Back to Journals » Journal of Pain Research » Volume 19
Trigger Point Electrical Dry Needling with Different Waveforms Plus Intra-Articular Corticosteroid for Knee Osteoarthritis: A Prospective Randomized Controlled Trial
Authors Lin Y, Jia W, Liu C, Tang Y, Yuan Y
Received 2 February 2026
Accepted for publication 11 April 2026
Published 23 April 2026 Volume 2026:19 595268
DOI https://doi.org/10.2147/JPR.S595268
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Alaa Abd-Elsayed
Yulian Lin,1,2,* Wensen Jia,1,2,* Chang Liu,1,2,* Yujia Tang,1,2 Yan Yuan2,3
1Department of Anesthesiology, The Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 2School of Anesthesiology, Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 3Department of Pain Treatment, the Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan Yuan, Department of Pain Treatment, the Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China, Tel + 86 18052268635, Email [email protected]
Background: Knee osteoarthritis is a common musculoskeletal disorder associated with pain, functional limitation, and substantial healthcare burden.
Purpose: To compare the efficacy of trigger point electrical dry needling (electrical-DN) with different waveforms, combined with intra-articular corticosteroid injection (CSI), in patients with knee osteoarthritis (KOA).
Methods: A total of 138 participants were randomized to the sham stimulation group (Group S), dense-disperse wave group (Group D), or continuous wave group (Group C). All groups received a single CSI. Group S had no electrical stimulation, while Group D and Group C were treated with dense-disperse wave and continuous wave, respectively. Electrical stimulation was administered for 20 minutes per session, once weekly for two weeks. Assessments were obtained at the following time points: baseline, post-treatment weeks 1, 4, 8, and 12. Clinical outcomes were assessed using the numerical rating scale (NRS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Short-Form McGill Pain Questionnaire (SF-MPQ), Pittsburgh Sleep Quality Index (PSQI), Hamilton Anxiety Rating Scale (HAMA), Knee Flexion Range of Motion (FROM), rescue medication use, and adverse events. Repeated measures were analyzed using generalized estimating equations (GEE), and other comparisons were performed using appropriate parametric or nonparametric tests.
Results: Group D showed lower NRS scores than Group C at weeks 8 and 12 and a lower WOMAC score at week 12 (all P < 0.05). Compared with Group S, both electrical-DN groups showed lower NRS and WOMAC scores at all follow-up time points. At week 1, both electrical-DN groups also showed lower SF-MPQ scores and greater improvement in FROM than Group S (all P < 0.05). In GEE analysis, with Group S and week 12 as the reference categories, both Group D (β = − 1.152, 95% CI: − 1.560 to − 0.744) and Group C (β = − 0.652, 95% CI: − 1.033 to − 0.271) showed lower NRS scores at week 12.
Conclusion: Trigger point electrical dry needling may provide additional benefit in pain relief for patients with KOA when used after CSI. Among the two electrical-DN groups, the dense-disperse waveform was associated with a modest advantage in pain relief at later follow-up time points.
Keywords: osteoarthritis, knee, dry needling, trigger points
A Letter to the Editor has been published for this article.
A Response to Letter by Ms Yu has been published for this article.
Introduction
Knee osteoarthritis (KOA) is one of the most common musculoskeletal disorders and a major cause of pain and functional disability worldwide.1 Persistent pain and physical limitation related to KOA substantially impair quality of life and may also contribute to psychological distress.2,3 Globally, KOA represents an important and growing public health problem, with both prevalence and disability burden showing an increasing trend.4 As the disease progresses, KOA may lead to marked functional impairment and increase the likelihood of joint replacement, thereby further exacerbating the socioeconomic burden on healthcare systems. Previous studies have shown that joint replacements performed for symptomatic hip and knee osteoarthritis are associated with substantial socioeconomic costs.5,6
Emerging evidence suggests that pain in knee osteoarthritis is not solely driven by intra-articular pathology, but may also involve a relevant myofascial component. Studies have reported a relatively high prevalence of latent and active myofascial trigger points (MTrPs) in muscles acting on or functionally related to the knee, including the quadriceps, hip adductors, gastrocnemius, hamstrings, and tensor fasciae latae, in patients with painful KOA.7,8 In addition, active trigger points in lower-extremity muscles may reproduce patients’ familiar knee pain and are associated with greater pain intensity and disability. These findings indicate that MTrPs in knee- and hip-related muscles may contribute to pain amplification, movement restriction, and abnormal biomechanics in KOA.9,10 Therefore, targeting trigger points not only in local knee-stabilizing muscles but also in proximal myofascial chains may have therapeutic relevance.
Previous studies have suggested that electrical dry needling may improve pain and function in patients with knee osteoarthritis, but evidence regarding the optimization of stimulation parameters remains limited.11,12 In particular, few studies have directly compared different electrical waveforms in this population. Dense-disperse and continuous waveforms may differ in their effects on pain modulation because alternating stimulation patterns may reduce neural habituation and engage broader analgesic pathways than fixed-frequency stimulation.13 In addition, intra-articular corticosteroid injection (CSI) primarily targets intra-articular inflammatory and nociceptive components, whereas electrical dry needling may additionally address myofascial trigger points and neuromuscular pain modulation. Therefore, combining these interventions may provide additive benefit.14 Given that a 2-point reduction on the NRS is often considered clinically meaningful, further clarification of the magnitude and durability of these effects is clinically relevant.15
Therefore, this study aimed to compare the efficacy of trigger point electrical dry needling with different waveforms in participants with KOA.
Methods
Study Design
This was an assessor-blinded, randomized controlled trial conducted at the Pain Management Clinic of the Affiliated Hospital of Xuzhou Medical University between 2025 and 2026. This study was conducted in accordance with the Declaration of Helsinki, approved by the Research Ethics Committee of Xuzhou Medical University (Approval No.: XYFY2024-KL553-01) and registered with the Chinese Clinical Trial Registry (Registration No.: ChiCTR2500102033). The trial protocol reviewed and approved by the ethics committee included the planned use of intra-articular corticosteroid injection and the permitted rescue medication during the study period. All participants provided written informed consent. The study includes a follow-up period of three months.
Patient Selection
Inclusion Criteria: People aged ≥18 years who met the American College of Rheumatology clinical criteria for KOA; with unilateral anterior/medial knee pain; NRS score >3; at least one MTrP in the affected lower limb muscles. Exclusion Criteria: Contraindications to corticosteroid injection or dry needling; a history of adverse reactions to needling or metal allergy; severe cardiovascular, cerebrovascular, hepatic, renal, hematopoietic disorders, or malignancy; other knee-affecting conditions (eg., gouty arthritis, rheumatoid arthritis); poor compliance or inability to complete the study; MRI-confirmed bursitis; clinically significant knee stiffness or suspected intra-articular adhesions/arthrofibrosis that could interfere with intra-articular injection or outcome assessment; failure of previous non-surgical treatment, recurrent/severe knee symptoms, significant functional limitation, or Kellgren–Lawrence grade IV; acupuncture, intra-articular injection, or lower limb surgery within the past 6 months. Withdrawal criteria: voluntary withdrawal from the study; receipt of other invasive therapies during the study period; poor treatment adherence resulting in failure to complete the scheduled treatment as required.
