Back to Journals » Clinical Ophthalmology » Volume 17
Steroid Response Following Dropless Cataract Surgery Using Subconjunctival Triamcinolone
Authors Wu AM, Pitts KM ![]() , Pineda R, Chen SH, Wang M, Johnson G, Shen LQ
, Pineda R, Chen SH, Wang M, Johnson G, Shen LQ ![]() , Margeta MA
, Margeta MA
Received 11 July 2023
Accepted for publication 8 September 2023
Published 22 September 2023 Volume 2023:17 Pages 2803—2814
DOI https://doi.org/10.2147/OPTH.S426200
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Annie M Wu,1,2 Kristen M Pitts,1,3 Roberto Pineda,1 Sherleen H Chen,1 Mengyu Wang,3 Grace Johnson,1 Lucy Q Shen,1,* Milica A Margeta1,3,*
1Massachusetts Eye and Ear, Harvard Medical School, Boston, MA, USA; 2Kellogg Eye Center, University of Michigan, Ann Arbor, MI, USA; 3Harvard Ophthalmology AI Lab, Schepens Eye Research Institute of Massachusetts Eye and Ear, Harvard Medical School, Boston, MA, USA
*These authors contributed equally to this work
Correspondence: Annie M Wu, Kellogg Eye Center, 1000 Wall Street, Ann Arbor, MI, 48108, USA, Tel +1 408 628 8420, Email [email protected]
Purpose: To assess the rates of postoperative steroid response following dropless cataract surgery using a subconjunctival depot of triamcinolone versus conventional cataract surgery using topical prednisolone.
Patients and Methods: We reviewed consecutive cataract surgery cases performed by a single surgeon to determine the likelihood of steroid response, defined as intraocular pressure (IOP) 50% above baseline or IOP > 24 mmHg postoperatively, excluding the first 72 hours. Logistic regression models were performed including baseline characteristics as exposures in the model and steroid response as the outcome. Main outcome measures were the proportion of eyes developing steroid response, risk factors for developing steroid response, and duration of steroid response.
Results: Of the 150 dropless and 218 conventional cases, 26 eyes developed steroid response (15 dropless and 11 conventional cases [10% vs 5%, P=0.096]). Risk factors for steroid response included dropless surgery (OR=2.43, 95% CI=1.03– 6.02], P=0.046) and prior diagnosis of glaucoma (OR=7.18, 95% CI=2.66– 19.22], P< 0.001). Baseline IOP, age, sex, race, and axial length did not increase risk for steroid response. Of the eyes with steroid response, more dropless cases had an IOP elevation ≥ 30 days (9/15 eyes vs 1/11 eyes; P=0.008), including one patient with refractory IOP elevation in the dropless group who required urgent bilateral trabeculectomy for IOP control.
Conclusion: Dropless cataract surgery increases the risk of prolonged steroid response postoperatively. Patients with glaucoma have an increased risk of steroid response and may not be good candidates for dropless cataract surgery with subconjunctival triamcinolone.
Keywords: ocular hypertension, glaucoma, intraocular pressure, triamcinolone depot, postoperative
Introduction
Cataract surgery is one of the most common surgical procedures performed worldwide.1 Despite its safety and predictability, cataract surgery is continuously being improved to optimize post-operative outcomes.1 Dropless cataract surgery, in which a steroid depot is administered at the time of cataract surgery, has gained popularity as a technique that allows for less dependence on postoperative drops without compromising inflammation control or visual acuity outcomes.2–6 Surgical techniques for dropless cataract surgery are variable and include intravitreal or subconjunctival injections of triamcinolone, and sustained release formulations of dexamethasone as an intracanalicular insert or intraocular suspension.7,8 Dropless cataract surgery has the advantage of eliminating the need for costly and time-consuming eyedrop regimens known to result in poor adherence and undermine surgical results.9 The issue of adherence in the cataract patient population is further compounded by poor administration by individuals inexperienced with the use of conventional eyedrops.10
Despite several advantages to dropless approaches, ocular steroid depot injections are known to cause intraocular pressure (IOP) increase.11–14 Relatively few studies have evaluated the risk of steroid response following dropless cataract surgery, and the findings have thus far been mixed as to whether there is an increased risk for steroid response with ocular steroid depot, with many studies excluding patients with glaucoma.2,15–18 The purpose of this study was to evaluate the incidence and risk factors of steroid-related IOP increase following uncomplicated dropless cataract surgery using subconjunctival triamcinolone compared with conventional cataract surgery using topical prednisolone.
Materials and Methods
Study Population and Databases
This study was approved by the Institutional Review Board of Massachusetts Eye and Ear and adhered to the tenets of the Declaration of Helsinki and the Health Insurance Portability and Accountability Act. The electronic health record was used to extract all cataract surgeries performed by a single surgeon (RP) from January 1, 2020 to September 30, 2021 using the CPT codes 66984 (Extracapsular cataract removal with insertion of intraocular lens prosthesis) and 66982 (Extracapsular cataract extraction removal with insertion of intraocular lens prosthesis, complex). Patients with additional surgery being done at the same time as cataract surgery were excluded. None of the patients underwent concurrent Minimally Invasive Glaucoma Surgery (MIGS) procedures. Additionally, patients with existing retinal abnormalities (eg, retinitis pigmentosa) were excluded from the analysis, as their visual acuity was significantly affected by their retinal condition, and their IOP may have been affected by long-term dorzolamide use for the treatment of macular edema. Informed consent was provided by patients for case reports included in this manuscript.
Outcome
The outcome of interest was steroid response, defined as IOP 50% above baseline or IOP >24 mmHg in the postoperative period, excluding the first 72 hours. Although there is no consensus definition of steroid response in the literature,19–21 we defined steroid response as either a 50% increase in postoperative IOP above baseline or IOP greater than 24 mmHg, as this IOP cutoff has previously been used in major trials including the Ocular Hypertension Treatment Study.22 Our definition tries to capture steroid response in a way that includes significant increases in pressure for any particular case, including both patients with low baseline IOP (50% increase) as well as patients with a higher baseline IOP, in whom an increase that is less than 50% above baseline would nonetheless be clinically meaningful (eg, an increase to 28 mmHg from a baseline IOP of 20 mmHg, which is technically not a 50% increase). We excluded the first 72 hours after cataract surgery to avoid mischaracterizing early postoperative IOP increase due to retained viscoelastic or other early postoperative factors.23
Exposures
Exposure variables that were examined as potential risk factors associated with steroid response included mode of postoperative steroid administration (dropless vs conventional), patient demographics, preoperative variables, and postoperative variables. Conventional cataract surgery cases used 1% topical prednisolone acetate in the postoperative period starting at one drop 4-times daily for the first week, then decreasing by one drop every week over the next 3 weeks, while dropless cataract surgery cases received a subconjunctival injection of triamcinolone. A volume of 0.3–0.5 mL of triamcinolone at a concentration of 40 mg/mL (for a total steroid dose of 12 to 20 mg) was given at the end of the cataract surgery, injected approximately 5 mm posterior to the limbus. Only routine cataract cases were selected for dropless surgery. During the study period, the surgeon had a shift in clinical practice, such that prior to January 1, 2021, cases were preferentially done as conventional cataract surgery, and cases after this date were preferentially done as dropless cataract surgery. There were no prespecified criteria for deciding which patients would have dropless vs conventional type of steroid administration; this decision was based on both surgeon and patient preference.
