Back to Journals » Advances in Medical Education and Practice » Volume 16
Understanding Barriers to Nanotechnology Education in Medical Specialty Programs: A Qualitative Nominal Group Study Among Postgraduate Students
Authors Díaz-López MM, Bustos RH ![]() , Guevara-Ramírez JF
, Guevara-Ramírez JF ![]() , García JC
, García JC
Received 12 March 2025
Accepted for publication 3 July 2025
Published 20 August 2025 Volume 2025:16 Pages 1481—1499
DOI https://doi.org/10.2147/AMEP.S523258
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Mónica María Díaz-López,1 Rosa-Helena Bustos,2 Juan Francisco Guevara-Ramírez,3 Julio-Cesar García2,4
1Departamento de Educación Médica, Facultad de Medicina, Universidad de la Sabana, Chía, Colombia; 2Department of Clinical Pharmacology, Evidence-Based Therapeutics Group, Faculty of Medicine, Universidad de La Sabana, Chía, Colombia; 3Facultad de Medicina, Universidad de La Sabana, Chía, Colombia; 4Clínica Universidad de La Sabana, Chía, Colombia
Correspondence: Rosa-Helena Bustos, Department of Pharmacology, Evidence-Based Therapeutics Group, Faculty of Medicine, Universidad de La Sabana, Chía, Colombia, Tel/Fax +576018615555, Email [email protected]
Introduction: Nanotechnology has emerged as a promising field of study, aiming to revolutionize healthcare through the innovative development of drugs, diagnostic tools, and medical devices. As a result, healthcare professionals in training are constantly faced with the challenge of understanding and applying these emerging technologies. The objective of this study is to determine the factors to consider for including the teaching of nanotechnological tools in medical specialty postgraduate programs.
Methods: A study based on the Nominal Group Technique (NGT) was conducted to identify the factors that promote and hinder the implementation of nanotechnology in certain postgraduate programs where nanotechnology is employed, such as Internal Medicine, Critical Care Medicine, Family Medicine, and Clinical Pharmacology at the School of Medicine of Universidad de La Sabana. A framework analysis was used to analyze the collected data.
Results: Based on the two research questions, several aspects were identified for the inclusion of nanotechnology in the medical practice of specialties. Key challenges include lack of knowledge and resource availability, misinformation, and lack of knowledge, as well as paradigmatic analysis as the main obstacles to the use of nanotechnology.
Conclusion: The findings provide a first-time study on nanotechnology curricula within medical specialty programs in Colombia, with potential extrapolation to similar situations in other medical schools. These insights can inform the global development of medical education curricula by highlighting the need for structured nanotechnology training, fostering interdisciplinary collaboration, and addressing resource and knowledge gaps to prepare future healthcare professionals for advancing medical technology worldwide.
Keywords: nanotechnology, nominal group technique, NGT, medical education
Introduction
The current era is witnessing a profound scientific revolution, markedly diverging from the First Revolution’s focus on large-scale projects such as expansive operating rooms and skyscrapers. Today, the emphasis lies in developing smaller, more precise, and highly utilitarian tools. Nanotechnology epitomizes this shift, involving the design and manipulation of objects ranging from 1 to 100 nanometers—dimensions so minute they are one-hundredth the thickness of a sheet of paper.1,2
As a result, contemporary medicine is undergoing an unprecedented phase of innovation. The convergence of various scientific disciplines is pushing the boundaries of disease diagnosis, treatment, early detection, and prevention. Within this context, nanotechnology has emerged as a pivotal force, substantially transforming clinical practice and medical education in institutions worldwide, both in the West and the East, that have integrated it into their medical-surgical curricula.3–5 The concept of “nanomedicine” represents a paradigm shift, offering novel insights into the translation of advanced medical technologies from the laboratory to clinical practice.
The COVID-19 pandemic underscored the value of nanomedicine by accelerating the development of more effective diagnostic tools, therapeutic strategies, and vaccine delivery systems.6,7 This global health crisis has emphasized the urgent need for modern medical education to incorporate innovative technologies.3–5 Integrating nanotechnology into medical education not only enhances students’ understanding of disease diagnosis and treatment but also fosters practical skills in utilizing advanced medical technologies.
Nanotechnology has impacted various medical domains, including drug delivery systems8,9 and medical imaging.7,10 In drug delivery, nanotechnology has facilitated the development of systems that interact at cellular and molecular levels, improving therapeutic efficacy while minimizing side effects. Moreover, its focus on quality by design stresses the need to ensure both the efficacy and safety of treatments with minimal immune reactivity.8
In medical imaging, nanotechnology has revolutionized current technologies by enhancing image contrast and specificity, enabling more accurate and earlier disease diagnoses through advanced imaging agents.10 Nanotechnology also presents significant opportunities in preventing nosocomial infections and improving public health outcomes through faster diagnostics and timely responses to critical patient conditions.7 Research on antimicrobial nanoparticles is pioneering new strategies to combat hospital-acquired and opportunistic infections.3,7,8
However, the advancement of nanotechnology also raises ethical and regulatory challenges. The potential toxicity of nanoparticles and their impact on human health and the environment are growing concerns. Establishing appropriate regulatory frameworks and safety standards is crucial to ensuring the safe and sustainable application of nanotechnology in medicine.2,7
In the realm of precision and personalized medicine, nanotechnology plays an essential role in biomarker discovery, improving diagnostic accuracy, and optimizing individualized treatments, including advanced technologies such as CRISPR.2,7,11,12 Incorporating nanotechnology into postgraduate medical-surgical education programs is crucial for preparing healthcare professionals to fully leverage these innovations.6 However, while the transformative potential of nanotechnology in healthcare is well-documented and its importance is completely recognized, there remains a critical gap from empirical studies in understanding how to effectively integrate these advancements into postgraduate medical specialty training and curricula, particularly in resource-limited settings such as Latin America.
The reason behind that regional impact is the biased existing literature focusing on high-income countries or theoretical frameworks, where robust infrastructure, interdisciplinary collaborations, partnerships with nanotechnology research hubs, and funding mechanisms appear to facilitate curricular updates, leaving some context-specific barriers such as curricular rigidity that prioritizes traditional and urgent medical subjects over emerging and innovative technologies, adding the lesser faculty expertise, and infrastructural limitations that hinder implementation in countries like Colombia.
This gap is further exacerbated by a lack of participatory research involving the medical residents, which, as frontline trainees, possess firsthand insights into curricular relevance and practicality, yet their perspectives are underrepresented in pedagogical reforms. Without empirical data grounded in their experiences, efforts to modernize medical education risk misalignment with on-the-ground realities, perpetuating disparities in technological adoption.
By mastering both the foundational principles of nanomedicine and the practical use of diagnostic and therapeutic technologies, healthcare professionals trained in this field will be better equipped to meet future challenges. Therefore, incorporating nanotechnology into medical education is essential for equipping healthcare professionals with the skills and knowledge to lead in modern medicine, which increasingly influences diverse specialties and informs clinical decision-making considering future innovations.13–16
By advancing understanding of cutting-edge medical technologies and fostering the practical skills necessary for their clinical application, nanotechnology is paving the way for a new era in healthcare, where precision, efficacy, and innovation serve as the cornerstones of patient care.2,3,17,18 Despite its widely acknowledged transformative potential in medicine, diagnostics, and education, nanotechnology also involves substantial financial demands. These include significant investments in infrastructure, specialized equipment, research and development, skilled personnel, and regulatory compliance. As noted by Alardawe et al (2022), nanotechnology reshapes the structure of production costs by increasing fixed and indirect expenditures, thereby necessitating the implementation of advanced cost management strategies to ensure sustainability. Within the context of medical education, such economic requirements may pose challenges to scalability and equity, particularly in low-resource environments. Consequently, any effort to integrate nanotechnology must be accompanied by a critical assessment of its financial viability and logistical feasibility within the constraints of existing institutional systems.19 This article aims to identify the enabling factors and systemic obstacles perceived as essential by medical residents in medical-surgical specialties at our institution for implementing nanotechnology education within the medical curriculum and to assess key aspects of its impact on daily professional practice and medical education, through Nominal Group Technique (NGT) focus groups as a structured and participatory methodology fostering equitable participation by minimizing dominance by vocal individuals, and generating consensus-driven priorities within the iterative rounds of idea generation, discussion, and ranking.
