Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Understanding Patients’ Experiences with Borderline Personality Disorder: Qualitative Interviews
Authors DiBenedetti D ![]() , Kosa K, Waters HC
, Kosa K, Waters HC ![]() , Oberdhan D
, Oberdhan D ![]()
Received 2 June 2023
Accepted for publication 9 September 2023
Published 9 October 2023 Volume 2023:19 Pages 2115—2125
DOI https://doi.org/10.2147/NDT.S423882
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Dana DiBenedetti,1 Katherine Kosa,1 Heidi C Waters,2 Dorothee Oberdhan2
1Patient-Centered Outcomes Assessment, RTI Health Solutions, Research Triangle Park, NC, USA; 2Global Value & Real-World Evidence, Otsuka Pharmaceutical Development & Commercialization, Inc, Rockville, MD, USA
Correspondence: Dorothee Oberdhan, Otsuka Pharmaceutical Development & Commercialization, Inc, Rockville, MD, 20850, USA, Email [email protected]
Background: Patient perspectives of living with borderline personality disorder (BPD) are not traditionally captured in the literature. To overcome this gap, we explored participants’ experiences with BPD to gain a better understanding of symptoms and impacts related to the condition.
Methods: Two experienced researchers conducted semistructured interviews with a subset of participants from a randomized controlled trial evaluating a BPD treatment. The interview study was independent from the trial. Interviews focused on participants’ experiences with BPD prior to the trial, including the symptoms and impacts of BPD. Interview transcripts were analyzed to identify dominant trends and generate patterns in the way participants described their experiences with BPD.
Results: A total of 50 adults with BPD participated in the interview study. The mean age of the participants was 28.5 years (range, 18– 53 years) and 72.0% were female. All participants described having difficulties with extreme emotional responses and interpersonal relationships, and most participants reported experiencing issues with self-image, impulsivity, suspiciousness/distrust, feelings of emptiness, and anger. The symptoms that were most bothersome to participants were extreme moods or emotional responses and a pattern of unstable personal relationships. All participants remarked that their BPD-related symptoms negatively impacted their interpersonal relationships, and nearly two-thirds of the sample reported that the impact of BPD on their relationships was the most bothersome. Additionally, more than half of the participants discussed impacts on work or school, memory or thinking, self-care, and financial and legal issues.
Conclusion: Participants reported that the most bothersome symptoms of BPD were those related to extreme moods or emotional responses and interpersonal relationships. Participants similarly described the impact of BPD on their interpersonal relationships as the most bothersome. Overall, participant perspectives from this study indicate that the burden of BPD is significant and new treatments tailored to patients’ real-world needs are warranted.
Keywords: borderline personality disorder, patient experience, symptoms, impacts, patient perception
Introduction
Borderline personality disorder (BPD) is characterized by a pattern of instability in relationships, affect, self-image, and impulsivity.1 The prevalence of BPD is approximately 1% of the general population and ranges from 12% to 22% of the population in psychiatric care settings.2 Individuals with BPD face functional impairments and emotional dysregulation that can lead to difficulties with judgement, relationships, and employment, as well as legal entanglements.3–5 Additionally, the intense, volatile emotions and impulsive behaviors experienced by individuals with BPD can lead to self-harm and recurrent suicide threats or behavior.1
Treatment for BPD consists primarily of psychotherapy, with pharmacotherapy available as an adjunctive treatment component.3 Psychotherapy may be beneficial for several outcomes, such as suicidal and self-harming behaviors, but its effectiveness varies across individuals.3 While outcomes of treatments for BPD are described in the literature, patients’ perceptions of their condition and its impacts on their daily lives are not traditionally captured. Notably, in a study exploring patients’ perspectives of BPD treatment and recovery, patients expressed that current treatment approaches focused too narrowly on specific areas of functioning and that some of their personal recovery goals were not well-addressed.6
By exploring data on patients’ subjective experiences with BPD, clinicians may be able to better empathize with their patients, leading to improvements in the treatment of BPD.7 To date, many qualitative interview studies in individuals with BPD have focused on understanding specific aspects of the disorder, such as chronic feelings of emptiness;8 relationships to self and others;9 perceptions of suffering;10 self-image;11 and self-injury and overdosing.12 However, there are few comprehensive qualitative studies in the current literature focusing on patients’ perspectives of BPD. Furthermore, these studies typically have small sample sizes,13–15 limiting their generalizability to a broader patient population. A better understanding of the patient perspectives of BPD symptoms, impacts, and treatment outcomes is needed; such perspectives may support the development of effective treatments that are tailored to patients’ real-world needs.16 Accordingly, the present study explored participants’ experiences with BPD to gain a better understanding of symptoms and impacts related to the condition.