Randomization and Blinding
Participants were randomized at a 1:1:1 ratio to the sham stimulation group (Group S), dense-disperse wave group (Group D), or continuous wave group (Group C). An assistant not involved in the trial or statistical analysis generated the allocation sequence using a computer-generated random number table, and the group assignments were concealed in opaque, sealed envelopes. Outcome assessors and data analysts remained blinded to group allocation throughout all follow-up assessments.
Treatment
Functional Exercise and CSI
All participants received standardized exercise guidance, and the exercise program was determined by an experienced physician with reference to previous literature and adjusted according to individual characteristics.16 During the first week, participants received oral imrecoxib (100 mg once daily). Paracetamol-tramadol (37.5 mg) was permitted if pain persisted (NRS ≥7), and any use was recorded. During the same week, a single ultrasound-guided CSI was administered by an experienced physician. The participant was positioned supine with the affected knee flexed, and the physician performed the procedure under strict aseptic conditions. Under ultrasound guidance, the needle was inserted from the lateral approach. After aspiration of as much joint effusion as possible, the prepared injectate was administered. The injectate consisted of compound betamethasone (1 mL), lidocaine (1.5 mL), and normal saline (2.5 mL). After the injection, participants completed 10 cycles of knee flexion-extension to promote drug distribution.
Dry Needling Intervention
After CSI, participants were monitored for 30 minutes, and electrical dry needling was initiated only if no adverse reactions were observed. MTrPs on the affected side were initially identified by manual palpation by the same experienced practitioner. Identification was based on standard clinical features, including a palpable taut band, a hyperirritable tender point within the band, and reproduction of the participant’s typical pain on compression.
Based on the distribution of identified MTrPs, the following muscles were treated as appropriate: vastus medialis, rectus femoris, adductor muscles, tensor fasciae latae, gastrocnemius, gluteus maximus, gluteus medius, quadratus lumborum, and rectus abdominis. Depending on the depth of the target muscle, sterile filiform needles (0.30 × 40 mm, 0.30×60 mm, or 0.30×75 mm) were used. Under ultrasound guidance, needles were rapidly inserted into the target region to elicit local twitch responses (LTRs). Correct targeting was further supported by sonographic observation of muscle fasciculation during needling. Needling was repeated until no additional LTRs could be provoked (Figure 1).
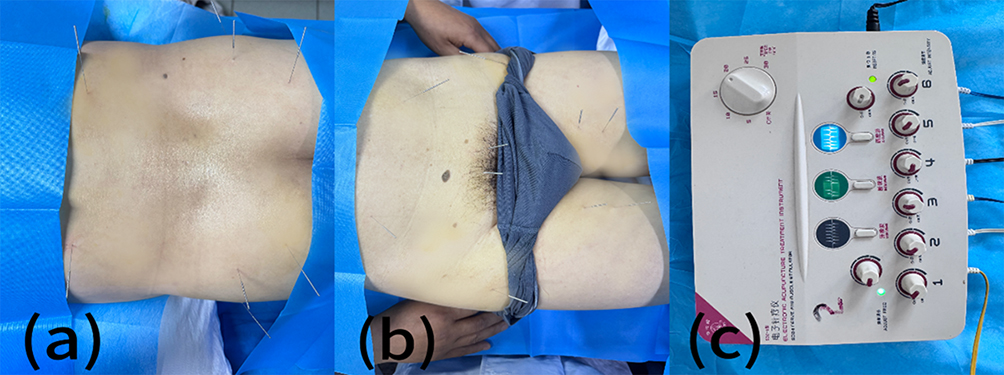 |
Figure 1 Photographs of the techniques used as interventions. Notes: (a) Illustrative figure of the lumbar and gluteal muscles; (b) Illustration figure of the abdominal and thigh muscles; (c) The image shows the electrical stimulator used in Groups C and D. |
Following needling, Group S received no electrical stimulation, Group D received dense-disperse stimulation (0.2-ms pulse width, 2/10 Hz), and Group C received continuous stimulation (0.2-ms pulse width, 2 Hz). Stimulation intensity was increased to the maximum level tolerable to the participant. Each treatment session lasted 20 minutes and all groups received treatment once per week for a total of two weeks.
The intervention protocol was standardized and based on previous clinical studies, and all procedures were performed by an experienced clinician under ultrasound guidance.
Assessment Scales and Outcome Measures
The primary outcome was pain intensity at week 12 post-treatment, assessed using the Numerical Rating Scale (NRS; 0–10, with higher scores indicating greater pain intensity). Secondary outcomes included the NRS at weeks 1, 4, and 8; Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC; higher scores indicating worse pain, stiffness, and functional limitation) and the Short-Form McGill Pain Questionnaire (SF-MPQ; higher scores indicating greater pain severity) at weeks 1, 4, 8, and 12; Knee Flexion Range of Motion (FROM) at week 1 post-treatment; and Pittsburgh Sleep Quality Index (PSQI; higher scores indicating poorer sleep quality) and Hamilton Anxiety Rating Scale (HAMA; higher scores indicating greater anxiety severity) at week 12 post-treatment. In addition, rescue medication use and adverse events were recorded throughout the study.15,17
FROM Measurement
FROM was measured using a universal goniometer. The participant was placed in the prone position, with the goniometer axis positioned over the lateral femoral epicondyle, the stationary arm aligned with the midline of the femur, and the movable arm aligned with the midline of the fibula. The participant was instructed to actively flex the knee to the maximum degree while avoiding compensatory movements such as pelvic elevation, hip abduction, or rotation. The angle at maximum active knee flexion was recorded. A greater angle indicated better knee flexion mobility.18
Statistical Analysis
Sample size estimation was based on the primary outcome, namely the NRS score at week 12. According to previous studies, the minimal clinically important difference (MCID) for the NRS was set at 2.0 points.15 Assuming a standard deviation of 2.0, 80% power, a two-sided α of 0.05, and a 10% dropout rate, the required total sample size for the three-group comparison was estimated to be 138 participants.
Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp., Armonk, NY, USA). Continuous variables were tested for normality using the Shapiro–Wilk test. Normally distributed data were expressed as mean ± SD, whereas non-normally distributed data were expressed as [M (P25, P75)]. Categorical variables were expressed as frequency and percentage.
For comparisons among the three groups at each time point, one-way analysis of variance (ANOVA) was used for normally distributed continuous variables, and the Kruskal–Wallis test was used for non-normally distributed variables. Post hoc pairwise comparisons were performed using the Bonferroni method or Dunn–Bonferroni test, as appropriate. Categorical variables were compared using the chi-square test or Fisher’s exact test, as appropriate.
