")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Trends in the Cost of Medicines, Consultation Fees and Clinic Visits in Malaysia’s Private Primary Healthcare System: Employer Health Insurance Coverage
Authors Zin CS , Ab Rahman NS , Mohamed Nazar NI, Kurdi A , Godman B
Received 14 April 2023
Accepted for publication 8 June 2023
Published 17 June 2023 Volume 2023:16 Pages 1683—1697
DOI https://doi.org/10.2147/JMDH.S403589
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Che Suraya Zin,1 Norny Syafinaz Ab Rahman,1 Nor Ilyani Mohamed Nazar,1 Amanj Kurdi,2,3,5 Brian Godman2,4,5
1Big Data Research Group, Kulliyyah of Pharmacy, International Islamic University Malaysia, Kuantan, Pahang, Malaysia; 2Strathclyde Institute of Pharmacy and Biomedical Sciences, University of Strathclyde, Glasgow, UK; 3Department of Pharmacology and Toxicology, College of Pharmacy, Hawler Medical University, Erbil, Kurdistan Region Government, Iraq; 4Centre of Medical and Bio-Allied Health Sciences Research, Ajman University, Ajman, United Arab Emirates; 5Division of Public Health Pharmacy and Management, School of Pharmacy, Sefako Makgatho Health Sciences University, Ga-Rankuwa, South Africa
Correspondence: Che Suraya Zin, Big Data Research Group, Kulliyyah of Pharmacy, International Islamic University Malaysia, Kuantan, Pahang, Malaysia, Tel +6 09 570 4909, Email [email protected]
Objective: To examine trends in the cost of medicines, consultation fees and clinic visits among the employees covered by the employer health insurance in Malaysia’s private primary healthcare system in Malaysia.
Designs: Retrospective cross-sectional study.
Setting: PMCare claims database from January 2016 to August 2019.
Participants: A total of 83,556 outpatient clinic visits involving 10,150 IIUM employees of the International Islamic University Malaysia (IIUM) to private general practitioners (GPs). During the study period, IIUM adopts the incentive structure of capping coverage at Ringgit Malaysia (RM) 45/outpatient visit (USD 10.58) to cover for consultation fees and medicine costs.
Main Outcome Measures: The monthly percentage change in the number of clinic visits, medicine costs, consultation fees and total costs between January 2016 and August 2019. A simple linear regression using Stata v15.1 was also performed to measure the association between the characteristics of the prescribed medicines and medicine charges.
Results: The number of clinic visits per patient increased by 17% from January 2016 to August 2019, with consultation fees increasing by 113.9% and total costs by 7.9% per clinic visit per patient. Conversely, the cost of medicines and the number of medicines prescribed per clinic visit per patient decreased by 39.7% and 6.3%, respectively.
Conclusion: Within the incentive structure of capping the total amount of coverage per clinic visit, medicine costs were reduced by decreasing the number of medicines prescribed, to offset the increased consultation fees. This may create perverse incentives that affect medicine use with negative consequences for the health system and health insurers.
Keywords: medicine costs, employer health insurance, incentive structure, private health system Malaysia, quality targets
Plain Language Summary
- This study is among the pioneering ones that examine the medicine use and costs associated with outpatient clinic visits to general practitioners (GPs) covered by employer health insurance.
- The use of patient-level data to identify the effect of insurance structure that caps the total amount per clinic visit on patient access to medicines and health systems is a strength.
- The implications of the present study’s findings extend to similar contexts concerning medicine use and costs within insurance coverage and healthcare settings. This pattern bears similarity to practices observed in other countries, including Vietnam, Ghana, United Kingdom and Iran.
- This study was conducted among private health clinics and therefore cannot be applied to other settings such as community pharmacies and public primary health clinics.
Introduction
Drug pricing, hence access and affordability, is a vital and critical issue for any country, including developed and developing countries, and a major contributor to high healthcare costs.1,2 We have seen that in low- and middle-income countries expenditure on medicines can account for up to 60% of total healthcare expenditure and can be catastrophic for some families, especially in countries with high co-payment levels as well as those seeking to implement universal healthcare.3–5 Vietnam, as an example, has encountered numerous challenges in its pursuit of achieving universal health coverage. The majority of the population exhibits significant reluctance to pay for healthcare services that amount to or exceed VND2 million (approximately US$90).6 Consequently, the government’s ambitious goal of achieving universal coverage appears to be both unrealistic and challenging to attain.7
Even in high-income countries, the cost of medicines is growing with the launch of new medicines for cancer and orphan diseases at ever-increasing prices, with expenditure on these medicines for complex, chronic and rare diseases likely to reach 50% of total medicine expenditure in developed countries by the end of 2023.8–10 In Malaysia, healthcare expenditure is increasing in recent years, which is a major challenge for the Malaysian government.11 In the latest Malaysian statistics on medicines published in February 2020, drug expenditure for 2015–2016 increased by 2.3% from RM 5.2 billion [USD 1.19 billion] in 2015 to RM 5.3 billion [USD 1.22 billion] in 2016.12 In the 2021 budget, the Ministry of Health Malaysia allocated RM 31.9 billion [USD 7.34 billion] to cover total health expenditures including COVID-19 related issues.13 The overall health expenditure has been estimated to account for 82% of total public expenditure in Malaysia.14 The increase in healthcare costs has been mainly attributed to an increase in the overall cost of medicines, the use of medicines and more public health programmes.15 For instance, the overall prevalence of diabetes among the population of Malaysia is 16.8% and growing, higher in some areas, with a corresponding impact on the costs of medicines and healthcare including the cost of complications.16
In Malaysia, the private health system is not under governmental drug pricing regulations but completely determined by free market forces. We see a similar situation in other countries with more liberal pricing systems among private health insurance companies.17,18 This has permitted manufacturers, wholesalers, and healthcare providers in the private sector in Malaysia to sell medicines at unregulated prices,19 generally leading to higher costs with high markups and profit margins.20–22 Research conducted in Iran comparing private and public health systems has also revealed a similar situation indicating that physicians tend to employ more costly practices when treating private patients compared to their approach with public patients.23
In the Malaysian primary private health system, general practitioners (GPs) are allowed to prescribe and sell medicine because there is no regulation that separates prescribing and dispensing, which facilitates the above practice. Similar situations can be observed in other nations, like Ghana, where the inadequate distinction between prescribing and dispensing medications within the private healthcare system brings about adverse consequences. Providers who both prescribe and dispense medicines or own pharmacies tend to engage in excessive prescribing. This context can also foster a phenomenon known as supplier induced demand, wherein the increased utilization of expensive and unsuitable medications occurs, while limiting the number of prescriptions that reach private pharmacies.24
A comparable scenario can be observed in the United Kingdom as well, where doctors practicing dispensing have shown a correlation between the number of patients they dispense medication to and the likelihood of prescribing expensive alternatives25 This finding has significant implications beyond just dispensing practices, as it reveals that clinical decision-making may not be solely motivated by patient requirements. It suggests that financial factors for doctors may contribute to unwarranted variations in care, highlighting the influence of financial considerations on medical decisions.
