")
Back to Journals » Infection and Drug Resistance » Volume 17
Two Cases of Superficial Fungal Infection Caused by Non-Albicans Candida Species Manifest Greenish-black Discoloration
Received 28 September 2023
Accepted for publication 22 January 2024
Published 19 February 2024 Volume 2024:17 Pages 665—672
DOI https://doi.org/10.2147/IDR.S438079
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Leyao Shi,1 Yahui Feng,2 Dongmei Shi2,3
1The Second Clinical Medical College, Shandong University of Traditional Chinese Medicine, Jinan, Shandong, People’s Republic of China; 2The Laboratory of Medical Mycology, Jining No. 1 People’s Hospital, Jining, Shandong, People’s Republic of China; 3Department of Dermatology, Jining No. 1 People’s Hospital, Jining, Shandong, People’s Republic of China
Correspondence: Dongmei Shi, Department of Dermatology, Jining No. 1 People’s Hospital, No. 6 Jiankang Road, Jining, Shandong Province, 272000, People’s Republic of China, Tel +86 537-6051008, Email [email protected]
Abstract: The clinical manifestation of superficial candidiasis varies depending on the infectious sites and causative Candida species that brings a great challenge to diagnose or treat without mycological or pathological evidence in clinical settings. Oral mucosal candidiasis and onychomycosis are most common types of superficial candidiasis. Typically, oral mucosal candidiasis manifests as white or erythematous thrush coated on the tongue and other interior oral cavity; and onychomycosis caused by Candida spp. presents with thick, fragile, or cracked fingernails or toenails in yellow or white discoloration. Here, we report one case of patient with a black hairy tongue caused by Candida tropicalis and one case of greenish discolored onychomycosis caused by Candida parapsilosis. The cases of superficial candidiasis with the same discolored lesions were searched in literature and compared with our cases in clinical manifestation, causative pathogen and treatment. These cases highlight the importance of mycological diagnosis for identifying non-Candida albicans Candida species (NCAC) in superficial infections to guide an effective therapy.
Keywords: Candida tropicalis, Candida parapsilosis, onychomycosis, black hairy tongue, nail discoloration
Introduction
Candida spp. is one of the most common causes of superficial and life-threatening systemic fungal diseases. Among the array of superficial fungal infections, notable examples include oral mucosal infections and onychomycosis.1 Candida albicans remains the most common species to cause superficial infections that is in consistence with its popular colonization in mucosal sites.2 Approximately half of all healthy individuals are carriers of Candida in their oral cavities at a nonpathogenic yeast state.3 The risk factors that favor yeast-to-pathogenic hyphae include broad-spectrum antibiotic therapy, corticosteroids, immune suppression, diabetes mellitus and nutritional deficiencies.4–6 Nevertheless, over the last 10–30 years non-Candida albicans Candida species (NCAC) have emerged as significant opportunistic human pathogens. Although C. albicans remains the predominant causative agent, the NCAC species are increasingly prevalent in specific patient groups, particularly among neutropenic patients.7,8
Their clinical manifestations of superficial candidiasis vary depending on the infective sites and causative Candida species, which could bring the great challenge to diagnose sometimes in clinical settings when based only on clinical presentations.9 Typically, oral mucosal candidiasis manifests as pseudomembranous thrush that is white coating or curdish patches on the tongue or other interior oral cavity.2 The clinical manifestations of onychomycosis caused by Candida spp. often present with thick, fragile, or cracked fingernails or toenails in yellow or white discoloration, which are not distinct from nail infections by dermophyte species.10 Here we present two cases of superficial candidiasis who presented with green-black changes on tongue and nails caused by non-Candida albicans Candida species.
Case Presentation
Case 1
A 50-year-old female patient was initially diagnosed with chronic myelogenous leukemia (CML), and received a genotypically matched hematopoietic stem cell transplantation donated by her brother. Seven months later, she was admitted to our hospital for developed graft versus host disease (GVHD). Patient noted that her tongue started turning black with a hairy appearance at the same time. She had no itch or pain and the lesion had no effect on the movements of mouth and tongue. The patient denies other oral hygiene illness and smoking in the past.
