")
Back to Journals » International Journal of General Medicine » Volume 13
Trends of Status of Hypertension in Southern China, 2012–2019
Authors Liu L, Chen C , Lo K , Huang J, Yu Y , Huang Y, Feng Y
Received 17 June 2020
Accepted for publication 12 August 2020
Published 14 September 2020 Volume 2020:13 Pages 599—608
DOI https://doi.org/10.2147/IJGM.S267346
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Lin Liu,1,* Chao-lei Chen,1,* Kenneth Lo,2 Jia-yi Huang,1 Yu-ling Yu,1 Yu-qing Huang,1 Ying-qing Feng1
1Department of Cardiology, Guangdong Cardiovascular Institute, Guangdong Provincial Key Laboratory of Coronary Heart Disease Prevention, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, Guangzhou, 510080, People’s Republic of China; 2Centre for Global Cardiometabolic Health, Department of Epidemiology, Brown University, Providence, RI, USA
*These authors contributed equally to this work
Correspondence: Yu-qing Huang; Ying-qing Feng
Department of Cardiology, Guangdong Cardiovascular Institute, Guangdong Provincial Key Laboratory of Coronary Heart Disease Prevention, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, No. 106, Zhongshan Second Road, Yuexiu District, Guangzhou 510080, People’s Republic of China
Tel/Fax +86-20-83827812
Email [email protected]; [email protected]
Purpose: Little is known about the recent trends of hypertension in southern China. The aim of the study was to investigate the trends of hypertension in Guangdong Province between 2012 and 2019.
Methods: We conducted two cross-sectional surveys in 2012 and 2019 in southern China, which included 10,970 and 27,483 participants, respectively, aged 35 to 75 years old using a method of stratified, multistage, and cluster sampling. Hypertension was defined as a mean systolic/diastolic blood pressure (SBP/DBP) ≥ 140/90mmHg, or a self-reported condition, or any pharmacological treatment in the last 2 weeks. In addition, according to the 2017 ACC/AHA guideline for high blood pressure, we estimated the prevalence and control rate of hypertension.
Results: According to the 2010 Chinese guideline, the age-standardized rate of hypertension prevalence was 34.7% in 2012 and 36.9% in 2019 with a slight increase, while the prevalence of prehypertension was stable (14.5% vs 14.3%). Over the period of our study, 45.6% and 60.7% of hypertensive patients knew their diagnosis in 2012 and 2019, and 40.8% and 51.5% were using antihypertensive medications, respectively. The control rates increased from 15.1% to 23.6%. Hypertension prevalence was 64.5% in 2012 and 63.2% in 2019, and the control rate increased from 3.0% to 4.8% during the study period under the 2017 ACC/AHA guideline.
Conclusion: Although the past 7 years have seen some progress in hypertension management, the rates of hypertension awareness, treatment, and control in southern Chinese remained regrettably low, and the prevalence rate was still high.
Keywords: hypertension, prevalence, awareness, treatment, control rate
Introduction
Hypertension and its cardiovascular complications have become a severe global health issue, accounting for nearly half of the cardiovascular morbidity and mortality.1,2 The global prevalence of hypertension was 40% among adults over 25 years of age in 2008, and affected individuals would amount to 1.56 billion by 2025.3 In China, the prevalence of hypertension was reported to increase from 18.8% to 23.2%, according to the Chinese national nutrition and health survey in 2002 and the China Hypertension Survey 2012–2015.4,5 Results from the PEACE (Patient-Centered Evaluative Assessment of Cardiac Event) Million Persons Project (MPP) showed that the age-standardized prevalence of hypertension was 37.2%.6 The presentation of hypertension, however, differs widely in different regions of China due to the great variation in demographic characteristics, cultural behaviors, and lifestyle habits. Hypertension prevalence in southern China, for example, was reported to be lower than that of northern China in a recent meta-analysis.7
Importantly, the rapid economic, social and cultural changes in the past decades in southern China came with improved nutrition and new lifestyle that may result in great burden of chronic diseases such as hypertension. Data from the Guangdong Provincial Chronic Disease Risk Factor Surveillance I (2004) and II (2007) showed that the prevalence of hypertension among Guangdong Province adults were 12.2% and 15.4%, respectively.8 A recent study showed that the prevalence of hypertension among southern China adults was 27.3%, but more detailed epidemiological results were not mentioned.4 Moreover, information on the recent trends of status of hypertension in Southern China is lacking. Therefore, the present study analyzed the trends of hypertension prevalence, awareness, treatment, and control rate along with related risk factors using data from two large-scale representative cross-sectional surveys conducted in 2012 and 2019.
Methods
Study Population
This study included two cross-sectional surveys conducted in southern China in 2012 and 2019, respectively. It was ensured that the samples were representative by using a method of multistage, stratified, and cluster sampling. The surveys were conducted from July 2012 to December 2012, and from January 2019 to August 2019, respectively. Six cities in 2012 and eight cities in 2019 were selected from southern China. Subsequently, by a simple random sampling method, three/four districts were selected within each city in 2012/2019. Thereafter, a total of six communities were randomly selected. All permanent residents aged 35 to 75 years old in these communities were eligible to participate. A total of 10,970 and 27,483 people were enrolled in 2012 and 2019, respectively (Figure 1). The survey protocol was approved by the Guangdong Provincial People’s Hospital (Guangzhou, China). Written informed consent was obtained from all participants.
