Back to Journals » Journal of Pain Research » Volume 19
Ultrasound-Guided Hydrodissection Combined with Acupotomy Release versus Hydrodissection Alone for Deep Gluteal Syndrome: A Retrospective Study on Short-Term Efficacy
Authors Tuo J, Wang J, Luo Y ![]() , Cao W
, Cao W
Received 22 September 2025
Accepted for publication 6 February 2026
Published 19 February 2026 Volume 2026:19 564639
DOI https://doi.org/10.2147/JPR.S564639
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Überall
Jingmei Tuo,1,* Jinfeng Wang,2,* Yunhao Luo,3 Wen Cao4
1Department of Ultrasound Medicine, Zhangjiakou First Hospital, Zhangjiakou, People’s Republic of China; 2Department of Ultrasound, Shandong Provincial Taishan Hospital (Shandong Provincial Geriatrics Hospital), Taian, People’s Republic of China; 3School of Medical and Life Sciences, Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China; 4Department of Ultrasound Medicine, Beijing Chaoyang Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wen Cao, Chuiyangliu Hospital Affiliated to Tsinghua University, Beijing, People’s Republic of China, Email [email protected] Yunhao Luo, School of Medical and Life Sciences, Chengdu University of Traditional Chinese Medicine, No. 1166, West Section, Liutai Avenue, Wenjiang District, Chengdu, 611137, People’s Republic of China, Tel +86 028 82632338, Email [email protected]
Purpose: To evaluate the short-term efficacy and safety of ultrasound-guided hydrodissection alone versus hydrodissection combined with acupotomy release for deep gluteal syndrome (DGS).
Methods: This retrospective study included 82 patients with DGS, divided into a hydrodissection group (n = 41) and a combined hydrodissection with acupotomy group (n = 41). Both groups underwent ultrasound-guided sciatic nerve hydrodissection; the combined group additionally received acupotomy to incise surrounding fascia. Primary outcomes were changes in Visual Analog Scale (VAS) and Oswestry Disability Index (ODI) scores at two weeks post-treatment.
Results: No complications (eg, bleeding, nerve injury) occurred in either group from immediately post-treatment to two weeks. At two weeks, both groups showed significant improvements in VAS and ODI scores compared to baseline (P< 0.001)). The combined group had greater VAS improvement [median (IQR): 4.00 (4.00, 5.00)] than the hydrodissection group [3.00 (2.00, 4.00); P < 0.001] and greater ODI improvement [40 (20, 60) vs 20 (20, 30); P = 0.004].
Conclusion: Ultrasound-guided hydrodissection combined with acupotomy release was associated with greater short-term pain relief (VAS) and functional improvement (ODI) in patients with DGS compared with hydrodissection alone.
Keywords: deep gluteal syndrome, ultrasound guidance, hydrodissection, acupotomy release, short-term efficacy
Introduction
Deep gluteal syndrome (DGS) is a non-discogenic condition characterized by sciatic nerve entrapment within the deep gluteal space, resulting in chronic buttock pain, sciatica-like symptoms, sensory abnormalities, and reduced lower limb strength.1–4 These symptoms, often arising from pathological changes in structures such as the piriformis muscle, external hip rotators, or bursae, significantly impair quality of life.1,5,6 Epidemiological data indicate that DGS accounts for approximately 0.3% to 6% of cases presenting with lower back or posterior thigh pain, highlighting its underdiagnosed nature and contribution to undiagnosed sciatica.7
The key challenge in managing DGS involves developing minimally invasive treatments that effectively alleviate pain and improve function while minimizing risks.8 Conservative strategies, including physical therapy and corticosteroid injections, frequently provide inconsistent relief, especially in cases with dense fibrotic adhesions.5,9,10 Surgical options, such as endoscopic or open nerve release, offer more definitive decompression but are associated with complications like nerve injury and extended recovery periods.9,11,12 Ultrasound-guided hydrodissection has gained attention as a safe, minimally invasive method to separate nerve adhesions and administer anti-inflammatory agents; however, it may be insufficient for resolving mechanical compression from fibrotic bands.13–16 Similarly, acupotomy enables precise incision of fibrotic tissues but lacks real-time imaging, potentially increasing procedural risks, and its application in DGS remains underexplored.17–19
The integration of ultrasound-guided hydrodissection with acupotomy may offer synergistic benefits by combining hydraulic separation of adhesions with targeted mechanical release of fibrotic structures. This retrospective cohort study evaluates the short-term efficacy and safety of ultrasound-guided hydrodissection alone compared with hydrodissection combined with acupotomy release in patients with DGS, with the hypothesis that the combined intervention yields superior improvements in pain and disability scores.