Demographic information collected included patient age at the time of cataract surgery, sex, and self-reported race. Preoperative variables included surgery laterality, axial length, baseline best corrected visual acuity (BCVA), and baseline IOP of the operated eye. Baseline IOP was defined as the most recent IOP recorded within 1 year prior to cataract surgery. IOP was measured using a Tonopen tonometer or Goldman applanation tonometry (GAT) at all clinic visits. Patients were identified as having a preoperative diagnosis of glaucoma or glaucoma suspect based on the presence of ICD-10-CM codes for glaucoma or glaucoma suspect in the electronic medical record in the year preceding cataract surgery, as cup-to-disc ratio, imaging, and visual field data were not available consistently for the majority of the patients.
Postoperative variables collected included BCVA at postoperative month 1 along with IOP at postoperative day 1 (POD1), week 1 (POW1), and month 1 (POM1) of the operated eye. Patients were required to have a minimum of 1 week of follow-up. Additional postoperative variables included use of IOP-lowering drops in the postoperative period, additional or prolonged steroid use after surgery, and duration of steroid response. Postoperative use of IOP-lowering drops was defined as additional IOP-lowering drops that were started in the postoperative period from 1 to 90 days following cataract surgery (patients who had preoperative glaucoma drops that were continued postoperatively were not included in this count). For conventional cataract cases, additional or prolonged steroid use was defined as any topical steroid use beyond the routine 1% topical prednisolone acetate four times per day for the first week, followed by a weekly taper (eg, more frequent use of steroid starting at POD1, a taper longer than 1 month, or the use of a more potent topical steroid such as difluprednate). For dropless cases, additional steroid use was defined as any topical steroid use in the postoperative period.
Statistical Analysis
Univariate comparisons were performed between dropless cataract surgery and conventional cataract surgery groups using chi-squared tests for categorical variables and t-tests for continuous variables. Sample means were confirmed to follow a normal distribution, which satisfies the requirements of the t-test. To identify multivariate predictors of having a steroid response in the postoperative period in each group, logistic regression models were performed including all baseline variables in the model as exposures and steroid response as the outcome. The main analysis included all consecutive cases of cataract surgery, including second eyes from the same patient. Second eye surgeries were done within 2–4 weeks of the first eye, and therefore outcomes of the first eye did not influence the postoperative steroid plan for the second eye. We performed a supplementary analysis that included only first eyes undergoing surgery in cases where both eyes of the same patient had surgery within the study period. All statistical analyses were conducted using SAS version 9.3 (SAS Institute, Inc, Cary, NC).
Results
A total of 368 eyes were included in the analysis: 150 dropless cases and 218 conventional cases. The mean age at the time of surgery was 69.9±10.4 years (range=34–95 years) and 66.5±12.7 years (range=11–89 years) for dropless and conventional eyes, respectively (P=0.004; Table 1). There was no significant difference in terms of sex, race, glaucoma diagnosis, or glaucoma suspect diagnosis between the two groups (P≥0.32). Baseline IOP was also not significantly different between the two groups (16.6±3.2 mmHg for dropless eyes and 16.4±3.6 mmHg for conventional eyes, P=0.54). Similarly, axial length of the operated eye was not significantly different between the two groups (25.0±2.2 mm for dropless eyes and 24.8±2.2 mm for conventional eyes, P=0.30). Postoperatively, the dropless group showed better BCVA than the conventional group (logMAR BCVA=0.1±0.2 for dropless eyes and 0.2±0.4 for conventional eyes at month 1, P=0.005); this is likely due to four patients in the conventional group with poor baseline visual potential (logMAR BCVA 2.0 or worse). Furthermore, both groups were similar with respect to the proportion of eyes requiring additional or prolonged steroids in the postoperative period for additional inflammation control (17 [11%] dropless eyes and 17 [8%] conventional eyes, P=0.27) and starting IOP-lowering medications in the first 3 postoperative months (20 [13%] dropless eyes and 26 [12%] conventional eyes, P=0.52). Of note, given the surgeon’s shift in practice pattern from default conventional to default dropless cataract surgery in the middle of the study period, most eyes received conventional cataract surgery prior to January 1, 2021 (153 out of 179) and most eyes received dropless cataract surgery after January 1, 2021 (124 out of 189).
 |
Table 1 Demographic, Preoperative, and Postoperative Information for Dropless vs Conventional Cataract Surgery Groups |
The two groups showed significant differences, however, in terms of postoperative IOP. At POD1, POW1, and POM1, the dropless group had significantly higher mean IOP compared with the conventional group (20.6±6.2 vs 19.2±5.8 mmHg at POD1, P=0.03; 16.4±3.5 vs 15.5±3.7 mmHg at POW1, P=0.03; and 16.8±4.0 vs 15.4±3.4 mmHg at POM1, P=0.0008 for dropless vs conventional cases, respectively; Figure 1A). We defined steroid response as IOP 50% above baseline or IOP >24 mmHg in the postoperative period, excluding the first 72 hours after surgery. Using this definition, 15 (10%) of the 150 dropless cases developed a steroid response, compared with 11 (5%) of the 218 conventional cases (P=0.096).
