Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Ultrasound Evaluation of Diaphragmatic and Intercostal Muscle Function as an Indicator of COPD Severity: A Prospective Cross-Sectional Study
Authors Dong Z ![]() , Zhao M, Zheng S, Gu H, Cao N, Sun X, Ge J, Yan X, Ye J, Huang B
, Zhao M, Zheng S, Gu H, Cao N, Sun X, Ge J, Yan X, Ye J, Huang B ![]()
Received 24 September 2025
Accepted for publication 18 December 2025
Published 25 December 2025 Volume 2025:20 Pages 4115—4128
DOI https://doi.org/10.2147/COPD.S569990
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Jill Ohar
Zeyang Dong,1,* Mengyao Zhao,1,* Sihui Zheng,2 Haibo Gu,2 Nan Cao,3 Xixi Sun,3 Jin Ge,3 Xianting Yan,2 Jian Ye,2 Bin Huang3
1The Second School of Clinical Medicine, Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Respiratory Medicine, Zhejiang Hospital, Hangzhou, Zhejiang, People’s Republic of China; 3Department of Ultrasound, Zhejiang Hospital, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bin Huang, Department of Ultrasound, Zhejiang Hospital, Hangzhou, Zhejiang, People’s Republic of China, Email [email protected] Jian Ye, Department of Respiratory Medicine, Zhejiang Hospital, Hangzhou, Zhejiang, People’s Republic of China, Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) is frequently accompanied by respiratory muscle dysfunction, particularly involving the diaphragm and intercostal muscles. This may limit the feasibility of traditional pulmonary function testing.
Purpose: To investigate the association between ultrasound-derived respiratory muscle parameters and COPD severity, and to evaluate the utility of respiratory muscle ultrasound for disease stratification.
Patients and Methods: This single-center, prospective study was conducted at Zhejiang Hospital between January 2024 and June 2025, 78 COPD patients (35 mild-to-moderate, 43 severe) and 50 healthy volunteers were enrolled. Muscle thickness, thickening fraction, excursion, and shear-wave elasticity of the diaphragm and intercostal muscles were measured. Group comparisons and logistic regression analyses were performed. Repeatability was evaluated in the healthy cohort.
Results: All 128 participants completed the study. Ultrasound measurements demonstrated excellent repeatability (ICC coefficients 0.851– 0.969). Gender (male vs female, OR = 4.934, P = 0.014), DE (OR=0.393, P=0.008), ICMTF (OR=10.053, P=0.025), and ICM-SWV (OR=6.419, P< 0.001) were predictive of screening-positive COPD, with an area under the curve (AUC) of 0.908. Within COPD severity stratification, end-inspiratory diaphragmatic thickness (OR=0.041, P=0.014), diaphragmatic thickening fraction (DTF; OR=0.188, P=0.027), and ICM-SWV (OR=5.662, P=0.024) were identified as independent predictors, with an AUC of 0.959.
Conclusion: Respiratory muscle ultrasound offers reproducible and clinically informative parameters that support both COPD diagnosis and severity assessment, providing a potential complementary tool to pulmonary function testing in clinical practice.
Keywords: COPD, pulmonary function, respiratory muscle ultrasound, diaphragm, shear-wave elasticity
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous respiratory disorder characterized by persistent respiratory symptoms such as dyspnea, cough, and sputum production. It arises from progressive airflow obstruction related to airway abnormalities (eg, chronic bronchitis, bronchiolitis) and/or alveolar destruction (eg, emphysema).1,2 As the fourth leading cause of death worldwide, both the incidence and healthcare burden of COPD continue to rise.3,4
In clinical practice, accurate assessment of COPD severity remains challenging. Comorbidities, advanced disease, or pronounced symptoms may limit the feasibility of pulmonary function testing, which is considered the diagnostic gold standard. COPD is typically confirmed when the post-bronchodilator ratio of forced expiratory volume in one second to forced vital capacity (FEV1/FVC) falls below 70%, after excluding alternative causes of airflow limitation. Disease severity is further staged according to the percentage of forced expiratory volume in one second relative to the predicted value (FEV1%pred). However, some elderly, frail, or poorly cooperative patients are unable to undergo pulmonary function testing, further complicating severity evaluation.5–7 Moreover, pulmonary function parameters often lag behind pathophysiological changes and are insensitive to early alterations in COPD. Compared with existing imaging modalities such as CT or MRI, ultrasound provides a radiation-free, bedside, functional evaluation of respiratory muscles, which may better support clinical decision-making.8,9
Respiratory muscles play a central role in alveolar ventilation, and their dysfunction contributes to dyspnea, respiratory failure, and increased mortality in COPD.10,11 Timely and accurate evaluation of respiratory muscle function is therefore of high clinical relevance. In recent years, ultrasound has emerged as a promising modality for assessing diaphragmatic and intercostal muscle structure and function. It is non-invasive, widely available, reproducible, and capable of providing real-time dynamic assessment.12
Despite these advances, important limitations remain in the existing literature. Many prior studies were single-parameter, included small or heterogeneous samples. Few studies have systematically combined structural, functional and elasticity measures in the same cohort, and there is limited information on the reproducibility of such combined assessments across different operators. In addition, intercostal muscles have been less frequently examined than the diaphragm, although they contribute substantially to respiratory mechanics and may undergo different pathological changes in COPD.
To address these gaps, we conducted a single-center prospective study that simultaneously assessed diaphragm and intercostal muscle structure, function, and elasticity using two-dimensional and shear-wave elastography. By integrating multiple indices and explicitly testing repeatability, we aimed to provide more robust evidence for the potential clinical applicability of respiratory muscle ultrasound in COPD assessment.
Materials and Methods
Study Participants and Design
This single-center, prospective cross-sectional study was conducted at Zhejiang Hospital in China. COPD patients and healthy volunteers were enrolled through voluntary recruitment. All participants underwent pulmonary function testing followed by respiratory muscle ultrasound to assess the structural, functional, and elasticity parameters of the respiratory muscles. To ensure the reliability of respiratory muscle ultrasound, we performed a repeatability assessment in healthy subjects. The research procedure is detailed in the flowchart (Figure 1).
 |
Figure 1 Subject Screening Flowchart. Abbreviations: COPD, chronic obstructive pulmonary disease; ICCs, intraclass correlation coefficients. |
This study was approved by the Ethics Review Committee of Zhejiang Hospital (Approval Numbers: 2024-007K; 2025-070K), and written informed consent was obtained from all participants.
Sample Size Calculation
The sample size for the primary study was calculated using G*Power 3.1™ software. Binary logistic regression was used to compare COPD patients with healthy controls and to differentiate between the mild-to-moderate and severe COPD groups. Predictor variables were included in the multivariate logistic regression model. Sample size calculations followed the event/variable ratio (EPV) method commonly used in logistic regression to minimize overfitting and ensure the stability of coefficient estimates. We pre-specified an expected event rate of 0.5 and accounted for a 10% dropout rate, resulting in a minimum requirement of 66 COPD patients and 33 healthy controls to ensure model stability.
For the repeatability analysis, the sample size was calculated using R version 4.4.2, based on the desired precision of the intraclass correlation coefficient (ICC). We assumed a conservative ICC of 0.80, as reported in prior diaphragm ultrasound studies.13 The target was to achieve a 95% confidence interval (CI) width of ≤ 0.25, sufficient to detect a clinically meaningful difference of 0.10.14 Using Bonnett’s adjusted formula for multi-rater designs, a minimum of 45 participants was required to achieve 90% statistical power. To account for potential data loss, facilitate subgroup analyses, and ensure robust Bland–Altman limits of agreement,15 the final target sample size was set at 50. This enrollment provided > 95% power to detect ICC differences of ≥ 0.10, with all 95% CI widths below 0.20.
