Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
U-Shaped Association of Standardized Serum 25-Hydroxyvitamin D with Risk of Low Muscle Mass: A Population-Based Cross-Sectional Study
Authors Zhang G, Wang X, Tong M, Chen J, Ji Q
Received 26 May 2023
Accepted for publication 18 July 2023
Published 31 July 2023 Volume 2023:16 Pages 2167—2177
DOI https://doi.org/10.2147/JMDH.S420963
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Gang Zhang,1 Xiaotong Wang,2 Mingyue Tong,1 Jian Chen,1 Qian Ji3
1Department of Rehabilitation, The First Affiliated Hospital of Anhui Medical University, Anhui Public Health Clinical Center, Hefei, Anhui, 230000, People’s Republic of China; 2Department of Cardiology, The Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, 221000, People’s Republic of China; 3Department of Emergency, The Second Hospital of Nanjing, Nanjing University of Chinese Medicine, Nanjing, Jiangsu, 210003, People’s Republic of China
Correspondence: Qian Ji, Department of Emergency, The Second Hospital of Nanjing, Nanjing University of Chinese Medicine, Nanjing, 210003, People’s Republic of China, Email [email protected]
Background: In the United States (U.S.) general population, the association between standardized serum 25-hydroxyvitamin D (25(OH)D) concentration and risk of low muscle mass (LMM) remains unclear. Our research aimed to determine whether or not there was a relationship between serum 25(OH)D concentration and risk of LMM.
Methods: We analyzed the cross-sectional data of the US population that participated in the National Health and Nutrition Examination Survey between 2011 and 2014. The relationship between serum 25(OH)D concentration and LMM risk was evaluated using restricted cubic spline (RCS) with multivariate logistic regression model and subgroup analysis.
Results: In all, we included 10,256 people in our analysis. The RCS plot demonstrated a U-shaped relationship between serum 25(OH)D concentration and risk of LMM (P for nonlinearity < 0.05). At a Vitamin D concentration of 38.5 nmol/L, LMM risk was at its lowest. Based on analyses stratified by age, sex, hypertension, and diabetes mellitus (DM), serum 25(OH)D concentration and risk of LMM were U-curve correlated for those age 40 or older, male, with hypertension, or without DM. However, LMM risk was positively related to serum 25(OH)D concentration in those younger than age 40 or in women.
Conclusion: There is a U-shaped relationship between serum 25(OH)D concentration and the risk of LMM in the general U.S. population. Careful monitoring and appropriate Vitamin D supplementation might lessen the risk of LMM.
Keywords: cross-sectional study, low muscle mass, serum 25-hydroxyvitamin D concentration, National Health and Nutrition Examination Survey, United States
Introduction
Rosenberg first proposed the term “sarcopenia” to describe the loss of muscle mass associated with aging in 1989.1 Sarcopenia is defined as a geriatric syndrome characterized by progressive and widespread loss of muscle mass and function, with adverse risks of decreased quality of life and increased mortality.2 The average prevalence among the elderly in the community was 12.8% worldwide.3 It is estimated to have a greater global disease burden than major depression and chronic respiratory illnesses combined.4
Studies have shown that sarcopenia is closely related to malnutrition.5 Casati and his team found that certain serum nutritional markers, including hemoglobin (Hb), albumin, selenium, magnesium, and Vitamin D, are also associated with sarcopenia.6 Among them, Vitamin D is an essential fat-soluble vitamin involved in the regulation of calcium and phosphorus, promoting bone mineralization and bone remodeling, and is closely related to bone metabolism.7 This clinical biomarker for Vitamin D status is serum 25-hydroxyvitamin D (25(OH)D).8 Vitamin D levels affect muscle cell contractility, proliferation, and differentiation, which are linked to skeletal muscle health.9 Vitamin D insufficiency results in muscle deficits, and Vitamin D supplementation has beneficial effects. Further, identification of the Vitamin D receptor in skeletal muscle provides evidence for its direct effect on sarcopenia.10 Muscle strength is affected by vitamin D deficiency, which may contribute to the onset of sarcopenia.11 The maintenance of sufficient serum 25(OH)D may prevent unfavorable changes in muscle mass in both young and middle-aged Korean adults.12 Ko et al found that the levels of 25(OH)D in men might be correlated positively with skeletal muscle mass.13 Kim and his team revealed that regardless of obesity, subjects with sarcopenia had significantly lower vitamin D levels than those without sarcopenia. Additionally, in the older Korean population, they also found a strong inverse association between 25(OH)D level and sarcopenia.14 Meanwhile, Park et al also found that among Korean women aged 50 years or older, serum 25(OH)D levels were a negative moderator of sarcopenia.15 Additionally, in postmenopausal Korean women, sarcopenia was associated with both insulin resistance and 25-hydroxyvitamin D levels, regardless of obesity status.16 However, the link between serum 25(OH)D and the risk of low muscle mass (LMM) have not been studied in recent years in the general United States (US) population. The National Center for Health Statistics (NCHS) conducts a population-based study called the National Health and Nutrition Examination Survey (NHANES) to monitor the health and nutritional status of civilians and non-medical personnel. Data collection and analysis is carried out using a multi-stage, probabilistic cluster design rather than a simple random sample based on the US population.17 Therefore, in this study, we aimed to determine whether serum 25(OH)D concentration has an influence on LMM in the general US population using NHANES data from 2011–2014.