Methods
Study Design
In this qualitative, observational study, semistructured interviews were conducted with participants selected from a randomized controlled trial evaluating a treatment for BPD (ClinicalTrials.gov: NCT04100096).17 The interview study focused on participants’ experiences with BPD prior to the trial; it was not part of NCT04100096 and no medical treatments were administered. To avoid selection bias, all English-speaking adults selected from 12 clinical sites in the United States participating in NCT04100096 were invited to be interviewed without regard to trial completion status or treatment assignment. To be eligible for inclusion, participants must have fulfilled the following criteria: (1) participated in NCT04100096; (2) been able to speak, read, and comprehend English with at least moderate to good conversational proficiency; and (3) been willing to provide written consent for audio recording and participation in a telephone interview. Clinical sites informed potential participants about the interview study and obtained written, informed consent from interested participants; consent was also confirmed verbally before proceeding with the interview. The study was approved by Advarra, a central institutional review board.
Semistructured Interviews
Interviews were conducted by 2 experienced qualitative researchers, including a clinical psychologist, using a semistructured interview guide. Interviews were approximately 60 minutes in duration, conducted over the phone, and audio recorded. The interview guide provided structure by maintaining a conversational flow with interviewees while ensuring data on participants’ experiences with BPD were collected in a systematic way to meet the study objectives. The interviews began with open-ended questions about the participants’ general experiences with BPD before transitioning to more-targeted, open-ended questions. These more-targeted questions were designed to gather information about the symptoms and impacts of BPD experienced by participants before their entry into the clinical trial, as well as the symptoms and impacts that were most bothersome to participants and the reason that these aspects of BPD bothered participants the most.
Analysis
Interview transcripts were analyzed using an iterative process to incorporate emerging themes as new concepts were identified.18 Specifically, dominant trends in each interview were identified and compared across interviews to describe the themes and the relative importance of concepts mentioned by participants. This process was used to generate patterns in the way participants described their experiences with BPD. Microsoft Excel and ATLAS.ti 7.5 software were used for analysis of the interview data, and participant characteristics were summarized with descriptive statistics. Anonymized participant quotes were used to illustrate the interview results and key concepts.
Results
Demographic and Clinical Characteristics
A total of 50 adults with BPD participated in the study (Table 1). The mean age of the participants was 28.5 years (range, 18–53 years), and the majority of the interview sample was female (n = 36; 72.0%). Prior to participating in NCT04100096, many participants (n = 36; 72.0%) had received medication (eg, antidepressants; antipsychotics and other mood stabilizers; anxiolytics; stimulants) to manage 1 or more of their BPD-related symptoms. However, 15 participants (41.7%) said their previous medication did not help with their BPD-related symptoms or they did not notice much difference from the medication. Conversely, 5 participants reported that their previous medication helped with some of their BPD-related symptoms, and 13 participants reported they helped either with 1 symptom but no other symptom(s) or came with side effects.
 |
Table 1 Interview Participant Characteristics |
Symptoms Related to Borderline Personality Disorder
The frequency of symptoms related to BPD and representative quotes of participants’ experiences with these symptoms are presented in Figure 1A and Table 2, respectively. All 50 participants (100%) reported experiencing extreme moods or emotional responses (eg, quickly changing emotions, intense anger, anxiety, irritability). Additionally, all participants (100%) reported that they had intense or unstable relationships, such as frequent arguments or repeated breakups, significant fears of abandonment or being left alone, or being very close to someone and then being very disappointed in them.
