Back to Journals » International Journal of General Medicine » Volume 18
Ultrasound Radiomics and Peripheral Blood Indices Model for Predicting Pregnancy and Recurrence After TCRA in Intrauterine Adhesion
Authors Wang L, Liu Y, Huang M, Wang B, He C, Ai Q, Qin L
Received 28 July 2025
Accepted for publication 29 November 2025
Published 11 December 2025 Volume 2025:18 Pages 7483—7499
DOI https://doi.org/10.2147/IJGM.S551666
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Kenneth Adler
Lu Wang,1,* Ying Liu,1,* Meihua Huang,1 Bo Wang,1 Chuanyong He,1 Qinxiu Ai,2 Li Qin1
1Department of Obstetrics and Gynecology, Central Hospital of Enshi Tujia and Miao Autonomous Prefecture, Enshi Clinical College of Wuhan University, Enshi, People’s Republic of China; 2Department of Ultrasound Imaging, Central Hospital of Enshi Tujia and Miao Autonomous Prefecture, Enshi Clinical College of Wuhan University, Enshi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Li Qin, Email [email protected] Qinxiu Ai, Email [email protected]
Objective: The postoperative prognosis (ie pregnancy and recurrence) of patients with intrauterine adhesions(IUA) has always been a concern for women of childbearing age, and there is a lack of prevention and treatment strategies. This study aimed to develop an IUA pregnancy and recurrence (IUA-PR) prediction model to guide clinical decision-making.
Materials and Methods: A retrospective analysis was conducted on 387 patients diagnosed with IUA between January 2021 and December 2023. Radiomic features were extracted from ultrasound images using manually designed feature sets, and peripheral blood parameters were integrated with these radiomic features to construct a classification model. The least absolute shrinkage and selection operator (LASSO) combined with the Bayesian information criterion (BIC) was employed to identify nonzero-coefficient features from the radiomic dataset. The predictive efficacy of the developed model was systematically evaluated via the area under the receiver operating characteristic curve (AUC) and decision curve analysis (DCA).
Results: A total of five peripheral blood inflammatory indices and six ultrasound radiomic parameters were finally used to construct the IUA-PR prediction model. Among them, the nomogram constructed based on platelet/lymphocyte ratio(PLR), neutrophil/lymphocyte ratio(NLR), aggregate index of systemic inflammation(AISI), ultrasound radiomic score (Rad-score), and postoperative menstrual status showed an AUC of 0.886 for predicting pregnancy outcomes. Additionally, the recurrence prediction model established with systemic inflammatory response index(SIRI), systemic immune-inflammation index(SII), Rad-score, and postoperative menstrual status achieved an AUC of 0.720 in the testing set.
Conclusion: We have successfully developed the IUA-PR prediction model constructed based on peripheral blood inflammatory parameters and ultrasound radiomics. Renowned for its convenience and low cost, this model, particularly the generalized linear regression model, exhibits superior predictive performance in forecasting postoperative pregnancy and recurrence, thereby assisting patients in guiding their postoperative fertility decisions.
Keywords: intrauterine adhesions, transcervical resection of adhesion, pregnancy, recurrence, ultrasound radiomics, peripheral blood cell indices, machine learning
Introduction
Intrauterine adhesions(IUAs), also known as Asherman syndrome, are a benign disease characterized by damage to the basal layer of the endometrium and adhesions between the uterine walls, leading to partial or complete occlusion of the uterine cavity and cervical canal.1,2 At present, the incidence rate of female infertility is about 17.5%, and 8% of infertility is secondary to IUAs.3,4 Intrauterine procedures during pregnancy are one of the main causes of IUAs, but with the popularity of hysteroscopy and the increasing number of curettage surgeries, the detection and incidence of IUAs are also increasing every year.5,6
In clinical practice, transcervical resection of adhesion(TCRA) is the main method for IUAs.7 Although there are various postoperative adjuvant treatments, the efficacy is still unsatisfactory, mainly manifested as low pregnancy and high recurrence rate after surgery, which brings serious psychological burden to women of childbearing age.3,8 Given this situation, it is particularly crucial to identify high-risk factors for TCRA postoperative infertility and recurrence, and develop individualized comprehensive treatment plans for patients before surgery.
In numerous studies, inflammatory response is recognized to play an important role in IUAs, and typical inflammatory factors such as neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and lymphocyte-to-monocyte ratio (LMR) can effectively reflect the severity of inflammatory response in the body.9–11 Besides, surgery is a traumatic procedure that can interrupt the secretion of inflammatory factors and interfere with the regeneration and repair of the endometrium.12 In view of this, systemic inflammatory biomarkers may be referred to as postoperative evaluation indicators after IUAs surgery, but there has been a lack of reports specifically addressing inflammatory factors in patients with IUAs. Up to now, transvaginal ultrasound has been widely used in early screening and diagnosis of IUAs and other gynecological diseases.13 With the rapid development of ultrasound-based radiomics, extracting image information from ultrasound images, realizing feature extraction and prediction model construction, has important guiding value for disease diagnosis and prognosis evaluation.14,15 However, the application of ultrasound-based radiomics in postoperative prognosis evaluation of IUAs has not been fully explored.