Beyond curricular reform, we aim to reshape residents training in nanotechnology applications and embedding it into competency-based assessments, reassuring that future clinicians not only understand nanoscale innovations but also apply them ethically and effectively. Then, it bridges a methodological and regional void in the literature, offering a replicable model for institutions navigating one of the complexities of 21st-century medical education, advocating for an equitable technology access.
Materials and Methods
A qualitative study was conducted using the adapted NGT,20,21 which could help identify the most important aspects of the challenge of implementing nanotechnology in the curricula of medical specialties. The rationale for using the NGT methodology in our study is that it enables small teams to participate and, through consensus, prioritize ideas and opinions on a common topic. This approach provides highly valuable qualitative information. This methodology is widely reported in the literature.21–24 The study was carried out at the Universidad de La Sabana, Chía, Colombia, and was approved by Research Ethics Committee of Universidad de La Sabana (protocol 01 18 May 2021), as part of the framework of a macro research project “Nanobiosensor platform for therapeutic drug monitoring (TDM) as a strategy in minimizing antimicrobial resistance”. The Nominal Group Technique (NGT) was planned and prepared during the second half of 2024, with its implementation carried out over a period of six weeks. This timeframe included the preparation of materials, recruitment and coordination of participants, the structured discussion sessions, and the subsequent thematic analysis.
The implementation of the Nominal Group Technique (NGT) took place within 120 minutes, providing sufficient time to complete all the planned phases: from the selection of experts to the analysis and validation of the consensus reached. It involves a sequential process composed of distinct phases: introduction and clarification of the research question, silent individual idea generation, structured round-robin sharing of ideas, group clarification and consolidation, followed by individual ranking or voting to prioritize responses.21–23,25 This method fosters equitable participation, minimizes groupthink, and enables the systematic collection of expert opinions.21–26 NGT is particularly valuable in medical education and health research for identifying priorities, evaluating curricular content, or eliciting expert consensus on emerging topics such as nanomedicine or artificial intelligence integration. The total duration of the technique’s implementation was adequate to ensure the experts’ active reflection and participation, as well as to consolidate the results of each phase without compromising the quality of the consensus. In this study, thematic analysis was integrated as an essential phase of the methodological process based on the Nominal Group Technique (NGT).
Indeed, as part of the methodological design, participants were previously provided with a selected introductory reading on nanotechnology applied to medicine, extracted from updated scientific literature and relevant to the objective of the study.3,5 This strategy aimed to ensure a minimum common knowledge among experts, promote informed participation, and facilitate a richer and more focused discussion during the Nominal Group Technique (NGT) session.
After the idea generation session by the expert participants, each idea was recorded verbatim and preliminarily grouped into tentative categories by the facilitators21–24 was carried out, allowing the identification of recurring patterns within the set of prioritized ideas.
This analysis consisted of several stages: (1) familiarization with the data generated in the TGN sessions, (2) initial coding of the ideas and associated observations, (3) grouping of codes into preliminary themes, (4) review of the themes based on their internal coherence and relevance to the study objectives, and (5) definition and final naming of the emerging themes. Each phase of the analysis was carried out independently by two researchers and consensus was subsequently reached through discussion, thus ensuring the validity and reliability of the process.
This methodological approach allowed for the rigorous systematization of the information obtained, consistent with the participatory and structured foundations that characterize the TGN. The statistical classification of ideas was complemented by this thematic analysis to offer a richer and more contextualized interpretation of the findings.
Participants
The participants for the NGT were medical residents from various specialties at Universidad de La Sabana. Recruitment was conducted through an open call inviting voluntary participation in the study (Figure 1S).
Prior of the NGT, each participant received a formal invitation to participate in the study, which explained the objectives, the voluntary nature of their participation, and the confidentiality conditions. Subsequently, all participants signed an informed consent form duly approved by the institutional ethics committee. The informed consent obtained from participants included their agreement to the publication of anonymized responses and direct quotes.
Before beginning the session, it was reiterated that the comments, interpretations, and positions expressed would be treated with strict confidentiality, and that no information would be used to individually identify the participants. It was also explicitly agreed that the verbal information shared during the clarification of the written documents would be systematized anonymously, without personal attribution, thus ensuring respect for the privacy of the contributions and the integrity of the process. These precautions created an atmosphere of trust and openness, in which participants felt safe to express their opinions freely, contributing to the quality of the consensus reached.
A total of 12 residents participated in the NGT, representing the specialties of internal medicine, critical care, family medicine, and clinical pharmacology (3 residents from each specialty). In this context, a small, intentional sample, such as 12 participants, is appropriate and consistent with the methodological approach, as it allows for effective interaction without compromising the diversity of ideas or the depth of analysis.20–24
Data Collection
The NGT Was Conducted in Three Phases
Phase I: The objectives of the NGT were shared with participants before starting the activity. The multiple purposes of the technique were explained, as it provides participants with the opportunity to begin thinking about their contributions to the topics discussed. A discussion about these topics followed. Additionally, participants were given time to ask clarifying questions about their role, their participation, and what would be expected of them.21
Phase II: The purpose of the meeting and the value of participants’ contributions were emphasized, as well as the voluntary and anonymous nature of their participation. Participants provided written informed consent before the focus group session began (Supplementary material 1). The information was anonymized and treated according to ethical principles of confidentiality. All participants agreed to be recorded during the NGT session.
Targeted questions were formulated following a thorough literature review and consultations with specialists in addiction treatment and nominal group technique methodologies. The questions were designed to address two key decision points in the treatment process:
Question 1 (Q1): “In your medical specialty residency, what are the factors that promote the use of nanotechnology?”
Question 2 (Q2): “In your medical specialty residency, what are the factors you believe hinder the implementation of nanotechnology?”
The participants were asked to write their ideas in silence for about 10 minutes. Subsequently, a turn-by-turn idea collection was carried out, where the moderator wrote each point mentioned on a whiteboard, allowing the entire group to see the growing list of ideas and be stimulated to think of additional ones.
This method of data collection served multiple purposes: it freed the facilitator from influencing group opinions, protected the anonymity of those presenting ideas, and focused on the idea rather than the author. This approach helped to address anchoring bias, a bias where participants attempt to align their responses with the group’s opinion, and also minimized social desirability bias, where respondents attempt to provide answers that present themselves in a socially favorable manner.
Afterward, forms were collected, and the participants’ comments on the listed elements were transcribed. The facilitator ensured that the information was complete and clearly explained to all participants. If there were questions about what was written, participants clarified the meaning. The session continued with the structured discussion of ideas for a limited time, followed by additional rounds of questions and idea generation until responses were saturated. Finally, a selection and ranking of ideas (voting) was conducted.
In some cases, a brief clarification dialogue took place.20 This step ensured that participants understood the meaning of each idea, allowing individuals to make informed decisions when ranking their priorities.26 The moderator ensured that dominant participants did not unduly influence the group.
Phase III (Analysis): In the third phase, participants were asked to silently rank the top five ideas (5 = highest priority and 1 = lowest priority). Votes were tallied, and ideas were ranked.27 A final discussion was held to determine if the group supported the top-ranked priorities. The nominal group session was audio-recorded and transcribed verbatim to aid in understanding and retaining participants’ considerations.
Our findings were reported in accordance with the RATS guidelines for qualitative research, which evaluate the relevance of the study question, appropriateness of the qualitative method, transparency of procedures, and soundness of the interpretive approach.28
Results
A total of 12 residents from 4 medical specialties participated in the NGT. Based on the questions asked, three key elements were highlighted: a) Aspects to consider for the inclusion of nanotechnology in medical-surgical education (MSE); b) Mechanisms for introducing nanotechnology into MSE; c) Competitive advantages of incorporating nanotechnology into MSE.
