Back to Journals » Infection and Drug Resistance » Volume 16
Understanding Public Knowledge and Behavior Regarding Antibiotic Use in Indonesia
Authors Sinuraya RK ![]() , Wulandari C, Amalia R
, Wulandari C, Amalia R ![]() , Puspitasari IM
, Puspitasari IM ![]()
Received 23 June 2023
Accepted for publication 19 October 2023
Published 26 October 2023 Volume 2023:16 Pages 6833—6842
DOI https://doi.org/10.2147/IDR.S427337
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Rano K Sinuraya,1– 3 Chalisma Wulandari,2 Riezki Amalia,2,3 Irma M Puspitasari2,3
1Unit of Global Health, Department of Health Sciences, University of Groningen, University Medical Center Groningen, Groningen, the Netherlands; 2Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 3Center of Excellence for Pharmaceutical Care Innovation, Universitas Padjadjaran, Sumedang, West Java, Indonesia
Correspondence: Rano K Sinuraya, Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Jalan Ir. Soekarno KM 21, Jatinangor, Sumedang, 45363, West Java, Indonesia, Email [email protected]; [email protected]
Background: Inappropriate use of antibiotics is a prominent factor contributing to the development of antibiotic resistance, which subsequently increases healthcare costs and heightens mortality rates.
Objective: This study sought to evaluate the level of knowledge and behavior pertaining to antibiotic usage within the Indonesian population.
Methods: This observational study was conducted in Indonesia between December 2019 and June 2020 and employed a validated questionnaire to survey 582 respondents. A comparative analysis was performed to investigate the differences in mean scores across various respondent characteristics, specifically related to their knowledge and practice regarding antibiotic usage. Regression analysis was used to identify the factors influencing the adoption of appropriate behavior in antibiotic utilization.
Results: Study participants comprised 68.2% males and 31.8% females. Participants achieved an average score of 4.86 ± 2.40 out of eight points for knowledge and behavior with an average score of 5.29 ± 1.85 out of seven points. Approximately 57.7% and 56.0% of the respondents have knowledge and behavior scores above the average score of the total population, respectively. The findings indicated notable variations in average knowledge scores associated with educational attainment and employment status regarding antibiotic use. Similarly, differences were observed in gender and employment status concerning behavior. Regression analysis highlighted that employment status, trust in physicians, and possessing sound knowledge of antibiotic usage were significant predictors of good behavior in utilizing antibiotics. Some misconceptions were identified, such as using antibiotics to kill viruses and believing antibiotics are effective for any kind of disease.
Conclusion: Less than 60% of the respondents have knowledge and behavior scores above the average score of the total population; however, there are some misconceptions regarding antibiotic utilization. This underscores the importance of implementing targeted strategies, such as health education and public health campaigns, to improve the population’s understanding of the correct antibiotic use.
Keywords: knowledge, attitudes, behavior, antibiotic, antibacterial drug resistance
Introduction
The increasing incidence of antibiotic resistance has emerged as a pressing global health concern.1 Antibiotic resistance is a consequence of bacterial evolution, whereby bacteria develop resistance to antibiotics that are conventionally employed to treat infections.1,2 This phenomenon can result in extended hospitalization periods, elevated healthcare expenditures, and increased mortality ratios.3
Within Indonesia, where the prevalence of infectious diseases is significant,4 the improper use of antibiotics is a prominent factor in the development of antibiotic resistance.4,5 The Indonesian government has undertaken measures to regulate the use of antibiotics by reinforcing its national antibiotic stewardship program and promoting their cautious consumption.6,7 However, despite these efforts, improper antibiotic use remains widespread in Indonesia.6
The insufficient knowledge regarding the appropriate use of antibiotics is commonly recognized as a significant factor that contributes to their misuse and subsequently contributes to the emergence of drug-resistant microorganisms.8 Reports have consistently found that various types of inappropriate antibiotic use exist, including the discontinuation of treatment before the recommended time, failure to follow dosing regimens, using leftover antibiotics from prior treatments, administering antibiotics for viral infections, using antibiotics for self-medication, and procuring antibiotics without a prescription.9
The World Health Organization (WHO) acknowledges the importance of addressing inappropriate antibiotic use and highlights the significance of promoting appropriate use by promoting behavioral change and increasing awareness.5,10 The WHO multifaceted strategy seeks to address antimicrobial resistance by placing significant emphasis on the fundamental roles of proficient communication and education. This approach underscores the crucial significance of public awareness in tackling the overall problem of antibiotic resistance.1,5,10
Limited research has been conducted to investigate the knowledge, attitude, and practice of antibiotic use in Indonesia.11 Our study aims to fill this gap by specifically examining the knowledge and behavior of the Indonesian population regarding antibiotic use, while also considering general information about primary healthcare to provide a comprehensive understanding of the topic. This study can contribute to understanding the underlying factors that lead to the misuse of antibiotics in Indonesia, as well as the development of targeted interventions and educational initiatives aimed at promoting responsible and appropriate antibiotic use.
