Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Uncapped Metered-Dose Inhalers: A Risk for Foreign Body Aspiration. A Case Report and Review of the Literature
Authors Schürmann D ![]() , Saccomanno J
, Saccomanno J ![]() , Temmesfeld-Wollbrück B, Witzenrath M, Hübner RH
, Temmesfeld-Wollbrück B, Witzenrath M, Hübner RH
Received 17 February 2023
Accepted for publication 24 July 2023
Published 1 September 2023 Volume 2023:18 Pages 1931—1935
DOI https://doi.org/10.2147/COPD.S408845
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Dirk Schürmann, Jacopo Saccomanno, Bettina Temmesfeld-Wollbrück, Martin Witzenrath, Ralf-Harto Hübner
Department of Infectious Diseases, Respiratory Medicine and Critical Care, Charité - Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin, Berlin Institute of Health, Berlin, 10117, Germany
Correspondence: Dirk Schürmann, Department of Infectious Diseases, Respiratory Medicine and Critical Care, Charité - Universitätsmedizin Berlin, Berlin, 10117, Germany, Tel +49 30 450 653318 ; +49 1723871964, Email [email protected]
Abstract: The risk of foreign body aspiration associated with uncapped handheld metered-dose inhalers (MDIs) is underestimated. We report a case in which a plastic cable clip accidentally lodged in the mouthpiece of an uncapped pressurized MDI was aspirated during its use. A literature search revealed 16 other cases of foreign body aspiration associated with uncapped handheld inhalers, all but one of which were pressurized inhalers. Patients should be informed of the risk of foreign body aspiration associated with uncapped pocket inhalers. The use of an uncuffed armoured tracheal tube with a separate oxygen tubing during flexible bronchoscopy for foreign body removal ensures a safe airway. Foreign bodies that exceed the lumen size of the tracheal tube can be pulled to the distal opening with forceps and removed when the tube is withdrawn.
Plain Language Summary: Handheld pocket inhalers have significantly improved the treatment of patients with chronic obstructive pulmonary disease. We report a case in which a plastic cable clip accidentally lodged in the mouthpiece of an uncapped pressurized pocket inhaler was aspirated during its use. Depressing the plunger of the inhaler released the inhalant in a high-velocity spray, which was inhaled with a deep breath while simultaneously aspirating the plastic cable clip. The risk of foreign body aspiration associated with uncapped pressurized metered-dose inhalers is underestimated. Patients using pocket inhalers should be informed of the risk of foreign body aspiration with uncapped inhalers. Inhalers should always be kept capped except during use to prevent small objects from accidentally entering the mouthpiece. The cap of the inhaler mouthpiece should only be removed when the inhaler is used. Foreign bodies that have accidentally become lodged in the mouthpiece of an inhaler and aspirated into the lungs can usually be removed by specialists during a short outpatient procedure.
Keywords: foreign body aspiration, metered-dose inhaler, removal of aspirated foreign bodies, uncuffed armoured tracheal tube with separate oxygen tubing
Introduction
Handheld pocket inhalers have significantly improved the treatment of patients with chronic obstructive pulmonary disease (COPD) and bronchial asthma. Proper handling and storage are prerequisites for efficacy and safety. We report a case of foreign body aspiration associated with the use of an uncapped pressurized inhaler. To obtain data on the incidence and relevance of such a rare complication associated with uncapped pocket inhalers, we searched the medical literature for other reported cases.
Case Report
A 45-year old male presented to the emergency department of a tertiary university hospital complaining about worsening respiratory distress after using a pressurized metered-dose salbutamol inhaler one hour earlier. He reported a foreign body sensation below the larynx that started immediately after using the salbutamol inhaler. Since then, the respiratory distress worsened and he began to cough up bloody discolored sputum. Vital parameters were as follows: Blood pressure 131/67 mmHg, breathing rate 22/min, heart rate 103/min. Oxygen saturation was 92% on room air. Auscultation revealed wheezing breath sounds over both lungs. The patient´s history revealed COPD, with an as needed use of a salbutamol pressurized metered-dose inhaler, and chronic cigarette smoking. Chest x-ray revealed signs of emphysema and no foreign body.
Because of the intensive sensation of a foreign body in the patient´s throat, we performed an emergency flexible bronchoscopy under sedation with midazolam and propofol. A bronchoscopy-guided oral endotracheal intubation was performed using an uncuffed armoured Rüsch BronchoFlex tracheal tube (inner diameter 7.5 mm) with separate oxygen tubing.