In view of this, this study will combine ultrasound-based radiomics and peripheral blood cell indices to predict pregnancy and recurrence risks using interpretable machine learning model (ie IUA-PR) in patients receiving TCRA, and ultimately guiding clinical decision-making.
Materials and Methods
Study Design and Population
We retrospectively selected 387 patients with IUAs who received TCRA treatment in the Obstetrics and Gynecology Department of Enshi Tujia and Miao Autonomous Prefecture Central Hospital from January 2021 and December 2023. Inclusion criteria: (1) Female patients of childbearing age; (2) Patients diagnosed with IUA through hysteroscopy examination; (3) Patients without contraindications for TCRA surgery; (4) Patients without contraindications for postoperative adjuvant drugs. Exclusion criteria: (1) Patients who require hysterectomy (such as malignant endometrial lesions, etc).; (2) Patients with infertility and amenorrhea caused by other reasons; (3) Patients with severe abnormalities in the reproductive tract; (4) Patients with infertility caused by male infertility; (5) Patients who have communication barriers and mental illnesses that prevent follow-up. The specific screening process and prediction model construction are shown in Figure 1.
 |
Figure 1 Flow chart of the study design. |
Ethic Statement
Due to the retrospective nature of this study, we strictly adhered to the Declaration of Helsinki. All patient data were anonymized and encrypted to protect privacy, with data processing methods reviewed for compliance with privacy regulations. For ethical review, we submitted the study to the Medical Ethics Committee of the Central Hospital of Enshi Tujia and Miao Autonomous Prefecture for approval as a retrospective study. The study uses existing anonymized data without interfering with patient treatment or posing additional risks, and after review, the committee granted approval (Approval Document Number: [2025–099-01]) and agreed to the study’s implementation. Regarding informed consent, as the study is a retrospective analysis of existing medical records with fully anonymized patient information, the above Ethics Committee approved a waiver. This was justified by the use of retrospective anonymized data (no direct patient contact or harm to rights), and the difficulty in obtaining consent from all patients due to the long study timeline.
Classification Criteria for IUAs Diagnosis
We referred to March, the American Society for Reproductive Medicine, the European Society for Gynecological Endoscopy, and the China Society of Gynecology Endoscopy scores. Among them, ESGE scores I–II are defined as mild, III as moderate, and IV–V as severe (As shown in Supplementary Table 1).
Surgical Procedure
Contraindications for TCRA surgery include acute pelvic inflammation, severe cervical stenosis that cannot be dilated, severe cardiac, hepatic, renal, or hematological diseases that cannot tolerate surgery, and active genital tract infections. Contraindications for postoperative adjuvant drugs include allergies to estradiol valerate, progesterone, or other components of the drugs, and a history of hormone-dependent tumors (such as breast cancer, endometrial cancer, etc).
The patient underwent bladder lithotomy, and after general anesthesia, routine vaginal disinfection and drape were performed, followed by dilation of the cervix with dilation strips. After the surgery begins, a hysteroscope is used to comprehensively explore the cervix and uterine cavity, clarify the location, nature, area, fallopian tube opening, uterine angle, and endometrial condition of the adhesion zone, and evaluate the severity of the adhesion. Select the surgical method based on the degree of adhesion, blunt separation of membranous adhesions, and electric knife resection for dense adhesions, and stop the surgery until the uterine cavity returns to normal shape. Finally, hyaluronic acid was injected into the patient’s uterine cavity and a Foley balloon catheter was placed, with 5–10 mL of physiological saline injected into the balloon. The above surgeries are all performed by the deputy chief physician or chief physician.
Routine antibiotics are given to prevent infection for 3 days after surgery. Within 3–7 days after surgery, the balloon is removed under hysteroscopy guidance and the uterine cavity is re examined. On the third day after surgery, 2mg/d estradiol valerate was administered continuously for 28 days, and 100mg/d progesterone was administered on the last 14 days of the cycle, for a total of 3 cycles.
Clinical Data Collection and Follow Up
We collect clinical data from all patients, including age, disease duration, reproductive history, menstrual status, previous history and frequency of intrauterine procedures, preoperative estrogen and progesterone pretreatment, preoperative endometrial thickness, preoperative fallopian tube opening, uterine angle, preoperative adhesion, and adhesion properties; Postoperative recurrence of IUAs, menstrual recovery, postoperative endometrial thickness, fallopian tube opening and uterine angle, as well as postoperative adhesion range, nature, and pregnancy status. In addition, we also collected the patient’s admission auxiliary examination report values, including blood routine, coagulation function, liver and kidney function electrolytes, and vaginal three-dimensional ultrasound reports, etc.