The private sector requires patients to pay for services out-of-pocket because this sector is not subsidized. However, there are employer health benefit schemes for some employees accessing the private sector, which are funded by non-profit institutions, private health insurance, and private institutions.26 Examples of such institutions include private universities and private corporations. Some public agencies also provide their employees with private insurance. This can be welcomed in view of the long waiting times that can be experienced by patients seeking to access ambulatory care within the public healthcare system in Malaysia.27,28 Arrangements for this type of health insurance are made by employers with insurance providers to offer medical care for their employees through panel medical clinics affiliated with insurance companies. Knowing that their basic health and well-being are being taken care of ensures that employees are fully focused on their daily tasks and contribute to the overall success of employer’s business.29
The coverage of medical care within different insurance companies in Malaysia depends on the insurance structure including coverage for outpatient, dental, or inpatient treatment. Some employers cap expenditure coverage per clinic visit and some cap according to annual medical utilization under their insurance structure. Under such arrangements, employees are not required to pay for the service rendered if the amount is within the approved limit because it will be covered by the insurance company. However, out-of-pocket payments are needed if the total amount exceeds the current coverage amount per visit.
In Vietnam, high costs associated with out-of-pocket expenses are one of the primary issues despite having insurance coverage.30 A large group of patients, who are non-residents, impoverished, and lacking adequate insurance coverage, face a very high likelihood of falling into destitution, estimated at around 70%. Additionally, there is a 58% probability that seriously ill low-income patients, burdened with increased healthcare expenses, may discontinue their treatment.31 Previous studies have evaluated medicine use and cost mainly among private retail pharmacies where patients pay out-of-pocket.19 We are currently unaware of any study conducted among private health clinics regarding medicine use and costs. However, we are aware that there can be differences in care provided between ambulatory care physicians in the public versus private sectors, especially the management of viral infectious diseases exacerbated by patient expectations.32 It is also unclear on how medicines are used and how much they cost in private medical clinics. Also, it is uncertain what effects the incentive structures of employer health benefit scheme have on medical consultation fees and medicine charges at panel clinics in Malaysia. We have seen differences in prescribing behaviour in other countries between the same physicians working in both sections again driven by issues such as patient expectations and incentive systems.33 Consequently, we wanted to study such issues further in Malaysia to provide future direction. As a result, this study sought to evaluate the trends in medicine costs, consultation fees, and the total costs per clinic visit to GP among employees covered by the incentive structure of employer health insurance. Also, to examine the potential influences of incentive structure on the aforementioned parameters as well as the number of medicines and the number of tablets prescribed per clinic visit.
Methods
Study Design and Setting
This retrospective cross-sectional study used PMCare claims data covering the period from January 2016 to August 2019. PMCare is an insurance company that manages and administers the International Islamic University Malaysia (IIUM) medical benefit scheme. It has approximately 650,000 members with approximately 2000 medical providers affiliated with PMCare throughout Malaysia.34 IIUM is a public university that was established in 1983 and has approximately 27,000 students from across the world.35 IIUM adopts the incentive structure of capping coverage at Ringgit Malaysia (RM) 45/outpatient visit (USD 10.58) to cover for consultation fees and medicine costs. This cap has been in place throughout the study period. IIUM panel private medical clinics provide outpatient services to IIUM community without any charges if the amount is less than RM 45 [USD 10.68] per outpatient clinic visit. Any coverage in excess of this amount must be paid out-of-pocket.
The study subjects were IIUM community members (employees and dependents). Dependents refer to children and spouses of employees of IIUM. All IIUM community members seeking outpatient treatment from IIUM panel medical clinics serviced by GPs during the study period were included. There were 1668 panel medical clinics visits included in this study. The extracted data from the PMCare claims database included claim codes, dates of clinic visit, patient codes, medicine costs, consultation fees, total costs, medicine names and doses, the treatment duration, and the number of tablets prescribed. Clinic visits without a charge for consultation fees were excluded because this is likely for patients taking medications only without having to see a GP.
Patient’s age, gender, and diagnoses were also recorded. Patients’ ages were calculated according to the date of the first visit included in the database. Missing information or incomplete data for variables such as claims codes and drug prices were excluded from the analysis. Overall, though, less than 0.5% of observations with incomplete data or extreme values, ie, more than two times of the 99th percentile value, were subsequently excluded from the analysis (Figure 1). This study used the term “patients” to refer to IIUM community (employees and their dependents).
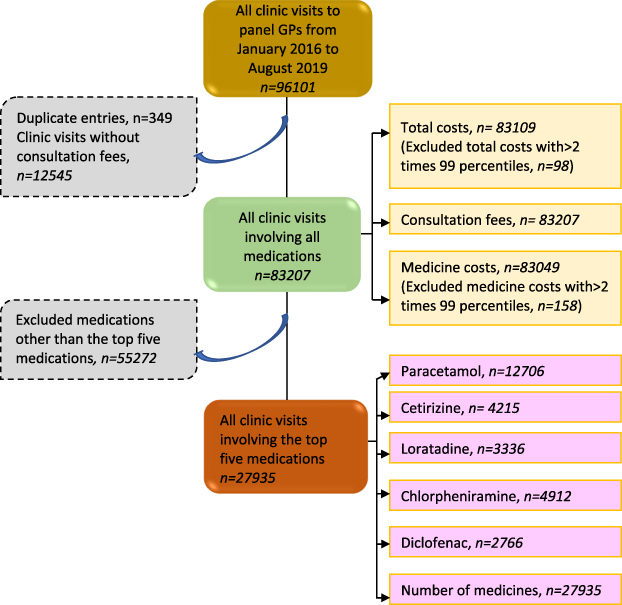 |
Figure 1 Cohort flow chart. Abbreviations: GPs, general practitioners; n, number. |
Outcome Measures
The total number of clinic visits and the number of clinics visit per patient were calculated monthly. The mean medicine costs, GP consultation fees, and total costs (medicine costs plus consultation fees) for each clinic visit per patient per month were also measured. The number of medicines prescribed for each patient per clinic visit per month was recorded. To evaluate whether the above cost is influenced by the quantity prescribed for each medicine within the employer coverage, this study included as examples the five most common prescribed medicines, namely paracetamol, loratadine, cetirizine, diclofenac, and chlorpheniramine. Detailed identification of these five common medicines can be found from our previous work.36 Only tablet formulations of these medicine were included. The number of tablets prescribed to each patient per clinic visit was calculated monthly.
