Back to Journals » Infection and Drug Resistance » Volume 16
Understanding Post-Sepsis Syndrome: How Can Clinicians Help?
Authors van der Slikke EC ![]() , Beumeler LFE
, Beumeler LFE ![]() , Holmqvist M, Linder A, Mankowski RT, Bouma HR
, Holmqvist M, Linder A, Mankowski RT, Bouma HR ![]()
Received 10 June 2023
Accepted for publication 21 September 2023
Published 29 September 2023 Volume 2023:16 Pages 6493—6511
DOI https://doi.org/10.2147/IDR.S390947
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Elisabeth C van der Slikke,1 Lise FE Beumeler,2,3 Madlene Holmqvist,4 Adam Linder,4 Robert T Mankowski,5 Hjalmar R Bouma1,6
1Department of Clinical Pharmacy and Pharmacology, University of Groningen, University Medical Center Groningen, Groningen, 9713GZ, the Netherlands; 2Department of Intensive Care, Medical Centre Leeuwarden, Leeuwarden, 8934AD, the Netherlands; 3Department of Sustainable Health, Campus Fryslân, University of Groningen, Groningen, 8911 CE, the Netherlands; 4Department of Infection Medicine, Skåne University Hospital Lund, Lund, 221 84, Sweden; 5Department of Physiology and Aging, University of Florida, Gainesville, FL, 32610, USA; 6Department of Internal Medicine, University of Groningen, University Medical Center Groningen, Groningen, 9713GZ, the Netherlands
Correspondence: Hjalmar R Bouma, Department of Clinical Pharmacy and Pharmacology, University Medical Center Groningen, P.O. Box 30.001, EB70, Groningen, 9700 RB, the Netherlands, Tel +31 (0) 50 361 7870, Email [email protected]
Abstract: Sepsis is a global health challenge, with over 49 million cases annually. Recent medical advancements have increased in-hospital survival rates to approximately 80%, but the escalating incidence of sepsis, owing to an ageing population, rise in chronic diseases, and antibiotic resistance, have also increased the number of sepsis survivors. Subsequently, there is a growing prevalence of “post-sepsis syndrome” (PSS). This syndrome includes long-term physical, medical, cognitive, and psychological issues after recovering from sepsis. PSS puts survivors at risk for hospital readmission and is associated with a reduction in health- and life span, both at short and long term, after hospital discharge. Comprehensive understanding of PSS symptoms and causative factors is vital for developing optimal care for sepsis survivors, a task of prime importance for clinicians. This review aims to elucidate our current knowledge of PSS and its relevance in enhancing post-sepsis care provided by clinicians.
Keywords: post-sepsis syndrome, sepsis, long-term outcome
Introduction
Sepsis is defined as a dysregulated host response to infection and is a leading cause of death worldwide, affecting over 49 million people and causing approximately 11 million deaths annually1 - a concern that the World Health Organization recognizes as a global health priority.2 Notably, these figures only include in-hospital deaths; the outcome of the other 38 million sepsis survivors discharged from the hospital varies significantly. The mortality rate within one year after hospital discharge ranges between 7% and 43%3 and five-year mortality rates after sepsis are between 44% and 82%.4–6 Due to the ageing population, increased prevalence of chronic diseases and antibiotic resistance, the incidence of sepsis is rising and thereby also the number of sepsis survivors.
The rising number of sepsis survivors warrants the need for appropriate care after sepsis. Around 75% of sepsis survivors develop at least one new medical, psychological, or cognitive diagnosis after hospital discharge.7 Only half of the sepsis survivors (both ICU and non-ICU) achieve complete or near-complete recovery within two years after hospital discharge.8 On the other hand, one in six patients experiences persistent impairments.8 As such, sepsis survivors are at risk for rehospitalization, recurrent infections and chronic illness and have a shorter life expectancy, and lower quality of life.9–14 Therefore, there is a need to increase awareness for the so-called “post-sepsis syndrome” (PSS): a constellation of long-term physical, medical, cognitive, and psychological issues following sepsis recovery that puts survivors at risk for hospital readmission, and is associated with a reduction in health and life span.
Within the first 30 days following hospital discharge, one in five sepsis survivors is readmitted to the hospital and one in three is readmitted within 90 days.9,15 Recurrent sepsis is the leading diagnosis for 30-day readmissions, accounting for almost one-third to half of them.11,15,16 Other common complications are pneumonia, kidney failure,17 heart and respiratory failure.11,15 Notably, sepsis survivors have a significantly increased risk of cardiac events up to 5 years after the sepsis episode as compared to age-/sex-matched population control subjects.18–21 Together, post-sepsis complications increase healthcare utilisation and societal burden.22
Additionally, many sepsis survivors struggle with physical and cognitive dysfunctions after sepsis. Compared to age-matched controls, individuals who survive sepsis have a decrease in health-related quality of life (QoL), particularly in the physical domain, persisting for at least five years following discharge.14 Moreover, almost 60% of severe sepsis survivors have worsened cognitive and/or physical function persisting at least 8 years after hospital discharge.23 This decline in physical function becomes evident during walking and taking the stairs amongst others, which results in limitations in carrying out routine daily activities.24 These consequences extend to their professional lives, with nearly half of previously employed sepsis survivors unemployed after recovery from an ICU-admitted sepsis episode.25
(Tentative) Definition and Pathophysiology of Post-Sepsis Syndrome
Post-sepsis syndrome can manifest in various ways including fatigue, weakness, difficulties in memories, anxiety and reduced quality of life.26 Thus, any individual who survived sepsis and is experiencing persistent long-term complaints can be identified as having PSS. PSS is associated with several pathophysiologic mechanisms that negatively affect long-term health and lifespan. These pathophysiologic mechanisms include a complex interplay of immune dysregulation,27 persistent inflammation,27 oxidative stress28 and mitochondrial dysfunction.29,30 These pathways of residual risk continue to be active even after the patient has clinically recovered from sepsis and thereby makes them more prone to long-term health problems (Figure 1). PSS shares many similarities with the post-intensive care syndrome (PICS). In fact, 70% of the sepsis survivors suffer from PICS within the first three months after ICU discharge.31 Further, long-COVID, which is also referred to as post-acute sequelae of SARS-CoV-2 infection (PASC), shows many similarities with both PICS and PSS.32 The overlap between these conditions in terms of symptoms and patients affected, raises the question whether these should be considered separate entities or whether they represent the same condition. However, it should be noted that PICS per definition affects only patients who had been admitted to the ICU, while PSS can also affect individuals with sepsis who had not been admitted to the ICU. The recent COVID-19 pandemic led to huge numbers of patients suffering from long-COVID syndrome. Although it is unclear whether long-COVID is a different disease entity or represents the same condition as PSS, we deliberately decided to describe the long-term sequelae of sepsis irrespective of the specific pathogen. The long-term consequences after COVID, including potential mechanisms and recommendations, are described in an excellent review by Davis et al and could apply to non-COVID sepsis as well.33 To our knowledge, there is no specific definition of PSS. Therefore, to facilitate identification of patients at risk for a reduced long-term health and life span, to support research and exchange of knowledge, we propose to use the following definition of PSS: “medical, psychological or cognitive problems arising after sepsis that required hospitalization, that persist weeks to months after hospital discharge, negatively impacts the functioning of the individual and for which no alternative diagnosis can be found”. Insight in the (cause of) long-term symptoms and health problems of PSS is essential to develop personalised post-sepsis care to manage the impact of sepsis and improve long-term outcome. In this review, we summarise important aspects of PSS and explore how clinicians can help to mitigate the health problems that may arise after sepsis.
 |
Figure 1 Conceptual model of post-sepsis syndrome. Abbreviations: BBB, blood–brain barrier; PTSD, post-traumatic stress disorder; DNA, deoxyribonucleic acid; QoL, quality of life. Notes: Proposed pathophysiological mechanism of PSS, including cerebral ischemia, damage to the blood–brain barrier (BBB), sustained neuroinflammation, immune dysfunction potentially linked to epigenetic modifications in leukocytes, mitochondrial dysfunction and mitochondrial DNA damage, pre-existing comorbidities, polypharmacy, and patient frailty. The manifestation of PSS spans across multiple organ systems, impairing overall functionality, diminishing the quality of life, and potentially curtailing survival rates in post-sepsis scenarios. The figure was created with Biorender and based on our review on the pathophysiology of post-sepsis syndrome.26 |
Mitigating Injury in Sepsis
There are various ways to mitigate the impact of sepsis on long-term morbidity and mortality. Apart from preventing sepsis itself, mitigating injury during sepsis is of utmost importance. Mitigating injury in sepsis involves a multi-pronged approach aimed at treating the underlying infection, supporting organ function, and managing inflammation.34–36 It is important to note that the management of sepsis is complex and requires a team-based approach involving critical care physicians, infectious disease specialists, and other healthcare professionals – both for individuals admitted to the intensive care unit (ICU) and those at the general wards. Early recognition and prompt treatment of sepsis are critically important to prevent injury and improve outcomes. Early administration of appropriate antibiotics remains the cornerstone of bacterial sepsis treatment and is essential for infection control, particularly if administered in the critical early hours.34 In addition to source control, providing optimal supportive care is critical to avert organ failure and comprises titrated oxygen therapy to prevent hypoxemia and hyperoxia, fluid resuscitation to stabilise blood pressure while trying to maintain euvolemia and administration of vasopressors as additional blood pressure support.35,36 Providing early nutritional support during sepsis is crucial, because sepsis results in increased metabolic demands, marked by a sudden catabolic response that triggers the breakdown of energy stores such as glycogen and lipid stores to facilitate glucose production, leading to rapid muscle loss.37,38 Determining appropriate calorie and protein requirements for septic patients can be challenging due to factors such as variations in metabolic rate, changing energy needs over time and between patients, and the potential for underfeeding when energy requirements are underestimated. Individualised caloric goals based on measuring resting energy expenditure using indirect calorimetry are ideal and nutritional screening at different stages of the septic process may be more appropriate than a single approach, as sepsis can impact the feeding process in various ways over time, due to multi-organ failure or gastrointestinal dysfunction amongst others.38,39
Mitochondria play a key role in energy homeostasis in sepsis and mitochondrial dysfunction is a common feature of sepsis that is associated with poor outcome.39,40 However, even with the correct administration of calories and nutrients, patients may not be able to process these delivered nutrients when mitochondrial dysfunction occurs. In turn, dysfunction of the mitochondria can lead to impaired cellular metabolism, oxidative stress, and cell death,41 thereby contributing to multi-organ failure, as well as long-term complications in survivors of sepsis.29 The increased oxidative stress resulting from dysfunctional mitochondria induces damage to lipid, proteins, and DNA and thereby affects mitochondrial integrity. Increased levels of oxidised nucleobases (ie, the building block of DNA and RNA) in sepsis are associated with lower long-term survival after sepsis.42 It is unclear whether mitochondrial damage is restored after sepsis. Strategies aimed at improving mitochondrial function may offer potential therapeutic benefits for patients with sepsis.43 Up to this point, interventions that target the renewal of mitochondria or use mitochondria-targeted antioxidants showed promising results in preclinical studies: such interventions can increase energy production (ATP), improve mitochondrial mass, reduce inflammation, and improve survival.30,44,45 One of these interventions, for example, is Mdivi-1, a pharmacological inhibitor of mitochondrial fission (ie, a process whereby mitochondria split into two daughter-organelles), which increases membrane potential and ATP production while decreasing ROS generation. The use of Mdivi-1 has been associated with improved survival rates in pre-clinical sepsis models.46–48
Another important factor in mitigating injury is managing inflammation. Sepsis was traditionally considered a hyper-inflammatory syndrome, but there is also an immunosuppressive phase that occurs concurrently with the hyperinflammatory phase.49 Immunosuppression is apparent early in sepsis and persists even after the patient is discharged from the hospital.50 Prolonged immunosuppression is a significant component of the post-sepsis syndrome, as it appears to be responsible for the high rate of lethal infections and sepsis recurrence.9,11,51 Sepsis causes long-term changes in cellular immune function and has a lasting impact on both innate and adaptive immune responses, leading to immune suppression, chronic inflammation, and persistence of bacterial infections.9,11 Improving immune function during sepsis and thereby improving long-term outcome have proven to be difficult, and the perfect solution has not yet been found.52,53 Considering the heterogeneity of sepsis syndrome and heterogeneity in patients as well, a single-agent approach would probably not work, but rather a combination of different agents, and if possible, personalised per patient in order to achieve the best outcome.53
Preventing Sepsis Recurrence
By prioritising the prevention of sepsis and sepsis recurrence, the number of patients suffering from PSS will be significantly reduced. Important factors in preventing sepsis and sepsis recurrence are antibiotic stewardship programs to prevent antibiotic resistance, hand hygiene, vaccination programs, preventing infections in healthcare settings, attention for nutrition and food, and creating awareness among the population. From these measures, the most important, cost-effective, and uncomplicated way to decrease the prevalence of healthcare-associated infections and antimicrobial resistance is proper hand hygiene.54 The combination of interactive educational programs and the provision of hand disinfectants has led to a substantial improvement in hand hygiene compliance.54 Another relatively simple measure to prevent some important causes of sepsis is vaccination. Examples of these are the annual vaccinations against COVID-19, influenza and pneumococcal disease.55,56 Immunisation has significantly reduced the incidence of bacterial meningitis, pneumonia, and overwhelming infections in children caused by Haemophilus influenzae type B and Streptococcus pneumoniae, which are the primary pathogens responsible for these illnesses.57 Implementing such practices to prevent sepsis can therefore reduce the incidence of PSS. Thus, it is crucial for clinicians to promote and encourage proper hand hygiene practices as well as vaccination among individuals.