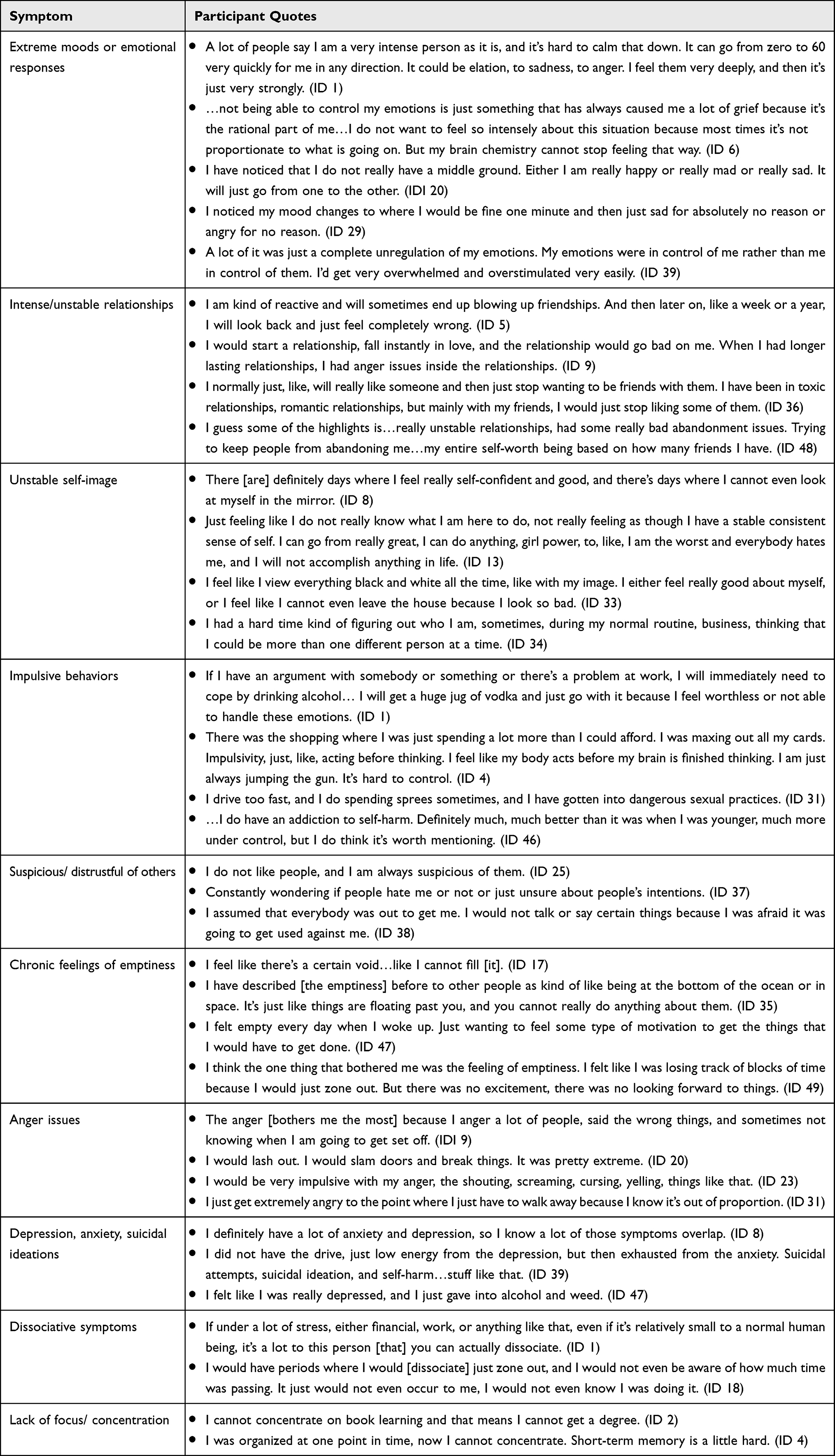 |
Table 2 Participant Quotes Describing Symptoms Related to Borderline Personality Disorder |
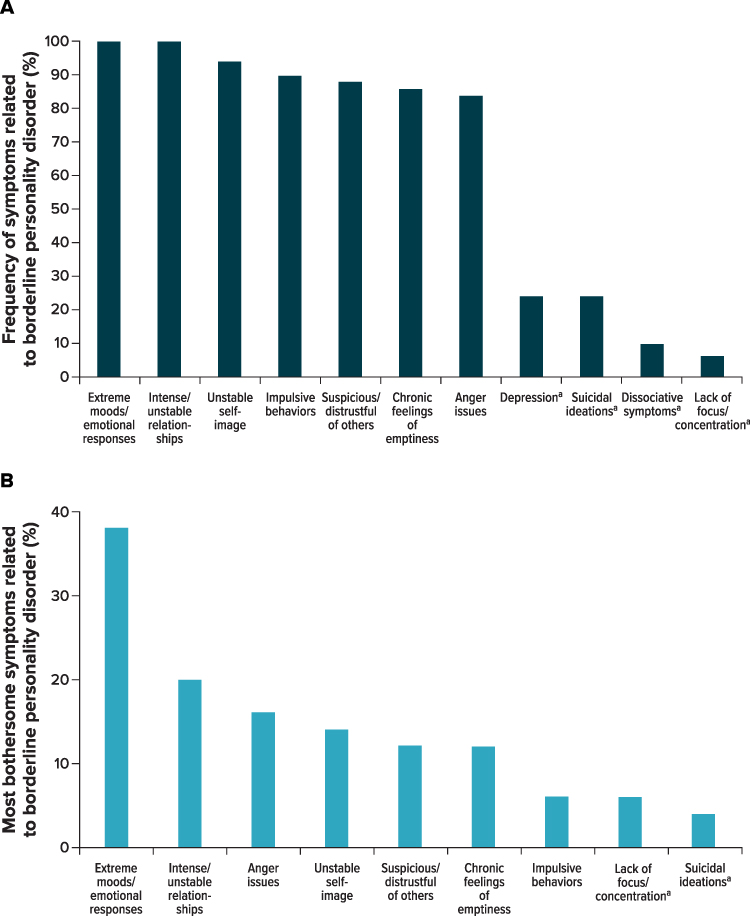 |
Figure 1 Symptoms Related to Borderline Personality Disorder. Notes: Frequency of symptoms (A) and most bothersome symptoms (B) of BPD reported by participants (N = 50). A few participants (n = 8) chose more than 1 most bothersome symptom. aSpontaneously reported by participants; not specifically probed. |
Participants also reported experiencing a number of other BPD-related symptoms. Nearly all participants (n = 47; 94.0%) reported that they had an unstable self-image (eg, sudden and dramatic shifts in self-image) and had engaged in impulsive behaviors that were potentially dangerous or harmful (n = 45; 90.0%), including spending sprees, sexual activities, reckless driving, drug use, binge drinking, or self-injurious behaviors. Most participants (n = 44; 88.0%) reported that they experienced feelings of suspiciousness or distrust of others, that they had chronic feelings of emptiness (n = 43; 86.0%), or that they experienced intense anger or had difficulty controlling their anger (n = 42; 84.0%), including frequent displays of temper, constantly being angry, or recurrent physical fights. Participants also spontaneously reported experiencing other symptoms that they thought were related to BPD, including depression (n = 12; 24.0%), suicidal ideations (n = 12; 24.0%), dissociative symptoms (n = 5; 10.0%), and having trouble focusing or concentrating (n = 3; 6.0%).
Participants most often described extreme moods or emotional responses as the symptom they found the most bothersome (n = 19; 38.0%), followed by intense or unstable relationships (n = 10; 20.0%), intense anger or difficulty controlling anger (n = 8; 16.0%), unstable self-image (n = 7; 14.0%), feelings of suspiciousness or distrust of