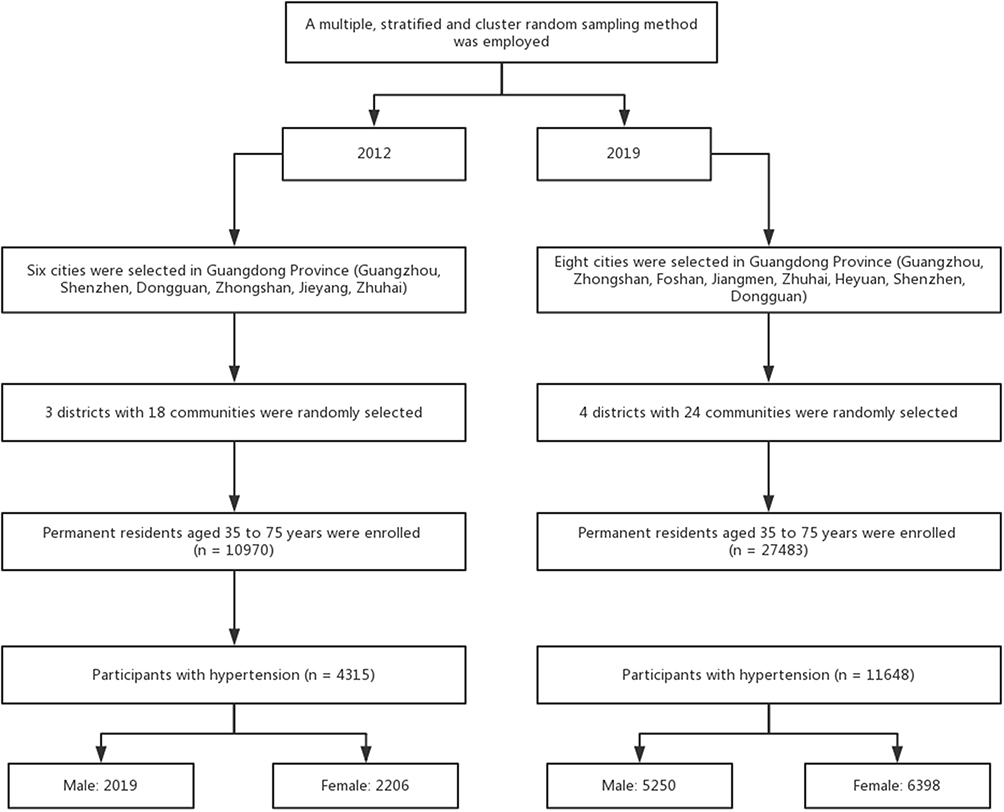 |
Figure 1 Flow chart of study participants. |
Training and Data Collection
Data were collected by investigators who were qualified to conduct this survey after undergoing a training program that oriented them to the methods and process of the study, using a face-to-face interview and a self-administered questionnaire during a single clinic visit. The standardized questionnaire was designed by the coordinating center of Guangdong Provincial People’s Hospital. Demographic characteristics including age, sex, education and lifestyle habits (eg, smoking, drinking) were collected using the above-mentioned questionnaire. Current smokers were defined as participants who currently smoke or have smoked more than 20 packets of cigarettes before the visit. Alcohol drinkers were defined as participants who consumed alcoholic drinks more than once a week in the past year. Physical measurements were taken during the interview, including height, weight and waist circumference (WC), following standard protocols. The participants were required to wear light-weight clothes and no shoes to take the measurements to the nearest 0.1 kg and 0.1 cm. Body mass index (BMI) was defined as the ratio of weight (kg) to the square of height (m2).
Blood Pressure Measurement
For each participant, we measured blood pressure (BP) on the right arm after 5 mins rest in a seated position for three times with a 30 s interval using the OMRON HBP-1300 Professional Portable Blood Pressure Monitor (OMRON, Kyoto, Japan). Three readings were averaged for data analysis. An enquiry was made to every participant during the interview about any use of antihypertensive drugs in the last 2 weeks.
Definitions
In the 2010 Chinese guideline for hypertension management,9 hypertension was defined as a mean systolic blood pressure (SBP) ≥ 140mmHg and/or a mean diastolic blood pressure (DBP) ≥ 90 mmHg, and/or self-report use of antihypertensive medication within 2 weeks. Prehypertension was defined as 120 mmHg ≤ SBP < 140 mmHg and 80 mmHg ≤ DBP < 90 mmHg without self-report use of antihypertensive medication.9 Awareness of hypertension was defined as a self-report of any previous diagnosis of hypertension by a health-care professional. Treatment was defined as self-report prescription for antihypertensive medication within 2 weeks prior to the interview. Control of hypertension was defined as an average SBP <140 mmHg and an average DBP < 90 mmHg over three readings in hypertensive patients. In addition, using criteria of the 2017 American College of Cardiology (ACC)/American Heart Association (AHA) High Blood Pressure Guideline, we recalculated the prevalence of hypertension (defined as SBP ≥ 130 or DBP ≥ 80 mmHg) and control rate (defined as SBP < 130 and DBP < 80 mmHg).10
Overweight was defined as between 24.0 ≤ BMI < 28 kg/m2 and obesity as a BMI ≥ 28.0. Central obesity was defined as WC ≥90 cm in men and ≥85 cm in women, based on the recommendations of defining abdominal obesity in Chinese.11 Trained investigators scanned the questionnaires for future reference, and manually recorded the data twice for each questionnaire to ensure data integrity.