Sepsis Awareness
Another important step in early recognition and potentially preventing sepsis is becoming aware of its existence. The awareness of sepsis among the population varies significantly between countries, region, sex, education level and ethnicity.58 For example, in an international survey using structured telephone interviews among 6021 interviewees in Europe and the United States, it was found that in Spain, the United Kingdom, Italy, France, and the United States, a mean of 88% of interviewees had never heard of the word sepsis, compared to 47% in Germany.59 Of these interviewees who knew sepsis, 58% did not recognize it as a leading cause of death. A Swedish study showed that only 21% of adults knew about sepsis in 2015, however this number has increased to 58% in 2023 according to the Swedish Sepsisfonden.60 A Canadian study, which administered an online structured survey to English- or French-literate adults, showed that 39% did not know the word sepsis.58 Of the 61% of persons who heard of sepsis, only 25% recognized vaccination as a preventive measure against sepsis.58 Furthermore, only 32% were aware of the symptoms and 17% of the risk factors of sepsis.58 Ambiguity surrounding the definition of sepsis may be a contributing factor to the low overall unawareness of the condition among the general population.61 The term “blood poisoning” often used indicates the presence of bacteria in the blood but the fact is that only one-third of sepsis patients have a positive blood culture contributes to the complicity in giving the correct diagnosis.62 In response to this unawareness, governments and non-governmental organisations worldwide are arranging major awareness campaigns. One example of this is the World Sepsis Day, first organised in 2012 by the Global Sepsis Alliance and founders.61 In a scoping review, media and internet were both cited as the most common source to find information about sepsis. People were more inclined to seek information on sepsis when high-profile sepsis-related stories were published, such as the death of a celebrity, which could increase the relative search volume on the internet with 550%.63,64 However, despite its prevalence and high fatality rate, sepsis relative search volume on the internet is lower than that of influenza, stroke, and myocardial infarction, indicating that awareness of sepsis should be improved.64 Clinicians could help by stimulating public education campaigns such as the World Sepsis Day61 and also by creating educational materials like brochures, posters, infographics, and pamphlets that explain what sepsis is, explain its risk factors and describe how to seek help when needed. Efforts made to collaborate with schools and universities to include sepsis awareness lectures in the education curriculum during biology-related classes for example, or create informative social media accounts should be further implemented.65
Antibiotic Stewardship
Furthermore, appropriate antimicrobial therapy is an essential part in the management of sepsis. Prompt administration of antimicrobial therapy is crucial in improving patient outcomes, as delays in treatment have been associated with increased mortality.66 However, potential unintended consequences of inappropriate antimicrobial prescribing, such as the development of antimicrobial resistance and healthcare-associated infections, are problematic. Antibiotic stewardship programs are important to address this issue, which use strategies aimed at improving the appropriate use of antibiotics. The implementation of antibiotic stewardship programs in hospitals can lead to a significant reduction in antibiotic consumption and rates of hospital-acquired infections such as C. difficile infections, without compromising clinical outcomes.67 As such, a meta-analysis showed that the risk of hospital-acquired infections was reduced by 48% in studies that included an infection control or hand hygiene program in addition to an antibiotic stewardship program. On the other hand, studies that did not have an infection control program did not show any significant reduction in the risk of hospital-acquired infections.67 In addition, antibiotic stewardship programmes significantly decrease the occurrence of infections and colonisation with antibiotic-resistant bacteria and C. difficile infections among hospitalised patients.68 Another systematic review and meta-analysis showed that de-escalation therapy and prescribing empirical therapy according to guidelines, two important antibiotic stewardship methods, significantly reduced mortality in hospitalized patients with infection. Guideline-adherent empirical therapy was associated with a relative risk reduction for mortality of 35% and for de-escalation of 56%.69 On the other hand, septic patients who are exposed to high-risk antibiotics or receive increased quantities of antibiotics during their hospitalisation have an elevated risk of sepsis within 90 days of discharge.70 Thus, antibiotic stewardship programs are important to not only optimise antibiotic use but also decrease the risk of sepsis and sepsis recurrence.68,70–73 This necessitates doctors to adhere to existing antibiotic guidelines and exercise thoughtful consideration before administering antibiotics.
Physical Complaints After Sepsis
Fatigue
Fatigue is a very common problem after sepsis and is reported in two out of three sepsis survivors during the first year after hospitalisation.74 Fatigue has a major impact on life, as it also influences the ability to focus during conversations, reading and overall concentration during the day.75 A large multinational survey taken among 1731 sepsis survivors within 5 years after hospital discharge demonstrated that one in three survivors was not back to normal pre-hospital health at the time of the survey. Sepsis survivors stated an increase in sensory, integumentary, digestive, breathing, chest pain, kidney and musculoskeletal problems, as compared to pre-hospitalization.24 More importantly, of those sepsis survivors only 5.5% said they felt very well after sepsis.24 Another common feature is (poly)neuropathy, also called critical illness polyneuropathy (CIP), which occurs in 70% of septic patients and up to 100% in patients with multi-organ failure.76,77 CIP is a large contributor to muscle weakness and thereby influences quality of life heavily. Thus, recovering from sepsis can be a challenging process, whereby fatigue and exercise intolerance are common symptoms experienced by many individuals. General measures to decrease fatigue such as taking enough time to rest, regularly exercising, stress-managing and supportive care could be helpful in improving symptoms; however, it is important to notice that recovery from sepsis takes time, and everyone’s journey is different. Clinicians can play a role in assisting individuals to reduce fatigue and other physical symptoms by giving advice on lifestyle modifications, medication review, education and psychological support.
Dysphagia
Post-sepsis dysphagia is a common complication of which many sepsis survivors suffer from. In a retrospective cohort study in elderly people with sepsis, approximately 17% experienced dysphagia. Of those with dysphagia, 84% did not regain their swallowing function by the time of hospital discharge.78 Another retrospective observational study showed that 35% of sepsis survivors had persisting dysphagia after hospital discharge.79 Importantly, dysphagia is a well-known risk factor for aspiration and aspiration-induced pneumonia, malnutrition due to delayed resumption of oral intake, reduced quality of life, longer ICU and hospital stays, and heightened morbidity and mortality.80 Risk factors for dysphagia are not yet fully discovered since studies are scarce and provide conflicting results. However, most accepted risk factors are duration of intubation and mechanical ventilation.80 Thus, it is imperative for survivors of severe critical illness, including sepsis, to undergo otorhinolaryngological evaluation for dysphagia at the time of ICU discharge in order to develop specific swallowing rehabilitation programs. Otorhinolaryngological evaluation is mainly done by a trained speech-language pathologist.81 Present treatment options for individuals with swallowing impairments include adjusting dietary texture, adopting specific postures, implementing compensatory techniques, engaging in therapeutic exercises, and utilising nerve stimulation. With the aid of speech-language pathologists, gastroenterologists, otolaryngologists, dieticians and neurologists, critical care practitioners can employ a collaborative, multidisciplinary approach to establish personalised therapies for each patient.82,83
Muscle Loss and Physical Dysfunction After Sepsis
Classification strategies of multiple-organ failure (MOF) in critically ill patients have historically centred on the most clinically obvious organ dysfunctions, primarily the pulmonary, renal, and cardiovascular systems.84,85 However, other peripheral organ systems, such as skeletal muscle, are also affected in patients who survive the initial septic event.86 Although wasting of skeletal muscle in critically ill patients was originally described approximately 5 decades ago,87–89 the acuity and magnitude of muscle wasting and weakness have been rediscovered and re-emphasized.90,91 For example, Puthucheary et al demonstrated a 15% reduction in rectus femoris muscle cross-sectional area within 7 days in patients with MOF, associated with muscle protein synthesis/catabolism imbalance.91 Pre-existing lower muscle mass (sarcopenia)90 and lower fat mass92 may contribute to poor clinical and functional outcomes after sepsis.
Significant and long-lasting functional defects are well described among survivors of critical illness, which may be the effect of acute and chronic muscle wasting, and amplified by greater age.93,94 For example, compared to the young patients, older surgical sepsis patients had poorer functional status and objectively measured physical function and handgrip strength after 12 months of follow-up.93 In addition, older patients remained persistently inflamed with ongoing catabolism.95 While a combination of bed rest and neurologic (dysregulation of neural inputs at the neuromuscular junction), hemodynamic (hypoperfusion) and molecular pathologic factors (mitochondrial and satellite cell dysfunction, and protein breakdown) likely play a role, the underlying mechanisms of the ICU-acquired weakness and long-term functional disability remain poorly understood.96 We will limit our discussion to local skeletal muscle-related mechanisms that contribute to muscle wasting and weakness.
Mitochondrial and Satellite Cell Dysfunction as Major Biological Mechanisms of Muscle Wasting
In addition to the detrimental effect of bed rest and muscle disuse on muscle mass,97 sepsis-induced skeletal muscle catabolism reflects impaired satellite cell and mitochondrial functions, increased proteolysis, decreased protein synthesis and release of degradation products that have pro-inflammatory features as damage-associated molecular patterns (DAMPs) from skeletal muscle mitochondria.30,96,98,99 Satellite cells are the muscle stem cells and a proper function is essential for muscle repair in response to factors such as injury and exercise.30 When activated, satellite cells turn from the quiescent state to start forming myotubes.30 Satellite cells are required for maintenance of lean mass as demonstrated in a mouse model of sepsis, but its function declines in response to sepsis.30,99 Transcriptomic changes of satellite cells induced by sepsis in mice were persistently changed at day 28 after sepsis compared to control, reflecting impaired energetic pathways representing oxidative phosphorylation and mitochondrial dysfunction. These observations reflect impaired satellite cell function and reduced muscle repair.99 The detrimental effect of mitochondrial and satellite cell dysfunctions on the maintenance of muscle energetics and repair warrant further research to develop strategies to target sepsis-induced muscle catabolism state with relevance to prevent muscle loss and functional decline after sepsis.