The physical examination revealed a greenish-black discolored patch covering the tongue with elongated “hair” on the dorsal side of tongue (Figure 1). The discolored lesion is 3×5 cm in size and surrounded by irregular white pseudomembranous patches. The hairy appearance is more pronounced in the middle of the dark greenish area. Specimen tissue was taken from the discolored area using a sterile blunt scalpel by alcohol pad and divided into two portions. One portion of specimen was stained with calcofluor-white fluorescent. A large number of spores and hyphae were found under florescent microscopy (Figure 2A). The second portion of specimen was inoculated on blood agar (BA) for bacterial growth and Sabouraud’s Dextrose Agar (SDA) and Potato Dextrose Agar (PDA) supplemented with chloramphenicol for fungal pathogens. All cultures remained in 27°C incubator. By day 3, the large amounts of cream-colored yeast-like colonies appears on SDA and PDA (Figure 2B), but few bacterial colonies were found. The fugal species obtained from isolation underwent identification through sequencing the internal transcribed spacer (ITS) and beta-tubulin (TB) gene, using the following primer sets: ITS1 (5′-TCCGTAGGTGAACCTGCGG-3′), ITS4 (5′-TCCTCCGCTTATTGATATGC-3), β-tubulin 2a (5′-AATTGGTGCCGCTTTCTGG-3′) and β-tubulin 2b (5′-AGTTGTCGGGACGGAATAG-3′).11 Following purification, the PCR products were sequenced, and upon a mega blast search of the ITS sequence in NCBI’s GenBank (https://blast.ncbi.nlm.nih.gov/Blast.cgi), our isolates were determined to be most closely related to Candida tropicalis (GenBank KC422426.1).
 |
Figure 1 Black hairy tongue on the dorsum of the tongue. |
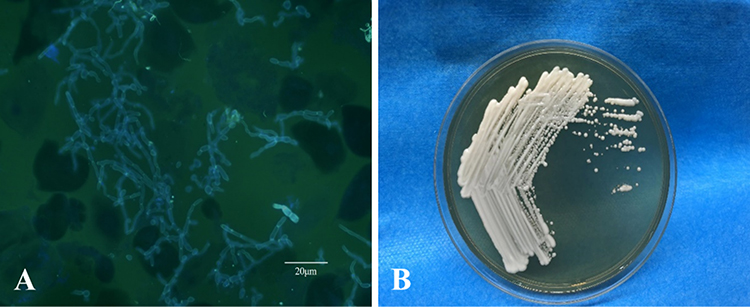 |
Figure 2 Direct fluorescence microscopy showed blastospores and pseudohyphae (A); On Sabourauds glucose agar at 27°C, cream-colored yeast-like colonies first developed in 3 days (B). |
The patient was diagnosed as black hairy tongue caused by C. tropicalis and anti-fungal treatment initiated right after diagnosis. Patient was given oral itraconazole 200 mg once a day and the black coloration of the tongue disappeared after 3 days’ treatment.
Case 2
A 52-year-old woman reported to the Department of Dermatology with a chief complaint of thickening and discoloration on her right thumbnail, the big and little toenails on her right foot, and the middle and little toenails of the left foot for 5 months duration (Figure 3A). She had no significant past medical condition and drug-used history. There was no nail trauma before the onset of nail infection. The patient received an empirical treatment regimen involving oral itraconazole at a dose of 200 mg twice daily for one week, followed by a 3-week interruption in each 4-week cycle. Notably, after months of treatment, a significant improvement was observed in the lesion on her toenails. However, there was no discernible improvement in her thumbnail. Instead, the affected area on the thumbnail exhibited an increase in size and greenish-black hue (Figure 3B). In addition, a noticeable distal onycholysis, characterized by the detachment of the nail plate, was observed when examining the inferior surface of the discolored nail.
 |
Figure 3 The lesion covered half of the outer edge of the nail plate with yellowish discoloration (A), after 3 months of therapy, and her thumbnail presented with green-black discoloration (B). |
Microscopic examination revealed sub-spherical budding yeast-like cells but no presence of pseudohyphae or hyphae structure in the specimen collected from her right thumbnail (Figure 4A). However, mycelium was easily found on her affected toenails. Based on direct microscopic results, the case was initially diagnosed as onychomycosis caused by dermatophytes.
