")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Trends, Uptake, and Predictors of Influenza Vaccination Among Healthcare Practitioners During the COVID-19 Pandemic Flu Season (2020) and the Following Season (2021) in Saudi Arabia
Authors Alkathlan M, Khalil R , Alhemaidani MF, Alaed GH, Almutairi SM, Almalki HA, Alghofaili RH, Al-Wutayd O
Received 18 July 2021
Accepted for publication 1 September 2021
Published 15 September 2021 Volume 2021:14 Pages 2527—2536
DOI https://doi.org/10.2147/JMDH.S330029
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Mohammed Alkathlan,1 Rehana Khalil,2 Munirah F Alhemaidani,3 Ghadah H Alaed,3 Shatha M Almutairi,3 Hala A Almalki,3 Renad H Alghofaili,3 Osama Al-Wutayd2
1Department of Infectious Diseases, King Fahad Specialist Hospital, Buraydah, Saudi Arabia; 2Department of Family and Community Medicine, Unaizah College of Medicine and Medical Sciences, Qassim University, Unaizah, Saudi Arabia; 3Unaizah College of Medicine and Medical Sciences, Qassim University, Unaizah, Saudi Arabia
Correspondence: Osama Al-Wutayd Email [email protected]
Background: Healthcare practitioners (HCPs) are at high risk of influenza. Seasonal influenza vaccines can reduce influenza-associated morbidity in healthcare settings, but despite mandatory influenza vaccination in the Kingdom of Saudi Arabia, the vaccination uptake rate among HCPs is below expectations. This study investigated vaccination trends from 2017 to 2020 to identify factors affecting vaccination among HCPs during the COVID-19 pandemic flu and subsequent seasons.
Methods: Cross-sectional study among HCPs was conducted in January 2021. A structured questionnaire was shared via social media. Vaccine uptake predictors were identified using descriptive statistics and logistic regression models (p-value 0.05).
Results: A total of 424 HCPs (118 physicians and 306 nurses) completed the questionnaire. Vaccine uptake increased from 2017 to 2019 (45% to 52% to 62%) but fell (to 59%) during the 2020 COVID-19 pandemic flu season. Multivariable analysis indicated participants > 40 years old (AOR 3.09, 95% CI 1.64– 5.83), female (AOR 1.74, 95% CI 1.13– 2.67), non-Saudi (AOR 2.62, 95% CI 1.72– 4.01), nurses (AOR 2.70, 95% CI 1.75– 4.17), and who possessed accurate knowledge of the flu vaccine efficacy duration (AOR 3.04, 95% CI 1.87– 4.94) were more likely to have received the vaccine. However, 79% of HCPs declared their intention to be vaccinated in the 2021 flu season, with participants > 40 years old, female (AOR 2.25, 95% CI 1.38– 3.68), non-Saudi (AOR 3.79, 95% CI 2.34– 6.16), or nurses (AOR 2.94, 95% CI 1.82– 4.76) more likely to do so.
Conclusion: Influenza vaccination uptake declined among HCPs during the 2020 flu season compared with the previous season but is expected to increase in the upcoming 2021 season. Nevertheless, the findings are encouraging and indicate increased willingness of HCPs to become vaccinated in the upcoming 2021 season, but coverage could be further increased by policymakers via a comprehensive plan focusing particularly on younger HCPs, Saudis, males, and physicians.
Keywords: influenza vaccine, trends, uptake, predictors, healthcare practitioners, COVID-19 pandemic, Saudi Arabia
Introduction
Seasonal influenza (flu) is highly contagious and spreads via respiratory droplets.1 Influenza places the health of millions at risk and has serious economic consequences, using up a large amount of healthcare resources.2 Annual global mortality due to severe influenza infection is estimated at between 290,000 and 640,000 persons.1,2 Healthcare practitioners (HCPs) are always at high risk of acquiring influenza and transmitting it to other HCPs and their patients.3 The World Health Organization (WHO) recommends annual vaccination as the prime strategy for preventing influenza,2,3 especially during the ongoing COVID-19 pandemic declared by the WHO on March 11, 2020.4
A huge burden has been placed on healthcare workers worldwide due to the marked increase in demand for care; thus, shortages of healthcare staff due to sickness can be ill-afforded,5 particularly as flu-like symptoms may not be due to influenza but rather COVID-19 or even co-infection involving both.6 This situation makes influenza vaccination critical, not only to prevent co-infection but also to decrease the number of flu patients in order to make room for COVID-19 patients.7 Protecting oneself from influenza infection may improve overall health by preventing the emergence of other health issues resulting from acquired infections, including COVID-19.5,6 In Saudi Arabia, influenza is given high priority because of numerous outbreaks that have occurred in recent years.8 The 2017 Infection Prevention and Control Guidelines from the Saudi Ministry of Health (MOH) recommended annual influenza vaccination for HCPs, in line with recommendations from the Advisory Committee on Immunization Practices, and HCPs were declared a high-risk group.9,10 The MOH recommended mandatory influenza vaccination for all healthcare personnel on a yearly basis. Furthermore, the vaccine is available free of charge to all HCPs.10,11
It has been noted that attitudes of patients and the general population toward vaccination are affected by the behavior and motivation of HCPs in their vicinity; thus, a positive attitude from HCPs is very important for avoiding vaccine-preventable diseases.12–15 The aim of this study was therefore to determine the trend in influenza vaccination from 2017 to 2020 and identify predictors of vaccination during the COVID-19 pandemic flu season (2020) and the following season (2021) among HCPs in the Qassim region of Saudi Arabia.