Statistical Analysis
Continuous values were reported as means ± standard (SD) deviation and compared using Student’s t-test, categorical variables were reported as numbers and percentages and compared by the χ2-test. Participants were stratified into 4 groups by age (35–44, 45–54, 55–64, 65–75 years old), and the hypertension prevalence, awareness, treatment and control rates were estimated in each group, respectively. We also estimated the age-standardized rate of hypertension prevalence according to China’s 2010 population census. Moreover, we estimated the prevalence of major risk factors including oldness (age ≥ 60 years), current smoking, alcohol drinking, overweight or obesity, and central obesity in hypertensive patients by sex. Then, we used univariate logistic regression model to explore the risk factors associated with awareness, treatment, and control rates. All P values were two-sided, and the significance level was set at 0.05. All analyses were done with R 3.5.1 (https://cran.r-project.org/mirrors.html).
Results
Characteristics of Study Population
Table 1 shows the basic features of the population in our study. In the 2012 survey, the average age of the 10,970 participants was 53.5 years old (standard error: 11.5 years), of which 46.1% was male (n=5065) and 53.9% was female (n=5905). In the 2019 survey, the average age of the 27,483 participants was 53.8 years old (standard error: 10.3 years), including 39.8% male (n=14,289) and 60.2% female (n=22,087).
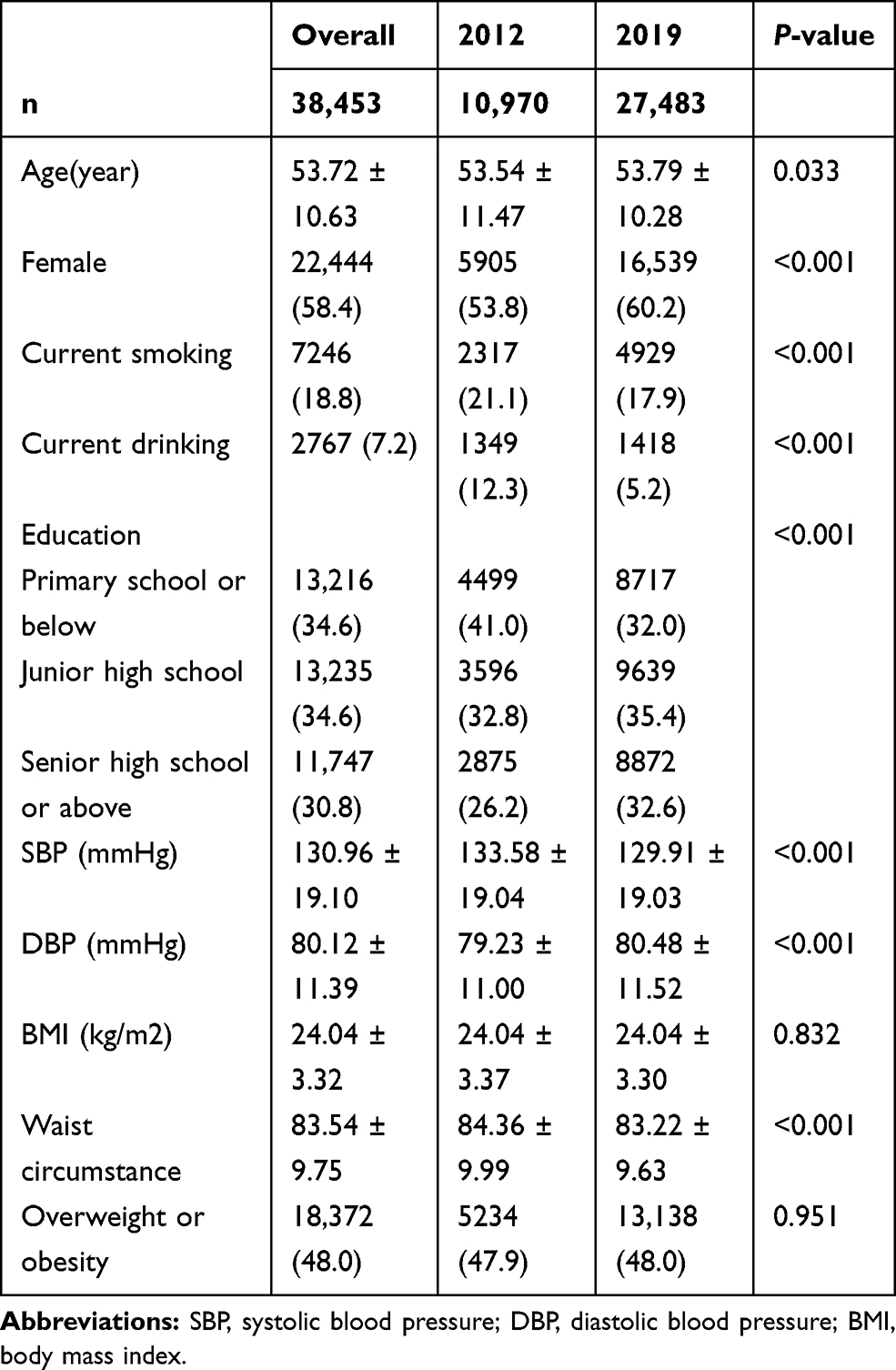 |
Table 1 Demographic Profiles of Participants in 2012 and 2019 |
Prevalence of Prehypertension and Hypertension
According to the 2010 Chinese guideline for hypertension management, 39.3% (4315/10,970) participants had hypertension in 2012, whereas 42.4% (11,653/27,483) participants were diagnosed with hypertension in 2019. The age-standardized prevalence of hypertension was 34.7% [95% confidence interval (CI): 34.1–35.2] and 36.9% (95% CI: 36.5–37.2) in 2012 and 2019, showing an increased trend in men, but evidence was insufficient to support a similar trend in women (37.4% in 2012 vs 43.2% in 2019, P < 0.05 for male; 32.3% in 2012 vs 33.0% in 2019, P > 0.05 for female). Hypertension prevalence was higher in men than that in women in 2012 (37.4 vs 32.3%) and 2019 (43.2 vs 33.0%) (Table 2). In addition, the prevalence of hypertension increased substantially with age in both sexes. The prehypertension prevalence slightly decreased from 14.5% to 14.3% from 2012 to 2019, with a decrease across all age-based subgroups except for female aged 45–54 years old in 2019 (Table 3, Figure S1).