Data Analysis
Descriptive statistics such as percentages and numbers for categorical variables or the mean ± SD for continuous variables were used to describe patient characteristics and outcome measures, as appropriate. These included the total number of clinic visits and number of clinic visits per patient. The percentage change between January 2016 and August 2019 was calculated for medicine costs, consultation fees, total costs, number of clinic visits, as well as the number of medicines and tablets prescribed. A linear trend analysis of these variables was performed over the years of the study period to assess the changes in trends of these variables. Data for total costs were not normally distributed; consequently, they were log transformed for analysis.
A simple linear regression was also used to measure the association between the characteristics of the prescribed medicines, ie the number of medicines and the number of tablets for paracetamol, loratadine, cetirizine, diclofenac, chlorpheniramine, alongside medicine charges. The medicine characteristics were the independent variables, and the medicine charges were the dependent variable. Regression coefficients and 95% confidence intervals (CIs) were used to present the results. These were considered statistically significant for a p-value <0.05. All analyses were performed using Stata version 15.3 (StataCorp, College Station, TX USA).37
Results
Patients and Clinic Visits
A total of 83,207 outpatient clinic visits were made by 10,356 IIUM community members (34% employees and 66% dependents) during the study period. Female patients comprised 48.97% of the total members (n = 5071), and the mean age of all patients was 26.33 ± 17.63 years. Female patients were slightly older than their male counterparts (26.32 ± 16.81 years vs 25.94 ± 17.370 years, Table 1).
 |
Table 1 Patient Demographics |
The number of clinic visits per patient per month increased by 17% from 1.41 visits in January 2016 to 1.65 visits in August 2019 (Figure 2). A linear trend analysis revealed that the number of clinic visits per patient increased significantly (p=0.046) over the study period (Table 2). The five most common diagnoses that were associated with clinic visits among all IIUM community, not only based on patients prescribed with five common drugs (used as examples for the analysis of number of medicines and number of tablets), included acute upper respiratory infections (39%), dermatitis and eczema (6.42%), infectious gastroenteritis and colitis (5.18%), acute tonsillitis (3.42%), and gastritis (3.01%).
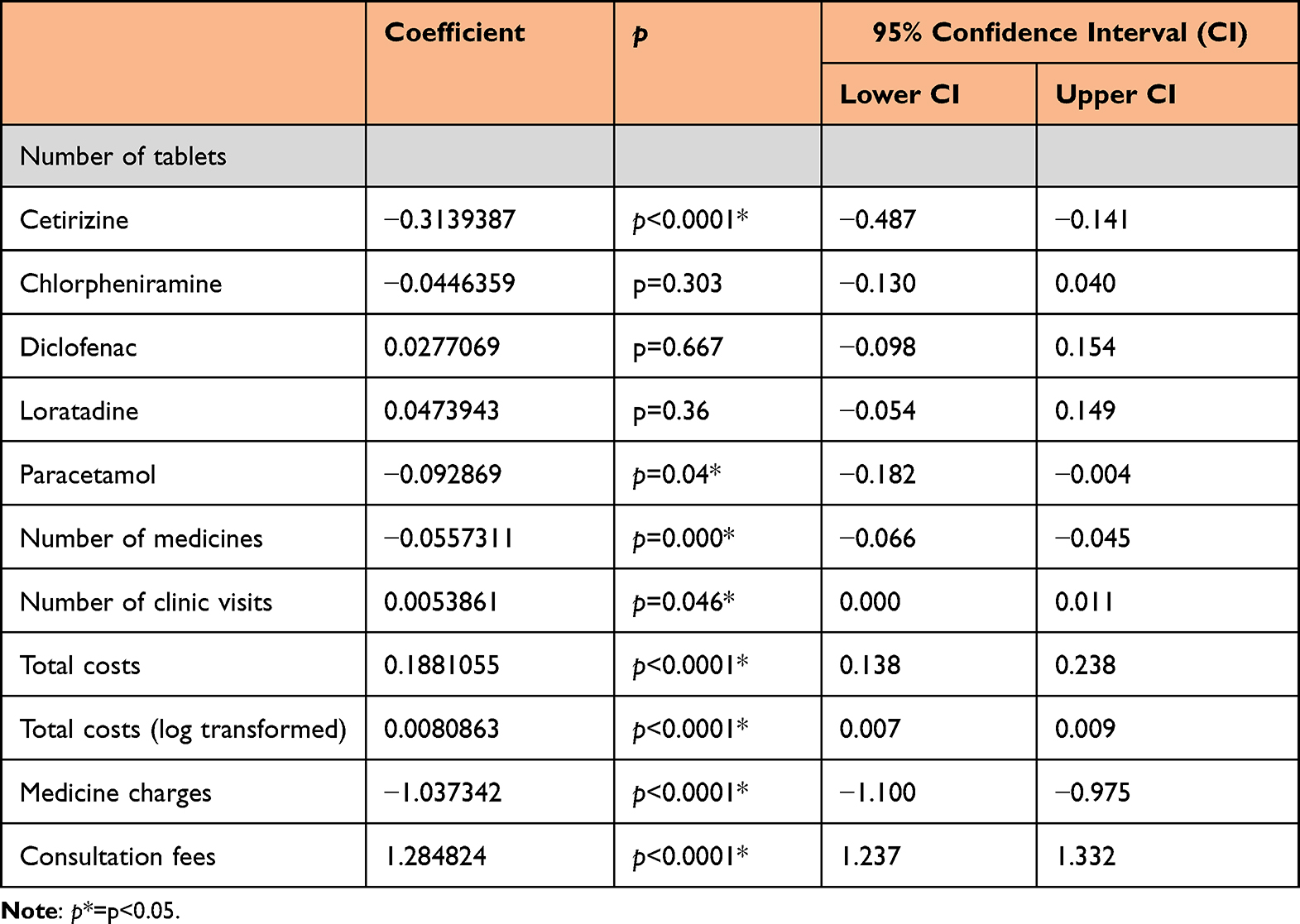 |
Table 2 Results of Linear Trend Analysis of All Variables Over Years of Study Period |
 |
Figure 2 Number of clinic visits and number of drugs per patient per clinic visit. |
Medicine Costs, GP Consultation Fees, and Total Costs
The mean medicine costs per clinic visit per patient decreased from RM 34.61 in January 2016 to RM 20.85 in August 2019 (a decrease, −39.75%, Table 3). The decreasing trend for medicine costs was first observed in late 2018. Conversely, the mean consultation fees per clinic visit per patient increased from RM 10.65 in January 2016 to RM 22.78 in August 2019 (an increase, 113.9%). Similarly, there was a slight increase in the mean total costs per clinic visit from RM 39.66 in January 2016 to RM 42.47 in August 2019 (an increase, 7.89%, Figure 3). Result from a linear trend analysis showed that there was significant decrease in medicine costs (p<0.0001) and total cost (p<0.0001), while increasing in consultation fees (p<0.0001) over the study period was also significant (Table 2).