Materials and Methods
Design and Subjects
A web-based cross-sectional study was conducted in January 2021 among HCPs at King Fahad Specialist Hospital and King Saud Hospital—the two major hospitals in the Qassim region of Saudi Arabia. A non-probability sampling technique was used: the study included HCPs (only physicians and nurses) working in the hospitals during data collection; other HCPs or those on vacation were excluded.
Questionnaire Description
A questionnaire written in the English language (s1) was developed using information published according to the objectives of the study.5,16 A pilot study was conducted among 10 HCPs, who were asked to answer the questionnaire and then report their feedback regarding the clarity of the questions and time required for completion. The pilot study results were not included in the main study. The questionnaire was also reviewed by 3 experts regarding the face and content validity, and their comments were considered in development of the final questionnaire.
Dependent Variables
The two dependent variables were influenza vaccination uptake in 2020 and intent to vaccinate in 2021. These variables were assessed via the question “Were you vaccinated against flu for last season, 2020, and do you intend to get vaccinated for next season, 2021?”
Independent Variables
The independent variables were of two types:
- Sociodemographic information, consisting of age range (≤30 years, 31–40 years, >40 years), gender (male, female), nationality (Saudi, non-Saudi), education level (bachelor’s, diploma, postgraduate), participant category (physician, nurse), history of comorbid conditions (diabetes mellitus, obesity, hypertension, cardiac disease, chronic respiratory illnesses, malignancy, other), and history of COVID-19 infection (yes, confirmed by test; yes, not confirmed by test; no).
- Flu vaccine–related information, consisting of the year(s) in which the participant was vaccinated (2017, 2018, 2019), the level of confidence in information from the MOH (high, low), and the believed duration of flu vaccine efficacy (life-long, 5 years, 1 year, 6 months).
Data Collection
A link to an online questionnaire was distributed via social media based on contact with heads of departments in the hospitals. Participants were also encouraged to pass the link to other colleagues. The study title, objective, and purpose were explained to the HCPs, and consent to participate was required on the front page before proceeding. The study was approved by the Qassim University ethics committee (reference number 20-03-05).
Sample Size Calculation
