")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Triglyceride-Glucose Index is a Risk Marker of Incident COPD Events in Women
Authors Zaigham S , Tanash H, Nilsson PM , Muhammad IF
Received 4 February 2022
Accepted for publication 30 April 2022
Published 17 June 2022 Volume 2022:17 Pages 1393—1401
DOI https://doi.org/10.2147/COPD.S360793
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Suneela Zaigham,1 Hanan Tanash,2 Peter M Nilsson,1,3 Iram F Muhammad1
1Department of Clinical Sciences, Lund University, Malmö, Sweden; 2Department of Respiratory Medicine, Skåne University Hospital, Lund University, Malmö, Sweden; 3Department of Internal Medicine, Skåne University Hospital, Malmö, Sweden
Correspondence: Suneela Zaigham, Department of Clinical Sciences, Lund University, Malmö, Sweden, Tel +46 708737179, Email [email protected]
Purpose: The triglyceride-glucose index (TyG index) is a marker of insulin resistance and metabolic dysfunction and has the advantage of being universally available. Although recent evidence suggests the TyG index has relevance to respiratory health, there have been no prospective studies assessing its value as a biomarker for chronic lung diseases. We aim to assess the TyG index as a potential risk marker for future incident COPD events in the general population.
Patients and Methods: Baseline TyG index was assessed in 28,282 middle-aged men and women without previous history of chronic obstructive pulmonary disease (COPD) from the Malmö Preventive Project (men between 1974 and 1982 and women between 1982 and 1992). All subjects were followed up prospectively, and Cox proportional hazards regression was used to assess incident COPD events according to quartiles of TyG index.
Results: After an average of 31 years of follow-up, TyG index was a strong predictor of future COPD events even after adjusting for potential confounders (Q4 (highest TyG index) HR (95% CI): 1.21 (1.09– 1.35) vs Q1 (reference), p-trend < 0.001). After stratifying by sex, the results remained statistically significant in women only (Q4 vs Q1 HR 1.72 (1.41– 2.09)). Additionally, the risk remained significant in a cohort of life-long never smokers (Q4 vs Q1 HR 1.47 (1.08– 2.01)).
Conclusion: A raised TyG index is a novel risk marker of future incident COPD events in women. Insulin resistance as reflected by the TyG index can precede the development of obstructive lung disease and as such may be an easily measurable and useful predictor of COPD in women.
Keywords: chronic obstructive pulmonary disease, cohort study, epidemiology, risk prediction, triglyceride-glucose index
Introduction
Disorders of glucose metabolism and insulin resistance such as the metabolic syndrome (MetS) and type 2 diabetes (T2DM) are prevalent in chronic obstructive pulmonary disease (COPD).1 Furthermore, COPD is thought to be a predictor of the development of T2DM2 resulting in a higher prevalence of T2DM in COPD patients than in the general population. Potential explanations include reduced physical activity associated with COPD3 and effects of low-grade systemic inflammation in COPD that has also been linked to the incidence of T2DM.4,5 The presence of T2DM has been suggested as a factor that may influence the progression and prognosis of COPD.6,7 The likely mechanisms include the direct effects of hyperglycaemia on the lung parenchyma – leading to changes in the connective tissue and elastic recoil of the lung, increased microangiopathy, muscle weakness and systemic inflammation.8 The incidence of COPD has been found to be greater in those with diabetes than in those without.9 MetS, insulin resistance and systemic inflammation have also been found to be important risk markers for reduced lung function in healthy, non-smoking subjects,10 however, fewer studies exist that assess the role of insulin resistance as a contributing factor in the pathogenesis of COPD and its progression.11
A novel marker of insulin resistance and associated metabolic dysfunction – the triglyceride-glucose index (TyG index) has been developed that is universally available and takes into account both glucotoxicity and lipotoxicity, key players in insulin resistance.12 It is measured using fasting glucose and triglycerides, which are clinically routine measurements. It is comparable to both the euglycaemic-hyperinsulinaemic clamp and the Homeostatic Model Assessment for Insulin Resistance (HOMA-IR) index for the assessment of insulin sensitivity.13,14 Although the HOMA-IR index has previously been associated with lower lung function,15 we are aware of only one previous study that has assessed the TyG index in relation to lung health,16 which provides recent evidence for a cross-sectional association between the TyG index and respiratory symptoms, chronic bronchitis and restrictive spirometry patterns. The study was based on National Health and Nutrition Examination Survey (NHANES) data and included a high proportion of subjects with MetS (55%).16 It concluded that validation of TyG index as a biomarker for impaired lung health is needed using prospective studies from various populations.
To our knowledge, no study has examined if the TyG index can be a prospective risk marker for future COPD. We therefore aim to assess the TyG index as a potential risk marker for future incident COPD events in the general population.