Participants Recruitment
Subjects were recruited from Zhejiang Hospital, comprising 78 patients with COPD and 50 healthy subjects. An additional assessment of the reproducibility of respiratory muscle ultrasound was conducted in the healthy cohort.
Healthy individuals were eligible if they met the following inclusion criteria: (1) no history of respiratory infection or newly diagnosed cardiac disease within the past month; (2) the results of the pulmonary function tests are normal. Healthy participants were excluded if they had any of the following conditions: (1) chronic respiratory or cardiovascular diseases; (2) history of smoking; (3) current use of respiratory or neurological medications; (4) diaphragmatic or phrenic nerve injury; (5) severe myasthenia gravis, stroke, or other conditions associated with central respiratory depression; (6) history of chest wall surgery or trauma; (7) inability to breathe normally or cooperate during examinations; and (8) inability to complete two full sessions of respiratory muscle ultrasound assessments.
Patients with COPD were included if they met the following criteria: (1) Clinically stable, defined as no acute exacerbation, respiratory infection, hospitalization, or change in maintenance medication within the past 4 weeks;1,16 (2) Diagnosis of COPD confirmed by pulmonary function testing, defined as post-bronchodilator FEV1/FVC < 0.70 according to the GOLD criteria.1 COPD patients were excluded if they had any of the following conditions: (1) diaphragmatic or phrenic nerve injury; (2) lung malignancy; (3) history of chest surgery or trauma; (4) severe myasthenia gravis, stroke, or other conditions associated with central respiratory depression; (5) restrictive lung disease; (6) severe cardiac insufficiency; and (7) inability to complete two full sessions of respiratory muscle ultrasound assessments.
To ensure comparability across participants and avoid the confounding effects of acute exacerbations or systemic corticosteroid exposure on respiratory muscle function, patients were required to be in a clinical stable condition for at least 4 weeks and no use of systemic corticosteroids prior to enrollment. A washout period of more than 4 weeks after the last systemic corticosteroid exposure was required before inclusion. Patients using maintenance inhaled corticosteroids were not excluded, as these agents represent standard COPD therapy and have minimal short-term impact on respiratory muscle function.
Ultrasound Assessment of Diaphragm and Intercostal Muscles (Figure 2)
All respiratory muscle ultrasound examinations were performed using the Mindray R9T system or Mindray M9 bedside ultrasound scanner (Mindray Bio-Medical Electronics, Shenzhen, China). Subjects were positioned in the supine posture. A linear array probe (L15-3WU) was placed perpendicular to the rib axis in the right anterior axillary line at the level of the 8th–10th intercostal spaces. In B-mode, the diaphragm was identified between the pleural and peritoneal layers, and diaphragm thickness (DT) was defined as the distance between these two boundaries. Subsequently, M-mode was applied to record at least three respiratory cycles, from which the end-inspiratory thickness (DTei) and end-expiratory thickness (DTee) were obtained. The diaphragm thickening fraction (DTF) was then calculated using the formula:

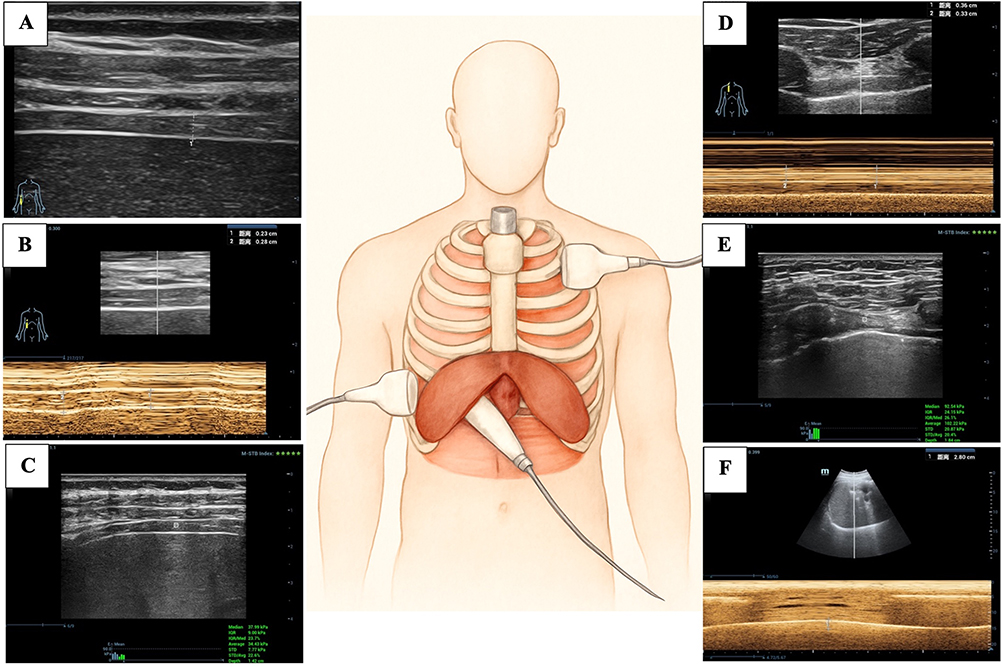 |
Figure 2 Schematic diagram of ultrasonography of the diaphragm and intercostal muscles. (A) Use the L15-3 WU line array probe, B-mode ultrasound was employed to measure diaphragm thickness across respiratory phases. (B) M mode was employed to measure changes in diaphragm thickness across respiratory phases, thereby calculating DTF. (C) Shear wave elastography was used to measure diaphragm stiffness parameters, specifically the median values of diaphragm SWV. (D) M-mode ultrasound measurement of intercostal muscle thickness during different respiratory phases, thereby calculating the ICMTF. (E) Employing shear wave elastography to measure intercostal muscle stiffness parameters, specifically the median values of intercostal muscle SWV. (F) Switch to the SP5-1U phased array probe, position it below the right costal margin, using the liver as the acoustic window, and employ M-mode ultrasound to measure DE. Abbreviations: DTF, diaphragm thickening fraction; SWV, shear wave velocity; ICMTF, intercostal muscle thickening fraction; DE, diaphragm excursion. |
For the measurement of diaphragm excursion (DE), a phased array probe (SP5-1U) was positioned at the junction of the right midclavicular line and the costal margin, using the liver as an acoustic window. With the M-mode sampling line oriented perpendicular to the diaphragmatic dome, respiratory movement was displayed as a sinusoidal waveform, and DE was determined as the vertical distance from the baseline to the peak of inspiration.
To evaluate intercostal muscle thickness, the L15-3WU probe was placed on the right anterior chest wall, perpendicular to the ribs and chest surface, between the 2nd and 3rd intercostal spaces and approximately 2–4 cm lateral to the sternum. The M-mode sampling line was aligned perpendicularly to the superficial and deep fascial layers of the intercostal muscles, and at least three respiratory cycles were observed. Thickness was measured at end-inspiration (ICMTei) and end-expiration (ICMTee), and the intercostal muscle thickening fraction (ICMTF) was calculated using the formula:

Shear Wave Elasticity Assessment of Diaphragm and Intercostal Muscles
Shear wave elastography (SWE) measurements were obtained using the Mindray R9T system. However, not all COPD patients were able to undergo SWE. A total of 28 COPD patients were excluded from SWE assessment due to activity limitations, including inability to maintain a semi-recumbent position, poor breath-hold cooperation, or general physical weakness. These patients were evaluated only with B-mode ultrasound. Due to constraints on diagnostic equipment funding within this institution, the Mindray M9 bedside system used for bedridden patients did not include an SWE module, further contributing to unavailable SWE data in this subgroup.
