Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 14
Tunnel Restoration: A Minimally Invasive Dentistry Practice
Authors Nizami MZI ![]() , Yeung C
, Yeung C ![]() , Yin IX, Wong AWY
, Yin IX, Wong AWY ![]() , Chu CH
, Chu CH ![]() , Yu OY
, Yu OY ![]()
Received 4 May 2022
Accepted for publication 12 July 2022
Published 15 July 2022 Volume 2022:14 Pages 207—216
DOI https://doi.org/10.2147/CCIDE.S372165
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Mohammed Zahedul Islam Nizami, Conson Yeung, Iris Xiaoxue Yin, Amy Wai Yee Wong, Chun Hung Chu, Ollie Yiru Yu
Faculty of Dentistry, The University of Hong Kong, Hong Kong Special Administrative Region, People’s Republic of China
Correspondence: Ollie Yiru Yu, 3B12 Prince Philip Dental Hospital, Faculty of Dentistry, The University of Hong Kong, 34 Hospital Road, Sai Ying Pun, Hong Kong Special Administrative Region, People’s Republic of China, Tel +852 2859 0310, Fax +852 2559 4194, Email [email protected]
Abstract: With advances in technology, dentists nowadays manage dental caries with the philosophy of minimally invasive dentistry. Dental restoration is now performed most conservatively with minimal destruction of tooth structure when operative dentistry is indicated. Some operative dentists suggested using tunnel restoration for treating proximal caries as a conservative alternative to the conventional box preparation. The main advantage of tunnel restoration over the conventional box or slot preparation includes being more conservative and increasing tooth integrity and strength by preserving the marginal ridge. However, tunnel restoration is technique sensitive and requires advanced operative skills. Tunnel restoration can be an option to restore proximal caries if the dentist selects the proper case and pays attention to the details of the restorative procedures. With the dentist’s advanced training, advanced light-emitting diode handpieces, magnifying loupes, precise digital imaging and new generation restorative materials, good results can be obtained in selected cases. This study reviews the literature on tunnel restoration and provides updated techniques and clinical data that can be used in tunnel restoration to oversee its limitations and the perspective on restorative treatment.
Keywords: minimally invasive, tunnel restoration, proximal caries, tunnel preparation, restorative dentistry
Introduction
Conventional cavity design is extensive for silver amalgam restoration to restore a caries lesion in the tooth’s interproximal surface, or a GV Black Class II cavity.1 The occlusal cavity should be at least 1.5 to 2.0 mm deep, regardless of the caries extension, to prevent the fracture of the restorative material during function.2 Non-carious fissure areas in the occlusal surface should be removed for caries prevention. The carious tooth’s marginal ridge and the interproximal contact area also need to be removed to access the caries lesion.3,4 However, the extensive cavity design has consequences. A study showed that dental restorations normally needed to be replaced within 3 to 10 years.5 The operative procedure of the restoration replacement further enlarges the cavity and damages the tooth’s structure and vitality.6 In addition, the reconstruction of the removed interproximal contact area is technique sensitive. Poor reconstruction of the proximal contact often causes food impaction.4 Therefore, a conservative cavity design should be recommended.
Tunnel restoration is a minimally invasive technique for restoring the caries lesion on the interproximal tooth surface. Tunnel restoration was proposed to restore disto-proximal carious lesions in deciduous second molars in 1960s.7 However, the failure rate of the restoration was high. With the improvement in adhesives and restorative materials, the new generation of small size electric motor dental handpieces with light-emitting diode (LED) light and the use of magnifying loupes to increase the visibility, this approach has been re-introduced and advocated as a conservative alternative to conventional cavity design for interproximal caries in posterior primary teeth.8–11 The tunnel restoration preserves the marginal ridge by preparing a tunnel from the occlusal surface to the carious interproximal surface.12 This study reviews the literature on tunnel restoration and provides updated techniques and clinical data that can be used in tunnel restoration to oversee its limitations and the perspective on restorative treatment.
Cavity Preparation for Tunnel Restoration
The cavity preparation of tunnel restoration removes less tooth tissue compared to the conventional Class II box and slot preparation (Figure 1). The demineralised enamel in the interproximal surface can be preserved in a tunnel preparation if it is not cavitated. With the preservation of different amounts of enamel in the interproximal surface, the tunnel preparation can be classified as (1) total tunnel (complete removal of the demineralized proximal enamel), (2) partial tunnel (partial removal of the proximal surface with the preservation of some demineralized proximal enamel) and (3) internal tunnel (preservation of proximal enamel).11,13
 |
Figure 1 Tooth structure loss in cavity designs. (A) Class II preparation - removal of occlusal and proximal tooth structure including the marginal ridge. (B) Slot preparation - removal of proximal tooth structure including the marginal ridge. (C) Tunnel preparation - removal of occlusal and proximal tooth structure. |
Restorative Materials for Tunnel Restorations
After the tunnel preparation, restorative materials are filled into the prepared tunnel to restore the cavity. Dental materials such as silver amalgam, composite resin, glass ionomer, or a combination of glass ionomer and composite resin have been used for tunnel restoration. The selection of restorative materials affects the tunnel restoration’s clinical results.