 |
Figure 4 Microscopic examination revealed sub-spherical budding yeast-like cells without pseudohyphae structure (A); Three days later at 27°C, creamy yeastlike colonies appeared on SDA plate (B). |
Clinical laboratory tests found no apparent abnormality in blood works. Physical examination showed a diffuse green discoloration on the nail plate extending to the proximal nail fold and distal onycholysis in affected right thumbnail. Specimen was collected and cultured on BA and SDA plate containing chloramphenicol at 27°C. Bacterial culture on BA was negative after 3 days. Repeated fluorescent microscopy examination of the nail samples revealed the same fungal structures as shown in Figure 4A. The repeated cultures yielded the same yeast-like colony appearance (Figure 4B). Despite multiple collection attempts, the analysis consistently confirmed the presence of the same fungus species. Morphological features and molecular sequencing, as described in Case 1, consistently identified C. parapsilosis as the causative agent responsible for the infection in the right thumbnail.
Antifungal susceptibility testing was performed following the Clinical and Laboratory Standards Institute M27-A3 protocol. The broth microdilution method was employed to test eight different agents against the isolate strain.12 The minimum inhibitory concentrations (MIC) were 1.0 μg/mL for itraconazole, 0.125 μg/mL for voriconazole, 1.0 μg/mL for amphotericin B, 0.25 μg/mL for posaconazole, 4.0 μg/mL for nystatin, 1.0 μg/mL for micafungin, 1.0 μg/mL for fluconazole, but greater than 0.5 μg/mL for terbinafine. After the drug sensitivity tests, treatment was changed to oral fluconazole 150 mg weekly for 3 months and nail discoloration faded and the new nail has no sign of relapse at one month follow-up.
Antifungal susceptibility testing was conducted following the Clinical and Laboratory Standards Institute M27-A3 protocol. The broth microdilution method was employed to test eight different agents against the isolated strain.
Discussion
We report a case of black hairy tongue caused by C. tropicalis in a immunocom-promised patient and a case of onychomycosis caused by C. parapsilosis in an otherwise healthy patient. Both cases are characterized by greenish-black lesions and good responses to azole antifungal treatment. The greenish-black discoloration caused by Candida spp. are less common in oral and skin fungal infection than pigment-producing bacterial and fungal pathogens, such as Aspergillus spp. and Pseudomonas spp.
Black hairy tongue (BHT) is often recognized by its distinctive black color as shown in Case 1. In Case 1, the painless black hair-like lesion appeared on the dorsum of the tongue anterior to the circumvallate papillae. BHT is a benign medical condition characterized by elongated filiform lingual papillae with typical carpet-like appearance on the dorsum of the tongue. The hairy surface of infected tongue can be accompanied with discoloration ranging from blackish-brown to yellowish green or unpigmented color.6 For HBT caused by Candida spp., the main manifestations include loss of papillae on the dorsal tongue, erythematous patches and fissuring of the tongue, and may extend to other mucosal surfaces or the corners of mouth (angular cheilitis).13 Generally speaking, BHT does not occur on the tip or sides of the tongue. The differential diagnosis for BHT include variant bacterial and fungal infections and unfortunately there are no distinct symptoms to indicate the fungal origin.14
Review of the medical literature shows that BHT is not uncommon, incidence ranges from 0.6% to 18% in different study populations.15,16 The etiology of BHT remains unclear and is likely multifactorial, resulting from combination of local and systemic insults. Many noninfectious predisposition factors are associated with BHT-like manifestation such as smoking, irritants to lead to a poor oral hygiene and cancer such as acanthosis nigricans and oral hairy leukoplakia. Previous clinical observations have linked heavy tobacco use to an increased risk of BHT.17,18
A comprehensive search of online databases, including PubMed and Web of Science, was conducted. In addition, the reference lists of all retrieved articles, including review articles, were examined. The search spanned 2000 to 2022, and the following terms were used: “black hairy tongue”, “black tongue”, “hyperpigmented tongue”, “lingua villosa nigra”, and “hairy tongue”. In total, six cases of Candida-related BHT were found in our literature search. The clinical characteristics of patients with Candida-related BHT are listed in Table 1. Of the six patients,19–24 two were male and four were female. The patients’ ages ranged from 3 months to 106 years old. Four patients with poor oral hygiene had one or two risk factors listed above for BHT, including smoking, drinking alcohol and coffee, and edentulism. The mycological identification found that none of them were caused by Candida tropicalis. All six patients responded well to antifungal therapy and ful recovery from BHT was achieved with by practicing good oral hygiene. It is worth noting that two articles have pointed out that allogeneic stem cell transplantation is also associated with the occurrence of BHT,25,26 the same as our reported Case 1 in this study.