Materials and Methods
Study Population
The NHANES database is a large, ongoing cross-sectional survey designed to be nationally representative (https://www.cdc.gov/nchs/nhanes/).18,19 Two two-year cycles (2011–2014) from the NHANES database were used in this analysis. Among the 19,134 participants in the total sample, we excluded participants for whom data on vitamin D levels (n = 2954) and information about LMM (n = 5924) were not available in the NHANES database. Finally, this research included a total of 10,256 individuals. The NCHS study ethics review board approved all NHANES protocols, and participants or their proxies provided informed consent prior to participation.20
Serum 25(OH)D Concentration
A blood sample was collected during the examination, centrifuged, divided, and frozen to −70 °C on site, then shipped on dry ice to a central laboratory, where it was stored at −70 °C until analysis. A radioimmunoassay kit (DiaSorin, Stillwater, MN) after acetonitrile-based extraction was used by the National Center for Environmental Health (Atlanta, GA) to measure serum 25(OH)D levels. For six two-year cycles (2007–2018), the United States Centers for Disease Control and Prevention laboratory used the LC-MS/MS method to analyze serum 25(OH)D metabolites, and the combined total serum 25(OH)D (nmol/L) was calculated by adding 25(OH)D2 and 25(OH)D3, excluding epi-25-hydroxyvitamin D3. The detailed information and procedure are described on the NHANES website https://wwwn.cdc.gov/nchs/nhanes/vitamind/analyticalnote.aspx.
LMM Ascertainment
Using the QDR-4500 Hologic Scanner (Bedford, MA), dual-energy x-ray absorptiometry (DEXA) was used to evaluate body composition (muscle mass and body fat). Except for false teeth and hearing aids, everything metal was removed before testing. Appendicular lean mass (ALM) was defined as the sum of the fat-free masses of all four extremities (arms and legs). For this study, Foundation for the National Institutes of Health criteria were used for ALM-defined LMM (<19.75kg in males, <15.02 kg in females) and ALM adjusted for body mass index (BMI) (<0.789 kg for males, <0.512 kg for females).21–23
Covariates
The following covariates were included: demographic data (age, sex, race/ethnicity, family poverty income ratio (PIR), education level, and marital status), complication data (hypertension, and diabetes mellitus (DM)), history of smoking and drinking, body measurement data (body mass index (BMI), waist circumference), blood pressure data (systolic blood pressure (SBP), diastolic blood pressure (DBP)), dietary data (mean energy intake, dietary Vitamin D intake), and laboratory test data (hemoglobin (Hb), fast glucose (FBG), glycosylated hemoglobin (HbA1C), high-density lipoprotein-cholesterol (HDL-C), total cholesterol (TC), triglyceride (TG), blood urea nitrogen (BUN), serum uric acid (sUA), serum creatinine (Scr), and estimated glomerular filtration rate (eGFR)). The dietary intake of Vitamin D and mean energy were assessed during an in-person 24-h dietary recall using the automated multiple-pass method.24 The following demographic data were collected by interview questionnaires: age, sex, race or ethnicity, education level, marital status, smoking and drinking status, and mean energy intake. Additionally, biospecimens were collected, processed, and stored in the mobile examination center until shipping to a laboratory for analysis. The following biomarkers were collected: data on Hb, FBG, HbA1C, HDL-C, TC, TG, BUN, sUA, Scr, and eGFR. The detailed information on the variables in this study can be found at www.cdc.gov/nchs/nhanes/.
Statistical Analysis
All analyses were performed using package R (version 4.2.0, http://www.R-project.org) and SPSS version 22.0 (SPSS Inc., Chicago, IL, USA). The serum 25(OH)D concentration was divided into quartiles (Q1, 9.37–43.2 nmol/L; Q2, 43.3–57.9 nmol/L; Q3, 58.0–72.9 nmol/L; and Q4, 73.0–250.0 nmol/L), and the lowest quartile served as the reference group (Q1). All estimates were calculated accounting for NHANES sample weights. Continuous variables are expressed as means (standard deviations, SDs), and categorical variables are presented as numbers (%). To calculate differences between groups, we used weighted linear regression models (continuous variables) and weighted chi-square tests (categorical variables). Three models were constructed, as follows: Model 1 was adjusted for age and sex; model 2 was adjusted for model 1 variables plus race/ethnicity, education level, marital status, family PIR, the complication of hypertension, DM, smoking, and drink status; model 3 was adjusted for model 2 variables plus waist circumference, SBP, DBP, mean energy intake, dietary Vitamin D intake, Hb, FBG, HbA1C, HDL-C, TC, TG, BUN, sUA, Scr, and eGFR, as the final model. A restricted cubic spline (RCS) is also used to fit the nonlinear relationship between the independent variable (iron metabolism) and the dependent variable (blood pressure). A spline curve is essentially a piecewise polynomial function that is limited by some control points, called “nodes”. Nodes are placed in multiple positions within the data range. The type of polynomial and the number and position of nodes determine the type of spline curve. In addition, the RCS model requires a minimum of three knots. A P-value of 0.05 was regarded as statistically significant.
Results
Baseline Characteristics
Table 1 shows the baseline characteristics of the research participants. The characteristics of the participants were subclassified based on serum 25(OH)D quartiles (Q1, 9.37–43.2 nmol/L; Q2, 43.3–57.9 nmol/L; Q3, 58.0–72.9 nmol/L; and Q4, 73.0–250.0 nmol/L). The prevalence of LMM in this study population was 5.3%. There is no significant difference in DBP or mean energy intake among the Q1, Q2, Q3, and Q4 groups (P >0.05). Other indicators were statistically significant among the four groups (P <0.05). Compared with the Q1, Q3, and Q4 groups, Individuals in the Q2 group had the highest levels of Hb and sUA and the lowest levels of HDL-C and TC. Participants in the Q3 group had a lower proportion of hypertension and DM. In addition, the Q4 group had the highest levels of family PIR, BUN, Scr, HDL-C, and TC and the lowest levels of eGFR and TG.