Silver amalgam is suitable for tunnel restoration in patients who have less aesthetic demand. It has good compressive strength and is easy to handle. One study reported that less than 10% of the tunnel restorations needed to be replaced after 10 years.5 The packability of silver amalgam allows clinicians to create a tight interproximal contact area.14 This is difficult to achieve with glass ionomers or composite resins because of the material’s nature.
Composite resin is used to fill the whole tunnel preparation or cover the occlusal surface of the tunnel preparation with glass ionomer beneath to increase the tunnel-restored teeth’s fracture resistance.15–18 Composite resin processes advanced mechanical properties compared to glass ionomer for tunnel restoration. One study found that composite resin restoration with appropriate tunnel preparation showed similar mechanical strength to the sound structure of the tooth.3 The composite resin could bond to enamel and dentin with adhesives.19 It showed an advanced marginal adaptation compared to glass ionomer, metal-reinforced glass ionomer cements, or silver amalgams when used for tunnel restorations.20 The use of flowable composite resin might further improve marginal adaptation and sealing in tunnel restorations.21
Glass ionomer is used for tunnel restoration without heavy occlusal loading.17,18,22,23 Glass ionomer possesses a number of desirable properties to serve as a restorative material for tunnel restoration, including radiopacity, chemical bond to enamel and dentin, and fluoride release.24–26 However, glass ionomer exhibited inadequate mechanical and adhesive properties. It might not be strong enough to withstand the occlusal force.27 Furthermore, glass ionomer or metal-reinforced glass ionomer exhibited various degrees of microleakage.28–31 Studies have demonstrated porosities within the restoration, and in the interface between restoration and the cavity wall were 32%.32 Therefore, glass ionomer was not recommended as definitive restorations in permanent dentition.33
Clinical Procedures of Tunnel Restorations with Different Restorative Materials
Tunnel Restoration Using Silver Amalgam
A patient with caries in the distal aspect of the left mandibular first molar was presented (Figure 2A and B). The patient’s informed consent for the dental treatment, the publication of the clinical photos, and the publication of the case report were obtained before the treatment. No institutional approval was required to publish this case report. Rubber dam isolation was applied. An occlusal cavity was drilled in the distal triangular fossa using the tapered diamond bur to gain access to caries. Caries were further removed using a small diamond round bur. Unsupported enamel was trimmed with an excavator. The marginal ridge’s width at the end of the preparation was 2 mm mesiodistally (Figure 2C). Tofflemire matrix band and wooden wedge were placed. Then, a dentin bonding agent that bonds the silver amalgam (Clearfil Liner Bond 2V, Kuraray Co., Ltd., Tokyo, Japan) was applied. The cavity was then overfilled with silver amalgam (Tytin FC, Kerr Corporation, Orange, CA, USA) (Figure 2D). The excess silver amalgam was carved to reproduce the original morphology (Figure 2E). The occlusion was adjusted after setting the silver amalgam. The postoperative radiograph confirmed the silver amalgam’s good adaptation against the cavity wall and the reconstruction of the proximal surface of the tooth (Figure 2F).
 |
Figure 2 Radiographs and photographs (mirror image) of a tunnel restoration using silver amalgam. (A) occlusal view (preoperative). (B) preoperative radiograph. (C) occlusal view (after cavity preparation). (D) occlusal view (after silver amalgam insertion). (E) occlusal view (after silver amalgam carving). (F) postoperative radiograph. |
Tunnel Restoration Using Composite Resin
A patient with caries in the distal aspect of the right mandibular second molar was presented (Figure 3A and B). The patient’s informed consent for the dental treatment, the publication of the clinical photos, and the publication of the case report were obtained before the treatment. No institutional approval was required to publish this case. A rubber dam was inserted before the operation. Cavity access from the occlusal distal fossa was achieved for caries removal of the distal proximal surface. Remaining caries in the distal surface was then removed (Figure 3C). Selective enamel etching with 40% phosphoric acid (K-etchant gel, Kuraray, Co., Ltd., Tokyo, Japan) for 30 seconds was performed. This was followed by applying a two-step self-etch dentin bonding system (Clearfil SE Bond 2, Kuraray Co., Ltd., Tokyo, Japan). The cavity was then restored with composite resin (Filtek Z250, 3M Company, St. Paul, MN, USA) using the layering technique to minimize polymerization shrinkage stress (Figure 3D and E). The occlusion was adjusted as necessary. The postoperative radiograph showed the proper adaptation of the restoration, though a negligible overhang can be noticed (Figure 3F).