Methods
Study Design
This retrospective cohort study received approval from the Ethics Committee of Zhangjiakou First People’s Hospital (No. 2025-LW-25) and was conducted in accordance with the principles outlined in the Declaration of Helsinki. Because the study utilized retrospectively collected, fully anonymized clinical data, the Ethics Committee granted a waiver of informed consent, citing the minimal risk to participants and the impracticability of obtaining consent from all eligible patients. Clinical data were extracted from individuals diagnosed with DGS at Beijing Chaoyang Hospital, Capital Medical University, between January 2023 and March 2025. Participants were allocated into two cohorts according to the intervention received: the hydrodissection group (ultrasound-guided sciatic nerve hydrodissection alone) and the combined-therapy group (hydrodissection supplemented with acupotomy).
Setting and Participants
Eighty-two patients were included (41 per group). Baseline demographics (age, sex), clinical data (BMI, disease history), and outcomes were systematically collected. Efficacy was assessed at baseline and two weeks post-treatment using VAS20 and ODI.21
Inclusion Criteria
(1) Age 18–80 years; (2) Confirmed DGS via imaging (MRI/ultrasound) and physical exam, with symptoms >3 months; positive piriformis test and/or FAIR test;5,22 (3) Imaging excluded significant lumbar pathology but showed piriformis abnormalities or sciatic nerve adhesions; (4) Failed conservative treatment ≥3 months.
Exclusion criteria
(1) Prior gluteal surgery or major trauma; (2) Contraindications to gluteal procedures; (3) Comorbid lumbar/hip conditions requiring priority treatment; (4) Active infection; (5) Pregnancy/lactation; (6) Coagulation disorders or anticoagulation without safe pause; (7) Severe psychiatric/cognitive impairment.
Variables
Primary outcomes: Changes in VAS (Visual Analogue Scale, assessed using a 0–10 integer, where 0 = no pain and 10 = worst imaginable pain) and ODI (disability, assessed using a percentage 0–100%, where 0% = no disability and 100% = worst imaginable disability) scores. Secondary: Safety (complications like bleeding, nerve injury). Variables were defined per standard scales; confounders (eg, age, BMI) were assessed for baseline balance.
Data Sources and Measurement
Interventions used a GE LOGIQ E10 ultrasound system (3–5 MHz convex probe). Hydrodissection solution: 20 mL mixture (5 mL 1% lidocaine, 1 mg betamethasone sodium phosphate, saline to volume).13,15 Acupotomy used a sterile needle-knife (0.8 × 80 mm; Hanzhang Medical Devices, Hebei, China).23
Procedure: Patients were positioned prone. For sciatic nerve ultrasound positioning, the probe was placed transversely at the gluteal fold to identify the sciatic nerve as a hypoechoic fascicular structure lateral to the ischial tuberosity and medial to the greater trochanter, with longitudinal views confirming its course between the quadratus femoris and biceps femoris muscles.14,24 For hydrodissection, a 23G needle was advanced under real-time guidance into the perineural fascial plane, and the solution was injected to create a fluid halo separating the nerve from surrounding tissues (Figure 1A).6 In the combined group, following hydrodissection, the 0.8 mm needle-knife was inserted along the same trajectory under ultrasound guidance; small, controlled incisions (typically 2–4 mm in length) were made in the identified fibrotic fascia or piriformis tendon, targeting areas of thickening or adhesion while avoiding vascular structures, with post-incision ultrasound confirming nerve decompression and fluid distribution (Figure 1B).17,23 Treatment concluded upon verification of an annular fluid halo on short-axis (Figure 1C) and long-axis (Figure 1D) views. The hydrodissection group omitted the acupotomy step.