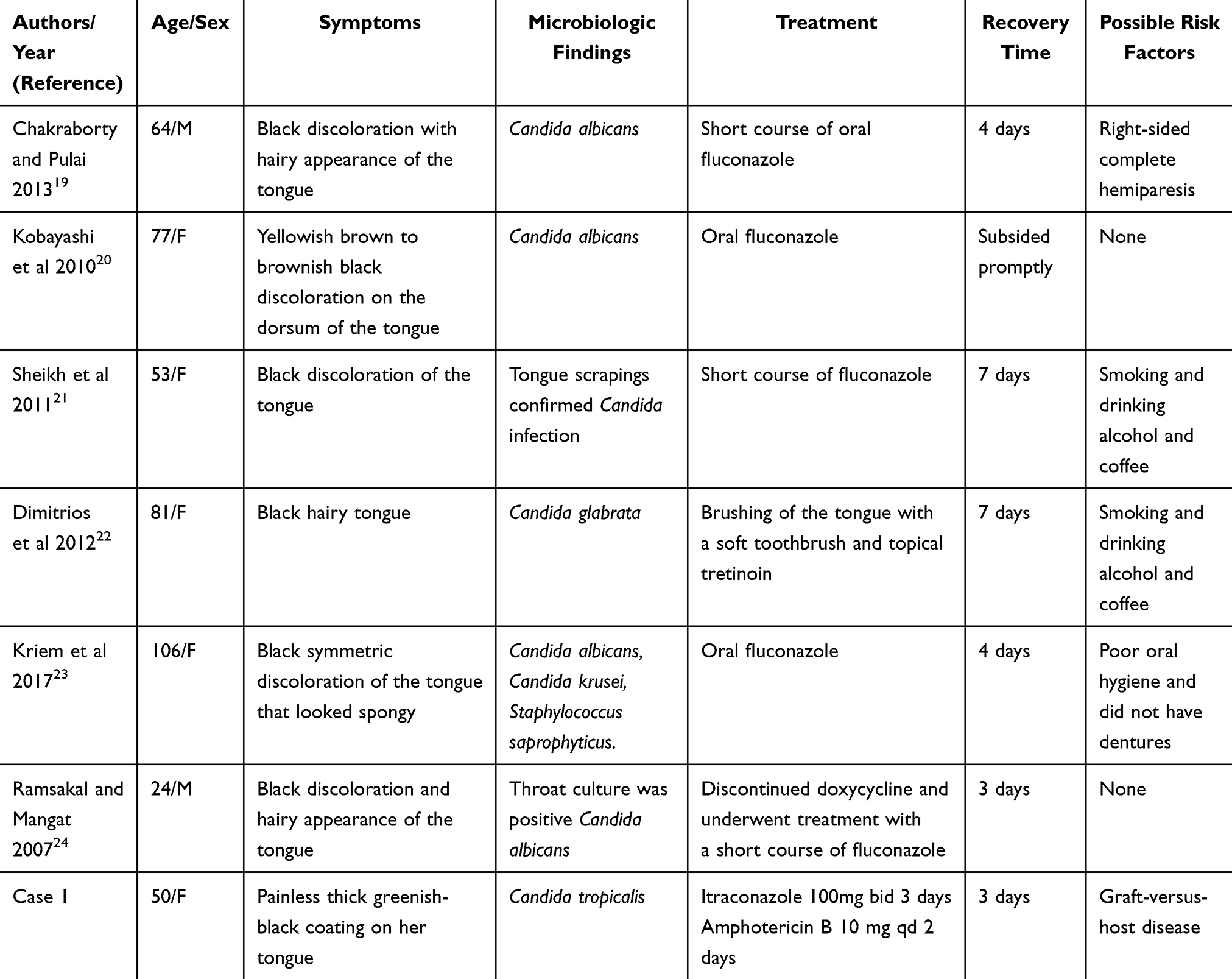 |
Table 1 The Cases Diagnosed with Black Hairy Tongue |
Use of systemic and local medications may induce or exacerbate BHT condition. Antibiotics associated with this disorder are linezolid, penicillin and erythromycin, and others.27–29 Yet the mechanisms to develop black hairy tongue with antibiotics are not known. It may be possible that antibiotic use alters the oral microbiota. Furthermore, the pronounced anatomical alteration in the filiform papillae may predispose the patient to trap foreign material or stimulate certain microbial overgrowth, leading to the typical color change in patients with BHT. One bacterium capable of producing the aforementioned findings is the porphyrin-producing black-pigmented gram-negative anaerobic rod Porphyromonas gingivalis, known for its implication in chronic periodontitis.30,31 However, this is an entirely speculative theory and which fails to explain the cases where the discoloration is yellow, green, or light color texture. Although it is not as common as C. albicans, C. tropicalis can be isolated from the oral cavities. However, the specific mechanism of microflora such as C. tropicalis-related to that found in a greenish-black discolor BHT is still unclear.19
Onychomycosis clinically presents with nail discoloration in a spectrum of white, yellow, and brown where the fungus is dense. The nail separation from the nail bed (onycholysis), brittleness, nail thickening, and subungual accumulation of scale are common symptoms.10 For onychomycosis caused by Candida spp., the discoloration also ranging from white, yellow to yellowish brown.9 The clinical presentation of Case 2 caused by C. parapsilosis presented with an atypical color from those described in the literature. The greenish-black discoloration only appeared in the right thumbnail, but not in other nails. Although such dark discoloration by C. parapsilosis has been reported previously,32 the exact mechanism remains unclear. However, previous studies have found melanin presence in conidia of C. parapsilosis,33 which may explain the dark colored lesions in this case.
A search of the online databases PubMed and Web of Science as well as the reference lists of all retrieved articles was performed for articles published from 2000 to 2022. The search terms were “Candida & Onychomycosis & green”, and “Candida & Onychomycosis & black”. After a review of the literature, it was found that some cases showed green or black skin and nail lesions caused by Candida spp. that are similar to Case 2.32–40 Of note is fungal melanonychia, a rare nail disorder that presents as a longitudinal dark pigmentation in the nail plate. The causative Candida-associated fungal melanonychia were Candida albicans and NCAC.33–40 These isolated Candida were considered to be the cause of the discoloration rather than a colonized status.41,42 In addition, some researchers have even introduced a term, viridionychia to specifically describe fungal etiology-associated green nail syndrome,32 which differs from chloronychia with bacterial-associated green nail syndrome. Interestingly, the proposed viridionychia term was based on a fungal nail infection caused by Candida parapsilosis. Although some Candida spp. such as C. parapsilosis may produce more melanin than others, melanonychia may commonly results from the activation of host melanocytes within the inflammatory area of the nailfold.43