 |
Figure 3 Radiographs and photographs (mirror image) of a tunnel restoration using composite resin. (A) occlusal view (preoperative). (B) preoperative radiograph. (C) occlusal view (after cavity preparation). (D) occlusal view (after composite resin insertion). (E) occlusal view (after composite polishing). (F) postoperative radiograph. |
Tunnel Restoration Using Glass Ionomer/Composite Resin (Sandwich Technique)
A patient with caries in the distal aspect of the right maxillary first molar was presented (Figure 4A and B). The patient’s informed consent for the dental treatment, the publication of the clinical photos, and the publication of the case report were obtained before the treatment. No institutional approval was required to publish this case. After placing the rubber dam, access to the caries was gained through removing the existing silver amalgam. A round bar was used for removing remaining caries (Figure 4C). Tofflemire matrix band and a wooden wedge were placed. The cavity was conditioned with 20% polyacrylic acid (Ketac Conditioner, 3M Company, St. Paul, MN, USA) for 15 seconds, rinsed and dried. The cavity was filled with glass ionomer (Ketac Molar, 3M Company, St. Paul, MN, USA) and gently condensed with a condenser to form a flat surface (Figure 4D). Selective etching of the cavity wall’s enamel and the occlusal fissure adjacent to the cavity with 40% phosphoric acid for 30 seconds was performed (K-etchant gel, Kuraray Co., Ltd., Tokyo, Japan). This was followed by applying a two-step self-etch dentin bonding system (Clearfil SE Bond 2, Kuraray Co., Ltd., Tokyo, Japan). The cavity was then restored with composite resin (Filtek Z250, 3M Company, St. Paul, MN, USA). The occlusion was adjusted as necessary (Figure 4E). The postoperative radiograph confirmed the restoration’s good adaption (Figure 4F).
 |
Figure 4 Radiographs and photographs (mirror image) of a tunnel restoration using glass ionomer and composite resin (sandwich technique). (A) occlusal view (preoperative). (B) preoperative radiograph. (C) occlusal view (after cavity preparation). (D) occlusal view (after glass ionomer insertion). (E) occlusal view (after composite resin insertion). (F) postoperative radiograph. |
Potential Problems and Solutions in Tunnel Restoration
Tunnel restorations have strengths and challenges. It can (i) preserve the marginal ridge, which contributes to maintaining tooth integrity and strength; (ii) preserve proximal contour including the proximal contact; (iii) reduce the risk of iatrogenic damage to the adjacent tooth; (iv) reduce the risk of the restoration having an overhang; and (v) preserve more tooth structure compared to conventional Class II.34 However, these advantages need to be balanced against potential problems including (i) increased risk of inadequate caries removal due to more restricted visual and instrumental access, (ii) accidental or intentional removal of the marginal ridge and (iii) increased risk of pulpal exposure.35
Inadequate Caries Removal
Inadequate caries removal includes under-preparing or over-preparing the tunnel. Under-preparing the tunnel leaves residual caries on-site, which may increase the risk of secondary caries and shorten the tunnel restoration’s lifespan. Of the partial tunnel preparations, 22–29% were found to have residual caries after caries removal.32,36,37 Over-preparation weakens or damages the tooth structure.