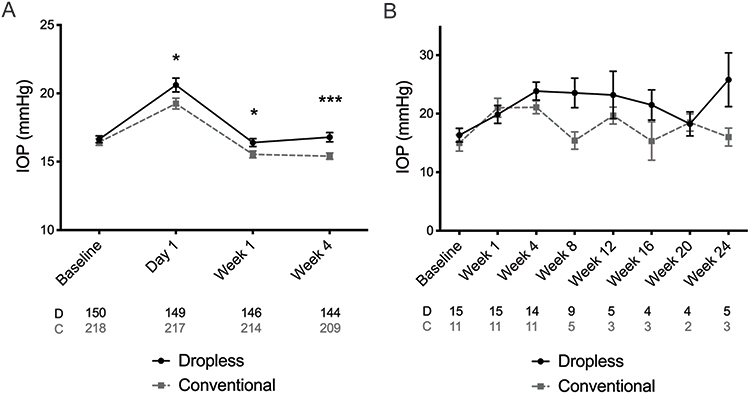 |
Figure 1 (A) Mean intraocular pressure (IOP) of all subjects at baseline, day 1, week 1, and week 4 after cataract surgery. (B) Mean IOP at baseline and postoperative weeks 1–24 in dropless vs conventional cataract surgery eyes with steroid response. The number of subjects in each group and at each timepoint is indicated below the diagram; “D” stands for dropless, “C” for conventional cataract surgery. *P<0.05, ***P<0.001. Error bars show standard error of the mean. |
We next performed univariate and multivariate analyses to identify which demographic, preoperative, and postoperative factors were significantly associated with steroid response (Table 2). In the univariate analysis we found that having a diagnosis of glaucoma was a significant predictor of steroid response (OR=5.65; 95% CI=2.21–13.82, P=0.0002); on the other hand, demographic variables, including age and sex, were not. Additionally, axial length, baseline IOP, glaucoma suspect diagnosis, and additional postoperative steroid use were not found to be predictors of steroid response. In the multivariate analysis, having a diagnosis of glaucoma (OR=7.18; 95% CI=.66–19.22, P<0.001) or having undergone dropless cataract surgery (OR=2.43; 95% CI=1.03–6.02; P=0.046) were significant predictors of steroid response (Table 2).
 |
Table 2 Predictors of Steroid Response in All Eyes Undergoing Cataract Surgery (Univariate and Multivariate Analysis) |
We next evaluated demographic and clinical characteristics of patients in both groups who developed a steroid response (Table 3). There were 15 eyes in the dropless group and 11 eyes in the conventional group with a steroid response. There were no significant demographic or preoperative differences between the two subgroups. While the postoperative IOP trended higher in the dropless group than in the conventional group (Figure 1B) and the duration of steroid response tended to be longer (Table 3), these differences were not statistically significant. However, the dropless surgery subgroup had a greater proportion of eyes with prolonged steroid response lasting 30 days or longer (9/15 eyes [60%] in the dropless group vs 1/11 eyes [18%] in the conventional group, P=0.008; Table 3).
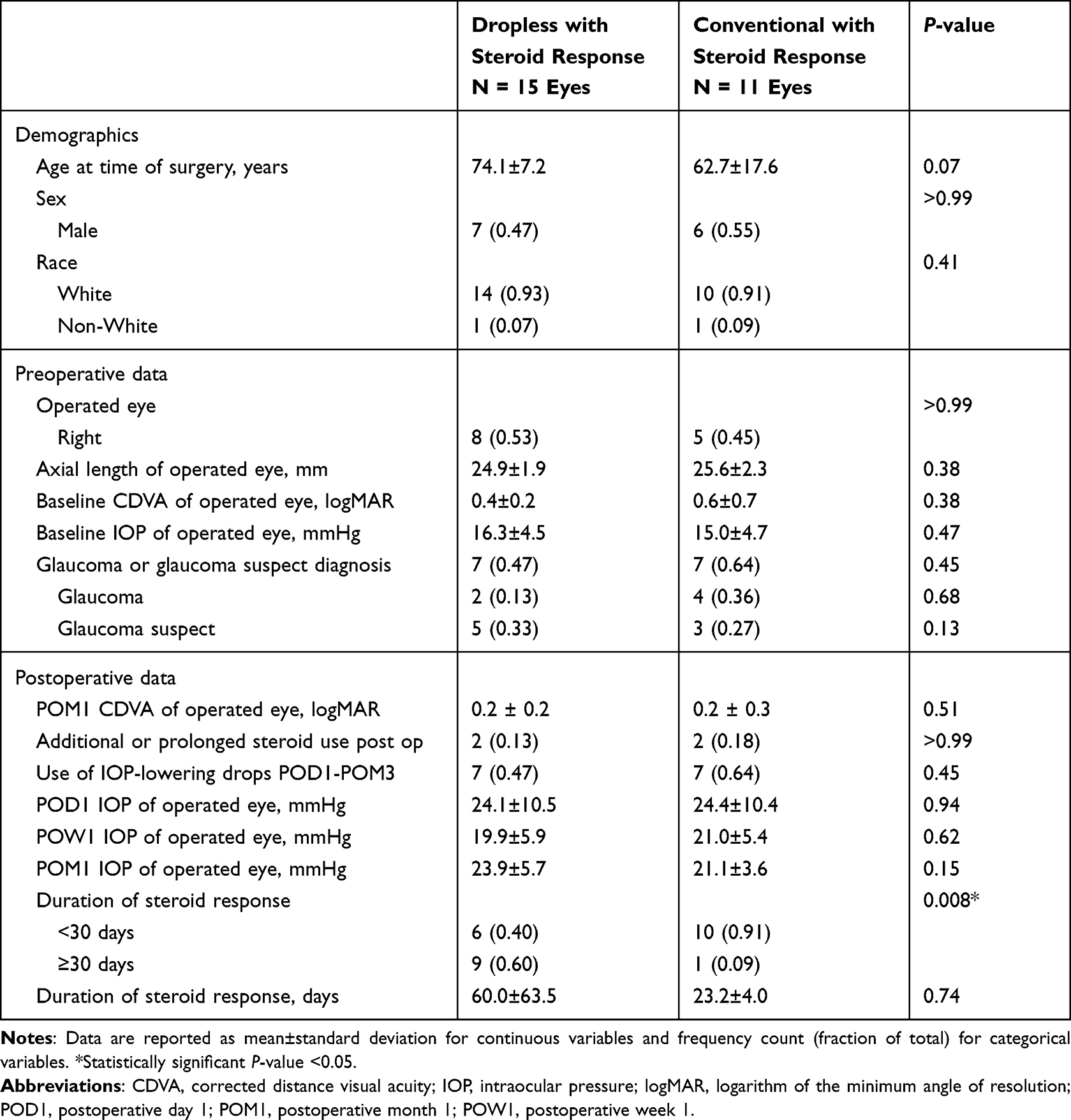 |
Table 3 Characteristics of Dropless vs Conventional Cataract Surgery Eyes That Developed Steroid Response |
Given the potential bias of studying a patient population undergoing bilateral cataract surgery, we performed an additional analysis in which we included only the first eye from each patient undergoing surgery (Supplemental Tables 1-3). This analysis of first eyes included 112 dropless cases and 173 conventional cases. Ten (9%) of the 112 dropless cases developed a steroid response, compared with 11 (6%) of the 173 conventional cases (P=0.49). Demographics were similar between groups, and baseline IOP remained not significantly different between the two groups (16.7±3.2 mmHg for dropless eyes and 16.3±3.6 mmHg for conventional eyes, P=0.35; Supplemental Table 1). Postoperative mean IOP was significantly higher in the dropless group compared with the conventional group at all three time points (20.9±6.5 vs 19.2±6.1 mmHg at POD1, P=0.03; 16.6±3.4 vs 15.6±3.9 mmHg at POW1, P=0.03; 16.7±4.2 vs 15.6±3.6 mmHg at POM1, P=0.02; for dropless vs conventional cases, respectively). In the multivariate analysis of first surgical eyes only, having a diagnosis of glaucoma (OR=4.49; 95% CI=1.30–14.05; P=0.012) or glaucoma suspect (OR=5.83; 95% CI=1.95–16.92; P=0.001) were significant predictors of steroid response (Supplemental Table 2). Dropless cataract surgery was no longer a significant predictor in the first-eyes-only analysis (Univariate analysis OR=1.44, 95% CI=0.58–3.54; P=0.419; Multivariate analysis OR=1.60, 95% CI=0.62–4.11; P=0.325). This may be due to a smaller sample size which excluded a greater proportion of dropless steroid response eyes (in the first-eyes-only analysis, five eyes with steroid response were excluded, all of which were in the dropless group).