For shear wave elastography, the L15-3WU linear probe was placed gently on the skin, with a sound-conducting pad positioned between the probe and chest wall to minimize external pressure and enhance image stability. A longitudinal view parallel to the orientation of diaphragmatic and intercostal muscle fibers was obtained throughout the respiratory cycle. For diaphragmatic evaluation, measurements were performed close to the costal insertion of the diaphragm, a region characterized by relatively smaller motion amplitude. After switching to two-dimensional shear wave elastography (SWE) mode, the probe was kept steady at a constant depth, and a 1×1 mm region of interest (ROI) was placed at the center of the diaphragm or intercostal muscle bundles. Subjects were instructed to suspend breathing at end-inspiration while elasticity maps were recorded. Each acquisition was repeated three to five times, and the system automatically provided the average values. Shear wave velocity (SWV) and Young’s modulus (E) were obtained for both diaphragm and intercostal muscles, which were used to determine diaphragm stiffness (DS) and intercostal muscle stiffness (ICMS).
Repeatability Assessment
To account for variability in disease progression and ensure the generalizability of reproducibility testing, assessments were performed in healthy volunteers. Ultrasound examinations of the diaphragm and intercostal muscles were conducted by two experienced operators using a Mindray Resona R9T system (Mindray Bio-Medical Electronics, Shenzhen, China), with less than 30 minutes between sessions. Each operator performed the scans independently, without access to the other’s measurements. After both assessments were completed, the ultrasound data from each subject were collected, and reproducibility was quantified by calculating the intraclass correlation coefficient (ICC).
Pulmonary Function Tests
All COPD patients underwent pulmonary function testing and a bronchodilator challenge using 400 μg salbutamol sulphate inhalation aerosol. Disease severity was classified using GOLD spirometric grading according to the 2025 GOLD report,1 which categorizes disease severity into four grades based on the FEV1%pred: GOLD 1 (FEV1%pred ≥ 80%), GOLD 2 (50% ≤ FEV1%pred < 80%), GOLD 3 (30% ≤ FEV1%pred < 50%), and GOLD 4 (FEV1%pred < 30%).
In this study, to ensure adequate sample sizes across groups, we combined GOLD stages 1 and 2 into the mild-to-moderate group (FEV1%pred ≥ 50%) and combined GOLD stages 3 and 4 into the severe group (FEV1%pred < 50%).
Comprehensive Clinical Assessment of COPD
Additional clinical assessments were conducted using the BODE score to determine patients’ baseline status. The BODE index was calculated using its four standardized components:2,17–19 Body mass index (BMI; ≤21 kg/m2=1 point, >21 kg/m2=0 points), airflow obstruction based on post-bronchodilator FEV1% predicted (≥65%=0 points; 50–64%=1 point; 36–49%=2 points; ≤35%=3 points), dyspnea assessed by the modified Medical Research Council (mMRC) scale (0–1=0 points; 2=1 point; 3=2 points; 4=3 points), and exercise capacity measured by the 6-minute walk test (6MWT; ≥350 m=0 points; 250–349 m=1 point; 150–249 m=2 points; ≤149 m=3 points), with total scores ranging from 0 to 10.
Total BODE scores were stratified into four severity grades: Grade 1 (0–2 points), Grade 2 (3–4 points), Grade 3 (5–6 points), and Grade 4 (7–10 points). These measures supported comprehensive clinical profiling but were not used to define severity groups for analysis, which were based solely on the GOLD spirometric grading as described above.
Statistical Analyses
All data were analyzed using SPSS 26.0 (IBM Corp, Armonk, NY, USA) and R version 4.4.2 (R Foundation for Statistical Computing, Vienna, Austria). Normal data are presented as mean ± standard deviation (SD), and comparisons between groups were performed using the independent samples t-test. Skewed data are presented as median with interquartile range (IQR), and comparisons between groups were conducted using the Mann–Whitney U-test. A two-sided P-value < 0.05 was considered statistically significant.
To ensure clarity, all intergroup comparisons were predefined as follows: healthy control group versus mild-to-moderate chronic obstructive pulmonary disease (COPD) group; healthy control group versus severe COPD group; mild-to-moderate COPD group versus severe COPD group. These groupings were consistently applied in baseline comparisons, correlation analyses, and logistic regression modelling. Three-group comparisons were first performed using global tests (Kruskal–Wallis for continuous variables, and chi-square tests for categorical variables). When the overall test reached statistical significance, post-hoc pairwise comparisons with Bonferroni correction were conducted.
Univariate and multivariate logistic regression analyses were used to identify significant determinants of respiratory muscle ultrasound parameters for diagnosing COPD subgroups. Prior to logistic regression analysis, all data were standardized using SPSS 26.0 to eliminate magnitude effects due to differences in the units and scale of the variables. Employing a data-driven variable selection strategy, all variables with a p-value < 0.10 in univariate logistic regression were incorporated into the multivariate model. Multivariate logistic regression was performed using stepwise regression in R version 4.4.2 to construct predictive models. The diagnostic performance of respiratory muscle ultrasound parameters was evaluated using receiver operating characteristic (ROC) curve analysis. Cutoff values were determined to maximize the Youden index, and the corresponding sensitivity, specificity, and accuracy for each threshold were calculated.
Spearman’s rank correlation coefficient (ρ) was used to assess the correlation between two skewed variables or between a categorical variable and a skewed variable. Intraclass correlation coefficients (ICCs) were calculated to assess the agreement between two respiratory muscle ultrasound measurements in repeatability assessments. The following definitions were used to interpret the ICC values for absolute agreement: 0–0.5 as poor; 0.5–0.75 as fair; 0.75–0.90 as good; and 0.90–1.0 as excellent.14
Results
Baseline Characteristics
Between January 2024 and June 2025, a total of 78 COPD patients and 50 healthy volunteers were enrolled at Zhejiang Hospital, based on the inclusion and exclusion criteria. According to the GOLD classification, 43 subjects were assigned to the severe group, while 35 subjects were assigned to the mild-to-moderate group. Statistically significant differences were observed between the mild-to-moderate group and the severe group in mMRC scores, 6MWD scores and BODE scores. No significant differences were found between the groups for other baseline characteristics, as detailed in Table 1.