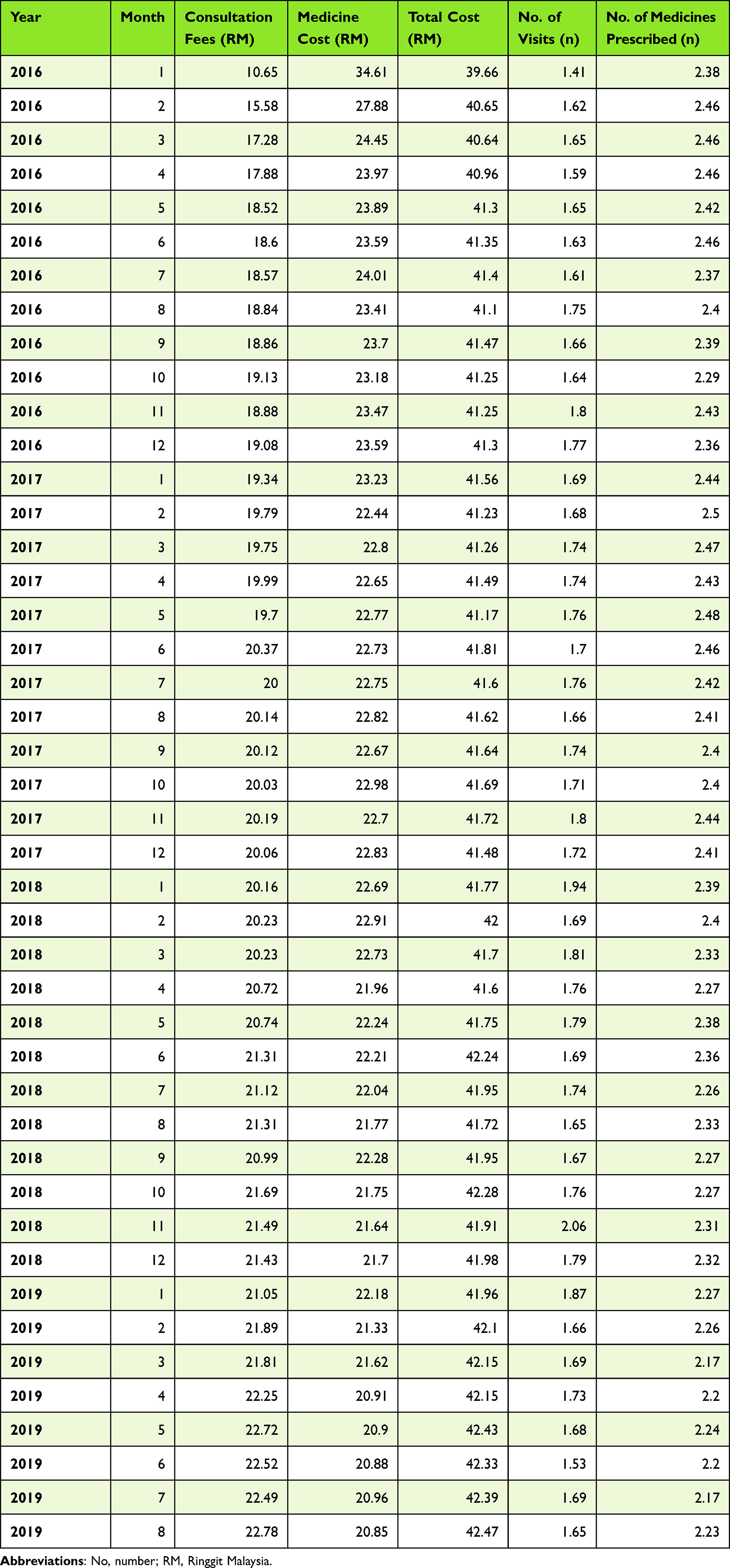 |
Table 3 Mean Cost of Consultation Fees, Medicines, Total and Mean Number of Clinic Visits and Prescribed Medicines per Patient per Clinic Visit |
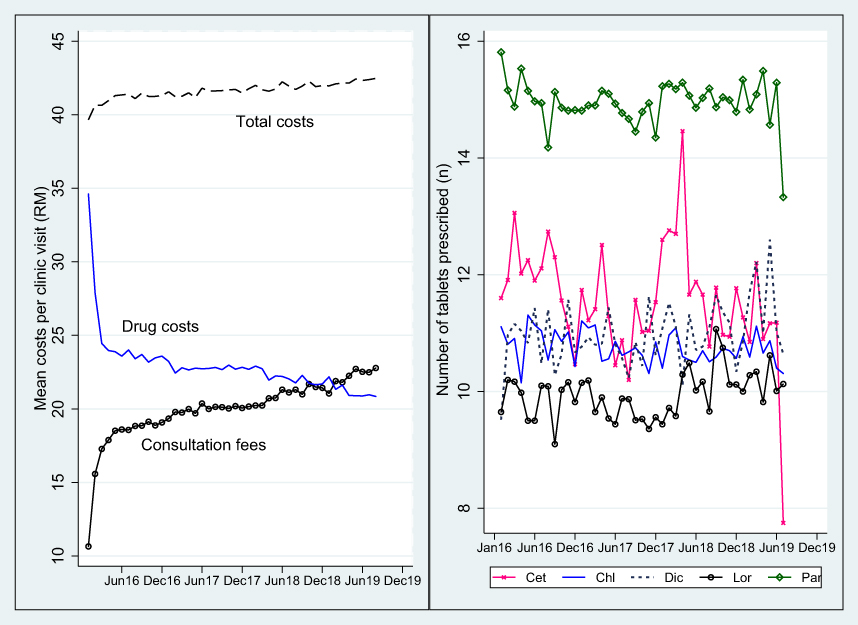 |
Figure 3 Mean drug charges, consultation fees, total charges and number of tablets prescribed per patient per clinic visit. |
Numbers of Medicines and Tablets Prescribed
The mean number of medicines prescribed per clinic visit per patient slightly decreased from 2.38 drugs in January 2016 to 2.23 drugs in August 2019 (a decrease, −6.30%, Figure 1). During the study period, the mean numbers of tablets of cetirizine (11.6 tablets in January 2016 vs 7.75 tablets in August 2019, a decrease, −33.18%), chlorpheniramine (11.11 tablets in January 2016 vs 10.31 tablets in August 2019, a decrease, −7.2%), and paracetamol (15.81 tablets in January 2016 vs 13.33 tablets in August 2019, a decrease, −15.68%) prescribed per patient per clinic visit modestly decreased over time. Contrarily, there were slight increases in the number of tablets prescribed per patient per clinic visit for diclofenac (9.52 tablets in January 2016 vs 10.64 tablets in August 2019, an increase, 11.47%) and loratadine (9.65 tablets in January 2016 vs 10.13 tablets in August 2019, an increase, 4.97%, Figure 2). A linear trend analysis showed that decreasing the number of medicines (p<0.0001), decreasing tablet cetirizine (p<0.0001) and paracetamol (p=0.04) over study period were significant, while other medicines were non-significant (Table 2).