The sample size was calculated for a cross-sectional study using OpenEpi statistical software, with 5% precision and 95% confidence. The prevalence of vaccine hesitancy among HCPs was assumed to be 50% in order to estimate the maximum sample size. We assumed a non-response rate of 10%, and the minimum sample size was thus calculated to be 424 HCPs.
Statistical Analyses
The data were received in Excel, and analyses were performed using STATA v.16. Frequencies and percentages of each variable are presented for categorical variables. Simple and multiple logistic regression analyses were used to assess the association of potential predictors as independent variables with influenza vaccination during the COVID-19 pandemic season (2020) and the following season (2021) as dependent variables. Simple logistic regression was used to assess the association between one potential predictor and the dependent variable to calculate the unadjusted odds ratio (OR) and 95% confidence interval (CI). Multiple logistic regression included potential predictors with p-values of <0.20 in simple logistic regression to calculate the adjusted odds ratios (AORs) and 95% CIs. A p-value of <0.05 was considered strong evidence against the null hypothesis.
Results
The response rate in our study was 85% (424/500). Table 1 shows the descriptive characteristics of participants according to the two outcome variables. A total of 424 HCPs completed the questionnaire, and their responses were analyzed. A total of 250 (59%) of the HCPs received the influenza vaccine in 2020, and 334 (79%) intended to get it in 2021.
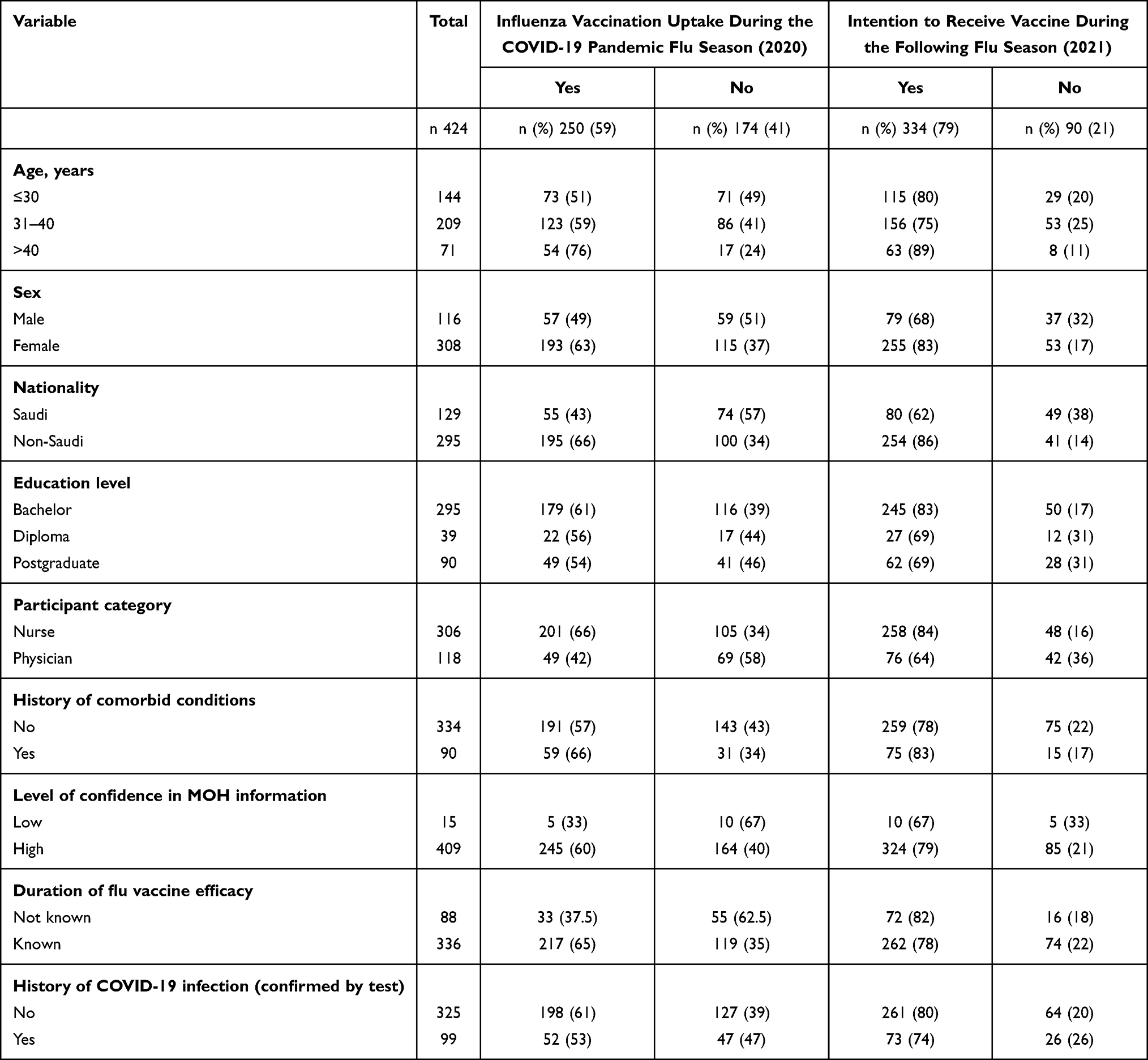 |
Table 1 Descriptive Statistics of the Participants |
Figure 1 shows the influenza vaccine uptake rate from 2017 to 2020 and the intent to take the vaccine in 2021. The vaccination coverage rates increased significantly, from 45% (n=191) in season 2017 to 52% (n=221) in season 2018 (p=0.002). In season 2019, an increase to 62% (n=266) was seen in this sample, which was a statistically significant (p<0.001) increase compared with season 2018. Vaccination uptake declined non-significantly from 62% (n=266) in 2019 to 59% (n=250) in season 2020 (p=0.15). With regard to the coming 2021 season, 79% (n=334) of participants intended to get vaccinated against influenza, and this rate was significantly higher than the vaccine uptake in season 2020 (p<0.001).
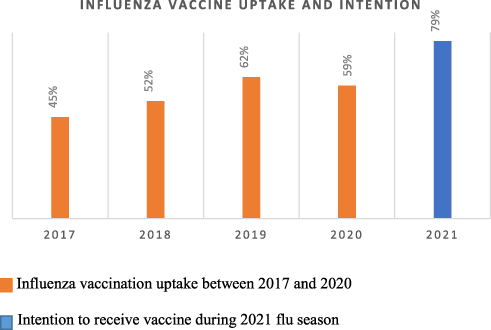 |
Figure 1 Influenza vaccination uptake between 2017 and 2020 and intention for 2021. |
Table 2 shows the unadjusted and adjusted associations between potential predictors and each of the two outcome variables.
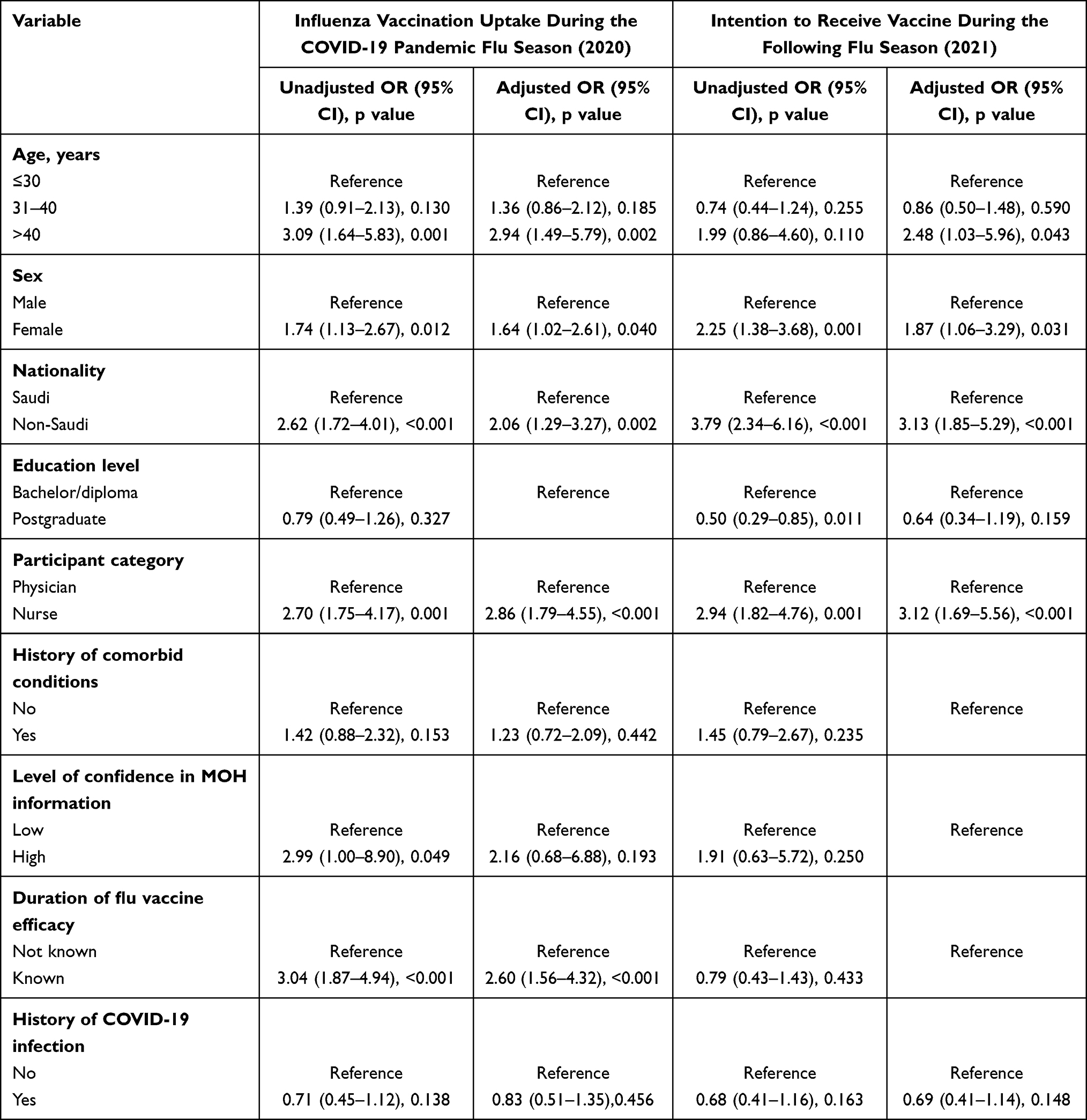 |