Materials and Methods
Study Population
The study population consisted of subjects examined as part of the Malmö Preventive Project (MPP).17 A total of 33,346 middle-aged subjects were screened at baseline between 1974 and 1992 (22,444 men and 10,902 women) with a participation rate of over 70%. Mail invitations were sent to complete birth-cohorts for the years 1921–1949, who were living in Malmö at the time. Subjects were invited for a physical examination, laboratory tests, spirometry and self-administered questionnaires. Men were mainly screened between 1974 and 1982, and women between 1982 and 1992. The baseline examinations were approved and funded by the health service authority of the city of Malmö. Written consent was not available at the time the study was conducted (1974–1992), however verbal consent was taken for all participants included in the study. The Regional Ethics Committee at Lund (LU 85–2004; LU 2011–412) approved prospective follow-up of the cohort and data linkage with the national Cause of Death and Patient Registers. Subjects with known prevalent COPD were excluded (n = 127). Spirometry was performed in birth cohorts during most but not all screening periods (94% of men and 71% of women); however, individuals were not selected based on symptoms or disease. Subjects with missing information on spirometry (n = 4386), baseline triglycerides and glucose (n = 166) or other key covariates (n = 324) were excluded. Subjects with an erythrocyte sedimentation rate (ESR) ≥50 mm/h were excluded (n = 61) as this could potentially indicate the presence of a specific inflammatory lung pathology at baseline. The final study population consisted of 28,282 subjects (20,892 men and 7390 women).
Baseline Examinations
Blood samples for triglycerides and glucose measurements were taken after an overnight fast and analysed at the Department of Clinical Chemistry, Malmö University Hospital. Plasma insulin was measured using a nonspecific radioimmunoassay (RIA) method, the detection limit being 3 mIU L-1. The RIA method was originally developed at the Department of Clinical chemistry in Malmö and was attached to a continuing standardization programme.18 ESR was determined according to the Westergren method. Height (metres) was measured using a fixed stadiometer; weight (kilograms, kg) was measured on a balance beam scale. Body mass index (BMI) was calculated as kg/m2. Information on smoking habits was assessed using a questionnaire, and participants were divided into never or ever (former and current) smokers. Subjects were also categorised as heavy smokers using the response to the question “Do you smoke more than 20 cigarettes/day?”. Information on physical activity was assessed using questionnaire responses. Details of these questions in men and women have been described in detail elsewhere.19 Information on prevalent diabetes was obtained using self-reported diabetes at baseline, fasting whole-blood glucose ≥6.1mmol/L at baseline (corresponding to a plasma glucose of ≥7.0 mmol/L) or any prior diagnosis of diabetes in diabetic or hospital registers. Information on prevalent cardiovascular disease (CVD) was obtained using self-reported CVD at baseline and registers of hospital inpatients. Forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC) were measured using a spirotron apparatus (Drägerwerk AG, Lübeck, Germany) and carried out by trained nursing staff. Only one acceptable manoeuvre was required.20
Exposure Definition
To calculate the TyG index, the following formula was used:21–23
Log (fasting triglycerides (mg per dL) × fasting glucose (mg per dL))/2.
The TyG index was then used as both a continuous variable and as quartiles for further analyses, where Q1 had the lowest (reference category) and Q4 had the highest value.
Endpoint Ascertainment
All subjects with a history of COPD at baseline (according to self-reported COPD or COPD recorded as part of any patient registers) were excluded. The International Classification of Diseases (ICD) 8 codes 490–492, ICD 9 codes 490–492 and 496, and ICD 10 codes J40-J44 were used to define incident COPD events.24,25 An incident COPD event was defined as a first COPD hospitalisation, outpatient visit or death due to COPD in those with no previous COPD diagnosis and was established from hospital discharge summaries, outpatient data from Swedish hospitals (additional outpatient data specifically from Region Skåne) and information on death certificates. COPD as the primary cause or 1st or 2nd secondary cause for hospital admission, outpatient review or death was used to define an incident COPD event. The Swedish inpatient registry had been operating in the south of Sweden during the entire follow-up period and became nationwide in 1987. Data from the Swedish inpatient registry has been found to be of acceptable validity for epidemiological research, including the outcome of COPD.25 All subjects were followed from the baseline examination until the first COPD event, death from other causes, emigration or last follow-up date (31st December, 2019).
Statistical Analysis
All analyses were carried out using SPSS version 26 (IBM Corp., Armonk, NY, USA). One-way analysis of variance (ANOVA) and Pearson’s chi-square test were used to analyse baseline characteristics across quartiles of TyG index. Cox regression models were used to obtain hazard ratios (HR) for incident COPD events per 1-unit increase in the TyG index and across the quartiles. Time from baseline examination to the first incident COPD event, death from other causes or emigration – whichever came first, was used. Cox proportional hazards assumption was tested using time-dependent covariate analysis for men and women separately and visually using Kaplan–Meier plots. Adjustments were made for potential confounders. Confounders to be included in the models were based on known risk factors for a raised TyG index and COPD that may affect the exposure–outcome relationship. As there was a significant interaction between sex and TyG index (p < 0.001), sex-specific quartiles were constructed to examine men and women separately. In order to fully exclude the role of smoking, we performed additional analyses in different categories of smoking status including life-long never smokers. A p-value <0.05 was regarded as statistically significant (two-sided). The p-trend across quartiles was calculated by entering the quartiles of TyG index variable as a continuous term in the Cox models.