Exercise Training and Nutrition as a Non-Pharmacological Treatment of Sepsis-Induced Physical Dysfunction
Exercise training, including aerobic and resistance exercise, is one of the most powerful interventions to gain and maintain skeletal muscle mass, skeletal muscle quality and overall physical function.100 Early rehabilitation aimed at maintaining muscle mass and cardiopulmonary function is important to facilitate recovery from critical illness.101,102 However, anabolic resistance and systemic inflammation associated with sepsis may prevent patients from obtaining improvements in the clinical setting. In particular, anabolic resistance is caused by the altered protein homeostasis, which is in turn amplified by intramuscular inflammation and bioenergetic failure from disrupted substrate use.103 Early movement in the ICU has therefore variable results. For example, electrical stimulation of both lower and upper limbs over 5 days in the ICU attenuated muscle loss and proteolysis, but there was no difference in muscle weakness.104 Additionally, electrical stimulation applied within the first 72 hours after ICU admission did not lead to muscle contractile response, but the responsiveness dependent on the disease severity and differed between responders and non-responders.105 Electrical stimulation appears more effective in increasing muscle oxygen uptake, as compared to no effect of passive movements.106
The effects of post-ICU exercise training on functional exercise capacity or health‐related quality of life remain unclear due to variability in intervention protocols and inter-personal heterogeneity.107 Since the anabolic resistance may be the reason for inter-personal heterogeneity in the response to exercise training in the ICU and post-discharge, there is a need for appropriate nutritional strategy related to nutrients and timing in order to stimulate anabolism.108 Early enteral or parenteral nutrition improves overall ICU outcomes, although most beneficial effects are seen with multimodal interventions combining different modalities of exercise training and nutritional regimens to preserve skeletal muscle mass in the ICU and prevent functional decline post-discharge.109 For example, the ExPrES study showed preservation of lower-limb muscle mass by a 14-day multimodal intervention including muscle electrical stimulation, high-protein supplementation and mobility and strength rehabilitation.110 In contrast, addition of a metabolite of leucine (β-Hydroxy-β-methylbutyrate) to the standard nutrition therapy in combination with electrical stimulation did not reduce muscle loss.111 Currently, there are no existing personalised approaches to improve sepsis survivors’ health status and physical function in-hospital and once they return home. To our knowledge, most clinical trials focusing on exercise training112 and nutrition (eg, protein supplementation)113–115 to preserve muscle strength and physical function showed variable results or failed because of the lack of understanding of the pathology and heterogeneity of sepsis-induced physical disability.116,117 Clinicians can play a pivotal role in enhancing the outcomes of sepsis survivors by advocating for and facilitating early rehabilitation, promoting patient-specific exercise and nutritional strategies, and actively participating in the design and execution of personalised care plans. Further, they can contribute to the advancement of our understanding of sepsis-induced physical disability through their involvement in clinical research, facilitating the development of evidence-based personalised approaches to prevent muscle wasting and mobility disability after sepsis.
Cardiovascular Disease
There is a strong correlation between sepsis and several aspects of cardiovascular disease (CVD). Firstly, pre-existing cardiovascular conditions are risk factors for sepsis.118 Secondly, cardiovascular complications such as septic cardiomyopathy are important during the acute phase and contribute to organ dysfunction.119 Thirdly, cardiovascular complications may occur in the post-acute phase after sepsis, both in the first period post discharge and up to several years later. The cause of the increased risk of cardiovascular complications after sepsis is probably multifactorial, including persistent inflammation or immunosuppression, neurohumoral activation, mitochondrial dysfunction, endothelial dysfunction, accelerated atherosclerosis and plaque instability.27 Also, the deprescription of beneficial primary or secondary preventive cardiovascular disease treatments during the acute sepsis episode may contribute to worsening of symptoms or disease progression.120
A meta-analysis of 27 observational studies demonstrated an elevated risk of both short- and long-term cardiovascular events (myocardial infarction, stroke, heart failure) and death after hospitalisation for sepsis, with pooled adjusted HR values of 1.65 to 1.77.121 The increased risk persisted for at least 5 years. However, there was a large variability across the studies, and some of the included studies were of low quality and had methodological drawbacks. Two recently published large studies further confirmed the link between sepsis and cardiovascular risk. The first study, including 250.000 sepsis survivors without pre-existing CVD, demonstrated a 1.3-fold increase in the hazard of major CVD events (myocardial infarction, stroke or cardiovascular death) up to 5 years of follow-up, compared to matched non-sepsis hospital survivors.122 The second study included approximately 2.250.000 patients with increased risk of CVD events who survived a non-surgical hospitalisation, of which approximately 800.000 patients had sepsis.20 The study showed an increased risk of hospitalisation for cardiovascular events in sepsis patients compared to non-sepsis patients (adjusted HR = 1.43). Findings from these two later studies also show that although the absolute risk for an event after sepsis is higher in older patients or in patients with a higher risk profile, the relative increase in CVD risk due to sepsis is higher in younger patients and in patients with few other risk factors for CVD.20,122
Heart failure is the most common cardiovascular event requiring readmission after sepsis.11,20 Sepsis patients have an up to a six-fold higher risk of developing atrial fibrillation compared to hospitalised patients without sepsis.123 The diagnosis of atrial fibrillation associated with sepsis could be either a newly developed arrhythmia or the detection of sub-clinical pre-existing atrial fibrillation. Atrial fibrillation development increases the risk of in-hospital stroke up to three times in sepsis patients.123 However, since there is also an increased risk of bleeding, anticoagulants are not generally recommended during the acute phase.124 Other studies showed that up to 36–61% of the patients with atrial fibrillation during sepsis have recurrent episodes of atrial fibrillation post-sepsis and an increased risk of stroke up to several years after the sepsis episode, with an adjusted HR of 1.22–1.91 as presented in a recent review by Induruwa et al.124 Another recent review and meta-analysis have addressed the long-term risk of cerebrovascular events following sepsis hospitalisation, showing an HR of 1.8 for ischemic or hemorrhagic stroke.125 Therefore, it is important to acknowledge that sepsis is a (non-traditional) risk factor for cardiovascular disease, both atherosclerotic and non-atherosclerotic (ie, heart failure and arrhythmias), and an episode of sepsis should be considered to be an important event in a patient’s medical history. Considering this, clinicians should offer personalised information to patients in order to enhance their understanding of potential signs and symptoms associated with cardiovascular disease.
Cardiovascular Risk Management and Stratification
According to Surviving Sepsis Campaign, there is insufficient evidence to make a general recommendation on early post-hospital discharge follow-up compared to routine post-hospital discharge follow-up for sepsis patients. However, early follow-up might be beneficial, as studies showed that early follow-up of other patient groups, such as elderly patients and patients with congestive heart failure, is associated with reduced hospital readmissions.126,127 Especially early in the post-discharge period it is valuable to reassess the need and dosage of cardiovascular pharmaceutical treatments, considering that deprescription during hospital care is common, and the dosage requirements may be different due to changes in body weight, renal function and cardiac function.8,120 Also, evaluating clinical symptoms and signs such as body weight, blood pressure, heart rate and oxygen saturation is important in order to avoid potential reasons for readmission.
Clinicians offering post-sepsis care should maximise their efforts to prevent the development or mitigate the progression of cardiovascular disease by optimising guideline‐directed pharmacological and non-pharmaceutical therapies, such as smoking cessation and lifestyle recommendations, monitoring and treatment of hypertension and hyperlipidemia, and the addition of antithrombotic therapy in those with established atherosclerotic cardiovascular disease.128 Performing cardiovascular risk factor stratification in patients with pre-existing cardiovascular disease or with known cardiovascular risk factors, as well as in younger, otherwise healthy patients is important to tailor cardiovascular risk management to the needs of the individual patient. Pharmacological preventive interventions such as beta blockers, statins and acetylsalicylic acid could be considered to lower cardiovascular complication risk after sepsis, but large studies providing supporting evidence for these strategies are missing, and they can therefore currently not be recommended on a general basis. Although there is an increased risk for ischaemic stroke in the long-term perspective in patients with sepsis-driven atrial fibrillation, current guidelines offer no recommendations on anticoagulation therapy once they have recovered from sepsis. Outside of guidelines, as Induruwa et al suggest, clinicians may consider offering tailored anticoagulation therapy in a patient-centred care setting124 after careful assessment of the risk of ischaemic stroke and haemorrhagic complications using the CHA2DS2-VASc and HAS-BLED scores. As a minimum, patients should be informed of the symptoms of a new episode of atrial fibrillation and if such symptoms occur they should be examined for the existence of recurrent atrial fibrillation. Early physical rehabilitation could well allow the patient to remobilize after sepsis to maintain an active, healthy lifestyle that is associated with a lower risk of cardiovascular events. Sepsis survivors mention prompt rehabilitation after discharge, physiotherapy and sports as important aspects that should be addressed to improve post-sepsis care,129 all of which could be stimulated by clinicians.
Psychological and Emotional Impact
Cognitive Problems After Sepsis
To date, there is limited information on the impact of sepsis on cognitive functioning. Delirium is most common in severely ill sepsis patients, as compared to patients without sepsis at the ICU.130 Studies describing the effect of sepsis and delirium on long-term cognitive function seem contradictory, as a study in 125 ICU patients with severe sepsis did not find a relation with either sepsis or delirium and self-rated cognitive dysfunction at 3 months after hospital discharge.130 However, another study among 516 severe sepsis survivors and 4517 patients who had been hospitalized for another reason demonstrated a substantial decline in cognitive function at 1 year after hospital discharge as compared to baseline. The incidence of moderate-to-severe cognitive impairments increased by 10% after sepsis and persisted for at least 8 years after sepsis.23 In line with these observations, neonatal sepsis and sepsis in paediatric patients were associated with neuromotor developmental impairments and new neurological disabilities.131,132 The pathophysiology of cognitive impairment in sepsis remains incompletely understood. Yet, several mechanisms have been put forward that appear to underlie cognitive dysfunction after sepsis, including blood–brain barrier (BBB) disruption, neuroinflammation resulting from a BBB disruption and over-activation of microglia and astrocytes, neurotransmitter dysregulation, and neuronal loss. Like dementia, this cognitive impairment is often irreversible, significantly impacting patient quality of life.133 Therefore, clinicians should be alert to these sequelae and act promptly. Although targeting the processes driving cognitive changes in sepsis seems pivotal in preventing or treating cognitive impairment, further studies are needed to expand our fundamental knowledge about the pathophysiology of sepsis-induced cognitive dysfunction and to develop effective treatment strategies.