others (n = 6; 12.0%), and chronic feelings of emptiness (n = 6; 12.0%) (Figure 1B). Symptoms related to BPD less frequently reported as most bothersome to participants included impulsive behaviors (n = 3; 6.0%), lack of focus/concentration (n = 3; 6.0%), and suicidal ideations (n = 2; 4.0%).
Impacts Related to Borderline Personality Disorder
Participants reported having problems with their relationships, work/school, memory/thinking, self-care, and finances due to their BPD-related symptoms (Figure 2A). All participants (100%) reported that their BPD-related symptoms impacted their relationships, including repeated breakups and conflicts in romantic relationships or with family/friends. Almost all participants (n = 47; 94.0%) noted that their BPD-related symptoms affected their work/school, including their ability to keep their job/stay in school; caused trouble with coworkers, employers, or teachers; and caused absences at work or school due to emotional concerns or hospitalizations. Additionally, 46 participants (92.0%) reported that BPD-related symptoms impacted their memory/thinking, which included having difficulty concentrating, focusing, planning, or organizing. Forty-three participants (86.0%) reported that their BPD-related symptoms negatively affected their self-care, including eating, showering, doing laundry, cleaning the house, exercising, or partaking in excessive smoking/alcohol/drug use. Thirty participants (60.0%) discussed the financial impacts of BPD-related symptoms, including getting into debt and the inability to pay bills on time. Lastly, 11 participants (22.0%) reported that they experienced legal issues due to their BPD-related symptoms, particularly due to their impulsive behaviors, extreme moods or emotional responses/control, and anger. Table 3 presents representative quotes describing the impact of the participants’ BPD-related symptoms.