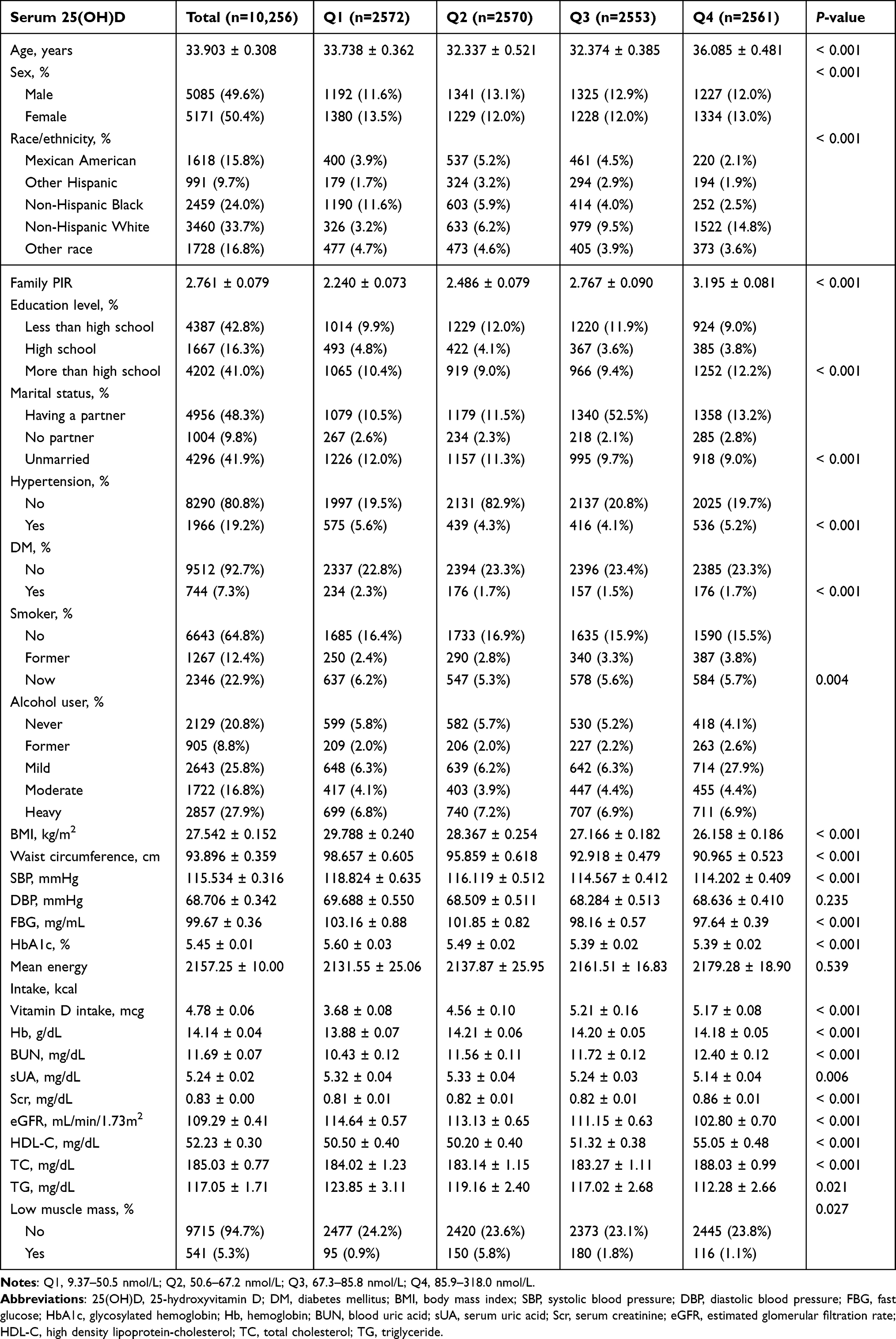 |
Table 1 Characteristics of the Study Population Based on Serum 25(OH)D Quartiles |
Association Between Serum 25(OH)D and LMM
As shown by the restricted cubic spline (RCS) plot, serum 25(OH)D is associated with a U-shaped association with the prevalence of LMM (P for nonlinearity <0.05, Figure 1). When the serum 25(OH)D concentration reached 38.5 nmol/l, the risk of LMM was the lowest. Then, as serum 25(OH)D concentration increased, so does the risk of LMM. Table 2 shows the findings of multivariate logistic regression analysis for the relationship between serum 25(OH)D concentration and LMM risk. After adjusting for interfering factors, the odds ratios with 95% confidence intervals for LMM across rising quartiles were 1.264 (0.877, 1.823), 1.978 (1.368, 2.861), and 2.186 (1.142, 2.315) for serum 25(OH)D, compared to the reference group (Q1).
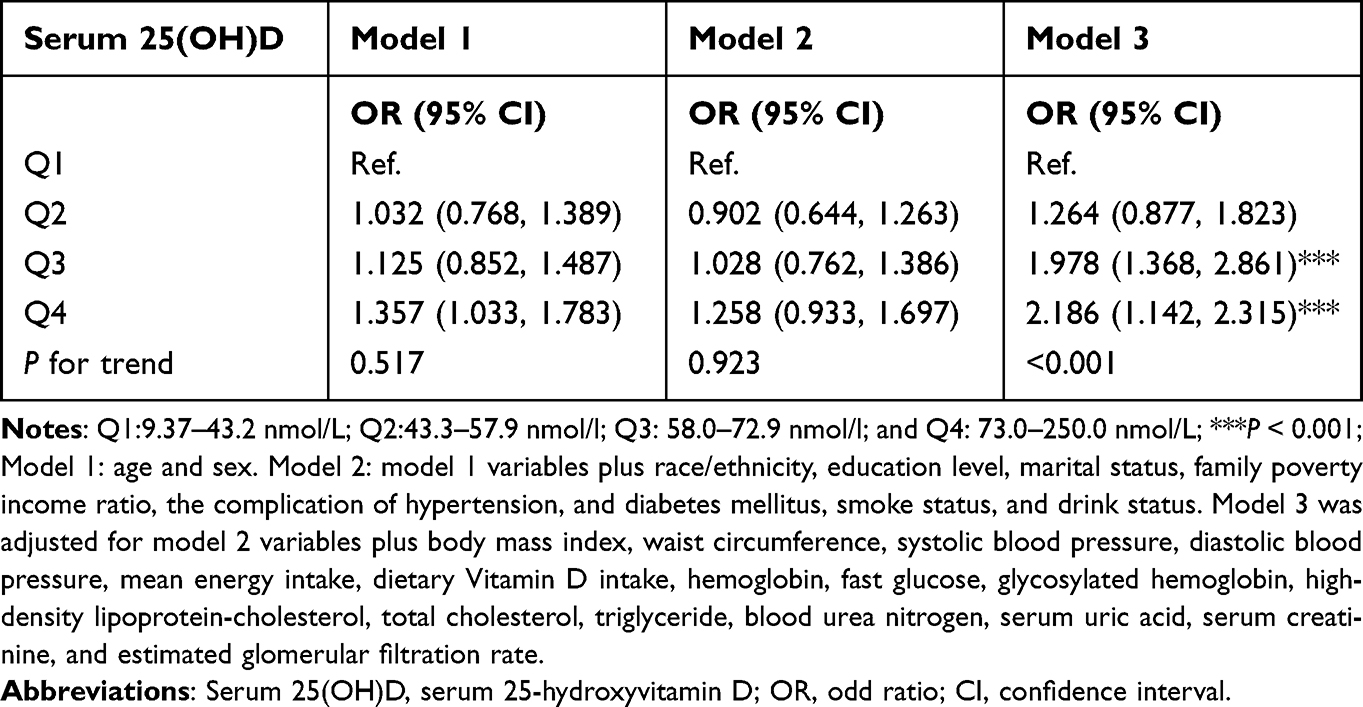 |
Table 2 Adjusted Odds Ratios for Associations Between Serum 25(OH)D and the Risk of Low Muscle Mass |
 |
Figure 1 The RCS plot of the association between serum 25(OH)D and the risk of low muscle mass. The levels of 25(OH)D were log2 transformed. Analyses were adjusted for age, sex, race/ethnicity, education level, marital status, family poverty income ratio, the complication of hypertension, and DM, body mass index, waist circumference, mean energy intake, dietary vitamin D intake, hemoglobin, fast glucose, glycosylated hemoglobin, high-density lipoprotein-cholesterol, total cholesterol, triglyceride, blood urea nitrogen, serum uric acid, serum creatinine, and estimated glomerular filtration rate. Solid and dashed lines represent the log-transformed odds ratios and the corresponding 95% confidence intervals. Abbreviations: RCS, restricted cubic spline; Serum 25(OH)D, serum 25-hydroxyvitamin D. |
Subgroup Analyses
Subgroup analyses, stratified by age, sex, hypertension, and DM were performed to estimate the association between serum 25(OH)D and LMM risk. The result of stratified subgroup analysis demonstrated the U-shaped relationship between serum 25(OH)D and risk of LMM existed in participants who were 40 years of age or older, male, with or without hypertension, and with or without DM. However, there was a linear and positive relationship between serum 25(OH)D concentration LMM risk among individuals who were < 40 years, and female (Table 3, and Figure 2). In addition, there were significant interactions for associations between age, sex, hypertension, as well as DM and serum 25(OH)D concentration (P for interaction <0.05).
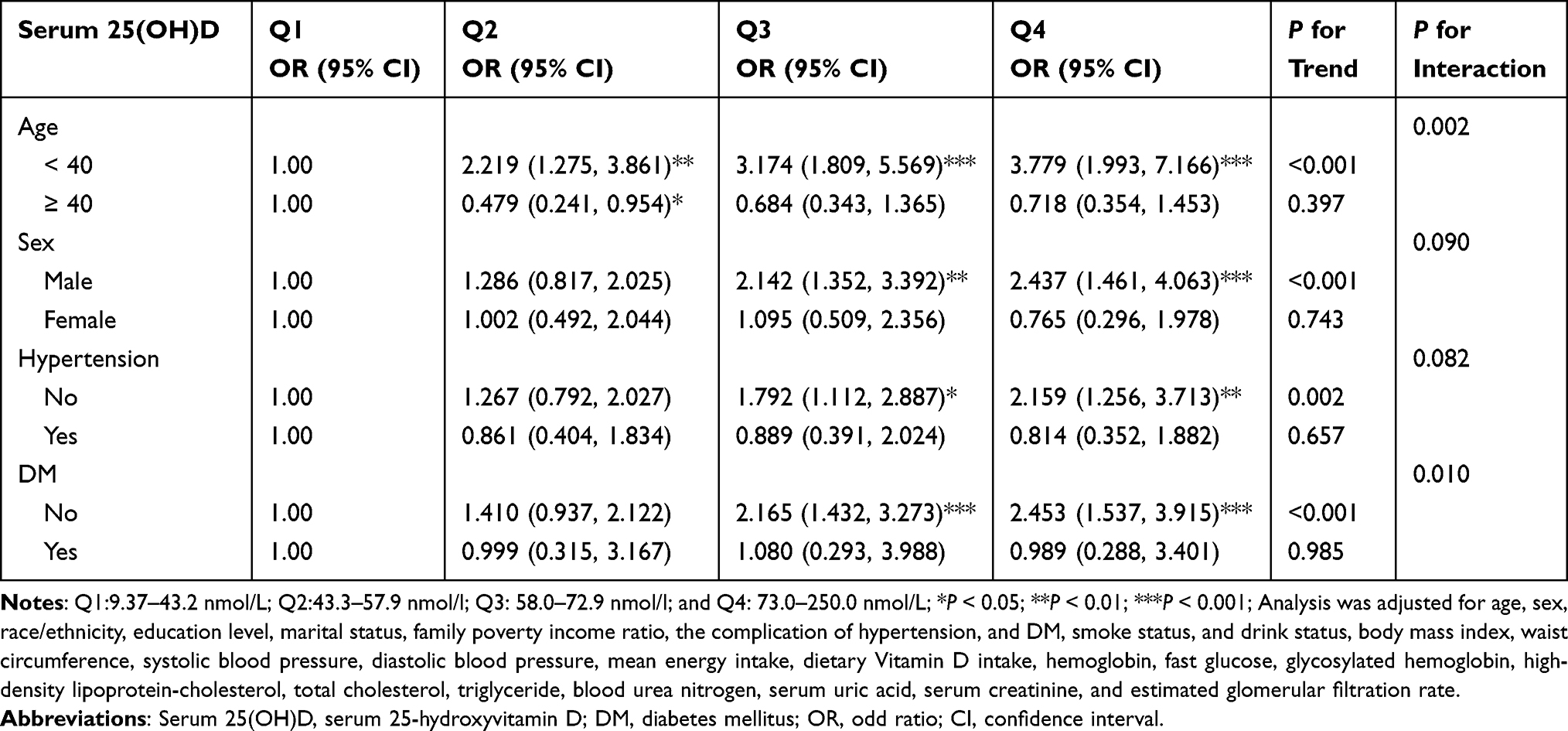 |
Table 3 Subgroups Analysis for the Associations of Serum 25(OH)D with the Risk of Low Muscle Mass |