Methods
A cross-sectional study was conducted on the Indonesian population from December 2019 to June 2020. This study was approved by the Health Research Ethics Committee of Universitas Padjadjaran with registration number 1380/UN.6.KEP/EC/2019. Initially, paper questionnaires were distributed to randomly selected participants in public areas such as drug stores, hospitals, and clinics. However, due to COVID-19 restrictions, the questionnaires were subsequently administered online via email and WhatsApp with approval from the Ethical Committee. Online respondents were recruited through our community engagement efforts. The online questionnaire was created using Google Forms, and the distribution process and data collection were closely monitored and supervised by research assistants. All data were securely stored and could only be accessed by the Principal Investigator. The study included participants aged 18 or older who were not employed in the healthcare sector. To participate in the online survey, individuals needed access to electronic communication devices and the Internet.
The minimum sample size required, calculated based on the formula in Charan et al,12 was 384 people. However, we successfully recruited 582 respondents. The study received ethical clearance from the Health Research Ethics Committee of Universitas Padjadjaran, Indonesia and was conducted in compliance with the principles of the Declaration of Helsinki 1964. Before participating, all participants provided written informed consent for their involvement in the study and the possible publication of research findings.
The questionnaire utilized in this study was adapted from previous research11,13 and underwent professional translation into Bahasa Indonesia. Subsequently, we tailored questions that broadly encompassed knowledge and behavior related to antibiotic use. A questionnaire was then developed, comprising three sections: respondent background information, a knowledge assessment consisting of eight items, and a behavior assessment featuring seven items (Supplementary File). Respondents provided answers to the knowledge and behavior questions using dichotomous options (Agree or Disagree), where a correct response was assigned a score of 1, while an incorrect response received a score of 0. Face validation was conducted by two experts, and a reliability test was conducted using a physical questionnaire administered to 30 respondents. The Cronbach’s alpha scores for knowledge and behavior were 0.76 and 0.74, respectively, indicating acceptable levels of reliability.
Descriptive statistics were used to present the characteristics of the respondents. A t-test was conducted to examine differences in knowledge and behavior based on factors such as age, gender, education attainment, employment status, chronic illness, use of herbal medicine, and general information about healthcare services. A linear multiple regression analysis was performed to identify variables that influenced successful practice. Nominal scales were transformed into dummy variables using binary codes (0 and 1). The Durbin–Watson coefficient of 1.905 indicated no autocorrelation. Multicollinearity was assessed through tolerance levels (0.78–0.99) and variation inflation