Before starting with the questions, basic aspects and concepts of nanotechnology were discussed to provide context for the questions. The concept of nanotechnology, although seemingly simple, proved to be a difficult term to define and was mostly based on the idea of scale.
Each resident received 3 votes for question 1 and 5 votes for question 2 for each of the established categories. The data obtained are presented in Table 1, which contains some of the participants’ narratives, categories, and thematic analysis in response to questions Q1 and Q2. Likewise, Figure 1 represents the representative percentage of each category designated for questions Q1 and Q2. In the first question, aimed at identifying factors that promote the use of nanotechnology, five main categories were obtained. The most notable was the construction of quality of knowledge and its application, with 17 votes (47.22%), followed by the availability of resources, with 9 votes (25%). Thirdly, two factors with equal weight were identified: cost-effectiveness of implementation and policies for its implementation, each with 4 votes (11.11%). Finally, interdisciplinary and intradisciplinary work received 2 votes, representing 5.6% of the total. Regarding the factors that hinder the implementation of nanotechnology, the most voted category was misinformation and lack of knowledge, with 27 votes (44.26%). This was followed by paradigmatic paralysis with 10 votes (16.39%), and the structure and security of the health system, with 7 votes (11.47%). Other obstacles noted included curricular articulation in practice (6 votes, 9.83%), approval of the national nanotechnology system (5 votes, 8.19%), industry influence (3 votes, 4.92%), conflict of interest (2 votes, 3.28%) and, finally, lack of critical judgment, with 1 vote (1.64%).
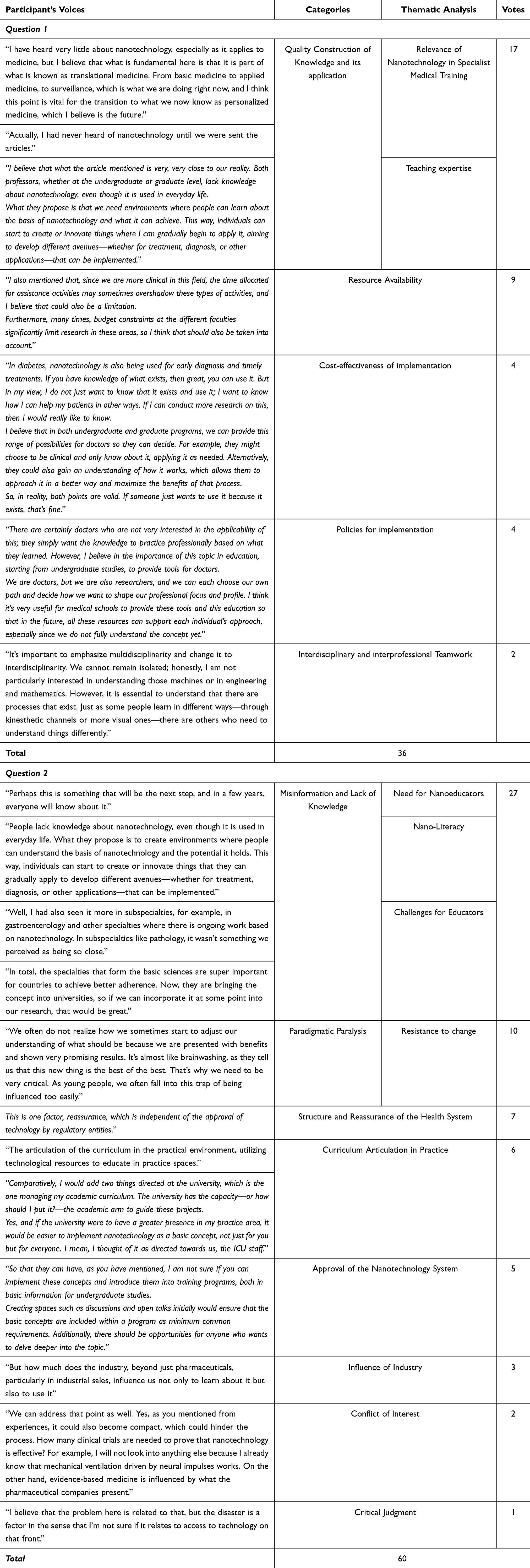 |
Table 1 Some Narratives From the Participants, Categories, and Thematic Analysis in Response to Questions Q1 and Q2 |
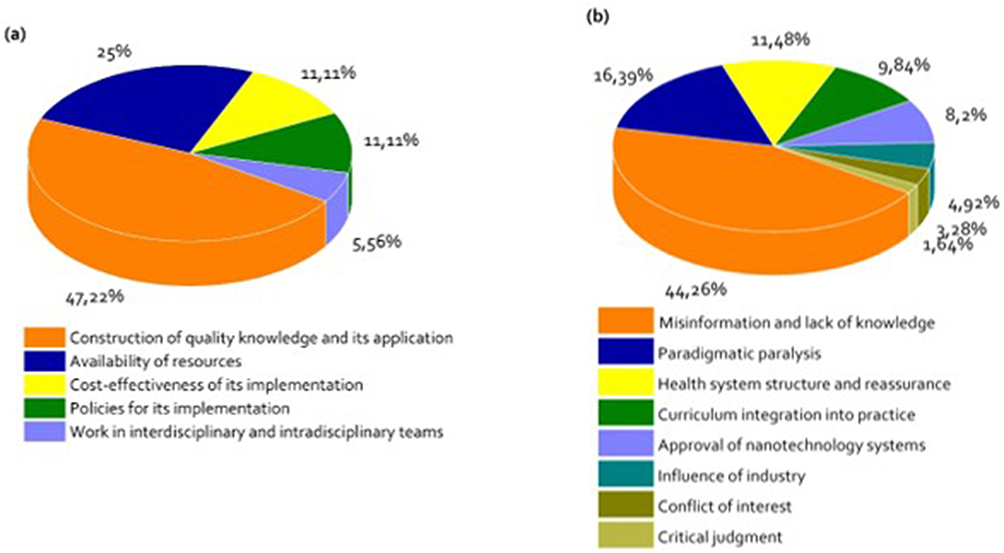 |
Figure 1 Percentage diagram of the analyzed categories from participants’ responses to Q1 (a) and Q2 (b) using the Nominal Group Technique (NGT). |
The categories analyzed for each of the responses using NGT provide valuable insights into the challenges and obstacles in the implementation of nanotechnology in medical specialty curricula.
A relationship was established between each emerging category and its potential curricular implications, highlighting how the elements prioritized by experts can guide the design of content, methodologies, and strategies for medical training in nanotechnology. This approach strengthens the applicability of the results by providing concrete evidence that can be used by decision-makers and curriculum designers to promote the effective inclusion of nanotechnology in specialized medical training. Table 2 presents a comparison of the different categories analyzed within the NTG.