 |
Figure 2 Subgroup analysis for the associations of serum 25(OH)D and the risk of low muscle mass based on (A) age, (B) sex, (C) hypertension, and (D) DM. The levels of 25(OH)D were log2 transformed. Analyses were adjusted for age, sex, race/ethnicity, education level, marital status, family poverty income ratio, the complication of hypertension, and DM, body mass index, waist circumference, mean energy intake, dietary vitamin D intake, hemoglobin, fast glucose, glycosylated hemoglobin, high-density lipoprotein-cholesterol, total cholesterol, triglyceride, blood urea nitrogen, serum uric acid, serum creatinine, and estimated glomerular filtration rate. Solid and dashed lines represent the log-transformed odds ratios and the corresponding 95% confidence intervals. Abbreviation: DM, diabetes mellitus. |
Discussion
Sarcopenia is a geriatric syndrome characterized by gradual and systemic muscular weakness, a decrease in muscle mass, and a drop in function. Loss of muscular strength and mobility issues are the primary symptoms, which diminish patients’ quality of life and increase their risk of falls, fractures, metabolic illnesses, and other morbidity as well as mortality.25,26 This research investigated the relationship between serum 25(OH)D and LMM risk. The study demonstrated a U-shaped relationship between serum 25(OH)D and the prevalence of LMM. Moreover, the risk of LMM was lowest when the serum 25(OH)D levels reached 38.5 nmol/L in the U. S. population.
The pathophysiological foundation of sarcopenia is an increase in pro-inflammatory cytokines in the blood, which is caused by pro-inflammatory immunogenic stimulation.27,28 Numerous studies have shown that inflammatory cytokines may activate many signaling pathways, resulting in an increase in protein catabolism and a reduction in anabolic metabolism. In addition, they may inhibit protein synthesis by lowering the levels of growth hormone and insulin-like growth factor-1, leading to skeletal muscle atrophy and ultimately sarcopenia.29 Additionally, previous studies have shown that inflammatory factors are negatively correlated with muscle strength and mass.30 Multiple in vitro investigations have shown that Vitamin D can inhibit the release of pro-inflammatory cytokines in adipose tissue, thereby reducing its chronic inflammatory response.31,32 Amer et al found that serum 25(OH)D levels less than 52.42 nmol/L were negatively correlated with C-reactive protein (CRP) levels. However, serum vitamin D levels ≥52.42 nmol/L were positively correlated with CRP levels.33 Zittermann et al found that interleukin-6, tumor necrosis factor, and high-sensitivity CRP levels decreased when vitamin D levels