Figure 2 highlights a striking case of sustained steroid response following dropless cataract surgery. This is a case of a 70-year-old White male patient who had a history of high myopia (axial length of 28.26 mm in the right eye and 28.12 mm in the left eye) and Laser-Assisted In Situ Keratomileusis (LASIK) in both eyes with central corneal thickness of 450 µm in the right eye and 470 µm in the left eye. He was noted to be a glaucoma suspect prior to cataract surgery based on his optic disc appearance; his preoperative untreated IOP range was 13–16 mmHg in both eyes. He underwent bilateral dropless cataract surgery 2 weeks apart and developed elevated IOP in the postoperative period starting at the first postoperative month, ranging from 23–38 mmHg in the right eye and 21–36 mmHg in the left eye that were refractory to medical management with multiple topical glaucoma medications and oral acetazolamide. He was referred to the glaucoma service for management 5 months after dropless cataract surgery and was found to have severe glaucomatous optic neuropathy with uncontrolled IOP of 42 mmHg in the right eye and 46 mmHg in the left eye. His glaucoma testing demonstrated significant retinal nerve fiber layer (RNFL) thinning on Optical Coherence Tomography (OCT) with average RNFL thicknesses of 47 and 41 μm, and dense arcuate visual field defects approaching fixation bilaterally on Humphrey Visual Field perimetry with mean deviations of −17.23 and −21.28 dB in the right and left eyes, respectively (Figure 2). He underwent emergent trabeculectomy in the right eye followed by the left eye and maintained IOP in the 10–16 mmHg range in both eyes afterwards with stable visual field testing.
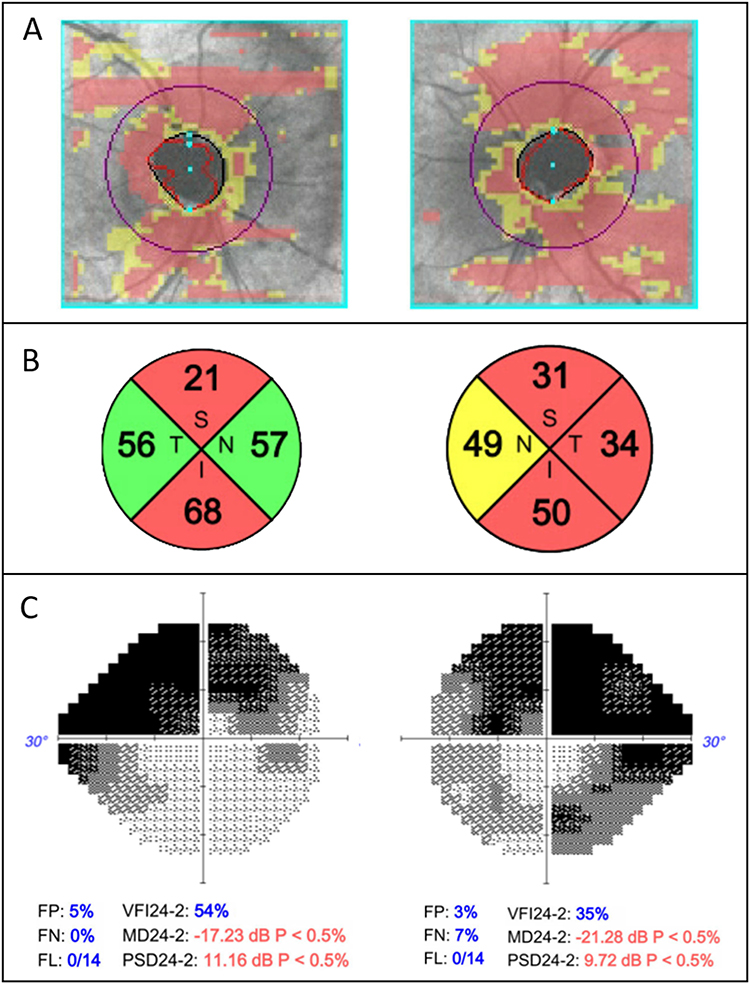 |
Figure 2 Optical Coherence Tomography and Humphrey Visual Field findings of a patient who developed severe glaucoma in the setting of prolonged steroid response following dropless cataract surgery. (A) Cirrus retinal nerve fiber layer (RNFL) Deviation Map for both eyes showing optic disc cupping and thinning of the peripapillary RNFL in both eyes. (B) RNFL thickness by quadrant showing superior and inferior thinning in the right eye and diffuse thinning in the left eye with mean RNFL thickness of 47 and 41 µm in the right and left eyes, respectively. (C) 24–2 SITA-Fast of right and left eyes showing significant arcuate defects in both eyes. |
Discussion
In this study we investigated the incidence and characteristics of steroid response following dropless cataract surgery with subconjunctival triamcinolone or conventional cataract surgery using topical prednisolone in a large patient cohort undergoing surgery with a single, highly experienced cataract surgeon. We found significantly higher mean IOP measurements at every postoperative timepoint in the dropless cataract surgery cohort compared to the conventional group. Furthermore, multivariate analysis demonstrated that dropless cataract surgery with subconjunctival triamcinolone was a significant predictor of steroid response, which occurred in 10% of eyes undergoing this procedure.