Results
Only 3.1% of the total population had prevalent diabetes at baseline and 4.7% were taking antihypertensive drugs. Less than half of the population had a BMI ≥25.0 kg/m2 (38.8%). Baseline characteristics are presented in Table 1. There was a lower proportion of women in Q4 of TyG index as compared to Q1. Height, BMI, ESR, proportion of ever-smokers, heavy smokers, subjects taking anti-hypertensive medicationand subjects with CVD or diabetes increased as the TyG index increased (p < 0.001 for all). The FEV1/FVC ratio decreased as the TyG index increased (p < 0.001). Broadly similar patterns were observed in women and men when examined separately (Supplement Table S1). A higher proportion of men were heavy smokers in Q4 compared to women, and a higher proportion of women were taking antihypertensive drugs in Q4 compared to men.
 |
Table 1 Baseline Characteristics per Quartile (Q1–4) of TyG Index (n = 28,282) |
Incidence of COPD
Mean follow-up time was 31.4 (SD ± 10.3) years from baseline. There were 3369 incident COPD events (n = 1019 in women and n = 2350 in men). Kaplan–Meier plots are shown in Figures 1–3. HR of incident COPD events by quartiles of the TyG index are shown in Table 2. After full adjustments (Model 3), there was still a 21% increase in risk for incident COPD events in Q4 vs Q1 (reference) (p-trend: <0.001). Sex-specific results are also presented in Table 2. The risk remained strongly significant in women but non-significant in men after full adjustments (HR in women Q4 vs Q1 1.72 (1.41–2.09), p-trend <0.001, HR in men Q4 vs Q1 1.01 (0.89–1.14), p-trend: >0.5). Similar associations were seen when assessing incident COPD events per 1-unit increase in the TyG index (Table 2). In a subset of never-smokers at baseline (n = 9898), there remained a 47% increase in risk for incident COPD events in Q4 of TyG index vs Q1 (reference) (Table 3 and Supplement Table S2) even after full adjustments. We additionally carried out a sensitivity analysis of incident COPD with sex-specific quartiles of TyG index after excluding subjects with prevalent diabetes at baseline (Supplement Table S3). Results remained largely unchanged from the results presented in Table 2 where the analysis was adjusted for prevalent diabetes.