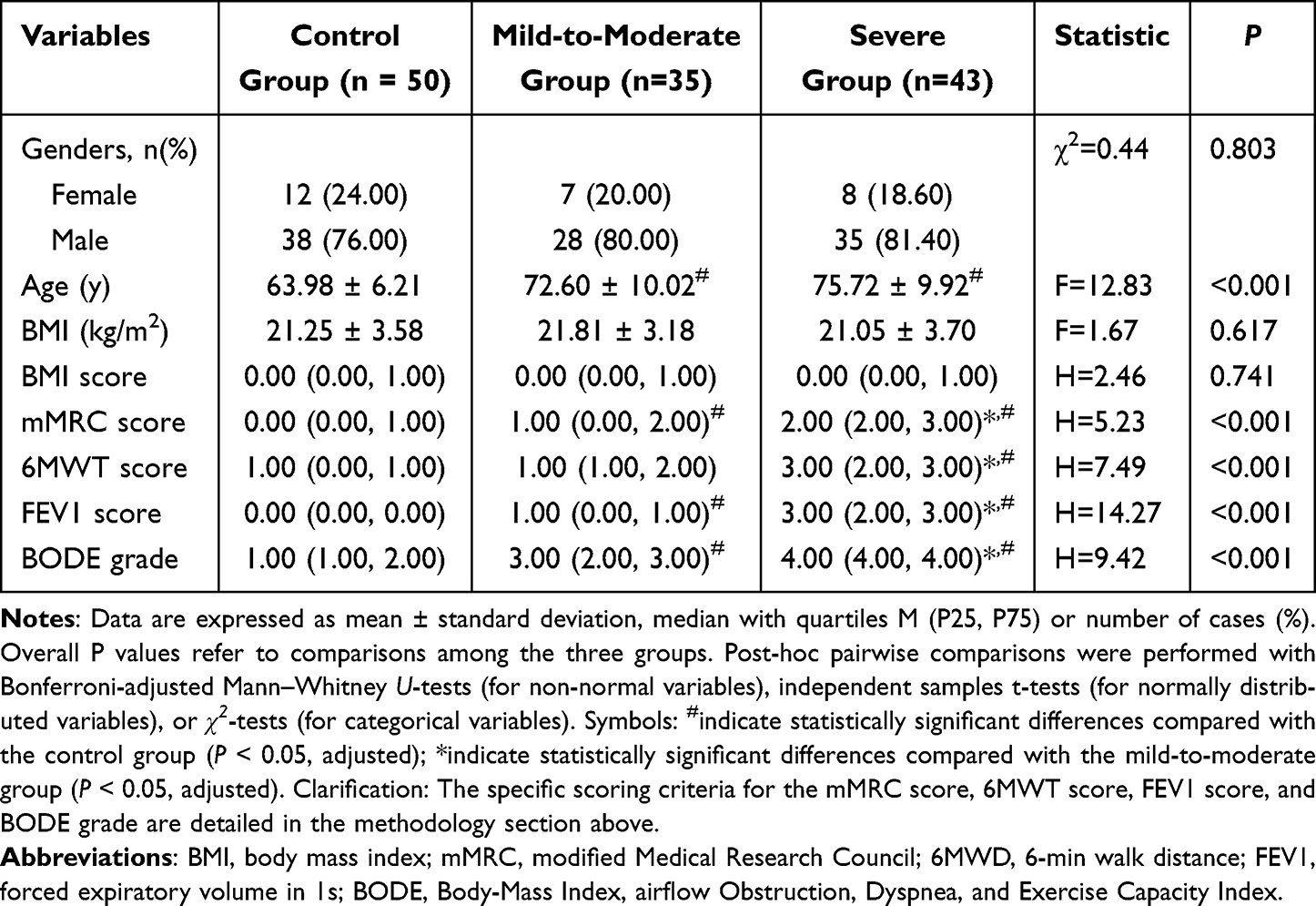 |
Table 1 Baseline Clinical Profile of Subjects |
Repeatability Assessment Results
A total of 50 healthy participants were enrolled to evaluate the reliability of respiratory muscle ultrasound measurements across different examiners. Intraclass correlation coefficients (ICCs) for repeated measurements of DTei, DTee, DTF, DE, diaphragmatic SWV, diaphragmatic E, ICMT, ICMTF, intercostal SWV, and intercostal E were 0.948, 0.953, 0.893, 0.877, 0.857, 0.897, 0.969, 0.851, 0.903, and 0.912, respectively. These findings demonstrate that all evaluated ultrasound indices exhibited high reproducibility and strong reliability in the functional assessment of respiratory muscles.
Differences Analysis of Respiratory Muscle Ultrasound Parameters Across Study Groups
Mann–Whitney U-tests and Spearman correlation analyses of two-dimensional ultrasound parameters revealed significant differences between the mild-to-moderate group and the control group for DE (rs = 0.359, P < 0.001) and ICMTei (rs = 0.228, P = 0.036). Between the severe group and the control group, significant differences were observed for DTei (rs = 0.241, P = 0.020), DE (rs = 0.579, P < 0.001) and DTF (rs = 0.584, P < 0.001). Meanwhile, between the mild-to-moderate and the severe groups, significant differences were noted in DTei (rs = 0.414, P < 0.001), DE (rs = 0.364, P = 0.001), and DTF (rs = 0.429, P < 0.001).
Due to activity limitations in some COPD patients, bedside ultrasound devices could not be used to measure SWE parameters. SWE data were collected from 22 severe, 28 mild-to-moderate COPD patients, and 50 controls. Statistical analysis using independent samples t-tests, Mann–Whitney U-tests, and Spearman correlation revealed significant intergroup differences in intercostal muscle mean SWV (rs = 0.369, P = 0.002) and intercostal muscle mean E (rs = 0.361, P = 0.002) between the mild-to-moderate and control groups. Between the severe and control groups, significant differences were found in diaphragm mean SWV (rs = 0.190, P = 0.050), intercostal muscle mean SWV (rs = 0.569, P < 0.001) and intercostal muscle mean E (rs = 0.450, P < 0.001). Between the severe and the mild-to-moderate groups, significant differences were observed in intercostal muscles mean SWV (rs = 0.354, P = 0.002) and the intercostal muscles mean E (rs = 0.344, P = 0.004). These findings are summarized in Table 2.
 |
Table 2 Intergroup Differences in Two-Dimensional Ultrasound and Shear Wave Elasticity Parameters Respiratory Muscles |
Multivariate Logistic Regression Analysis of Respiratory Muscle Ultrasound Indicators for Screening and Stratified Diagnosis of COPD
Multiple variance tests were conducted on all included parameters, yielding VIF values of 1.088 for the gender variable, 1.07 for DE, 1.04 for ICMTF, and 1.07 for ICM-SWV. As all VIF values were below 5, multicollinearity was excluded.
Multivariate logistic regression was used to compare respiratory muscle ultrasound parameters between healthy subjects and COPD patients. Among the two-dimensional parameters, gender (male vs female, OR = 5.252, P = 0.001), DE (OR = 0.438, P = 0.002), and ICMTF (OR = 4.137, P = 0.022) were identified as independent diagnostic factors for COPD. When combining two-dimensional parameters with elasticity parameters, gender (male vs female, OR = 4.934, P = 0.014), DE (OR = 0.393, P = 0.008), ICMTF (OR = 10.053, P = 0.025), and ICM-SWV (OR = 6.419, P < 0.001) emerged as independent predictors.
For distinguishing mild-to-moderate from severe COPD, among two-dimensional parameters, DTei (OR = 0.045, P = 0.005) and DTF (OR = 0.159, P = 0.006) were identified as independent predictors for severe COPD. Combining two-dimensional parameters with elasticity measures, DTei (OR = 0.041, P = 0.014), DTF (OR = 0.188, P = 0.027), and intercostal muscle mean SWV (OR = 5.662, P = 0.024) were independent predictors. These results are presented in Tables 3 and 4.