were significantly elevated in both the vitamin D and placebo groups.34 Previous research has shown that the anticipated response to vitamin D treatment is related to lower baseline vitamin D concentrations. The anticipated biological dosage response of vitamin D supplementation to inflammatory cytokines would vary depending on vitamin D levels at baseline.35 Aolin et al found that vitamin D supplementation inhibited the decline of muscle mass, muscle fiber and grip strength in gastritis muscle by reducing the expression of MuRF1, MAFbx and FOXO3a proteins.36 In addition, a systematic analysis shows some intervention effects of vitamin D in elderly patients with sarcopenia, but whether vitamin D supplementation has beneficial effects in patients with sarcopenia, such as inhibiting muscle atrophy and increasing muscle strength, is still controversial, in part due to the complex mechanism of the effect of vitamin D on muscle tissue.37 Studies have shown that Vitamin D supplementation could prevent and treat sarcopenia in older adults based on evidence from biological, experimental, and epidemiological studies.38 A 2009 intervention study enrolled 70-year-old community-dwelling men and women with vitamin D serum levels less than 78 nmol/l who supplemented with calcium and vitamin D daily (compared with calcium supplementation alone). Comparing the oral supplementation group to the placebo group after 12 months, the oral supplementation group demonstrated an increase in muscle strength and physical performance along with a decrease in fall rates of 27% and 39%, respectively.39 Moreover, in 2017, an observational cohort study also reported that vitamin D supplementation (20 μg a day) for 6 months in post-menopausal women with a diagnosis of osteoporosis and/or vitamin D deficiency (<30 ng/mL) was significantly correlated to an increase of appendicular muscle strength (hand grip strength and knee extension strength) and physical performance (SPPB and 4-m gait speed) with a parallel reduction in the risk of falls.40 As mentioned above, the risk of LMM was lowest when the serum 25(OH)D levels reached 38.5 nmol/L. When serum 25(OH)D levels increased (<50–≥50 nmol/L) or were persistently adequate (50 nmol/L) between baseline and follow-up visit, young and middle-aged Korean adults were less likely to develop incident low muscle mass than those with persistently low 25(OH)D levels.12 Additionally, among Korean women, lowering serum 25-OH-D by 10 ng/mL increased the risk of sarcopenia by 1.46-fold.15 With this in mind, it seems plausible to show a U-shaped association between serum 25(OH)D concentration and LMM risk in the American population, given the findings presented above.