Follow up will be conducted through telephone, outpatient, disease course, uterine adnexal ultrasound, and hysteroscopy reports. Pregnancy outcomes: Record the patient’s pregnancy outcomes and placental abnormalities within 6 months, 7~12 months, 1~2 years, and 2 years after surgery. If the patient confirms pregnancy, the follow-up period will be extended to 42 days after delivery. If the patient is not pregnant, the follow-up period will be until December 31, 2024. Postoperative recurrence: Record the diagnosis of IUAs recurrence based on ultrasound imaging at 3 months, 4~6 months, and 7~12 months after surgery.
Acquisition of Ultrasound Image
We used the GE Voluson E10 ultrasound diagnostic instrument and a vaginal ultrasound probe with a frequency of 3.0–9.0MHz. We instructed the patient to take a lithotomy position, continuously scan the uterine adnexa and pelvic cavity, observe the uterine cavity and endometrial lines in multiple sections, and store the images. Finally, we exported them in DICOM format.
Radiomics Feature Extraction and Analysis
Two obstetricians and gynecologists with over 5 years of work experience used 3D Slicer software to draw regions of interest on 3D ultrasound images, and used the built-in Radiomics plugin to extract radiomics features, including shape features, first-order statistical features, second-order statistical features, and high-order statistical features, from the original images and wavelet filtered images. As shown in Supplementary Table 2, to ensure consistency in feature extraction between two physicians, 20 ultrasound images were randomly selected and independently sketched and feature extracted by two physicians, followed by consistency analysis. Finally, all extracted radiomics features undergo Z-score normalization to eliminate scale differences, followed by feature dimensionality reduction and screening using minimum absolute shrinkage and selection operators, and a radiomics scoring formula is listed.
Construction of IUA-PR Prediction Model
All candidate variables included in the study were regularized, and Pearson correlation coefficients between variables were calculated. Then, LASSO logistic regression algorithm and ten fold cross validation were used to adjust the penalty parameters. Finally, after selecting the key feature factors from the candidate variables through feature screening, a logistic regression model and random forest were used to construct the IUA-PR prediction model. Draw the working characteristic curve and area under the curve of the subjects, and use DeLong test, calibration curve, and decision curve analysis to evaluate the predictive performance of the prediction model in the testing sets.
Statistical Analysis
All data analysis and visualization are implemented using R software (version 4.3.2). Quantitative data that conforms to a normal distribution are expressed as mean ± standard deviation and independent sample t-test is used. Measurement data that do not conform to normal distribution are represented by M (Q1, Q3), and Mann Whitney U-test is used for inter group comparison. Categorical data is presented as percentages (%), using chi square test or Fisher’s exact probability method. We calculate the AUC values of each prediction model to evaluate its predictive performance in the training and validation sets, and compare the differences between the prediction models using DeLong test. P<0.05 indicates a statistically significant difference.
Results
Population Characteristics and Postoperative Pregnancy and Recurrence Outcomes
As shown in Tablew 1 and 2, a total of 387 patients diagnosed with IUAs were included in the final analysis. Among them, the duration of illness for patients diagnosed with IUAs ranges from 1 month to 10 years, with a median duration of 9.7 months, and the median age of patients is 31.44 ± 4.26 years. 75 patients achieved successful pregnancies after treatment, with 65 naturally conceived and 10 conceived through assisted reproduction. The postoperative pregnancy rates for mild, moderate, and severe adhesions were 73.68%, 52.13%, and 20.7%, respectively, and decreased with the severity of adhesions. The pregnancy rate for moderate to severe IUAs was higher in the 7~10 months after surgery compared to other time periods, while the pregnancy rate showed a decreasing trend at 1 year after surgery. In addition, the overall postoperative recurrence rate was 10.85%, with 24 cases, 16 cases, and 2 cases experiencing mild, moderate, and severe adhesions, respectively. The highest recurrence rate was 23.8% at 4~6 months after surgery.