factor thresholds (1.00–1.28). The regression analysis showed statistical significance (p-value < 0.001). The residual standard deviation mean was 0, and the range was <3, suggesting the absence of outliers. The linear regression model was deemed appropriate based on its adherence to normality, residual analysis, multicollinearity, regression test, and independent error assessment standards. All statistical analyses were conducted using SPSS 27 software (SPSS Inc., Chicago, IL, United States).
Results
Table 1 presents the collected questionnaire data from 582 respondents. Among the respondents, over 60% were aged ≤22 years. Approximately 68.2% of the participants were male, while 31.8% were female. Furthermore, roughly 67% of the respondents had graduated from college or university, with 33% being employed. A small percentage reported having a chronic disease (5.5%), while 4.1% used herbal medicine. The majority of respondents resided near primary healthcare facilities (79.2%), and most of them indicated that they only visited a doctor when they fell ill (90.2%). Notably, approximately 80% of the participants expressed trust in the doctors who examined them.
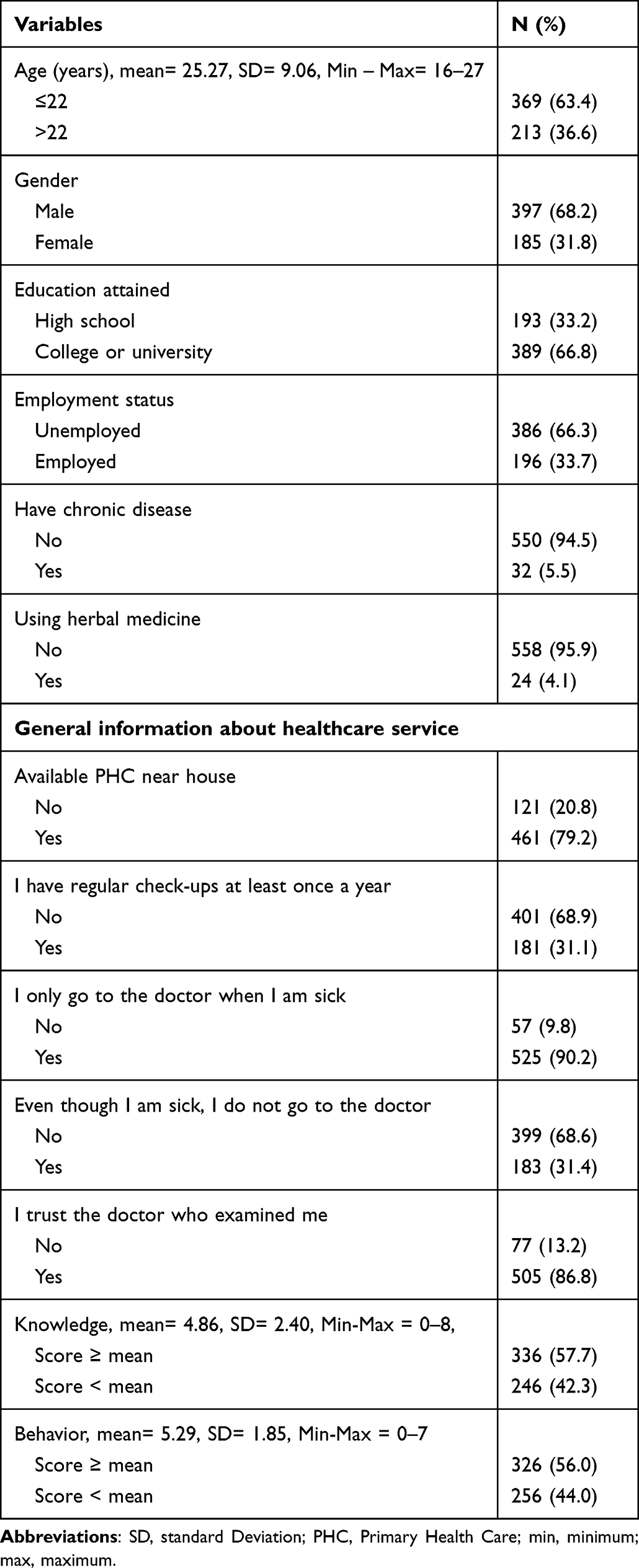 |
Table 1 Characteristics of Respondent (N= 582) |
For knowledge scores, the average score was 4.86 ± 2.40 out of eight points, and the behavior score was 5.29 ± 1.85 out of seven points. This indicates that the respondents possessed sufficient knowledge and exhibited good behavior regarding the use of antibiotics. Nevertheless, only 57.7% and 56.0% of the respondents scored above the average in terms of knowledge and behavior, respectively.
According to Figure 1, 63.5% of the respondents were aware that antibiotics are used for treating bacterial infections. However, nearly 50% of them had incorrect knowledge about using antibiotics for viral infections. Additionally, above 70% of the participants agreed that consuming antibiotics does not affect the effectiveness of vitamins. Furthermore, more than 60% of the respondents correctly understood that antibiotics are not indicated for treating coughs or headaches. However, approximately 45% of the respondents mistakenly believed that antibiotics can be used for various diseases.
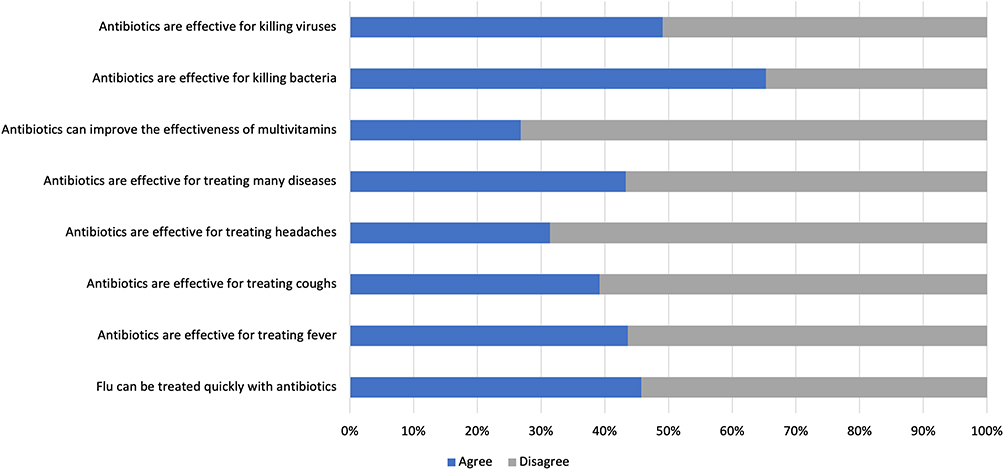 |
Figure 1 Participants’ responses to the questions on the knowledge of antibiotic use. Questions were adapted from these studies. Both are creative commons.11,13 |
Regarding the participants’ behavior, the majority (80.9%) agreed that antibiotic prescriptions should not be saved for later use, and 79% understood that antibiotics should not be shared with others, as shown in Figure 2. Approximately 75% of the participants were committed to completing their prescribed course of antibiotics. However, approximately 29% of the respondents admitted to stopping antibiotic use once they start feeling better, even when doses remained. Furthermore, approximately 26% of the respondents expected to receive antibiotics when visiting a doctor, while 22% felt that antibiotics were necessary whenever they were sick. Additionally, 28% of the respondents believed that they could use the same antibiotic for recurring symptoms without seeking a doctor’s assessment first.