By using subgroup analysis, we found that serum 25(OH)D concentration and risk of LMM were U-curve correlated for those 40 or older, male, with hypertension, with or without DM. However, there was a linear and positive relationship between serum 25(OH)D concentration and LMM risk among individuals who were <40 years old and female. Sarcopenia and serum 25(OH)D deficiency among elderly people have been associated with epidemiological studies.41 The aging of organs and tissues, arteriosclerosis, changes in heart function, and the connective tissue surrounding blood vessels will affect the microcirculation as the age of patients increases. Serum 25 (OH)D may decrease pro-inflammatory factor activity and ameliorate sarcopenia. In terms of gender, the incidence rate in women was 16% compared to 11% in men, which may be related to the fact that women live longer and have higher disability rates.42 Simultaneously, there are considerable gender disparities in immune response homeostasis and the risk of age-related illnesses. Decreased estrogen levels impact the skeletal musculoskeletal system, which is also one of the causes of the high prevalence of sarcopenia among women.43
The levels of vitamin D are closely related to autoimmune diseases, including rheumatoid arthritis, spondylarthritis, systemic sclerosis, inflammatory bowel disease, and autoimmune diabetes, and play an important role in the pathophysiology and treatment of these conditions.44,45 There was an average increase in parathyroid hormone (PTH) concentration for any plasma 25(OH) vitamin D range among patients with autoimmune rheumatic diseases (ARD), which suggests that vitamin D metabolism is impaired.46 In addition, the results of a prospective, population-based study revealed that older men and women with lower 25(OH)D concentrations and higher PTH levels are more likely to suffer from sarcopenia.47 A history of ARD is not associated with a lower serum 25(OH)vitamin D concentration or influences its increments after vitamin D supplementation. Among rheumatic patients, hypovitaminosis D is very common, especially among women and the elderly. Moreover, supplementation with vitamin D at 750–1000 IU daily is insufficient to normalize 25(OH)vitamin D values, so higher dose regimens should be considered.48
Sarcopenia is a global age-related disease affected by chronic inflammation, physical activity, nutritional status, hormones, and other factors. The specific pathogenesis of sarcopenia remains unclear. Therefore, more basic and clinical studies are needed to further explore the pathogenesis and intervention of sarcopenia in the future. Through the study, we found that appropriate vitamin D supplementation can reduce the incidence of sarcopenia. The strength of the current research was to include a representative sampling design and a rigorous and standard protocol for data collection, which made our results of a U-shaped relationship between serum 25(OH)D concentration and risk of LMM more reliable. In addition, leveraging the extensive set of covariates and large sample size in the NHANES, we could have performed multiple subgroup analyses in accordance with participants’ characteristics. Of note, our study had some limitations. First, all of the patients we utilized for analysis came from the NHANES public database, which spanned the years 2011 to 2014. Participants from other nations should be further employed to corroborate our findings, particularly the inflection point (38.5 nmol/L). Second, as a retrospective study, bias cannot be avoided in some relevant results. Third, when investigating the relationship between 25(OH)D and LMM in this population, the results could be biased. In young people, sarcopenia may be related to some acute disease, while in older adults, it is due to aging. Finally, the underlying mechanism of Serum 25(OH)D and the prevalence of LMM must also be studied.
Conclusion
In conclusion, there was a U-shaped relationship between serum 25(OH)D and the risk of LMM. In our study, an inflection point for serum 25(OH)D was observed, and the prevalence of LMM was lowest when the serum 25(OH)D level was 38.5 nmol/L. Appropriate vitamin D supplementation can reduce the prevalence of LMM.
Data Sharing Statement
The NHANES data are publicly available on the internet for data users and researchers (https://www.cdc.gov/nchs/nhanes/).
Ethics Approval and Informed Consent
The NHANES 2011–2014 was approved by the NCHS Research Ethics Review Board (Continuation of Protocol #2011–2014), and each participant signed the written informed consent. In addition, the study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of the First Affiliated Hospital of Anhui Medical University. Due to the retrospective and public nature of the study data, the review board waived the requirement for written informed consent.
Acknowledgments
We thanks to the staff and the participants of the NHANES study for their valuable contributions.
Funding
The project was supported by the School Foundation of Anhui Medical University (2021xkj065), and Scientific Research and Cultivation Foundation of Anhui Public Health Clinical Center, The Frist Affiliated Hospital of Anhui Medical University North District [No.2023YKJ08 to G.Z].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rosenberg IH. Sarcopenia: origins and clinical relevance. J Nutr. 1997;127(5 Suppl):990s–991s. doi:10.1093/jn/127.5.990S
2. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in Older People. Age Ageing. 2010;39(4):412–423. doi:10.1093/ageing/afq034