Repeated-measures outcomes were further analyzed using generalized estimating equations (GEE) with a normal distribution, identity link function, and exchangeable correlation structure to assess the effects of group, time, and group-by-time interaction. Bonferroni correction was applied for post hoc multiple comparisons.
Results
Patient Enrollment and Baseline Characteristics
The study flowchart is shown in Figure 2. A total of 170 participants were screened, of whom 138 met the eligibility criteria and were randomized into the three groups.
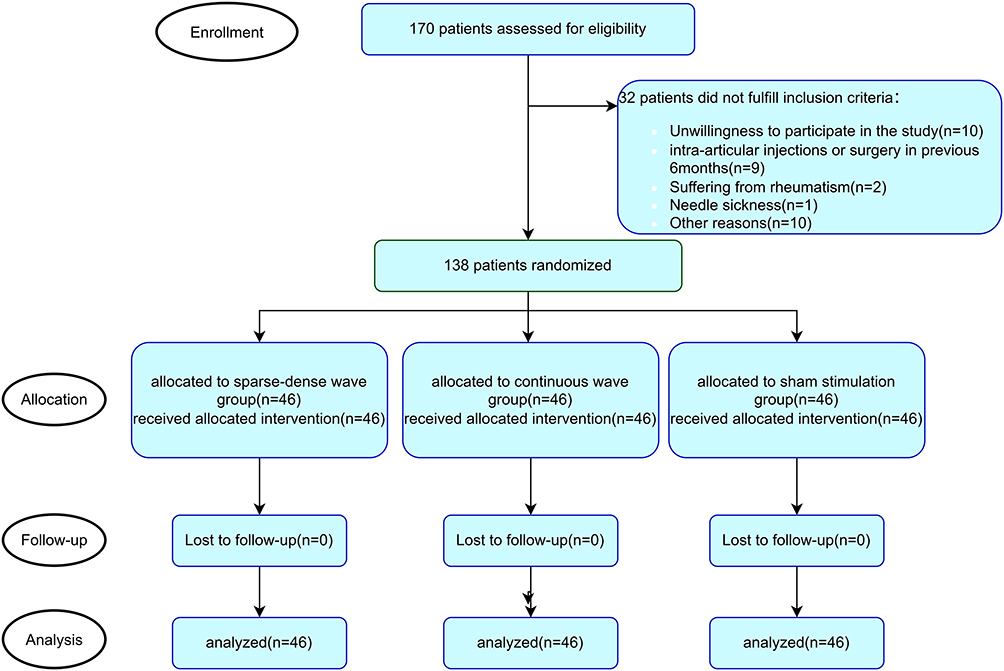 |
Figure 2 Flowchart of participant recruitment, randomization, allocation, follow-up, and analysis. |
All randomized participants completed the study and were included in the final analysis; therefore, no imputation for missing data was required. No significant differences in demographic characteristics or baseline data were observed among the three groups (all P > 0.05) (Table 1).
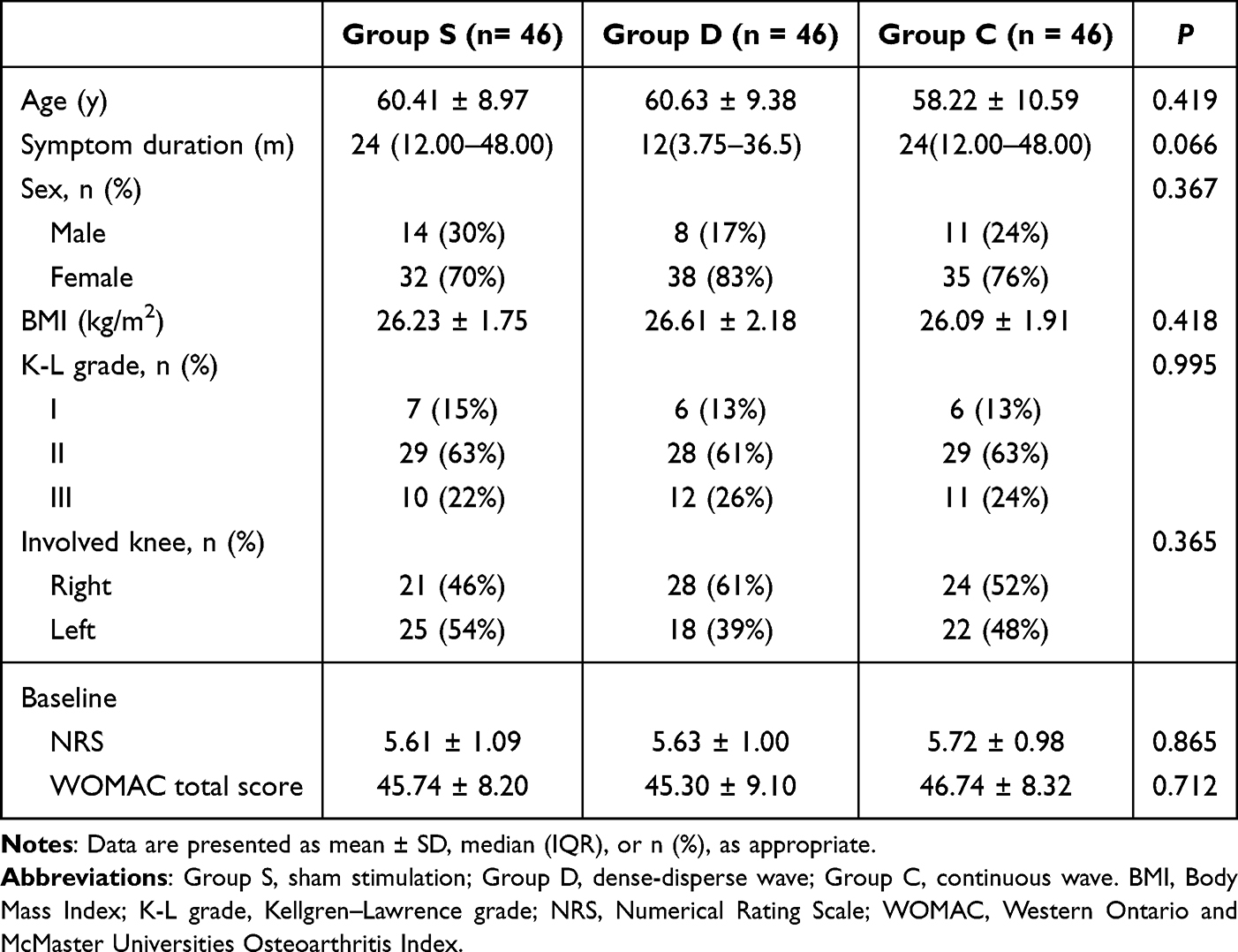 |
Table 1 Baseline Demographic and Clinical Characteristics of the Participants |
Within-Group Comparisons
All three groups showed significant improvements in NRS, WOMAC, SF-MPQ, and PSQI scores at week 12 compared with baseline (all P < 0.05) (Tables 2–4). In all three groups, NRS and WOMAC scores reached their lowest levels at week 1. Although the scores increased slightly thereafter, they remained significantly improved compared with baseline (Figure 3). FROM also improved significantly at week 1 in all three groups. No significant post-treatment changes in HAMA scores were observed in any group (Table 4).