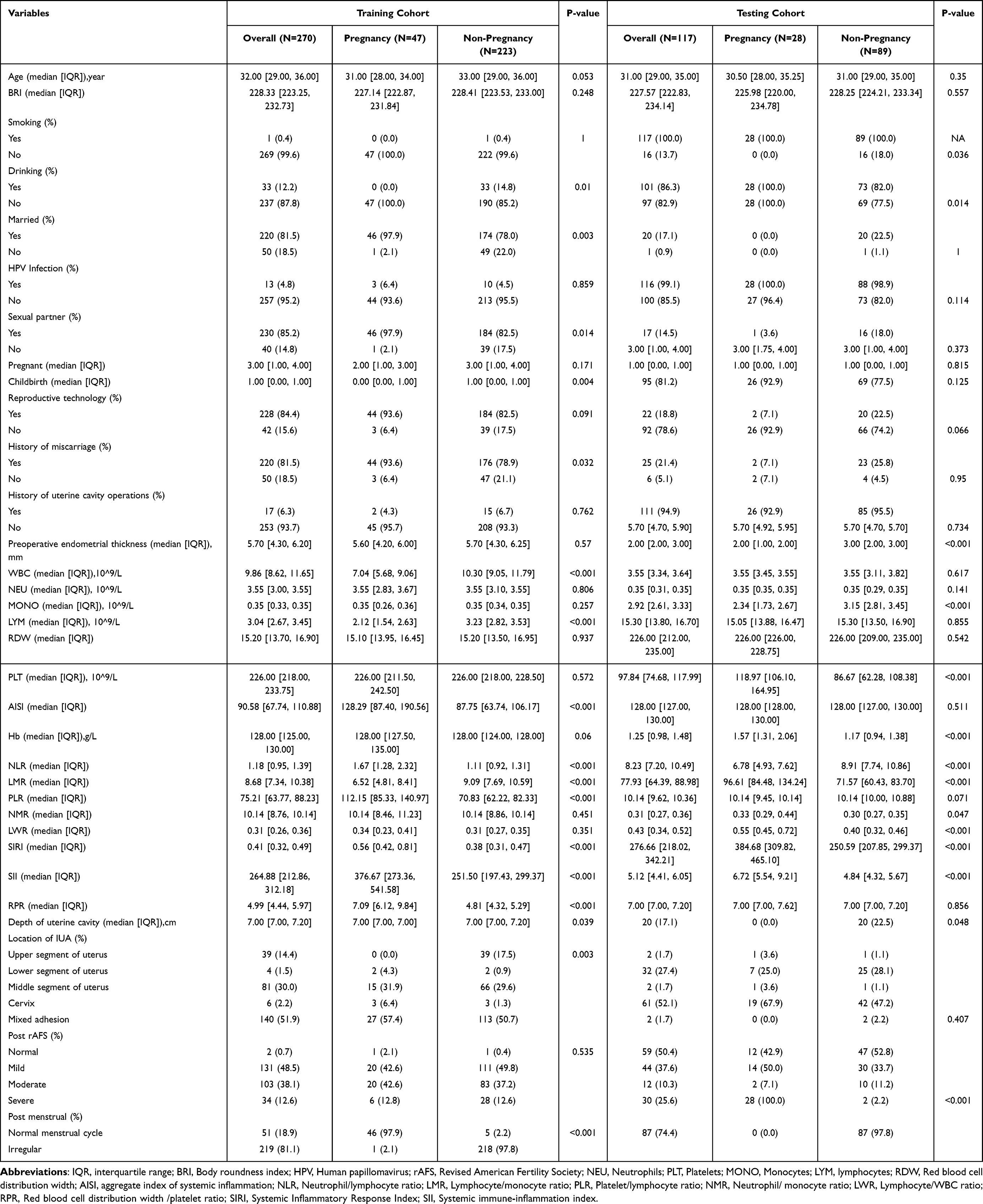 |
Table 1 Comparison of Baseline Data Between Pregnancy and Non-Pregnancy Groups |
 |
Table 2 Comparison of Baseline Data Between Postoperative Recurrence and Non-Recurrence Groups |
Selection of Candidate Features for IUA-PR Prediction Model
As shown in Supplementary Figure 1, we conducted Pearson correlation analysis on all candidate feature factors with pregnancy and recurrence outcomes. The results showed that peripheral blood inflammatory parameters, and pregnancy and recurrence outcomes were significantly correlated (r>0.7). In view of this, we used LASSO to screen for the optimal Lambda coefficient and determine the candidate variables for the minimum penalty coefficient combination. As shown in Figure 2, when the Lambda value was seven and five, the optimal threshold can be determined. As shown in Supplementary Figure 2, six ultrasound radiomic parameters were finally used to construct the IUA-PR prediction model. The Rad-score formula for predicting pregnancy based on ultrasound radiomics calculations is as follows: Rad-score=0.06*Logarithm_RunLengthNonUniformityNormalized+0.87*Wavelet_LLL_ngtdm_Coarseness+0.19*Wavelet_LLH_glszm_SmallAreaHighGrayLevelEmphsis+0.79*Wavelt_HHH_glszm_ZonePercentage+0.25*Wavelet_HHH_glcm_JointAverage+0.90*Logarithm_glrlm_GrayLevelNonUniformity.The Rad-score formula for predicting recurrence based on ultrasound radiomics calculations is as follows: Rad-score=1.22*Logarithm_RunLengthNonUniformityNormalized+1.01*Wavelet_LLL_ngtdm_Coarseness+1.02*Wavelt_HHH_glszm_ZonePercentage+1.12*Wavelet_HHH_glcm_JointAverage.Consistent with the results, as shown in Table 3, we also demonstrated through multivariate logistic regression analysis that peripheral blood inflammatory parameters and ultrasound radiomics scores were independent risk factors for predicting postoperative pregnancy and recurrence of IUAs (P<0.05). Finally, we sorted the candidate feature variables based on Shapley value, which are platelet/lymphocyte ratio(PLR), neutrophil/lymphocyte ratio(NLR), aggregate index of systemic inflammation(AISI), systemic inflammatory response index(SIRI), systemic immune-inflammation index(SII),ultrasound radiomic score (Rad-score), and postoperative menstrual status.