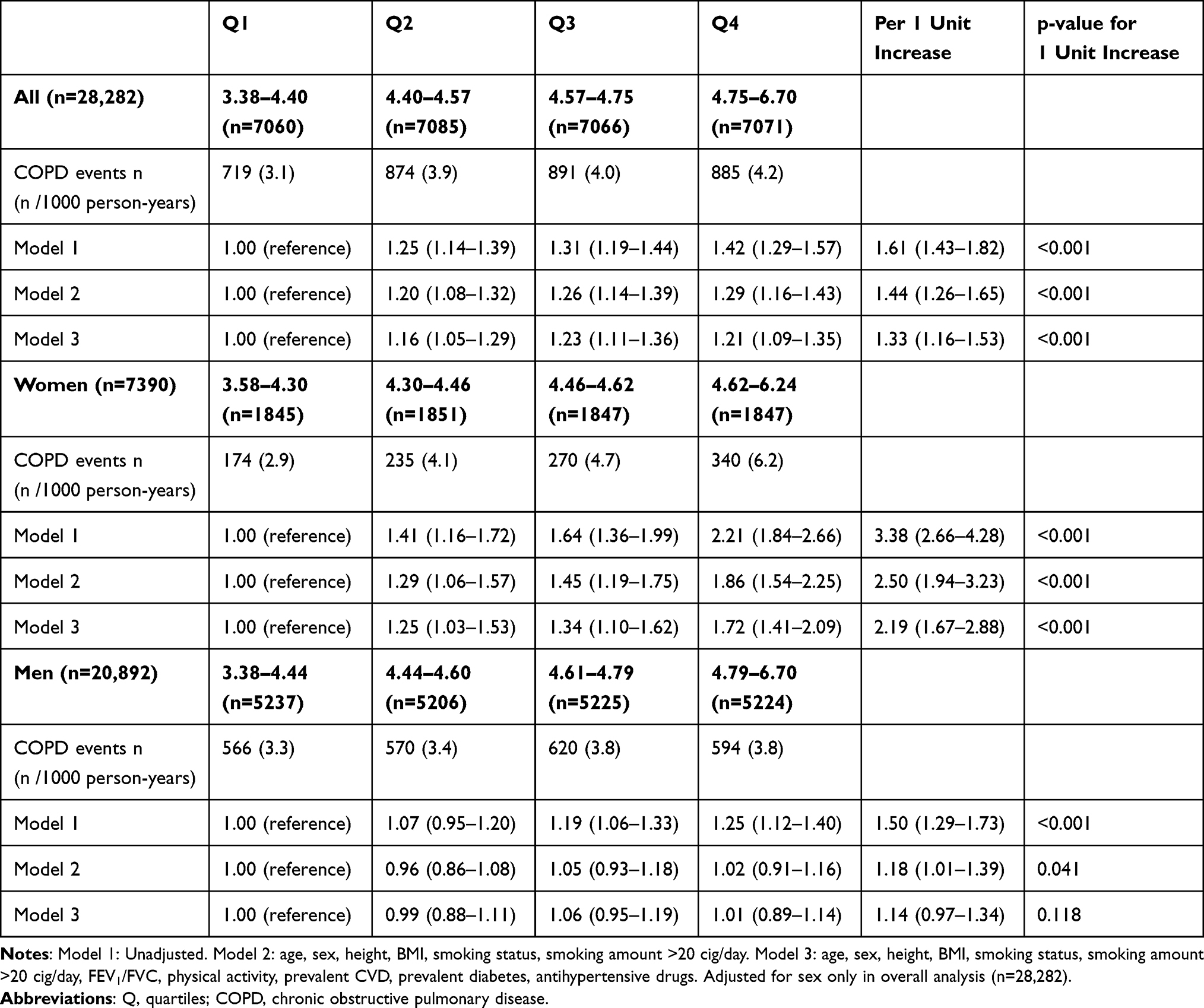 |
Table 2 Incidence of COPD Events by Quartiles of and by 1 Unit Increase in TyG Index |
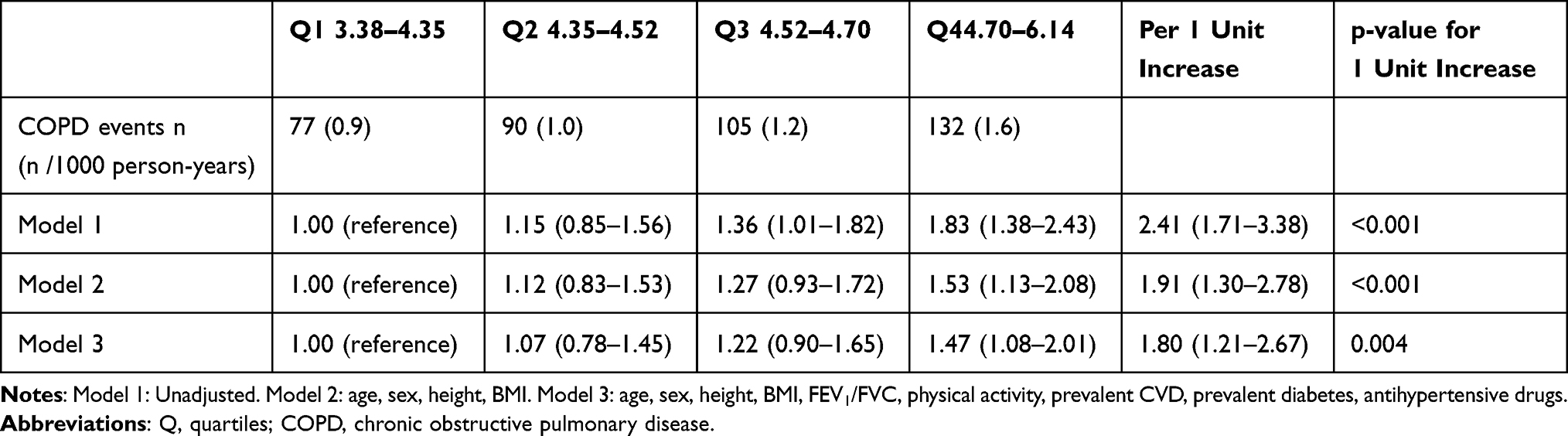 |
Table 3 Incidence of COPD Events by Quartiles of and by 1 Unit Increase in the TyG Index in Never Smokers (n = 9898) |
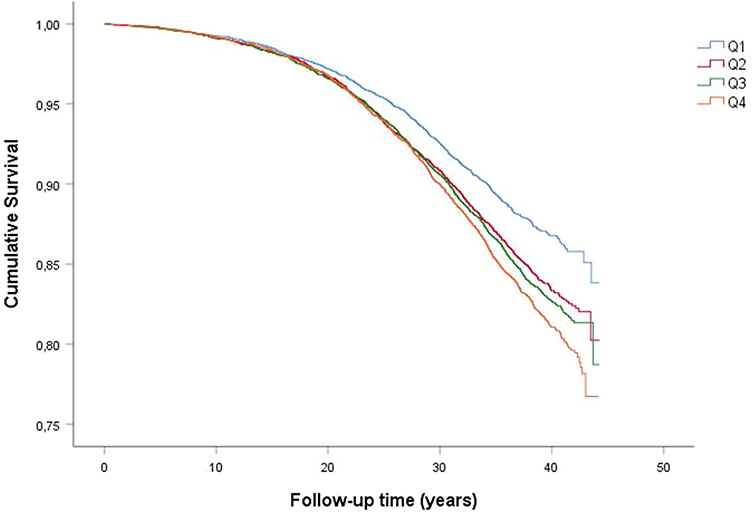 |
Figure 1 Kaplan–Meier survival curves of incident COPD by quartiles of TyG index. Q1: lowest TyG index, Q4: Highest TyG index. |
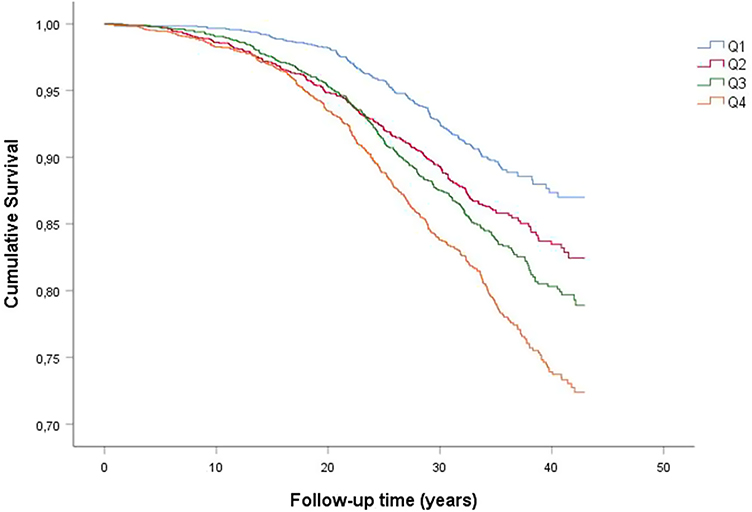 |
Figure 2 Kaplan–Meier event-free survival curves of incident COPD by quartiles of TyG index in women Q1: lowest TyG index, Q4: Highest TyG index. |
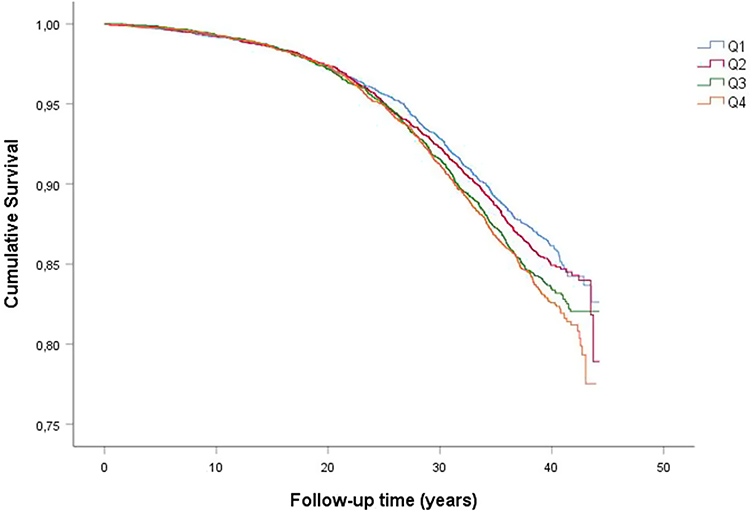 |
Figure 3 Kaplan–Meier event-free survival curves of incident COPD by quartiles of TyG index in men Q1: lowest TyG index, Q4: Highest TyG index. |
Discussion
The main finding of this study is that the TyG index is a strong predictor of future COPD events in women. This is a novel finding illustrating sex-differences in the association between estimated insulin resistance using TyG index and COPD risk.