Table 2 Unadjusted and Adjusted Associations Between Potential Predictors and Influenza Vaccination Uptake in 2020 (Covid-19 Pandemic), and Intention to Receive Vaccine During 2021 Flu Season |
Influenza Vaccination Uptake During the COVID-19 Pandemic Flu Season (2020)
Table 2 shows the ORs and AORs between potential predictors and the first outcome variable (influenza vaccination uptake in 2020). The unadjusted analysis showed that the OR of influenza vaccine uptake was significantly higher among participants who were older than 40 years (OR 3.09, 95% CI 1.64–5.83, p=0.001), female (OR 1.74, 95% CI 1.13–2.67, p=0.012), non-Saudi (OR 2.62, 95% CI 1.72–4.01, p<0.001), and nurses (OR 2.70, 95% CI 1.75–4.17, p=0.001); among those whose degree of confidence in MOH information was high (OR 2.99, 95% CI 1.00–8.90, p=0.049); and among those who had correct knowledge of the duration of flu vaccine efficacy (OR 3.04, 95% CI 1.87–4.94, p<0.001). The AOR of influenza vaccine uptake was significantly higher among females than males (AOR 1.64, 95% CI 1.02–2.61, p=0.040) and higher among nurses than physicians (AOR 2.86, 95% CI 1.79–4.55, p<0.001). Participants aged over 40 years were 2.94 times (95% CI 1.49–5.79, p=0.002) more likely to receive the vaccine than participants 30 years old or younger. Non-Saudi respondents were 2.06 times (95% CI 1.29–3.27, p=0.002) more likely to receive the influenza vaccine than Saudi nationals, and influenza vaccine uptake was 2.60 times (95% CI 1.56–4.32, p≤0.001) more likely among participants with correct knowledge of the duration of flu vaccine efficacy than those without.
Intention to Receive Vaccine During the Following Flu Season (2021)
Table 2 shows the ORs and AORs between the potential predictors and the second outcome variable (influenza vaccination intent for 2021). The unadjusted analysis showed that the OR for intention to take the influenza vaccine was significantly higher among females (OR 2.25, 95% CI 1.38–3.68, p=0.001), non-Saudis (OR 3.79, 95% CI 2.34–6.16, p<0.001), and nurses (OR 2.94, 95% CI 1.82–4.76, p=0.001) but significantly lower among postgraduates than those with a bachelor’s degree/diploma (OR 0.50, 95% CI 0.29–0.85, p=0.011). The adjusted analysis showed that the AOR of intention to receive the vaccine was 2.48 times (95% CI 1.03–5.96, p=0.043) higher among participants over 40 years of age than among participants 30 years of age or younger. Female HCPs were 1.87 times more likely to receive the influenza vaccine than males (95% CI 1.06–3.29, p=0.031), and nurses were 3.12 times more likely to receive the influenza vaccine than physicians (95% CI 1.69–5.56, p<0.001). Non-Saudi participants were 3.13 times (95% CI 1.85–5.29, p≤0.001) more likely to receive the vaccine than Saudi nationals.