Proper visualization could possibly achieve adequate caries removal. Three essential conditions should be attained in the operation process to achieve the proper visualization for preventing inadequate enamel/dentin removal in the cavity preparation: (i) a clear operation field, (ii) strict moisture control and (iii) suitable magnification.38 A clear operation field should be obtained before the operative intervention. Removing supra-/sub-gingival plaque, debris and calculus are essential.11 In addition, to ensure that the lesion is cavitated and to improve visual access, it is useful to separate teeth by placing an orthodontic elastic separator for a week to develop a small interproximal space.38 Moisture control via applying a rubber dam is helpful for restoration with high quality. In addition, using magnifying loupes helped reduce marginal overhangs by up to 40%.39 Overhang may affect the evaluation of the clinical result of the restoration on follow-up visits by causing the misinterpretation of the failure reason. The restoration failure may be due to the overhang and the leakage instead of the tunnel itself. Other contradictory approaches to facilitate adequate caries removal include increasing the size of the occlusal access32,36 and adopting radiographic examination. However, increasing the size of the tunnel preparation lowers the tooth’s fracture resistance. One study reported that even onsite radiographic examination during tunnel preparation could not increase the efficacy of caries removal. It suggested not to consider radiography as a suitable diagnostic tool for caries determination during tunnel preparation.40
Fracture of the Marginal Ridge
Inadequate width or height of the remaining marginal ridge after tunnel preparation increases the risk of marginal ridge fracture. A tunnel preparation closed to the marginal ridge and/or that has a large occlusal opening leads to reduced marginal ridge width. It had a 2–7 times higher risk of fracture compared to a tunnel preparation with a greater distance to the marginal ridge or a smaller opening.41,42 The bur’s horizontal orientation in tunnel preparation reduced the marginal ridge’s height. Studies showed that total tunnel preparation resulted in a weakened marginal ridge.39,41–43
To enhance the tunnel restoration’s fracture resistance, the marginal ridge’s width should be at least 2 mm41 and the height should be ideally 2.5 mm.3 The occlusal opening of the tunnel restoration should be conservative. One study discovered that small-sized tunnel preparations showed maximum marginal ridge strength compared to sound teeth.41 The tunnel restoration with a 2.5-mm-high marginal ridge had similar fracture resistance to that of sound teeth.3 In addition, having the bur angulation vertically initially and then changing to a more horizontal angulation might preserve more dentin under the marginal ridge when preparing the tunnel. However, note that this operation may result in a higher risk of pulpal exposure.44
Invasion of Vital Pulp
Another consideration is the violation or irritation of vital pulp in the tunnel preparation or restoration. To avoid pulp exposure, a careful pre-operative examination with the assistance of a radiograph should be performed. The bur’s orientation should be well controlled with the radiograph as a reference. To avoid irritating the pulp during the operative procedure or due to the restorative materials, resin-modified glass ionomer or calcium hydroxylate liner is recommended for indirect pulp capping if the tunnel is closed to the dental pulp.45 This layer of liner not only acted as a protective barrier for the pulp but also enhanced the remineralisation of the caries-affected dentin.
Clinical Outcomes of Tunnel Restorations Using Different Restorative Materials
Clinical studies published in the past 40 years on the survival rate of tunnel restorations were searched to discover the clinical outcomes of tunnel restorations using different restorative materials. Twenty-three clinical trials were found and included in the search. Table 1 summarises survival rate of the tunnel restoration using different restorative materials and their causes of failure.
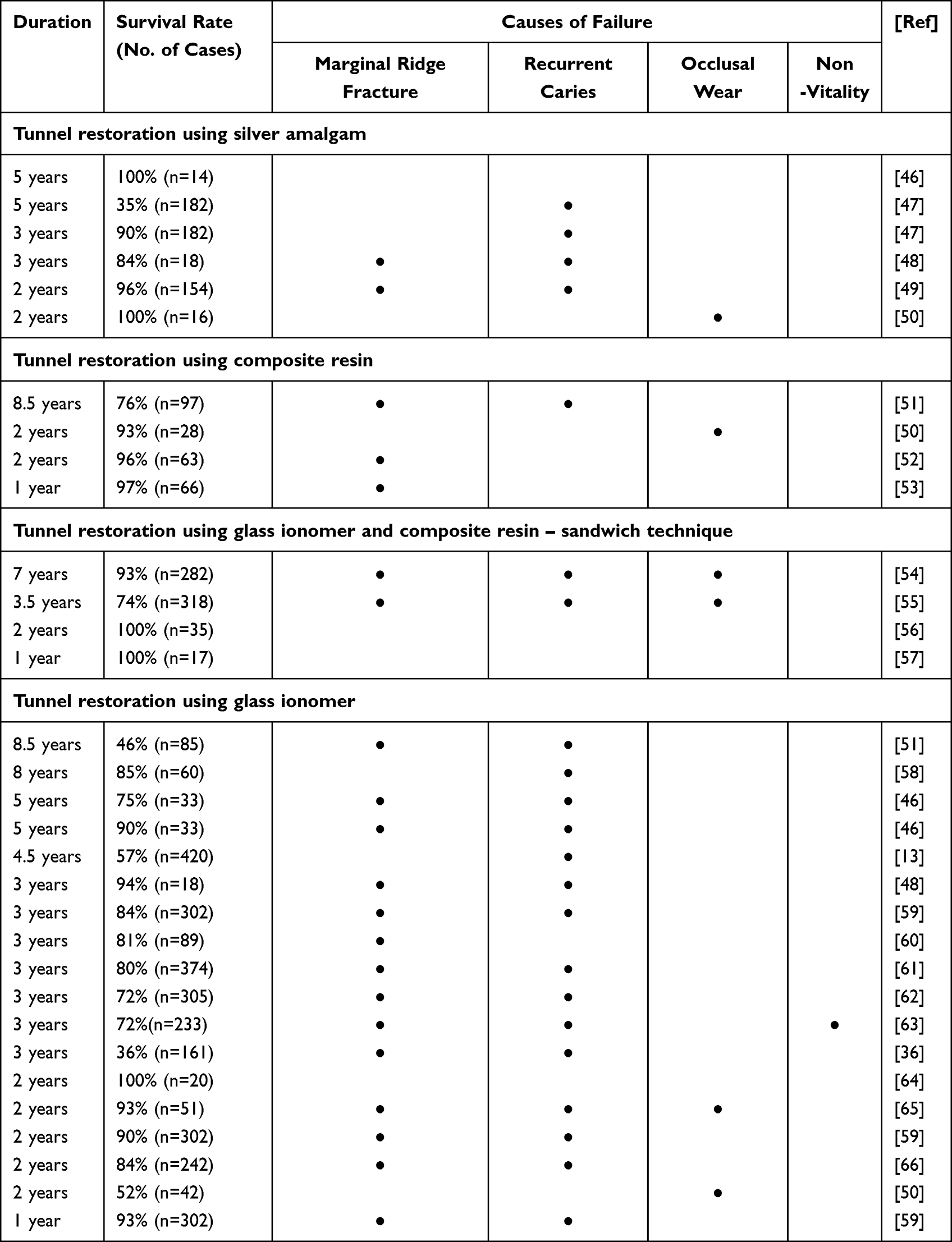 |
Table 1 The Survival Rate of Tunnel Restorations and Their Causes of Failure |