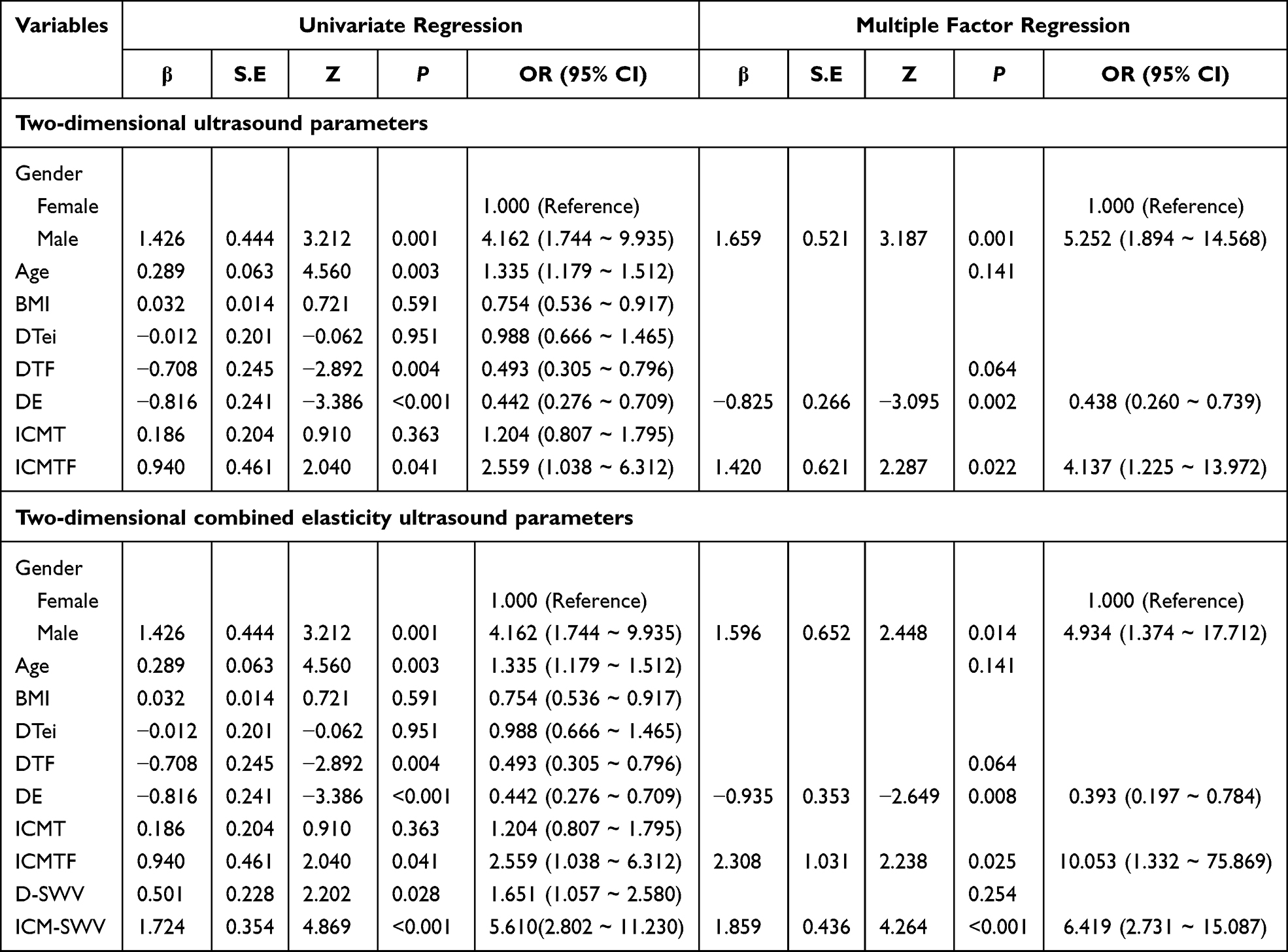 |
Table 3 Multivariate Logistic Regression Results for Respiratory Muscle Ultrasound Parameters Between the Control Group and the COPD Patient Group |
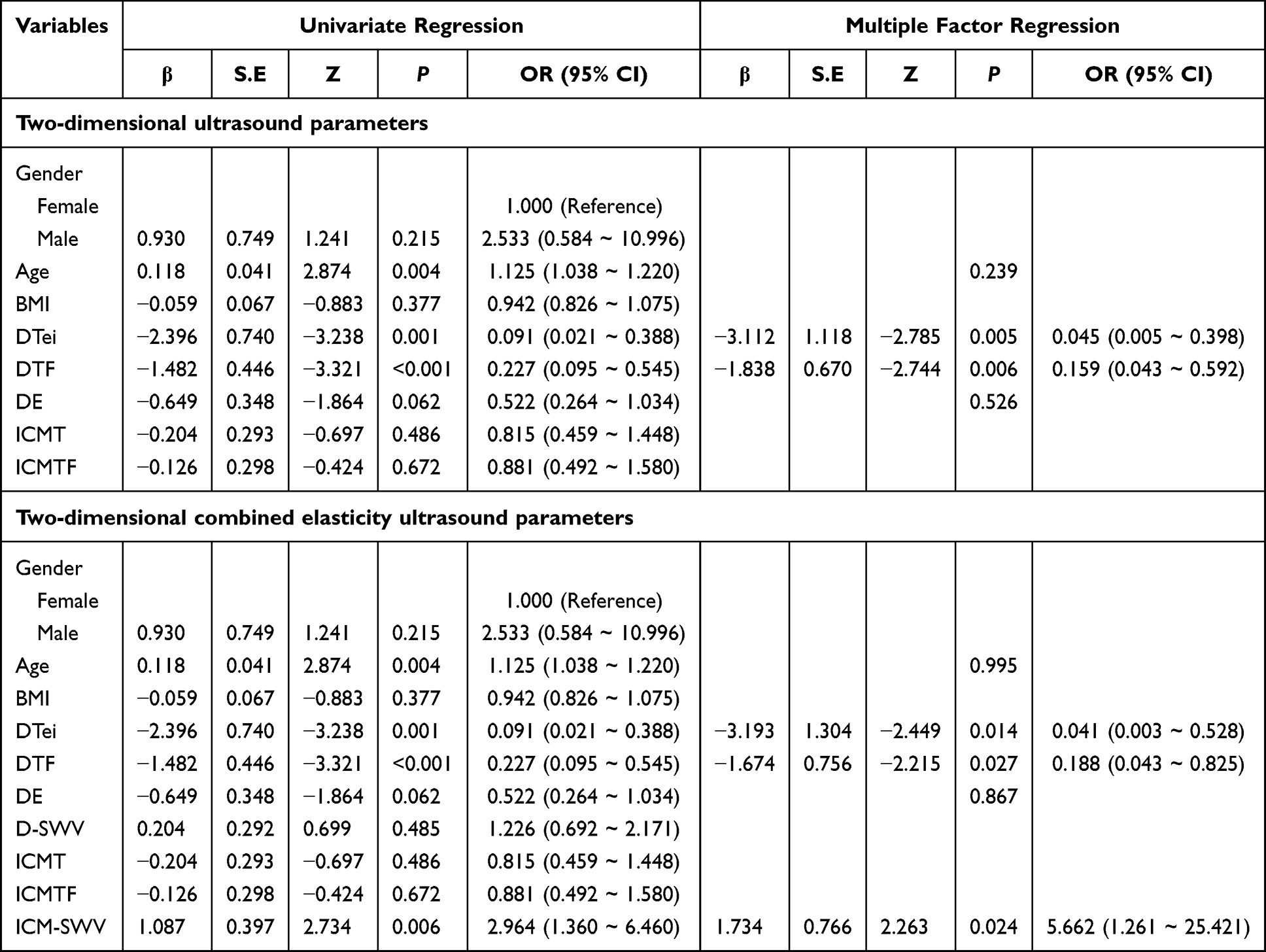 |
Table 4 Multivariate Logistic Regression Results for Respiratory Muscle Ultrasound Parameters Between the Mild-to-Moderate Group and the Severe Group |
Diagnostic Performance of Respiratory Muscle Ultrasound in Screening and Stratified Diagnosis of COPD
A multiple variance test was conducted on all included parameters, yielding VIF values of 1.191 for DTei, 1.202 for DTF, and 1.013 for ICM-SWV. As all VIF values were below 5, multicollinearity was excluded.
For differentiating COPD patients from healthy controls, the logistic regression model based on two-dimensional ultrasound parameters achieved an area under the curve (AUC) of 0.804 (95% CI: 0.721–0.887), accuracy of 0.730 (95% CI: 0.632–0.814), sensitivity of 0.860 (95% CI: 0.764–0.956), and specificity of 0.600 (95% CI: 0.464–0.736). By contrast, the model combining two-dimensional and elasticity parameters yielded an AUC of 0.908 (95% CI: 0.852–0.964), accuracy of 0.860 (95% CI: 0.776–0.921), sensitivity of 0.900 (95% CI: 0.817–0.983), and specificity of 0.820 (95% CI: 0.714–0.926) (Figure 3 and Table 5).