Psychological Problems After Sepsis
Although reduced QoL after severe illness, like in PSS and PICS, is most prominently linked to long-term physical health complaints, the psychological and emotional consequences are relatively unexplored. Sepsis survivors mention that there is a need for psychological care as one of the unmet needs after hospital discharge.129 The impact of critical illness can reflect in several mental health-related problems, like symptoms of PTSD, anxiety or depression with or without cognitive impairment, as described in several studies in survivors of critical illness, independent of sepsis admission status.134,135 Risk factors like treatment-related stressors may leave patients vulnerable to develop long-term mental and cognitive health problems which can last for years.136,137 Sepsis as primary admission diagnosis was an independent risk factor of stress disorders after critical illness, but specific information on the role of mental health problems within the PSS is lacking.138,139 When comparing mental health-related Qol of survivors of severe sepsis to the general population average, the mental component score and/or mental health domain score were significantly reduced in several studies.14,140,141 Although the difference in mental health-related QoL is less pronounced than in the physical domain scores, survivors may experience unpleasant memories and recall of ICU events which are often stated as trauma-related symptoms. However, other studies show only a temporary decline in mental health-related QoL or no difference with the healthy control at all.142,143 In general, mental health problems such as anxiety, depression, fatigue and sleep disturbances after sepsis are underreported and present in various degrees among the adult patients experiencing PSS.24
Importance of Addressing Psychological and Emotional Complaints After Sepsis
Taking into account the sepsis associated risk factors and long-term outcomes associated with PSS and PICS, the possible vulnerability of the patient group and the possible impact of PSS on the patient and their informal caregivers, addressing psychological and emotional complaints after sepsis in the clinical and primary care setting is essential. Specifically, early screening for and awareness of frailty and impaired resilience may prove effective in identifying patients at risk of PSS.144,145 Nevertheless, clinicians may face important challenges during triage practices when it comes to prioritising the rule of rescue over societal benefits and outcomes of patients, as was described in ICU clinicians previously.146 Awareness of the effects of triage decisions and case management within the post-sepsis recovery period may be essential for clinicians working with patients suffering from PSS.
In addition, patients and informal caregivers may benefit from multidisciplinary aftercare in the post-hospital period. However, this structure is lacking and patients report dissatisfaction with a number of support services in hospital and after discharge.24 Patients report a lack of psychological counselling, education about sepsis and PSS and social support.24 However, implementing aftercare services can be troublesome due to several barriers. A study on enablers and barriers to implementing ICU aftercare from the Thrive collaboratives showed significant barriers to this included lack of access to clinics, clinic funding, limited attendance by patients and relatives and difficulties in the selection and advertising process.147 Enablers for successful implementation that were specified involved beneficial infrastructures, flexibility in scheduling and belonging to an international learning consortium. Taking into account these enablers and barriers to provide adequate support for professionals that want to initiate aftercare services is therefore essential, because more structured aftercare services for patients suffering from PSS and PICS are urgently needed. Especially important in making efforts to create “tailor made sepsis aftercare” is involving patients and relatives and ask them what they think can contribute to their quality of life.
Interventions for Emotional and Psychological Support
Although support in the post-sepsis recovery period is scarce for both patients and informal caregivers, increased awareness of PSS may lead to more initiatives for adequate aftercare. One primary care management intervention including training of patients and primary care physicians in evidence-based post-sepsis care, case management by trained nurses and clinical decision support for primary care physicians by consulting colleagues resulted in a decrease of PTSD-related symptoms compared to usual care.148 However, this study did not find a significant effect on other mental health-related outcomes. Another randomised-controlled trial on a primary care intervention rendered similar results, with no change in mental health-related QoL at six months after ICU discharge.149 Another RCT that investigated recovery after hospitalisation for sepsis and randomised 291 patients to a multicomponent primary care management intervention or usual care also did not find improvements in mental health-related QoL.149 One explanation for the limited effect of post-sepsis interventions could be the need to involve the patient’s social support system, as, for example, a partner.150 When taking a closer look at the general ICU population, there is limited evidence on non-pharmacological interventions. A systematic review showed that the use of diaries and exercise programs during and after admission had a positive impact on mental health outcomes.151 In addition, consultation with a clinical psychologist may help ICU patients with trauma symptoms in their recovery,152 and supporting caregivers can improve short-term anxiety and depression symptoms.153 In conclusion, there is limited support for specific evidence-based interventions to improve mental health in patients suffering from PSS or PICS.
Despite the lack of evidence on interventions to improve mental health outcomes in patients after sepsis, research in other patient groups suggests that patient support programs can be beneficial to improve emotional well-being. For example, an emotional support-focused nursing intervention had a positive impact on psychosocial adjustment of breast cancer patients.154 In addition, involving family members and loved-ones within the patient journey is valued and appreciated by surgical patients.155 Also, social support has been found to improve well-being of cognitively impaired elderly individuals.156 Former sepsis patients mention structural non-medical support frameworks, structures for medical aftercare, financing of aftercare, involvement of relatives and contact point for sepsis aftercare as unmet medical needs after sepsis.129 Clinicians can support patients and caregivers by exploring and recommending appropriate (digital) treatments, delivering or referring to generally adopted interventions to treat anxiety and depression, like cognitive behavioural therapy, or incorporate CBT interventions into their care plans.157,158 Also referring to peer support groups can help patients find support and reflect on the significance of religion and spirituality in the process, a topic that clinicians often neglect.159,160 However, further research with the involvement of experienced experts and patient representatives is needed to investigate support programs specifically targeted towards patients suffering from PSS.
Socio-Medical Aspects of PSS
Surviving sepsis can have far-reaching consequences for patients, and often also their relatives,129 beyond the immediate physical and mental impact described in this review. Patients suffering from PSS often face long-term sociomedical consequences that affect their QoL. One of such consequences is difficulty of returning to work, as the toll of PSS can make it problematic to resume their normal work-related activities. Although studies on the sociomedical consequences of PSS are limited, it has been described that return-to-work rates are similar to those in critical illness survivors, ranging from 60 to 70% up to six years after hospital discharge.161 In addition, sepsis is associated with high morbidity and mortality and survivors usually experience increased healthcare utilisation and financial burden. A retrospective study conducted in the United States found that there was an almost threefold increase in adjusted healthcare utilisation post-sepsis compared to the pre-sepsis levels.162 The extent of this increase was strongly correlated with the age of the patient at the time of admission. Other patient factors that are already present during admission may have a similar impact on post-sepsis healthcare utilisation, like prior comorbidities and a history of high utilisation pre-sepsis. Similar results have been found in patients surviving critical illness, as sepsis during admission was found to result in higher healthcare resource use and costs compared to matched ICU-patients without sepsis.162 There are no targeted interventions to improve return-to-work or reduce healthcare utilisation in patients suffering from PSS. However, previously described interventions in similar populations, like patients suffering from PICS, may be a first step to providing tailored aftercare for patients suffering from PSS.
Personalised Post-Sepsis Care
Given the large interindividual differences in clinical presentation and outcomes among patients with an infection and sepsis, a one-size-fits-all approach is unlikely to benefit every patient. Tailoring post-sepsis care to the specific needs of each patient would pose an opportunity to provide effective support by a multidisciplinary team of healthcare professionals (Table 1). To estimate long-term sepsis outcomes and thereby predicting specific needs, pre-existing risk factors for poor long-term outcomes should be considered.8 Important to realise is the difference in co-morbidities and frailty in individual patients pre-sepsis, but also the social aspects such as having spouses and a well-functioning social safety net.8,163 A promising tool in helping to predict the needs after sepsis is endotype stratification. New research has revealed the possibility of categorising patients with sepsis into different phenotypes based on retrospective clinical data164 or transcriptome data obtained from whole blood.165,166 This type of endotype stratification, utilising clinical and/or molecular data, has the potential to identify patients who may be at higher risk for post-sepsis health problems165 as well as long-term outcomes.164,165 Being aware of potential problems ahead of time allows for timely intervention and mitigation by clinicians.
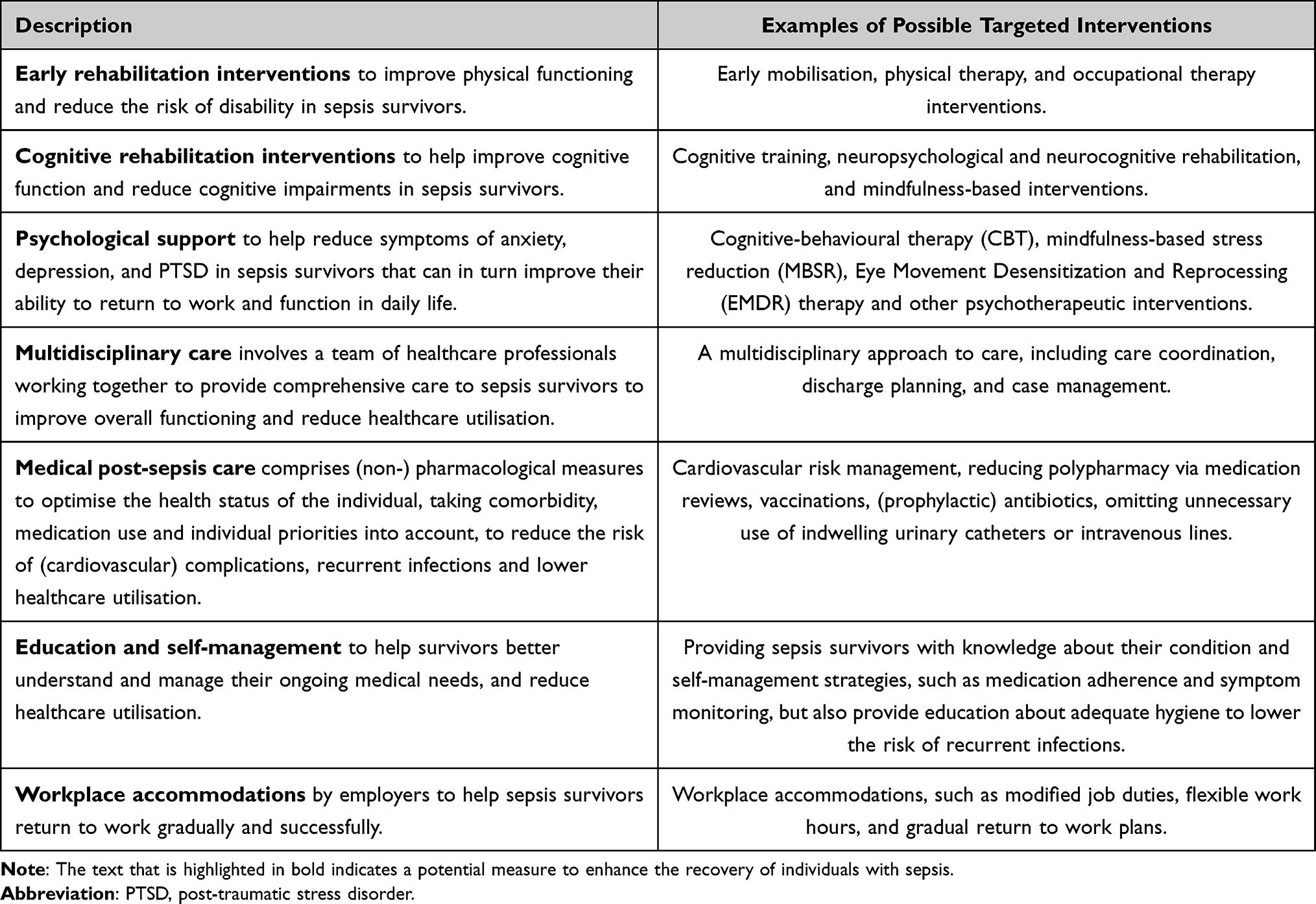 |
Table 1 Possible Multi-Disciplinary Interventions to Improve Recovery in Sepsis Patients by Physiotherapists, Psychologists, Social Workers and Clinicians (Internal Medicine, General Practitioners, Family Doctors and Rehabilitation Physicians Amongst Others) |
Current Advice
More information about risk factors is required to select those individuals at risk for poor long-term outcome to be seen by a specialized post-sepsis outpatient clinic for personalized post-sepsis care. Until this information becomes available, it seems most appropriate to invite all patients with sepsis in hospital, either being admitted to the ward or ICU, to a post-sepsis outpatient clinic to be seen by a consultant in general/internal medicine, geriatrics (in case of frail or elderly persons), general practitioner of family doctor. Based on a comprehensive assessment of medical and functional status, a critical review of current (preventive) treatment should be performed with the main aims to lower risk of recurrent infections and cardiovascular disease, lower healthcare use and improve quality of life (Table 2). Former patients indicate information about what to expect after sepsis as a relevant knowledge gap, which should be addressed during the outpatient follow-up.167 Ideally, given the lack of knowledge about PSS and the information that is required to develop personalized post-sepsis care, the assessment during outpatient follow-up should employ standardized instruments and obtain consent from the patient to use such data for (future) research. Outstanding questions are amongst others: a) how can we identify individuals at risk for poor long-term outcome, who could benefit from personalized post-sepsis care, b) what are effective interventions to improve long-term outcome after sepsis, and c) when should such care be offered? Currently available information suggests that the optimal timing for a first follow-up contact would already be within a month after discharge, since one in three sepsis survivors will be readmitted to the hospital within three months, of which the majority is readmitted within one month.9,15 However, given that most patients may still receive antibiotic treatment and are recovering in this early phase after hospital discharge (eg, temporary nursing home, physiotherapy) this first follow-up visit can be brief and remote (eg, by telephone or video connection) with the aim to evaluate the effect of actual treatment on recovery. A visit to the outpatient clinic at approximately three months after sepsis allows for a more comprehensive evaluation (Table 2) after the initial recovery phase. Future research should provide insight into the questions addressed above, including the optimal timing and content of the follow-up visits.