Studies found the survival rate of composite resin and silver amalgam was higher compared to that of glass ionomer. The median survival time of glass ionomer tunnel restorations was 6 years, whereas those of composite resin and silver amalgam Class II restorations were between 9 and 13 years.27,54 The annual failure rate of glass ionomer in tunnel restorations was 7–10%,13,54,55 which was higher than that of conventional Class II silver amalgam (3.3%) and composite resin (2.3%) restorations.54 The weighted mean survival rate of tunnel restoration restored with glass ionomer and silver amalgam as a function of time was plotted (Figure 5). The weighted mean survival rate was calculated by

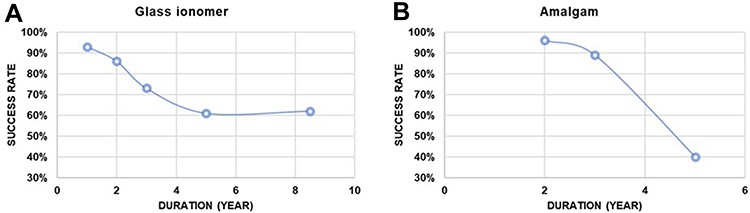 |
Figure 5 The survival rate of tunnel restorations using (A) glass ionomer and (B) silver amalgam. |
Where “m” denotes the total number of studies which has covered the survival rate of the time in service of the restoration under consideration. With this plot, it can be assumed that the glass ionomer success rate steadily declined with time. However, the amalgam success rate drastically fell on long-term follow-up. The survival rate of tunnel restoration with composite resin was not plotted because there were only a few studies with a limited sample size.
Note that most of the reported studies were conducted approximately two decades ago. New technologies have been developed since then. These include magnifying loupes and light-emitting diode handpieces. These technologies enhance the micro-detailed visibility in the tiny operative field of dentistry.66,67 Digital radiography has improved the quality of dental imaging and reduced radiation hazards. This may facilitate diagnosing proximal caries and close monitoring of post-treatment success.68–70 Hence, clinicians can achieve higher success rates compared with those in the reviewed studies. It was also found that the survival rate of tunnel restoration was significantly associated with the clinician’s skill.13,47 The 3-year failure rates of individual dentists were reported as ranging from 9% to 50%.61 Although, higher success rates were observed for operators with more experience.61,71
Other factors related to the failure of tunnel restoration conflicted in the literature. Several studies found that the failure rate was not related to the type of tooth or the type of tunnel restoration.13,54,61,62,72 On the contrary, some studies observed higher failure rates for molars than those for premolars.14,59 Some studies found better outcomes for partial tunnel restorations59,71 because partial tunnel restorations might result in less tooth structure removal and thereby a stronger marginal ridge.59,71 Others observed better outcomes for total tunnel restorations13,72 because adequate caries removal was more easily achieved in total tunnel preparation.13,72 Regarding the effect of caries risk on the failure rate, some studies14,61 found no correlation between the two. However, a study showed a higher median survival time of tunnel restorations in patients with moderate caries risk compared to the median survival time of the restorations in patients with high caries risk.47 Another study observed significantly higher failure rates in patients with high caries risk.72
Therefore, experienced operators adopting new technologies, such as a magnifying loupe, and bonding, and using durable materials (composite resin, silver amalgam) may indicate higher success rates of tunnel restorations.38,66,69
Conclusion
The tunnel restoration is a viable and conservative permanent restoration procedure for proximal caries. There is a clear need for research to improve the diagnostic methods, develop site-specific indicators of future caries risk and establish clear guidelines on managing caries. Generally, tunnel restoration is a technically demanding procedure. Proper case selection, preparation technique and selection of restorative materials are important. Using advanced technologies, such as magnifying loupes, digital radiography and dental handpieces with LED lights, is essential. Further long-term clinical studies should be undertaken to determine the success and failure rates of these restoration techniques using the latest technologies available compared with other restoration techniques.