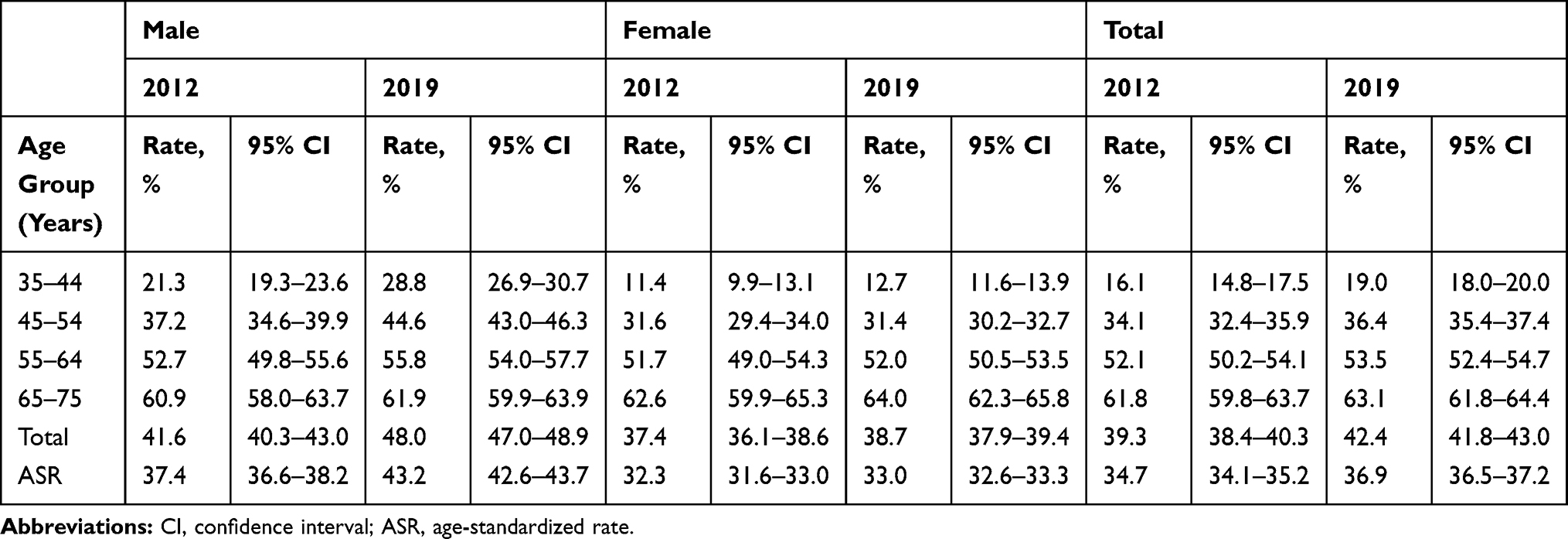 |
Table 2 Prevalence of Hypertension Among Southern Chinese Adults Between 2012 and 2019 According to Sex |
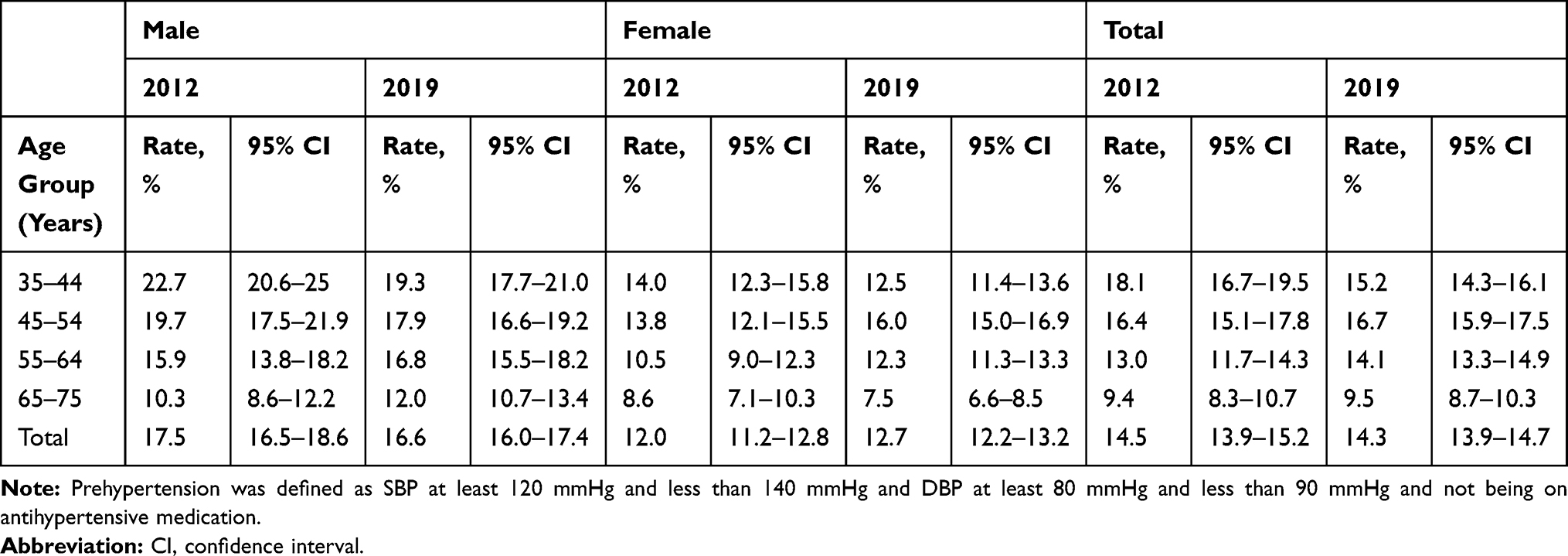 |
Table 3 Distribution of Prehypertension in 2012 and 2019 |
Age and Sex-Specific Distributions of Awareness, Treatment, and Control Rates of Hypertension
During the study period, 45.6% and 60.7% of hypertensive patients knew their diagnosis in 2012 and 2019, and 40.8% and 51.5% were taking antihypertensive drugs, respectively (Figure 2, Table S1); the control rate increased from 15.1% to 23.6% and among patients receiving antihypertensive treatment, 36.9% and 41.4% achieved BP targets, respectively. Overall, the rates of hypertension awareness, control and treatment during this period showed an increased trend which was accompanied with increasing age. Moreover, in 2012, men were more likely to be aware of their diagnosis and to receive medications than women. However, it showed the opposite for awareness and no difference for treatment between the sexes in 2019. The control rate among men became higher than women in 2019 while being similar in 2012.
