Back to Journals » Vascular Health and Risk Management » Volume 19
Unconventional Cardiovascular Risk Factors and Systematic Coronary Risk Estimation (SCORE) in the Lebanese Rural Population: The Forgotten Factors
Authors Gebara N ![]() , Abdel-Massih T, Sahakian JP, Sleilaty G, Bazzi M, Ashoush R, Jebara V, Habib J
, Abdel-Massih T, Sahakian JP, Sleilaty G, Bazzi M, Ashoush R, Jebara V, Habib J
Received 4 April 2023
Accepted for publication 20 July 2023
Published 7 August 2023 Volume 2023:19 Pages 507—517
DOI https://doi.org/10.2147/VHRM.S411864
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Nicole Gebara,1 Tony Abdel-Massih,2 Jean-Paul Sahakian,2 Ghassan Sleilaty,3 Mariam Bazzi,4 Ramzi Ashoush,3 Victor Jebara,3 Jad Habib1
1Department of Family Medicine, Faculty of Medicine, Saint Joseph University, Beirut, Lebanon; 2Department of Cardiology, Faculty of Medicine, Saint Joseph University, Beirut, Lebanon; 3Department of Cardiovascular and Thoracic Surgery, Faculty of Medicine, Saint Joseph University, Beirut, Lebanon; 4Higher Institute of Public Health, Faculty of Medicine, Saint Joseph University, Beirut, Lebanon
Correspondence: Nicole Gebara, Email [email protected]
Purpose: To evaluate the correlation between unconventional risk factors and the Systematic Coronary Risk Estimation (SCORE), and estimate the prevalence of conventional and unconventional cardiovascular (CV) risk factors in the rural Lebanese population in order to assess their CV risk.
Methods: This is a retrospective descriptive study conducted between November 2017 and June 2019 among the Lebanese rural population. The risk factors were analyzed from the files of the patients who presented for the CV disease screening days organized by a non governmental organization. The CV risk estimation tool is the SCORE. The classification of socio-economic level ranges from zero (low level) to 3 (high level).
Results: A total of 433 patients were included. The prevalence of hypertension, diabetes, dyslipidemia, smoking, and metabolic syndrome was 45.1%, 31.2%, 39.2%, 50% and 42.9% respectively. Only 13.6% of hypertensive patients and 6.7% of diabetics were controlled. A total of 0 or 1 point for the classification of socio-economic status was found in 62.6% of cases. A family history of CV diseases was present in 87.3% of participants. The SCORE was correlated with diabetes and metabolic syndrome (p = 0.000), without being correlated to socio-economic status (HR = − 0.104; p = 0.059) or to family history (p = 0.834).
Conclusion: The socio-economic status and the family history of CV disease must be evaluated in addition to the classical risk calculation of the SCORE to better pinpoint the actual risk of the targeted population. The risk factors are prevalent but poorly controlled, hence the need for a national effort to ensure better care for the rural Lebanese population.
Keywords: screening, cardiovascular disease, conventional risk factors, unconventional risk factors, SCORE, Lebanon
Introduction
The synergistic nature of cardiovascular risk factors (CVRF) is well-established.1 Therefore, there are tools used to calculate the risk of developing cardiovascular diseases (CVD), such as the Systematic Coronary Risk Estimation (SCORE) and the Pooled Cohort Equation (PCE).1,2
These tools only consider conventional risk factors (CRF) which include age, sex, arterial hypertension (HTN), diabetes, dyslipidemia, and smoking status. However, there are also unconventional risk factors (URF) that significantly increase the risk of CV pathologies.2,3 URF such as a family history of early CV diseases, metabolic syndrome, lifestyle factors (physical activity or sedentary behavior, nutrition), socio-economic status, ethnicity, and coronary calcium score can be added to these CRF.
The prevalence of CVRF varies depending on genetic profile, environmental factors, socio-economic status, and access to healthcare.4 In Lebanon, in 2016, CV mortality was estimated to account for 47% of all causes of death combined, and 8% of the population was identified as being at high risk of CV disease. However, only 58% of them were being monitored by healthcare providers.5
To the best of our knowledge, there are no studies conducted on the rural Lebanese population to assess their CV risk and estimate the prevalence of CVRF. This study aims to specifically target the following CRF and URF: age, sex, hypertension, diabetes, dyslipidemia, smoking status, metabolic syndrome, socio-economic status, and familial history of early CV diseases. Our objectives are to evaluate the epidemiology of these CVRFs, calculate the CV risk using the SCORE, and establish correlations between this risk and the CVRFs included in our study, particularly the unconventional risk factors.
Methods
Study Design and Data Collection
This is a retrospective descriptive study. Data were collected with oral consent from the records of patients who attended cardiovascular disease screening days organized by the Lebanese NGO “Heartbeat” between November 2017 and June 2019 (see Supplementary Material 1).