On inspection of the bronchi, a plastic cable clip (Figure 1) was visualized occluding the terminal right main bronchus. The foreign body was grasped with a foreign body removal forceps and pulled up to the distal end of the endotracheal tube. Since the cable clip was larger than the tube´s inner diameter, forceps and tube were removed together. After awakening from sedation the patient reported complete resolution of his complaints and was discharged from the hospital two hours later.
 |
Figure 1 Plastic cable clip (left side: top, bottom, and side views) that accidentally got caught in the mouthpiece of the uncapped metered inhaler (right side) and was aspirated into the lung during inhalation. |
The patient reported to have had the plastic cable clip in the same trouser pocket as his uncapped salbutamol inhaler. The clip must have inadvertently been dislodged into the mouthpiece lumen of the inhaler (Figure 1) so that it was inhaled while using the salbutamol inhaler (Figure 2).
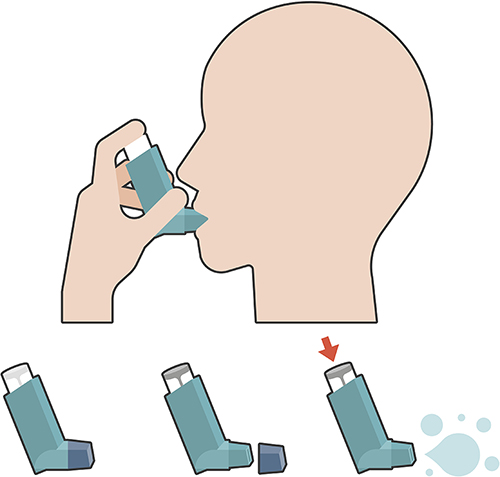 |
Figure 2 Use of a pressurized inhaler and aspiration of a plastic cable clip that was accidentally in the mouthpiece of the inhaler before use (Figure 1). The inhaler was stored in the pocket without the cap after it was lost. Depressing the inhaler plunger resulted in the release of the inhalent within high velocity spray, which was inhaled with a deep breath while simultaneously aspirating the plastic cable clip into the lung. |
Discussion
Aspiration of a foreign body hidden in an uncapped handheld inhaler carried in the pocket is an infrequent cause of foreign body aspiration. We performed a literature search in the PubMed database using the terms “foreign body aspiration” and “uncapped inhaler” through December 31, 2022. In addition we screened cited literature of cases reported and journal review articles dealing with foreign body aspiration.
Sixteen previous reports of foreign body aspiration in adults associated with uncapped pocket inhalers necessitating removal by bronchoscopy were retrieved.1–16 Objects aspirated included coins, lid of a make-up pencil, tablet, peanut, valve cap from a car tyre, cap of a nasal spray bottle, plastic cigarette filter, earring, LED light bulb, and plastic rawl plug with screw. With the exception of one case11 the inhalers were pressurized inhalers such as jet inhalers or pressurized metered-dose inhalers. This suggests that the risk could be considerable lower with other inhalers, such as dry powder inhalers or soft mist inhalers.
Notably, in seven out of 16 patients reported chest x-ray failed to demonstrate aspirated foreign bodies. Flexible or rigid bronchoscopy were used in six cases each, while the procedure for removal had not been reported in the remaining four cases.
Two other patients aspirated a capsule fragment and earwigs, respectively, but were eventually able to expectorate them.6,17 In a further case obstruction of the larynx by an inhaled coin hidden in an uncapped inhaler necessitated laryngoscopic removal.18
The actual number of cases of foreign body aspiration after use of uncapped pressurized metered inhalers is possibly underestimated. The United Kingdom (UK) Medicines and Healthcare products Regulatory Agency (MHRA) reported to have received 22 reports from accidental inhalation of the mouthpiece cover or loose objects trapped in the inhaler when stored by patients since 1987 and to be aware of 36 such cases reported outside of the UK.19 Reports included cases with pharyngeal injuries and aspirated foreign bodies requiring removal by bronchoscopy or surgery.
Flexible bronchoscopy can replace rigid bronchoscopy for removal of aspirated foreign bodies in adults in most cases.20 Use of a tracheal tube providing a secure airway has been recommended to perform interventional flexible bronchoscopies.21 An uncuffed armoured tracheal tube with separate oxygen tubing optimally fulfils this requirement. Foreign bodies extending the lumen size of the tracheal tube can be pulled up to the distal aperture and removed while withdrawing the tube.
Our case shows that foreign body aspiration may be associated with the use of uncapped metered-dose inhalers with objects accidentally placed in the mouthpiece. Patients using inhalers need to be informed about the risk of foreign body aspiration associated with uncapped handheld inhalers. Patient education should state that inhalers should always be kept capped except during use and checked for small objects in the mouthpiece before use. The cap of the inhaler mouthpiece should only be removed when the inhaler is used.
Data Sharing Statement
The patient file is not publicly accessible for legal reasons. All data obtained and analyzed are included in this article. Further inquiries can be directed to the corresponding author.
Ethical Review Board
Ethical approval is not required for this study in accordance with local guidelines.