It is worth mentioning that, green nail syndrome may be differentiated from a paronychial infection due to bacterial pathogens such as Pseudomonas aeruginosa, or mixture of bacterial and fungal pathogens, which often results in the same green discoloration on the nail plate.44,45 P. aeruginosa is a gram-negative coccobacillus with a predilection for moist, aquatic environments. It produces pyocyanin and pyoverdine, which are pigmented virulence factors that give its characteristic blue-green color in green nail syndrome.46 However, when P. aeruginosa is associated with green nail discoloration, it is usually described as Goldman–Fox syndrome.47 To the best of our knowledge, fungal-associated green nail syndrome are less common than bacterial origins.48 This may be related to the fact that P. aeruginosa has been shown to inhibit fungal growth,49 which may be more meaningful in the case of mixed yeast and P. aeruginosa infection. Studies have suggested the use of nail dermoscopy for identifying the mixed infection.
The discolored thumbnail in Case 2 responded to fluconazole treatment after failure with itraconazole. Since we the yeast-like colonies were not identified in the specie level, this non-itraconazole response suggest a possible of mixture of Candida spp. in thumbnail. Thus, the individual nail specimen collection may be necessary, especially when treatment responses are significantly different among nails involved. In such cases, the nonresponsive nails need to be reevaluated for antifungal regimen after repeat fungal identification. When C. parapsilosis is identified, an oral treatment by terbinafine or fluconazole in combination with topical application amphotericin B are recommended. As our susceptibility tests shown in Case 2, C. parapsilosis is sensitive to above drugs.50
Conclusions
In conclusion, the distinct greenish-black discoloration was found in C. tropicalis – and C. parapsilosis – caused superficial candidiasis in our and other reports. Immunosuppressive therapy and nail damage could be the risk factors of our two cases, however, fungal or host agents that are responsible for the greenish-black discoloration are unknown but may be due to multiple factors. We could not establish a correlation between Candida species and a greenish-black discoloration since the fungal-associated BHT and the green nail syndrome are still rare.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Informed Consent
This study was approved by the Institutional Research and Ethics Committee of Jining No. 1 People’s Hospital to publish the case details (Ethical approval no. 2022-029). All patients provided written informed consent for publication of this case report and any accompanying images. The study was carried out in accordance with the principles of the Declaration of Helsinki.