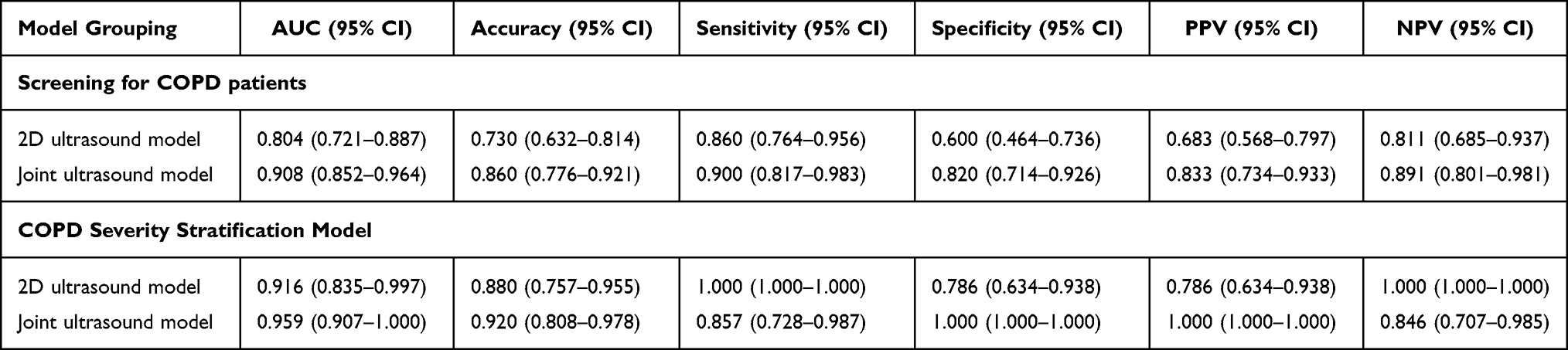 |
Table 5 Diagnostic Performance of Ultrasound-Based Predictive Models for Respiratory Muscles |
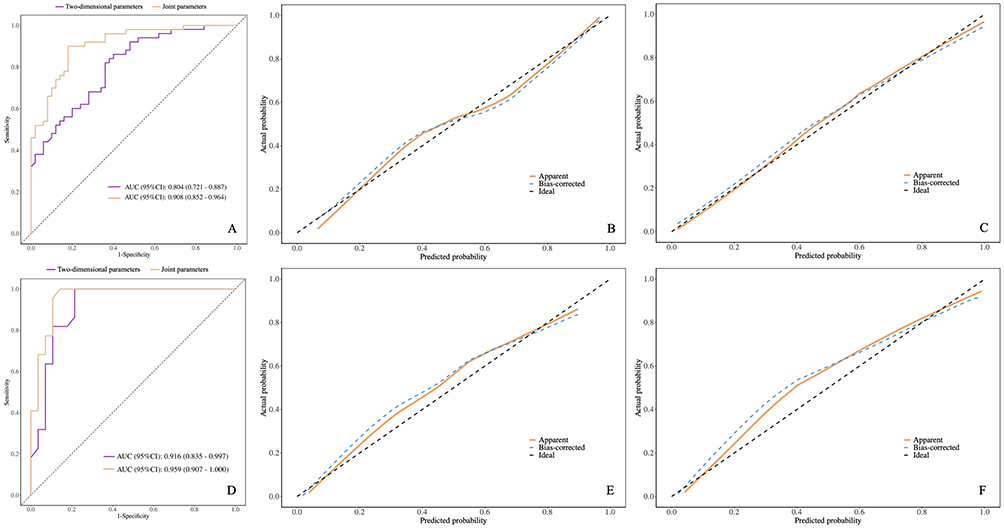 |
Figure 3 Diagnostic performance evaluation of the ultrasound parameter prediction model for respiratory muscles. (A) Receiver operating characteristic (ROC) curves for identifying COPD using logistic regression models derived from respiratory muscle ultrasound parameters. The purple curve represents the model based solely on two-dimensional (2D) parameters, and the yellow curve represents the combined 2D with shear-wave elastography (SWE) model. (B) Calibration curve of the 2D-based model for COPD screening corresponding to (A). (C) Calibration curve of the combined 2D with SWE model corresponding to (A). (D) ROC curves for stratifying COPD severity (mild–moderate vs severe) using logistic regression models. The purple curve represents the 2D-based model, while the yellow curve represents the combined 2D with SWE model. (E) Calibration curve of the 2D-based severity-stratification model corresponding to (D). (F) Calibration curve of the combined 2D with SWE severity-stratification model corresponding to (D). |
For stratifying COPD severity, the logistic regression model using two-dimensional ultrasound parameters achieved an AUC of 0.916 (95% CI: 0.835–0.997), accuracy of 0.880 (95% CI: 0.757–0.955), sensitivity of 0.786 (95% CI: 0.634–0.938), and specificity of 1.000 (95% CI: 1.000–1.000). In comparison, the combined two-dimensional and elasticity parameter model further improved diagnostic performance, with an AUC of 0.959 (95% CI: 0.907–1.000), accuracy of 0.920 (95% CI: 0.808–0.978), sensitivity of 0.857 (95% CI: 0.728–0.987), and specificity of 1.000 (95% CI: 1.000–1.000) (Figure 3 and Table 5).
Discussion
Our study demonstrated that respiratory muscle ultrasound provides reliable and clinically meaningful parameters for evaluating COPD. Among all measurements, DE, DTF, DTei, ICMTF, and ICM-SWV showed the strongest associations with both the presence of COPD and disease severity. These findings align with previous research indicating that traditional pulmonary function parameters alone may not fully capture disease complexity and that additional physiological markers are needed for more comprehensive assessment.20–22 By providing quantitative information on both diaphragm and intercostal muscle function, respiratory muscle ultrasound may serve as a useful complementary tool in situations where pulmonary function testing is limited or unavailable.
Striated muscle dysfunction is a common complication of COPD, manifesting as systemic skeletal and respiratory muscle atrophy. This dysfunction reduces exercise tolerance and weakens pulmonary ventilation. Increased airway resistance, oxidative stress, systemic inflammation, hypercapnia, hypoxia, and acidosis activate proteolytic mechanisms, leading to respiratory muscle atrophy and dysfunction, which further exacerbates pulmonary ventilation impairment. This creates a vicious cycle of respiratory muscle wasting and worsened respiratory function.23–25
Ultrasound offers distinct advantages in respiratory muscle function assessment due to its real-time, non-invasive, and convenient nature.12,26–28 In recent years, the development of advanced ultrasound techniques—such as SWE and tissue Doppler imaging—has further expanded its capability to quantify muscle mechanics, tissue stiffness, and contractile performance.12,29,30 Building on these technical advances, an increasing number of studies have investigated the relationship between respiratory muscle ultrasound parameters and pulmonary function in COPD. Schulz et al observed 140 COPD patients and found that DE was significantly positively correlated with pulmonary function parameters reflecting ventilatory muscle strength, while DTF was significantly correlated with FEV1%pred.31 Alqahtani et al conducted a systematic review of 35 studies, revealing markedly reduced DE and DT in COPD patients, both of which were negatively correlated with disease severity.32 Chen et al compared shear wave elastography results with pulmonary function outcomes in 219 COPD patients and 20 healthy adults, found that diaphragmatic stiffness and intercostal muscle stiffness were positively correlated with disease severity.33 These technological advancements directly underpin the rationale of our study, which integrates both two-dimensional ultrasound and SWE to evaluate respiratory muscle structure, function, and elasticity. By applying these updated imaging techniques, our work provides new evidence supporting the use of respiratory muscle ultrasound as a multidimensional and more sensitive tool for assessing COPD severity.