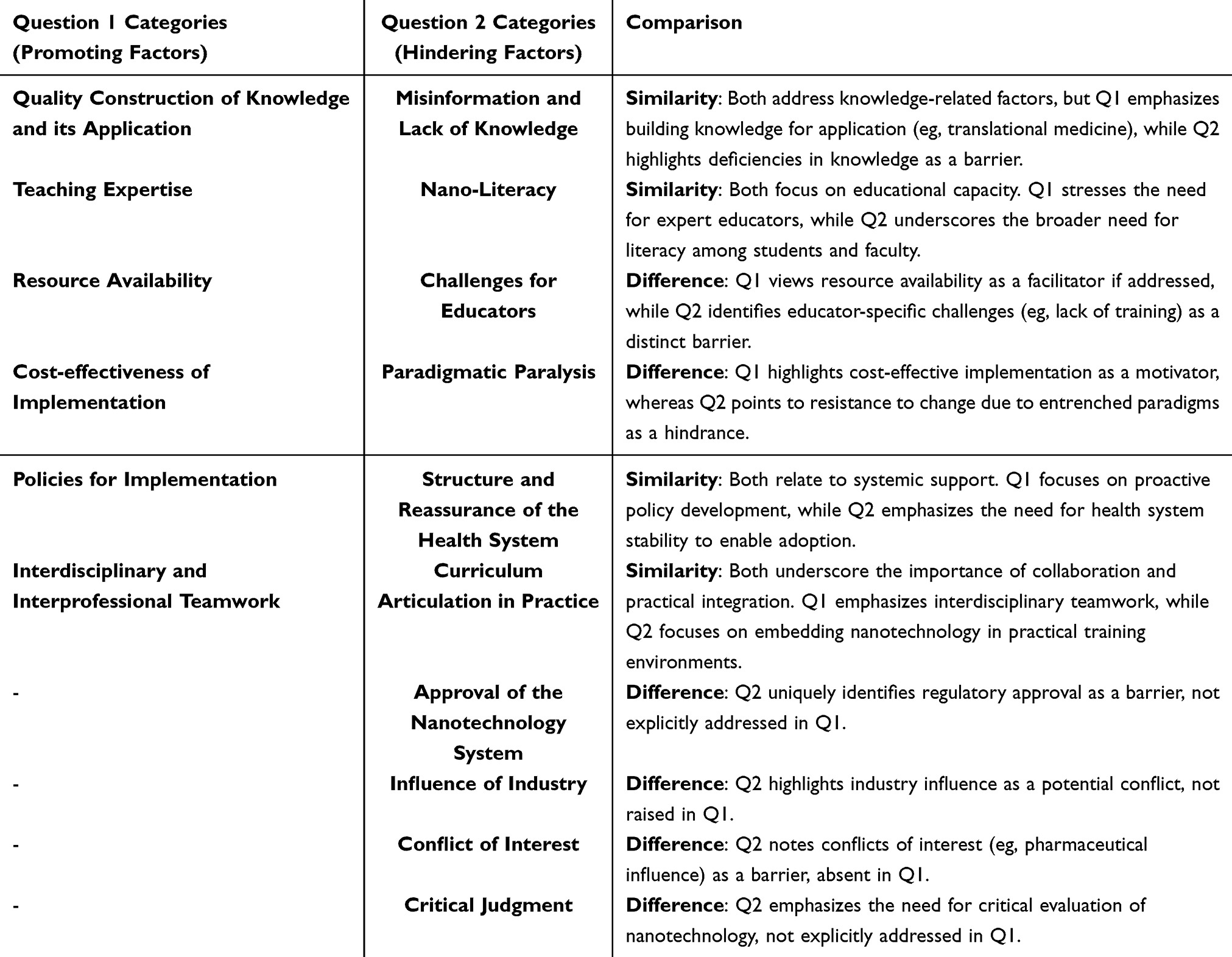 |
Table 2 ComparativeAnalysis of Categories for Question 1 and Question 2 |
Discussion
This section presents an analysis of the significance of the results obtained from the NGT activity, focusing on the main challenges faced by medical specialty residents in implementing nanotechnology in their curricula, as well as the key aspects for promoting the use of nanotechnology. The analysis is subdivided according to the questions posed.
Question 1
Category 1: Quality Construction of Knowledge and its Application
This category addresses critical aspects of the educational process initiated at the undergraduate level, highlighting that a solid foundation in basic sciences is essential to understand the role and applications of nanotechnology in medicine.
Nanotechnology is often referred to as a pillar of the next industrial revolution, due to its potential to transform multiple sectors through precise manipulation of matter at the nanoscale. To ensure that its research, development, and social implications achieve a meaningful impact, it is essential to promote continuing education programs that address its risks, benefits, limitations, and ethical considerations.29 These advances present significant challenges for academic institutions—not only in content delivery but also in the pedagogical approaches required to train new generations of professionals capable of leading in this emerging field.
The demand for a scientifically literate workforce, equipped to understand and apply nanotechnological tools, is growing in response to this technological shift. Nanotechnology is not limited to medicine; its relevance extends to consumer goods, electronics, energy, environmental solutions, and data technologies.30,31 This breadth underscores the need for educational systems to adapt and to prepare learners for a society deeply intertwined with nanoscale innovations.
In the medical field, nanotechnology has enabled novel applications under the umbrella of nanomedicine, including nanoparticles for drug delivery, advanced imaging agents, diagnostic systems, implants, and tissue engineering solutions.9,17 For instance, chemotherapeutic drugs can now be administered more safely, with reduced systemic toxicity. Wearable and implantable nanodevices offer real-time monitoring of physiological parameters and early detection of pathological changes, such as infections or cancer. These technologies position clinicians closer to the source of disease signals, enabling faster and more precise interventions. Furthermore, the convergence of nanotechnology with artificial intelligence and predictive analytics expands the frontiers of personalized and preventive medicine.30 During the NGT plenary session, participants strongly emphasized the need for nanotechnology to be integrated transversally across the medical curriculum. They suggested that this integration be both horizontal and vertical, allowing for the progressive accumulation of knowledge throughout medical education, culminating in its consolidation during postgraduate training. The MEDICUS curricular model at our institution reflects this integrated vision.32 This approach is aligned with the principles of spiral integration, wherein complex subjects are introduced at a basic level and revisited through successive stages of increasing depth and complexity. Such a curriculum promotes deeper learning by reinforcing knowledge over time, applying it in different contexts, and building strong connections between theoretical foundations and clinical practice.33
In this context, an integrated curriculum is defined as one that delivers synchronized, transdisciplinary content across all years of medical education, bridging fundamental and clinical sciences and supporting the real-world application of innovations like nanotechnology.34
Subcategory: Relevance of Nanotechnology in Specialist Medical Training
Basic biomedical sciences continue to face challenges in maintaining relevance within medical curricula. A solid command of these sciences is a prerequisite for medical training success, as many modern diagnostic and therapeutic tools are built on their principles.35 In this context, However, significant disparities exist in students’ baseline knowledge, which can hinder their ability to grasp complex concepts such as nanotechnology.36 When foundational understanding is insufficient, students may struggle with biochemical, physiological, and pathophysiological concepts, which can compromise clinical reasoning and lead to academic disengagement or dropout.37 This situation underscores the importance of improving the quality of basic science instruction, especially as it relates to emerging fields. Ensuring students are adequately prepared during early training phases increases their capacity to transfer and apply this knowledge in advanced, context-specific domains such as nanomedicine.
Subcategory 2: Teaching Expertise
Participants also highlighted the crucial role of educators in enabling meaningful learning of scientific content. They emphasized that instructors should not only transmit knowledge but also cultivate critical thinking, ethical reasoning, and the ability to interpret complex information relevant to nanotechnology and healthcare. Medical educators must be equipped to help students understand how emerging technologies work, what their limitations are, and how they can be responsibly applied within the healthcare system.
Nanotechnology itself can serve as a powerful pedagogical tool—one that fosters engagement in STEM fields by stimulating curiosity and innovation. Integrating nanotechnology into formal curricula can contribute to more inclusive, dynamic, and interdisciplinary educational experiences, preparing students to navigate and lead within the highly interconnected world of the Society 5.0 paradigm, where human-centered innovation is key.38 Thus, incorporating nanotechnology into medical education is not merely about adding content; it requires a shift in educational philosophy—one that prepares future physicians to engage with complex systems, make informed decisions, and contribute to global healthcare innovation.
Category 2: Resource Availability
This category emphasizes the importance of aligning educational strategies with national and regional development priorities. Participants noted that the successful integration of nanotechnology into medical education requires a clear understanding of the country’s scientific, technological, and healthcare needs. This includes coherence with public policies, institutional missions, and national innovation agendas.7 Participants also highlighted the value of promoting multidisciplinary and cross-sectoral research, as well as fostering partnerships between universities and industry. These alliances enable the development of applied research, the transfer of technology, and the creation of innovation ecosystems necessary for implementing nanotechnology in real-world medical settings. In this sense, the formation of research consortia and collaborative networks is essential for consolidating critical mass and maximizing available resources.39 Importantly, building scientific and technological capacity should occur within a robust legal and institutional framework, capable of responding dynamically to market demands and innovation cycles. Without such support systems, the integration of nanotechnology into curricula risks being disconnected from broader national strategies and lacking the institutional sustainability needed for long-term impact.