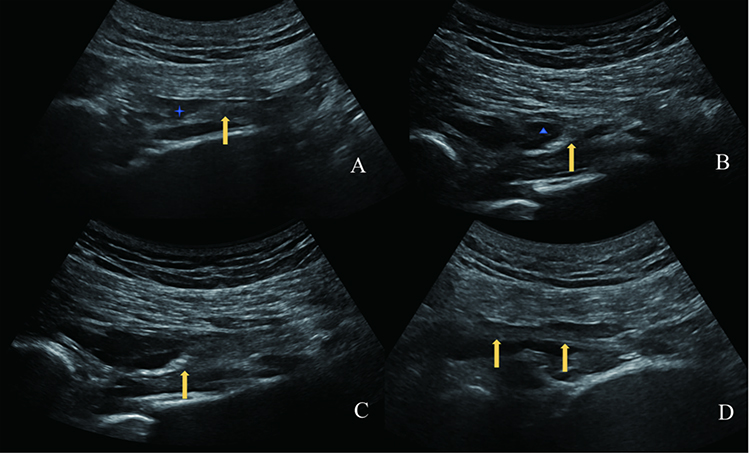 |
Figure 1 Ultrasound-Guided DGS Release Procedure. (A) Short-axis hydrodissection; (B) Short-axis acupotomy release of superficial fascia; (C) Short-axis fluid enveloping sciatic nerve; (D) Long-axis fluid enveloping sciatic nerve. Yellow arrow: Sciatic nerve; Star: Hydrodissection needle tip; Triangle: Acupotomy tip. |
Bias and Study Size
To minimize selection bias in this retrospective design, all eligible patients during the period were included without sampling. Data from electronic medical records were reviewed for completeness; no missing data for key variables. Study size was determined by available cases; post-hoc power analysis confirmed adequate power (VAS/ODI differences, α = 0.05, power > 0.8). Potential biases (eg, retrospective data inaccuracies) were addressed via standardized record review.
Statistical Methods
Data analyzed using SPSS 26.0. Non-normal data described as median (IQR). Between-group comparisons: Mann–Whitney U-test. Within-group: Wilcoxon signed-rank test. Categorical: Chi-square/Fisher’s exact test. P < 0.05 significant. Missing data: None for outcomes; complete case analysis.