 |
Table 2 Proposed Content of Post-Sepsis Outpatient Follow-Up by a Clinician |
Conclusion
In conclusion, sepsis is a life-threatening condition with a rising incidence and consequently, an increasing number of sepsis survivors. These survivors are at increased risk of rehospitalization, recurrent infections, chronic illness, a decline in quality of life and shortening of lifespan. The constellation of long-term physical, medical, cognitive, and psychological issues following sepsis recovery is termed post-sepsis syndrome (PSS). PSS can have major effects on health and life span, potentially precluding previously employed patients to return to work after hospital discharge. Addressing this problem necessitates a comprehensive, multi-faceted approach to improve long-term outcomes for survivors.
The pathophysiology of PSS is complex and far from completely understood. Logically, both pre-existing factors such as co-morbidity, polypharmacy and frailty affect outcome, as well as injury induced by sepsis. Consequently, strategies to mitigate injury during sepsis are key to optimise recovery and will entail early recognition of sepsis to allow timely administration of antibiotics and supportive care, as well as unravelling the pathophysiology to develop targeted therapy to avert organ failure. Recurrence of infections – and sepsis – is a frequently encountered problem and could be curtailed through raising sepsis awareness, increasing vaccination rates, practising good hygiene, and promoting appropriate use of antibiotics to ensure effective antibiotic stewardship, as well as preventing infections by omitting unnecessary use of indwelling urinary catheters or intravenous lines. Given the increased cardiovascular risk in sepsis survivors, it is imperative to manage these risks comprehensively, employing not only pharmacological treatment of common cardiovascular risk factors like hypertension, hypercholesterolemia and diabetes mellitus but also physical rehabilitation, optimised nutrient intake and lifestyle advices (eg, stop smoking, maintain an active lifestyle). Furthermore, it is vital to appropriately address the psychological, emotional and cognitive sequelae of sepsis, for example, by implementing support programs aimed at enhancing emotional well-being and quality of life in the long term. Finally, it should be noted that although new physical complaints after sepsis can be part of PSS, it can also represent another underlying disease. Failure to recover or progressive complaints after sepsis recovery should alert the physician to consider other causes of the complaints.
A personalised, patient-centred approach appears to offer the most promise in managing PSS; however, thus far, no personalized approaches to improve sepsis survivors’ health status exist. Managing PSS begins with recognizing and understanding the symptoms, identifying individual risk factors, and elucidating the underlying causes. Such a deep understanding paves the way for selecting patients for specific therapies tailored to their unique needs. Further research is warranted to develop and refine these personalised treatment strategies, with the goal of transforming post-sepsis care and improving the lives of sepsis survivors. More research funding and realisation of centres of expertise that can initiate and coordinate clinical trials can offer sepsis survivors access to novel, potentially effective treatments, before such drugs have obtained market authorization. To this end, it is essential that policymakers realise the societal burden of sepsis and sepsis survivorship.
Acknowledgments
The authors wish to thank I. Nutma, former sepsis patient and chair of the sepsis survivor group “Sepsis-en-daarna” (https://www.sepsis-en-daarna.nl/) for critically revising the manuscript.
Funding
This review received no external funding.
Disclosure
The authors declare that they have no competing interests.
References
1. Fleischmann-Struzek C, Mellhammar L, Rose N, et al. Incidence and mortality of hospital- and ICU-treated sepsis: results from an updated and expanded systematic review and meta-analysis. Intensive Care Med. 2020;46(8):1552–1562. doi:10.1007/s00134-020-06151-x
2. Reinhart K, Daniels R, Kissoon N, Machado FR, Schachter RD, Finfer S. Recognizing Sepsis as a Global Health Priority - A WHO Resolution. N Engl J Med. 2017;377(5):414–417. doi:10.1056/NEJMp1707170
3. Winters BD, Eberlein M, Leung J, Needham DM, Pronovost PJ, Sevransky JE. Long-term mortality and quality of life in sepsis: a systematic review. Crit Care Med. 2010;38(5):1276–1283. doi:10.1097/CCM.0b013e3181d8cc1d
4. Rahmel T, Schmitz S, Nowak H, et al. Long-term mortality and outcome in hospital survivors of septic shock, sepsis, and severe infections: the importance of aftercare. PLoS One. 2020;15(2):e0228952. doi:10.1371/journal.pone.0228952
5. Wang HE, Szychowski JM, Griffin R, Safford MM, Shapiro NI, Howard G. Long-term mortality after community-acquired sepsis: a longitudinal population-based cohort study. BMJ Open. 2014;4(1):e004283. doi:10.1136/bmjopen-2013-004283
6. Iwashyna TJ, Cooke CR, Wunsch H, Kahn JM. Population burden of long-term survivorship after severe sepsis in older Americans. J Am Geriatr Soc. 2012;60(6):1070–1077. doi:10.1111/j.1532-5415.2012.03989.x
7. Fleischmann-Struzek C, Rose N, Freytag A, et al. Epidemiology and Costs of Postsepsis Morbidity, Nursing Care Dependency, and Mortality in Germany, 2013 to 2017. JAMA Netw Open. 2021;4(11):e2134290. doi:10.1001/jamanetworkopen.2021.34290
8. Prescott HC, Angus DC. Enhancing Recovery From Sepsis: a Review. JAMA. 2018;319(1):62–75. doi:10.1001/jama.2017.17687
9. DeMerle KM, Royer SC, Mikkelsen ME, Prescott HC. Readmissions for Recurrent Sepsis: new or Relapsed Infection? Crit Care Med. 2017;45(10):1702–1708. doi:10.1097/CCM.0000000000002626
10. Dahlberg J, Linder A, Mellhammar L. Use of healthcare before and after sepsis in Sweden: a case-control study. BMJ Open. 2023;13(2):e065967. doi:10.1136/bmjopen-2022-065967
11. Prescott HC, Langa KM, Iwashyna TJ. Readmission diagnoses after hospitalization for severe sepsis and other acute medical conditions. JAMA. 2015;313(10):1055–1057. doi:10.1001/jama.2015.1410
12. Ou SM, Chu H, Chao PW, et al. Long-Term Mortality and Major Adverse Cardiovascular Events in Sepsis Survivors. A Nationwide Population-based Study. Am J Respir Crit Care Med. 2016;194(2):209–217. doi:10.1164/rccm.201510-2023OC
13. Linder A, Guh D, Boyd JH, Walley KR, Anis AH, Russell JA. Long-term (10-year) mortality of younger previously healthy patients with severe sepsis/septic shock is worse than that of patients with nonseptic critical illness and of the general population. Crit Care Med. 2014;42(10):2211–2218. doi:10.1097/CCM.0000000000000503
14. Cuthbertson BH, Elders A, Hall S, et al. Mortality and quality of life in the five years after severe sepsis. Crit Care. 2013;17(2):R70. doi:10.1186/cc12616
15. Chang DW, Tseng CH, Shapiro MF. Rehospitalizations Following Sepsis: common and Costly. Crit Care Med. 2015;43(10):2085–2093. doi:10.1097/CCM.0000000000001159
16. Guirgis FW, Brakenridge S, Sutchu S, et al. The long-term burden of severe sepsis and septic shock: sepsis recidivism and organ dysfunction. J Trauma Acute Care Surg. 2016;81(3):525–532. doi:10.1097/TA.0000000000001135
17. Linder A, Fjell C, Levin A, Walley KR, Russell JA, Boyd JH. Small acute increases in serum creatinine are associated with decreased long-term survival in the critically ill. Am J Respir Crit Care Med. 2014;189(9):1075–1081. doi:10.1164/rccm.201311-2097OC
18. Yende S, Linde-Zwirble W, Mayr F, Weissfeld LA, Reis S, Angus DC. Risk of cardiovascular events in survivors of severe sepsis. Am J Respir Crit Care Med. 2014;189(9):1065–1074. doi:10.1164/rccm.201307-1321OC
19. Bergh C, Fall K, Udumyan R, Sjoqvist H, Frobert O, Montgomery S. Severe infections and subsequent delayed cardiovascular disease. Eur J Prev Cardiol. 2017;24(18):1958–1966. doi:10.1177/2047487317724009
20. Jentzer JC, Lawler PR, Van Houten HK, Yao X, Kashani KB, Dunlay SM. Cardiovascular Events Among Survivors of Sepsis Hospitalization: a Retrospective Cohort Analysis. J Am Heart Assoc. 2023;12(3):e027813. doi:10.1161/JAHA.122.027813
21. Musher DM, Abers MS, Corrales-Medina VF. Acute Infection and Myocardial Infarction. N Engl J Med. 2019;380(2):171–176. doi:10.1056/NEJMra1808137
22. Koster-Brouwer ME, van de Groep K, Pasma W, et al. Chronic healthcare expenditure in survivors of sepsis in the intensive care unit. Intensive Care Med. 2016;42(10):1641–1642. doi:10.1007/s00134-016-4442-0
23. Iwashyna TJ, Ely EW, Smith DM, Langa KM. Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA. 2010;304(16):1787–1794. doi:10.1001/jama.2010.1553
24. Huang CY, Daniels R, Lembo A, et al. Life after sepsis: an international survey of survivors to understand the post-sepsis syndrome. Int J Qual Health Care. 2019;31(3):191–198. doi:10.1093/intqhc/mzy137
25. Norman BC, Jackson JC, Graves JA, et al. Employment Outcomes After Critical Illness: an Analysis of the Bringing to Light the Risk Factors and Incidence of Neuropsychological Dysfunction in ICU Survivors Cohort. Crit Care Med. 2016;44(11):2003–2009. doi:10.1097/CCM.0000000000001849
26. van der Slikke EC, An AY, Hancock REW, Bouma HR. Exploring the pathophysiology of post-sepsis syndrome to identify therapeutic opportunities. EBioMedicine. 2020;61:103044. doi:10.1016/j.ebiom.2020.103044
27. Mira JC, Gentile LF, Mathias BJ, et al. Sepsis Pathophysiology, Chronic Critical Illness, and Persistent Inflammation-Immunosuppression and Catabolism Syndrome. Crit Care Med. 2017;45(2):253–262. doi:10.1097/CCM.0000000000002074
28. Nagar H, Piao S, Kim CS. Role of Mitochondrial Oxidative Stress in Sepsis. Acute Crit Care. 2018;33(2):65–72. doi:10.4266/acc.2018.00157
29. Brealey D, Brand M, Hargreaves I, et al. Association between mitochondrial dysfunction and severity and outcome of septic shock. Lancet. 2002;360(9328):219–223. doi:10.1016/S0140-6736(02)09459-X
30. Rocheteau P, Chatre L, Briand D, et al. Sepsis induces long-term metabolic and mitochondrial muscle stem cell dysfunction amenable by mesenchymal stem cell therapy. Nat Commun. 2015;6(1):10145. doi:10.1038/ncomms10145
31. Inoue S, Nakanishi N, Sugiyama J, et al. Prevalence and Long-Term Prognosis of Post-Intensive Care Syndrome after Sepsis: a Single-Center Prospective Observational Study. J Clin Med. 2022;11(18):5257. doi:10.3390/jcm11185257
32. Nakanishi N, Liu K, Kawakami D, et al. Post-Intensive Care Syndrome and Its New Challenges in Coronavirus Disease 2019 (COVID-19) Pandemic: a Review of Recent Advances and Perspectives. J Clin Med. 2021;10(17):3870. doi:10.3390/jcm10173870
33. Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. 2023;21(3):133–146. doi:10.1038/s41579-022-00846-2
34. Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345(19):1368–1377. doi:10.1056/NEJMoa010307
35. Cecconi M, Evans L, Levy M, Rhodes A. Sepsis and septic shock. Lancet. 2018;392(10141):75–87. doi:10.1016/S0140-6736(18)30696-2