Consent for Publication
Written informed consent was obtained from the patient described in this report. A copy of the written consent is available by request.
Acknowledgments
We thank the patients for granting permission to publish this information.
The abstract of this paper appeared in a substantially similar prepublication form as part of the 11th Congress on Trends in Medical Mycology (TIMM-11), where much of the current work was accepted for poster presentation. However, the abstract was not published in the Proceedings of the Congress. The earlier version of the abstract can be retrieved at https://www.timm2023.org/resources/uploads/sites/92/2023/11/Abstract-book-Accepted-Posters-TIMM-11.pdf “Abstract-book-Accepted-Posters-TIMM-11.pdf (timm2023.org)”.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from the National Nature Science Foundation of China (NM 82272358), the Key Research and Development Plan of Jining (NM 2021YXNS121), and the Traditional Chinese Medicine Science and Technology Program of Shandong Province (NM 2021M080).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Latgé JP, Calderone R. Host-microbe interactions: fungi invasive human fungal opportunistic infections. Curr Opin Microbiol. 2002;5(4):355–358. doi:10.1016/S1369-5274(02)00343-0
2. Millsop JW, Fazel N. Oral candidiasis. Clin Dermatol. 2016;34(4):487–494. doi:10.1016/j.clindermatol.2016.02.022
3. Arendorf TM, Walker DM. The prevalence and intra-oral distribution of Candida albicans in man. Arch Oral Biol. 1980;25(1):1–10. doi:10.1016/0003-9969(80)90147-8
4. Warrier SA, Sathasivasubramanian S. Human immunodeficiency virus induced oral candidiasis. J Pharm Bioallied Sci. 2015;7(Suppl 2):S812–S814. doi:10.4103/0975-7406.163577
5. Shetti A, Gupta I, Charantimath SM. Oral candidiasis: aiding in the diagnosis of HIV-A case report. Case Rep Dent. 2011;2011:929616. doi:10.1155/2011/929616
6. Gurvits GE, Tan A. Black hairy tongue syndrome. World J Gastroenterol. 2014;20(31):10845–10850. doi:10.3748/wjg.v20.i31.10845
7. Nucci M, Colombo AL. Candidemia due to Candida tropicalis: clinical, epidemiologic, and microbiologic characteristics of 188 episodes occurring in tertiary care hospitals. Diagn Microbiol Infect Dis. 2007;58(1):77–82. doi:10.1016/j.diagmicrobio.2006.11.009
8. Silva S, Negri M, Henriques M, Oliveira R, Williams DW, Azeredo J. Candida glabrata, Candida parapsilosis and Candida tropicalis: biology, epidemiology, pathogenicity and antifungal resistance. FEMS Microbiol Rev. 2012;36(2):288–305. doi:10.1111/j.1574-6976.2011.00278.x
9. Hay RJ, Baran R, Moore MK, Wilkinson JD. Candida onychomycosis--an evaluation of the role of Candida species in nail disease. Br J Dermatol. 1988;118(1):47–58. doi:10.1111/j.1365-2133.1988.tb01749.x
10. Lipner SR, Scher RK. Onychomycosis: treatment and prevention of recurrence. J Am Acad Dermatol. 2019;80(4):853–867. doi:10.1016/j.jaad.2018.05.1260
11. Korabecná M, Liska V, Fajfrlík K. Primers ITS1, ITS2 and ITS4 detect the intraspecies variability in the internal transcribed spacers and 5.8S rRNA gene region in clinical isolates of fungi. Folia Microbiol. 2003;48(2):233–238. doi:10.1007/BF02930961
12. Wayne P. Clinical and Laboratory Standards Institute: Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeasts; Approved Standard; CLSI Document M27-A3. Clinical and Laboratory Standards Institute; 2008.