Our findings are in accordance with the results of previously published studies using HOMA-IR to assess insulin resistance.10,11,15,26,27 Zuberi et al assessed HOMA-IR index in relation to COPD and found a high prevalence of insulin resistance in non-hypoxaemic COPD.26 The relationship between insulin resistance using HOMA-IR index and lung function has been found in relation to lung volumes and it has therefore been suggested that this relationship may reflect childhood exposures that affect both lung growth and programming effects on insulin sensitivity.15 The effects of insulin and insulin resistance on the lung and airways have been found to begin early in life. Insulin receptors are important during development of the foetal lung and therefore maternal glycaemic levels are thought to influence foetal lung maturation.28 Long-term raised insulin levels, reflecting underlying insulin resistance, have been found to be associated with reduced lung function in adults even in those without known diabetes.27 An additional explanation could be the role of advanced glycation end-products (AGEs) and its receptor (receptor for advanced glycation end-products (RAGE)) on the lung. AGEs are formed in response to hyperglycaemia and are implicated in the pathophysiology of COPD. Binding of AGEs to their receptor RAGE – which is highly expressed in the lung, causes an increase in inflammatory response and has been therefore implicated in the development of COPD.29
We are aware of only one previous study that has assessed the TyG index as a marker of respiratory health.16 The study found the TyG index to have a cross-sectional association with respiratory symptoms, restrictive spirometry pattern, and the presence of self-reported chronic bronchitis. In our prospective analysis, we found an association between TyG index and incident COPD events which included inpatient and outpatient COPD events as well as deaths due to COPD. The trajectory of restrictive spirometry (or preserved ratio impaired spirometry) has included a transition to COPD later in life30 which may explain the long-term relationship to COPD risk found in our cohort. An important difference in our study is that the population at baseline was considerably healthier. The previous cross-sectional study found a high proportion of overweight/obese participants at baseline, high proportion of hypertension and more than half with MetS at baseline. In our cohort, we found a low baseline prevalence of diabetes, low use of anti-hypertensive medication and less than half of the population had a BMI over 25 kg/m2. This adds strength to our study as we see a potential role for a measure of insulin sensitivity to be a biomarker for future COPD events earlier in life when subjects are relatively healthy.
We did, however, see this risk in women only, which may suggest some sex-differences in the life-time risks of COPD in relation to early insulin resistance. The prevalence and mortality of COPD in women has increased31 and as women are generally thought as being less “heavy” smokers than men (as evidenced also in the present study), it is thought that women may therefore be more susceptible to the effects of smoking and development of COPD.32 There are also differences in the histological pattern of COPD between men and women. Women tend to have more pronounced small airway disease and less emphysema, whereas men tend to exhibit more emphysema.32 We also found the association in women to be present after adjusting for smoking. Interestingly, COPD that is associated with household air pollution is also associated with small airways disease compared to emphysema33 and it is additionally more likely to occur in women in a global perspective.32 It may be possible that the effects of insulin resistance on the pathophysiology of lung disease differ in men and women, leading to more small airway disease in women. The risk of coronary heart disease associated with T2DM or insulin resistance as measured by the TyG index has been found to be more significant in women.34,35 Oestrogen elicits a protective effect on insulin resistance by promoting insulin sensitivity and an increase in insulin resistance and the MetS is seen in post-menopausal women, increasing the CVD risk.36 However, the association with COPD in these women seems to be less clear,37 therefore it is unlikely that this explains the sex-differences in our findings.
Although a recent cross-sectional study found an association between the TyG index and respiratory symptoms after adjusting for the HOMA-IR, the association between TyG index and chronic bronchitis became non-significant after adjusting for HOMA-IR.16 After further adjusting the association between TyG index and respiratory symptoms for MetS, only cough remained significant. The study concludes that the TyG index is an adequate measure of metabolic dysfunction with importance for pulmonary outcomes.16 Further studies are needed to assess the long-term risk of pulmonary outcomes associated with TyG index, and we feel that we have addressed a notable knowledge gap being the first prospective study to assess the role of the TyG index as a risk biomarker for impaired lung health.
Limitations
Prospective studies of this nature are prone to certain biases that can occur over the long course of follow-up. Certain risk factors/markers measured at baseline could have changed over the long follow-up period such as a subject’s smoking status, medication use, BMI and co-morbidities. A change in smoking status during follow-up would affect the outcome of COPD. However, it is unlikely that study participants would have taken up smoking during the duration of the study as the prevalence of smoking in Sweden declined over the follow-up period.38 It is likely that many of the subjects with raised TyG index at baseline developed T2DM during follow-up acting therefore as a mediator. We adjusted the analysis for prevalent diabetes and also carried out a sensitivity analysis after excluding those with prevalent diabetes. Although our COPD endpoints include inpatient, outpatient and deaths due to COPD, the incident outpatient diagnoses make up a small proportion of the total incident cases. Therefore, the majority of the cases reflect COPD hospitalisations or deaths due to COPD, which represent the more severe end of the disease spectrum. Our findings may therefore be more relevant for more severe COPD than for milder cases that are managed in primary health care. However, our findings remain significant after both adjusting for smoking status and in a cohort of life-long never smokers. These findings provide considerable support to our hypothesis that there is potentially a role of the insulin resistance, as estimated by the TyG index, in the pathogenesis of future COPD, which goes beyond the role of smoking.
Conclusion
A raised TyG index is a novel risk marker of future incident COPD events in women. Insulin resistance as estimated by the TyG index can precede the development of obstructive lung disease and as such may be an easily measurable and useful biomarker predictor of COPD in women.
Disclosure
SZ, HT, PMN and IFM have no conflicts of interests in relation to this work to declare. The baseline screening of participants in the Malmö Preventive Project (MPP) study was supported by the City of Malmö, the Swedish Medical Research Council, and the Swedish Heart and Lung Foundation. All data accessed complied with the relevant data protection and privacy regulations.