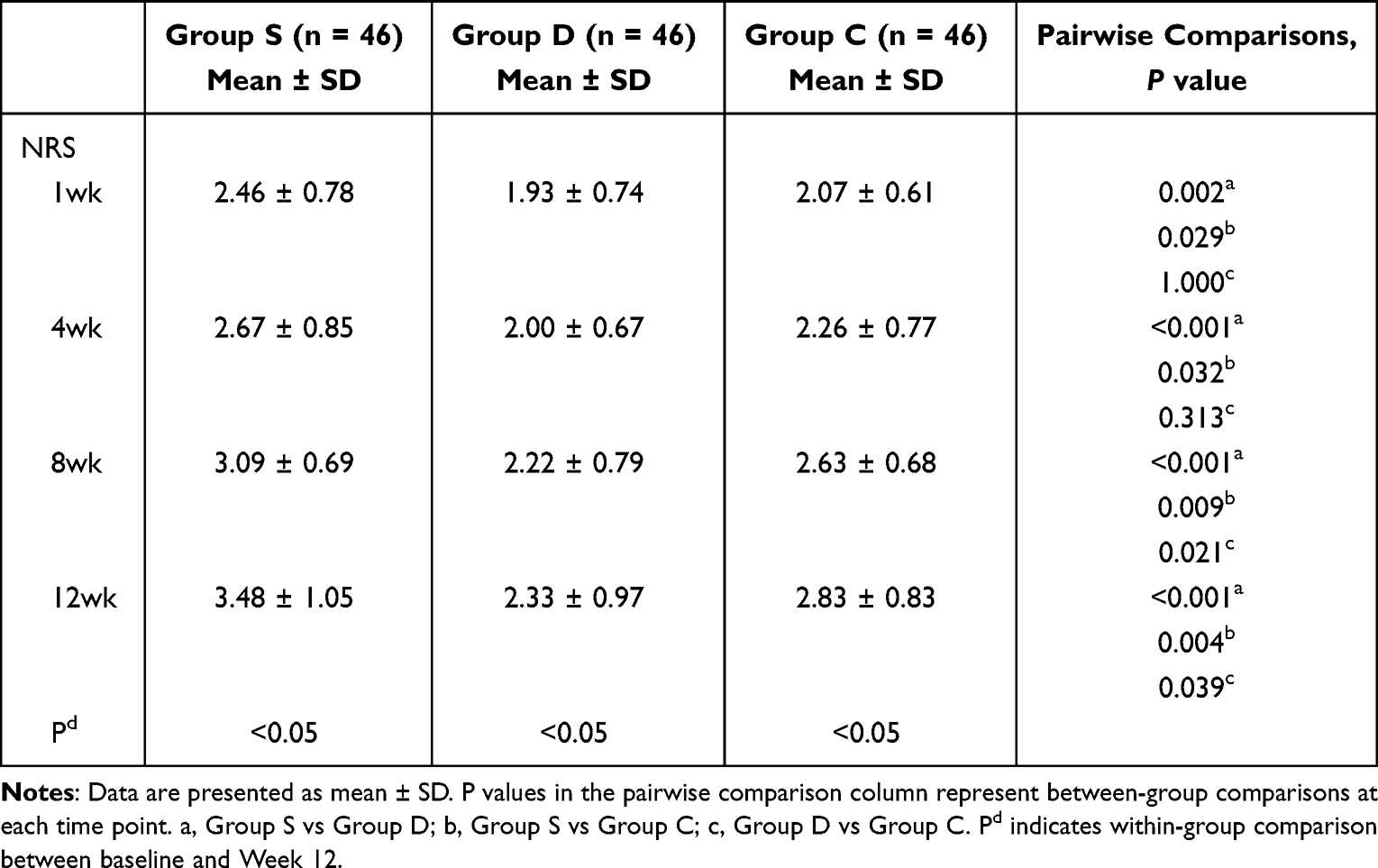 |
Table 2 Changes in NRS Scores Over Time Among the Three Groups |
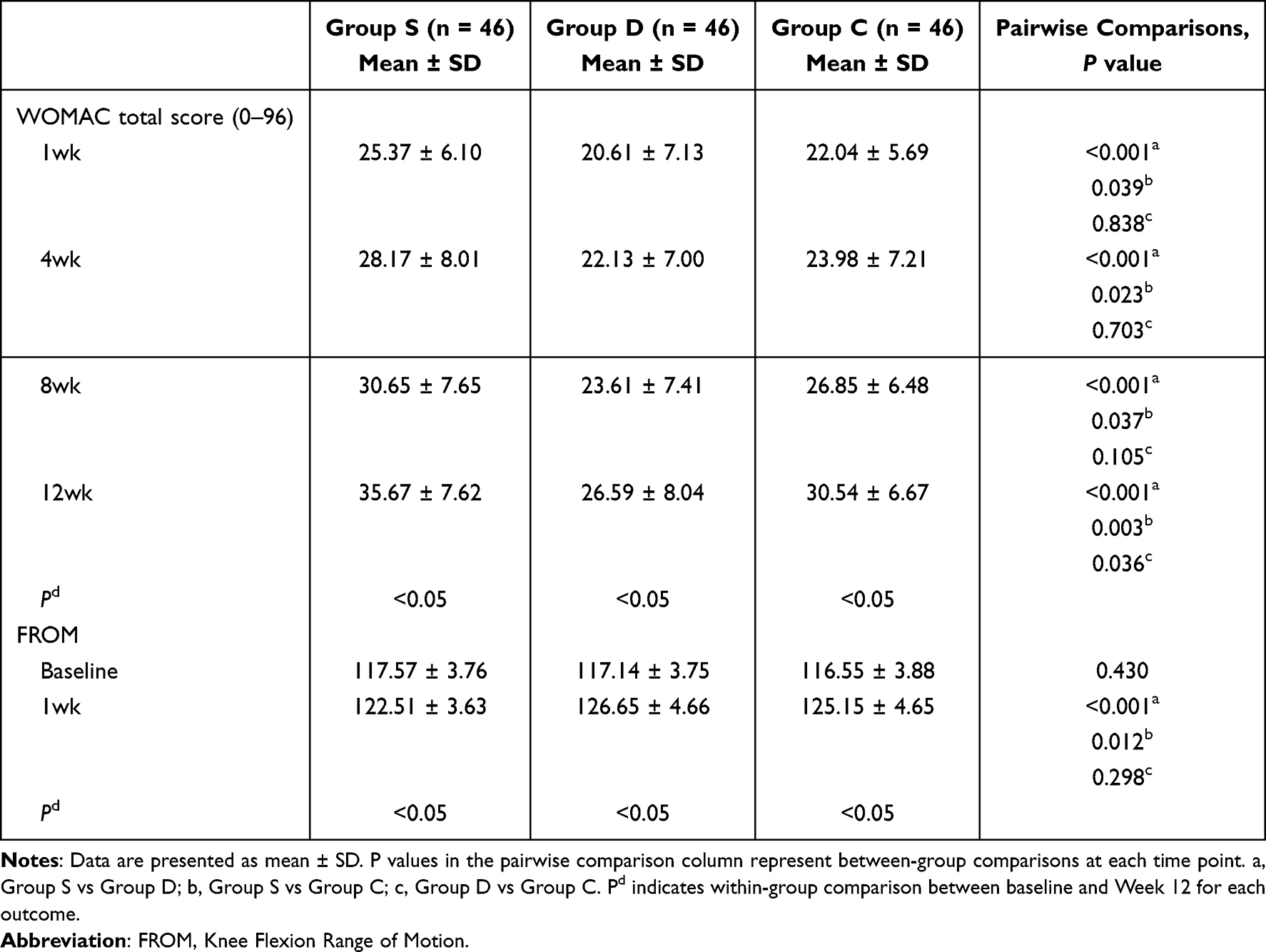 |
Table 3 Changes in WOMAC Total Score and FROM Over Time Among the Three Groups |
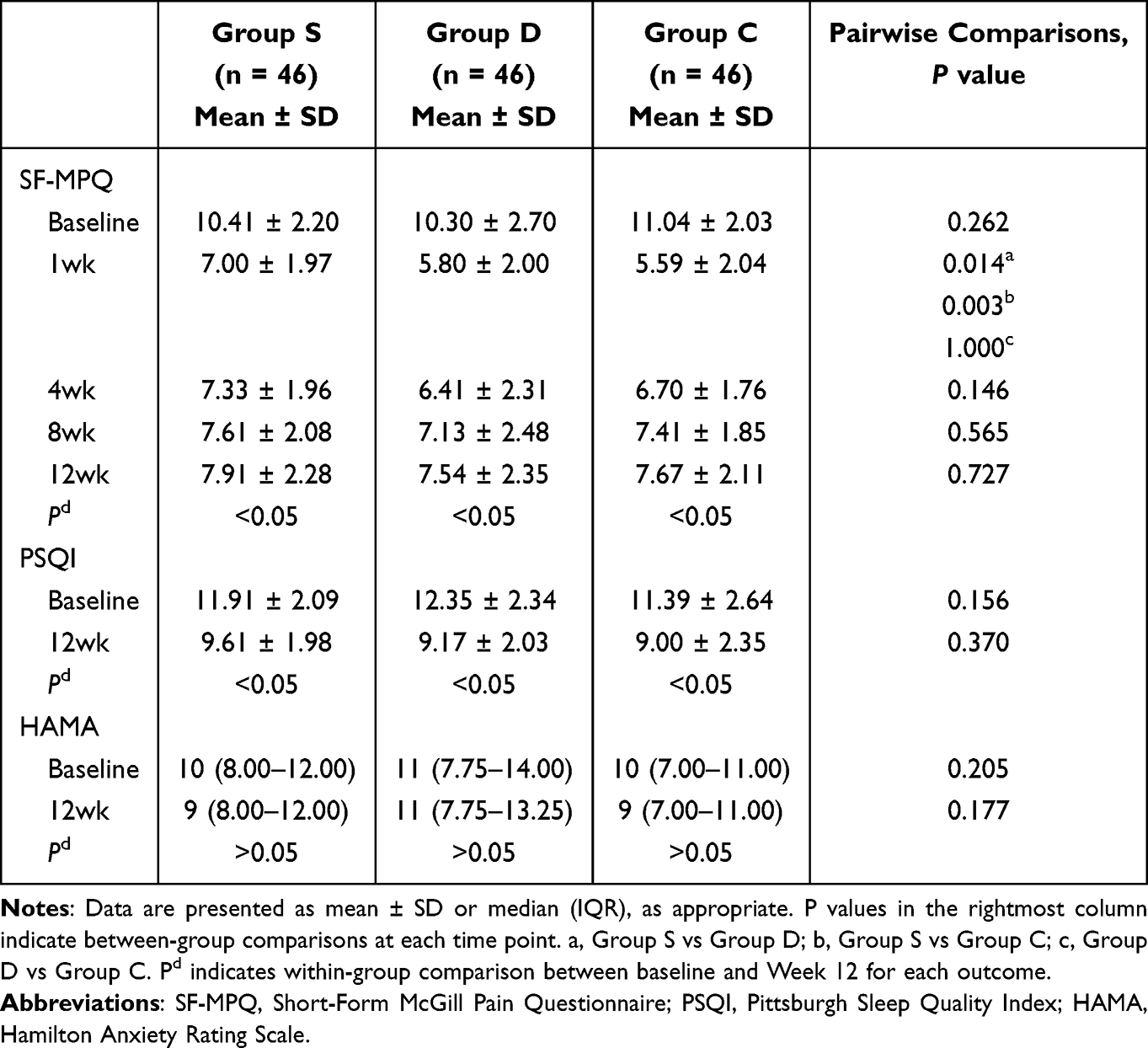 |
Table 4 Changes in SF-MPQ, PSQI, and HAMA Scores Over Time Among the Three Groups |
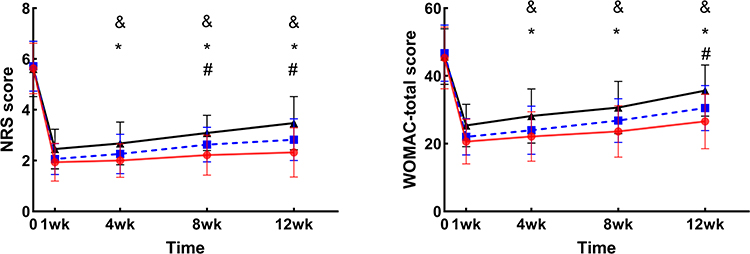 |
Figure 3 Changes in mean NRS and WOMAC scores over time in the three groups. Notes: Group D is shown in red, Group C in blue, and Group S in black. Error bars represent SD. & P < 0.05 for Group S vs Group D; * P < 0.05 for Group S vs Group C; # P < 0.05 for Group D vs Group C. |
Between-Group Comparisons
Compared with Group C, Group D showed lower NRS scores at weeks 8 and 12 (2.22 ± 0.79 vs. 2.63 ± 0.68, Pc = 0.021; 2.33 ± 0.97 vs. 2.83 ± 0.83, Pc = 0.039) and a lower WOMAC score at week 12 (26.59 ± 8.04 vs. 30.54 ± 6.67, Pc = 0.036). In addition, at all follow-up time points, Groups D and C showed lower NRS and WOMAC scores than Group S (all P < 0.05) (Tables 2 and 3). Improvements in FROM at week 1 were also more pronounced in Groups D and C than in Group S (Pa < 0.001, Pb = 0.012) (Table 3). At week 1 follow-up, the electrical-DN groups had significantly lower SF-MPQ scores than Group S (Pa = 0.014, Pb = 0.003). No significant intergroup differences in PSQI or HAMA were found at week 12 (Table 4).