The cardiovascular risk estimation tool used in this study was the SCORE, which estimates the risk of developing fatal cardiovascular disease over a 10-year period. It takes into account the following risk factors: age, gender, smoking status, systolic blood pressure (SBP), and total cholesterol levels.6 Since the Lebanese population is considered to be at high cardiovascular risk,5 the calculation and classification models used in this study are those employed for high-risk European countries7 (see Table 1). Table 2 and Table 3 provide a summary of the criteria used to define the conventional risk factors (CRF) and the unconventional risk factors (URF) evaluated in this study.
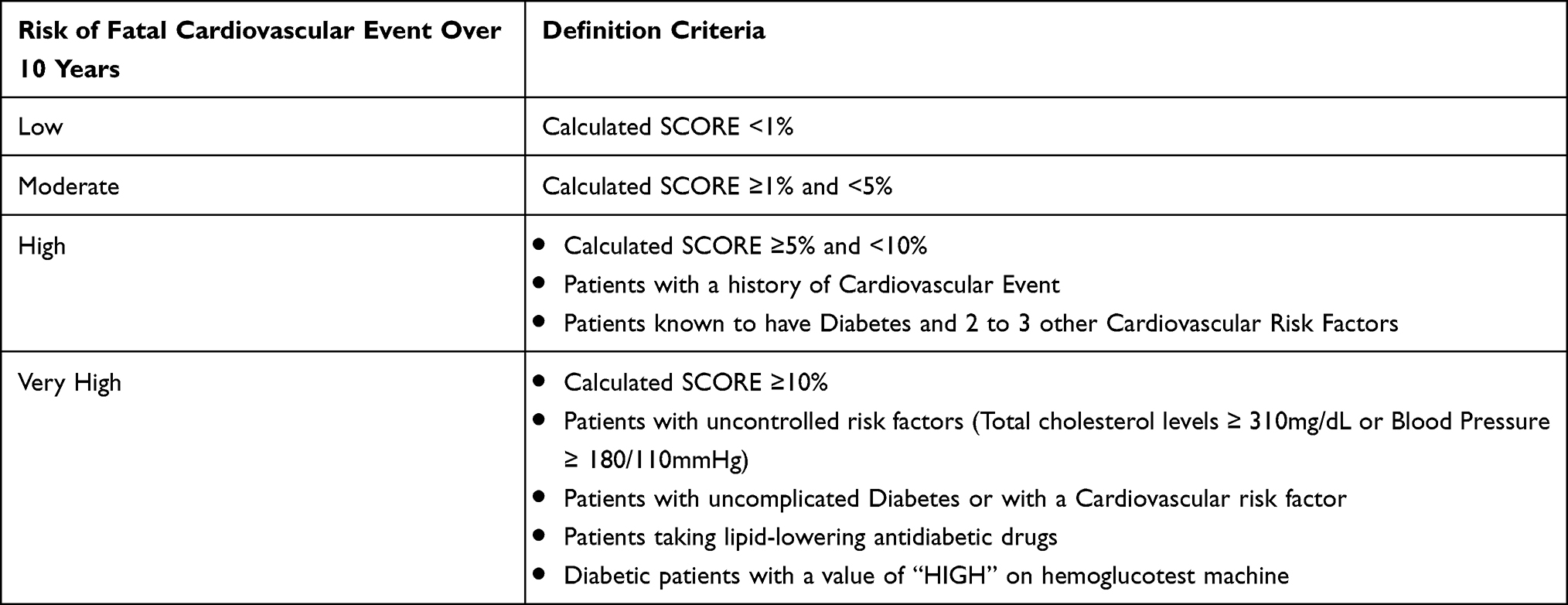 |
Table 1 Classification of Cardiovascular Risk According to the SCORE |
 |
Table 2 Criteria Used in This Study for Defining the Assessed Conventional and Unconventional Risk Factors |
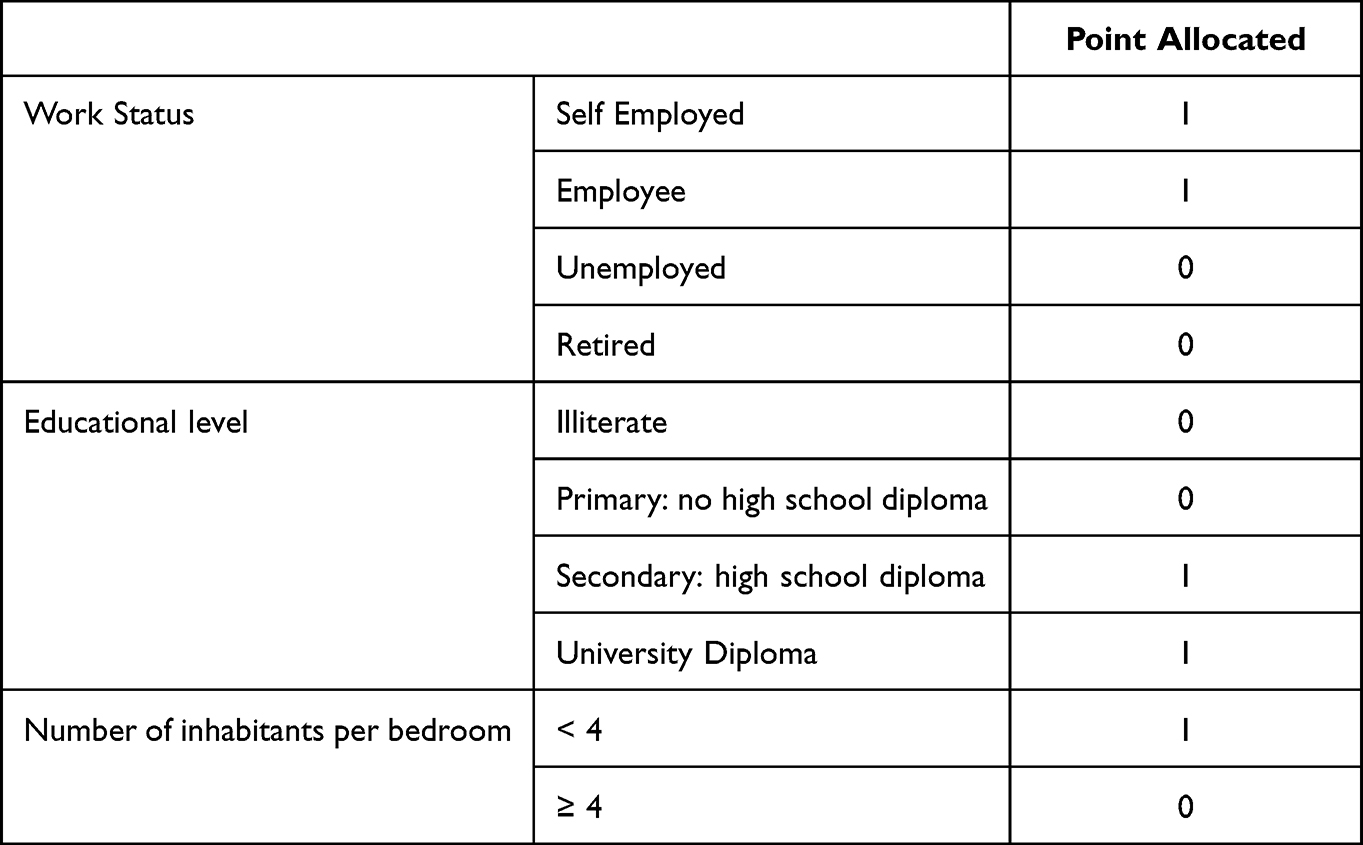 |
Table 3 Classification of the Socio-Economic Status of the Studied Population |
It should be noted that triglycerides and total cholesterol levels were only measured during three out of the five Heartbeat screening days. Therefore, the SCORE calculation was performed based on data from those three days only.
Patients’ Characteristics
We included patients who presented to the screening days, aged between 40 and 70 years old, and who gave their oral consent. Patients were excluded if they were non Lebanese or unable to give an oral consent.
Statistical Analysis