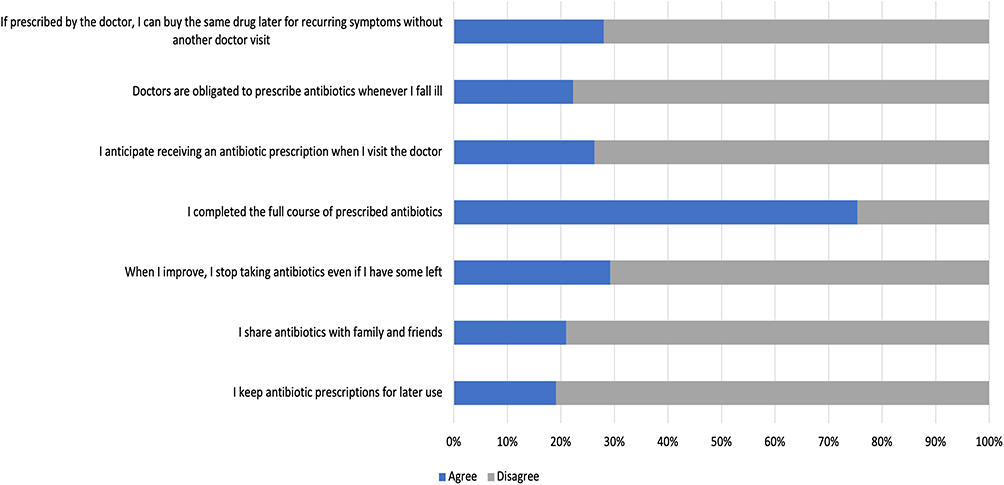 |
Figure 2 Participants’ responses to the questions on behavior regarding antibiotic use. Questions were adapted from these studies. Both are creative commons.11,13 |
Further analysis also revealed a moderate but significant correlation (rho = 0.528) with a p-value < 0.001, indicating that higher knowledge scores are associated with higher behavior scores. This suggests that individuals with better knowledge tend to engage in more appropriate practices when it comes to antibiotic use.
Table 2 presents the comparison of respondents’ characteristics with regards to their knowledge and behavior regarding antibiotics. The findings indicate significant differences (p < 0.05) in knowledge based on education level, employment status, and the habit of regular annual check-ups. As for behavior, significant differences were observed in gender, education level, employment status, regular annual check-ups, only visiting the doctor when sick, and trust in the examining doctor.
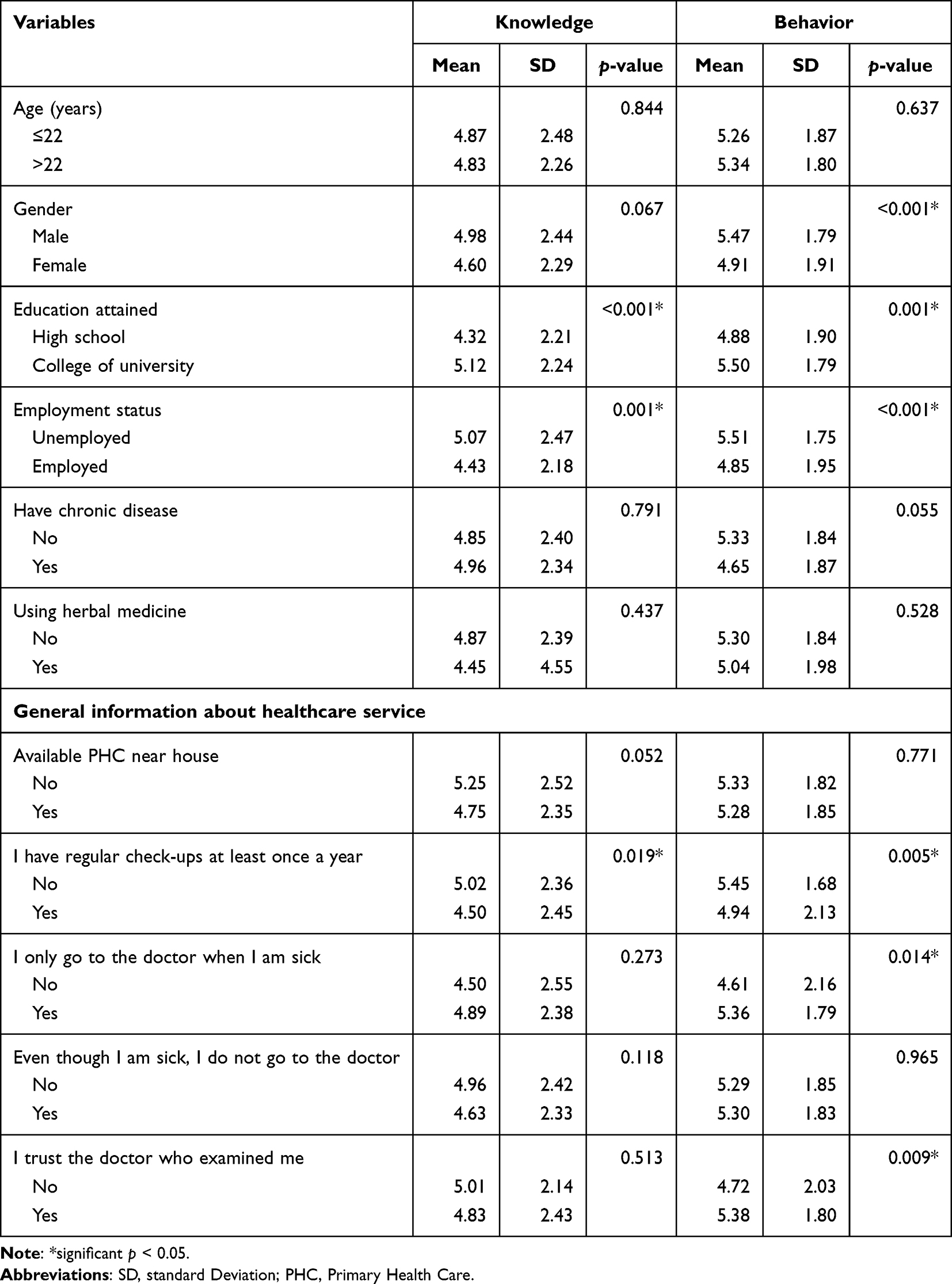 |
Table 2 Comparison of Participants’ Characteristics and Mean Scores of Knowledge and Behavior in Using Antibiotics |
To identify the variables associated with good behavior in antibiotic use, this study used a linear multiple regression analysis (Table 3). Twelve variables, including age, gender, education, employment status, chronic disease, herbal medicine consumption, general healthcare information (five items), and knowledge, were examined. The results indicated that employment status (p = 0.004, β = −0.451), trust in the examining doctor (p = 0.004, β = 0.568), and knowledge about antibiotics (p < 0.001, β = 0.361) were significantly linked to good behavior in antibiotic use. Collectively, these factors accounted for 29% of the variance in the outcomes (F = 20.77, p < 0.001).
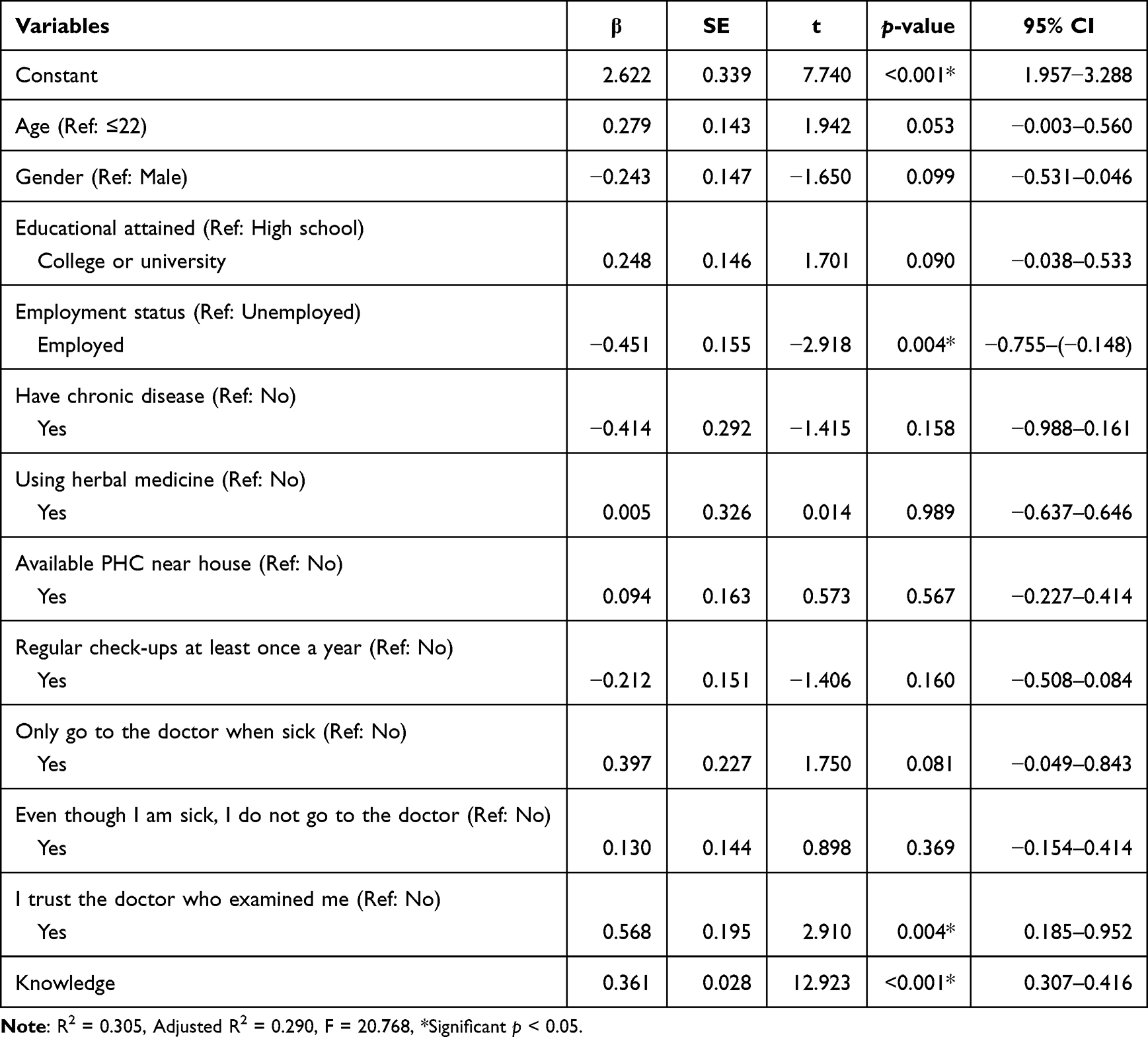 |
Table 3 Factors Influencing the Appropriate Use of Antibiotics |
Discussion
This study provides a descriptive indication that less than 60% of the respondents possessed moderate to adequate knowledge and behavior regarding the utilization of antibiotics, with scores exceeding the mean of the total scores for knowledge and behavior. Participants also demonstrated awareness of the appropriate indications for antibiotics in treating