Category 3: Cost-Effectiveness of Implementation
This category addresses one of the most pressing concerns for policymakers and academic institutions: the economic feasibility of integrating nanotechnology into healthcare and education systems. The group discussions acknowledged that the advancement of nanotechnology is closely tied to the evolution of the knowledge society and the specific policies that each country implements based on its socio-political context.
In high-income countries, the growing costs of healthcare—driven by demographic changes such as population aging, increasing prices of medications and treatments, and inefficiencies in service delivery—have led to significant pressures on public health systems. In this context, cost-effectiveness becomes a central argument for promoting innovations that can enhance efficiency and outcomes.40 Nanotechnology offers promise in reducing long-term costs through improved diagnostics, personalized treatments, and early interventions. However, its integration into medical curricula and practice also involves substantial initial investments in infrastructure, human resources, and regulatory adaptation. Therefore, policymakers and health administrators must evaluate whether these investments yield proportional benefits in patient care and system-wide performance. Although nanotechnology is expected to improve healthcare efficiency and outcomes, its implementation poses significant economic challenges. The integration of nanotechnology into industrial and health systems leads to a cost restructuring process that increases fixed and indirect costs, particularly in production, human resource training, and quality assurance. These shifts require a transition from traditional to strategic cost management models to avoid inaccurate pricing and potential loss of competitiveness. Therefore, it is essential that educational institutions and health systems assess whether the long-term benefits of nanotechnology justify its substantial initial investment, especially in resource-constrained environments.19
Category 4: Policies for Implementation
Participants emphasized the need for coherent and supportive public policies to facilitate the implementation of nanotechnology in both educational and healthcare systems. In particular, they noted the absence of a critical mass of specialized professionals—including economists, legal experts, and administrators—who can guide processes such as technology foresight, regulatory compliance, intellectual property management, and market access.41 In Colombia, and in many similar settings, nanotechnology remains largely confined to academic and scientific research environments, with limited emphasis on its translational potential to improve population health, industrial development, or clinical practice.42 This gap underscores the importance of articulating national innovation policies with curricular reform efforts, ensuring that educational advances are aligned with long-term economic and societal goals. Moreover, integrating nanotechnology into medical training requires clear regulatory guidelines, funding mechanisms, and quality assurance systems. These conditions are necessary to ensure safe, ethical, and equitable access to emerging technologies across the healthcare system.
Category 5: Interdisciplinary and Interprofessional Teamwork
Participants also highlighted the lack of a collaborative culture among healthcare professionals as a barrier to innovation. Effective integration of nanotechnology into practice requires interdisciplinary and interprofessional collaboration, bringing together experts from medicine, engineering, basic sciences, business, and public health. The absence of such alliances limits the formation of research teams and innovation clusters capable of addressing local or regional health challenges using nanotechnological approaches.43 Therefore, building networks, bioregions, and strategic alliances is critical for promoting knowledge exchange and technological development. This includes not only clinical and academic actors, but also professionals in resource management, health economics, and commercialization, who play a key role in scaling and sustaining innovation.44 Strengthening these ecosystems will accelerate the translation of nanotechnology from academic discourse into impactful, real-world healthcare solutions.
Question 2 (Q2)
Category 1: Misinformation and Lack of Knowledge
A key obstacle to integrating nanotechnology into medical education is the lack of accessible, accurate information. The rapid evolution of nanoscience has outpaced the adaptation of medical curricula, leaving students with limited exposure to foundational concepts. As this field becomes increasingly relevant across multiple domains—from diagnostics to therapeutics—there is an urgent need to prepare a new generation of professionals, including clinicians, scientists, educators, and policymakers, who are competent in its principles and applications. Participants highlighted the importance of establishing direct connections with national and international nanotechnology research centers to foster experiential learning. Such interactions would allow students to gain practical insights and contextualize the role of nanotechnology in 21st-century healthcare.
Subcategory: Need for Nanoeducators
To bridge this gap, institutions must prioritize the training of educators who possess not only subject-matter expertise in nanoscience but also pedagogical strategies tailored to emerging scientific content. The inclusion of specialists from engineering, material sciences, and biomedicine could facilitate cross-disciplinary knowledge transfer and ensure curricular alignment with technological advances. Furthermore, nanoeducators should serve as catalysts for institutional partnerships with industry and research centers, enhancing both instruction and translational research.
Subcategory: Nano-Literacy
Developing nano-literacy entails more than imparting content—it requires the cultivation of metacognitive, procedural, and critical-thinking skills. Teachers must continuously update their knowledge and incorporate tools for conceptual modeling, simulation, and problem-solving that reflect the complexity and interdisciplinarity of nanotechnology. Instructional designs should promote collaborative learning environments that allow students to articulate, reassess, and deepen their understanding, linking nanoscience to clinical reasoning and public health impact.
Subcategory: Challenges for Educators
The incorporation of nanotechnology into medical curricula necessitates rethinking core competencies for future physicians. This includes adopting innovative pedagogical approaches, reconfiguring assessment strategies, and integrating the social and ethical implications (SEI) of nanotechnological applications. As educational programs rapidly evolve, there is a narrow but critical opportunity to shape curricula that reflect best practices in nanotechnology and prepare students to address real-world healthcare problems.45
Most medical faculty are trained in disciplines outside of nanoscience, underscoring the need for professional development focused on the content and pedagogy of nanoeducation. Building nano-literacy among faculty can promote innovation, foster engagement with research centers, and ensure the delivery of high-quality, inclusive, and impactful learning experiences. Effective teaching in this area also requires fluency with diverse technological tools and platforms, combined with sound pedagogical and evaluative strategies.
In this context, education must extend beyond knowledge transmission. It should empower students to select, interpret, and apply knowledge in ways that strengthen higher-order cognitive functions such as planning, creativity, reflection, and problem-solving.46,47
Category 2: Paradigmatic Paralysis
Participants identified a significant level of paradigmatic paralysis within institutions—understood as rigid belief systems regarded as unquestionable truths, often invoked to resist new ideas. These entrenched mental models obstruct the assimilation of emerging knowledge, hinder change, and delay efforts to integrate nanotechnology into medical education.48 To address this, institutions must adopt new paradigms based on empowerment, belonging, and intrinsic motivation. These values can drive risk-taking and innovation in research and resource management. Developing mechanisms for students to acquire skills related to nanotechnological advancement is essential.49 One strategy to overcome resistance is to introduce incremental change—“doing something different every day”—thus embedding innovation within the culture of medical education. Organizational processes must also evolve to support research, collaboration, and technology implementation, while enhancing adaptability, teamwork, and responsiveness to environmental and technological needs.
Subcategory: Resistance to Change
Resistance to change, often expressed as discomfort or hesitancy in adopting new methods or technologies, is a common phenomenon in academic institutions. Despite nanotechnology’s relevance and potential, some faculty prefer to remain within the bounds of familiar content. This reluctance may limit the inclusion of innovative material such as nanoscience in medical curricula.
As dynamic organizations, educational institutions must anticipate and manage resistance to change. Effective strategies include identifying institutional incentives and creating pathways for professional development. Successful curricular innovation depends on the motivation and engagement of faculty and staff—a responsibility that lies with institutional leadership.50 To overcome resistance, broad participation across all organizational levels is necessary.51 In addition, some educators question the relevance of nanoscience to medical training, asserting that there is no space for such content within an already saturated curriculum.45
Category 3: Structure and Reassurance of the Health System
This category emphasizes the potential benefits of nanotechnology for patients, healthcare providers, and health systems. These include improved medication management, time efficiency, more rational therapeutic decisions, and cost containment. The approach aims to enhance access, quality, and outcomes in care delivery. However, participants acknowledged that current political and regulatory dynamics, such as changes to health insurance systems, may hinder the development and implementation of improved diagnostic and therapeutic technologies.52
Category 4: Curriculum Articulation in Practice
Participants stressed the importance of aligning nanotechnology instruction with clinical practice. They highlighted the role of technological resources in training and the need for curricular coherence in practical settings. This is aligned with the ongoing MEDICUS curricular reform,32 and frameworks such as Entrustable Professional Activities (EPAs), which enable competency-based evaluations in workplace contexts. The use of instructional models like 4C/ID promotes logical and structured progression in knowledge and skills acquisition.