13. Hu L, He C, Zhao C, Chen X, Hua H, Yan Z. Characterization of oral candidiasis and the Candida species profile in patients with oral mucosal diseases. Microb Pathog. 2019;134:103575. doi:10.1016/j.micpath.2019.103575
14. McGrath EE, Bardsley P, Basran G. Black hairy tongue: what is your call. CMAJ. 2008;178(9):1137–1138. doi:10.1503/cmaj.071611
15. Redman RS. Prevalence of geographic tongue, fissured tongue, median rhomboid glossitis, and hairy tongue among 3611 Minnesota schoolchildren. Oral Surg Oral Med Oral Pathol. 1970;30(3):390–395. doi:10.1016/0030-4220(70)90320-8
16. Avcu N, Kanli A. The prevalence of tongue lesions in 5150 Turkish dental outpatients. Oral Dis. 2003;9(4):188–195. doi:10.1034/j.1601-0825.2003.02933.x
17. Korber A, Dissemond J. Images in clinical medicine. Black hairy tongue. N Engl J Med. 2006;354(1):67. doi:10.1056/NEJMicm050117
18. Guhl G, Díaz Ley B. Lengua negra vellosa [Black hairy tongue]. Med Clin. 2011;137(4):192. Spanish. doi:10.1016/j.medcli.2010.01.022
19. Chakraborty PP, Pulai D. Black hairy tongue (lingua villosa nigra). J Assoc Physicians India. 2013;61(12):908.
20. Kobayashi K, Takei Y, Sawada M, Ishizaki S, Ito H, Tanaka M. Dermoscopic features of a black hairy tongue in 2 Japanese patients. Dermatol Res Pract. 2010;2010:1–2. doi:10.1155/2010/145878
21. Sheikh Z, Khan AS, Khan S. Lingua villosa nigra. Lancet. 2011;377(9772):1183. doi:10.1016/S0140-6736(10)60930-0
22. Dimitrios S, Maria-Aikaterini P, Alexandre F, Nikolaos S. Lingua villosa nigra. Intern Med. 2012;51(11):1453. doi:10.2169/internalmedicine.51.7505
23. Kriem S, Peretz A, Blum A. Lingua Villosa Nigra. Isr Med Assoc J. 2017;19(2):131.
24. Ramsakal A, Mangat L. Images in clinical medicine. Lingua villosa nigra. N Engl J Med. 2007;357(23):2388. doi:10.1056/NEJMicm065655
25. Luo Y, Zou P, Li QB, You Y. Black hairy tongue associated with allo peripheral blood hematopoietic stem cell transplantation. Chin Med J. 2010;123(13):1807–1808. doi:10.3760/cma.j.issn.0366-6999.2010.13.037
26. Akay BN, Sanli H, Topcuoglu P, Zincircioğlu G, Gurgan C, Heper AO. Black hairy tongue after allogeneic stem cell transplantation: an unrecognized cutaneous presentation of graft-versus-host disease. Transplant Proc. 2010;42(10):4603–4607. doi:10.1016/j.transproceed.2010.09.177
27. Aijazi I, Abdulla FM. Linezolid induced black hairy tongue: a rare side effect. J Ayub Med Coll Abbottabad. 2014;26(3):401–403.