Discussion
The current study found a steep upward trend in seasonal influenza vaccination uptake among HCPs from 2017 to 2019 and a decline in uptake during the COVID-19 pandemic in 2020. Even though the decline in vaccination uptake in season 2020 compared to season 2019 was statistically non-significant, in the context of strong recommendations (by the MOH, CDC, and WHO) to take the flu vaccine during the current pandemic, even a small decline in KSA was unexpected. Keeping this in mind, we therefore considered this small reduction as alarming and worth reporting. There was thus a promising trend in increased flu vaccine acceptability among HCPs in Saudi Arabia before the pandemic, suggesting success of the MOH’s flu vaccination campaign, which was established according to the WHO’s Global Action Plan for influenza vaccines.10 The response of the human immune system to influenza viruses wanes over time due to the high viral mutation rate, and the WHO therefore updates the flu vaccine annually to keep pace with the changing influenza virus. It is therefore highly recommended that people at risk, including health sector personnel, pregnant women, and patients with chronic diseases, receive the vaccine annually.3
The MOH organizes an annual influenza vaccine campaign through MOH hospitals and public healthcare centers in all regions of Saudi Arabia, with the influenza vaccine provided free of cost.10,11 The COVID-19 pandemic affected everyone’s life, the economy, and nearly every part of the world. The disease has sickened more than 181 million people worldwide, and more than 3.9 million people have died to date. According to the WHO, as of June 25, 2021, there were 479,390 confirmed cases of COVID-19 and 7730 deaths in Saudi Arabia.17 Seasonal influenza vaccine is recommended every year, and there are additional reasons in the context of the ongoing pandemic. Even though flu vaccines do not provide protection against COVID-19 infection, they are particularly recommended this year by the CDC and WHO to reduce pressure on healthcare systems that are still battling the coronavirus.1,3 There is also evidence that influenza and COVID-19 co-infection may result in a more severe disease, and co-infection can certainly complicate diagnosis; as more information becomes available, understanding of this issue will increase.18
In most years, the seasonal influenza vaccine is approximately 70–90% effective in preventing the flu.19 If someone still becomes ill even after getting the flu vaccine or contracts a co-infection with another virus, such as a coronavirus, the vaccine can still reduce the severity of the disease. While the world was waiting for a COVID-19 vaccine at the start of winter 2020, a vaccine for influenza was available at little or no cost, making it particularly beneficial for conserving scarce medical resources to care for people with COVID-19 infections. Another benefit is a reduction in the prevalence of flu in the community, which can reduce the need for doctors’ visits, the risk of developing fever and respiratory symptoms, and thus the risk of being quarantined.20
Unlike the study conducted in Italy by Giorgia Della Polla and colleagues21 and other studies involving a variety of methodologies and populations21–25 and showed an increased likelihood of vaccination during the current pandemic, in our study, 59% of HCPs received an influenza vaccine in the year 2020. This rate was slightly higher as compared with the mean adherence of HCPs to influenza vaccination reported by Mereckiene et al26 and Di Pumpo et al27 (30% and 24.19%, respectively) and within the mean adherence range (22–83%) reported in a systematic review by Bish et al28 but lower than expected in 2020 in the Kingdom of Saudi Arabia. A similar decline in influenza vaccination among HCPs was observed in Europe during the 2010–2011 pandemic, in which Germany, France, Norway, Spain, Slovenia, and Wales reported a range of 14% to 28% vaccination coverage.26 We speculate that one reason for this relatively low uptake in 2020 as compared with 2019 was the successful crisis management of the COVID-19 pandemic in Saudi Arabia, which was among the countries that implemented timely interventions against COVID-19 infection and successfully mitigated the impact of the disease nationally.29 Ironically, this led to HCPs deciding that getting the seasonal influenza vaccination themselves was of little importance for the 2020 winter season because of social distancing and face mask practices providing greater protection.30–32 This complacency decreased the uptake of the vaccine. A second reason for the reduction in influenza vaccinations among HCPs may have been research evidence that showed increased risk of coronavirus infection in people receiving the vaccine. Cowling et al33 found a high risk (relative risk 4.40) of confirmed non-influenza respiratory virus infection among influenza vaccine recipients.33 Similarly, a study by Wolff34 examined different respiratory viruses and their association with the influenza vaccine and concluded that there is an increased risk of coronavirus infection in individuals receiving influenza vaccinations, a phenomenon known as virus interference. Viral interference is a phenomenon in which infection with one virus limits infection and replication of a second virus. In other words, a cell infected by a virus becomes resistant toward a second outcoming infection by a superinfectant virus. Natural influenza infection may reduce the risk of non-influenza respiratory viruses by providing temporary, non-specific immunity against these viruses.