Disclosure
The authors declare no conflicts of interest.
References
1. Mount GJ, Hume WR. Classification and Cavity Preparation for Caries Lesions; Preservation and Restoration of Tooth Structure. Knowledge Books and Software; 2005.
2. Ritter AV. Sturdevant’s Art and Science of Operative Dentistry - Elsevier EBook on Vitalsource (Retail Access Card). Mosby; 2018.
3. Ji W, Chen Z, Frencken JE. Strength of tunnel-restored teeth with different materials and marginal ridge height. Dent Mater. 2009;25(11):1363–1370. doi:10.1016/j.dental.2009.06.007
4. Loomans BAC, Opdam NJM, Roeters JFM, Bronkhorst EM, Plasschaert AJM. Influence of composite resin consistency and placement technique on proximal contact tightness of Class II restorations. J Adhes Dent. 2006;8(5):305–310.
5. Schwendicke F, Lamont T, Innes N. Removing or controlling? How caries management impacts on the lifetime of teeth. Monogr Oral Sci. 2018;27:32–41. doi:10.1159/000487829
6. Brantley CF, Bader JD, Shugars DA, Nesbit SP. Does the cycle of rerestoration lead to larger restorations? J Am Dent Assoc. 1995;126(10):1407–1413. doi:10.14219/jada.archive.1995.0052
7. Jinks GM. Fluoride-impregnated cements and their effect on the activity of interproximal caries. J Dent Child. 1963;30:87–91.
8. Hunt PR. A modified Class II cavity preparation for glass ionomer restorative materials. Quintessence Int Dent Dig. 1984;15(10):1011–1018.
9. Knight GM. The use of adhesive materials in the conservative restoration of selected posterior teeth. Aust Dent J. 1984;29(5):324–331. doi:10.1111/j.1834-7819.1984.tb05294.x
10. Knight GM. The tunnel restoration. Dent Outlook. 1984;10:53–57.
11. Ratledge DK, Kidd EAM, Treasure ET. The tunnel restoration. Br Dent J. 2002;193(9):501–506. doi:10.1038/sj.bdj.4801609
12. Wiegand A, Attin T. Treatment of proximal caries lesions by tunnel restorations. Dent Mater. 2007;23(12):1461–1467. doi:10.1016/j.dental.2006.12.004
13. Strand GV, Nordbø H, Leirskar J, von der Fehr FR, Eide GE. Tunnel restorations placed in routine practice and observed for 24 to 54 months. Quintessence Int. 2000;31(7):453–460.
14. Bharti R, Wadhwani KK, Tikku AP, Chandra A. Dental amalgam: an update. J Conserv Dent. 2010;13(4):204–208. doi:10.4103/0972-0707.73380
15. Maitland RI. Current concepts in successful posterior class II direct composites. Dent Econ. 1993;83(6):101–103.
16. Yaman SD, Yetmez M, Türköz E, Akkas N. Fracture resistance of Class II approximal slot restorations. J Prosthet Dent. 2000;84(3):297–302. doi:10.1067/mpr.2000.108452
17. Croll TP. Glass ionomer-silver cermet bonded composite resin Class II tunnel restorations. Quintessence Int. 1988;19(8):533–539.
18. McLean JW. Limitations of posterior composite resins and extending their use with glass ionomer cements. Quintessence Int. 1987;18(8):517–529.
19. Chu CH, Zhang CF, Jin LJ. Treating a maxillary midline diastema in adult patients: a general dentist’s perspective. J Am Dent Assoc. 2011;142(11):1258–1264. doi:10.14219/jada.archive.2011.0110
20. Chalker SA, Lumley PJ. An in vitro assessment of cavity margin finishing and marginal adaptation of tunnel restorations. Eur J Prosthodont Restor Dent. 1993;1(4):151–156.
21. Ebert J, Frankenberger R, Petschelt A. A novel approach for filling tunnel prepared teeth with composites of two different consistencies: a case presentation. Quintessence Int. 2012;43:93–96.
22. McLean JW. Clinical applications of glass-ionomer cements. Oper Dent. 1992;Suppl 5(Suppl 5):184–190.
23. Tay WM, Lynch E. Glass-ionomer cements–clinical usage and experience: 2. Dent Update. 1990;17(2):51–56.
24. Chu CH, King NM, Lee AM, Yiu CK, Wei SH. A pilot study of the marginal adaptation and surface morphology of glass-cermet cements. Quintessence Int. 1996;27(7):493–501.