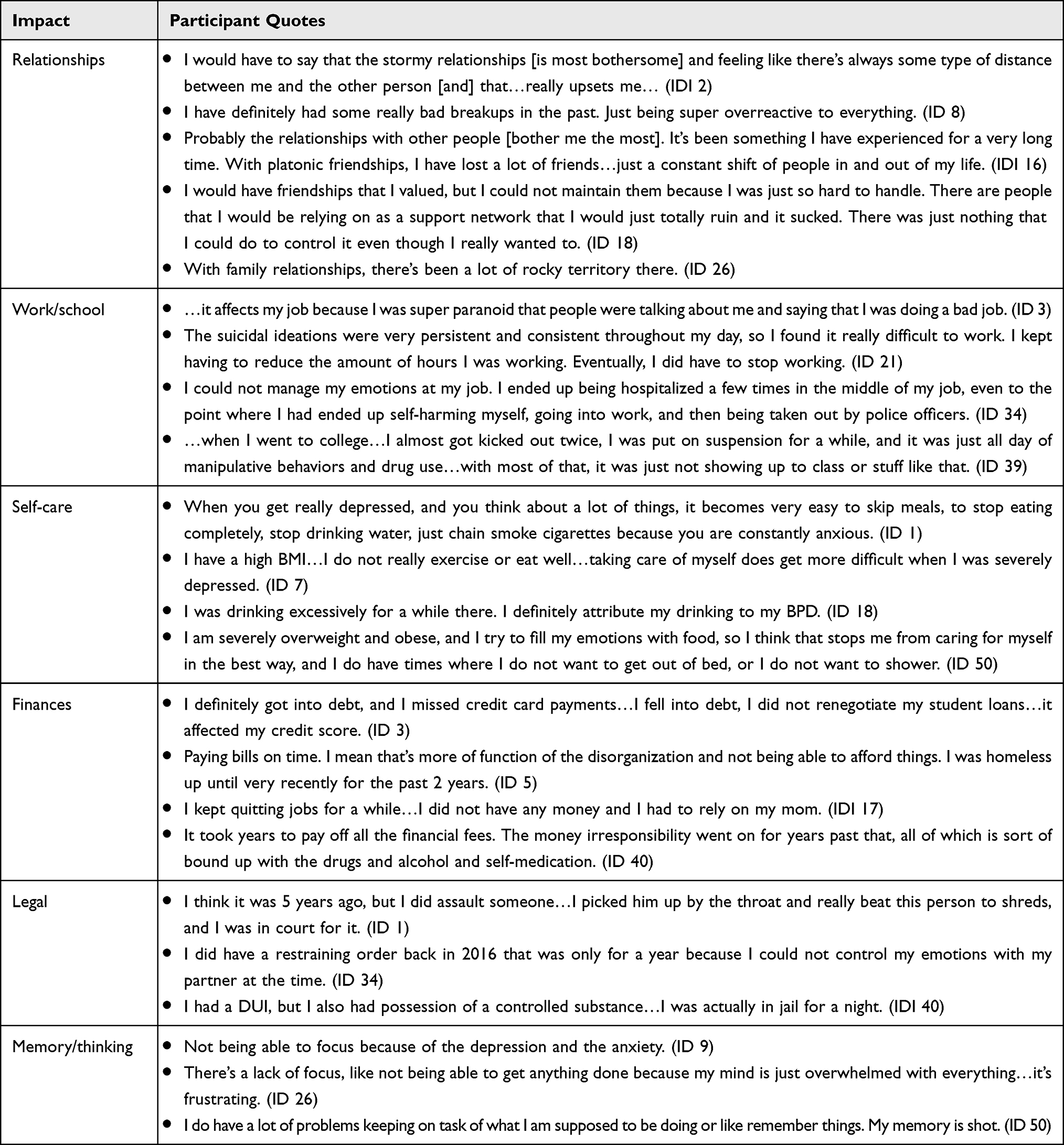 |
Table 3 Participant Quotes Describing Impacts of Borderline Personality Disorder |
 |
Figure 2 Impacts of Symptoms Related to Borderline Personality Disorder. Notes: Frequency of impacts (A) and most bothersome impacts (B) of BPD-related symptoms reported by participants (N = 49). A few participants (n = 6) chose more than 1 most bothersome impact of BPD-related symptoms. One participant in the sample reported that extreme moods/emotional response was most bothersome in response to questions regarding most bothersome symptom and most bothersome impact related to BPD; thus, this response was not included in the current figure, as it was included in Figure 1. |
Figure 2B presents the most bothersome impacts of BPD-related symptoms. Of the 49 participants who described the most bothersome impacts of BPD-related symptoms, nearly two-thirds of the sample (n = 31; 63.3%) reported that the impact of BPD on their relationships was the most bothersome, because these participants desired stable and healthy familial and nonfamilial relationships. Impacts related to BPD that were less frequently reported as most bothersome to participants included experiencing financial problems (n = 7; 14.3%), issues with work/school (n = 6; 12.2%), issues with memory/thinking (n = 6; 12.2%), legal complications (n = 3; 6.1%), and issues with self-care (n = 2; 4.1%).