Results
Participant Flow and Baseline Characteristics
All 82 patients met criteria and were analyzed (no exclusions or losses). Baseline characteristics (age, height, weight, BMI, pre-treatment VAS/ODI, sex, location) showed no significant differences (P > 0.05; Table 1). No complications occurred immediately post-treatment or at two weeks.
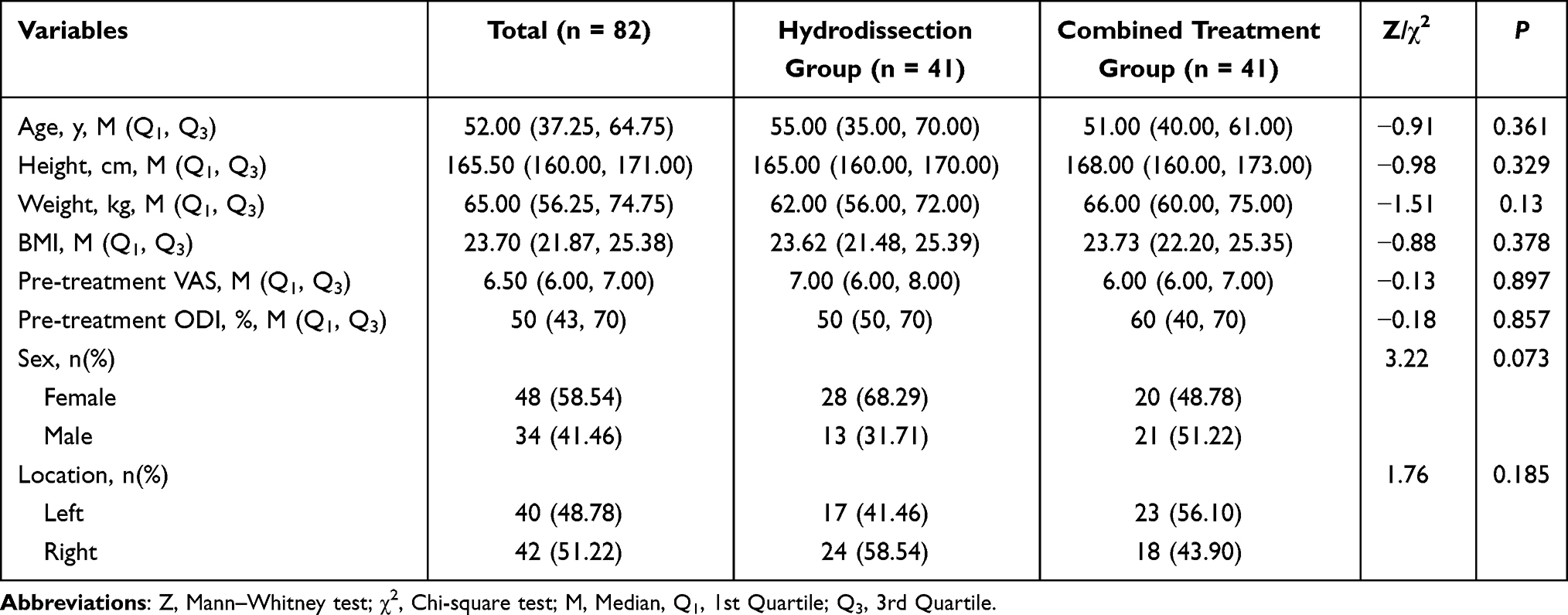 |
Table 1 Baseline Characteristics Before Treatment |
Treatment Outcomes
Hydrodissection group: VAS and ODI significantly decreased at two weeks vs baseline (P < 0.001; Table 2). Combined group: Similar significant decreases (P < 0.001; Table 3).
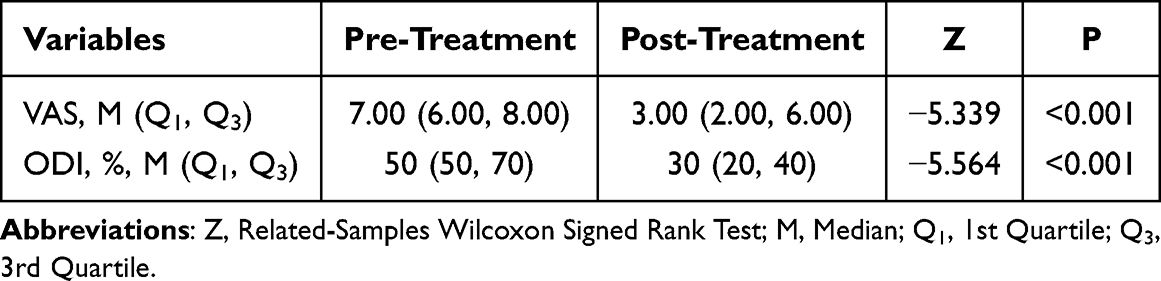 |
Table 2 Hydrodissection Group Outcomes (n = 41) |
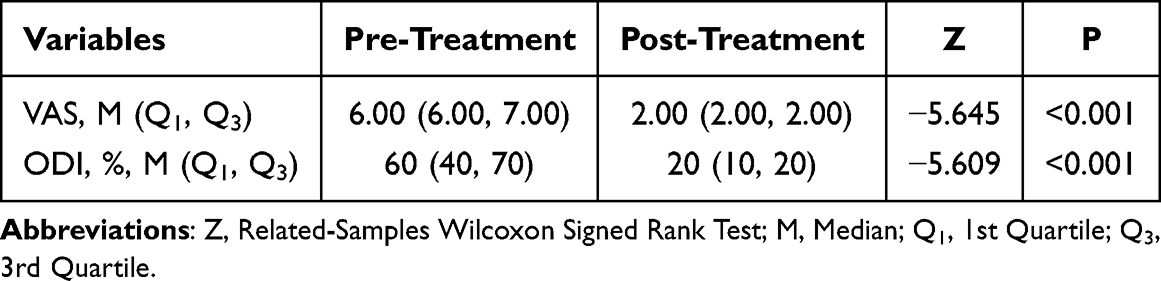 |
Table 3 Combined Group Outcomes (n = 41) |
Comparative Analysis
Combined group showed greater VAS and ODI improvements than hydrodissection group (P < 0.001 and P = 0.004; Table 4).