Comparison of Adverse Event Distribution and Rescue Medication Use Among the Three Groups
Although paracetamol-tramadol was permitted as rescue analgesia for participants with persistent pain of NRS ≥ 7 according to the study protocol, no participant actually required rescue medication during follow-up.
Adverse events were further presented by group. Local soreness occurred in 11 participants in Group D, 7 in Group C, and 9 in Group S (27 cases in total, 19.6% of all participants). Mild bruising occurred in 0, 2, and 2 participants, respectively (4 cases in total), and needle syncope occurred in 0, 1, and 0 participants, respectively (1 case in total). All adverse events were mild and resolved spontaneously within 1–3 days. No significant between-group difference was found in the overall distribution of adverse events (χ2 = 0.081, P = 0.960) (Table 5).
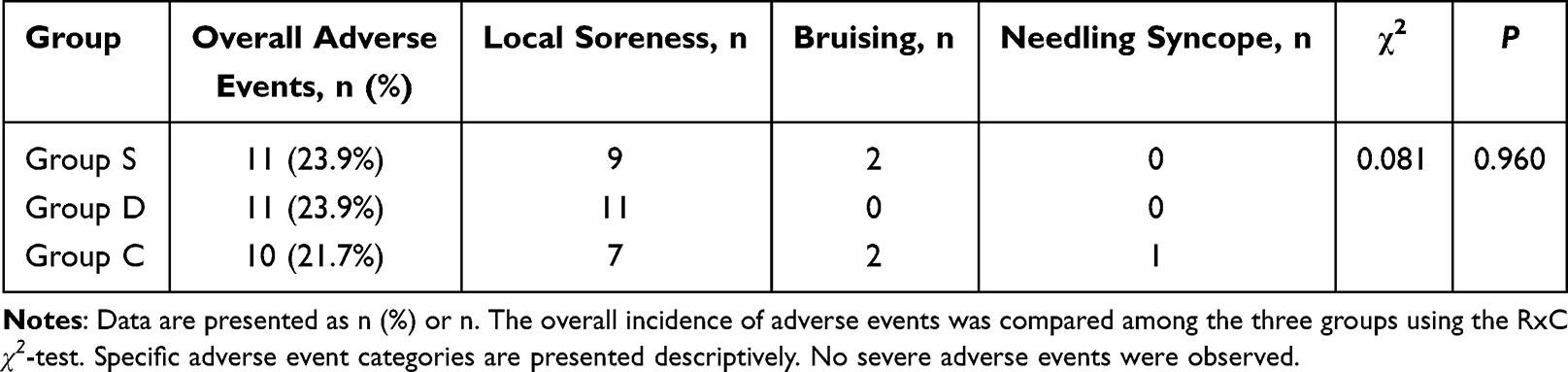 |
Table 5 Comparison of Adverse Events Among the Three Groups |
Group × Time Interaction
A statistically significant group × time interaction was observed (P < 0.001). Compared to Group S, Group D exhibited a substantially slower rate of pain recurrence at weeks 1, 4, and 8 (all P < 0.05). In contrast, Group C demonstrated no significant differences from Group S. These findings suggest that the dense-disperse waveform may be associated with more sustained pain relief than the continuous waveform over the present 12-week follow-up (Table 6).
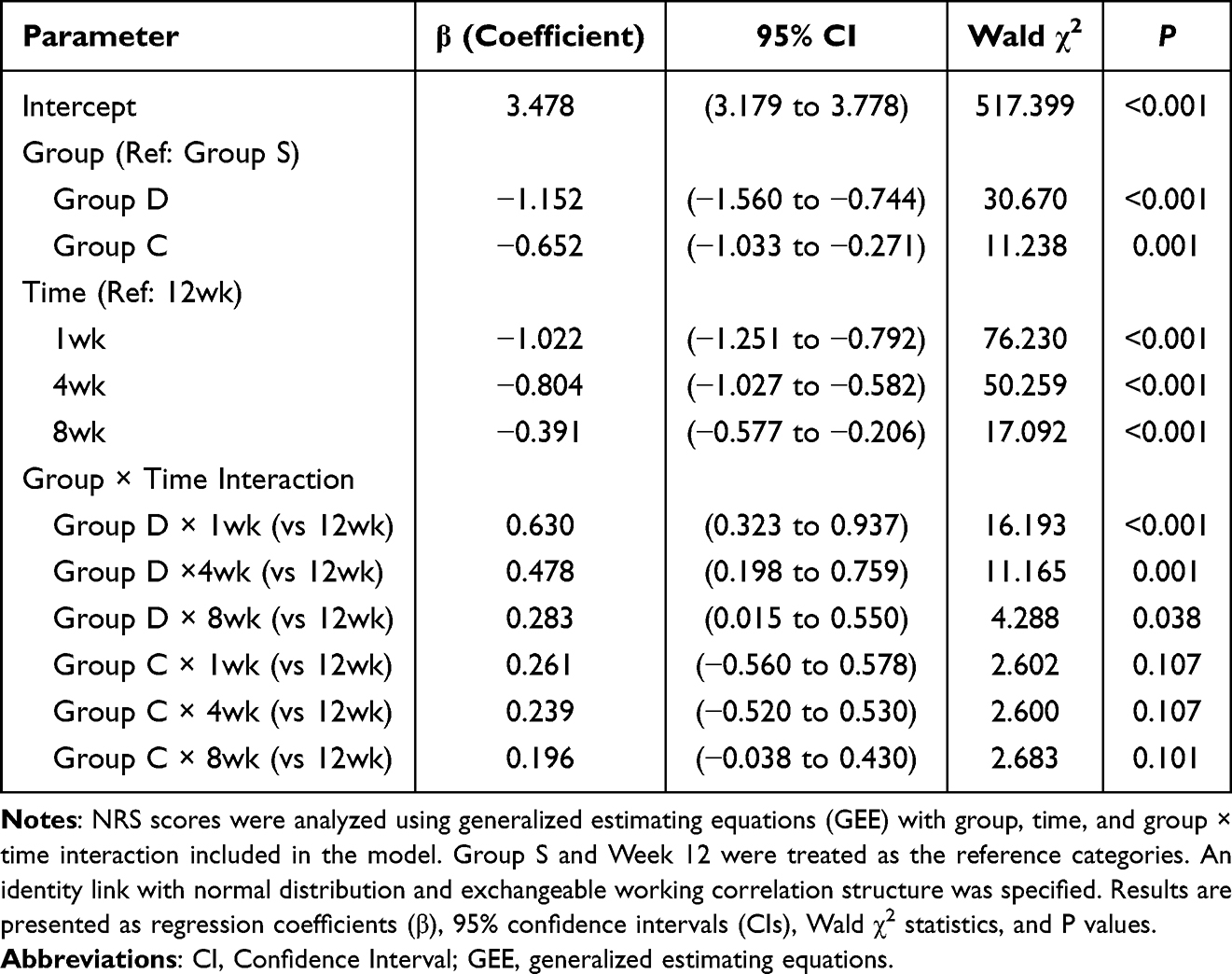 |
Table 6 GEE Analysis of Group, Time, and Group-by-Time Interaction Effects on NRS Scores |
Discussion
In the present study, both electrical-DN regimens combined with CSI were associated with greater improvements in pain and function than sham stimulation in participants with KOA. More specifically, both the dense-disperse wave group and the continuous wave group showed lower NRS and WOMAC scores than the sham stimulation group during follow-up, while the dense-disperse wave group demonstrated additional advantages over the continuous wave group in NRS at weeks 8 and 12 and in WOMAC at week 12. In addition, all interventions were generally well tolerated, and the adverse events observed were mild and self-limiting.