The simple linear regression analysis showed that increasing number of medicines prescribed (coefficient, 4.488, 95% CI 4.412, 4.565 p<0.0001), increasing tablets of cetirizine (coefficient 0.130, 95% CI 0.094, 0.166 p<0.0001), chlorpheniramine (coefficient 0.066, 95% CI 0.0003-, 0.132 p=0.049), diclofenac (coefficient 0.095, 95% CI 0.013, 0.177 p=0.023), loratadine (coefficient 0.235, 95% CI 0.156, 0.313 p<0.0001) and paracetamol (coefficient 0.066, 95% CI 0.040, 0.091 p<0.0001) were all associated with increasing overall medicine charges.
Discussion
This study discussed the trends of medicine costs, consultation fees, and clinic visits, as well as the effects of the incentive structure of employer health insurance on patient-prescribed drugs and their related costs in the private primary healthcare system. Overall, the cost of medicines decreased over the study period, whereas consultation fees and total costs per clinic visit increased. From the perspective of expenditure on medicines, decreased drug spending is desired, but whether the trade-off between decreasing drug costs and increasing consultation fees reduces patient access to prescription drugs must be clarified to ensure optimal patient care. Since this study evaluated the prescribed medicines and associated costs within the coverage of employer health insurance, it is difficult to compare these findings directly with those of other studies, which typically reported employer drug benefit plans, changes in employer sponsored health insurance and employee preference for health insurance.38–40 These studies found that increasing co-payments or coinsurance rates, as well as requiring mandatory generic substitution, all reduced plan payments and overall drug spending among working-age enrollees with employer-provided drug coverage.38 The majority of private insurance plans, which are employer-sponsored, are becoming more expensive for the elderly and provide less comprehensive coverage, with coverage availability also limited.39 Overall, employers’ plans on average are more generous in firms with a higher proportion of high-wage workers, and variation in health risks and wages among workers is positively associated with the probability of offering a choice of plans.40
Medicine costs were found to decrease over time in this study, with the reduction appearing toward the end of the study period. Simultaneously, consultation fees increased at a faster rate than the reduction in medicine costs, resulting in total costs that approached the maximum allowable coverage of RM 45/clinic visit. This situation is most likely attributed to the incentive structure of health insurance that provides general allowable coverage of capping the total charges per clinic visit. With this structure in place, medicine costs and consultation fees can be modified to achieve the allowable coverage. We believe it is unlikely that the observed reduction in medicine costs in this study is due to increased product competition and hence potentially lower prices.4 This is because a previous study showed that despite the availability of multiple generic brands in Malaysia, only a few off-patent medicines were procured at relatively high prices.20 This suggests that the competition in this free market is not effectively driving reduction in prices which may again reflect the current incentive structures including any rebates or incentives from pharmaceutical companies.
The reason for the observed reduction in medicine costs in the current study is most likely due to a reduction in the number of medicines prescribed. In this case, the increase in consultation fees appears to result in private GPs reducing the cost of medicines they prescribed by reducing the number of medicines prescribed per clinic visit. To illustrate further, instead of receiving three types of medications, patients are now only receiving two types per clinic visit. Patients may also use out-of-pocket money to cover excess costs. A small reduction of 6% in number of common medicines prescribed for acute illness observed in the current study may not undermine patient care, but the increased cost to employer insurer for a separate claim and the increase out-of-pocket money for patients is a cause for concern.
Personal communication with GPs indicated that only drug charges within the coverage (≤RM 45) were captured in the database, whereas excess charges covered out-of-pocket by the patients themselves were not recorded. Although such a situation would permit patients to be prescribed all necessary drugs, rising out-of-pocket expenditure could limit patient access to suggested medicines and affect their care over the long term. From a social welfare viewpoint, the increase in out-of-pocket spending will lead to higher expenditures on medicines because seeking treatment is not a luxury commodity but is required by patients particularly patients with chronic diseases. For those who can afford to pay, a high price is not a deterrent and they (patients and families) are willing to pay higher prices in order to alleviate symptoms and prolong their lives.41 Those who cannot afford to pay would not necessarily be taking higher cost medicines leading to lower use. All of these can contribute to high consumer spending in the longer term which will reduce social welfare.42 Consequently, employees, employers, and health insurers could potentially pay a high price for the cost of medicines and services offered that eventually compromising patient care. However, we need to investigate the appropriateness of any prescriptions before we can say anything with certainty.
Apart from decreasing in number of medicines prescribed, we also saw that the number of tablets prescribed per patient per month decreasing over time for cetirizine, chlorpheniramine, and paracetamol, which may explain decreases in the costs of these medicines. Given that these are common medicines used to treat acute minor illnesses such as coughs and colds as well as minor pain, there are only concerns if the reductions mean an increase in the inappropriate short-term use of antibiotics for upper respiratory tract infections, which will compromise future care.
The decreases in the numbers of prescribed medicine and tablets may also be partly attributable to the coverage provided by employer’s insurance and a desire to reduce any sizable increase in out-of-pocket expenditures. As such, timely revision of the limit by employers is necessary to accommodate current healthcare costs. Insufficient insurance coverage can cause patients to discontinue their treatment. A study carried out in Vietnam revealed that patients with more severe illnesses or injuries were more likely to abandon their treatment if they believed that the financial burden of medical expenses would significantly impact their families’ financial situation. Without receiving proper treatment, there is a high likelihood of experiencing fatal consequences akin to “near-suicide” in the near future.43
There are a number of cost-cutting strategies that employers can implement including a review of current payments to physicians given appreciable increases in recent years (113.9% in 4 years). Under Schedule 7 of the Private Healthcare Facilities and Services Act (PHFSA) 1998, private clinic GPs consultation fees are capped at RM10 to RM35 per clinic visit.44 Consultation fees based on the complexity of clinical cases may also be capped in addition to the fee range specified. However, this is a secondary consideration to generally improving the quality of care provided within targeted expenditures. The recent announcement in December 2019 on the deregulation of consultation fees for private GPs is expected to result in immediate higher charges among private health practitioners. However, whilst patients can choose from a large number of GPs based on their reputation or service quality, it is still burden for patients to pay high consultation fees which may compromise future care.