 |
Table 4 Change Scores Comparison |
Discussion
Summary of Findings
This retrospective study suggests that ultrasound-guided hydrodissection combined with acupotomy release may offer greater short-term clinical benefit than hydrodissection alone for patients with deep gluteal syndrome (DGS), as evidenced by greater improvements in Visual Analog Scale (VAS) scores [median change (IQR): 4.00 (4.00, 5.00) vs 3.00 (2.00, 4.00); P < 0.001] and Oswestry Disability Index (ODI) scores [40 (20, 60) vs 20 (20, 30); P = 0.004], with no observed complications such as bleeding or nerve injury in either group.
Comparison with Previous Research
Our findings align with prior studies on ultrasound-guided hydrodissection for peripheral nerve entrapments, including DGS, which have demonstrated its efficacy in reducing pain by separating adhesions and delivering anti-inflammatory agents.13,15,16 For example, a recent case-series by Yen et al reported improved clinical outcomes in DGS patients treated with sciatic nerve hydrodissection, consistent with our hydrodissection group’s significant VAS and ODI reductions (P<0.001)).12 The potential role of acupotomy in relieving musculoskeletal pain, such as in piriformis syndrome, is consistent with the more pronounced improvements observed in our combined group, as it facilitates precise mechanical decompression of fibrotic tissues.17–19,25 This study contributes to the literature by being among the first to evaluate the combination of these techniques. The observed results suggest a potential synergistic effect that may surpass the outcomes of hydrodissection alone, particularly for dense fibrosis, which previous studies noted as a limitation of hydrodissection alone.15,26,27 The absence of complications in our cohort is encouraging and appears favorable when compared to the risk profiles associated with more invasive surgical approaches (eg, endoscopic or open release) reported in prior work,28 which noted potential nerve injuries.1,9,11 Additionally, our results are supported by recent reports emphasizing the safety of ultrasound-guided interventions due to real-time visualization.24,29,30
Study Limitations
This study has several limitations: (1) its single-center retrospective design may introduce selection bias and limit generalizability to diverse populations; (2) the short 2-week follow-up period precludes assessment of long-term efficacy or recurrence rates, the lack of formal calculation of effect sizes and minimal clinically important difference (MCID), and the limited sample size for assessing safety over a longer term; (3) the absence of objective neurophysiological measures, such as electromyography (EMG) or nerve conduction studies, limits the ability to quantify nerve function improvements; (4) reliance on subjective outcome measures (VAS, ODI) without blinded assessment may inflate effect sizes; (5) No multivariable adjustment (eg, regression analysis) was performed to control for potential confounding factors; therefore, claims of baseline comparability alone are insufficient to fully address the risk of residual bias.
Potential Solutions to Limitations
To address these limitations, future studies could consider: (1) employing multicenter, prospective randomized controlled trials to reduce bias and enhance external validity; (2) extending follow-up to 6–12 months with interim assessments to evaluate sustained outcomes; (3) incorporating EMG and dynamic ultrasound to objectively assess nerve function and mobility; and (4) using blinded outcome assessors or placebo-controlled designs to minimize subjectivity in outcome reporting.
Future Research Directions
Future research could explore modifications to the treatment protocol, such as varying acupotomy needle sizes or hydrodissection injectate compositions (eg, adjusting corticosteroid doses) to optimize outcomes. New questions include whether this combined approach is equally effective in specific subgroups (eg, athletes vs elderly) or compared to endoscopic release. Additionally, investigating its efficacy in preventing DGS recurrence in high-risk groups could be valuable. We recommend large-scale RCTs with advanced imaging follow-up and neurophysiological assessments to confirm long-term efficacy and explore these variations.