This study analyzed differences in respiratory muscle ultrasound parameters between groups using differential testing and multiple regression analysis. Statistically significant differences in DE were observed across all three groups. DE reflects the amplitude of diaphragmatic movement during the respiratory cycle and serves as an indicator of diaphragmatic ventilatory function, which is closely correlated with pulmonary ventilation. Diaphragm thickness and DTF exhibited a marked reduction in the severe COPD group, showing statistically significant differences when compared to the mild-to-moderate group and the control group. These findings suggest that severe COPD patients experience varying degrees of diaphragmatic dysfunction and atrophy as the disease progresses. Numerous studies have indicated that diaphragmatic dysfunction correlates with poorer prognosis and elevated mortality risk in COPD patients.34 The difference in ICMTei between the control group and the mild-to-moderate group was statistically significant. This may be attributed to the intercostal muscles, which act as the primary accessory inspiratory muscles and can compensate for early diaphragmatic dysfunction. Some researchers have suggested that increased intercostal muscle work could serve as an early indicator of diaphragmatic atrophy.35 However, no significant differences in ICMTei were found in the severe COPD group, nor were there differences in ICMTF across all groups. This may suggest a limited compensatory role of the intercostal muscles in patients with severe COPD.
In the shear wave elasticity data, the diaphragm mean SWV is markedly elevated in the severe group, which may be attributed to diminished diaphragmatic contractility. Reduced myofibrillar sliding, along with proliferative changes in the muscle interstitial connective tissue, contributes to increased diaphragmatic stiffness. Additionally, both the mean SWV and Young’s modulus of the intercostal muscles increased significantly with worsening COPD severity, potentially due to mechanisms such as prolonged tissue hypoxia and inflammatory extravasation. These factors can lead to remodeling of the intermuscular connective tissue, thereby increasing intercostal muscle stiffness. Interestingly, these alterations were more pronounced than changes in diaphragm elasticity parameters and appeared earlier in the disease course.36
This study developed prediction models based on two-dimensional ultrasound parameters and combined two-dimensional ultrasound and elasticity parameters to distinguish COPD patients from healthy controls and to stratify COPD severity. The results demonstrated that models incorporating combined two-dimensional ultrasound and elasticity parameters exhibited higher AUC values and superior diagnostic performance compared to models using only two-dimensional ultrasound parameters. A noteworthy finding was that intercostal muscle shear wave velocity emerged as an independent influencing factor in both combined models, exhibiting a high odds ratio. This represents a novel observation, highlighting the significant potential of intercostal muscle shear wave elasticity in respiratory muscle ultrasound for COPD patients. This parameter may reflect early alterations in respiratory muscle function, potentially preceding detectable changes in pulmonary function.
Despite the strengths of this prospective study, several limitations should be noted. Firstly, as a single-center, cross-sectional study with geographical and demographic constraints, the findings require validation through multicenter studies with larger sample sizes. Secondly, while we included a healthy control group and COPD patients with varying severity, the sample size may limit the statistical power and robustness of the models. Thirdly, due to constraints on equipment and funding at our institution, our bedside ultrasound devices lacked shear wave elastography modules, leading to missing shear wave elasticity data for some patients with limited mobility. Therefore, further research is needed to evaluate the feasibility and application of bedside shear wave elastography in COPD patients requiring prolonged bed rest. Lastly, although clinical parameters such as gender, age, and BMI were incorporated into our logistic regression analysis, the limited sample size may have hindered the identification of independent influencing factors. Further large-scale studies are needed to investigate these confounding variables more comprehensively. These aspects will be explored in our subsequent studies.
Conclusions
Two-dimensional and shear wave elastography respiratory muscle ultrasound demonstrate good correlation and consistency in assessing the severity of COPD. They exhibit favorable feasibility and diagnostic efficacy in screening for COPD and stratifying its severity. Clinically, respiratory muscle ultrasound may serve as a practical complementary tool—particularly for elderly, bedridden, or non-cooperative patients who are unable to complete pulmonary function tests—by providing an accessible bedside method to assist diagnosis, guide severity assessment, and support individualized disease management.
Abbreviations
COPD, chronic obstructive pulmonary disease; BMI, body mass index; mMRC, modified Medical Research Council; 6MWD, 6-min walk distance; FEV1, forced expiratory volume in 1s; BODE, Body-Mass Index, airflow Obstruction, Dyspnea, and Exercise Capacity Index; DTee, diaphragm thickness of end-expiratory; DTei, diaphragm thickness of end-inspiratory; DTF, diaphragm thickening fraction; DE, diaphragm excursion; ICMTei, intercostal muscle thickness at the end of inspiration; ICMTee, intercostal muscle thickness at the end of expiration; ICMTF, intercostal muscle thickening fraction; ICCs, intraclass correlation coefficients; SWV, shear wave velocity; E, young’s elastic modulus.
Data Sharing Statement
The research data supporting this study are available for evaluation by the editors and reviewers during the peer-review process. Due to patient privacy concerns and institutional ethical restrictions, the datasets generated and analyzed during the current study are not publicly available. However, data may be obtained from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All participants were informed of this study in advance and consent and informed consent were obtained from all participants. Written informed consent was obtained from all participants (or their legal guardians) for the publication of clinical details and/or images.
The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by the ethics board of Zhejiang Hospital (NO.2024.007K; NO.2025.070K). Participation consents were obtained and were approved and supported by the Ethics Review Committee of Zhejiang Hospital.
Acknowledgments
We are indeed to thank the patients for their support and understanding.
Author Contributions
Jian Ye and Bin Huang are Co-corresponding authors of this work. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study have no funding to declare.
Disclosure
All authors have completed the ICMJE uniform disclosure form. The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Venkatesan P. GOLD COPD report: 2025 update. Lancet Respir Med. 2025;13(1):e7–e8. doi:10.1016/S2213-2600(24)00413-2
2. DeMeo DL. Sex, Gender, and COPD. Annu Rev Physiol. 2025;87(1):471–490. doi:10.1146/annurev-physiol-042022-014322
3. GBD 2023 Causes of Death Collaborators. Global burden of 292 causes of death in 204 countries and territories and 660 subnational locations, 1990–2023: a systematic analysis for the Global Burden of Disease Study 2023. Lancet. 2025;406(10513):1811–1872. doi:10.1016/S0140-6736(25)01917-8
4. GBD 2021 Global Sepsis Collaborators. Global, regional, and national sepsis incidence and mortality, 1990–2021: a systematic analysis. Lancet Glob Health. 2025;13(12):e2013–e2026. doi:10.1016/S2214-109X(25)00356-0
5. Stolz D, Mkorombindo T, Schumann DM, et al. Towards the elimination of chronic obstructive pulmonary disease: a Lancet Commission. Lancet. 2022;400(10356):921–972. doi:10.1016/S0140-6736(22)01273-9
6. Kakavas S, Kotsiou OS, Perlikos F, et al. Pulmonary function testing in COPD: looking beyond the curtain of FEV1. NPJ Prim Care Respir Med. 2021;31(1):23. doi:10.1038/s41533-021-00236-w
7. Kim SH, Han MK. Challenges and the future of pulmonary function testing in Chronic Obstructive Pulmonary Disease (COPD): toward earlier diagnosis of COPD. Tuberc Respir Dis. 2025;88(3):413–418. doi:10.4046/trd.2025.0009
8. Mizusawa H, Matsumoto H, Shiraishi M, et al. Evaluation of patients with chronic obstructive pulmonary disease by maximal inspiratory pressure and diaphragmatic excursion with ultrasound sonography. Respir Investig. 2024;62(2):234–239. doi:10.1016/j.resinv.2023.12.013
9. Zhang T, Liu Y, Wang M, et al. Diaphragm assessment by multimodal ultrasound imaging in patients with chronic obstructive pulmonary disease: a prospective observational study. Int J Chron Obstruct Pulmon Dis. 2025;20:2629–2638. doi:10.2147/COPD.S527119
10. Silva RN, Goulart CDL, de Oliveira CR, et al. Respiratory muscle strength can improve the prognostic assessment in COPD. Sci Rep. 2024;14(1):12360. doi:10.1038/s41598-024-54264-w
11. Furukawa Y, Miyamoto A, Asai K, et al. Respiratory muscle strength as a predictor of exacerbations in patients with chronic obstructive pulmonary disease. Respirology. 2025;30(5):408–416. doi:10.1111/resp.70003
12. Dres M, Doorduin J, Boussouar S, et al. Advancements in imaging techniques for monitoring the respiratory muscles. Crit Care. 2025;29(1):110.