25. Mount GJ. Clinical placement of modern glass ionomer cements. Quintessence Int. 1993;24:99–107.
26. Forsten L. Fluoride release and uptake by glass ionomers. Scand. J Dent Res. 1991;99:241–245.
27. Manhart J, Chen H, Hamm G, Hickel R. Buonocore memorial lecture. Review of the clinical survival of direct and indirect restorations in posterior teeth of the permanent dentition. Oper Dent. 2004;29(5):481–508.
28. Prabhu NT, Munshi AK, Shetty TR. Marginal ridge fracture resistance, microleakage and pulpal response to glass ionomer/glass cermet partial tunnel restorations. J Clin Pediatr Dent. 1997;21(3):241–246.
29. Robbins JW, Cooley RL. Microleakage of Ketac-Silver in the tunnel preparation. Oper Dent. 1988;13(1):8–11.
30. Shetty R, Munshi AK. Tunnel restorations using glass ionomer or glass cermet: in vitro marginal ridge fracture and microleakage. J Clin Pediatr Dent. 1996;21(1):77–84.
31. Garcia-Godoy F, Marshall TD, Mount GJ. Microleakage of glass ionomer tunnel restorations. Am J Dent. 1988;1(2):53–56.
32. Strand GV, Tveit AB. Effectiveness of caries removal by the partial tunnel preparation method. Eur J Oral Sci. 1993;101(5):270–273. doi:10.1111/j.1600-0722.1993.tb01118.x
33. McLean JW, Gasser O. Glass-cermet cements. Quintessence Int. 1985;16(5):333–343.
34. Tyas MJ, Anusavice KJ, Frencken JE, Mount GJ. Minimal intervention dentistry–a review. FDI commission project 1-97. Int Dent J. 2000;50:1–12.
35. Papa J, Wilson PR, Tyas MJ. Tunnel restorations: a review. J Esthet Dent. 1992;4:4–9. doi:10.1111/j.1708-8240.1992.tb00708.x
36. Strand GV, Tveit AB, Eide GE. Cavity design and dimensions of tunnel preparations versus composite resin Class-II preparations. Acta Odontol Scand. 1995;53(4):217–221. doi:10.3109/00016359509005975
37. Strand GV, Tveit AB. Espelid, I. Variations among operators in the performance of tunnel preparations in vitro. Scand J Dent Res. 1994;102:151–155.
38. Yu OY, Zaeneldin AM, Hamama HHH, Mei ML, Patel N, Chu CH. Conservative composite resin restoration for proximal caries - two case reports. Clin Cosmet Investig Dent. 2020;12:415–422. doi:10.2147/CCIDE.S270453
39. Frankenberger R, Krämer N, Pelka M, Petschelt A. Internal adaptation and overhang formation of direct Class II resin composite restorations. Clin Oral Investig. 1999;3(4):208–215. doi:10.1007/s007840050103
40. Wenzel A, Hintze H, Hörsted-Bindslev P. Accuracy of radiographic detection of residual caries in connection with tunnel restorations. Caries Res. 1998;32:17–22. doi:10.1159/000016425
41. Fasbinder DJ, Davis RD, Burgess JO. Marginal ridge strength in Class II tunnel restorations. Am J Dent. 1991;4(2):77–82.
42. Strand GV, Tveit AB, Gjerdet NR, Eide GE. Marginal ridge strength of teeth with tunnel preparations. Int Dent J. 1995;45(2):117–123.
43. James T, Gilmour ASM. Magnifying loupes in modern dental practice: an update. Dent Update. 2010;37(9):633–636. doi:10.12968/denu.2010.37.9.633
44. Papa J, Cain C, Messer HH. Efficacy of tunnel restorations in the removal of caries. Quintessence Int. 1993;24(10):715–719.
45. Ritter AV, Swift EJ. Current restorative concepts of pulp protection. Endod Topics. 2003;5(1):41–48. doi:10.1111/j.1601-1546.2003.00022.x
46. Lumley PJ, Fisher FJ. Tunnel restorations: a long-term pilot study over a minimum of five years. J Dent. 1995;23(4):213–215. doi:10.1016/0300-5712(95)91185-p
47. Nicolaisen S, von der Fehr FR, Lunder N, Thomsen I. Performance of tunnel restorations at 3–6 years. J Dent. 2000;28(6):383–387. doi:10.1016/s0300-5712(00)00024-5
48. Svanberg M. Class II amalgam restorations, glass-ionomer tunnel restorations, and caries development on adjacent tooth surfaces: a 3-year clinical study. Caries Res. 1992;26(4):315–318. doi:10.1159/000261459
49. Ehrlich J, Yaffe A. A modified cavity preparation for restoring interproximal caries. Compendium. 1987;8(1):62–64.
50. Wilkie R, Lidums A, Smales R. Class II glass ionomer cermet tunnel, resin sandwich and amalgam restorations over 2 years. Am J Dent. 1993;6(4):181–184.