Conclusion
Ultrasound-guided hydrodissection combined with acupotomy release was associated with greater short-term pain relief and functional improvement in patients with DGS compared with hydrodissection alone, appearing as a promising and well-tolerated therapeutic approach. Further high-quality, long-term studies are warranted to confirm these preliminary findings and refine the treatment strategy.
Funding
No external funding was received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Elzeiny A, Giai Via R, Donis A, et al. Endoscopy for sciatic nerve entrapment in deep gluteal syndrome. A systematic review of literature. Eurn J Orthop Surg Traumatol. 2025;35(1):223. doi:10.1007/s00590-025-04349-7
2. Gonzalez-Lomas G. Deep gluteal pain in orthopaedics: a challenging diagnosis. JAAOS. 2021;29(24):e1282–7. doi:10.5435/jaaos-d-21-00707
3. Akhaddar A. Deep gluteal syndrome (including piriformis syndrome). In: Atlas of Sciatica: Etiologies, Diagnosis, and Management. Springer; 2024:947–954.
4. Hernando MF, Cerezal L, Pérez-Carro L, Abascal F, Canga A. Deep gluteal syndrome: anatomy, imaging, and management of sciatic nerve entrapments in the subgluteal space. Skelet Radiol. 2015;44(7):919–934. doi:10.1007/s00256-015-2124-6
5. Park JW, Lee Y-K, Lee YJ, Shin S, Kang Y, Koo K-H. Deep gluteal syndrome as a cause of posterior hip pain and sciatica-like pain. Bone Joint J. 2020;102(5):556–567. doi:10.1302/0301-620X.102B5.BJJ-2019-1212.R1
6. Kong L, Gao X, Qian Y, Sun W, You Z, Fan C. Biomechanical microenvironment in peripheral nerve regeneration: from pathophysiological understanding to tissue engineering development. Theranostics. 2022;12(11):4993. doi:10.7150/thno.74571
7. Belyak EA, Lazko FL, Sufianov AA, et al. Endoscopic treatment of deep gluteal syndrome: 3-portal technique. Arthroscopy Techniques. 2024;13(9):103052. doi:10.1016/j.eats.2024.103052
8. Y-we H, Ho GW, Tortland PD. Deep gluteal syndrome: a pain in the buttock. Curr Sports Med Rep. 2021;20(6):279–285. doi:10.1249/JSR.0000000000000848
9. M-s P, Jeong S-Y, Yoon S-J. Endoscopic sciatic nerve decompression after fracture or reconstructive surgery of the acetabulum in comparison with endoscopic treatments in idiopathic deep gluteal syndrome. Clin J Sport Med. 2019;29(3):203–208. doi:10.1097/JSM.0000000000000504
10. Langevin HM, Bouffard NA, Badger GJ, Churchill DL, Howe AK. Subcutaneous tissue fibroblast cytoskeletal remodeling induced by acupuncture: evidence for a mechanotransduction‐based mechanism. J Cell Physiol. 2006;207(3):767–774. doi:10.1002/jcp.20623
11. Martin HD, Hatem MA, Champlin K, Palmer IJ. The endoscopic treatment of sciatic nerve entrapment/deep gluteal syndrome. Tech Orthopaedics. 2012;27(3):172–183. doi:10.1097/BTO.0b013e3182652d81
12. Yen Y-S, Lin C-H, Chiang C-H, Wu C-Y. Ultrasound-guided sciatic nerve hydrodissection can improve the clinical outcomes of patients with deep gluteal syndrome: a case-series study. Diagnostics. 2024;14(7):757. doi:10.3390/diagnostics14070757
13. Lam KHS, Hung C-Y, Chiang Y-P, et al. Ultrasound-guided nerve hydrodissection for pain management: rationale, methods, current literature, and theoretical mechanisms. J Pain Research. 2020;13:1957–1968. doi:10.2147/JPR.S247208
14. Koh E. Imaging of peripheral nerve causes of chronic buttock pain and sciatica. Clin Radiol. 2021;76(8):626.e1–626.e11. doi:10.1016/j.crad.2021.03.005