Teaching proposals for incorporating nanotechnology into medical and postgraduate training must be dynamic, flexible, and participatory. These approaches not only support innovation and research but also contribute to closing the implementation gap in nanoeducation.
Category 5: Approval of the Nanotechnology System
Medicine is undergoing a paradigmatic shift toward personalization, supported by nanotechnology and other converging technologies. Advances such as electrochemical nanobiosensors enable real-time monitoring of biomarkers at the molecular level, facilitating individualized health assessments.53
Smart diagnostics are central to the development of Healthcare 4.0, encompassing big data analytics, IoT, machine learning, and mobile health technologies. These systems promise greater efficiency and accessibility but face challenges related to scalability, cost, and integration with existing infrastructures.54
Implementing these technologies on a large scale requires strategic planning and cost-benefit analyses. Precision medicine, supported by nanotechnology, has the potential to reduce clinical trial costs, patient risk, and timelines. However, systemic adoption hinges on demonstrating clear clinical and economic advantages.
Category 6: Influence of Industry
Participants noted that the commercialization of nanotechnology products outpaces the educational preparation of healthcare professionals, complicating decision-making regarding their use. This reflects a disconnect between innovation supply and clinical demand. There is a need for structured educational content that prepares students and practitioners to critically evaluate products, understand their mechanisms, and apply them responsibly.
Category 7: Conflict of Interest
The integration of nanotechnology in healthcare introduces ethical complexities related to data ownership, surveillance, and industry influence. As technologies enable real-time biomedical data generation and analysis, it is essential to ensure transparency and protect patient rights. Educational efforts must emphasize the importance of ethical literacy and conflict-of-interest management. Precision and translational medicine are at the forefront of this shift, converging multiple disciplines to accelerate innovation. Collaboration among clinicians, scientists, engineers, epidemiologists, and regulators is critical to ensuring that technological advances benefit both individual and public health.
Category 8: Critical Judgment
Participants stressed that critical judgment is indispensable in the implementation of nanotechnology. Healthcare professionals must be equipped to analyze and apply basic scientific concepts to assess the risks, uncertainties, and societal implications of emerging technologies. This includes scrutinizing innovations through ethical, clinical, and contextual lenses to support safe, effective, and socially responsible healthcare delivery.
In the context study, incorporating nanotechnology into medical education is essential for equipping healthcare professionals with the skills and knowledge needed to navigate the rapidly evolving field of nanomedicine. By focusing on foundational principles, practical applications, and interdisciplinary training, medical education can prepare the next generation of healthcare professionals to harness the full potential of nanotechnology to improve patient outcomes and address global health challenges. However, current educational offerings are often inadequate, highlighting the necessity for standardized, high-quality training to ensure future professionals are well-prepared in this evolving field.3
Based on the emerging categories of this study, an explicit link has been established between each category and its potential curricular implications, highlighting how the elements prioritized by experts can guide the design of content, methodologies, and strategies for medical training in nanotechnology. This study provides a novel perspective by identifying, through expert consensus, the critical factors that influence the integration of nanotechnology into medical specialty programs, a topic still underexplored in the literature.
The combination of the Nominal Group Technique (NGT) with thematic analysis not only allowed for the prioritization of key ideas but also revealed practical connections between identified challenges and opportunities for curricular improvement. This approach reinforces the applicability of the results by providing concrete evidence that can be used by decision-makers and curriculum designers to promote the effective inclusion of nanotechnology in specialized medical training.
In this sense, the integration of nanotechnology in health science programs has been addressed through similar participatory methodologies, such as focus groups and expert panels, also reporting institutional barriers, lack of specific teacher training and poor curricular articulation as common challenges, as evidenced in other studies.55–59
The incorporation of emerging content such as nanotechnology into medical curricula necessitates the development of flexible and collaborative curricular frameworks that respond to evolving scientific and societal demands. This aligns with the emergent thematic categories identified in our study. In this context, the engagement of subject-matter experts through structured consensus methodologies—particularly the Nominal Group Technique (NGT)—has proven to be an effective strategy for identifying curricular priorities and formulating educational proposals that are contextually relevant and responsive to local needs. Establishing this connection highlights the broader applicability of our findings within the global landscape of medical education. The convergence between the expert-prioritized factors in our study and those reported in other international educational settings reinforces the validity and robustness of our methodological approach, positioning our results as a meaningful contribution to the ongoing international discourse on the integration of nanotechnology in medical training.
Limitations
This study was conducted at a single university center in Colombia, which may limit the generalizability of the conclusions. However, the number of participating residents and the results found in the literature allow the results to be extrapolated to other contexts. However, similar multicenter studies with different educational conditions should be conducted.
Conclusions
This study presents preliminary insights based on the opinions of a small group of 12 medical residents from a single university in Colombia. We recognize that these findings are context-specific and exploratory, and therefore should not be generalized without further research. Despite these limitations, the growing importance of nanotechnology as a transformative scientific and industrial frontier—often described as the next “industrial revolution”—makes it critical to establish clear educational objectives to foster success in research, development, and societal engagement. Immediate action is required to integrate nanotechnology education, as delays could hinder scientific progress by limiting the number of qualified researchers and informed consumers. It is essential to develop policies that support new standards, curricula, teacher training, and informal education related to nanoscale science. Moreover, designing interdisciplinary courses and medical programs that integrate nanotechnology is vital. The field faces several educational challenges, including the need for learning standards, curricular materials, and teacher training in nanoeducation, as well as the expansion of informal science education. The healthcare professionals must engage in lifelong learning through continuing education and professional development programs, particularly in nanoscience, to ensure they can critically assess and implement nanotechnology in their medical practice.
To translate these imperatives into practice, we propose the following actionable recommendations:
- Curriculum Development: Medical schools should form interdisciplinary committees, including nanotechnology researchers, medical educators, and clinicians, to design courses that integrate nanoscale science principles with clinical applications, such as targeted drug delivery and diagnostics. These courses should be piloted within 2–3 years, with outcomes evaluated through student performance metrics, such as competency in nanotechnology applications.
- Educator Training Programs: Universities and professional organizations should establish certified training programs for medical educators, focusing on nanotechnology pedagogy. These programs should include workshops, online modules, and hands-on laboratory sessions to build expertise in teaching nanoscale science. Implementation could begin within 1–2 years through partnerships with nanotechnology research centers.
- Policy and Resource Allocation: Policymakers should allocate funding for nanoeducation initiatives, including curriculum development, teacher training, and informal science education programs. National medical education bodies should update accreditation standards to include nanotechnology literacy as a core competency, with guidelines developed within 3–5 years to ensure consistency across institutions.
- Informal Education Expansion: Informal science education platforms, such as science museums, public lectures, and online courses, should be leveraged to increase public and professional awareness of nanotechnology’s medical applications. Collaborative initiatives with educational outreach programs could be launched within 1–2 years to enhance accessibility.
- Lifelong Learning Infrastructure: Continuing education programs for healthcare professionals should incorporate nanotechnology-focused modules, offered through online platforms, professional conferences, and hospital-based training. These modules should emphasize critical evaluation of nanotechnology’s clinical utility, ethical considerations, and safety protocols, with regular updates to reflect emerging advancements.
The proposed recommendations are designed to be scalable and adaptable to diverse medical schools and regions. In high-resource settings, such as urban academic medical centers, institutions can invest in advanced laboratory facilities and direct partnerships with nanotechnology industries to enrich experiential learning. Conversely, in low- and middle-income countries or rural medical schools, open-access educational resources, virtual training platforms, and regional collaborations can mitigate resource constraints. For example, global initiatives, such as those supported by the World Health Organization or international nanotechnology consortia, can provide shared curricula and training materials to standardize nanoeducation across regions. Additionally, the modular nature of the proposed courses allows institutions to prioritize nanotechnology applications relevant to local healthcare needs, such as point-of-care diagnostics in resource-limited settings or personalized medicine in advanced healthcare systems. To ensure successful extrapolation, medical schools should conduct needs assessments to tailor implementation strategies to their specific infrastructure, faculty expertise, and student demographics. Pilot programs can be evaluated using standardized metrics (eg, technological literacy, clinical application skills) to facilitate knowledge sharing and best practices across institutions and regions.