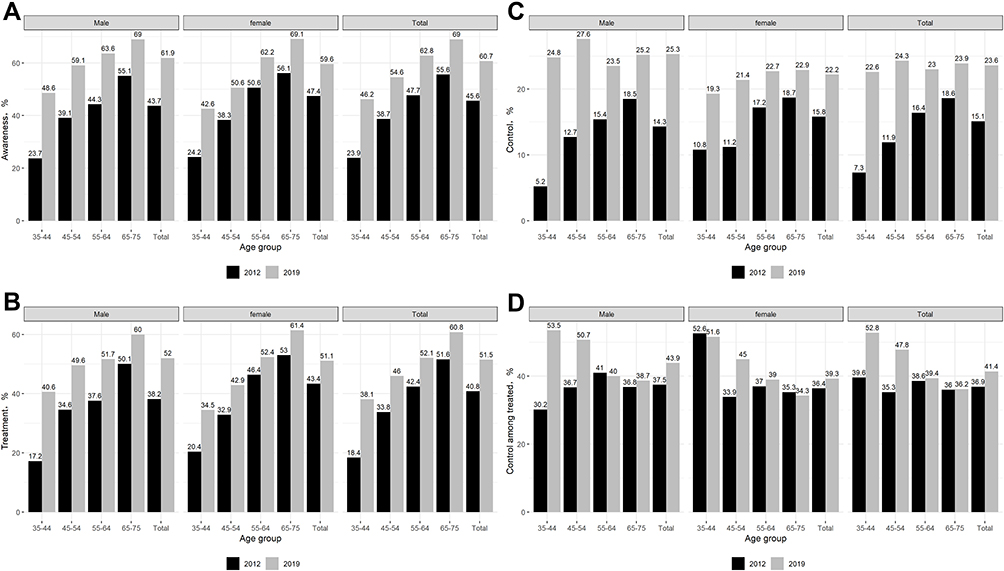 |
Figure 2 Rates of awareness (A), treatment (B), control overall (C) and control in treated patients (D) among southern Chinese classified by age and sex between 2012 and 2019. |
Trends of Related Risk Factors for Hypertension
During the study period, the rates of oldness, current smoking, and current alcohol drinking decreased from 2012 to 2019 (52.7 vs 46.5%, 22.7 vs 19.6%, and 12.8 vs 6.4%, respectively), however, rate of overweight or obesity increased a little from 2012 to 2019 (58.7 vs 59.5%). Men were more likely to be overweight or obesity than women. On the contrary, rate of central obesity decreased from 52.1% to 48.0%. (Table S2).
Risk Factors Associated with Awareness, Treatment and Control Rates
The results from the logistic regression model analyzing factors associated with awareness, treatment, and control rates of hypertension were shown in Table S3. Awareness of hypertension was positively associated with older age, being a man, lower education levels, higher BMI, being a nonsmoker, being a nondrinker, and being central obesity; however, smoking was no longer associated with hypertension awareness in 2019. Factors associated with a higher treatment rate of hypertension were similar while the association with gender and education levels were not significant in 2019. The control rate among participants with central obesity and higher education levels had better control of hypertension in 2019, although all factors of interest were not significantly related with control rate in 2012.
Classification According to the 2017 ACC/AHA Guideline
Based on 2017 ACC/AHA guideline, the prevalence of hypertension was 64.5% and 63.2% in 2012 and 2019, respectively (Figure 3, Table S4). The control rate increased from 3.0% to 4.8% during this period. Only 12.2% and 14.0% became normotensive in 2012 and 2019, respectively, among participants who received antihypertensive treatment. Prevalence of hypertension was higher in males than females, while control rate was lower in the same region, except for the same rate of control between the two sexes in 2019.