36. De Blasi RA. Severe sepsis and septic shock. N Engl J Med. 2013;369(21):2062–2063.
37. Preiser JC, van Zanten AR, Berger MM, et al. Metabolic and nutritional support of critically ill patients: consensus and controversies. Crit Care. 2015;19(1):35. doi:10.1186/s13054-015-0737-8
38. De Waele E, Malbrain M, Spapen H. Nutrition in Sepsis: a Bench-to-Bedside Review. Nutrients. 2020;12(2):395. doi:10.3390/nu12020395
39. Marik PE, Hooper MH. Normocaloric versus hypocaloric feeding on the outcomes of ICU patients: a systematic review and meta-analysis. Intensive Care Med. 2016;42(3):316–323. doi:10.1007/s00134-015-4131-4
40. van der Slikke EC, Star BS, van Meurs M, Henning RH, Moser J, Bouma HR. Sepsis is associated with mitochondrial DNA damage and a reduced mitochondrial mass in the kidney of patients with sepsis-AKI. Crit Care. 2021;25(1):36. doi:10.1186/s13054-020-03424-1
41. Singer M. The role of mitochondrial dysfunction in sepsis-induced multi-organ failure. Virulence. 2014;5(1):66–72. doi:10.4161/viru.26907
42. van der Slikke EC, Star BS, Quinten VM, et al. Association between oxidized nucleobases and mitochondrial DNA damage with long-term mortality in patients with sepsis. Free Radic Biol Med. 2022;179:156–163. doi:10.1016/j.freeradbiomed.2021.12.305
43. Parikh SM. Therapeutic targeting of the mitochondrial dysfunction in septic acute kidney injury. Curr Opin Crit Care. 2013;19(6):554–559. doi:10.1097/MCC.0000000000000038
44. Haden DW, Suliman HB, Carraway MS, et al. Mitochondrial biogenesis restores oxidative metabolism during Staphylococcus aureus sepsis. Am J Respir Crit Care Med. 2007;176(8):768–777. doi:10.1164/rccm.200701-161OC
45. Lowes DA, Thottakam BM, Webster NR, Murphy MP, Galley HF. The mitochondria-targeted antioxidant MitoQ protects against organ damage in a lipopolysaccharide-peptidoglycan model of sepsis. Free Radic Biol Med. 2008;45(11):1559–1565. doi:10.1016/j.freeradbiomed.2008.09.003
46. Zhu Y, Kuang L, Wu Y, et al. Protective Effects of Inhibition of Mitochondrial Fission on Organ Function After Sepsis. Front Pharmacol. 2021;12:712489. doi:10.3389/fphar.2021.712489
47. Deng S, Ai Y, Gong H, et al. Mitochondrial dynamics and protective effects of a mitochondrial division inhibitor, Mdivi-1, in lipopolysaccharide-induced brain damage. Biochem Biophys Res Commun. 2018;496(3):865–871. doi:10.1016/j.bbrc.2018.01.136
48. Gonzalez AS, Elguero ME, Finocchietto P, et al. Abnormal mitochondrial fusion-fission balance contributes to the progression of experimental sepsis. Free Radic Res. 2014;48(7):769–783. doi:10.3109/10715762.2014.906592
49. Venet F, Monneret G. Advances in the understanding and treatment of sepsis-induced immunosuppression. Nat Rev Nephrol. 2018;14(2):121–137. doi:10.1038/nrneph.2017.165
50. Arens C, Bajwa SA, Koch C, et al. Sepsis-induced long-term immune paralysis--results of a descriptive, explorative study. Crit Care. 2016;20:93. doi:10.1186/s13054-016-1233-5
51. Boomer JS, To K, Chang KC, et al. Immunosuppression in patients who die of sepsis and multiple organ failure. JAMA. 2011;306(23):2594–2605. doi:10.1001/jama.2011.1829
52. Delano MJ, Moldawer LL. Magic bullets and surrogate biomarkers circa 2009. Crit Care Med. 2009;37(5):1796–1798. doi:10.1097/CCM.0b013e3181a09440
53. Davies R, O’Dea K, Gordon A. Immune therapy in sepsis: are we ready to try again? J Intensive Care Soc. 2018;19(4):326–344. doi:10.1177/1751143718765407
54. Sjoberg M, Eriksson M. Hand disinfectant practice: the impact of an education intervention. Open Nurs J. 2010;4:20–24. doi:10.2174/1874434601004010020
55. Schlapbach LJ, Kissoon N, Alhawsawi A, et al. World Sepsis Day: a global agenda to target a leading cause of morbidity and mortality. Am J Physiol Lung Cell Mol Physiol. 2020;319(3):L518–L522. doi:10.1152/ajplung.00369.2020
56. Zheng C, Shao W, Chen X, Zhang B, Wang G, Zhang W. Real-world effectiveness of COVID-19 vaccines: a literature review and meta-analysis. Int J Infect Dis. 2022;114:252–260. doi:10.1016/j.ijid.2021.11.009
57. Riley C, Wheeler DS. Prevention of sepsis in children: a new paradigm for public policy. Crit Care Res Pract. 2012;2012:437139. doi:10.1155/2012/437139
58. Parsons Leigh J, Brundin-Mather R, Moss SJ, et al. Public awareness and knowledge of sepsis: a cross-sectional survey of adults in Canada. Crit Care. 2022;26(1):337. doi:10.1186/s13054-022-04215-6
59. Rubulotta FM, Ramsay G, Parker MM, et al. An international survey: public awareness and perception of sepsis. Crit Care Med. 2009;37(1):167–170. doi:10.1097/CCM.0b013e3181926883
60. Sepsisfondsen. Sweden: sepsisfondens Insamlingsstiftelse. Available from: www.sepsisfonden.se.
61. Vincent JL. Increasing awareness of sepsis: world Sepsis Day. Crit Care. 2012;16(5):152. doi:10.1186/cc11511
62. Towns ML, Jarvis WR, Hsueh PR. Guidelines on blood cultures. J Microbiol Immunol Infect. 2010;43(4):347–349. doi:10.1016/S1684-1182(10)60054-0
63. Fiest KM, Krewulak KD, Brundin-Mather R, et al. Patient, Public, and Healthcare Professionals’ Sepsis Awareness, Knowledge, and Information Seeking Behaviors: a Scoping Review. Crit Care Med. 2022;50(8):1187–1197. doi:10.1097/CCM.0000000000005564
64. Jabaley CS, Blum JM, Groff RF, O’Reilly-Shah VN. Global trends in the awareness of sepsis: insights from search engine data between 2012 and 2017. Crit Care. 2018;22(1):7. doi:10.1186/s13054-017-1914-8
65. Farsi D, Martinez-Menchaca HR, Ahmed M, Farsi N. Social Media and Health Care (Part II): narrative Review of Social Media Use by Patients. J Med Internet Res. 2022;24(1):e30379. doi:10.2196/30379
66. Naucler P, Huttner A, van Werkhoven CH, et al. Impact of time to antibiotic therapy on clinical outcome in patients with bacterial infections in the emergency department: implications for antimicrobial stewardship. Clin Microbiol Infect. 2021;27(2):175–181. doi:10.1016/j.cmi.2020.02.032
67. Lee CF, Cowling BJ, Feng S, et al. Impact of antibiotic stewardship programmes in Asia: a systematic review and meta-analysis. J Antimicrob Chemother. 2018;73(4):844–851. doi:10.1093/jac/dkx492
68. Baur D, Gladstone BP, Burkert F, et al. Effect of antibiotic stewardship on the incidence of infection and colonisation with antibiotic-resistant bacteria and Clostridium difficile infection: a systematic review and meta-analysis. Lancet Infect Dis. 2017;17(9):990–1001. doi:10.1016/S1473-3099(17)30325-0
69. Schuts EC, Hulscher M, Mouton JW, et al. Current evidence on hospital antimicrobial stewardship objectives: a systematic review and meta-analysis. Lancet Infect Dis. 2016;16(7):847–856. doi:10.1016/S1473-3099(16)00065-7
70. Baggs J, Jernigan JA, Halpin AL, Epstein L, Hatfield KM, McDonald LC. Risk of Subsequent Sepsis Within 90 Days After a Hospital Stay by Type of Antibiotic Exposure. Clin Infect Dis. 2018;66(7):1004–1012. doi:10.1093/cid/cix947
71. Campion M, Scully G. Antibiotic Use in the Intensive Care Unit: optimization and De-Escalation. J Intensive Care Med. 2018;33(12):647–655. doi:10.1177/0885066618762747
72. Shin DH, Kim HS, Heo E, et al. Stepwise Expansion of Antimicrobial Stewardship Programs and Its Impact on Antibiotic Use and Resistance Rates at a Tertiary Care Hospital in Korea. Microbiol Spectr. 2022;10(3):e0033522. doi:10.1128/spectrum.00335-22
73. Fitzpatrick F, Tarrant C, Hamilton V, Kiernan FM, Jenkins D, Krockow EM. Sepsis and antimicrobial stewardship: two sides of the same coin. BMJ Qual Saf. 2019;28(9):758–761. doi:10.1136/bmjqs-2019-009445
74. Stallmach A, Kesselmeier M, Bauer M, et al. Comparison of fatigue, cognitive dysfunction and psychological disorders in post-COVID patients and patients after sepsis: is there a specific constellation? Infection. 2022;50(3):661–669. doi:10.1007/s15010-021-01733-3
75. Apitzsch S, Larsson L, Larsson AK, Linder A. The physical and mental impact of surviving sepsis - A qualitative study of experiences and perceptions among a Swedish sample. Arch Public Health. 2021;79(1):66. doi:10.1186/s13690-021-00585-5
76. Hund E. Neurological complications of sepsis: critical illness polyneuropathy and myopathy. J Neurol. 2001;248(11):929–934. doi:10.1007/s004150170043
77. Axer H, Grimm A, Pausch C, et al. The impairment of small nerve fibers in severe sepsis and septic shock. Crit Care. 2016;20(1):64. doi:10.1186/s13054-016-1241-5
78. Sasegbon A, O’Shea L, Hamdy S. Examining the relationship between sepsis and oropharyngeal dysphagia in hospitalised elderly patients: a retrospective cohort study. Frontline Gastroenterol. 2018;9(4):256–261. doi:10.1136/flgastro-2018-100994
79. Hongo T, Yumoto T, Naito H, et al. Frequency, associated factors, and associated outcomes of dysphagia following sepsis. Aust Crit Care. 2022;36(4):521–527. doi:10.1016/j.aucc.2022.06.003
80. Zuercher P, Moret CS, Dziewas R, Schefold JC. Dysphagia in the intensive care unit: epidemiology, mechanisms, and clinical management. Crit Care. 2019;23(1):103. doi:10.1186/s13054-019-2400-2
81. Goldsmith T. Evaluation and treatment of swallowing disorders following endotracheal intubation and tracheostomy. International Anesthesiology Clinics. 2000;38(3):219–242. doi:10.1097/00004311-200007000-00013
82. Macht M, White SD, Moss M. Swallowing dysfunction after critical illness. Chest. 2014;146(6):1681–1689. doi:10.1378/chest.14-1133
83. Farneti D, Consolmagno P. The Swallowing Centre: rationale for a multidisciplinary management. Acta Otorhinolaryngol Ital. 2007;27(4):200–207.