Another option to reduce the cost to employers is to have panel community pharmacies under their incentive structure of employer health insurance. Looking at the findings from this current study, most common illnesses seen by GPs are acute illnesses, which are manageable by community pharmacies. The top five common prescribed medicines observed from our previous work and included in the current study are common medicines under pharmacist supervision that do not require prescription from doctors. All these are well suited for including community pharmacies as panel pharmacies. Furthermore, there is no consultation fee charged by community pharmacists (CPs), which will provide greater saving to employers. Studies showed that a sizeable proportion of these cases can be effectively managed in the community pharmacy setting with a high degree of patient satisfaction depending on the nature and severity of these ailments.45 Data from the UK shows that more than one in 10 GP visits and one in 20 emergency department visits are for minor ailments that could be managed in community pharmacies.46 This structure is vital to maximising the efficiency of health service delivery in Malaysia in the future.47
In addition, a review of the appropriateness of medicines prescribed is also required. We know from previous research that adherence to robust guidelines improves the quality of ambulatory care, which is certainly a consideration on this occasion.4,48,49 In addition, there has been high adherence to a limited number of well-proven medicines in ambulatory care in Stockholm, Sweden, enhanced by physician trust in the recommended medicines and the introduction of quality targets efficiently improving the quality of care.50–52 Such developments can improve employee care within finite resources that eventually will benefit the organization. In addition to the revision of the maximum coverage amount, the employer may also consider capping individual medicine costs in addition to capping the total charges per clinic visit.36 We know for instance in Europe that increased competition among the manufacturers of multiple sourced medicines and biosimilars has resulted in appreciable price reductions down by 98% from pre-patent loss prices in some occasions.4,9 This is to prevent the individual drug price modification and also to improve accessibility and affordability of medicines for employees.53–56
Overall, drug price control mechanisms include reference pricing, tiered formularies, preferential suppliers, greater transparency in pricing as well as price caps.53,55,57 These could also be considered by employers at their organization level.58,59 Additional considerations include compulsory generic substitution given the robust quality control mechanisms in Malaysia, well publicized details on individual prices and charges for medicines as well as consultation fees at each clinic visit thereby making these costs more transparent to both the patient and the payer before the treatment is provided. The employer should also conduct regular monitoring on the individual pattern of employee medicine use and related claims against agreed guidance, with the employer organisation also looking to improve the quality of care provided through developing robust guidelines and monitoring adherence to them. Figure 4 summarizes all of the above recommendations.
 |
Figure 4 Recommendation to employer to reduce costs and improve quality care. |
The implications of the present study’s findings extend to similar contexts concerning medicine use and costs within insurance coverage and healthcare settings. This pattern bears similarity to practices observed in other countries, including Vietnam, Ghana, United Kingdom and Iran. These findings can serve as a foundation for conducting comparative analyses with other health systems, aiming to enhance patient access to medicines and improve overall patient care. It is worth noting that the delivery and financing of health services can vary across different locations, and understanding the differences between healthcare systems enables researchers, policymakers, and practitioners to identify novel approaches, highlight challenges, tailor interventions and policies to specific settings. It has also laid the groundwork for future research to improve healthcare outcomes globally.
Among the limitations of the current study are the following: this study evaluates the prescribing of medicines and its associated costs within the context of employer health insurance coverage and we do not have information on supply and demand of healthcare that may also influence the prescribing. Another limitation that needs to be acknowledged is that this study is unable to characterise details of consultation fees and the exact type of cases seen by GPs, in which case complexity determines consultation fees. This, however, has no bearing on the study’s findings. In addition, we could not assess the appropriateness of physician prescribing and patient health outcomes. This is important going forward and will be the subject of future research projects.
Conclusions
We believe this study is among the pioneering ones that examine the medicine use and costs associated with outpatient clinic visits to general practitioners (GPs) covered by employer health insurance. This study revealed that the cost of medicines decreased over the study period, whereas consultation fees and total costs per clinic visit increased. Reducing the number of medicines and tablets prescribed for some treatments in order to modify the overall cost of medicines to come within approved expenditures limits patients’ ability to be prescribed with a complete drug regimen. As a result, potentially compromising patient care if this is the case.
Overall, the current incentive structure of employers’ health insurance, which caps the amount covered per clinic visit, does appear to influence the number of medicines prescribed and the costs associated with them, exacerbated by an appreciable increase in the costs of physician visits in recent years. Improved monitoring of prescribing patterns would enable the identification of outliers in terms of cost, effectiveness, and safety. Taking stronger measures in response to these outliers is likely to lead to cost reductions and enhance the overall effectiveness of prescribing practices.
Employers may consider mechanisms to optimise future drug prescribing and drug use including price capping of individual medicines, introducing guidelines and quality targets in addition to capping the total amount per clinic visit of their insurance incentive. Such considerations would improve the accessibility and affordability of appropriate medicines for employees, thereby making care more cost-effective and improving long-term outcomes benefiting both employees and employers.
Data Sharing Statement
The datasets generated and/or analysed during the current study are not publicly available. Request to access the datasets should be directed to International Islamic University Malaysia Research Ethical Committee. The de-identified data could be shared with interested researchers after obtaining the approval from the above ethical committee (http://www.iium.edu.my/centre/irec). The reason for the restriction on public data deposition is due to the privacy and confidentiality of patients’ health data.
Ethics Approval
Ethics approval for this study was granted by the International Islamic University Malaysia Ethical Committee (IREC-2019-212). De-identified data were used, and the results were reported in an aggregated manner. The analysis of patient information for research purposes without any direct involvement of patients or public required the approval from the Ethical Committee only and waived the requirement for informed consent.