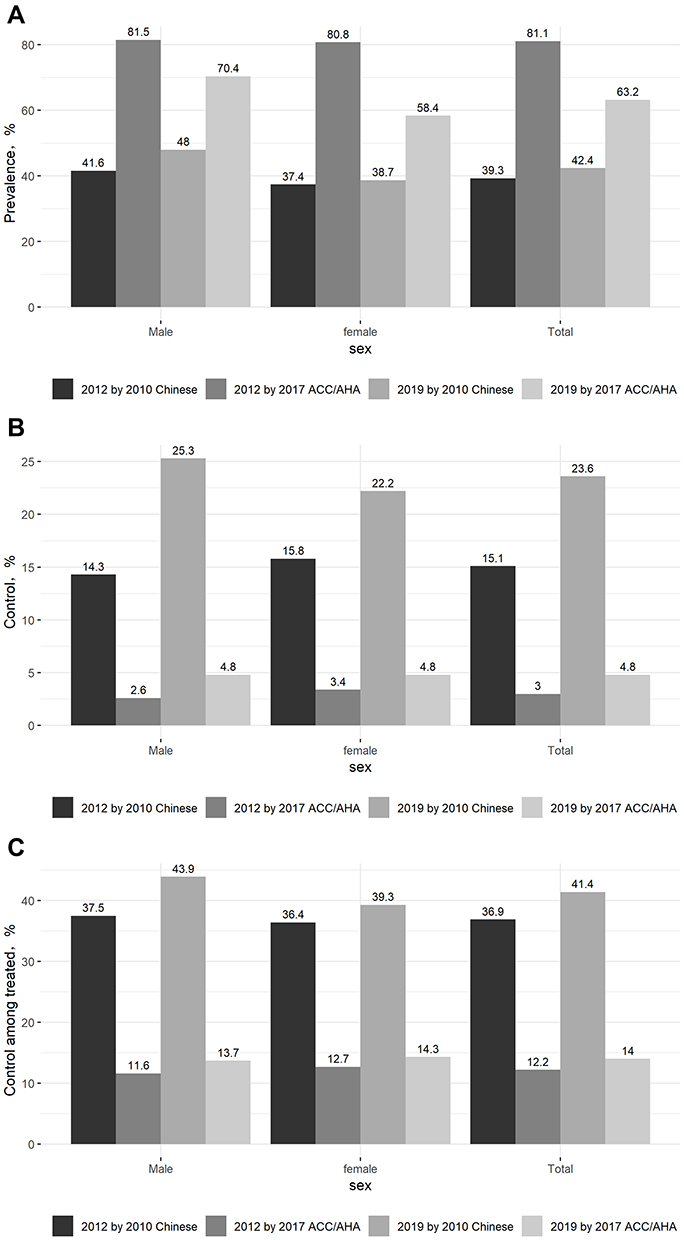 |
Figure 3 The prevalence (A), control rate overall (B), and control rate in patients with antihypertensive medication (C) according to the 2010 Chinese high blood pressure guideline and the 2017 ACC/AHA guideline. |
Discussion
The current study provided comprehensive temporal trends of hypertension status among people aged 35–75 years in Southern China. Overall, hypertension prevalence has slightly increased from 34.7% in 2012 to 36.9% in 2019; moreover, the prevalence of prehypertension during the period was stable at approximately 14%. Notably, hypertension control rate in southern Chinese population was worrying (15.1 vs 23.6%). Drinking, smoking, being overweight or obesity, and central obesity were still major contributing risk factors, leading to further development of hypertension and huge burden of cardiovascular diseases. The prevalence of hypertension increased significantly when classified by the 2017 ACC/AHA guideline (64.5% in 2012 and 63.2% in 2019) while the control rate was unacceptable low control rate (3.0% and 4.8% in 2012 and 2019, respectively). Thus, urgent and comprehensive strategies are needed to delay hypertension development and manage risk factors related to southern Chinese adults.
An increased prevalence of hypertension has been found in recent years in southern China. Actually, the standardized prevalence rate in southern China in 1979 was only 4.7%.12 In 2002, the prevalence of hypertension increased to 20.5%, exceeding the national rate of the same period.13 Recently, the China National Nutrition and Health Survey 2002 (GNHS 2002) revealed that the age-standardized prevalence rates of hypertension in southern China were 15.4% in 2007 and 13.3% in 2010.8,14 The corresponding prevalence in our population was extremely higher (34.7% in 2012 and 36.9% in 2019), a bit lower than the national population aged 35–75 years old in 2017 (37.2%) according to data from the China PEACE Million Persons Project.6 All three studies conducted in southern China with a large Chinese population aged 18 years or 20 years or above, which to some extent explained why the results of this study were much higher than previous studies. On the other hand, Southern China has experienced huge changes in economic development, lifestyle and diet, and an increased in life expectancy in the past decades,15 the prevalence of hypertension has sharply increased and will continue to set at a high level. Moreover, a recent study showed the prevalence of hypertension in northern China was 60.6% in 2018,16 which was much higher than that in southern China and the results were consistent with previous studies.7 Overall, the high prevalence of hypertension is worrying in southern China compared with the Western countries, whose hypertension status are showing a decreasing trend in the past few decades.17,18
It was noteworthy that many prehypertensive population in our survey will be classified as having hypertension based on the 2017 ACC/AHA guideline, which lowered BP standards for the diagnosis of hypertension to 130/80 mmHg.10 The hypertension prevalence in southern China has a nearly 150% increase under the new guideline, which is significantly higher than the national value of China as well as the United States.4,19 Prehypertension was proved to be correlated with elevated risk of organ damage and cardiovascular diseases compared with normotension.20–22 In the Chinese population, it was also be related to higher risk of hypertension and major cardiovascular diseases.23,24 Clearly, urgent attention should be paid to preventing prehypertension, and in people already with prehypertension, comprehensive screening and management strategies are needed. Importantly, the high prevalence of overweight and obesity and higher BMI and central obesity remained to be closely associated with higher hypertension prevalence in southern China. Comprehensive and effective strategies should be carried out to better manage this huge population.