84. Slutsky AS, Tremblay LN. Multiple system organ failure. Is mechanical ventilation a contributing factor? Am J Respir Crit Care Med. 1998;157(6 Pt 1):1721–1725. doi:10.1164/ajrccm.157.6.9709092
85. Lefer AM. Induction of tissue injury and altered cardiovascular performance by platelet-activating factor: relevance to multiple systems organ failure. Crit Care Clin. 1989;5(2):331–352. doi:10.1016/S0749-0704(18)30440-8
86. Fredriksson K, Hammarqvist F, Strigard K, et al. Derangements in mitochondrial metabolism in intercostal and leg muscle of critically ill patients with sepsis-induced multiple organ failure. Am J Physiol Endocrinol Metab. 2006;291(5):E1044–1050. doi:10.1152/ajpendo.00218.2006
87. Long CL, Schiller WR, Blakemore WS, Geiger JW, O’Dell M, Henderson K. Muscle protein catabolism in the septic patient as measured by 3-methylhistidine excretion. Am J Clin Nutr. 1977;30(8):1349–1352. doi:10.1093/ajcn/30.8.1349
88. Bilmazes C, Kien CL, Rohrbaugh DK, et al. Quantitative contribution by skeletal muscle to elevated rates of whole-body protein breakdown in burned children as measured by N tau-methylhistidine output. Metabolism. 1978;27(6):671–676. doi:10.1016/0026-0495(78)90004-5
89. Moldawer LL, Copeland EM. Proinflammatory cytokines, nutritional support, and the cachexia syndrome: interactions and therapeutic options. Cancer. 1997;79(9):1828–1839. doi:10.1002/(SICI)1097-0142(19970501)79:9<1828::AID-CNCR28>3.0.CO;2-Z
90. Baggerman MR, van Dijk DPJ, Winkens B, et al. Muscle wasting associated co-morbidities, rather than sarcopenia are risk factors for hospital mortality in critical illness. J Crit Care. 2020;56:31–36. doi:10.1016/j.jcrc.2019.11.016
91. Puthucheary ZA, Rawal J, McPhail M, et al. Acute skeletal muscle wasting in critical illness. JAMA. 2013;310(15):1591–1600. doi:10.1001/jama.2013.278481
92. Goossens C, Marques MB, Derde S, et al. Premorbid obesity, but not nutrition, prevents critical illness-induced muscle wasting and weakness. J Cachexia Sarcopenia Muscle. 2017;8(1):89–101. doi:10.1002/jcsm.12131
93. Mankowski RT, Anton SD, Ghita GL, et al. Older Sepsis Survivors Suffer Persistent Disability Burden and Poor Long-Term Survival. J Am Geriatr Soc. 2020;68(9):1962–1969. doi:10.1111/jgs.16435
94. Herridge MS, Azoulay E. Outcomes after Critical Illness. N Engl J Med. 2023;388(10):913–924. doi:10.1056/NEJMra2104669
95. Mankowski RT, Anton SD, Ghita GL, et al. Older Adults Demonstrate Biomarker Evidence of the Persistent Inflammation, Immunosuppression, and Catabolism Syndrome (PICS) After Sepsis. J Gerontol a Biol Sci Med Sci. 2022;77(1):188–196. doi:10.1093/gerona/glab080
96. Mankowski RT, Laitano O, Darden D, et al. Sepsis-Induced Myopathy and Gut Microbiome Dysbiosis: mechanistic Links and Therapeutic Targets. Shock. 2022;57(1):15–23. doi:10.1097/SHK.0000000000001843
97. Dirks ML, Wall BT, van de Valk B, et al. One Week of Bed Rest Leads to Substantial Muscle Atrophy and Induces Whole-Body Insulin Resistance in the Absence of Skeletal Muscle Lipid Accumulation. Diabetes. 2016;65(10):2862–2875. doi:10.2337/db15-1661
98. van Gassel RJJ, Baggerman MR, van de Poll MCG. Metabolic aspects of muscle wasting during critical illness. Curr Opin Clin Nutr Metab Care. 2020;23(2):96–101. doi:10.1097/MCO.0000000000000628
99. Schmitt RE, Dasgupta A, Arneson-Wissink PC, Datta S, Ducharme AM, Doles JD. Muscle stem cells contribute to long-term tissue repletion following surgical sepsis. J Cachexia Sarcopenia Muscle. 2023;14(3):1424–1440. doi:10.1002/jcsm.13214
100. Pahor M, Guralnik JM, Ambrosius WT, et al. Effect of structured physical activity on prevention of major mobility disability in older adults: the LIFE study randomized clinical trial. JAMA. 2014;311(23):2387–2396. doi:10.1001/jama.2014.5616
101. Fuke R, Hifumi T, Kondo Y, et al. Early rehabilitation to prevent postintensive care syndrome in patients with critical illness: a systematic review and meta-analysis. BMJ Open. 2018;8(5):e019998. doi:10.1136/bmjopen-2017-019998
102. Puthucheary Z, Rooyackers O. Anabolic Resistance: an Uncomfortable Truth for Clinical Trials in Preventing Intensive Care-acquired Weakness and Physical Functional Impairment. Am J Respir Crit Care Med. 2022;206(6):660–661. doi:10.1164/rccm.202206-1059ED
103. Klaude M, Mori M, Tjader I, Gustafsson T, Wernerman J, Rooyackers O. Protein metabolism and gene expression in skeletal muscle of critically ill patients with sepsis. Clin Sci (Lond). 2012;122(3):133–142. doi:10.1042/CS20110233
104. Nakanishi N, Oto J, Tsutsumi R, et al. Effect of Electrical Muscle Stimulation on Upper and Lower Limb Muscles in Critically Ill Patients: a Two-Center Randomized Controlled Trial. Crit Care Med. 2020;48(11):e997–e1003. doi:10.1097/CCM.0000000000004522
105. Grunow JJ, Goll M, Carbon NM, Liebl ME, Weber-Carstens S, Wollersheim T. Differential contractile response of critically ill patients to neuromuscular electrical stimulation. Crit Care. 2019;23(1):308. doi:10.1186/s13054-019-2540-4
106. Medrinal C, Combret Y, Prieur G, et al. Comparison of exercise intensity during four early rehabilitation techniques in sedated and ventilated patients in ICU: a randomised cross-over trial. Crit Care. 2018;22(1):110. doi:10.1186/s13054-018-2030-0
107. Connolly B, Salisbury L, O’Neill B, et al. Exercise rehabilitation following intensive care unit discharge for recovery from critical illness: executive summary of a Cochrane Collaboration systematic review. J Cachexia Sarcopenia Muscle. 2016;7(5):520–526. doi:10.1002/jcsm.12146
108. Hermans AJH, Laarhuis BI, Kouw IWK, van Zanten ARH. Current insights in ICU nutrition: tailored nutrition. Curr Opin Crit Care. 2023;29(2):101–107. doi:10.1097/MCC.0000000000001016
109. McKendry J, Thomas ACQ, Phillips SM. Muscle Mass Loss in the Older Critically Ill Population: potential Therapeutic Strategies. Nutr Clin Pract. 2020;35(4):607–616. doi:10.1002/ncp.10540
110. Verceles AC, Serra M, Davis D, et al. Combining exercise, protein supplementation and electric stimulation to mitigate muscle wasting and improve outcomes for survivors of critical illness-The ExPrES study. Heart Lung. 2023;58:229–235. doi:10.1016/j.hrtlng.2022.11.013
111. Nakamura K, Kihata A, Naraba H, et al. beta-Hydroxy-beta-methylbutyrate, Arginine, and Glutamine Complex on Muscle Volume Loss in Critically Ill Patients: a Randomized Control Trial. JPEN J Parenter Enteral Nutr. 2020;44(2):205–212. doi:10.1002/jpen.1607
112. Berney S, Hopkins RO, Rose JW, et al. Functional electrical stimulation in-bed cycle ergometry in mechanically ventilated patients: a multicentre randomised controlled trial. Thorax. 2021;76(7):656–663. doi:10.1136/thoraxjnl-2020-215093
113. Barraud D, Blard C, Hein F, et al. Probiotics in the critically ill patient: a double blind, randomized, placebo-controlled trial. Intensive Care Med. 2010;36(9):1540–1547. doi:10.1007/s00134-010-1927-0
114. Shimizu K, Yamada T, Ogura H, et al. Synbiotics modulate gut microbiota and reduce enteritis and ventilator-associated pneumonia in patients with sepsis: a randomized controlled trial. Crit Care. 2018;22(1):239. doi:10.1186/s13054-018-2167-x
115. Suez J, Zmora N, Segal E, Elinav E. The pros, cons, and many unknowns of probiotics. Nat Med. 2019;25(5):716–729. doi:10.1038/s41591-019-0439-x
116. van Zanten ARH, De Waele E, Wischmeyer PE. Nutrition therapy and critical illness: practical guidance for the ICU, post-ICU, and long-term convalescence phases. Crit Care. 2019;23(1):368. doi:10.1186/s13054-019-2657-5
117. Batt J, Herridge MS, Dos Santos CC. From skeletal muscle weakness to functional outcomes following critical illness: a translational biology perspective. Thorax. 2019;74(11):1091–1098. doi:10.1136/thoraxjnl-2016-208312
118. Walker AMN, Drozd M, Hall M, et al. Prevalence and Predictors of Sepsis Death in Patients With Chronic Heart Failure and Reduced Left Ventricular Ejection Fraction. J Am Heart Assoc. 2018;7(20):e009684. doi:10.1161/JAHA.118.009684
119. Beesley SJ, Weber G, Sarge T, et al. Septic Cardiomyopathy. Crit Care Med. 2018;46(4):625–634. doi:10.1097/CCM.0000000000002851
120. Bell CM, Brener SS, Gunraj N, et al. Association of ICU or hospital admission with unintentional discontinuation of medications for chronic diseases. JAMA. 2011;306(8):840–847. doi:10.1001/jama.2011.1206
121. Kosyakovsky LB, Angriman F, Katz E, et al. Association between sepsis survivorship and long-term cardiovascular outcomes in adults: a systematic review and meta-analysis. Intensive Care Med. 2021;47(9):931–942. doi:10.1007/s00134-021-06479-y
122. Angriman F, Rosella LC, Lawler PR, Ko DT, Wunsch H, Scales DC. Sepsis hospitalization and risk of subsequent cardiovascular events in adults: a population-based matched cohort study. Intensive Care Med. 2022;48(4):448–457. doi:10.1007/s00134-022-06634-z
123. Walkey AJ, Wiener RS, Ghobrial JM, Curtis LH, Benjamin EJ. Incident stroke and mortality associated with new-onset atrial fibrillation in patients hospitalized with severe sepsis. JAMA. 2011;306(20):2248–2254. doi:10.1001/jama.2011.1615
124. Induruwa I, Hennebry E, Hennebry J, Thakur M, Warburton EA, Khadjooi K. Sepsis-driven atrial fibrillation and ischaemic stroke. Is there enough evidence to recommend anticoagulation? Eur J Intern Med. 2022;98:32–36. doi:10.1016/j.ejim.2021.10.022
125. Arero AG, Vasheghani-Farahani A, Tigabu BM, Arero G, Ayene BY, Soltani D. Long-term risk and predictors of cerebrovascular events following sepsis hospitalization: a systematic review and meta-analysis. Front Med. 2022;9:1065476. doi:10.3389/fmed.2022.1065476
126. Hernandez AF, Greiner MA, Fonarow GC, et al. Relationship between early physician follow-up and 30-day readmission among Medicare beneficiaries hospitalized for heart failure. JAMA. 2010;303(17):1716–1722. doi:10.1001/jama.2010.533
127. Shen E, Koyama SY, Huynh DN, et al. Association of a Dedicated Post-Hospital Discharge Follow-up Visit and 30-Day Readmission Risk in a Medicare Advantage Population. JAMA Intern Med. 2017;177(1):132–135. doi:10.1001/jamainternmed.2016.7061
128. European Society of Cardiology. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Available from: https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines/Acute-and-Chronic-Heart-Failure.