Acknowledgments
The authors would like to thank the staff from PMCare and IIUM Health Wellness Centre for their assistance and cooperation with data extraction.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
CSZ was supported by a research grant from The Ministry of Education Malaysia (Fundamental Research Grant Scheme, FRGS/1/2022/SKK16/UIAM/01/3). The funders were not involved in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Danzon P, Mulcahy A, Towse AK, et al. Pharmaceutical pricing in emerging markets: effects of income, competition, and procurement. Health Econ. 2015;24(2):238–252. doi:10.1002/hec.3013
2. Danzon P, Towse A, Mestre-Ferrandiz J. Value-based differential pricing: efficient prices for drugs in a global context. Health Econ. 2015;24(3):294–301. doi:10.1002/hec.3021
3. Rahman MM, Zhang C, Swe KT, et al. Disease-specific out-of-pocket healthcare expenditure in urban Bangladesh: a Bayesian analysis. PLoS One. 2020;15(1):e0227565. doi:10.1371/journal.pone.0227565
4. Godman B, Fadare J, Kwon H-Y, et al. Evidence-based public policy making for medicines across countries: findings and implications for the future. J Comp Eff Res. 2021;10(12):1019–1052. doi:10.2217/cer-2020-0273
5. Swetha NB, Shobha S, Sriram S. Prevalence of catastrophic health expenditure and its associated factors, due to out-of-pocket health care expenses among households with and without chronic illness in Bangalore, India: a longitudinal study. J Prev Med Hyg. 2020;61(1):E92–E97. doi:10.15167/2421-4248/jpmh2020.61.1.1191
6. Vuong QH, Ho TM, Nguyen HK, Vuong TT. Healthcare consumers’ sensitivity to costs: a reflection on behavioural economics from an emerging market. Palgrave Commun. 2018;4(1):1–10. doi:10.1057/s41599-018-0127-3
7. Vuong Q-H. Sociodemographic factors influencing Vietnamese patient satisfaction with healthcare services and some meaningful empirical thresholds. Iran J Public Heal. 2018;47(1):119–126.
8. Luzzatto L, Hyry H, Schieppati A, et al. Outrageous prices of orphan drugs: a call for collaboration. Lancet. 2018;1(10149):31069. doi:10.1016/S0140-6736(18)31069-9
9. Godman B, Hill A, Simoens S, et al. Potential approaches for the pricing of cancer medicines across Europe to enhance the sustainability of healthcare systems and the implications. Expert Rev Pharmacoecon Outcomes Res. 2021;21(4):527–540. doi:10.1080/14737167.2021.1884546
10. The global use of medicine in 2019 and outlook to 2023; 2019. Available from: https://www.iqvia.com/-/media/iqvia/pdfs/institute-reports/the-global-use-of-medicine-in-2019-and-outlook-to-2023.pdf?_=1642424548771.
11. See S. Malaysia’s healthcare expenditure to “increase considerably” in short term despite reforms: report. Singapore; 2021. Available from: https://www.businesstimes.com.sg/asean-business/malaysias-healthcare-expenditure-to-increase-considerably-in-short-term-despite.
12. Fong MCC, Shanizza AIA. Malaysian statistics on medicine 2015–2016; 2020. Available from: https://www.pharmacy.gov.my/v2/sites/default/files/document-upload/malaysian-statistics-medicines-2015-2016.pdf.
13. New Straights Times. Medical experts weigh in on 2021 budget; 2020. Available from: https://www.nst.com.my/news/nation/2020/11/638881/medical-experts-weigh-2021-budget.
14. World Health Organization. A system of health accounts; 2011. Available from: https://www.who.int/health-accounts/methodology/sha2011.pdf?ua=1.
15. Islands S. Asia pacific observatory on health systems and policies: Malaysia health system review. 2012.
16. Rahim FF, Abdulrahman SA, Maideen SFK, Rashid A. Prevalence and factors associated with prediabetes and diabetes in fishing communities in Penang, Malaysia: a cross-sectional study. PLoS One. 2020;15(2):e0228570. doi:10.1371/journal.pone.0228570
17. Datamonitor Healthcare. Market access trends in the US, Europe, and emerging market; 2019. Available from: https://pharmaintelligence.informa.com/~/media/informa-shop-window/pharma/2019/files/whitepapers/global-market-access-whitepaper_.pdf.
18. Kasonde L, Tordrup D, Naheed A, Zeng W, Ahmed S, Babar ZUD. Evaluating medicine prices, availability and affordability in Bangladesh using World Health Organisation and Health Action International methodology. BMC Health Serv Res. 2019;19(1):1–12. doi:10.1186/s12913-019-4221-z
19. Hassali M, Shafie A, Babar Z, Khan T. A study comparing the retail drug prices between Northern Malaysia and Australia. J Pharm Heal Serv Res. 2012;3:103–107. doi:10.1111/j.1759-8893.2011.00080.x
20. Wong SL, Ibrahim S, Kadir NA, Salleh SM. Access and affordability of medicines in Malaysia: need for a national pricing policy. Appl Health Econ Health Policy. 2019;17:641–654. doi:10.1007/s40258-019-00480-9
21. A price control headache; 2019. Available from: https://www.thestar.com.my/news/nation/2019/05/12/a-price-control-headache.
22. Health ministry contemplating medicine price control; 2018. Available from: https://www.nst.com.my/news/nation/2018/07/391832/health-ministry-contemplating-medicine-price-control.
23. Soleymani F, Godman B, Yarimanesh P, Kebriaeezadeh A. Prescribing patterns of physicians working in both the direct and indirect treatment sectors in Iran; findings and implications. J Pharm Heal Serv Res. 2019;10(4):407–413. doi:10.1111/jphs.12322
24. Ashigbie PG, Azameti D, Wirtz VJ. Challenges of medicines management in the public and private sector under Ghana’s National Health Insurance Scheme - a qualitative study. J Pharm Policy Pract. 2016;9(1):1–10. doi:10.1186/s40545-016-0055-9
25. Goldacre B, Reynolds C, Powell-Smith A, et al. Do doctors in dispensing practices with a financial conflict of interest prescribe more expensive drugs? A cross-sectional analysis of English primary care prescribing data. BMJ Open. 2019;9(2):1–8. doi:10.1136/bmjopen-2018-026886
26. Jaafar S, Mohd Noh K, Abdul Muttalib K, Othman HJ. Malaysia Health System Review. Health Syst Transit. 2013;3(1):221.