Discussion
The present study characterized participants’ experiences of BPD and provides a deeper understanding of BPD symptoms and the impact of these symptoms on the lives of individuals with BPD. All participants described having difficulties with extreme emotional responses and interpersonal relationships. Additionally, most participants reported experiencing issues with self-image, impulsivity, suspiciousness/distrust, feelings of emptiness, and anger. All participants remarked that their BPD-related symptoms negatively impacted their interpersonal relationships. Furthermore, more than half of the participants discussed other impacts related to their BPD symptoms, including impacts on work or school, memory or thinking, self-care, and financial and legal issues.
Given the paucity of qualitative research in this patient population, the current study provides valuable information on interview participants’ perspectives of their BPD-related symptoms and impacts, including the aspects of BPD that bothered participants the most. The symptoms that were most bothersome to participants were extreme moods or emotional responses and a pattern of unstable personal relationships. The most bothersome impact experienced by participants was consistent with these most bothersome symptoms, with nearly two-thirds of the sample reporting that they were most bothered by the impact of BPD on their interpersonal relationships. In agreement with these findings, social relationships were a common theme identified in previous qualitative studies in individuals with BPD.13,14 In an interview study in 9 adults with BPD, 8 of whom were female, Black et al14 found predominant themes of self-harming behavior, suicidality, and BPD-related impacts on interactions with family and friends. Miller13 conducted qualitative interviews with 10 patients with BPD and identified common themes of estrangement, inadequacy, and despair. In an early phenomenological study about the experiences of 30 adult female participants living with BPD, Nehls19 similarly identified themes of living with a label and living with self-destructive behavior but did not emphasize social relationships among the key themes. Given the diversity of symptoms and impacts experienced by those with BPD, the qualitative data from the present study on a larger sample of adults, including both males and females, provides a more comprehensive picture of the symptoms and impacts that are most important to these individuals.
The results of this study align with the DSM-51 as well as with results from both qualitative and quantitative studies suggesting that individuals with BPD lack a sense of belonging and experience impairments in their social interactions.20–23 The participants in the present study desired stable, healthy relationships, which are understood as an essential component of the recovery process.24,25 Notably, individuals with personality disorders describe meaningful engagement in relationships and a sense of belonging and integration as important aspects of their personal recovery.6,15,22,26 For example, Fallon26 conducted unstructured interviews with 7 patients with BPD and found that relationships were viewed as the most important supportive variable in patients’ lives and that these relationships played a crucial role in patients’ abilities to contain their distressing emotions. Furthermore, in a qualitative study by Ng et al,15 the authors recommended an increased focus on patients’ relationships in the treatment of BPD. Taken together, these findings suggest that the development of therapies focused on relationship building may be important for individuals with BPD.
A limitation of this study is that the data obtained from clinical trial participants may not be representative of the larger, non–clinical trial population of individuals with BPD. However, the symptoms experienced by the interview participants closely align with the diagnostic criteria of the disorder,27 which support that these qualitative findings are credible and trustworthy.28,29 Additionally, a strength of this study was the experienced qualitative interviewers, which included a clinical psychologist. Interviewing participants with a personality disorder about sensitive topics of a very personal nature can be challenging, and it is critical that qualitative interviews are conducted by experts to engage interviewees, maintain conversational flow, and augment concept elicitation.30,31 Finally, the present study’s large sample size and focus on the most bothersome aspects of BPD provide an important contribution to the landscape of literature on this topic.