References
1. Cebron Lipovec N, Beijers RJH, van den Borst B, Doehner W, Lainscak M, Schols AM. The prevalence of metabolic syndrome in chronic obstructive pulmonary disease: a systematic review. COPD. 2016;13(3):399–406. doi:10.3109/15412555.2016.1140732
2. Jones PW, Nadeau G, Small M, Adamek L. Characteristics of a COPD population categorised using the GOLD framework by health status and exacerbations. Respir Med. 2014;108(1):129–135. doi:10.1016/j.rmed.2013.08.015
3. Park SK, Larson JL. The relationship between physical activity and metabolic syndrome in people with chronic obstructive pulmonary disease. J Cardiovasc Nurs. 2014;29(6):499–507. doi:10.1097/JCN.0000000000000096
4. Duncan BB, Schmidt MI, Pankow JS, et al. Low-grade systemic inflammation and the development of type 2 diabetes: the atherosclerosis risk in communities study. Diabetes. 2003;52(7):1799–1805. doi:10.2337/diabetes.52.7.1799
5. Muhammad IF, Borné Y, Hedblad B, Nilsson PM, Persson M, Engström G. Acute-phase proteins and incidence of diabetes: a population-based cohort study. Acta Diabetol. 2016;53(6):981–989. doi:10.1007/s00592-016-0903-8
6. Miller J, Edwards LD, Agustí A, et al. Comorbidity, systemic inflammation and outcomes in the ECLIPSE cohort. Respir Med. 2013;107(9):1376–1384. doi:10.1016/j.rmed.2013.05.001
7. Parappil A, Depczynski B, Collett P, Marks GB. Effect of comorbid diabetes on length of stay and risk of death in patients admitted with acute exacerbations of COPD. Respirology. 2010;15(6):918–922. doi:10.1111/j.1440-1843.2010.01781.x
8. Glaser S, Kruger S, Merkel M, Bramlage P, Herth FJ. Chronic obstructive pulmonary disease and diabetes mellitus: a systematic review of the literature. Respir Int Rev Thoracic Dis. 2015;89(3):253–264. doi:10.1159/000369863
9. Ehrlich SF, Quesenberry CP, Van Den Eeden SK, Shan J, Ferrara A. Patients diagnosed with diabetes are at increased risk for asthma, chronic obstructive pulmonary disease, pulmonary fibrosis, and pneumonia but not lung cancer. Diabetes Care. 2010;33(1):55–60. doi:10.2337/dc09-0880
10. Lim SY, Rhee E-J, Sung K-C. Metabolic syndrome, insulin resistance and systemic inflammation as risk factors for reduced lung function in Korean nonsmoking males. J Korean Med Sci. 2010;25(10):1480–1486. doi:10.3346/jkms.2010.25.10.1480
11. Sagun G, Gedik C, Ekiz E, Karagoz E, Takir M, Oguz A. The relation between insulin resistance and lung function: a cross sectional study. BMC Pulm Med. 2015;15(1):139. doi:10.1186/s12890-015-0125-9
12. Simental-Mendía LE, Rodríguez-Morán M, Guerrero-Romero F. The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metab Syndr Relat Disord. 2008;6(4):299–304. doi:10.1089/met.2008.0034
13. Guerrero-Romero F, Simental-Mendía LE, González-Ortiz M, et al. The product of triglycerides and glucose, a simple measure of insulin sensitivityComparison with the euglycemic-hyperinsulinemic clamp. J Clin Endocrinol Metab. 2010;95(7):3347–3351. doi:10.1210/jc.2010-0288
14. Vasques ACJ, Novaes FS, de Oliveira M, et al. TyG index performs better than HOMA in a Brazilian population: a hyperglycemic clamp validated study. Diabetes Res Clin Pract. 2011;93(3):e98–e100. doi:10.1016/j.diabres.2011.05.030
15. Lawlor DA, Ebrahim S, Davey Smith G. Associations of measures of lung function with insulin resistance and Type 2 diabetes: findings from the British Women’s Heart and Health Study. Diabetologia. 2004;47(2):195–203. doi:10.1007/s00125-003-1310-6
16. Wu TD, Fawzy A, Brigham E, et al. Association of triglyceride-glucose index and lung health: a population-based study. Chest. 2021;160(3):1026–1034. doi:10.1016/j.chest.2021.03.056
17. Berglund G, Nilsson P, Eriksson KF, et al. Long-term outcome of the Malmö preventive project: mortality and cardiovascular morbidity. J Intern Med. 2000;247(1):19–29. doi:10.1046/j.1365-2796.2000.00568.x
18. Nilsson P, Nilsson JA, Hedblad B, Eriksson KF, Berglund G. Hyperinsulinaemia as long-term predictor of death and ischaemic heart disease in nondiabetic men: the Malmö Preventive Project. J Intern Med. 2003;253(2):136–145. doi:10.1046/j.1365-2796.2003.01064.x