The handwritten data collected was manually computerized in May 2020 and analyzed using IBM-SPSS Statistics software, version 26.0 for Windows.
Qualitative data is represented as frequencies with their percentage corresponding and the 95% Confidence Interval (CI). Continuous data not deviating from normal distribution are expressed as mean ± standard deviation. Continuous data deviating from normal distribution and ordinal data are represented by median with its interquartile range 1 and 3 (Q1 and Q3). Spearman’s rank correlation coefficient was used to correlate the continuous and ordinal data. Numerical and categorical variables were compared using the Mann–Whitney U-test and the Kruskal–Wallis test.
Ethical Considerations
The authors assert that all procedures contributing to this work comply with the ethical principles established in the World Medical Association’s (WMA’s) Helsinki Declaration, as revised in 2013, and in the Council for International Organizations of Medical Sciences (CIOMS) International Ethical Guidelines, as revised in 2016, in collaboration with the World Health Organization (WHO). Verbal informed consent was obtained because this study is done in the rural population among which many cannot read or write. Two oral consent were obtained by two different persons: the first upon arrival at the screening center and the second, prior to filling the medical files. To ensure confidentiality, all data was anonymous. The verbal informed consent process was approved by the ethics committee of Saint-Joseph University of Beirut (File code: CEHDF 1546).