13. Zhao H, Long L, Liu Y, et al. Multimodal diaphragmatic ultrasound indicators in healthy adults: reliability and consistency observation by ultrasound physician and critical care physician. Front Med. 2025;12:1542979.
14. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–163. doi:10.1016/j.jcm.2016.02.012
15. Jan SL, Shieh G. The Bland-Altman range of agreement: exact interval procedure and sample size determination. Comput Biol Med. 2018;100:247–252. doi:10.1016/j.compbiomed.2018.06.020
16. Miravitlles M, Calle M, Molina J, et al. Update 2025 of the Spanish COPD Guidelines (GesEPOC): pharmacological treatment of stable COPD. Arch Bronconeumol. 2025;61(12):766–782. doi:10.1016/j.arbres.2025.10.008
17. Celli BR, Cote CG, Marin JM, et al. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(10):1005–1012. doi:10.1056/NEJMoa021322
18. Mahler DA, Wells CK. Evaluation of clinical methods for rating dyspnea. Chest. 1988;93(3):580–586. doi:10.1378/chest.93.3.580
19. ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111–117. doi:10.1164/ajrccm.166.1.at1102
20. McDonald MN, Wouters EFM, Rutten E, et al. It’s more than low BMI: prevalence of cachexia and associated mortality in COPD. Respir Res. 2019;20(1):100. doi:10.1186/s12931-019-1073-3
21. Sievi NA, Sepin J, Roeder M, et al. Are predictors for overall mortality in COPD patients robust over time? J Clin Med. 2023;12(4):1587. doi:10.3390/jcm12041587
22. Kwan HY, Maddocks M, Nolan CM, et al. The prognostic significance of weight loss in chronic obstructive pulmonary disease-related cachexia: a prospective cohort study. J Cachexia Sarcopenia Muscle. 2019;10(6):1330–1338. doi:10.1002/jcsm.12463
23. Henrot P, Dupin I, Schilfarth P, et al. Main pathogenic mechanisms and recent advances in COPD peripheral skeletal muscle wasting. Int J Mol Sci. 2023;24(7):6454. doi:10.3390/ijms24076454
24. Gosker HR, Langen RC, Simons SO. Role of acute exacerbations in skeletal muscle impairment in COPD. Expert Rev Respir Med. 2021;15(1):103–115. doi:10.1080/17476348.2021.1843429
25. Gea J, Ausín P, Martínez-Llorens JM, Barreiro E. Respiratory muscle senescence in ageing and chronic lung diseases. Eur Respir Rev. 2020;29(157):200087. doi:10.1183/16000617.0087-2020
26. Haaksma ME, Smit JM, Boussuges A, et al. EXpert consensus On Diaphragm UltraSonography in the critically ill (EXODUS): a Delphi consensus statement on the measurement of diaphragm ultrasound-derived parameters in a critical care setting. Crit Care. 2022;26(1):99. doi:10.1186/s13054-022-03975-5
27. Zhou EF, Fu SN, Huang C, Huang XP, Wong AYL. Reliability and validity of ultrasonography in evaluating the thickness, excursion, stiffness, and strain rate of respiratory muscles in non-hospitalized individuals: a systematic review. BMC Oral Health. 2023;23(1):959. doi:10.1186/s12903-023-03558-y
28. Molina-Hernández N, Chicharro JL, Becerro-de-Bengoa-Vallejo R, et al. Ultrasonographic reliability and repeatability of simultaneous bilateral assessment of diaphragm muscle thickness during normal breathing. Quant Imaging Med Surg. 2023;13(10):6656–6667. doi:10.21037/qims-23-329
29. Dong Z, Zhao M, Sun X, Huang B Beyond feasibility: standardisation and reproducibility as the next frontier for respiratory muscle ultrasound. Crit Care. 2025;29(1):314. doi:10.1186/s13054-025-05571-9
30. Dong Z, Chen J, Ge J, Zhao Zhao M, Zhao Y, Zheng S, Ye J, Sun X and Huang B. Respiratory and peripheral muscle ultrasound, including shear-wave elastography, for sarcopenia screening in COPD. Front. Nutr. 2025;12:1687103. doi:10.3389/fnut.2025.1687103
31. Schulz A, Erbuth A, Boyko M, et al. Comparison of ultrasound measurements for diaphragmatic mobility, diaphragmatic thickness, and diaphragm thickening fraction with each other and with lung function in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2022;17:2217–2227. doi:10.2147/COPD.S375956
32. Alqahtani JS, Oyelade T, Sreedharan J, et al. Diagnostic and clinical values of non-cardiac ultrasound in COPD: a systematic review. BMJ Open Respir Res. 2020;7(1):e000717. doi:10.1136/bmjresp-2020-000717
33. Chen Y, Li J, Dong B, Zhu Z, Lyu G. Two-dimensional shear wave elastography: a new tool for evaluating respiratory muscle stiffness in chronic obstructive pulmonary disease patients. BMC Pulm Med. 2022;22(1):441. doi:10.1186/s12890-022-02231-4
34. Rittayamai N, Chuaychoo B, Tscheikuna J, Dres M, Goligher EC, Brochard L. Ultrasound evaluation of diaphragm force reserve in patients with chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2020;17(10):1222–1230. doi:10.1513/AnnalsATS.202002-129OC
35. Rittayamai N, Marinpong V, Chuaychoo B, Tscheikuna J, Brochard LJ. Ultrasound evaluation of parasternal intercostal, diaphragm activity, and their ratio in male patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2024;209(8):1016–1018. doi:10.1164/rccm.202310-1769LE
36. Wallbridge P, Parry SM, Das S, et al. Parasternal intercostal muscle ultrasound in chronic obstructive pulmonary disease correlates with spirometric severity. Sci Rep. 2018;8(1):15274. doi:10.1038/s41598-018-33666-7
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Singing on Symptoms in Stable COPD: A Systematic Review and Meta-Analysis
Fang X, Qiao Z, Yu X, Tian R, Liu K, Han W
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2893-2904
Published Date: 14 November 2022
The Importance of the Diaphragm in Neuromotor Function in the Patient with Chronic Obstructive Pulmonary Disease
Bordoni B, Escher A, Compalati E, Mapelli L, Toccafondi A
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:837-848
Published Date: 11 May 2023
The Effects of Smoking and Airway Restriction on Subclinical Atherosclerosis
Yeşildağ M, Keskin Z, Yavşan DM, Bekci TT, Osmanoglu UO
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1217-1226
Published Date: 24 April 2025
Effects of Diabetes Mellitus and Glycemic Traits on COPD and Pulmonary Function Traits: Insights From Mendelian Randomization and NHANES
Wang N, Wang G, Liu T, Ji W, Li M, Li T, Hu T, Shi Z
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:3575-3590
Published Date: 4 November 2025