By adopting these steps, medical education can prepare healthcare professionals to critically assess and implement nanotechnology, fostering innovation in research and clinical practice. These reforms address the educational challenges of nanoscale science, including the development of learning standards, curricular materials, and teacher training, while ensuring adaptability to diverse global contexts. Ultimately, integrating nanotechnology into medical curricula will position future physicians to leverage its potential for improved patient outcomes worldwide.
Finally, the incorporation of nanotechnology content into the medical curriculum is not only relevant but also strategic for preparing future professionals for the critical and interdisciplinary analysis of new technological tools, including those based on AI, which is advancing at a rapid pace. Therefore, the integration of nanotechnology and artificial intelligence (AI) into the medical curriculum constitutes an urgent and strategic necessity for the training of health professionals capable of facing the technological challenges of the 21st century. Nanotechnology, by enabling the manipulation of matter at the atomic and molecular scale, opens new frontiers in early diagnosis, targeted drug delivery, and personalized medicine. Simultaneously, AI provides advanced tools for the massive analysis of clinical data, complex pattern recognition, and assisted clinical decision-making. The convergence of these technologies not only transforms the healthcare landscape but also demands a curricular approach that promotes critical analysis, interdisciplinarity, and technological literacy from the earliest stages of medical training. Including this content in curriculum is essential to training future physicians in the ethical, effective, and safe use of these disruptive tools, benefiting from more precise, predictive, and personalized medicine.
InstitutionalReview Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Research Ethics Committee of Universidad de La Sabana (protocol 01 18 May 2021) due to the participation of the residents in the NGT.
Informed Consent Statement
Written informed consent has been obtained from all residents involved in the NGT.
Author Contributions
Conceptualization, R.-H.B., and J.-C.G.; methodology, R.-H.B., J.-C.G., M.M.D.-L., and J.-F-G.-R.; formal analysis, R.-H.B., J.-C.G., M.M.D.-L., and J.-F-G.-R.; investigation, R.-H.B., J.-C.G., M.M.D.-L., and J.-F-G.-R.; resources, R.-H.B., and J.-C.G; data curation, R.-H.B., J.-C.G., M.M.D.-L.; writing—original draft preparation, R.-H.B., J.-C.G., M.M.D.-L.; writing—review and editing, R.-H.B.; visualization, R.-H.B; supervision, R.-H.B., and J.-C.G.; project administration, R.-H.B; funding acquisition, R.-H.B., and J.-C.G.
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Acknowledgments
The authors would like to acknowledge the enormous support of the Universidad de La Sabana. This manuscript was previously uploaded as a preprint on Preprints.org (https://www.preprints.org/manuscript/202409.2439/v1.
Funding
This research was funded by Universidad de La Sabana MED-303-2021.
Disclosure
The authors declare no conflicts of interest.
References
1. National Nanotechnology Initiative. What is so special about “nano”? 2023. https://www.nano.gov/about-nanotechnology/what-is-so-special-about-nano.
2. Staggers N, McCasky T, Brazelton N, Kennedy R. Nanotechnology: the coming revolution and its implications for consumers, clinicians, and informatics. Nurs Outlook. 2008;56(5):268–274. doi:10.1016/j.outlook.2008.06.004
3. Huertas JD, Fuentes YV, Garcia JC, Bustos RH. The role of education in nanomedicine as a current need for academic programs related to the healthcare field: a scoping review. Adv Med Educ Pract. 2024;15:65–74. doi:10.2147/AMEP.S431359
4. Nasser JS, Chung KC. Recommendations for the reform of medical education in China: a SWOT analysis. Health Policy Open. 2020;1:100018. doi:10.1016/j.hpopen.2020.100018
5. Sweeney AE. Nanomedicine concepts in the general medical curriculum: initiating a discussion. Int J Nanomed. 2015;10:7319–7331. doi:10.2147/IJN.S96480
6. Alfonso MT, García M. The social accountability of medical schools. An urgent requirement to adapt to the needs of the population. Dialnet. 2021;22(2):99–105.
7. Malik S, Muhammad K, Waheed Y. Emerging applications of nanotechnology in healthcare and medicine. Molecules. 2023;28(18):6624. doi:10.3390/molecules28186624
8. Colombo S. Chapter 4 - Applications of artificial intelligence in drug delivery and pharmaceutical development. In: Adam B, editor. Artificial Intelligence in Healthcare. Academic Press; 2020:85–116.
9. Nance E. Careers in nanomedicine and drug delivery. Adv Drug Deliv Rev. 2019;144:180–189. doi:10.1016/j.addr.2019.06.009
10. Singh A, Amiji MM. Application of nanotechnology in medical diagnosis and imaging. Curr Opin Biotechnol. 2022;74:241–246.
11. Ho D, Quake SR, McCabe ERB, et al. Enabling technologies for personalized and precision medicine. Trends Biotechnol. 2020;38(5):497–518. doi:10.1016/j.tibtech.2019.12.021
12. Mele C. Nanotechnology in pediatrics: science fiction or reality? J Pediatr Nurs. 2011;26(4):379–382. doi:10.1016/j.pedn.2011.04.028
13. Das Neves J. Nanotechnology inclusion in pharmaceutical sciences education in portugal. Am J Pharm Educ. 2018;82(9):6403. doi:10.5688/ajpe6403
14. Friedman A, Nasir A. Nanotechnology and dermatology education in the United States: data from a pilot survey. J Drugs Dermatol. 2011;10(9):1037–1041.
15. Gómez López A. Nanomedicina y su impacto en la práctica médica. Repertorio de Medicina y Cirugía. 2017;26(3):129–130. doi:10.1016/j.reper.2017.06.003
16. Sunshine JC, Paller AS. Which nanobasics should be taught in medical schools? AMA J Ethics. 2019;21(4):E337–346.
17. Alghamdi MA, Fallica AN, Virzì N, Kesharwani P, Pittalà V, Greish K. The promise of nanotechnology in personalized medicine. J Pers Med. 2022;12(5):673. doi:10.3390/jpm12050673
18. Vélez J, Vélez J. The eminent need for an academic program in universities to teach nanomedicine. Int J Nanomed. 2011;6:1733–1738. doi:10.2147/IJN.S21133
19. Alardawe A. Nanotechnology practices and cost restructure for effective cost management under industry 4.0 based manufacturing systems. TEM J. 2022;1193–1199.
20. Muthulingam D, Bia J, Madden LM, Farnum SO, Barry DT, Altice FL. Using nominal group technique to identify barriers, facilitators, and preferences among patients seeking treatment for opioid use disorder: a needs assessment for decision making support. J Subst Abuse Treat. 2019;100:18–28. doi:10.1016/j.jsat.2019.01.019
21. Olsen J. The nominal group technique (NGT) as a tool for facilitating pan-disability focus groups and as a new method for quantifying changes in qualitative data. Int J Qual Methods. 2019;18:1609406919866049. doi:10.1177/1609406919866049
22. Wiggins ST, Colby S, Moret L, et al. A modified nominal group technique (mNGT) - finding priorities in research. Am J Health Behav. 2020;44(3):345–352. doi:10.5993/AJHB.44.3.7
23. Nel C, Wolvaardt JE, Toit PD. Using a nominal group technique to inform a curriculum of a short learning programme for peer mentor training in a health sciences context. Educ Health. 2023;36(3):94–103. doi:10.4103/efh.efh_225_23
24. Humphrey-Murto S, Varpio L, Gonsalves C, Wood TJ. Using consensus group methods such as delphi and nominal group in medical education research*. Med Teach. 2017;39(1):14–19. doi:10.1080/0142159X.2017.1245856
25. Aarnoutse RE, Schapiro JM, Boucher CA, Hekster YA, DMJD B. Therapeutic drug monitoring. Drugs. 2003;63(8):741–753. doi:10.2165/00003495-200363080-00002
26. McMillan SS, Kelly F, Sav A, et al. Using the Nominal Group Technique: how to analyse across multiple groups. Health Serv Outcomes Res Methodol. 2014;14(3):92–108. doi:10.1007/s10742-014-0121-1
27. Sav A, McMillan SS, Kelly F, et al. The ideal healthcare: priorities of people with chronic conditions and their carers. BMC Health Serv Res. 2015;15(1):551. doi:10.1186/s12913-015-1215-3