Despite the increasing trend of rates of awareness, treatment, and control of hypertension, they are still significantly lower than that in developed countries.25–27 When compared with different regions of China, the rates were much higher than those of rural northeast China (awareness, treatment, and control rates were 47.5%, 35.4%, and 3.6%, respectively).16 Similarly, in southwestern China, values were 47.9%, 40.1%, and 10.3%, respectively.28 Moreover, the hypertension awareness rate (60.7% in 2019) among adults aged at 35–75 years in southern China was much higher than the national level (44.7%) from 2014 to 2017, while the treatment rate (51.5%) and control rate (23.6%) were both higher than that in the national survey (30.1% and 7.2%, respectively).6 The government has made significant efforts to improve the worsening situation of hypertension in the past few decades, including promoting the development of basic medical care, implementing a basic health insurance plan that covers all residents, and building effective drug system that makes antihypertensive drugs affordable for more people.29 However, there is still a large population who is unable to recognize hypertension and untreated or inadequately treated, which is worrisome.
Although many efforts and progress have been made in the past 7 years, there remains a big gap of hypertension status between southern China and developed and other developing countries.26,30 Previous studies have shown that during the past decades in China, high prevalence of overweight and obesity, low health education, and poor compliance with treatment, significantly affect control of hypertension among low-income populations.31,32 In addition, the reasons why the control rate is still low could be partly explained by three fundamental problems.33,34 First, the simple screening process without subsequent follow-up, further treatment or referral. The second reason for poor control of hypertension lies with the perverse incentives offered within the health system. Finally, the insufficient primary prevention of hypertension. Overall, more strong and effective measures should be taken to reduce the huge burden of hypertension in southern China, as well as all over the country.
The present study included two representative surveys conducted in southern Chinese adults using analogous methods and both have large sample sizes, which constituted a major strength of this study. However, the major limitation of our study was that the relationship between risk factors and hypertension and its related diseases burden was not fully assessed regarding the cross-sectional design. Moreover, the study lacked data on blood tests, such as lipids, fasting blood glucose, all of which would have strengthened the characterization of the participants and reduced the bias on the potentially inaccurate self-reported data. Furthermore, the considerable increase in the number of individuals with hypertension under the new ACC/AHA guideline and subsequent impact on hypertension management in Chinese adults needs to be completely evaluated.
Conclusion
In totality, the prevalence of prehypertension and hypertension in southern China is basically stable, but it is still at a high level between 2012 and 2019. Although the rates of awareness, control, and treatment of hypertension improved significantly, there are still at an extremely low level. The prevalence of hypertension increased significantly while the rate of control decreased sharply based on the new 2017 ACC/AHA guideline. Therefore, hypertension remains to be still a serious public problem, and urgent and aggressive strategies are necessary to improve hypertension control and intervention in the future.
Ethical Statement
Our study was conducted in accordance with the Declaration of Helsinki and approved by the institutional medical ethical committee the Guangdong Provincial People’s Hospital, Guangzhou, China. The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Written informed consent was obtained from all participants.
Acknowledgments
We thank all the participants in this survey.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Naghavi M, Abajobir AA, Abbafati C; GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the global burden of disease study 2016. Lancet. 2017;390(10100):1151–1210. doi:10.1016/S0140-6736(17)32152-9
2. GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the global burden of disease study 2013. Lancet. 2015;385(9963):117–171. doi:10.1016/S0140-6736(14)61682-2
3. Kearney PM, Whelton M, Reynolds K, et al. Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365(9455):217–223. doi:10.1016/S0140-6736(05)17741-1
4. Wang Z, Chen Z, Zhang L, et al. Status of hypertension in China: results from the China hypertension survey, 2012–2015. Circulation. 2018;137(22):2344–2356. doi:10.1161/CIRCULATIONAHA.117.032380
5. Li-Ming LI, Rao KQ, Kong LZ, et al. A description on the Chinese national nutrition and health survey in 2002. Chin J Epidemiol. 2005;26(7):478.
6. Lu J, Lu Y, Wang X, et al. Prevalence, awareness, treatment, and control of hypertension in China: data from 1.7 million adults in a population-based screening study (China PEACE Million Persons Project). Lancet. 2017;390(10112):2549–2558. doi:10.1016/S0140-6736(17)32478-9
7. Wang X, Bots ML, Yang F, et al. Prevalence of hypertension in China: a systematic review and meta-regression analysis of trends and regional differences. J Hypertens. 2014;32(10):1919–1927. doi:10.1097/HJH.0000000000000252
8. Xu B, Xu Z, Xu X, et al. Prevalence, awareness, treatment, and control of hypertension among residents in Guangdong Province, China, 2004 to 2007. Circ Cardiovasc Qual Outcomes. 2013;6(2):217–222. doi:10.1161/CIRCOUTCOMES.111.000062
9. Liu LS. [2010 Chinese guidelines for the management of hypertension]. Zhonghua Xin Xue Guan Bing Za Zhi. 2011;39(7):579–615. Chinese.
10. Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. J Am Coll Cardiol. 2018;71(19):e127–e248. doi:10.1016/j.jacc.2017.11.006
11. Weng J, Ji L, Jia W, et al. Standards of care for type 2 diabetes in China. Diabetes Metab Res Rev. 2016;32(5):442–458. doi:10.1002/dmrr.2827
12. Rao XXCR, Mai JZ. Recent trend of hypertension in Guangdong Province. South China J Cardiol. 1996;2:1–3.
13. Ma WJ, Tang JL, Zhang YH, et al. Hypertension prevalence, awareness, treatment, control, and associated factors in adults in southern China. Am J Hypertens. 2012;25(5):590–596. doi:10.1038/ajh.2012.11
14. Lao XQ, Xu YJ, Wong MC, et al. Hypertension prevalence, awareness, treatment, control and associated factors in a developing southern Chinese population: analysis of serial cross-sectional health survey data 2002–2010. Am J Hypertens. 2013;26(11):1335–1345. doi:10.1093/ajh/hpt111
15. Ma WJ, Nie SP, Xu YJ, et al. Risk factors related to hypertension in Guangdong Province. South China J Prev Med. 2003;29:25–27.
16. Xing L, Liu S, Tian Y, et al. Trends in status of hypertension in rural northeast China: results from two representative cross-sectional surveys, 2013–2018. J Hypertens. 2019;37(8):1596–1605. doi:10.1097/HJH.0000000000002076
17. Redondo A, Benach J, Subirana I, et al. Trends in the prevalence, awareness, treatment, and control of cardiovascular risk factors across educational level in the 1995–2005 period. Ann Epidemiol. 2011;21(8):555–563. doi:10.1016/j.annepidem.2011.02.008
18. Burt VL, Cutler JA, Higgins M, et al. Trends in the prevalence, awareness, treatment, and control of hypertension in the adult US population. Data from the health examination surveys, 1960 to 1991. Hypertension. 1995;26(1):60–69. doi:10.1161/01.HYP.26.1.60
19. Khera R, Lu Y, Lu J, et al. Impact of 2017 ACC/AHA guidelines on prevalence of hypertension and eligibility for antihypertensive treatment in United States and China: nationally representative cross sectional study. BMJ. 2018;362:k2357. doi:10.1136/bmj.k2357
20. Rahman M, Zaman MM, Islam JY, et al. Prevalence, treatment patterns, and risk factors of hypertension and pre-hypertension among Bangladeshi adults. J Hum Hypertens. 2018;32(5):334–348. doi:10.1038/s41371-017-0018-x
21. Piaditis G, Markou A, Papanastasiou L, et al. Progress in aldosteronism: a review of the prevalence of primary aldosteronism in pre-hypertension and hypertension. Eur J Endocrinol. 2015;172(5):R191–203. doi:10.1530/EJE-14-0537
22. Natali A, Muscelli E, Casolaro A, et al. Metabolic characteristics of prehypertension: role of classification criteria and gender. J Hypertens. 2009;27(12):2394–2402. doi:10.1097/HJH.0b013e3283316c31
23. Yu D, Huang J, Hu D, et al. Association between prehypertension and clustering of cardiovascular disease risk factors among Chinese adults. J Cardiovasc Pharmacol. 2009;53(5):388–400. doi:10.1097/FJC.0b013e3181a02238
24. Gu D, Chen J, Wu X, et al. Prehypertension and risk of cardiovascular disease in Chinese adults. J Hypertens. 2009;27(4):721–729. doi:10.1097/HJH.0b013e328323ad89
25. Zhang Y, Moran AE. Trends in the prevalence, awareness, treatment, and control of hypertension among young adults in the United States, 1999 to 2014. Hypertension. 2017;70(4):736–742. doi:10.1161/HYPERTENSIONAHA.117.09801
26. Joffres M, Falaschetti E, Gillespie C, et al. Hypertension prevalence, awareness, treatment and control in national surveys from England, the USA and Canada, and correlation with stroke and ischaemic heart disease mortality: a cross-sectional study. BMJ Open. 2013;3(8):e003423. doi:10.1136/bmjopen-2013-003423
27. Egan BM, Zhao Y, Axon RN. US trends in prevalence, awareness, treatment, and control of hypertension, 1988–2008. JAMA. 2010;303(20):2043–2050. doi:10.1001/jama.2010.650
28. Huang XB, Zhang Y, Wang TD, et al. Prevalence, awareness, treatment, and control of hypertension in southwestern China. Sci Rep. 2019;9(1):19098. doi:10.1038/s41598-019-55438-7
29. Liu X, Gu W, Li Z, et al. Hypertension prevalence, awareness, treatment, control, and associated factors in Southwest China: an update. J Hypertens. 2017;35(3):637–644. doi:10.1097/HJH.0000000000001203
30. Joshi SR, Shah SN. Control of blood pressure in India: rule of halves still very much valid. J Assoc Physicians India. 2003;51:151–152.
31. Huang G, Xu JB, Liu Y, et al. Temporal trends in prevalence, awareness, treatment, and control of hypertension from 2000 to 2010 in Chengdu, China. Sci Rep. 2017;7(1):8964. doi:10.1038/s41598-017-09579-2
32. Jiang XJ, Liu ZL, She Q, et al. Blood pressure control rate and associated risk factors in hospitals of different grades in Chongqing, China. Int J Cardiol. 2014;176(3):800–804. doi:10.1016/j.ijcard.2014.07.263
33. Su M, Zhang Q, Bai X, et al. Availability, cost, and prescription patterns of antihypertensive medications in primary health care in China: a nationwide cross-sectional survey. Lancet. 2017;390(10112):2559–2568. doi:10.1016/S0140-6736(17)32476-5
34. Hesketh T, Zhou X. Hypertension in China: the gap between policy and practice. Lancet. 2017;390(10112):2529–2530. doi:10.1016/S0140-6736(17)32743-5
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.