Topical corticosteroids after cataract surgery are known to produce steroid-related IOP elevation through mechanisms that increase resistance in the trabecular meshwork.24 In our study, the incidence of steroid response was 5% in the conventional surgery group. This is comparable to prior studies, although the incidence of reported steroid response following cataract surgery varies depending on the IOP cutoff being used.19,20 Chang et al20 reported a 2.4% incidence of postoperative steroid response from topical prednisolone, which is less than our study. However, they defined steroid response as an IOP elevation of 25% above baseline and a minimum of 28 mmHg, since this was the level deemed high enough by the study authors to warrant intervention. A separate study by Bojikian et al19 comparing eyes with and without glaucoma found that the incidence of steroid response in patients receiving topical prednisolone was 2.1% in control eyes and 8.4% in glaucoma eyes, with steroid response defined as IOP >50% above baseline, occurring at or after the second postoperative week. Other studies have used the cutoff of IOP increase greater than 10 mmHg above baseline to characterize steroid response.25–27 In our study, we defined steroid response as either a 50% increase in postoperative IOP above baseline or IOP greater than 24 mmHg, as this IOP cutoff has previously been used in major trials including the Ocular Hypertension Treatment Study, which found that IOP >25.75 mmHg significantly increases the risk of developing primary open angle glaucoma.22 The advantage of our definition is that it includes eyes that started with a low IOP and had a significant IOP increase in the postoperative period, as well as eyes that started with a higher baseline IOP and rose to clinically significant levels, even if that level was not strictly 50% above their baseline.
Steroid depot injections may provide better postoperative inflammation control than topical steroid drops alone, though findings from existing studies are mixed.3–6,28 Several studies have found that eyes receiving steroid injections have lower incidence of cystoid macular edema (CME) following cataract surgery, but there were no significant visual acuity differences between the steroid depot and topical steroid groups on postoperative follow-up.3,28 Other studies found no significant difference in CME but did find lower rates of anterior chamber cell and flare, without a difference in postoperative visual acuity between steroid depot and topical steroid eyes (although the study examiners were not blinded to the type of steroid patients received).4,6 While we did not have OCT data for all eyes in our study to assess the presence of CME, we did not find any difference between dropless and conventional groups with respect to requiring additional steroids in the postoperative period for inflammation control. This would suggest that steroid type did not significantly affect postoperative inflammation control. Larger randomized studies are required to better assess differences in inflammation control following dropless vs conventional cataract surgery.
Relatively few studies have evaluated the risk of steroid response following dropless cataract surgery, and the findings have thus far been mixed. In existing studies there is much variation in steroid type and dosages administered, with many studies using a short duration of follow-up and excluding patients with glaucoma or family history of glaucoma.2,15–18,29 In the Prevention of Macular Edema after cataract surgery (PREMED) randomized controlled clinical trial, patients receiving a 40 mg subconjunctival injection of triamcinolone had a significantly higher IOP compared to patients who did not.29 Additionally, six of the 51 (12%) patients who received subconjunctival triamcinolone developed IOP elevation of 25 mmHg or higher at 12 weeks postoperatively.29 In a separate randomized controlled trial, Paganelli et al2 compared patients receiving 40 mg of sub-Tenon’s triamcinolone with patients receiving an equal volume of sub-Tenon’s balanced salt solution and 1% topical prednisolone acetate following cataract surgery. Surprisingly, the authors found that the sub-Tenon’s triamcinolone group had lower mean IOP measurements at several postoperative visits up to day 28 post-op, and no patient had an IOP rise in the postoperative period up to 2 months post-op. However, this study was relatively small, with 50 patients per group, and notably excluded patients with prior topical steroid use, diagnosis of glaucoma, and prior steroid-related ocular hypertension. Additionally, steroid response may not occur until months after the exposure, and 2 months of follow-up may not have been enough to capture late responders.30 Negi et al16 reported on the results of a smaller prospective trial of 54 patients, with 27 patients in the topical prednisolone and 27 patients in the steroid depot group, some of whom received 20 mg, and others 30 mg triamcinolone. The authors found consistently higher mean IOP measurements in the triamcinolone depot group at each post-operative visit up to 90 days after surgery, which was similar to our findings (Table 1), although the differences in their study were not statistically significant. Of note, this trial excluded patients with a family history of glaucoma. We did not assess for family history of glaucoma as this information was not consistently available. However, we did include patients with glaucoma and glaucoma suspect in our study, which is more representative of how dropless cataract surgery is performed in an actual clinical setting, where patients may present with these diagnoses to a comprehensive ophthalmology clinic.31
Some studies have proposed that the location of triamcinolone depot could affect the likelihood of steroid response. Intravitreal triamcinolone has been reported to result in higher rates of steroid response than we found in our study, with even low doses of 4 mg of intravitreal triamcinolone resulting in 32–50% incidence of steroid response.13,32 With sub-Tenon’s injection of triamcinolone, a more posterior site of injection may be less likely to induce IOP elevation.33–36 Prior studies on dropless cataract surgery using triamcinolone injected approximately 3.5 mm or 10 mm posterior to the limbus did not result in greater risk for IOP increase postoperatively.2,28 Our injection distance was within range of these studies, at 5 mm posterior to the limbus. Herschler34 reported on a small series of 13 eyes receiving 40 mg of triamcinolone for various inflammatory conditions, 10 of which were in the anterior sub-Tenon’s space, and all 10 of which experienced an IOP increase. Of note, the authors reported that several patients who did not have a history of IOP rise secondary to topical steroids still ended up with IOP elevation after sub-Tenon’s triamcinolone. However, this study and others are limited by their relatively small sample size; more work needs to be done using larger sample sizes to evaluate the effects of steroid dosing and depot location on the risk of developing a steroid response.