3. Cruz-Jentoft AJ, Sayer AA. Sarcopenia. Lancet. 2019;393(10191):2636–2646. doi:10.1016/S0140-6736(19)31138-9
4. Chang CD, Wu JS, Mhuircheartaigh JN, et al. Effect of sarcopenia on clinical and surgical outcome in elderly patients with proximal femur fractures. Skeletal Radiol. 2018;47(6):771–777. doi:10.1007/s00256-017-2848-6
5. Cruz-Jentoft AJ, Kiesswetter E, Drey M, Sieber CC. Nutrition, frailty, and sarcopenia. Aging Clin Exp Res. 2017;29(1):43–48. doi:10.1007/s40520-016-0709-0
6. Casati M, Costa AS, Capitanio D, et al. The biological foundations of sarcopenia: established and promising markers. Front Med. 2019;6:184. doi:10.3389/fmed.2019.00184
7. Cranney A, Weiler HA, O’Donnell S, Puil L. Summary of evidence-based review on vitamin D efficacy and safety in relation to bone health. Am J Clin Nutr. 2008;88(2):513s–9s. doi:10.1093/ajcn/88.2.513S
8. Naesgaard PA, León De La Fuente RA, Nilsen ST, et al. Serum 25(OH)D is a 2-year predictor of all-cause mortality, cardiac death and sudden cardiac death in chest pain patients from Northern Argentina. PLoS One. 2012;7(9):e43228. doi:10.1371/journal.pone.0043228
9. Freedman LP. Transcriptional targets of the vitamin D3 receptor-mediating cell cycle arrest and differentiation. J Nutr. 1999;129(2S Suppl):581s–6s. doi:10.1093/jn/129.2.581S
10. Bischoff HA, Borchers M, Gudat F, et al. In situ detection of 1,25-dihydroxyvitamin D3 receptor in human skeletal muscle tissue. Histochem J. 2001;33(1):19–24. doi:10.1023/A:1017535728844
11. Mizuno T, Hosoyama T, Tomida M, et al. Influence of vitamin D on sarcopenia pathophysiology: a longitudinal study in humans and basic research in knockout mice. J Cachexia Sarcopenia Muscle. 2022;13(6):2961–2973. doi:10.1002/jcsm.13102
12. Kim Y, Chang Y, Ryu S, et al. Serum 25-hydroxy vitamin D and the risk of low muscle mass in young and middle-aged Korean adults. Eur J Endocrinol. 2022;186(4):477–487. doi:10.1530/EJE-21-1229
13. Ko MJ, Yun S, Oh K, Kim K. Relation of serum 25-hydroxyvitamin D status with skeletal muscle mass by sex and age group among Korean adults. Br J Nutr. 2015;114(11):1838–1844. doi:10.1017/S0007114515003633
14. Kim MK, Baek KH, Song KH, et al. Vitamin D deficiency is associated with sarcopenia in older Koreans, regardless of obesity: the fourth Korea National Health and Nutrition Examination Surveys (KNHANES IV) 2009. J Clin Endocrinol Metab. 2011;96(10):3250–3256. doi:10.1210/jc.2011-1602
15. Park S, Ham JO, Lee BK. A positive association of vitamin D deficiency and sarcopenia in 50 year old women, but not men. Clin Nutr. 2014;33(5):900–905. doi:10.1016/j.clnu.2013.09.016
16. Lee JH, Kim S, Kim MK, et al. Relationships between 25(OH)D concentration, sarcopenia and HOMA-IR in postmenopausal Korean women. Climacteric. 2018;21(1):40–46. doi:10.1080/13697137.2017.1395410
17. Xiao S, Zhou Y, Wu Q, et al. Prevalence of cardiovascular diseases in relation to total bone mineral density and prevalent fractures: a population-based cross-sectional study. Nutr Metab Cardiovasc Dis. 2022;32(1):134–141. doi:10.1016/j.numecd.2021.09.009
18. Golabi P, Gerber L, Paik JM, Deshpande R, de Avila L, Younossi ZM. Contribution of sarcopenia and physical inactivity to mortality in people with non-alcoholic fatty liver disease. JHEP Rep. 2020;2(6):100171. doi:10.1016/j.jhepr.2020.100171
19. Cromwell EA, Osborne JCP, Unnasch TR, et al. Predicting the environmental suitability for onchocerciasis in Africa as an aid to elimination planning. PLoS Negl Trop Dis. 2021;15(7):e0008824. doi:10.1371/journal.pntd.0008824
20. Zipf G, Chiappa M, Porter KS, Ostchega Y, Lewis BG, Dostal J. National health and nutrition examination survey: plan and operations, 1999–2010. Vital Health Stat. 2013;56:1–37.
21. Batsis JA, Mackenzie TA, Emeny RT, Lopez-Jimenez F, Bartels SJ. Low lean mass with and without obesity, and mortality: results from the 1999–2004 national health and nutrition examination survey. J Gerontol A Biol Sci Med Sci. 2017;72(10):1445–1451. doi:10.1093/gerona/glx002
22. Rippberger PL, Emeny RT, Mackenzie TA, Bartels SJ, Batsis JA. The association of sarcopenia, telomere length, and mortality: data from the NHANES 1999–2002. Eur J Clin Nutr. 2018;72(2):255–263. doi:10.1038/s41430-017-0011-z
23. Studenski SA, Peters KW, Alley DE, et al. The FNIH sarcopenia project: rationale, study description, conference recommendations, and final estimates. J Gerontol A Biol Sci Med Sci. 2014;69(5):547–558. doi:10.1093/gerona/glu010
24. Moshfegh AJ, Rhodes DG, Baer DJ, et al. The US department of agriculture automated multiple-pass method reduces bias in the collection of energy intakes. Am J Clin Nutr. 2008;88(2):324–332. doi:10.1093/ajcn/88.2.324
25. Larsson L, Degens H, Li M, et al. Sarcopenia: aging-related loss of muscle mass and function. Physiol Rev. 2019;99(1):427–511. doi:10.1152/physrev.00061.2017
26. Welch C, Hassan-Smith ZH, Greig CA, Lord JM, Jackson TA. Acute sarcopenia secondary to hospitalisation - an emerging condition affecting older adults. Aging Dis. 2018;9(1):151–164. doi:10.14336/AD.2017.0315
27. Wiedmer P, Jung T, Castro JP, et al. Sarcopenia - molecular mechanisms and open questions. Ageing Res Rev. 2021;65:101200. doi:10.1016/j.arr.2020.101200
28. Tournadre A, Vial G, Capel F, Soubrier M, Boirie Y. Sarcopenia. Joint Bone Spine. 2019;86(3):309–314. doi:10.1016/j.jbspin.2018.08.001
29. Koshikawa M, Harada M, Noyama S, et al. Association between inflammation and skeletal muscle proteolysis, skeletal mass and strength in elderly heart failure patients and their prognostic implications. BMC Cardiovasc Disord. 2020;20(1):228. doi:10.1186/s12872-020-01514-0