129. Born S, Matthaus-Kramer C, Bichmann A, et al. Sepsis survivors and caregivers perspectives on post-acute rehabilitation and aftercare in the first year after sepsis in Germany. Front Med. 2023;10:1137027. doi:10.3389/fmed.2023.1137027
130. Bruck E, Schandl A, Bottai M, Sackey P. The impact of sepsis, delirium, and psychological distress on self-rated cognitive function in ICU survivors-A prospective cohort study. J Intensive Care. 2018;6:2. doi:10.1186/s40560-017-0272-6
131. Ferreira RC, Mello RR, Silva KS. Neonatal sepsis as a risk factor for neurodevelopmental changes in preterm infants with very low birth weight. J Pediatr (Rio J). 2014;90(3):293–299. doi:10.1016/j.jped.2013.09.006
132. Feng MF, Henney CS. Studies on NK cell-target interactions. Shi Yan Sheng Wu Xue Bao. 1987;20(2):145–154.
133. Li Y, Ji M, Yang J. Current Understanding of Long-Term Cognitive Impairment After Sepsis. Front Immunol. 2022;13:855006. doi:10.3389/fimmu.2022.855006
134. Marra A, Pandharipande PP, Girard TD, et al. Co-Occurrence of Post-Intensive Care Syndrome Problems Among 406 Survivors of Critical Illness. Crit Care Med. 2018;46(9):1393–1401. doi:10.1097/CCM.0000000000003218
135. Beumeler BC, Hoogstins-Vlagsma TT, Zutphen T, et al. The prevalence of mental frailty in ICU survivors and informal caregiver strain: a 1-year retrospective study of the Frisian aftercare cohort. Sage J. 2021. doi:10.1177/17511437221139547
136. Calsavara AJ, Costa PA, Nobre V, Teixeira AL. Prevalence and risk factors for post-traumatic stress, anxiety, and depression in sepsis survivors after ICU discharge. Braz J Psychiatry. 2021;43(3):269–276. doi:10.1590/1516-4446-2020-0986
137. Haas LEM, Boumendil A, Flaatten H, et al. Frailty is associated with long-term outcome in patients with sepsis who are over 80 years old: results from an observational study in 241 European ICUs. Age Ageing. 2021;50(5):1719–1727. doi:10.1093/ageing/afab036
138. Wintermann GB, Brunkhorst FM, Petrowski K, et al. Stress disorders following prolonged critical illness in survivors of severe sepsis. Crit Care Med. 2015;43(6):1213–1222. doi:10.1097/CCM.0000000000000936
139. Bienvenu OJ, Gellar J, Althouse BM, et al. Post-traumatic stress disorder symptoms after acute lung injury: a 2-year prospective longitudinal study. Psychol Med. 2013;43(12):2657–2671. doi:10.1017/S0033291713000214
140. Nesseler N, Defontaine A, Launey Y, Morcet J, Malledant Y, Seguin P. Long-term mortality and quality of life after septic shock: a follow-up observational study. Intensive Care Med. 2013;39(5):881–888. doi:10.1007/s00134-013-2815-1
141. Nannan Panday RS, Minderhoud TC, Chantalou DS, Alam N, Nanayakkara PWB. Health related quality of life in sepsis survivors from the Prehospital Antibiotics Against Sepsis (PHANTASi) trial. PLoS One. 2019;14(10):e0222450. doi:10.1371/journal.pone.0222450
142. Hofhuis JG, Spronk PE, van Stel HF, Schrijvers AJ, Rommes JH, Bakker J. The impact of severe sepsis on health-related quality of life: a long-term follow-up study. Anesth Analg. 2008;107(6):1957–1964. doi:10.1213/ane.0b013e318187bbd8
143. Heyland DK, Hopman W, Coo H, Tranmer J, McColl MA. Long-term health-related quality of life in survivors of sepsis. Short Form 36: a valid and reliable measure of health-related quality of life. Crit Care Med. 2000;28(11):3599–3605. doi:10.1097/00003246-200011000-00006
144. Jaenichen D, Brunkhorst FM, Strauss B, Rosendahl J. Physical and mental long-term sequelae following intensive care of severe sepsis in patients and relatives. Psychother Psychosom Med Psychol. 2012;62(9–10):335–343. doi:10.1055/s-0032-1306354
145. Odden AJ, Rohde JM, Bonham C, et al. Functional outcomes of general medical patients with severe sepsis. BMC Infect Dis. 2013;13(1):588. doi:10.1186/1471-2334-13-588
146. Kohn R, Rubenfeld GD, Levy MM, Ubel PA, Halpern SD. Rule of rescue or the good of the many? An analysis of physicians’ and nurses’ preferences for allocating ICU beds. Intensive Care Med. 2011;37(7):1210–1217. doi:10.1007/s00134-011-2257-6
147. Haines KJ, McPeake J, Hibbert E, et al. Enablers and Barriers to Implementing ICU Follow-Up Clinics and Peer Support Groups Following Critical Illness: the Thrive Collaboratives. Crit Care Med. 2019;47(9):1194–1200. doi:10.1097/CCM.0000000000003818
148. Schmidt KF, Schwarzkopf D, Baldwin LM, et al. Long-Term Courses of Sepsis Survivors: effects of a Primary Care Management Intervention. Am J Med. 2020;133(3):381–385 e385. doi:10.1016/j.amjmed.2019.08.033
149. Schmidt K, Worrack S, Von Korff M, et al. Effect of a Primary Care Management Intervention on Mental Health-Related Quality of Life Among Survivors of Sepsis: a Randomized Clinical Trial. JAMA. 2016;315(24):2703–2711. doi:10.1001/jama.2016.7207
150. Rosendahl J, Brunkhorst FM, Jaenichen D, Strauss B. Physical and mental health in patients and spouses after intensive care of severe sepsis: a dyadic perspective on long-term sequelae testing the Actor-Partner Interdependence Model. Crit Care Med. 2013;41(1):69–75. doi:10.1097/CCM.0b013e31826766b0
151. Geense WW, van den Boogaard M, van der Hoeven JG, Vermeulen H, Hannink G, Zegers M. Nonpharmacologic Interventions to Prevent or Mitigate Adverse Long-Term Outcomes Among ICU Survivors: a Systematic Review and Meta-Analysis. Crit Care Med. 2019;47(11):1607–1618. doi:10.1097/CCM.0000000000003974
152. Peris A, Bonizzoli M, Iozzelli D, et al. Early intra-intensive care unit psychological intervention promotes recovery from post traumatic stress disorders, anxiety and depression symptoms in critically ill patients. Crit Care. 2011;15(1):R41. doi:10.1186/cc10003
153. Cherak SJ, Rosgen BK, Amarbayan M, et al. Mental Health Interventions to Improve Psychological Outcomes in Informal Caregivers of Critically Ill Patients: a Systematic Review and Meta-Analysis. Crit Care Med. 2021;49(9):1414–1426. doi:10.1097/CCM.0000000000005011
154. Gumus AB, Cam O. Effects of emotional support-focused nursing interventions on the psychosocial adjustment of breast cancer patients. Asian Pac J Cancer Prev. 2008;9(4):691–697.
155. Majasaari H, Sarajarvi A, Koskinen H, Autere S, Paavilainen E. Patients’ perceptions of emotional support and information provided to family members. AORN J. 2005;81(5):1030–1039. doi:10.1016/S0001-2092(06)60469-9
156. Oppikofer S, Albrecht K, Martin M. Effect of increased social support on the well-being of cognitively impaired elderly people. Z Gerontol Geriatr. 2010;43(5):310–316. doi:10.1007/s00391-009-0066-0
157. Biagianti B, Foti G, Di Liberto A, Bressi C, Brambilla P. CBT-informed psychological interventions for adult patients with anxiety and depression symptoms: a narrative review of digital treatment options. J Affect Disord. 2023;325:682–694. doi:10.1016/j.jad.2023.01.057
158. Jonassaint CR, Kang C, Prussien KV, et al. Feasibility of implementing mobile technology-delivered mental health treatment in routine adult sickle cell disease care. Transl Behav Med. 2020;10(1):58–67. doi:10.1093/tbm/iby107
159. Mikkelsen ME, Jackson JC, Hopkins RO, et al. Peer Support as a Novel Strategy to Mitigate Post-Intensive Care Syndrome. AACN Adv Crit Care. 2016;27(2):221–229. doi:10.4037/aacnacc2016667
160. Raman S, English A, O’Keefe M, et al. Designing Support Structures Post Sepsis in Children: perspectives of the Queensland Paediatric Sepsis Program. Front Pediatr. 2021;9:759234. doi:10.3389/fped.2021.759234
161. Zhang K, Mao X, Fang Q, et al. Impaired long-term quality of life in survivors of severe sepsis: Chinese multicenter study over 6 years. Anaesthesist. 2013;62(12):995–1002. doi:10.1007/s00101-013-2257-8
162. Liu V, Lei X, Prescott HC, Kipnis P, Iwashyna TJ, Escobar GJ. Hospital readmission and healthcare utilization following sepsis in community settings. J Hosp Med. 2014;9(8):502–507. doi:10.1002/jhm.2197
163. Prescott HC, Costa DK. Improving Long-Term Outcomes After Sepsis. Crit Care Clin. 2018;34(1):175–188. doi:10.1016/j.ccc.2017.08.013
164. Seymour CW, Kennedy JN, Wang S, et al. Derivation, Validation, and Potential Treatment Implications of Novel Clinical Phenotypes for Sepsis. JAMA. 2019;321(20):2003–2017. doi:10.1001/jama.2019.5791
165. Scicluna BP, van Vught LA, Zwinderman AH, et al. Classification of patients with sepsis according to blood genomic endotype: a prospective cohort study. Lancet Respir Med. 2017;5(10):816–826. doi:10.1016/S2213-2600(17)30294-1
166. Davenport EE, Burnham KL, Radhakrishnan J, et al. Genomic landscape of the individual host response and outcomes in sepsis: a prospective cohort study. Lancet Respir Med. 2016;4(4):259–271. doi:10.1016/S2213-2600(16)00046-1
167. Waalders ZE, Smits V, et al. A nationwide survey to explore sepsis awareness among the Dutch general public and former patients. Nederlandse Vereniging voor Intensive Care. 2023.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.