A particular concern highlighted by our study is the risk of prolonged and severe intraocular pressure elevation with steroid depot injections. The mean postoperative IOP was higher in the dropless group compared to the conventional group (Figure 1A), and more dropless eyes had a steroid response lasting ≥30 days compared with conventional surgery eyes (Table 3), likely related to the residual steroid depot remaining in the eye longer than the usual postoperative course of topical prednisolone. IOP increase following sub-Tenon’s or subconjunctival triamcinolone injection can often be refractory to medical management, and may require surgical intervention.29,34,35 In the case series by Herschler,34 nine out of the 10 patients with steroid response following sub-Tenon’s triamcinolone required excision of the depot due to medically refractory IOP rise, and one patient required goniotomy. One patient in the PREMED study required excision of the subconjunctival triamcinolone depot after IOP elevation to 42 mm Hg that was refractory to medical management.29 We report on a striking case of bilateral and medically refractory IOP elevation in a patient with a history of LASIK and prior high myopia, who was considered a glaucoma suspect prior to cataract surgery due to optic disc appearance but was not using glaucoma drops prior to cataract surgery. When the patient presented to the glaucoma service with IOP of over 40 mmHg in each eye, the decision was made to proceed emergently with trabeculectomy rather than excision of the steroid depot, given the severity of glaucomatous damage that had already occurred. At the time of trabeculectomy (5 months after the initial cataract surgery), the triamcinolone depot was noted to have not yet fully dissolved, which may have contributed to ongoing IOP elevation in this patient. In addition to this striking case, several other patients in the dropless cataract group required prolonged treatment with glaucoma medications in the postoperative period, including one patient who required 5 months of oral methazolamide to control IOP after dropless surgery.
Another key finding of our study was that eyes with glaucoma were significantly more likely to have a steroid response than non-glaucoma eyes (P<0.001). Glaucoma is a known risk factor for steroid response, irrespective of the route of steroid administration.19,32,37,38 Other studies have previously also identified younger age, male sex, and higher axial length as additional risk factors for steroid response.19–21,38 We did not find these characteristics to be risk factors for steroid response, and by far the most significant risk factor was a prior diagnosis of glaucoma. Of note, however, over 50% of patients with steroid response in our study had an axial length greater than 24.5 mm, and the highlighted case of bilateral severe IOP elevation involved a highly myopic patient with axial length exceeding 28 mm in each eye. It is possible that larger sample sizes are needed to better evaluate whether age, sex, and axial length are significant risk factors for steroid response in this surgical context.
Our study had several limitations. As this was a retrospective study, patients were not randomized into dropless vs conventional surgery groups. Although we only included uncomplicated cataract cases, there may have been inherent selection bias by the surgeon and the patients in choosing the type of postoperative steroid. Interestingly, the dropless group had a higher mean age than the conventional group; thus, it is possible that dropless surgery was preferentially performed in older individuals since they may have more difficulty instilling drops in the postoperative period. However, as mentioned, given the shift in practice pattern from default conventional to default dropless cataract surgery in the middle of the study period, most eyes received conventional cataract surgery prior to January 1, 2021, and most eyes received dropless cataract surgery after January 1, 2021, thus likely reducing selection bias. Another limitation is that the diagnoses of glaucoma or glaucoma suspect were based on chart review and existing ICD-10-CM diagnosis codes present before surgery, and most patients were not formally screened for glaucoma with OCT or visual field testing prior to undergoing cataract surgery. Thus, there may have been mischaracterization or under-characterization of glaucoma patients in our study. If a patient had bilateral cataract surgery during the study period, both eyes were included in the analysis, although we provide analysis of first-operative-eyes-only in Supplemental Tables 1–3. While including both eyes may have introduced inter-eye bias, it made our study more in line with real-world practice patterns, in which patients most commonly undergo sequential cataract surgery within a short period of time. Additionally, we did not include patients undergoing MIGS given the nature of practice at our hospital, where surgeons performing dropless cataract surgery are not glaucoma specialists and do not routinely perform MIGS at the time of cataract surgery. The use of concurrent MIGS with dropless cataract surgery has been explored in a previous study and may warrant additional research.39 Finally, our study population was predominantly White; future work will need to address if the same findings are present in patients from other racial groups, some of which have a higher baseline incidence of glaucoma and therefore may be expected to have a heightened steroid response following dropless cataract surgery.40–42
Conclusion
Dropless cataract surgery has become preferred by many anterior segment surgeons and patients given that it offers good postoperative control of inflammation while reducing drop dependence and potentially leads to more consistent outcomes after cataract surgery.2–6 However, caution must be exercised in light of possible increased rates of steroid response and greater likelihood of prolonged steroid response following steroid depot injection. Going forward, quality prospective studies will be needed to evaluate whether steroid depot dosage or location affect risk for IOP elevation following dropless cataract surgery. Nonetheless, patient selection prior to surgery will continue to be critical, and we propose that patients suspicious for glaucoma or with a known diagnosis of glaucoma should be carefully identified and evaluated prior to dropless cataract surgery given their significant risk for IOP elevation and irreversible vision loss in response to steroids.
Acknowledgments
Lucy Q Shen and Milica A Margeta are co-senior authors for this study.
Disclosure
M. A. M. has been supported by NIH/NEI K12 EY016335, NIH/NEI K08 EY030160, an American Glaucoma Society Young Clinician Scientist Award, a Research to Prevent Blindness Career Development Award, Glaucoma Research Foundation Catalyst for a Cure Initiative to Prevent and Cure Neurodegeneration Award, Alcon Research Institute Young Investigator Award, Massachusetts Lions Eye Research Fund, Robert M. Sinskey Foundation, Ruettgers Family Charitable Foundation, and B.L. Manger Foundation. M. A. M. is also a consultant for Idorsia Pharmaceuticals. L. Q. S. is supported by NIH/NEI R01EY031696. L. Q. S. is also a consultant for FireCyte Therapeutics, Inc and AbbVie Inc. M. W. is supported by NIH R00 EY028631, Research to Prevent Blindness International Research Collaborators Award and Alcon Young Investigator Grant. R. P. is a consultant for Sanofi-Genzyme and Elsevier. The authors report no other conflicts of interest in this work.