 |
Table 3 Univariate and Multivariate Logistic Regression Results for Pregnancy and Recurrence |
 |
Figure 2 Screening of predictive variables. (A) Pearson correlation analysis between pregnancy outcomes and predictive factors. (B) Lasso regression for screening optimal subsets of pregnancy predictors.(C) Pearson correlation analysis between recurrence outcomes and predictive factors. (D) Lasso regression for screening optimal subsets of recurrence predictors. |
Construction of Predictive Model for Postoperative Pregnancy Outcomes
As shown in Table 3, through regression analysis of risk factors for pregnancy outcomes, we included candidate variables in the nomogram and assigned quantitative scores (Figure 3). Among them, nomogram displays in detail the quantitative scores of ultrasound radiomics, PLR, NLR, AISI, Rad-score and postoperative menstrual status, and based on the sum of the risk factor scores mentioned above, the multiplier value of pregnancy risk can be directly calculated. At the same time, the random forest also relied on ultrasound radiomics and peripheral blood inflammatory indicators to construct visual prediction models, with low value AUC of 0.549 in the validation set.
 |
Figure 3 Nomogram for predicting postoperative pregnancy. (A) Visualization of the nomogram; (B) Cross-line diagram of the prediction mo. (C) ROC curve of the prediction model. |
Construction of Postoperative Recurrence Prediction Model
After integrating ultrasound radiomics and peripheral blood inflammatory parameters, we also conducted machine learning algorithm analysis on the risk of postoperative recurrence of IUAs. The nomogram included selected parameters such as SIRI, SII, NLR, AISI, and Rad-score, as shown in Figure 4, with AUC of 0.720 in the validation sets. However, the recurrence prediction model based on random forest has low value AUC of 0.540 in the validation set.
 |
Figure 4 Nomogram for predicting postoperative recurrence. (A) Visualization of the nomogram; (B) Cross-line diagram of the prediction mo. (C) ROC curve of the prediction model. |
Evaluation of the Efficiency of IUA-PR Prediction Model
As shown in Figure 5, the calibration curve analysis of two types of machine learning prediction models showed that the C-index of nomogram, RFM in the training set was 0.812, and 0.628, respectively, while the C-index in the validation set also reached 0.799, and 0.613, respectively. We further confirmed this result through DCA. As shown in Supplementary Figure 3, when setting the horizontal axis (ie probability threshold) to distinguish whether events occur, we set the risk threshold probability ranges of 15%~76% and 75~84%, respectively. By using nomogram to predict pregnancy and recurrence outcomes, we can infer that patients benefit clinically, which also confirms the optimal net benefit obtained by the IUA-PR prediction model in DCA.
 |
Figure 5 Robustness evaluation of the prediction models. (A) Calibration curve for pregnancy prediction in the test set; (B) Calibration curve for recurrence prediction in the test set. |
Discussion
As an organic lesion of the uterine cavity, the main cause of IUAs is fibrosis of the damaged endometrium, which leads to occlusion or partial occlusion of the uterine cavity or cervical canal.16,17 In clinical practice, patients may have no obvious symptoms, or may have reduced menstrual flow, amenorrhea, periodic lower abdominal pain with cervical adhesions, infertility, miscarriage, and even an increased risk of placental implantation, placenta previa, and postpartum hemorrhage after surgery.18 So far, TCRA has been the main method for treating IUAs, combined with postoperative adjuvant therapy such as intrauterine barrier therapy, treatment to promote endometrial regeneration, drugs to increase endometrial blood flow, anti bioelectric stimulation therapy to improve blood circulation, and traditional Chinese medicine treatment.19,20 Undoubtedly, there are numerous measures to prevent IUAs from reattaching, but due to current treatment outcomes, the expected pregnancy and cure rates for patients are still unsatisfactory. Previous studies have shown that for moderate to severe IUAs, the recurrence rate after comprehensive treatment is as high as 62.5%, and the successful pregnancy rate is only 22.5% to 33.3%.21,22 In view of this, we realize that minimizing the secondary damage caused by surgery to the uterine cavity and seeking alternative high-quality therapies are crucial for improving the pregnancy outcomes and reducing the recurrence rate of IUAs.
