865
13. Leveratt M. Rural and remote Australia-equity of access to health care services. Aust Health Consumer. 2006;2(2006–2007):16–17.
14. Van Spijker BA, Salinas-Perez JA, Mendoza J, et al. Service availability and capacity in rural mental health in Australia: analysing gaps using an Integrated Mental Health Atlas. Aust N Z J Psychiatry. 2019;53(10):1000–1012. doi:10.1177/0004867419857809
15. Thomas SL, Wakerman J, Humphreys JS. Ensuring equity of access to primary health care in rural and remote Australia-what core services should be locally available? Int J Equity Health. 2015;14(1):1–8. doi:10.1186/s12939-015-0228-1
16. Finch J. Facilitating sub-acute care ‘closer to home’ for rural and remote patients.
17. Colorafi K, Evans B. Qualitative descriptive methods in health science research. HERD. 2016;9(4):16–25. doi:10.1177/1937586715614171
18. Australia Commission on Safety and Quality in Health Care (ACSQHC). Person-centred care. Sydney: ACSQHC; 2019. Available from: https://www.safetyandquality.gov.au/our-work/partnering-consumers/person-centred-care.
19. World Health Organization. People at the centre of care. Geneva: World Health Organization; 2014. Available from http://www.wpro.who.int/health_services/people_at_the_centre_of_care/definition/en/.
20. Freeman GK, Olesen F, Hjortdahl P. Continuity of care: an essential element of modern general practice? Fam Pract. 2003;20(6):623–627. doi:10.1093/fampra/cmg601
21. Booth A, Hannes K, Harden A, Noyes J, Harris J, Tong A. COREQ (consolidated criteria for reporting qualitative studies). In: Moher D, Altman DG, Schulz KF, Simera I, Wager E editors. Guidelines for Reporting Health Research: A User’s Manual. West Sussex: John Wiley & Sons; 2014:214–226.
22. Wladkowski SP, Kusmaul N, Latimer A. Grief and loss during care transitions: experiences of direct care workers. Omega. 2021;2021:1–15.
23. Mitchell SE, Laurens V, Weigel GM, et al. Care transitions from patient and caregiver perspectives. Ann Fam Med. 2018;16(3):225–231. doi:10.1370/afm.2222
24. Elliott J, Forbes D, Chesworth BM, Ceci C, Stolee P. Information sharing with rural family caregivers during care transitions of Hip fracture patients. Int J Integr Care. 2014;14:e018.
25. Cott C. Client-centred rehabilitation: client perspectives. Disabil Rehabil. 2004;26(24):1411–1422. doi:10.1080/09638280400000237
26. Asif M, Cadel L, Kuluski K, Everall AC, Guilcher SJ. Patient and caregiver experiences on care transitions for adults with a Hip fracture: a scoping review. Disabil Rehabil. 2020;42(24):3549–3558. doi:10.1080/09638288.2019.1595181
27. Dossa A, Bokhour B, Hoenig H. Care transitions from the hospital to home for patients with mobility impairments: patient and family caregiver experiences. Rehabil Nurs. 2012;37(6):277–285. doi:10.1002/rnj.047
28. Jensen CM, Smith AC, Overgaard S, Wiil UK, Clemensen J. “If only had I known”: a qualitative study investigating a treatment of patients with a Hip fracture with short time stay in hospital. Int J Qual Stud Health Well-Being. 2017;12(1):1307061. doi:10.1080/17482631.2017.1307061
29. Storm M, Siemsen IM, Laugaland K, Dyrstad DN, Aase K. Quality in transitional care of the elderly: key challenges and relevant improvement measures. Int J Integr Care. 2014;14(2):e013. doi:10.5334/ijic.1194
30. Harrison AL, Hunter EG, Thomas H, Bordy P, Stokes E, Kitzman P. Living with traumatic brain injury in a rural setting supports and barriers across the continuum of care. Disabil Rehabil. 2017;39(20):2071–2080. doi:10.1080/09638288.2016.1217081
31. Jackson SM, Neibling BA, Barker RN. Stroke survivors’ perspectives on recovering in rural and remote Australia: a systematic mixed studies review. Aust Occup Ther J. 2021;68:1–17. doi:10.1111/1440-1630.12719
32. Mbuzi V, Fulbrook P, Jessup M. Indigenous peoples’ experiences and perceptions of hospitalisation for acute care: a metasynthesis of qualitative studies. Int J Nurs Stud. 2017;71:39–49. doi:10.1016/j.ijnurstu.2017.03.003
33. Neville S, Napier S, Adams J, Shannon K. Accessing rural health services: results from a qualitative narrative gerontological study. Australas J Ageing. 2020;39(1):e55–61. doi:10.1111/ajag.12694
34. Wong S, Regan S. Patient perspectives on primary health care in rural communities: effects of geography on access, continuity and efficiency. Rural Remote Health. 2009;9(1):1–2.
35. Clark RA, Coffee N, Turner D, et al. Application of geographic modeling techniques to quantify spatial access to health services before and after an acute cardiac event: the Cardiac Accessibility and Remoteness Index for Australia (ARIA) project. Circulation. 2012;125(16):2006–2014. doi:10.1161/CIRCULATIONAHA.111.083394
36. Dew A, Bulkeley K, Veitch C, et al. Addressing the barriers to accessing therapy services in rural and remote areas. Disabil Rehabil. 2013;35(18):1564–1570. doi:10.3109/09638288.2012.720346
37. McGrath P. Exploring Aboriginal peoples’ experience of relocation for treatment during end-of-life care. International Journal of Palliative Nursing. 2006;12(3):102–108. doi:10.12968/ijpn.2006.12.3.20692
38. Loughery J, Woodgate R. Supportive care needs of rural individuals living with cancer: a literature review. Can Oncol Nurs J. 2015;25(2):157–166. doi:10.5737/23688076252157166
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.