Pain intensity, assessed by the NRS as the primary outcome, showed a between-group difference. Compared with sham stimulation, both electrical-DN regimens achieved greater pain relief throughout follow-up, suggesting an additional analgesic effect of electrical stimulation in this combined-treatment setting. Furthermore, the dense-disperse waveform provided more sustained pain reduction than the continuous waveform at weeks 8 and 12, suggesting that waveform selection may influence the durability of treatment effects; however, the magnitude of the statistical difference was limited. This finding is in line with previous studies showing that electrical stimulation-based needling interventions may offer greater analgesic benefit than non-electrical needling approaches, and it extends prior work by directly comparing two waveform patterns in KOA.12,19,20
Functional outcomes showed a similar pattern. WOMAC scores were significantly lower in both electrical-DN groups than in the sham group across follow-up, and the dense-disperse wave group also showed an advantage over the continuous wave group at week 12. These findings indicate that pain reduction was accompanied by improvement in joint-related symptoms and physical function.21 In addition, the significantly greater improvement in FROM in the two electrical-DN groups at week 1 suggests that electrical stimulation may help reduce movement restriction in the early post-treatment phase. SF-MPQ scores were significantly lower in the electrical-DN groups than in the sham group at week 1, indicating an early benefit in multidimensional pain experience, although the between-group difference was not maintained at later follow-up. Taken together, these results suggest that electrical-DN may contribute to symptomatic relief and short-term functional improvement in KOA.
By contrast, no significant between-group differences were found in PSQI or HAMA at week 12, although PSQI improved compared with baseline within all three groups. These findings suggest that improvements in local pain do not necessarily translate into measurable differences in sleep quality or anxiety over a relatively short follow-up period. Sleep and emotional status are influenced by multiple biological, psychological, and behavioral factors, and may require longer intervention duration, longer follow-up, or more targeted psychosocial support to demonstrate clear between-group effects. Therefore, the absence of significant differences in PSQI and HAMA should be interpreted cautiously rather than as evidence of no clinical relevance.
The more sustained short- to mid-term analgesic effect of the dense-disperse waveform may be related to reduced neural habituation compared with continuous stimulation.22,23 Different frequencies of peripheral electrical stimulation may promote the release of different neurotransmitters, with low-frequency stimulation being associated with increased enkephalin release and high-frequency stimulation potentially enhancing dynorphin release.24 On this basis, dense-disperse stimulation, which provides variable frequency input, may engage a broader range of neurophysiological analgesic pathways and thereby contribute to more sustained pain relief. Zhang et al supported this by finding that dense-disperse wave was superior to continuous wave in treating acute facial paralysis, improving microcirculation, boosting nerve recovery, and reducing inflammation.25
In addition, our intervention targeted not only local knee-related muscles but also proximal muscles involved in lumbopelvic stability, such as the gluteal and trunk-related muscles. This broader myofascial approach may have contributed to improvements in force transmission, dynamic stability, and lower-limb biomechanics. However, this biomechanical explanation remains inferential, and future studies are needed to further clarify the mechanisms underlying these effects.26,27
Limitations
Several limitations should be acknowledged. First, the absence of imaging or biomarker data limited the objective assessment of structural or inflammatory changes after treatment. Second, maintaining participant blinding was challenging because those undergoing electrical dry needling could perceive muscle twitching or stimulation-related sensations, which may have introduced performance bias and placebo-related effects. Formal assessment of blinding integrity was not performed. Third, although all participants received standardized exercise guidance, daily activity levels outside the study protocol were not quantitatively assessed, and high-intensity physical activities were not strictly restricted, which may have introduced uncontrolled confounding. Fourth, as all groups received ultrasound-guided CSI and the sham group also underwent mechanical dry needling, the present findings are more appropriately interpreted as reflecting the additional effects of electrical dry needling within a combined-treatment setting. Finally, the 12-week follow-up period may be insufficient to evaluate the long-term durability of treatment effects in a chronic condition such as KOA.
Future studies should include larger sample sizes, incorporate more objective outcome measures, and use longer follow-up durations to further clarify the mechanisms underlying the observed effects and validate the present findings.
Conclusion
These findings suggest that trigger point electrical dry needling may provide additional pain-relieving benefit in patients with KOA when used in combination with CSI. Among the two electrical-DN groups, the dense-disperse waveform was associated with a modest advantage in pain relief at later follow-up time points, although the clinical magnitude of this between-waveform difference should be interpreted cautiously.
Trial Registration
This study was prospectively registered at the Chinese Clinical Trial Registry under registration number ChiCTR2500102033. The registered protocol corresponds to the present study, and no interim analysis from the same dataset has been published previously.
Abbreviations
KOA, Knee osteoarthritis; Electrical-DN, Electrical Dry Needling; CSI, intra-articular Corticosteroid Injection; MPS, Myofascial Pain Syndrome; MTrPs, Myofascial Trigger Points; LTR, Local Twitch Response; MCID, Minimal Clinically Important Difference; NRS, Numerical Rating Scale; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index; SF-MPQ, Short-Form McGill Pain Questionnaire; PSQI, Pittsburgh Sleep Quality Index; HAMA, Hamilton Anxiety Rating Scale; FROM, Knee Flexion Range of Motion; CI, Confidence Interval; SD, Standard Deviation.