In this study, we focused on the high-risk factors of IUAs and explored the prognostic factors, in order to construct a predictive model that can help patients avoid risk factors and provide individual assessment and treatment. Increasing studies demonstrate that IUA may be closely related to the inflammatory cascade that occurs after severe damage to the endometrium.10,23,24 In theory, after local tissue damage occurs in the body, downstream inflammatory cascade reactions are rapidly induced under the mediation of inflammatory factors. Various peripheral blood cells, represented by neutrophils, lymphocytes, platelets, etc., gather through the vascular wall under the action of various chemokines to engulf pathogens, tissue fragments, and foreign objects at the site of tissue damage, while releasing multiple inflammatory mediators to exert immune effects.25–27 Consistent with previous research findings, we plotted independent combined ROC curves for inflammatory markers. The results suggest that all of these inflammatory markers have a certain predictive power for postoperative recurrence and pregnancy outcomes of IUAs (AUC>0.6). Among them, SIRI and AISI have the greatest predictive value for postoperative recurrence of IUAs. We speculate that this may be due to their inclusion of more peripheral blood cell parameters compared to other inflammatory indicators, which can more comprehensively reflect the immune inflammatory status of the body.
In addition, excessive inflammatory activation of the endometrium not only leads to inflammatory and damaging changes in the endometrium, but also alters inflammatory factors in the endometrium, thereby affecting pregnancy outcomes.28,29 Interestingly, our study also found that SIRI and SII can be candidate parameters for predicting postoperative pregnancy in IUAs. Previous studies have shown that the impact of damaging changes in endometritis on fertilized egg implantation may be divided into two types: one is that the diseased endometrium receives embryo implantation, followed by normal pregnancy or miscarriage; The second reason is that the embryo does not adhere to the diseased endometrium, which directly leads to pregnancy failure.30–32Collectively, our use of peripheral blood cell indicators to predict pregnancy outcomes has reference value in terms of predictive efficacy. However, the potential molecular mechanisms underlying the combination of other classic indicators and inflammation with IUAs, as well as pregnancy or infertility, still require further exploration in the future.
Radiomics has opened up new horizons and provided new means for early, quantitative, and non-invasive prediction of IUAs.In this study, we attempted to mine high-throughput quantitative information from ultrasound imaging images to establish a predictive model for predicting postoperative prognosis of IUAs, in order to support clinical decision-making. All radiomics features extracted from the images were selected through feature selection, and the final feature set used for the predictive model was called the “radiomics label”. Interestingly, based on the optimal combination of ultrasound radiomics labels and inflammatory indicators, the nomogram prediction model achieved AUC values of 0.886 and 0.720 for predicting postoperative pregnancy and recurrence of IUAs in the training set, respectively. This indicates that the feature factors provided by ultrasound radiomics have irreplaceable predictive power.
Previous studies have shown that transvaginal three-dimensional ultrasound can accurately describe the echo intensity, evenness, lesion, and muscle layer relationship of endometrial lesions, especially the classification of color Doppler blood flow signals and vascular morphology of lesions.33,34 It has now been used for clinical evaluation of preoperative staging of endometrial malignant tumors.34,35 However, using grayscale extraction values from ultrasound radiomics to construct a co-occurrence grayscale matrix for predicting IUAs is still a pioneering approach in endometrial lesions. We have repeatedly iterated and analyzed the predictive model, and the results are robust and confirm that the grayscale values of ultrasound radiomics are reliable. Moreover, 3D slicer based capture is easy and convenient. In the future, we will focus on the 3D reconstruction of IUAs uterine cavity imaging images in clinical applications, in order to capture more imaging information from a stereoscopic perspective and apply it to clinical prediction models to improve the effectiveness of IUA-PR prediction models.
Our research still inevitably has the following shortcomings that urgently need to be improved.Firstly, although we have collected clinical and ultrasound imaging data from single center patients as much as possible, the population cohort still requires a large sample for promotion and debugging. Therefore, in the future, we need to focus on prospective multi-center large sample studies to further improve; Secondly, we retrospectively collected ultrasound radiomics data, as well as blood routine and other indicators. There are inevitably selection biases and missing values in data quality control, so prospective studies are still needed in the future to obtain more objective and comprehensive clinical data. Meanwhile, we will also conduct ultrasound 3D reconstruction technology to obtain a wider range of ultrasound radiomics data for predicting model feature factor screening; Thirdly, the data we collect is mainly clinically accessible. For future screening of candidate feature prediction parameters, multi-omics fusion features, and high-precision algorithms, significant investment is still needed, especially in AI based optimization algorithms, which are crucial for improving the predictive performance of IUAs prognosis. Nevertheless, the IUA-PR prediction model we constructed is still very inspiring, and further extrapolation and generalization of the prediction model are needed in the future to continuously improve its overall performance.
Conclusion
In summary, the radiological features based on ultrasound combined with peripheral blood inflammatory parameters may be used to accurately predict the risk of postoperative pregnancy and recurrence in patients diagnosed with IUAs. Especially the use of generalized linear model can improve the performance of IUA-PR prediction model. These findings suggest that these models may reduce invasive diagnostic procedures and aid in selecting appropriate treatment strategies, thereby improving the management of patients diagnosed with IUAs.
Acknowledgement
This work was supported by the Enshi Prefecture Science and Technology Plan Research and Development Project (Project Title: Mechanism Study on Selenoprotein S Regulating Vaginal Macrophage-Fibroblast Crosstalk in Uterine Prolapse via Energy Metabolism Reprogramming; Undertaking Institution: Central Hospital of Enshi Tujia and Miao Autonomous Prefecture; Principal Investigator: Bo Wang; Project Duration: June 2024 to June 2026).