Results
A total of 433 patients were included in the data analysis (see Figure 1). The average age of the participants was 55 years, with a majority of women (N=249, 57.5%). Table 4 provides a summary of the socio-demographic characteristics of the studied population.
 |
Figure 1 Flowchart of the study population. |
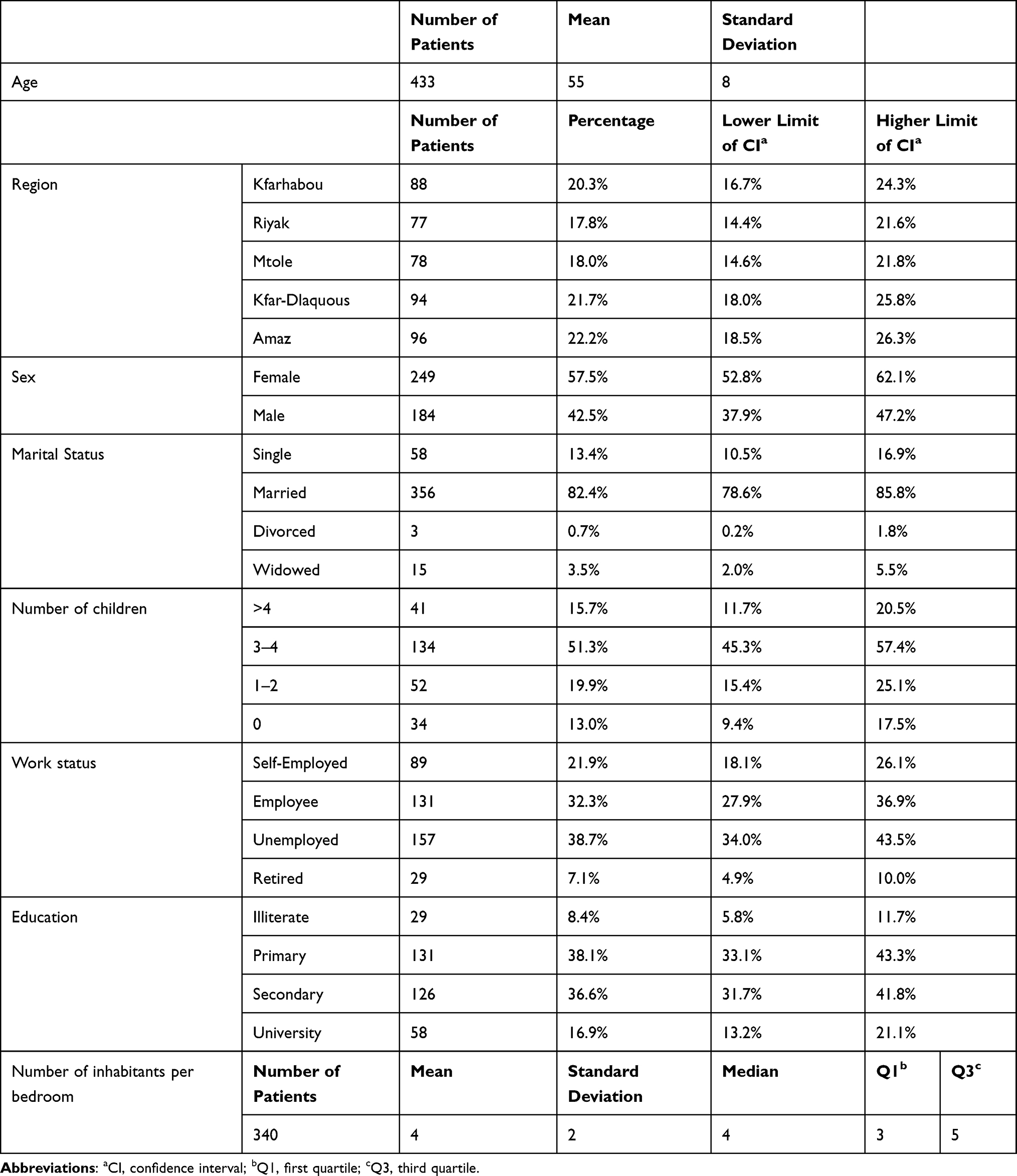 |
Table 4 Socio-Demographic Characteristics of the Studied Population |
In addition to age and sex, the analyzed CRF were hypertension, diabetes, dyslipidemia, and smoking status (see Table 5). In the general population, the mean systolic blood pressure (SBP) and diastolic blood pressure (DBP) were 138 mmHg and 85 mmHg, respectively. Out of the total patients, 123 were known to be hypertensive (29.5%), and 116 were receiving antihypertensive drug therapy (27.8%). The prevalence of hypertension was 66% (N=279), but only 13.6% of hypertensive patients, as per the protocol, had their blood pressure controlled (N=37). Diabetes was present in 31.2% of cases (N=131), and only 6.3% of diabetic patients, according to the protocol, had their diabetes controlled (N=8). The median levels of total cholesterol and triglycerides were 4.79 mmol/L (equivalent to 186.5 mg/dL) and 2.03 mmol/L (equivalent to 179.65 mg/dL), respectively. Based on our definition criteria, 103 patients were considered dyslipidemic (39.2%). Half of the patients were smokers (N=209, 50.0%). It is worth noting that 39 patients had previously experienced a cardiovascular event (9.4%).
 |
Table 5 Epidemiology of Conventional Risk Factors |
The URF studied were the metabolic syndrome, socio-economic status, and family history (see Table 6 and Table 7). The prevalence of metabolic syndrome was 42.9% (N=115). The classification of socio-economic status, defined by the composite score, resulted in 182 patients with 1 point (42%) and 89 patients with 0 points (20.6%). The majority of participants had a family history of cardiovascular disease in their parents, children, or siblings (N=365, 87.5%), and 364 had a family history in either parents or children only (87.3%).