15. Buntragulpoontawee M, Chang K-V, Vitoonpong T, et al. The effectiveness and safety of commonly used injectates for ultrasound-guided hydrodissection treatment of peripheral nerve entrapment syndromes: a systematic review. Front Pharmacol. 2021;11:621150. doi:10.3389/fphar.2020.621150
16. Silver D, Esener D, Rose G. Ultrasound guided transgluteal sciatic nerve hydrodissection for the treatment of acute sciatica in the emergency department. Am J Emerg Med. 2023;69:219.e3–219.e6. doi:10.1016/j.ajem.2023.02.026
17. Li X, Zhang H, Zhang S, et al. Musculoskeletal ultrasound-guided needle knife therapy in the treatment of refractory nonspecific low back pain: a single-blind, randomized controlled trial. Medicine. 2024;103(52):e41066. doi:10.1097/MD.0000000000041066
18. Zhu Q, Zhu S, Xiong J, et al. Little needle-scalpel for piriformis syndrome: a protocol for systematic review and meta-analysis. Medicine. 2021;100(12):e25242. doi:10.1097/MD.0000000000025242
19. He Y, Miao F, Fan Y, et al. Acupuncture methods for piriformis syndrome: a protocol for systematic review and network meta-analysis. J Pain Res. 2023;16:2357–2364. doi:10.2147/JPR.S417211
20. Faiz KW. VAS–visuell analog skala. Tidsskr nor Laegeforen. 2014;134:323. doi:10.4045/tidsskr.13.1145
21. Fairbank JC, Pynsent PB. The Oswestry disability index. Spine. 2000;25(22):2940–2953. doi:10.1097/00007632-200011150-00017
22. Külcü DG. Deep gluteal syndrome: an underestimated cause of posterior hip pain. Turkish J Phys Med Rehabil. 2024;70(1):4. doi:10.5606/tftrd.2024.14668
23. Li Y, Li S, Zhou Q, Ou Y. Ultrasound-guided needle knife for releasing Osborne’s ligament: an anatomical study. Quantitative Imaging Med Surg. 2025;15(2):1151. doi:10.21037/qims-24-1450
24. Finnoff JT, Hall MM, Adams E, et al. American Medical Society for Sports Medicine position statement: interventional musculoskeletal ultrasound in sports medicine. Clin J Sport Med. 2015;25(1):6–22. doi:10.1097/JSM.0000000000000175
25. Hu J, Tong H, Zhang J, Jiang L. Acupotomy for musculoskeletal pain: exploring therapeutic potential and future directions. J Pain Res. 2025;18:3027–3036. doi:10.2147/JPR.S518705
26. Burke CJ, Walter WR, Adler RS. Targeted ultrasound-guided perineural hydrodissection of the sciatic nerve for the treatment of piriformis syndrome. Ultrasound Quarterly. 2019;35(2):125–129. doi:10.1097/RUQ.0000000000000360
27. Tempski J, Fibiger G, Majka K, et al. Clinical anatomy of the inferior gluteal nerve-systematic review and meta-analysis. Ann Anat. 2025;260:152661. doi:10.1016/j.aanat.2025.152661
28. Leite MJ, Pinho AR, Silva MR, Lixa JC, Madeira MD, Pereira PG. Deep gluteal space anatomy and its relationship with deep gluteal pain syndromes. Hip Int. 2022;32(4):510–515. doi:10.1177/1120700020966255
29. Park GY, Jung JI, Kim KL. Ultrasound-guided nerve hydrodissection for sciatic neuropathy caused by piriformis rhabdomyolysis: a case report. Joint Dis Related Surg. 2025;36(2):461. doi:10.52312/jdrs.2025.2183
30. Colorado B, McNeill D, Norbury J. Ultrasound‐guided nerve hydrodissection for peripheral entrapment neuropathies. Muscle Nerve. 2025;72:1052–1059. doi:10.1002/mus.28471
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Ultrasound-Guided the Prevertebral Fascia Incise and the C5 Root Hydrodissection for the Treatment of Neurogenic Thoracic Outlet Syndrome: an Application Study

Liao Z, Zhou Y, Cao W
Journal of Pain Research 2025, 18:2973-2982
Published Date: 14 June 2025