Disclosure
Lu Wang and Ying Liu contributed equally to this study and share the first co-authors. The authors report no conflicts of interest in this work.
References
1. Lee WL, Liu CH, Cheng M, Chang WH, Liu WM, Wang PH. Focus on the primary prevention of intrauterine adhesions: current concept and vision. Int J Mol Sci. 2021;22(10). doi:10.3390/ijms22105175
2. Gilman AR, Dewar KM, Rhone SA, Fluker MR. Intrauterine adhesions following miscarriage: look and learn. J Obstet Gynaecology Canada. 2016;38(5):453–457. doi:10.1016/j.jogc.2016.03.003
3. Zhang W, French H, O’Brien M, Movilla P, Isaacson K, Morris S. Incidence of intrauterine adhesions after hysteroscopic myomectomy in patients seeking fertility. J. Minim. Invasive Gynecol. 2023;30(10):805–812. doi:10.1016/j.jmig.2023.05.013
4. Mortimer RM, Lanes A, Srouji SS, Waldman I, Ginsburg E. Treatment of intrauterine adhesions and subsequent pregnancy outcomes in an in vitro fertilization population. Am J Clin Exp Obstet Gynecol. 2024;231(5):536.e1–e10. doi:10.1016/j.ajog.2024.05.026
5. Vitale SG, Riemma G, Carugno J, et al. Postsurgical barrier strategies to avoid the recurrence of intrauterine adhesion formation after hysteroscopic adhesiolysis: a network meta-analysis of randomized controlled trials. Am J Clin Exp Obstet Gynecol. 2022;226(4):487–98.e8. doi:10.1016/j.ajog.2021.09.015
6. Hooker A, Fraenk D, Brölmann H, Huirne J. Prevalence of intrauterine adhesions after termination of pregnancy: a systematic review. Eur J Contracept Reprod Health Care. 2016;21(4):329–335. doi:10.1080/13625187.2016.1199795
7. Ma J, Zhan H, Li W, et al. Recent trends in therapeutic strategies for repairing endometrial tissue in intrauterine adhesion. Biomater Res. 2021;25(1):40. doi:10.1186/s40824-021-00242-6
8. Capmas P, Mihalache A, Duminil L, Hor LS, Pourcelot AG, Fernandez H. Intrauterine adhesions: what is the pregnancy rate after hysteroscopic management? J Gynecol Obstet Hum Reprod. 2020;49(7):101797. doi:10.1016/j.jogoh.2020.101797
9. Zan J, Shuai Y, Zhang J, Zhao J, Sun B, Yang L. Hyaluronic acid encapsulated silver metal organic framework for the construction of a slow-controlled bifunctional nanostructure: antibacterial and anti-inflammatory in intrauterine adhesion repair. Int J Biol Macromol. 2023;230:123361. doi:10.1016/j.ijbiomac.2023.123361
10. Zhao G, Hu Y. Mechanistic insights into intrauterine adhesions. Semin Immunopathol. 2024;47(1):3. doi:10.1007/s00281-024-01030-9
11. Islam MM, Satici MO, Eroglu SE. Unraveling the clinical significance and prognostic value of the neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, systemic immune-inflammation index, systemic inflammation response index, and delta neutrophil index: an extensive literature review. Turk J Emerg Med. 2024;24(1):8–19. doi:10.4103/tjem.tjem_198_23
12. Di Spiezio Sardo A, Calagna G, Scognamiglio M, O’Donovan P, Campo R, De Wilde RL. Prevention of intrauterine post-surgical adhesions in hysteroscopy. A systematic review. Eur J Obstet Gynecol Reprod Biol. 2016;203:182–192. doi:10.1016/j.ejogrb.2016.05.050
13. Amin TN, Saridogan E, Jurkovic D. Ultrasound and intrauterine adhesions: a novel structured approach to diagnosis and management. Ultrasound Obstet Gynecol. 2015;46(2):131–139. doi:10.1002/uog.14927
14. Jia Y, Yang J, Zhu Y, et al. Ultrasound-based radiomics: current status, challenges and future opportunities. Med Ultrasonography. 2022;24(4):451–460. doi:10.11152/mu-3248
15. Moro F, Albanese M, Boldrini L, et al. Developing and validating ultrasound-based radiomics models for predicting high-risk endometrial cancer. Ultrasound Obstet Gynecol. 2022;60(2):256–268. doi:10.1002/uog.24805
16. Shabanian S, Khazaie M, Ferns GA, Arjmand MH. Local renin-angiotensin system molecular mechanisms in intrauterine adhesions formation following gynecological operations, new strategy for novel treatment. J Obstetrics Gynaecol. 2022;42(6):1613–1618. doi:10.1080/01443615.2022.2036972