Conclusion
This study provides much-needed data on the patient perspective, including in-depth quotes representative of the participants’ lived experiences with BPD. Interview participants reported that the most bothersome symptoms of BPD were those related to extreme moods or emotional responses and those related to interpersonal relationships. Participants similarly described the impact of BPD on their interpersonal relationships as the most bothersome impact of their BPD-related symptoms. Overall, results from this study indicate that the burden of BPD is significant and new treatments are warranted that target the BPD-related symptoms and impacts that matter most to individuals with BPD.
Data Sharing Statement
Data are primarily in the form of transcripts and field notes and cannot be made available in order to protect participant privacy in accordance with the principles of the Belmont Report.
Ethics Approval and Informed Consent
This study complies with the Declaration of Helsinki and was approved by Advarra, a central institutional review board (IRB Number Pro00046283). Participants provided written, informed consent prior to participation in the interview study as well as verbal consent prior to the start of each interview.
Consent for Publication
Participants provided consent for publication of anonymized study findings.
Acknowledgments
The authors thank Cassondra Saande, PhD, and Brian Samsell, PhD, of RTI Health Solutions for medical writing assistance. Otsuka Pharmaceutical Development & Commercialization, Inc. provided funding for publication support in the form of manuscript writing, styling, and submission.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Otsuka Pharmaceutical Development & Commercialization, Inc. and H. Lundbeck A/S provided the financial support for the study. RTI Health Solutions, an independent nonprofit research organization, received funding under a research contract with Otsuka Pharmaceutical Development & Commercialization, Inc. to conduct this study and provide publication support in the form of manuscript writing, styling, and submission.
Disclosure
DD and KK are full time employees of RTI Health Solutions, an independent nonprofit research organization, which was retained by Otsuka Pharmaceutical Development & Commercialization, Inc. to conduct the research that is the subject of this manuscript. Their compensation is unconnected to the studies on which they work. HCW and DO are employees of Otsuka Pharmaceutical Development & Commercialization, Inc. The authors report no other conflicts of interest in this work.
References
1. American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Washington, DC: American Psychiatric Publishing; 2013.
2. Ellison WD, Rosenstein LK, Morgan TA, Zimmerman M. Community and clinical epidemiology of borderline personality disorder. Psychiatr Clin North Am. 2018;41(4):561–573. doi:10.1016/j.psc.2018.07.008
3. Leichsenring F, Leibing E, Kruse J, New AS, Leweke F. Borderline personality disorder. Lancet. 2011;377(9759):74–84. doi:10.1016/S0140-6736(10)61422-5
4. Stone MH. Borderline personality disorder: clinical guidelines for treatment. Psychodyn Psychiatry. 2019;47(1):5–26. doi:10.1521/pdps.2019.47.1.5
5. Chapman J, Jamil RT, Fleisher C. Borderline Personality Disorder. Treasure Island (FL): StatPearls Publishing LLC.; 2022.
6. Katsakou C, Marougka S, Barnicot K, et al. Recovery in Borderline Personality Disorder (BPD): a qualitative study of service users’ perspectives. PLoS One. 2012;7(5):e36517. doi:10.1371/journal.pone.0036517
7. Flanagan EH, Davidson L, Strauss JS. The Need for Patient-Subjective Data in the DSM and the ICD. Psychiatry. 2010;73(4):297–307. doi:10.1521/psyc.2010.73.4.297
8. Miller CE, Townsend ML, Grenyer BFS. Understanding chronic feelings of emptiness in borderline personality disorder: a qualitative study. Borderline Personal Disord Emot Dysregul. 2021;8(1):24. doi:10.1186/s40479-021-00164-8
9. Moltu C, Kverme B, Veseth M, Natvik E. How people diagnosed with borderline personality disorder experience relationships to oneself and to others. A qualitative in-depth study. Int J Qual Stud Health Well-Being. 2023;18(1):2152220. doi:10.1080/17482631.2022.2152220
10. Perseius KI, Ekdahl S, Asberg M, Samuelsson M. To tame a volcano: patients with borderline personality disorder and their perceptions of suffering. Arch Psychiatr Nurs. 2005;19(4):160–168. doi:10.1016/j.apnu.2005.05.001
11. Dammann G, Hügli C, Selinger J, et al. The self-image in borderline personality disorder: an in-depth qualitative research study. J Pers Disord. 2011;25(4):517–527. doi:10.1521/pedi.2011.25.4.517
12. Brooke S, Horn N. The meaning of self-injury and overdosing amongst women fulfilling the diagnostic criteria for ‘borderline personality disorder’. Psychol Psychother. 2010;83(Pt 2):113–128. doi:10.1348/147608309X468211
13. Miller S. Borderline personality disorder from the patient’ perspective. Hosp Community Psychiatry. 1994;45(12):1215–1219. doi:10.1176/ps.45.12.1215
14. Black G, Murray J, Thornicroft G. Understanding the phenomenology of borderline personality disorder from the patient’s perspective. J Ment Health. 2014;23(2):78–82. doi:10.3109/09638237.2013.869570
15. Fyy N, Townsend ML, Miller CE, Jewell M, Grenyer BFS. The lived experience of recovery in borderline personality disorder: a qualitative study. Borderline Personality Disorder Emotion Dysregulation. 2019;6(1):10. doi:10.1186/s40479-019-0107-2
16. United States Food and Drug Administration. Patient-Focused Drug Development Guidance: methods to Identify What is Important to Patients and Select, Develop or Modify Fit-for-Purpose Clinical Outcome Assessments. Available from: https://www.fda.gov/drugs/news-events-human-drugs/patient-focused-drug-development-guidance-methods-identify-what-important-patients-and-select.