28. Ren J, Zheng Y, Du H, et al. Antibiotic-induced black hairy tongue: two case reports and a review of the literature. J Int Med Res. 2020;48(10):300060520961279. doi:10.1177/0300060520961279
29. Nowak DA, Nowak BE. Black hairy tongue: a spooky sign associated with penicillin therapy. Med J Aust. 2022;217(3):132. doi:10.5694/mja2.51636
30. Fyrestam J, Bjurshammar N, Paulsson E, Mansouri N, Johannsen A, Östman C. Influence of culture conditions on porphyrin production in Aggregatibacter actinomycetemcomitans and Porphyromonas gingivalis. Photodiagnosis Photodyn Ther. 2017;17:115–123. doi:10.1016/j.pdpdt.2016.11.001
31. Dashper SG, Cross KJ, Slakeski N, et al. Hemoglobin hydrolysis and heme acquisition by Porphyromonas gingivalis. Oral Microbiol Immunol. 2004;19(1):50–56. doi:10.1046/j.0902-0055.2003.00113.x
32. Forouzan P, Cohen PR. Fungal viridionychia: onychomycosis-induced chloronychia caused by Candida parapsilosis-associated green nail discoloration. Cureus. 2021;13(12):e20335. doi:10.7759/cureus.20335
33. Noguchi H, Matsumoto T, Kimura U, et al. Fungal melanonychia caused by Candida parapsilosis successfully treated with oral fosravuconazole. J Dermatol. 2019;46(10):911–913. doi:10.1111/1346-8138.15024
34. Parlak AH, Goksugur N, Karabay O. A case of melanonychia due to Candida albicans. Clin Exp Dermatol. 2006;31(3):398–400. doi:10.1111/j.1365-2230.2006.02115.x
35. Lee SW, Kim YC, Kim DK, Yoon TY, Park HJ, Cinn YW. Fungal melanonychia. J Dermatol. 2004;31(11):904–909. doi:10.1111/j.1346-8138.2004.tb00624.x
36. Cohen PR, Shurman J. Fungal melanonychia as a solitary black linear vertical nail plate streak: case report and literature review of candida-associated longitudinal melanonychia striata. Cureus. 2021;13(4):e14248. doi:10.7759/cureus.14248
37. Cho E, Lee YB, Park HJ, Cho BK. Fungal melanonychia due to Candida albicans. Int J Dermatol. 2013;52(12):1598–1600. doi:10.1111/j.1365-4632.2011.05211.x
38. Rieder E, Hu SW, Meehan SA, Adigun C. Candida parapsilosis of the nail-bed without onychomycosis. Dermatol Online J. 2014;20(12):10.
39. Vélez A, Fernández-Roldán JC, Linares M, Casal M. Melanonychia due to Candida humicola. Br J Dermatol. 1996;134(2):375–376. doi:10.1111/j.1365-2133.1996.tb07639.x
40. Gautret P, Rodier MH, Kauffmann-Lacroix C, Jacquemin JL. Case report and review. onychomycosis due to Candida parapsilosis. Mycoses. 2000;43(11–12):433–435. doi:10.1111/j.1439-0507.2000.00602.x
41. Morris-Jones R, Gomez BL, Diez S, et al. Synthesis of melanin pigment by Candida albicans in vitro and during infection. Infect Immun. 2005;73(9):6147–6150. doi:10.1128/IAI.73.9.6147-6150.2005
42. Editors T. Melanins in fungal pathogens. J Med Microbiol. 2002;51(3):189–191.
43. Finch J, Arenas R, Baran R. Fungal melanonychia. J Am Acad Dermatol. 2012;66(5):830–841. doi:10.1016/j.jaad.2010.11.018
44. Maes M, Richert B, de la Brassinne M. Fungal melanonychia [Green nail syndrome or chloronychia]. Rev Med Liege. 2002;57(4):233–235. French.
45. Lipner SR, Scher RK. Evaluation of nail lines: color and shape hold clues. Cleve Clin J Med. 2016;83(5):385–391. doi:10.3949/ccjm.83a.14187
46. Díaz-Pérez SP, Solis CS, López-Bucio JS, et al. Pathogenesis in Pseudomonas aeruginosa PAO1 biofilm-associated is dependent on the pyoverdine and pyocyanin siderophores by quorum sensing modulation. Microb Ecol. 2022;86(1):727–741. doi:10.1007/s00248-022-02095-5
47. Schwartz RA, Reynoso-Vasquez N, Kapila R. Chloronychia: the Goldman–Fox syndrome - implications for patients and healthcare workers. Indian J Dermatol. 2020;65(1):1–4. doi:10.4103/ijd.IJD_277_19
48. Ohn J, Yu DA, Park H, Cho S, Mun JH. Green nail syndrome: analysis of the association with onychomycosis. J Am Acad Dermatol. 2020;83(3):940–942. doi:10.1016/j.jaad.2020.01.040
49. Kerr JR, Taylor GW, Rutman A, Høiby N, Cole PJ, Wilson R. Pseudomonas aeruginosa pyocyanin and 1-hydroxyphenazine inhibit fungal growth. J Clin Pathol. 1999;52(5):385–387. doi:10.1136/jcp.52.5.385
50. Nenoff P, Paasch U, Handrick W. [Infections of finger and toe nails due to fungi and bacteria]. Hautarzt. 2014;65(4):337–348. German. doi:10.1007/s00105-013-2704-0
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.