17. Wang F, Jin Y, Wang M, et al. Combined anti-PD-1, HDAC inhibitor and anti-VEGF for MSS/pMMR colorectal cancer: a randomized Phase 2 trial. Nature Med. 2024;30(4):1035–1043. doi:10.1038/s41591-024-02813-1
18. Dreisler E, Kjer JJ. Asherman’s syndrome: current perspectives on diagnosis and management. Int J Women’s Health. 2019;11:191–198. doi:10.2147/IJWH.S165474
19. Kou L, Jiang X, Xiao S, Zhao YZ, Yao Q, Chen R. Therapeutic options and drug delivery strategies for the prevention of intrauterine adhesions. J Control Release. 2020;318:25–37. doi:10.1016/j.jconrel.2019.12.007
20. Lv H, Wu B, Song J, Wu W, Cai W, Xu J. Hydrogel, a novel therapeutic and delivery strategy, in the treatment of intrauterine adhesions. J Mat Chem B. 2021;9(33):6536–6552. doi:10.1039/D1TB01005K
21. Tanbo T, Fedorcsak P. Endometriosis-associated infertility: aspects of pathophysiological mechanisms and treatment options. Acta obstetricia et gynecologica Scandinavica. 2017;96(6):659–667. doi:10.1111/aogs.13082
22. Carbonnel M, Pirtea P, de Ziegler D, Ayoubi JM. Uterine factors in recurrent pregnancy losses. Fertil Sterility. 2021;115(3):538–545. doi:10.1016/j.fertnstert.2020.12.003
23. Cui X, Xiao HC, Pan W. The predictive value of serum IL-17A and IL-6 expression in postoperative recurrence in patients with intrauterine adhesion. Am J Reprod Immunol. 2024;91(1):e13808. doi:10.1111/aji.13808
24. Hooker AB, de Leeuw RA, Emanuel MH, et al. The link between intrauterine adhesions and impaired reproductive performance: a systematic review of the literature. BMC Pregnancy Childbirth. 2022;22(1):837. doi:10.1186/s12884-022-05164-2
25. Channer B, Matt SM, Nickoloff-Bybel EA, et al. Dopamine, Immunity, and Disease. Pharmacol Rev. 2023;75(1):62–158. doi:10.1124/pharmrev.122.000618
26. Fioranelli M, Roccia MG, Flavin D, Cota L. Regulation of inflammatory reaction in health and disease. Int J Mol Sci. 2021;22(10):5277. doi:10.3390/ijms22105277
27. Picca A, Calvani R, Coelho-Junior HJ, Marzetti E. Cell death and inflammation: the role of mitochondria in health and disease. Cells. 2021;10(3):537. doi:10.3390/cells10030537
28. Pirtea P, Cicinelli E, De Nola R, de Ziegler D, Ayoubi JM. Endometrial causes of recurrent pregnancy losses: endometriosis, adenomyosis, and chronic endometritis. Fertil Sterility. 2021;115(3):546–560. doi:10.1016/j.fertnstert.2020.12.010
29. Yang X, Tian Y, Zheng L, Luu T, Kwak-Kim J. The update immune-regulatory role of pro- and anti-inflammatory cytokines in recurrent pregnancy losses. Int J Mol Sci. 2022;24(1):132. doi:10.3390/ijms24010132
30. Kimura F, Takebayashi A, Ishida M, et al. Review: chronic endometritis and its effect on reproduction. J Obstet Gynaecol Res. 2019;45(5):951–960. doi:10.1111/jog.13937
31. Vitagliano A, Laganà AS, De Ziegler D, et al. Chronic endometritis in infertile women: impact of untreated disease, plasma cell count and antibiotic therapy on ivf outcome-a systematic review and meta-analysis. Diagnostics. 2022;12(9):2250. doi:10.3390/diagnostics12092250
32. Cicinelli E, Trojano G, Vitagliano A. Management of chronic endometritis before in vitro fertilization: lights and shadows. Fertil Sterility. 2022;118(2):347–348. doi:10.1016/j.fertnstert.2022.06.022
33. Costas T, Belda R, Alcazar JL. Transvaginal three-dimensional ultrasound for preoperative assessment of myometrial invasion in patients with endometrial cancer: a systematic review and meta-analysis. Med Ultrasonography. 2022;24(1):77–84. doi:10.11152/mu-2961
34. Harmsen MJ, Van den Bosch T, de Leeuw RA, et al. Consensus on revised definitions of Morphological Uterus Sonographic Assessment (MUSA) features of adenomyosis: results of modified Delphi procedure. Ultrasound Obstet Gynecol. 2022;60(1):118–131. doi:10.1002/uog.24786
35. Spagnol G, Noventa M, Bonaldo G, et al. Three-dimensional transvaginal ultrasound vs magnetic resonance imaging for preoperative staging of deep myometrial and cervical invasion in patients with endometrial cancer: systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2022;60(5):604–611. doi:10.1002/uog.24967
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.