Data Sharing Statement
The raw data supporting the conclusions of this article are available from the corresponding author, Yan Yuan (Email: [email protected]), upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Giorgino R, Albano D, Fusco S, Peretti GM, Mangiavini L, Messina C. Knee osteoarthritis: epidemiology, pathogenesis, and mesenchymal stem cells: what else is new? an update. Int J Mol Sci. 2023;24(7):6405. doi:10.3390/ijms24076405
2. Fearon A, Neeman T, Smith P, Scarvell J, Cook J. Pain, not structural impairments may explain activity limitations in people with gluteal tendinopathy or Hip osteoarthritis: a cross sectional study. Gait Posture. 2017;52:237–12. doi:10.1016/j.gaitpost.2016.12.005
3. Veronese N, Stubbs B, Solmi M, et al. Association between lower limb osteoarthritis and incidence of depressive symptoms: data from the osteoarthritis initiative. Age Ageing. 2017;46(3):470–476. doi:10.1093/ageing/afw216
4. Lv Y, Sui L, Lv H, Zheng J, Feng H, Jing F. Burden of knee osteoarthritis in China and globally from 1992 to 2021, and projections to 2030: a systematic analysis from the global burden of disease study 2021. Front Public Health. 2025;13:1543180. doi:10.3389/fpubh.2025.1543180
5. Stubnya BG, Schulz M, Váncsa S, Szilágyi GS, Szatmári A, Bejek Z. Global trends in joint arthroplasty: a systematic review and future projections. J Clin Med. 2025;14(22):8214. doi:10.3390/jcm14228214
6. Moldovan F, Moldovan L, Bataga T. A comprehensive research on the prevalence and evolution trend of orthopedic surgeries in romania. Healthcare. 2023;11(13):1866. doi:10.3390/healthcare11131866
7. Ma YT, Dong YL, Wang B, Xie WP, Huang QM, Zheng YJ. Dry needling on latent and active myofascial trigger points versus oral diclofenac in patients with knee osteoarthritis: a randomized controlled trial. BMC Musculoskelet Disord. 2023;24(1):36. doi:10.1186/s12891-022-06116-9
8. Henry R, Cahill CM, Wood G, et al. Myofascial pain in patients waitlisted for total knee arthroplasty. Pain Res Manag. 2012;17(5):321–327. doi:10.1155/2012/547183
9. Leetun DT, Ireland ML, Willson JD, Ballantyne BT, Davis IM. Core stability measures as risk factors for lower extremity injury in athletes. Med Sci Sports Exerc. 2004;36(6):926–934. doi:10.1249/01.mss.0000128145.75199.c3
10. Rozenfeld E, Finestone AS, Moran U, Damri E, Kalichman L. The prevalence of myofascial trigger points in Hip and thigh areas in anterior knee pain patients. J Bodyw Mov Ther. 2020;24(1):31–38. doi:10.1016/j.jbmt.2019.05.010
11. Moro MZ, de Oliveira Vidal EI, Pinheiro Módolo NS, Bono Fukushima F, Moreira de Barros GA. Dry needling, trigger point electroacupuncture and motor point electroacupuncture for the treatment of myofascial pain syndrome involving the trapezius: a randomised clinical trial. Acupunct Med. 2024;42(1):3–13. doi:10.1177/09645284231207865
12. Chen N, Wang J, Mucelli A, Zhang X, Wang C. Electro-acupuncture is beneficial for knee osteoarthritis: the evidence from meta-analysis of randomized controlled trials. Am J Chin Med. 2017;45(5):965–985. doi:10.1142/S0192415X17500513
13. Wu X, Li S, Wu M. Advances in electroacupuncture for treatment of knee osteoarthritis: mechanisms, efficacy, and future directions. J Pain Res. 2025;18:5083–5108. doi:10.2147/JPR.S543346
14. Wang X, Sun Q, Wang M, et al. Electrical dry needling plus corticosteroid injection for osteoarthritis of the knee: a randomized controlled trial. Arch Phys Med Rehabil. 2022;103(5):858–866. doi:10.1016/j.apmr.2021.12.026
15. Farrar JT, JP Y Jr, LaMoreaux L, Werth JL, Poole MR. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94(2):149–158. doi:10.1016/S0304-3959(01)00349-9
16. Deyle GD, Allison SC, Matekel RL, et al. Physical therapy treatment effectiveness for osteoarthritis of the knee: a randomized comparison of supervised clinical exercise and manual therapy procedures versus a home exercise program. Phys Ther. 2005;85(12):1301–1317. doi:10.1093/ptj/85.12.1301
17. Xie F, Li SC, Goeree R, et al. Validation of Chinese Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) in patients scheduled for total knee replacement. Qual Life Res. 2008;17(4):595–601. doi:10.1007/s11136-008-9340-7
18. Hancock GE, Hepworth T, Wembridge K. Accuracy and reliability of knee goniometry methods. J Exp Orthop. 2018;5(1):46. doi:10.1186/s40634-018-0161-5
19. Wang TQ, Li YT, Wang LQ, et al. Electroacupuncture versus manual acupuncture for knee osteoarthritis: a randomized controlled pilot trial. Acupunct Med. 2020;38(5):291–300. doi:10.1177/0964528419900781
20. Chen J, Liu XX, Liu XX. Tackling osteoarthritic knee pain with electroacupuncture. Chin J Integr Med. 2018;24(11):803–805. doi:10.1007/s11655-018-2929-3
21. Dunning J, Butts R, Young I, et al. Periosteal electrical dry needling as an adjunct to exercise and manual therapy for knee osteoarthritis: a multicenter randomized clinical trial. Clin J Pain. 2018;34(12):1149–1158. doi:10.1097/AJP.0000000000000634
22. Wang LF, Xi Q. Current status of parameter selection in clinical electro-acupuncture treatment of knee osteoarthritis. Guid J Tradit Chin Med Pharm. 2019;25(08):108–113.
23. Tianyi ZHAO, Qiang XI, Yi GUO. Current research status and analysis of electroacupuncture parameters for post-operative pain. Shanghai J Acupuncture Moxibustion. 2015;464–467.
24. Han JS. Acupuncture: neuropeptide release produced by electrical stimulation of different frequencies. Trends Neurosci. 2003;26(1):17–22. doi:10.1016/s0166-2236(02)00006-1
25. Zhang H, Chen F. Efficacy of electroacupuncture with sparse-dense-wave on patients suffered acute facial paralysis. Clin Cosmet Invest Dermatol. 2023;16:1811–1819. doi:10.2147/CCID.S405569
26. Powers CM. The influence of abnormal Hip mechanics on knee injury: a biomechanical perspective. J Orthop Sports Phys Ther. 2010;40(2):42–51. doi:10.2519/jospt.2010.3337
27. Zarei H, Bervis S, Piroozi S, Motealleh A. Added value of gluteus medius and quadratus lumborum dry needling in improving knee pain and function in female athletes with patellofemoral pain syndrome: a randomized clinical trial. Arch Phys Med Rehabil. 2020;101(2):265–274. doi:10.1016/j.apmr.2019.07.009
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.