References
1. Grzybowski A. Recent developments in cataract surgery. Ann Transl Med. 2020;8(22):1540. doi:10.21037/atm-2020-rcs-16
2. Paganelli F, Cardillo JA, Melo LA Jr, Oliveira AG, Skaf M, Costa RA. A single intraoperative sub-Tenon’s capsule triamcinolone acetonide injection for the treatment of post-cataract surgery inflammation. Ophthalmology. 2004;111(11):2102–2108. doi:10.1016/j.ophtha.2004.04.026
3. Lindholm JM, Taipale C, Ylinen P, Tuuminen R. Perioperative subconjunctival triamcinolone acetonide injection for prevention of inflammation and macular oedema after cataract surgery. Acta Ophthalmol. 2020;98(1):36–42. doi:10.1111/aos.14175
4. Dieleman M, Wubbels RJ, van Kooten-Noordzij M, de Waard PW. Single perioperative subconjunctival steroid depot versus postoperative steroid eyedrops to prevent intraocular inflammation and macular edema after cataract surgery. J Cataract Refract Surg. 2011;37(9):1589–1597. doi:10.1016/j.jcrs.2011.03.049
5. Reddy JK, Chaitanya V, Shah N, Guduru VP, Khan S, Kuttupalayam S. Safety & efficacy of single subconjunctival triamcinolone 5 mg depot vs topical loteprednol post cataract surgery: less drop cataract surgery. Int J Ophthalmol. 2019;12(5):774–778. doi:10.18240/ijo.2019.05.11
6. Kuriakose RK, Cho S, Nassiri S, Hwang FS. Comparative Outcomes of Standard Perioperative Eye Drops, Intravitreal Triamcinolone Acetonide-Moxifloxacin, and Intracameral Dexamethasone-Moxifloxacin-Ketorolac in Cataract Surgery. J Ophthalmol. 2022;2022:4857696. doi:10.1155/2022/4857696
7. Shorstein NH, Myers WG. Drop-free approaches for cataract surgery. Curr Opin Ophthalmol. 2020;31(1):67–73. doi:10.1097/icu.0000000000000625
8. Assil KK, Greenwood MD, Gibson A, Vantipalli S, Metzinger JL, Goldstein MH. Dropless cataract surgery: modernizing perioperative medical therapy to improve outcomes and patient satisfaction. Curr Opin Ophthalmol. 2021;32(Suppl 1):S1–s12. doi:10.1097/icu.0000000000000708
9. Hermann MM, Ustündag C, Diestelhorst M. Electronic compliance monitoring of topical treatment after ophthalmic surgery. Int Ophthalmol. 2010;30(4):385–390. doi:10.1007/s10792-010-9362-3
10. An JA, Kasner O, Samek DA, Lévesque V. Evaluation of eyedrop administration by inexperienced patients after cataract surgery. J Cataract Refract Surg. 2014;40(11):1857–1861. doi:10.1016/j.jcrs.2014.02.037
11. Kuley B, Storey PP, Pancholy M, et al. Ocular hypertension following 40 mg sub-Tenon triamcinolone versus 0.7 mg dexamethasone implant versus 2 mg intravitreal triamcinolone. Can J Ophthalmol. 2020;55(6):480–485. doi:10.1016/j.jcjo.2020.06.021
12. Rezkallah A, Mathis T, Abukhashabah A, et al. Long-term incidence and risk factors of ocular hypertension following dexamethasone-implant injections: the safodex-2 study. Retina. 2021;41(7):1438–1445. doi:10.1097/iae.0000000000003080
13. Rhee DJ, Peck RE, Belmont J, et al. Intraocular pressure alterations following intravitreal triamcinolone acetonide. Br J Ophthalmol. 2006;90(8):999–1003. doi:10.1136/bjo.2006.090340
14. Jonas JB, Degenring RF, Kreissig I, Akkoyun I, Kamppeter BA. Intraocular pressure elevation after intravitreal triamcinolone acetonide injection. Ophthalmology. 2005;112(4):593–598. doi:10.1016/j.ophtha.2004.10.042
15. Merkoudis N, Wikberg Matsson A, Granstam E. Comparison of peroperative subconjunctival injection of methylprednisolone and standard postoperative steroid drops after uneventful cataract surgery. Acta Ophthalmol. 2014;92(7):623–628. doi:10.1111/aos.12358
16. Negi AK, Browning AC, Vernon SA. Single perioperative triamcinolone injection versus standard postoperative steroid drops after uneventful phacoemulsification surgery: randomized controlled trial. J Cataract Refract Surg. 2006;32(3):468–474. doi:10.1016/j.jcrs.2005.12.102
17. Choopong P, Taetrongchit N, Boonsopon S, et al. Efficacy of subtenon 20-mg triamcinolone injection versus 0.1% dexamethasone eye drops for controlling inflammation after phacoemulsification: a randomized controlled trial. Sci Rep. 2022;12(1):16471. doi:10.1038/s41598-022-20522-y
18. Paganelli F, Cardillo JA, Melo LA Jr, et al. A single intraoperative sub-tenon’s capsule injection of triamcinolone and ciprofloxacin in a controlled-release system for cataract surgery. Invest Ophthalmol Vis Sci. 2009;50(7):3041–3047. doi:10.1167/iovs.08-2920
19. Bojikian KD, Nobrega P, Roldan A, Forrest SL, Tsukikawa M, Chen PP. Incidence of and Risk Factors for Steroid Response After Cataract Surgery in Patients With and Without Glaucoma. J Glaucoma. 2021;30(4):e159–e163. doi:10.1097/ijg.0000000000001785
20. Chang DF, Tan JJ, Tripodis Y. Risk factors for steroid response among cataract patients. J Cataract Refract Surg. 2011;37(4):675–681. doi:10.1016/j.jcrs.2010.10.051
21. Rajendrababu S, Pallamparthy S, Arunachalam A, et al. Incidence and risk factors for postoperative intraocular pressure response to topical prednisolone eye drops in patients undergoing phacoemulsification. Int Ophthalmol. 2021;41(12):3999–4007. doi:10.1007/s10792-021-01972-1
22. Gordon MO, Beiser JA, Brandt JD, et al. The Ocular Hypertension Treatment Study: baseline factors that predict the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120(6):714–720. doi:10.1001/archopht.120.6.714
23. Probst LE, Hakim OJ, Nichols BD. Phacoemulsification with aspirated or retained Viscoat. J Cataract Refract Surg. 1994;20(2):145–149. doi:10.1016/s0886-3350(13)80154-x
24. Raghunathan VK, Morgan JT, Park SA, et al. Dexamethasone Stiffens Trabecular Meshwork, Trabecular Meshwork Cells, and Matrix. Invest Ophthalmol Vis Sci. 2015;56(8):4447–4459. doi:10.1167/iovs.15-16739