bacterial infections. Similar results were also observed in studies conducted in Thailand,14 Myanmar,15 and Sweden,16 suggesting that individuals in both developed and developing countries understand that antibiotics are intended for the treatment of bacterial infections. This knowledge is an important step in promoting appropriate antibiotic use and combating the global issue of antibiotic resistance.17 However, certain studies highlighted a concerning finding, where a significant number of individuals believe that antibiotics can be used to treat various illnesses indiscriminately.11,17 This misconception poses a challenge to effective antibiotic stewardship efforts.
Moreover, differentiating between bacterial and viral infections is crucial in determining the appropriate use of antibiotics.18 Unfortunately, some individuals struggle to identify the causative agent of their infection, producing the misconception that antibiotics can also effectively treat viral infections.17,18 This lack of clarity regarding the nature of infections further contributes to the inappropriate use of antibiotics and the potential development of antibiotic resistance.
Consistent with findings from previous studies,11,17 the study participants demonstrated knowledge regarding certain aspects of appropriate antibiotic use. Participants were aware that it is not advisable to save antibiotic prescriptions for future use and that antibiotics should not be shared with others. Additionally, most participants acknowledged the importance of completing the full course of antibiotics as prescribed. These findings align with those from a similar study conducted in Saudi Arabia,19 where individuals were also aware of these principles.
Importantly, a small percentage of participants in our study held misconceptions regarding the necessity of antibiotics. They expected to be prescribed antibiotics whenever they fell ill, and in some cases, believed it was acceptable to purchase previously prescribed antibiotics without consulting a healthcare professional. These misconceptions mirror the findings from studies conducted in Malawi20 and Bangladesh,21 where a significant number of respondents engaged in self-medication practices involving antibiotics. Unfortunately, in these instances, individuals were not fully aware of the potential