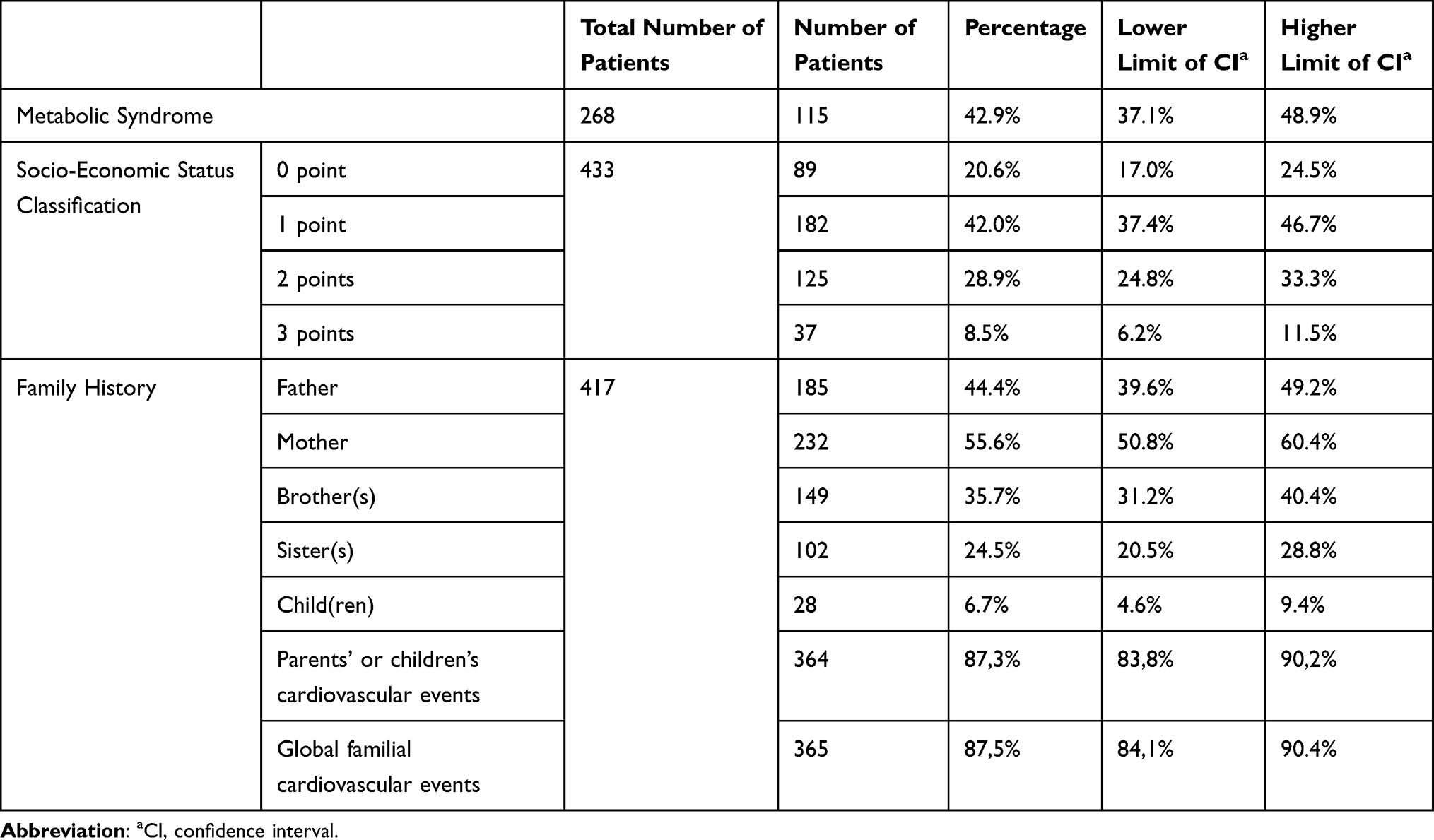 |
Table 6 Epidemiology of Unconventional Risk Factors |
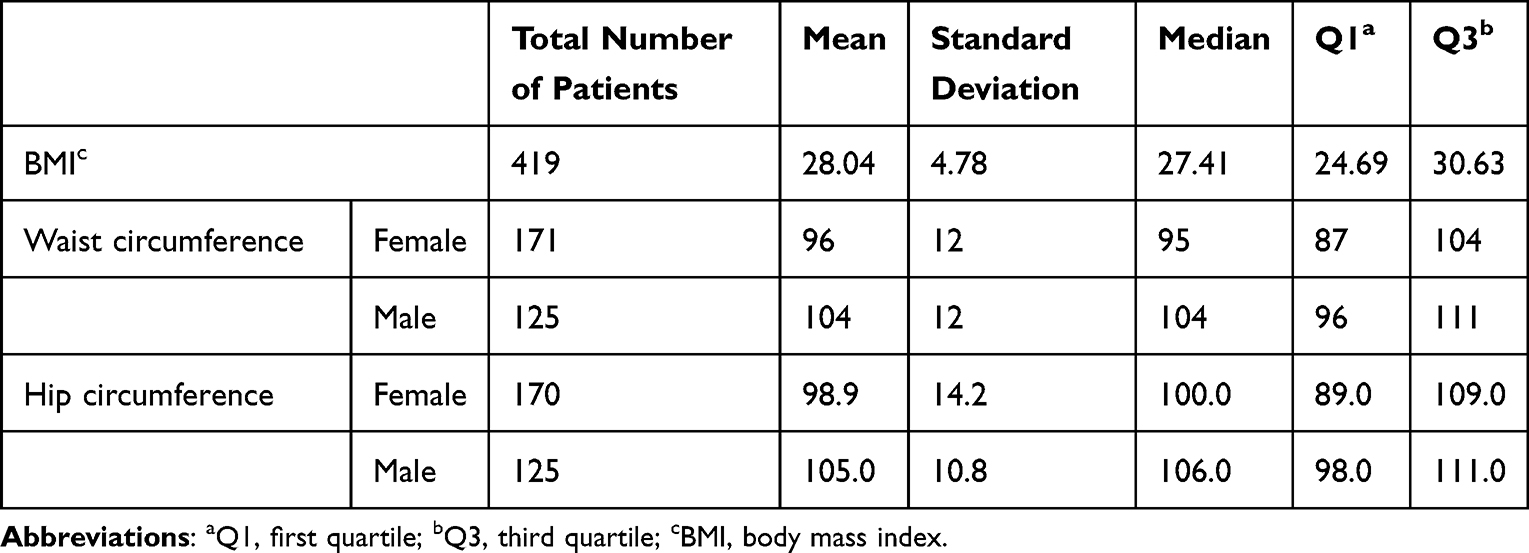 |
Table 7 Anthropometric Measurements |
In our studied population, 67.2% of participants (N=163) were classified as being at high or very high cardiovascular risk (22.4%) (see Table 8). Correlations were examined between the SCORE and risk factors that were not included in the risk calculation. Diabetes and metabolic syndrome showed a strong positive relationship with the SCORE (p=0.000). This positive relationship was also observed with body mass index (BMI) (correlation coefficient CC = 0.179; p = 0.005). Socio-economic status did not show a significant correlation with cardiovascular risk (CC = −0.104; p = 0.059), and neither did family history of parents and children (p = 0.834) or family history including siblings (p = 0.975) (see Table 9).
 |
Table 8 Cardiovascular Risk of the Rural Lebanese Population Studied |
 |
Table 9 Correlations Between Risk Factors and SCOREa |
Discussion
CV diseases are the leading cause of morbidity and mortality worldwide, including in Lebanon.3,8 Given the lack of recent data in Lebanon, our study not only establishes an epidemiological database but also provides a roadmap for implementing a primary and secondary prevention strategy.
The SCORE is a tool that assesses the risk of fatal CV events, unlike the PCE, which calculates the total number of events (both fatal and non-fatal). The inclusion of non-fatal events is complicated due to varying definitions and evolving diagnostic methods, leading to confounding factors. Additionally, recalibrating the calculation models for total events is challenging for validation in each population. Efforts are underway to develop specific tables for different regions worldwide.6 In the absence of such tables, the risk calculation model for fatal CV events used in this study is based on that of high-risk European countries.
In our population, 65.2% of subjects have a high or very high risk of experiencing a CV event. This significant risk aligns with observations from daily medical practice, although recent publications lack a clear assessment. The World Health Organization (WHO) data from 2002 classified Lebanon as a country with a low risk of CV mortality.9 However, data published in 2018 indicates a CV mortality prevalence of 47%.5 Unfortunately, the WHO has not updated the risk status of the Lebanese population since 2002.
The pathogenesis of CV diseases is multifactorial, but the SCORE only considers age, sex, tobacco use, total cholesterol levels, and blood pressure. These factors are inherently interconnected, which is why they are not included in the correlation analyses.