25. Stewart RH, Smith JP, Rosenthal AL. Ocular pressure response to fluorometholone acetate and dexamethasone sodium phosphate. Curr Eye Res. 1984;3(6):835–839. doi:10.3109/02713688409000796
26. Korenfeld MS, Silverstein SM, Cooke DL, Vogel R, Crockett RS. Difluprednate ophthalmic emulsion 0.05% for postoperative inflammation and pain. J Cataract Refract Surg. 2009;35(1):26–34. doi:10.1016/j.jcrs.2008.09.024
27. Donnenfeld ED, Holland EJ, Solomon KD, et al. A multicenter randomized controlled fellow eye trial of pulse-dosed difluprednate 0.05% versus prednisolone acetate 1% in cataract surgery. Am J Ophthalmol. 2011;152(4):609–617.e1. doi:10.1016/j.ajo.2011.03.018
28. Karasu B, Kesim E, Kaskal M, Celebi ARC. Efficacy of topical dexamethasone eye drops in preventing ocular inflammation and cystoid macular edema following uncomplicated cataract surgery with or without injection of a single dose perioperative subtenon triamcinolone acetonide. Cutan Ocul Toxicol. 2022;41(4):310–317. doi:10.1080/15569527.2022.2136193
29. Wielders LHP, Schouten J, Winkens B, et al. Randomized controlled European multicenter trial on the prevention of cystoid macular edema after cataract surgery in diabetics: ESCRS PREMED Study Report 2. J Cataract Refract Surg. 2018;44(7):836–847. doi:10.1016/j.jcrs.2018.05.015
30. Kalina RE. Increased intraocular pressure following subconjunctival corticosteroid administration. Arch Ophthalmol. 1969;81(6):788–790. doi:10.1001/archopht.1969.00990010790006
31. Pham TQ, Wang JJ, Rochtchina E, Maloof A, Mitchell P. Systemic and ocular comorbidity of cataract surgical patients in a western Sydney public hospital. Clin Exp Ophthalmol. 2004;32(4):383–387. doi:10.1111/j.1442-9071.2004.00842.x
32. Vasconcelos-Santos DV, Nehemy PG, Schachat AP, Nehemy MB. Secondary ocular hypertension after intravitreal injection of 4 mg of triamcinolone acetonide: incidence and risk factors. Retina. 2008;28(4):573–580. doi:10.1097/IAE.0b013e31816079e8
33. Mueller AJ, Jian G, Banker AS, Rahhal FM, Capparelli E, Freeman WR. The effect of deep posterior subtenon injection of corticosteroids on intraocular pressure. Am J Ophthalmol. 1998;125(2):158–163. doi:10.1016/s0002-9394(99)80085-3
34. Herschler J. Increased intraocular pressure induced by repository corticosteroids. Am J Ophthalmol. 1976;82(1):90–93. doi:10.1016/0002-9394(76)90669-3
35. Akduman L, Kolker AE, Black DL, Del Priore LV, Kaplan HJ. Treatment of persistent glaucoma secondary to periocular corticosteroids. Am J Ophthalmol. 1996;122(2):275–277. doi:10.1016/s0002-9394(14)72027-6
36. Liu X, Li Y, Zhang Y, et al. Comparison of intraocular pressure elevation after anterior versus posterior subtenon triamcinolone acetonide acetate injection: a retrospective study. Retina. 2012;32(9):1838–1843. doi:10.1097/IAE.0b013e31824fd384
37. Becker B, Mills DW. CORTICOSTEROIDS AND INTRAOCULAR PRESSURE. Arch Ophthalmol. 1963;70:500–507. doi:10.1001/archopht.1963.00960050502012
38. Malclès A, Dot C, Voirin N, et al. SAFETY OF INTRAVITREAL DEXAMETHASONE IMPLANT (OZURDEX): the SAFODEX study. Incidence and Risk Factors of Ocular Hypertension. Retina. 2017;37(7):1352–1359. doi:10.1097/iae.0000000000001369
39. Jackson KJ, Akrobetu D, Guduru A, Herndon LW. Intracanalicular Dexamethasone Insert or Topical Prednisolone Following iStent and Hydrus Surgery for Glaucoma. J Glaucoma. 2022;31(8):694–699. doi:10.1097/ijg.0000000000002037
40. Tielsch JM, Sommer A, Katz J, Royall RM, Quigley HA, Javitt J. Racial variations in the prevalence of primary open-angle glaucoma. The Baltimore Eye Survey. JAMA. 1991;266(3):369–374.
41. Friedman DS, Jampel HD, Muñoz B, West SK. The prevalence of open-angle glaucoma among blacks and whites 73 years and older: the Salisbury Eye Evaluation Glaucoma Study. Arch Ophthalmol. 2006;124(11):1625–1630. doi:10.1001/archopht.124.11.1625
42. Rodriguez J, Sanchez R, Munoz B, et al. Causes of blindness and visual impairment in a population-based sample of U.S. Hispanics. Ophthalmology. 2002;109(4):737–743. doi:10.1016/s0161-6420(01)01008-9
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Patient Tolerability of Omidenepag Isopropyl in the Treatment of Glaucoma and Ocular Hypertension
Matsuo M, Matsuoka Y, Tanito M
Clinical Ophthalmology 2022, 16:1261-1279
Published Date: 26 April 2022
Treatment of Open-Angle Glaucoma and Ocular Hypertension with the Fixed-Dose Combination of Preservative-Free Tafluprost/Timolol: Clinical Outcomes from Ophthalmology Clinics in Italy
Oddone F, Scorcia V, Iester M, Sisto D, De Cilla S, Bettin P, Cagini C, Figus M, Marchini G, Rossetti L, Rossi G, Salgarello T, Scuderi GL, Staurenghi G
Clinical Ophthalmology 2022, 16:1707-1719
Published Date: 1 June 2022
Retrospective Analysis of Switching Bimatoprost 0.01% to Bimatoprost 0.03% in Patients with Various Types of Glaucoma and Ocular Hypertension
Xu KM, Cho R, Chan TYB
Clinical Ophthalmology 2022, 16:2385-2390
Published Date: 29 July 2022
Late-Onset Ocular Hypotensive Effect of Ripasudil on Primary Open-Angle Glaucoma
Sano K, Terauchi R, Fukai K, Ogawa S, Noro T, Tatemichi M, Nakano T
Clinical Ophthalmology 2024, 18:3905-3912
Published Date: 24 December 2024
Ocular Hypertension Following Open Globe Injury in Patients Undergoing Pars Plana Vitrectomy
Karimaghaei S, Al-Hindi H, Chauhan MZ, Elhusseiny AM, Sanvicente CT, Uwaydat SH
Clinical Ophthalmology 2025, 19:1339-1344
Published Date: 19 April 2025