Written Informed Consent for Publication: Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors have no conflicts of interest to declare for this work.
References
1. Wiesel JM, Bar ZG, Feinmesser R. Intrabronchial tablets - jet propelled. A case report. J Laryngol Otol. 1981;95(2):219–220. doi:10.1017/s0022215100090629
2. Hannan SE, Pratt DS, Hannan JM, Brienza LT. Foreign body aspiration associated with the use of an aerosol inhaler. Am Rev Respir. 1984;129:1025–1927. doi:10.1164/arrd.1984.129.6.1025
3. McGonagle M, Reams CL. The jet propelled dime. JAMA. 1984;251(11):1431. doi:10.1001/jama251.11.1431c
4. Bray WR, Francis PB, Jacobs J, Burris AS. Two-penny aspiration: unusual complication of a metered-dose inhaler. South Med J. 1985;78(12):1527. doi:10.1097/00007611-198512000-00039
5. Cuckow PM, English TA. Foreign body inhalation: a danger of metered dose inhalers. J R Coll Gen Pract. 1989;39(328):476.
6. Schultz CH, Hargarten SW, Babbitt J. Inhalation of a coin and a capsule from metered-dose inhalers. NEJM. 1991;325(6):431–432.
7. Taskar VS, Bradley BB, Moussali HM, Hilton AM. Foreign body aspiration: a hazard of metered dose inhalers. BMJ. 1993;306(6877):575–576. doi:10.1136/bmj.306.6877.575
8. O´Donnell JJ, Harte BH, Sharkey A. Importance of the inhaler mouthpiece cover. Intensive Care Med. 1995;21(8):698–700. doi:10.1007/BF01711554
9. Ricketti AJ, Cleri DJ, Muddassir S, Ramos-Bonner LS, Seelagy MM. Aspiration of the cap from a metered-dose inhaler. J Bronchol. 2007;14(3):204–206. doi:10.1097/LBR.0b013e318073d763
10. Elicora A, Liman ST, Asli T, Hosten T, Topcu S. Aspiration of a cigarette filter from a bronchodilator inhaler. Respir Care. 2013;58(4):e39–41. doi:10.4187/respcare.01898
11. Pelham A. An unusual mechanism of foreign body aspiration: a vignette from the emergency department. BMJ Case Rep. 2014;2014. doi:10.1136/bcr-2013-202248
12. McCowan Blake LK, Silverstone E, Yates DH. Treasure in the chest. BMJ Case Rep. 2015. doi:10.1136/bcr-2014-207398
13. Tsui J, Caughey G, Elicker BM, Lafemina M. Coin Aspiration: an underappreciated hazard of metered dose inhalers. Am J Respir Crit Care Med. 2016;193:A3289.
14. Gomez Hernandez MT, Novoa NM, Jimenez MF. Foreign body aspiration during inhaled bronchodilator administration. Arch Broncopneumol. 2017;53(5):272. doi:10.1016/j.arbr.2017.03.012
15. Rodrigo Garzon MR, Garcia JR, Diaz XA. Foreign body aspiration during inhaled bronchodilator administration. Arch Broncopneumol. 2018;54(3):173. doi:10.1016/j.arbres.2017.09.014
16. Arooj P, Plant R, Doddakula K, Plant BJ. Inhaler screw-up: a real world cystic fibrosis (CF) case. Pediatr Pulmonol. 2019;54(1):E1–E3. doi:10.1002/ppul.24158
17. Valori AM. Aspiration of earwigs from metered dose inhaler. BMJ. 1993;306(6880):797. doi:10.1136/bmj.306.6880.797-c
18. Dayan SH, Portugal LG, Walner DL, Berkowitz R. Laryngeal obstruction after inhalation of a penny from a metered-dose inhaler. Otolaryngol Head Neck Surg. 1999;120(4):548–551. doi:10.1053/hn.1999.v120.a81754
19. UK Medicines and Healthcare products Regulatory Agency (Internet). Other safety alerts. United Kingdom (GOV.UK). Pressurized metered dose inhalers (pMDI): risk of airway obstruction from aspiration of loose objects. Drug Safety Update. 2018;11(12):2.
20. Sehgal IS, Dhooria S, Ram B, et al. Foreign body inhalation in the adult population: experience of 25,998 bronchoscopies and systematic review of the literature. Respir Care. 2015;60(10):1438–1448. doi:10.4187/respcare.03976
21. Du Rand IA, Barber PV, Goldring J, et al.; on behalf of the British Thoracic Society Interventional Bronchoscopy Guideline Group. British Thoracic Society guideline for advanced diagnostic and therapeutic flexible bronchoscopy in adults. Thorax. 2011. doi:10.1136/thoraxjnl-2011-200713
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.