On the other hand, influenza-vaccinated individuals may show vaccine-associated virus interference; that is, vaccinated individuals may be at increased risk for other respiratory viruses because they do not develop the non-specific immunity associated with natural infection.34 The current study also sought to assess the intention of HCPs to get vaccinated for the 2021 season and found that 79% intended to do so, which is a 20% increase compared to 2020. This finding is consistent with a study done on HCPs in Italy,27 which showed an increase from 24.19% (2019–2020) to 54.56% in the upcoming season 2020–2021. Another study reported 68% willingness for future vaccination in the 2020–2021 season, where 95% of participants were vaccinated and 45.8% of participants never vaccinated in the previous six influenza seasons.35 Intent does not guarantee performance, but this finding is unsurprising due to recent studies, such as that by Belingheri et al36 which have refuted the association between flu vaccinations and COVID-19 infection and recommended influenza vaccinations for HCPs. Another relevant finding was reported by Iacobucci et al18 who found that co-infection doubles the risk of death.18 Research studies have identified psychological, contextual, sociodemographic, and physical barriers that may affect seasonal vaccination campaigns and make them less impactful than might be expected.12,13
In this study, being over 40 years of age, female, a nurse, a non-Saudi, and having correct knowledge of the duration of flu vaccine efficacy were independently associated with greater uptake of the influenza vaccination. With the exception of knowledge of efficacy duration, the same variables predicted intention to receive the influenza vaccine in the 2021 flu season. In the present study, older (>40 years of age, p=0.001)—and likely more professionally experienced—participants were more likely to be vaccinated against seasonal influenza, and this greater professional experience may be explanatory. This finding was similar to that reported by Esposito et al37 who found that age 45 years (p=0.015) or older (p<0.001) was positively associated with influenza vaccination in an Italian sample. In that study, the authors recommended an intervention explicitly focused on young HCPs to improve the vaccination rate. Female respondents in the present study were found to be more compliant (63%, OR 1.74) with influenza vaccination than their male counterparts (49%), consistent with the report of Qureshi et al38 in which females were 9.11 times more likely to undergo vaccination as compared with males. However, our result was in contrast to those of Esposito et al37 who reported that females were 0.76 times less likely to receive the vaccine than males, and in contrast to the results of Asma et al39 in which 51.7% of females were compliant and 66% noncompliant, compared with 48.3% compliant males and 33% noncompliant males. Most of the nurses in the present study were female, and nurses were also significantly more likely (66%, OR 2.70) to get vaccinated against influenza. However, this result is in contrast to those of Asma et al39 (8.2%) and Trivalle et al40 who reported nurses were 2.41 times less likely to get the vaccine than physicians; thus, in those studies, nurses were more likely to refuse the vaccine.
Non-Saudi respondents were considerably more likely to take the influenza vaccine than Saudi nationals. The most plausible explanation for this difference involves work contracts for non-Saudi nationals, who may need to show a valid vaccination certificate for contract renewal.
We also found a 2.41 times greater likelihood of influenza vaccine uptake among participants with correct knowledge of the duration of flu vaccine efficacy than participants without such knowledge (p=0.001), consistent with the report of Asma et al39 who found that inaccurate understanding among HCPs negatively influences their response to influenza vaccination. There is little doubt that adequate knowledge about influenza vaccination is a salient factor in addressing false beliefs,41 but a number of research studies have shown that knowledge alone is not sufficient to address behaviors.40,42–46 Looijmans-van den Akker et al47 found no significant difference between physicians’ and the general population’s analytical knowledge when risk perception was low, and likewise, physicians’ attitudes were found to be no different from those of the general population when there was a high perception of risk. Single-factor interventions, such as improving information or a strategy focused on young HCPs, have not proven effective,45,46 and a sustainable multi-strategy approach should therefore be used to address sub-optimal seasonal influenza vaccinations among HCPs.47–49
This study has a number of limitations. First, the study was a cross-sectional design, so we cannot establish any causal inference, and we also used a non-probability sampling technique that limited the generalizability of the results. Furthermore, there is a possibility of recall bias in the self-reporting of vaccination status by the HCPs. Those spending time on social media during the pandemic likely have different attitudes towards the vaccine compared with those not responding to web-based surveys, and there may also be social desirability bias in reporting intent to be vaccinated next year. We believe a qualitative study could broaden the perspective and help in the formulation of interventions.
Conclusions
The rate of influenza vaccination uptake among HCPs was lower during the season of 2020 as compared with the previous season, but it is expected to increase in the upcoming season of 2021. Nevertheless, the findings are encouraging and ensure an increased willingness among HCPs to receive the influenza vaccine in the upcoming season of 2021. However, coverage could be maximized further by policymakers through implementation of a comprehensive plan with a special focus on younger HCPs, Saudis, males, and physicians.
Ethics Approval
The study was approved by the Qassim University ethics committee (reference number 20-03-05). All procedures performed in the study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments. The study title, objective, and purpose were explained to the HCPs and consent to participate required on the front page before proceeding.
Acknowledgments
The researchers would like to thank the Deanship of Scientific Research, Qassim University, for funding the publication of this project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Centers for Disease Control and Prevention. Influenza; 2021. Available from: https://www.cdc.gov/flu/about/index.html.
2. Abalkhail MS, Alzahrany MS, Alghamdi KA, et al. Uptake of influenza vaccination, awareness and its associated barriers among medical students of a university hospital in Central Saudi Arabia. J Infect Public Health. 2017;10(5):644–648. doi:10.1016/j.jiph.2017.05.001
3. World Health Organization. Influenza (seasonal); 2018. Available from: https://www.who.int/news-room/fact-sheets/detail/influenza-(seasonal).