28. Clark JP. How to Peer Review a Qualitative Manuscript. Peer Review in Health Sciences.
29. Jones MG, Blonder R, Gardner GE, Albe V, Falvo M, Chevrier J. Nanotechnology and nanoscale science: educational challenges. Int J Sci Educat. 2013;35(9):1490–1512. doi:10.1080/09500693.2013.771828
30. Haleem A, Javaid M, Singh RP, Rab S, Suman R. Applications of nanotechnology in medical field: a brief review. Global Health J. 2023;7(2):70–77. doi:10.1016/j.glohj.2023.02.008
31. Dorouka P, Kalogiannakis M, Blonder R. Tablets and apps for promoting nanoliteracy in early childhood education: results from an experimental study. J Sci Educ Technol. 2024;33(6):910–927. doi:10.1007/s10956-024-10132-w
32. Universidad de La Sabana. Modelo Académico de MEDICUS. 2024; https://www.unisabana.edu.co/programas/carreras/facultad-de-medicina/medicina/modelo-academico-de-medicus/.
33. Shariati K, Peikani S, Karimi Moonaghi H, Ghazanfarpour M. Application of spiral programming model in medical education: a review. Med Educ Bulletin. 2021;2(3):233–241.
34. Sakhnini S, Blonder R. Essential concepts of nanoscale science and technology for high school students based on a delphi study by the expert community. Int J Sci Educat. 2015;37(11):1699–738.
35. Kouz K, Eisenbarth S, Bergholz A, Mohr S. Presentation and evaluation of the teaching concept “enhance” for basic sciences in medical education. PLoS One. 2020;15(9):e0239928. doi:10.1371/journal.pone.0239928
36. Spencer AL, Brosenitsch T, Levine AS, Kanter SL. Back to the basic sciences: an innovative approach to teaching senior medical students how best to integrate basic science and clinical medicine. Acad Med. 2008;83(7):662–669. doi:10.1097/ACM.0b013e318178356b
37. Woods NN, Neville AJ, Levinson AJ, Howey EH, Oczkowski WJ, Norman GR. The value of basic science in clinical diagnosis. Acad Med. 2006;81(10 Suppl):S124–127. doi:10.1097/00001888-200610001-00031
38. Basma El Z, Ali E, Mohanad D, Ahmed Al J, Ghassan J. Perspective Chapter: Nano and Society y5.0 – Advancing the Human-Centric Revolution. Industry 4.0 Transformation Towards Industry 5.0 Paradigm. Rijeka: IntechOpen; 2024. Ch. 5.
39. Rambaran T, Schirhagl R. Nanotechnology from lab to industry – a look at current trends. Nanoscale Adv. 2022;4(18):3664–3675. doi:10.1039/D2NA00439A
40. Bosetti R, Jones SL. Cost–effectiveness of nanomedicine: estimating the real size of nano-costs. Nanomedicine. 2019;14(11):1367–1370. doi:10.2217/nnm-2019-0130
41. Pokrajac L, Abbas A, Chrzanowski W, et al. Nanotechnology for a sustainable future: addressing global challenges with the international network4sustainable nanotechnology. ACS Nano. 2021;15(12):18608–18623. doi:10.1021/acsnano.1c10919
42. Ól HS, Vásquez Ochoa Y. Ciencias y tecnologías convergentes (NBCI): fundamentación teórica de la Maestría en Bioingeniería y Nanotecnología. Ingeciencia. 2021;4:120–123.
43. Urquilla A. Impacto de la nanotecnología como revolución industrial a nivel mundial. Realidad y Reflexión. 2019;49(49):66–78. doi:10.5377/ryr.v49i49.8063
44. Aguirre Echavarría FJ, López Gómez M, Durango Yepes CM. Desarrollo de las capacidades nanotecnológicas en las Instituciones de Educación Superior en Antioquia-Colombia. Ciencia y Academia. 2020;2020(1):22–46. doi:10.21501/2744838X.3722
45. Huang ZW, Huang YQ. Research on nanosciences involvement in pharmaceutical education should be reinforced. World J Exp Med. 2023;13(5):156–160. doi:10.5493/wjem.v13.i5.156
46. Azorín C, Fullan M. Leading new, deeper forms of collaborative cultures: questions and pathways. J Educ Change. 2022;23(1):131–143. doi:10.1007/s10833-021-09448-w
47. Schmid JM, Veith JM, Truong MH, et al. Nanoscience and technology in secondary education: a systematic literature review. EURASIA J Math Sci Technol Educ. 2023;19(12):em2361. doi:10.29333/ejmste/13834
48. Ling L. Methods and paradigms in education research. Methods Paradigms Educ Res. 2017;19–41.
49. Vivekananth P. Nanolearning: a new paradigm shift in teaching and learning. Inter J Enginee Manage Res. 2022;12(1):112–114. doi:10.31033/ijemr.12.1.14
50. McBride K, null N, null N, null N. Leadership in higher education: handling faculty resistance to technology through strategic planning. Acad Leadership. 2010. doi:10.58809/JMKD5552
51. Córica JL. Resistencia docente al cambio: caracterización y estrategias para un problema no resuelto. RIED-Revista Iberoamericana de Educación a Distancia. 2020;23(2):255–272. doi:10.5944/ried.23.2.26578
52. Sandow J Pharmacodynamic Evaluation: Endocrinology. In: Vogel HG, Maas J Gebauer A, editors. Drug Discovery and Evaluation: Methods in Clinical Pharmacology. Berlin, Heidelberg: Springer; 2011. doi:10.1007/978-3-540-89891-7_35
53. Garzón V, Pinacho DG, Bustos R-H, Garzón G, Bustamante SJB. Optical biosensors for therapeutic drug monitoring. Biosensors. 2019;9(4):132. doi:10.3390/bios9040132
54. Orozco J. Nanociencia, nanotecnología y tecnologías disruptivas en el contexto de la medicina de precisión. Revista de la Academia Colombiana de Ciencias Exactas Físicas y Naturales. 2023;47(183):221–241. doi:10.18257/raccefyn.1895
55. Åberg O, Cheung O, Xu C, Varghese O, Ferraz N, Mihranyan A. Educational challenges for teaching nanotechnology: part 1. In: Global and Local Perspectives for Teaching Nanotechnology. Uppsala: Uppsala Universitet; 2023. Available from: https://urn.kb.se/resolve?urn=urn:nbn:se:uu:diva-504580.
56. Barton AE, Borchard G, Wacker MG, et al. Need for expansion of pharmacy education globally for the growing field of nanomedicine. Pharmacy. 2022;10(1). doi:10.3390/pharmacy10010017.
57. Freire DT, Martins LA, Miranda JA, et al. Navigating the challenges of teaching nanotechnology to pharmacy students in a developing country. Curr Pharm Teach Learn. 2025;17(8):102372. doi:10.1016/j.cptl.2025.102372
58. Pnevmatikos D, Peikos G, Christodoulou P, Papadopoulou P. Nanoscience-nanotechnology education for all: promoting nano-literacy across educational levels. Emerg Soc Issues Targe Drug Delive. 2024;221–254.
59. Weissig V, Elbayoumi T, Flühmann B, Barton A. The growing field of nanomedicine and its relevance to pharmacy curricula. Am J Pharm Educ. 2021;85(8):8331. doi:10.5688/ajpe8331
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Role of Education in Nanomedicine as a Current Need for Academic Programs Related to the Healthcare Field: A Scoping Review
Huertas JD, Fuentes YV, Garcia JC, Bustos RH
Advances in Medical Education and Practice 2024, 15:65-74
Published Date: 27 January 2024