17. Clinicaltrials.gov. A trial of brexpiprazole in the treatment of borderline personality disorder. ClinicalTrials.gov Identifier: NCT04100096. Available from: https://clinicaltrials.gov/ct2/show/study/NCT04100096.
18. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
19. Nehls N. Borderline personality disorder: the voice of patients. Res Nurs Health. 1999;22(4):285–293. doi:10.1002/(SICI)1098-240X(199908)22:4<285::AID-NUR3>3.0.CO;2-R
20. Kalpakci A, Venta A, Sharp C. Beliefs about unmet interpersonal needs mediate the relation between conflictual family relations and borderline personality features in young adult females. Borderline Personal Disord Emot Dysregul. 2014;1(1):11. doi:10.1186/2051-6673-1-11
21. Dixon-Gordon KL, Gratz KL, Breetz A, Tull M. A laboratory-based examination of responses to social rejection in borderline personality disorder: the mediating role of emotion dysregulation. J Pers Disord. 2013;27(2):157–171. doi:10.1521/pedi.2013.27.2.157
22. Ikhtabi S, Pitman A, Toh G, Birken M, Pearce E, Johnson S. The experience of loneliness among people with a “personality disorder” diagnosis or traits: a qualitative meta-synthesis. BMC Psychiatry. 2022;22(1):130. doi:10.1186/s12888-022-03767-9
23. Lis S, Bohus M. Social interaction in borderline personality disorder. Curr Psychiatry Rep. 2013;15(2):338. doi:10.1007/s11920-012-0338-z
24. Leamy M, Bird V, Boutillier CL, Williams J, Slade M. Conceptual framework for personal recovery in mental health: systematic review and narrative synthesis. Brit J Psychiatry. 2011;199(6):445–452. doi:10.1192/bjp.bp.110.083733
25. Kverme B, Natvik E, Veseth M, Moltu C. Moving toward connectedness – a qualitative study of recovery processes for people with borderline personality disorder. Front Psychol. 2019;10:10. doi:10.3389/fpsyg.2019.00010
26. Fallon P. Travelling through the system: the lived experience of people with borderline personality disorder in contact with psychiatric services. J Psychiatr Ment Health Nurs. 2003;10(4):393–401. doi:10.1046/j.1365-2850.2003.00617.x
27. Biskin RS, Paris J. Diagnosing borderline personality disorder. Can Med Assoc J. 2012;184(16):1789–1794. doi:10.1503/cmaj.090618
28. Leung L. Validity, reliability, and generalizability in qualitative research. J Family Med Prim Care. 2015;4(3):324–327. doi:10.4103/2249-4863.161306
29. Patton MQ. Enhancing the quality and credibility of qualitative analysis. Health Serv Res. 1999;34(5 Pt 2):1189–1208.
30. DeMuro CJ, Lewis SA, DiBenedetti DB, Price MA, Fehnel SE. Successful implementation of cognitive interviews in special populations. Exp Rev Pharmacoecon Outcomes Res. 2012;12(2):181–187. doi:10.1586/erp.11.103
31. DiBenedetti DB, Price MA, Andrews EB. Cognitive interviewing in risk minimization survey development: patient and healthcare professional surveys. Exp Rev Clin Pharmacol. 2013;6(4):369–373. doi:10.1586/17512433.2013.811824
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.