adverse drug reactions or the development of antibiotic resistance associated with inappropriate antibiotic use. Therefore, the importance of a correct understanding of antibiotic usage should not be underestimated, a point further supported by a study conducted by Bert et al22, which found a positive correlation between knowledge of antibiotics and adherence to treatment guidelines.
In this study, we discovered that employment status serves as a significant determinant of proper antibiotic utilization. This finding is consistent with a previous study conducted in Italy,23 which revealed that unemployed participants possessed less knowledge about antibiotics. It is essential to address the specific challenges and knowledge gaps faced by unemployed individuals. This can be achieved by offering accessible and tailored educational resources, conducting awareness campaigns in job centers or community support programs, and involving healthcare professionals in these initiatives. Such efforts can contribute to enhancing understanding and promoting appropriate antibiotic use among this group.24,25
Another factor found in this study that correlates with the proper use of antibiotics is the trust individuals place in their healthcare providers. Trust plays a pivotal role in determining the appropriateness of antibiotic use. A previous study by Guo et al26 found that by building on cultural capital related to appropriate antibiotic use and leveraging the trust in doctors, there are also opportunities to educate the community on the proper use of antibiotics.
Furthermore, according to the findings of this study, the primary approach to addressing the inappropriate use of antibiotics should be to raise public awareness regarding the responsible utilization of antibiotics. Emphasizing the importance of consulting with a healthcare professional before initiating antibiotic therapy is paramount. By correcting misconceptions and disseminating accurate information, it is possible to enhance individuals’ understanding of the potential risks and consequences associated with self-administration or improper use of antibiotics. Enhancing comprehension of antibiotic use can ultimately contribute to improved healthcare practices and the reduction of adverse outcomes resulting from inappropriate antibiotic usage.