19. Zaigham S, Nilsson PM, Wollmer P, Engstrom G. The temporal relationship between poor lung function and the risk of diabetes. BMC Pulm Med. 2016;16(1):75. doi:10.1186/s12890-016-0227-z
20. Engstrom G, Hedblad B, Nilsson P, Wollmer P, Berglund G, Janzon L. Lung function, insulin resistance and incidence of cardiovascular disease: a longitudinal cohort study. J Intern Med. 2003;253(5):574–581. doi:10.1046/j.1365-2796.2003.01138.x
21. Guerrero-Romero F, Villalobos-Molina R, Jiménez-Flores JR, et al. Fasting triglycerides and glucose index as a diagnostic test for insulin resistance in young adults. Arch Med Res. 2016;47(5):382–387. doi:10.1016/j.arcmed.2016.08.012
22. Simental-Mendía LE, Gamboa-Gómez CI, Aradillas-García C, Rodríguez-Morán M, Guerrero-Romero F. The triglyceride and glucose index is a useful biomarker to recognize glucose disorders in apparently healthy children and adolescents. Eur J Pediatr. 2020;179(6):953–958. doi:10.1007/s00431-020-03570-2
23. Simental-Mendía LE, Guerrero-Romero F. The correct formula for the triglycerides and glucose index. Eur J Pediatr. 2020;179(7):1171. doi:10.1007/s00431-020-03644-1
24. Engström G, Segelstorm N, Ekberg-Aronsson M, Nilsson PM, Lindgärde F, Löfdahl C-G. Plasma markers of inflammation and incidence of hospitalisations for COPD: results from a population-based cohort study. Thorax. 2009;64(3):211–215. doi:10.1136/thx.2008.102079
25. Inghammar M, Engstrom G, Lofdahl CG, Egesten A. Validation of a COPD diagnosis from the Swedish inpatient registry. Scand J Public Health. 2012;40(8):773–776. doi:10.1177/1403494812463172
26. Zuberi FF, Bader N, Rasheed T, Zuberi BF. Association between insulin resistance and BMI with FEV1 in non-hypoxemic COPD out-patients. Clin Respir J. 2021;15(5):513–521. doi:10.1111/crj.13336
27. Baffi CW, Wood L, Winnica D, et al. Metabolic Syndrome and the Lung. Chest. 2016;149(6):1525–1534. doi:10.1016/j.chest.2015.12.034
28. Singh S, Prakash YS, Linneberg A, Agrawal A. Insulin and the lung: connecting asthma and metabolic syndrome. J Allergy. 2013;2013:627384. doi:10.1155/2013/627384
29. Wu L, Ma L, Nicholson LFB, Black PN. Advanced glycation end products and its receptor (RAGE) are increased in patients with COPD. Respir Med. 2011;105(3):329–336. doi:10.1016/j.rmed.2010.11.001
30. Wijnant SRA, De Roos E, Kavousi M, et al. Trajectory and mortality of preserved ratio impaired spirometry: the Rotterdam Study. Eur Respir J. 2020;55(1):1901217. doi:10.1183/13993003.01217-2019
31. McIvor ER, Saraiva I, Denning J, McIvor RA. Women with COPD. Breathe. 2020;16(4):200239. doi:10.1183/20734735.0239-2020
32. Barnes PJ. Sex differences in chronic obstructive pulmonary disease mechanisms. Am J Respir Crit Care Med. 2016;193(8):813–814. doi:10.1164/rccm.201512-2379ED
33. Assad NA, Balmes J, Mehta S, Cheema U, Sood A. Chronic obstructive pulmonary disease secondary to household air pollution. Semin Respir Crit Care Med. 2015;36(3):408–421. doi:10.1055/s-0035-1554846
34. Juutilainen A, Kortelainen S, Lehto S, Rönnemaa T, Pyörälä K, Laakso M. Gender difference in the impact of type 2 diabetes on coronary heart disease risk. Diabetes Care. 2004;27(12):2898–2904. doi:10.2337/diacare.27.12.2898
35. Tian X, Zuo Y, Chen S, et al. Triglyceride–glucose index is associated with the risk of myocardial infarction: an 11-year prospective study in the Kailuan cohort. Cardiovasc Diabetol. 2021;20(1):19. doi:10.1186/s12933-020-01210-5
36. Carr MC. The emergence of the metabolic syndrome with menopause. J Clin Endocrinol Metab. 2003;88(6):2404–2411. doi:10.1210/jc.2003-030242
37. Campbell B, Davis SR, Abramson MJ, et al. Menopause, lung function and obstructive lung disease outcomes: a systematic review. Climacteric. 2018;21(1):3–12. doi:10.1080/13697137.2017.1392504
38. Midlov P, Calling S, Sundquist J, Sundquist K, Johansson SE. The longitudinal age and birth cohort trends of smoking in Sweden: a 24-year follow-up study. Int J Public Health. 2014;59(2):243–250. doi:10.1007/s00038-013-0535-5
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.