The percentage of patients who experienced non-fatal CV events is low (9.4%), but both CRF and URF are common in our population. Limiting the study population to individuals aged between 40 and 70 years may explain this observation, as CV risk factors develop early in life, while their complications manifest later. The prevalence of cardiovascular diseases significantly increases with age in both men and women. Although advanced age exposes individuals to risk factors for a longer period, age itself is a major independent risk factor for cardiovascular disease.10 It’s worth noting that women tend to develop cardiovascular diseases at an older age than men due to hormonal changes in postmenopausal women.11,12
The prevalence of hypertension, diabetes, dyslipidemia, and smoking in our study is higher than the rates reported in a study conducted in the suburbs of Beirut (36.4%, 12.8%, 24%, and 43.1%, respectively). This difference can be attributed to the fact that our study defined CV risk factors based on patient-reported information rather than adhering strictly to protocol guidelines.13
Hypertension is the most significant risk factor for cardiac events,14 and it is highly prevalent in the rural Lebanese population, with 66% of participants being hypertensive. However, only 13.6% of hypertensive patients have controlled blood pressure. These percentages differ from those reported by Matar et al (36.9% and 54%, respectively).15 Factors such as the white coat effect, blood pressure measurement techniques, and limited access to healthcare in rural areas may contribute to these variations. Blood pressure control remains a challenge, even in developed countries. For instance, the Health Study on the Environment, Biomonitoring, Physical Activity and Nutrition (ESTEBAN) conducted in metropolitan France estimated that 31.3% of the French population is hypertensive, of whom 50.0% are receiving antihypertensive drug therapy. Among hypertensive patients, only 24.3% have controlled blood pressure.16
Diabetes is also a major risk factor for CV events. In our population, the prevalence of diabetes is 31.2%, but only 6.3% of diabetic patients have their condition under control. However, a study published in 2019 reported that 30% of diabetics in Lebanon had their diabetes under control.17 Similar to hypertension, the lack of healthcare facilities, clinics, and physicians in rural areas may result in delayed diagnosis and inadequate management.
Dyslipidemia is present in 39.2% of participants. One noteworthy characteristic of the Lebanese population is the high prevalence of Familial Hypercholesterolemia, often referred to as the “Lebanese allele”. This can be attributed to the heterozygosity of the gene and the high rates of consanguinity within the Lebanese population, particularly in rural areas.8 Additionally, educational level is inversely correlated with the risk of dyslipidemia.18 However, the study was unable to calculate the percentage of patients with controlled dyslipidemia since LDL-cholesterol, which is used for control assessment, was not measured.
According to WHO data, 33% of Lebanese individuals are smokers. In the rural population, smoking is the second most prevalent CRF, with a prevalence of 50%. When compared to smoking rates among men and women in Jordan, Syria, and Palestine, Lebanon ranks second among men and first among women in smoking prevalence.19 Smoking in Lebanon is more common among individuals with low economic status or educational level, and it is more prevalent in rural areas. Another notable aspect of the Lebanese population is the high prevalence of water-pipe smoking.8
The concept of URF emerged more than 30 years ago20 and has gained importance due to advancements in research, diagnostics, and therapeutics. International recommendations emphasize the significance of considering URF without a specific decision-making algorithm.2,6 Metabolic syndrome is strongly associated with the occurrence of CV events and CV mortality.21 Its definition relies on several factors, including hypertension, diabetes, and hypertriglyceridemia, which explains its high prevalence and its correlation with the SCORE (as CRFs are correlated with the SCORE). Consequently, the CV risk associated with the metabolic syndrome is indirectly reflected in the SCORE calculation. The literature reports a metabolic syndrome prevalence of 20 to 30% in the general population.22
Socio-economic status does not show a correlation with the SCORE. However, in Lebanon, individuals with low income and low educational level have a higher prevalence of CV diseases, independent of CV risk factors.23 Therefore, socio-economic status should be considered as a risk factor independently of CV risk calculation.
Similarly, family history is not correlated with the SCORE. However, CV diseases have a significant genetic component, especially when there is a history of CV events in relatives.24 Given the high rates of consanguinity, family history plays a notable role in CV risk. While not directly correlated with CV risk calculation, family history should be considered as an additional risk factor.
The two main limitations of this study are selection bias and recall bias. The non-random sampling method used in the study introduces selection error, as the sample was chosen from five Lebanese rural regions without proportional representation based on population size per district or governorate. Due to political uncertainties and the COVID-19 pandemic, expanding the study to other governorates was postponed. To minimize recall bias, particularly regarding drug intake, the questionnaire specified therapeutic classes.
Conclusion
Our study showed that diabetes and metabolic syndrome are correlated to SCORE and therefore indirectly reflected by it. The socio-economic status and the family history, as for them, are not correlated with the SCORE and put the affected population at risk; therefore, they should be included in the overall patient assessment in addition to the risk calculation. Moreover, CRF and URF are prevalent in our population but are poorly managed in the majority of cases. A national effort is required to ensure better control of the risk factors in the Lebanese population in general, and in the rural population in particular. Primary prevention should be the pillar of the strategy of the Ministry of Health in order to reduce the costs of the inevitable complications of CV risk factors. The involvement of non-medical staff could contribute to improving care and better patient compliance.25
Disclosure
The authors report no conflicts of interest in this work.
References
1. Goff DC, Lloyd-Jones DM, Bennett G, et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association task force on practice guidelines. J Am Coll Cardiol. 2014;63(25 Pt B):2935–2959.
2. Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation. 2019;140(11):e596–e646. doi:10.1161/CIR.0000000000000678
3. Piepoli MF, Hoes AW, Agewall S, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: the sixth joint task force of the European Society of Cardiology and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of 10 societies and by invited experts) developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2016;37(29):2315–2381. doi:10.1093/eurheartj/ehw106
4. Levi F, Lucchini F, Negri E, La Vecchia C. Trends in mortality from cardiovascular and cerebrovascular diseases in Europe and other areas of the world. Heart. 2002;88(2):119–124. doi:10.1136/heart.88.2.119
5. World Health Organization Noncommunicable diseases country profiles; 2018. Available from: https://www.who.int/nmh/publications/ncd-profiles-2018/en/.
6. Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41(1):111–188. doi:10.1093/eurheartj/ehz455
7. Access HeartScore online; 2020. Available from: http://www.heartscore.org/en_GB/access.
8. Deek H, Newton P, Inglis S, et al. Heart health in Lebanon and considerations for addressing the burden of cardiovascular disease. Collegian. 2015;22(3):333–339. doi:10.1016/j.colegn.2014.04.004
9. World Health Organization. Prevention of cardiovascular disease. World Health Organization; 2020. Available from: https://www.who.int/cardiovascular_diseases/publications/Prevention_of_Cardiovascular_Disease/en/.
10. Kane AE, Howlett SE. Differences in cardiovascular aging in men and women. Adv Exp Med Biol. 2018;1065:389–411.
11. Möller-Leimkühler AM. Gender differences in cardiovascular disease and comorbid depression. Dialogues Clin Neurosci. 2007;9(1):71–83. doi:10.31887/DCNS.2007.9.1/ammoeller
12. Gender matters: heart disease risk in women. Harv Womens Health Watch. 2004;11(9):1–3.
13. Isma’eel HA, Almedawar MM, Breidy J, et al. Worsening of the cardiovascular profile in a developing country: the Greater Beirut area cardiovascular cohort. Glob Heart. 2018;13(4):275–283. doi:10.1016/j.gheart.2018.03.001
14. Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2224–2260. doi:10.1016/S0140-6736(12)61766-8
15. Matar D, Frangieh AH, Abouassi S, et al. Prevalence, awareness, treatment, and control of hypertension in Lebanon. J Clin Hypertens. 2015;17(5):381–388. doi:10.1111/jch.12485
16. Vallée A, Gabet A, Grave C, Sorbets E, Blacher J, Olié V. Patterns of hypertension management in France in 2015: the ESTEBAN survey. J Clin Hypertens. 2020;22(4):663–672. doi:10.1111/jch.13834
17. Ahmadieh H, Sawaya M-T, Azar ST. Management and control of type 2 diabetes mellitus in Lebanon: results from the International Diabetes Management Practices Study Wave 6. World J Diabetes. 2019;10(4):249–259. doi:10.4239/wjd.v10.i4.249
18. Wang C-J, Y-Q L, Wang L, et al. Development and evaluation of a simple and effective prediction approach for identifying those at high risk of dyslipidemia in rural adult residents. PLoS One. 2012;7(8):e43834. doi:10.1371/journal.pone.0043834
19. Abdulrahim S, Jawad M, El Bcheraoui C. Socioeconomic differences in smoking in Jordan, Lebanon, Syria, and Palestine: a cross-sectional analysis of national surveys. PLoS One. 2018;13(1):e0189829. doi:10.1371/journal.pone.0189829
20. Acevedo M, Tagle R, Simpfendorfer C. Non-traditional risk factors for atherosclerosis. Rev Med Chil. 2001;129(10):1212–1221. doi:10.4067/S0034-98872001001000016
21. Galassi A, Reynolds K, He J. Metabolic syndrome and risk of cardiovascular disease: a meta-analysis. Am J Med. 2006;119(10):812–819. doi:10.1016/j.amjmed.2006.02.031
22. Pucci G, Alcidi R, Tap L, et al. Sex- and gender-related prevalence, cardiovascular risk and therapeutic approach in metabolic syndrome: a review of the literature. Pharmacol Res. 2017;120:34–42.
23. Ramahi T, Khawaja M, Abu-Rmeileh N, Abdulrahim S. Socio-economic disparities in heart disease in the Republic of Lebanon: findings from a population-based study. Heart Asia. 2010;2(1):67–72. doi:10.1136/ha.2009.000851
24. Allport SA, Kikah N, Abu Saif N, Ekokobe F, Atem FD, Aalto-Setala K. Parental age of onset of cardiovascular disease as a predictor for offspring age of onset of cardiovascular disease. PLoS One. 2016;11(12):e0163334. doi:10.1371/journal.pone.0163334
25. Jafar TH, Gandhi M, de Silva HA, et al. A community- based intervention for managing hypertension in rural South Asia. N Engl J Med. 2020;382(8):717–726. doi:10.1056/NEJMoa1911965
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comorbid Psoriasis and Metabolic Syndrome: Clinical Implications and Optimal Management
De Brandt E, Hillary T
Psoriasis: Targets and Therapy 2022, 12:113-126
Published Date: 25 May 2022