Limitations
This study has certain limitations, particularly regarding the methods employed and the data collected. First, important data related to respondents’ history of healthcare facility visits, infection history, previous antibiotic use, and specific antibiotic names were not included, which may introduce bias into the findings. Additionally, the study did not differentiate between urban and rural respondents, potentially impacting the results. Furthermore, the research primarily included a high number of undergraduate students, raising concerns about the generalizability of the findings to other populations or contexts. To address these limitations, future investigations should validate the findings using larger and more diverse cohorts. Employing objective measures of medication adherence would ensure a more accurate assessment of behavior.
Despite these limitations, the present research highlights the importance of employment status, trust in physicians, and a good knowledge base in determining the appropriateness of antibiotic use. Building upon prior research, our study emphasizes the need for customized interventions, healthcare policies, and patient education programs to promote responsible antibiotic use. These findings underscore the significance of adopting comprehensive strategies that address the diverse factors influencing antibiotic use, with the goal of improving patient outcomes and minimizing the risks associated with inappropriate antibiotic use.
Conclusion
This study emphasizes the importance of knowledge and behavior regarding antibiotic use within the Indonesian population. Overall, respondents with knowledge and behavior scores above the population’s average are below 60%. Furthermore, a significant number of respondents exhibited misconceptions regarding the efficacy of antibiotics for viral infections. Addressing these misconceptions through targeted educational interventions and promoting responsible antibiotic use is a priority in combating antibiotic resistance and ensuring optimal treatment outcomes in Indonesia.
Compliance with Ethical Standards
The study was approved by Health Research Ethics Committee of Universitas Padjadjaran, Indonesia (registration number: 1380/UN.6.KEP/EC/2019).
Acknowledgment
We would like to express our gratitude to Anggia Diani Amaliah, Vania Putri, Hidayatun Nisa, Ellena Maggyvin, and Giovanni Wijonarko for their invaluable support and assistance in the data collection process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Universitas Padjadjaran through a research grant for RA (Grant Number 1397/UN6.3.1/PM/2020).
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. WHO. Antimicrobial resistance; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance.
2. Davies J, Davies D. Origins and evolution of antibiotic resistance. Microbiol Mol Biol Rev. 2010;74(3):417–433. doi:10.1128/MMBR.00016-10
3. Kardas P, Devine S, Golembesky A, Roberts C. A systematic review and meta-analysis of misuse of antibiotic therapies in the community. Int J Antimicrob Agents. 2005;26(2):106–113. doi:10.1016/j.ijantimicag.2005.04.017
4. Hadi U, Kuntaman K, Qiptiyah M, Paraton H. Problem of antibiotic use and antimicrobial resistance in Indonesia: are we really making progress. Indones J Trop Infect Dis. 2013;4(4):5–8. doi:10.20473/ijtid.v4i4.222
5. WHO. Global antimicrobial resistance surveillance system (GLASS) report: early implementation 2020. Geneva: World Health Organization; 2020.
6. Limato R, Lazarus G, Dernison P, et al. Optimizing antibiotic use in Indonesia: a systematic review and evidence synthesis to inform opportunities for intervention. Lancet Reg Health. 2022;2:100013. doi:10.1016/j.lansea.2022.05.002
7. Limato R, Broom A, Nelwan EJ, Hamers RL. A qualitative study of barriers to antimicrobial stewardship in Indonesian hospitals: governance, competing interests, cost, and structural vulnerability. Antimicrob Resist Infect Control. 2022;11(1):85. doi:10.1186/s13756-022-01126-7
8. Davey P, Pagliari C, Hayes A. The patient’s role in the spread and control of bacterial resistance to antibiotics. Clin Microbiol Infect. 2002;8 Suppl 2:43–68. doi:10.1046/j.1469-0691.8.s.2.6.x
9. Spellberg B, Bartlett JG, Gilbert DN. The future of antibiotics and resistance. N Engl J Med. 2013;368(4):299–302. doi:10.1056/NEJMp1215093
10. WHO. Antimicrobial stewardship programmes in health-care facilities in low- and middle-income countries; 2019. Available from: https://apps.who.int/iris/bitstream/handle/10665/329404/9789241515481-eng.pdf.
11. Widayati A, Suryawati S, de Crespigny C, Hiller JE. Knowledge and beliefs about antibiotics among people in Yogyakarta City Indonesia: a cross sectional population-based survey. Antimicrob Resist Infect Control. 2012;1(1):38. doi:10.1186/2047-2994-1-38
12. Charan J, Biswas T. How to calculate sample size for different study designs in medical research? Indian J Psychol Med. 2013;35(2):121–126. doi:10.4103/0253-7176.116232
13. Awad AI, Aboud EA. Knowledge, attitude and practice towards antibiotic use among the public in Kuwait. PLoS One. 2015;10(2):e0117910. doi:10.1371/journal.pone.0117910
14. Tangcharoensathien V, Chanvatik S, Kosiyaporn H, et al. Population knowledge and awareness of antibiotic use and antimicrobial resistance: results from national household survey 2019 and changes from 2017. BMC Public Health. 2021;21(1):2188. doi:10.1186/s12889-021-12237-y
15. Miyano S, Htoon TT, Nozaki I, Pe EH, Tin HH. Public knowledge, practices, and awareness of antibiotics and antibiotic resistance in Myanmar: the first national mobile phone panel survey. PLoS One. 2022;17(8):e0273380. doi:10.1371/journal.pone.0273380
16. André M, Vernby A, Berg J, Lundborg CS. A survey of public knowledge and awareness related to antibiotic use and resistance in Sweden. J Antimicrob Chemother. 2010;65(6):1292–1296. doi:10.1093/jac/dkq104
17. WHO. WHO multi-country survey reveals widespread public misunderstanding about antibiotic resistance; 2015. Available from: https://www.who.int/news/item/16-11-2015-who-multi-country-survey-reveals-widespread-public-misunderstanding-about-antibiotic-resistance.