4. Cucinotta D, Vanelli M. WHO declares COVID-19 a pandemic. Acta Biomed. 2020;91(1):157–160. doi:10.23750/abm.v91i1.9397
5. Alabbad AA, Alsaad AK, Al Shaalan MA, Alola S, Albanyan EA. Prevalence of influenza vaccine hesitancy at a tertiary care hospital in Riyadh, Saudi Arabia. J Infect Public Health. 2018;11(4):491–499. doi:10.1016/j.jiph.2017.09.002
6. Aghbash PS, Eslami N, Shirvaliloo M, Baghi HB. Viral coinfections in COVID-19. J Med Virol. 2021;93(9):5310-5322. doi:10.1002/jmv.27102
7. Huang K, Lin SW, Sheng WH, et al. Influenza vaccination and the risk of COVID-19 infection and severe illness in older adults in the United States. Sci Rep. 2021;11(1):11025. doi:10.1038/s41598-021-90068-y
8. Alenazi BR, Hammad SM, Mohamed AE. Prevalence of seasonal influenza vaccination among primary healthcare workers in Arar city, Saudi Arabia. Electron Physician. 2018;10(8):7217–7223. doi:10.19082/7217
9. Grohskopf LA, Sokolow LZ, Broder KR, et al. Prevention and control of seasonal influenza with vaccines: recommendations of the advisory committee on immunization practices–United States, 2017–18 influenza season. MMWR Recomm Rep. 2017;66(RR–2):1–20. doi:10.15585/mmwr.rr6602a1
10. Ministry of Health of the Kingdom of Saudi Arabia. Infection prevention and control guidelines for seasonal influenza in healthcare setting; 2017. Available from: https://www.moh.gov.sa/en/CCC/StaffRegulations/Influenza/Documents/Seasonal-Influenza-IC-guidelines_2017-Updated%2030-11.pdf.
11. Data Management Unit. Influenza-A surveillance 2016, national cumulative report. Ministry of Health of the Kingdom of Saudi Arabia; 2017. Available from: https://www.moh.gov.sa/CCC/healthp/regulations/Documents/ISSA%20Protocol.pdf.
12. Awadalla NJ, Al-Musa HM, Al-Musa KM, et al. Seasonal influenza vaccination among primary health care workers in Southwestern Saudi Arabia. Hum Vaccines Immunother. 2020;16(2):321–326. doi:10.1080/21645515.2019.1666500
13. Schmid P, Rauber D, Betsch C, Lidolt G, Denker ML. Barriers of influenza vaccination intention and behavior: a systematic review of influenza vaccine hesitancy, 2005–2016. PLoS One. 2017;12:e0170550.
14. Hopman CE, Riphagen-Dalhuisen J, Looijmans-van den Akker I. Determination of factors required to increase uptake of influenza vaccination among hospital-based healthcare workers. J Hosp Infect. 2011;77(4):327–331. doi:10.1016/j.jhin.2010.10.009
15. Looijmans-van den Akker I, van Delden JJM, Verheij TJM, et al. Which determinants should be targeted to increase influenza vaccination uptake among health care workers in nursing homes? Vaccine. 2009;27(34):2730–4724. doi:10.1016/j.vaccine.2009.05.013
16. Al Wutayd O, Siddiqui AR, Al-Jasser F, et al. Influenza vaccination hesitancy among health care workers at the tertiary care hospital, Buraydah, Qassim, Saudi Arabia. Aljouf Uni Med J. 2018;5(3):33–39.
17. World Health Organization. Saudi Arabia situation; 2020. Available from: https://covid19.who.int/region/emro/country/sa.
18. Iacobucci G. Covid-19: risk of death more than doubled in people who also had flu, English data show. BMJ. 2020;370:m3720. doi:10.1136/bmj.m3720
19. Fiore AE, Bridges CB, Cox NJ. Seasonal influenza vaccines. Curr Top Microbiol Immunol. 2009;333:43–82. doi:10.1007/978-3-540-92165-3_3
20. Grech V, Borg M. Influenza vaccination in the COVID-19 era. Early Hum Dev. 2020;148:105116. doi:10.1016/j.earlhumdev.2020.105116
21. Della Polla G, Licata F, Angelillo S, Pelullo CP, Bianco A, Angelillo IF. Characteristics of healthcare workers vaccinated against influenza in the era of COVID-19. Vaccines. 2021;9(7):695. doi:10.3390/vaccines9070695
22. Domnich A, Cambiaggi M, Vasco A, et al. Attitudes and beliefs on influenza vaccination during the COVID-19 pandemic: results from a representative Italian Survey. Vaccines. 2020;8(4):711. doi:10.3390/vaccines8040711
23. Wang K, Wong ELY, Ho KF, et al. Intention of nurses to accept coronavirus disease 2019 vaccination and change of intention to accept seasonal influenza vaccination during the coronavirus disease 2019 pandemic: a cross-sectional survey. Vaccine. 2020;38(45):7049–7056. doi:10.1016/j.vaccine.2020.09.021
24. Kelly BJ, Southwell BG, McCormack LA, et al. Predictors of willingness to get a COVID-19 vaccine in the U.S. BMC Infect Dis. 2021;21(1):383. doi:10.1186/s12879-021-06085-9
25. Sturm L, Kasting ML, Head KJ, Hartsock JA, Zimet GD. Influenza vaccination in the time of COVID-19: a national U.S. survey of adults. Vaccine. 2021;39(14):1921–1928. doi:10.1016/j.vaccine.2021.03.003
26. Mereckiene J, Cotter S, Nicoll A, et al.; VENICE Project Gatekeepers Group. Seasonal influenza immunisation in Europe. Overview of recommendations and vaccination coverage for three seasons: pre-pandemic (2008/09), pandemic (2009/10) and post-pandemic (2010/11). Euro Surveill. 2014;19(16):20780. doi:10.2807/1560-7917.ES2014.19.16.20780
27. Di Pumpo M, Vetrugno G, Pascucci D, et al. Is COVID-19 a real incentive for flu vaccination? Let the numbers speak for themselves. Vaccines. 2021;9(3):276. doi:10.3390/vaccines9030276
28. Bish A, Yardley L, Nicoll A, Michie S. Factors associated with uptake of vaccination against pandemic influenza: a systematic review. Vaccines. 2011;29(38):6472–6484. doi:10.1016/j.vaccine.2011.06.107
29. Vision Realization Office. Health Vision. Ministry of Health of the Kingdom of Saudi Arabia; 2021. Available from: https://www.moh.gov.sa/Ministry/vro/Documents/Health-Vision-7.pdf.