51. Hörsted-Bindslev P, Heyde-Petersen B, Simonsen P, Baelum V. Tunnel or saucer-shaped restorations: a survival analysis. Clin Oral Investig. 2005;9(4):233–238. doi:10.1007/s00784-005-0011-6
52. Kinomoto Y, Inoue Y, Ebisu S. A two-year comparison of resin-based composite tunnel and Class II restorations in a randomized controlled trial. Am J Dent. 2004;17(4):253–256.
53. de Freitas AR, de Andrada MA, Baratieri LN, Monteiro Júnior S, de Sousa CN. Clinical evaluation of composite resin tunnel restorations on primary molars. Quintessence Int. 1994;25(6):419–424.
54. Hasselrot L. Tunnel restorations in permanent teeth. A 7 year follow up study. Swed Dent J. 1998;22(1–2):1–7.
55. Hasselrot L. Tunnel restorations. A 3 1/2-year follow up study of Class I and II tunnel restorations in permanent and primary teeth. Swed Dent J. 1993;17(5):173–182.
56. Wang Y, Yang PS. Clinical evaluation of tunnel-restoration. Shanghai Kou Qiang Yi Xue. 2003;12(1):7–8.
57. Ratledge DK. A clinical and laboratory investigation of the tunnel restoration. 1999.
58. Jones SE. The theory and practice of internal “tunnel” restorations: a review of the literature and observations on clinical performance over eight years in practice. Prim Dent Care. 1999;6:93–100.
59. Holst A, Brännström M. Restoration of small proximal dentin lesions with the tunnel technique. A 3-year clinical study performed in Public Dental Service clinics. Swed Dent J. 1998;22(4):143–148.
60. Odman P. A 3-year clinical evaluation of Cerana prefabricated ceramic inlays. Int J Prosthodont. 2002;15(1):79–82.
61. Pilebro CE, van Dijken JW. Analysis of factors affecting failure of glass cermet tunnel restorations in a multi-center study. Clin Oral Investig. 2001;5(2):96–101. doi:10.1007/s007840100106
62. Pilebro CE, van Dijken JW, Stenberg R. Durability of tunnel restorations in general practice: a three-year multicenter study. Acta Odontol Scand. 1999;57(1):35–39. doi:10.1080/000163599429084
63. Markovic D, Peric T. Clinical evaluation of glass-ionomer tunnel restorations in primary molars: 36 months results. Aust Dent J. 2008;53(1):41–45. doi:10.1111/j.1834-7819.2007.00007.x
64. Zenkner JE, Baratieri LN, Monteiro SJ, de Andrada MA, Vieira LC. Clinical and radiographic evaluation of cermet tunnel restorations on primary molars. Quintessence Int. 1993;24(11):783–791.
65. Pyk N, Mejàre I. Tunnel restorations in general practice. Influence of some clinical variables on the success rate. Acta Odontol Scand. 1999;57(4):195–200. doi:10.1080/000163599428779
66. Chu CH, Mei ML, Nalliah RP. A survey of practices of tunnel preparation among dentists who attended the 100th FDI Annual World Dental Congress. J Investig Clin Dent. 2015;6(1):63–68. doi:10.1111/jicd.12081
67. Othman NI, Ismail HU, Mohammad N, Ghazali N, Alauddin MS. An evaluation on deep caries removal method and management performed by undergraduate dental students: a Malaysia experience. Eur J Dent. 2021;15(2):281–289. doi:10.1055/s-0040-1721546
68. Bin-Shuwaish M, Dennison JB, Yaman P, Neiva G. Estimation of clinical axial extension of Class II caries lesions with ultraspeed and digital radiographs: an in-vivo study. Oper Dent. 2008;33(6):613–621. doi:10.2341/07-167
69. Chu CH, Lo ECM, You DSH. Clinical diagnosis of fissure caries with conventional and laser-induced fluorescence techniques. Lasers Med Sci. 2010;25(3):355–362. doi:10.1007/s10103-009-0655-6
70. Alauddin MS, Baharuddin AS, Mohd Ghazali MI. The modern and digital transformation of oral health care: a mini review. Healthcare. 2021;9(2):118. doi:10.3390/healthcare9020118
71. Restorations HLT. A 3 1/2-year follow up study of Class I and II tunnel restorations in permanent and primary teeth. Swed Dent J. 1993;17:173–182.
72. Strand GV, Nordbø H, Tveit AB, Espelid I, Wikstrand K, Eide GE. A 3-year clinical study of tunnel restorations. Eur J Oral Sci. 1996;104(4):384–389. doi:10.1111/j.1600-0722.1996.tb00096.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.