18. Gunasekera YD, Kinnison T, Kottawatta SA, Silva-Fletcher A, Kalupahana RS. Misconceptions of Antibiotics as a Potential Explanation for Their Misuse. A Survey of the General Public in a Rural and Urban Community in Sri Lanka. Antibiotics (Basel). 2022;11(4). doi:10.3390/antibiotics11040454
19. Alnasser AHA, Al-Tawfiq JA, Ahmed HAA, et al. Public knowledge, attitude and practice towards antibiotics use and antimicrobial resistance in Saudi Arabia: a web-based cross-sectional survey. J Public Health Res. 2021;10(4):
20. Sambakunsi CS, Småbrekke L, Varga CA, Solomon V, Mponda JS. Knowledge, attitudes and practices related to self-medication with antimicrobials in Lilongwe, Malawi. Malawi Med J. 2019;31(4):225–232. doi:10.4314/mmj.v31i4.2
21. Biswas M, Roy MN, Manik MI, et al. Self medicated antibiotics in Bangladesh: a cross-sectional health survey conducted in the Rajshahi City. BMC Public Health. 2014;14:847. doi:10.1186/1471-2458-14-847
22. Bert F, Gualano MR, Gili R, et al. Knowledge and attitudes towards the use of antibiotics in the paediatric age group: a multicenter survey in Italy. Eur J Public Health. 2016;27(3):506–512.
23. Napolitano F, Izzo MT, Di Giuseppe G, Angelillo IF. Public knowledge, attitudes, and experience regarding the use of antibiotics in Italy. PLoS One. 2013;8(12):e84177. doi:10.1371/journal.pone.0084177
24. Andermann A. Taking action on the social determinants of health in clinical practice: a framework for health professionals. Cmaj. 2016;188(17–18):E474–e83. doi:10.1503/cmaj.160177
25. Mathew P, Sivaraman S, Chandy S. Communication strategies for improving public awareness on appropriate antibiotic use: bridging a vital gap for action on antibiotic resistance. J Family Med Prim Care. 2019;8(6):1867–1871. doi:10.4103/jfmpc.jfmpc_263_19
26. Guo H, Hildon ZJ, Chow A. ”Antibiotics are for everyone, our past and our future generations, right? If antibiotics are dead, we will be in big trouble”: building on community values for public engagement on appropriate use of antibiotics in Singapore. Front Public Health. 2022;10:1001282. doi:10.3389/fpubh.2022.1001282
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Psychiatric Nurses’ Knowledge, Attitudes, and Practice Regarding Physical Restraint in China: A Multicentre Cross-Sectional Study
Chong Y, Wang C, Zhi T, Fang S, Min H, Zhang L, Wu X, Wang Y
Journal of Multidisciplinary Healthcare 2023, 16:1475-1489
Published Date: 29 May 2023
Assessing the Knowledge, Attitudes, and Vaccination Practices Towards COVID-19 Vaccination Among Mainland Chinese Nursing Students and Interns: A Multicenter Cross-Sectional Study

Qin Z, Ye X, Liu H, Tao Y, Zheng X, Zhong Y, Chen D, Ye W, Zhan C
Infection and Drug Resistance 2023, 16:4717-4728
Published Date: 20 July 2023
Public Knowledge, Attitudes, and Practices Regarding the Use of Over-The-Counter (OTC) Analgesics in Indonesia: A Cross-Sectional Study
Sinuraya RK, Wulandari C, Amalia R, Puspitasari IM
Patient Preference and Adherence 2023, 17:2569-2578
Published Date: 17 October 2023
Comprehensive Knowledge, Attitudes, Behaviors, and Associated Factors of HIV/AIDS in Gondar City Public Health Facilities Among HIV Testing and Counselling Service Users, Northwest Ethiopia, 2022; an Ordinal Logistic Regression Analysis
Terefe B, Techane MA, Assimamaw NT
HIV/AIDS - Research and Palliative Care 2023, 15:713-726
Published Date: 7 December 2023
Oral Health Knowledge, Attitude, and Behavior Among Health Professions’ Students at Kabul University of Medical Sciences
Ehsan H, Ahmadzai N, Orfani Z, Rezayee BM, Wally M, Daftani S
Clinical, Cosmetic and Investigational Dentistry 2023, 15:349-358
Published Date: 13 December 2023