30. Bish A, Michie S. Demographic and attitudinal determinants of protective behaviours during a pandemic: a review. Br J Health Psychol. 2010;15(4):797–824. doi:10.1348/135910710x485826.
31. Noh JY, Seong H, Yoon JG, Cheong HJ, Kim WJ. Social distancing against COVID-19: implication for the control of influenza. J Korean Med Sci. 2020;35(19):e182. doi:10.3346/jkms.2020.35.e182
32. Olsen SJ, Azziz-Baumgartner E, Budd AP, et al. Decreased influenza activity during the COVID-19 pandemic–United States, Australia, Chile, and South Africa, 2020. Morb Mortal Wkly Rep. 2020;69(37):1305. doi:10.15585/mmwr.mm6937a6
33. Cowling BJ, Fang VJ, Nishiura H, et al. Increased risk of noninfluenza respiratory virus infections associated with receipt of inactivated influenza vaccine. Clin Infect Dis. 2012;54(12):1778–1783. doi:10.1093/cid/cis307
34. Wolff GG. Influenza vaccination and respiratory virus interference among Department of Defense personnel during the 2017–2018 influenza season. Vaccine. 2020;38(2):350–354. doi:10.1016/j.vaccine.2019.10.005
35. Di Giuseppe G, Pelullo CP, Paolantonio A, Della Polla G, Pavia M. Healthcare workers’ willingness to receive influenza vaccination in the context of the COVID-19 pandemic: a survey in Southern Italy. Vaccines. 2021;9(7):766. doi:10.3390/vaccines9070766
36. Belingheri M, Paladino ME, Latocca R, De Vito G, Riva MA. Association between seasonal flu vaccination and COVID-19 among healthcare workers. Occup Med. 2020;70(9):665–671. doi:10.1093/occmed/kqaa197
37. Esposito S, Bosis S, Pelucchi C, et al. Influenza vaccination among healthcare workers in a multidisciplinary university hospital in Italy. BMC Public Health. 2008;8(1):422. doi:10.1186/1471-2458-8-422
38. Qureshi AM, Hughes NJ, Murphy E, Primrose WR. Factors influencing uptake of influenza vaccination among hospital-based health care workers. Occup Med. 2004;54(3):197–201. doi:10.1093/occmed/kqg087
39. Asma S, Akan H, Uysal Y, et al. Factors effecting influenza vaccination uptake among health care workers: a multi-center cross-sectional study. BMC Infect Dis. 2016;16(1):192. doi:10.1186/s12879-016-1528-9
40. Trivalle C, Okenge E, Hamon B, Taillandier J, Falissard B. Factors that influence influenza vaccination among healthcare workers in a French geriatric hospital. Infect Control Hosp Epidemiol. 2006;27(11):1278–1280. doi:10.1086/508833
41. Pelullo CP, Della Polla G, Napolitano F, Di Giuseppe G, Angelillo IF. Healthcare workers’ knowledge, attitudes, and practices about vaccination: a cross-sectional study in Italy. Vaccines. 2020;8(2):148. doi:10.3390/vaccines8020148
42. Ciblak M, Nohutçu N, Gürbüz İ, Badur S, Güldal D. Aile hekimliğinde grip ve grip aşısı: bilmek uygulama için yeterli mi. Influenza and influenza vaccine in family practice: is knowledge sufficient for practice? Türk Aile Hek Derg. 2012;16(4):157–163.
43. Betsch C. Overcoming healthcare workers’ vaccine refusal – competition between egoism and altruism. Euro Surveill. 2014;19(48):48. doi:10.2807/1560-7917.ES2014.19.48.20979
44. Zvi HA, Orit L. Influenza vaccination among primary healthcare workers. Vaccine. 2008;26(20):2482–2489. doi:10.1016/j.vaccine.2008.03.011
45. Seale H, Macintyre CR. Seasonal influenza vaccination in Australian hospital health care workers: a review. Med J Aust. 2011;195(6):336–338. doi:10.5694/mja11.10067
46. Doratotaj S, Macknin ML, Worley S. A novel approach to improve influenza vaccination rates among health care professionals: a prospective randomized controlled trial. Am J Infect Control. 2008;36(4):301–303. doi:10.1016/j.ajic.2007.10.019
47. Looijmans-van den Akker I, Hulscher ME, Verheij TJ, Riphagen-Dalhuisen J, van Delden JJ, Hak E. How to develop a program to increase influenza vaccine uptake among workers in health care settings? Implement Sci. 2011;6(1):47. doi:10.1186/1748-5908-6-47
48. Looijmans-van den Akker I, van Delden JJ, Verheij TJ, et al. Effects of a multi-faceted program to increase influenza vaccine uptake among health care workers in nursing homes: a cluster randomised controlled trial. Vaccine. 2010;28(31):5086–5092. doi:10.1016/j.vaccine.2010.05.003
49. Heinrich-Morrison K, McLellan S, McGinnes U, et al. An effective strategy for influenza vaccination of healthcare workers in Australia: experience at a large health service without a mandatory policy. BMC Infect Dis. 2015;15(1):42. doi:10.1186/s12879-015-0765-7
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.