30. Hida T, Imagama S, Ando K, et al. Sarcopenia and physical function are associated with inflammation and arteriosclerosis in community-dwelling people: the Yakumo study. Mod Rheumatol. 2018;28(2):345–350. doi:10.1080/14397595.2017.1349058
31. Gao D, Trayhurn P, Bing C. 1,25-dihydroxyvitamin D3 inhibits the cytokine-induced secretion of MCP-1 and reduces monocyte recruitment by human preadipocytes. Int J Obes. 2013;37(3):357–365. doi:10.1038/ijo.2012.53
32. Wamberg L, Cullberg KB, Rejnmark L, Richelsen B, Pedersen SB. Investigations of the anti-inflammatory effects of vitamin D in adipose tissue: results from an in vitro study and a randomized controlled trial. Horm Metab Res. 2013;45(6):456–462. doi:10.1055/s-0032-1331746
33. Amer M, Qayyum R. Relation between serum 25-hydroxyvitamin D and C-reactive protein in asymptomatic adults (from the continuous national health and nutrition examination survey 2001 to 2006). Am J Cardiol. 2012;109(2):226–230. doi:10.1016/j.amjcard.2011.08.032
34. Zittermann A, Frisch S, Berthold HK, et al. Vitamin D supplementation enhances the beneficial effects of weight loss on cardiovascular disease risk markers. Am J Clin Nutr. 2009;89(5):1321–1327. doi:10.3945/ajcn.2008.27004
35. Heaney RP. Vitamin D--baseline status and effective dose. N Engl J Med. 2012;367(1):77–78. doi:10.1056/NEJMe1206858
36. Li CW, Yu K, Shyh-Chang N, et al. Circulating factors associated with sarcopenia during ageing and after intensive lifestyle intervention. J Cachexia Sarcopenia Muscle. 2019;10(3):586–600. doi:10.1002/jcsm.12417
37. Singh NA, Quine S, Clemson LM, et al. Effects of high-intensity progressive resistance training and targeted multidisciplinary treatment of frailty on mortality and nursing home admissions after hip fracture: a randomized controlled trial. J Am Med Dir Assoc. 2012;13(1):24–30. doi:10.1016/j.jamda.2011.08.005
38. Remelli F, Vitali A, Zurlo A, Volpato S. Vitamin D deficiency and sarcopenia in older persons. Nutrients. 2019;11(12):2861. doi:10.3390/nu11122861
39. Brouwer-Brolsma EM, Bischoff-Ferrari HA, Bouillon R, et al. Vitamin D: do we get enough? A discussion between vitamin D experts in order to make a step towards the harmonisation of dietary reference intakes for vitamin D across Europe. Osteoporos Int. 2013;24(5):1567–1577. doi:10.1007/s00198-012-2231-3
40. Bischoff-Ferrari HA. Optimal serum 25-hydroxyvitamin D levels for multiple health outcomes. Adv Exp Med Biol. 2014;810:500–525. doi:10.1007/978-1-4939-0437-2_28
41. Kim JA, Hwang SY, Yu JH, et al. Association of the triglyceride and glucose index with low muscle mass: KNHANES 2008–2011. Sci Rep. 2021;11(1):450. doi:10.1038/s41598-020-80305-1
42. Launer LJ, Harris T, Rumpel C, Madans J. Body mass index, weight change, and risk of mobility disability in middle-aged and older women. the epidemiologic follow-up study of NHANES I. JAMA. 1994;271(14):1093–1098. doi:10.1001/jama.1994.03510380049036
43. Berghella AM, Contasta I, Marulli G, et al. Ageing gender-specific “Biomarkers of Homeostasis”, to protect ourselves against the diseases of the old age. Immun Ageing. 2014;11(1):3. doi:10.1186/1742-4933-11-3
44. Bellan M, Andreoli L, Mele C, et al. Pathophysiological role and therapeutic implications of vitamin D in autoimmunity: focus on chronic autoimmune diseases. Nutrients. 2020;12(3):789. doi:10.3390/nu12030789
45. An HJ, Tizaoui K, Terrazzino S, et al. Sarcopenia in autoimmune and rheumatic diseases: a comprehensive review. Int J Mol Sci. 2020;21(16):5678. doi:10.3390/ijms21165678
46. Sainaghi PP, Bellan M, Antonini G, Bellomo G, Pirisi M. Unsuppressed parathyroid hormone in patients with autoimmune/inflammatory rheumatic diseases: implications for vitamin D supplementation. Rheumatology. 2011;50(12):2290–2296. doi:10.1093/rheumatology/ker314
47. Visser M, Deeg DJ, Lips P. Low vitamin D and high parathyroid hormone levels as determinants of loss of muscle strength and muscle mass (sarcopenia): the longitudinal aging study Amsterdam. J Clin Endocrinol Metab. 2003;88(12):5766–5772. doi:10.1210/jc.2003-030604
48. Sainaghi PP, Bellan M, Carda S, et al. Hypovitaminosis D and response to cholecalciferol supplementation in patients with autoimmune and non-autoimmune rheumatic diseases. Rheumatol Int. 2012;32(11):3365–3372. doi:10.1007/s00296-011-2170-x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association of Systemic Immune-Inflammation Index with Non-Alcoholic Fatty Liver Disease: A Population-Based Cross-Sectional Study
Zhao B, Liu Y, Yang Y, He J
Risk Management and Healthcare Policy 2023, 16:1581-1592
Published Date: 16 August 2023
Association Between Triglyceride-Glucose Index and Hearing Threshold Shifts of Adults in the United States: National Health and Nutrition Examination Survey, 2015–2016
Pan JY, Chen Y, Lin ZH, Lv B, Chen L, Feng SY
Journal of Multidisciplinary Healthcare 2024, 17:1791-1801
Published Date: 23 April 2024
Association Between Composite Dietary Antioxidant Index and Endometriosis from NHANES 2001–2006: A Cross-Sectional Study
Xu X, Wu H, Liu Y
International Journal of Women's Health 2024, 16:1845-1854
Published Date: 5 November 2024
Association Between Nephrolithiasis and the Prevalence of Sarcopenia in Chinese Older Adults: A Cross-Sectional Study Using Propensity Score Matching
Wu C, Li XQ, Lu SS, Shen ZK, Lu X
Clinical Interventions in Aging 2025, 20:2353-2362
Published Date: 2 December 2025