27. Godman B, Haque M, Kumar S, et al. Current utilization patterns for long-acting insulin analogues including biosimilars among selected Asian countries and the implications for the future. Curr Med Res Opin. 2021;37(9):1529–1545. doi:10.1080/03007995.2021.1946024
28. Rezal RS, Hassali MA, Alrasheedy AA, et al. Prescribing patterns for upper respiratory tract infections: a prescription-review of primary care practice in Kedah, Malaysia, and the implications. Expert Rev Anti Infect Ther. 2015;13(12):1547–1556. doi:10.1586/14787210.2015.1085303
29. O’Brien E. Employers’ benefits from workers’ health insurance. Milbank Q. 2003;81(1):5–43. doi:10.1111/1468-0009.00037
30. Viet Nguyen C. The impact of voluntary health insurance on healthcare utilization and out-of-pocket payments: new evidence for Vietnam. Heal Econ. 2012;21:946–966. doi:10.1002/hec.1768
31. Vuong QH. Be rich or don’t be sick: estimating Vietnamese patients’ risk of falling into destitution. Springerplus. 2015;4(1). doi:10.1186/s40064-015-1279-x
32. Hassali MA, Kamil TKT, Yusof FAM, et al. General practitioners’ knowledge, attitude and prescribing of antibiotics for upper respiratory tract infections in Selangor, Malaysia: findings and implications. Expert Rev Anti Infect Ther. 2015;13(4):511–520. doi:10.1586/14787210.2015.1012497
33. Soleymani FGB, Yarimanesh PKA, Yarimanesh P, Kebriaeezadeh A. Prescribing patterns of physicians working in boqth the direct and indirect treatment sectors in Iran: findings and implications. J Pharm Heal Serv Res. 2019;10(4):407–413. doi:10.1111/jphs.12322
34. PMCare. About us. Available from: https://www.pmcare.com.my/about.
35. International Islamic University Malaysia. Available from: https://en.wikipedia.org/wiki/International_Islamic_University_Malaysia.
36. Zin CS, Taufek NH, Bux SH. Drug utilization and drug pricing in the private primary healthcare system in Malaysia: an employer price control mechanism. Front Public Heal. 2020;8:1–9. doi:10.3389/fpubh.2020.551328
37. StataCorp. Stata: Release 15. College Station, TX: StataCorp LLC; 2015.
38. Joyce GF, Escarce JJ, Solomon MD, Goldman DP. Employer drug benefit plans and spending on prescription drugs. JAMA. 2002;288:1733–1740. doi:10.1001/jama.288.14.1733
39. Chan FKI, McGrail K, Majumdar SR, Law MR. Changes in employer-sponsored private health insurance among retirees in Ontario: a cross-sectional study. C Open. 2019;7(1):E15–E22. doi:10.9778/cmajo.20180067
40. Bundorf MK. Employee demand for health insurance and employer health plan choices. J Health Econ. 2002;21(1):65–88. doi:10.1016/S0167-6296(01)00127-8
41. Vincent Rajkumar S. The high cost of prescription drugs: causes and solutions. Blood Cancer J. 2020;10(6). doi:10.1038/s41408-020-0338-x
42. Gonçalves R, Rodrigues V. Reference pricing with elastic demand for pharmaceuticals. Scand J Econ. 2018;120(1):159–182. doi:10.1111/sjoe.12207
43. Vuong Q-H, Le -T-T, Jin R, et al. Near-suicide phenomenon: an investigation into the psychology of patients with serious illnesses withdrawing from treatment. Int J Environ Res Public Health. 2023;20(6):5173. doi:10.3390/ijerph20065173
44. Pillai V. Higher specialist fees expected, but curbed by competition; 2020. Available from: https://codeblue.galencentre.org/2020/01/17/higher-specialist-fees-expected-but-curbed-by-competition/.
45. Motulsky A, Weir DL, Liang M, et al. Patient-initiated consultations in community pharmacies. Res Soc Adm Pharm. 2021;17(2):428–440. doi:10.1016/j.sapharm.2020.03.001
46. Fielding S, Porteous T, Ferguson J, et al. Estimating the burden of minor ailment consultations in general practices and emergency departments through retrospective review of routine data in North East Scotland. Fam Pract. 2015;32(2):165–172. doi:10.1093/fampra/cmv003
47. Cadogan CA, Hughes CM. On the frontline against COVID-19: community pharmacists’ contribution during a public health crisis. Res Soc Adm Pharm. 2021;17(1):2032–2035. doi:10.1016/j.sapharm.2020.03.015
48. Campbell SM, Meyer JC, Godman B. Why compliance to national prescribing guidelines is important especially across Sub-Saharan Africa and suggestions for the future. J Biomed Pharma Sci. 2021;4:35.
49. Niaz Q, Godman B, Massele A, et al. Validity of World Health Organisation prescribing indicators in Namibia’s primary healthcare: findings and implications. Int J Qual Heal Care. 2019;31(5):338–345. doi:10.1093/intqhc/mzy172
50. Gustafsson LL, Wettermark B, Godman B, et al. The “wise list”- a comprehensive concept to select, communicate and achieve adherence to recommendations of essential drugs in ambulatory care in Stockholm. Basic Clin Pharmacol Toxicol. 2011;108(4):224–233. doi:10.1111/j.1742-7843.2011.00682.x
51. Eriksen J, Gustafsson LL, Ateva K, et al. High adherence to the “Wise List” treatment recommendations inStockholm: a 15-year retrospective review of a multifaceted approach promoting rational use of medicines. BMJ Open. 2017;7:e014345. doi:10.1136/bmjopen-2016-014345
52. Norman C, Zarrinkoub R, Hasselström J, Godman B, Granath F, Wettermark B. Potential savings without compromising the quality of care. Int J Clin Pract. 2009;63(9):1320–1326. doi:10.1111/j.1742-1241.2009.02129.x
53. Vogler S. Fair prices for medicines? Exploring competent authorities’ and public payers’ preferences on pharmaceutical policies. Empirica. 2019;46(3):443–469. doi:10.1007/s10663-019-09446-5
54. Vogler S, Zimmermann N, de Joncheere K. Policy interventions related to medicines: survey of measures taken in European countries during 2010–2015. Health Policy (New York). 2016;120(12):1363–1377. doi:10.1016/j.healthpol.2016.09.006
55. Danzon PM. Differential pricing of pharmaceuticals: theory, evidence and emerging issues. Pharmacoeconomics. 2018;36(12):1395–1405. doi:10.1007/s40273-018-0696-4
56. Hinsch M, Kaddar M, Schmitt S. Enhancing medicine price transparency through price information mechanisms. Glob Heal. 2014;10(34):54.
57. Luiza V, Chaves L, Silva R, et al. Pharmaceutical policies: effects of cap and co-payment on rational use of medicines (Review) summary of findings for the main comparison. Cochrane Database Syst Rev. 2015;(5). doi:10.1002/14651858.CD007017
58. Van Woerkom M, Piepenbrink H, Godman B, et al. Ongoing measures to enhance the efficiency of prescribing of proton pump inhibitors and statins in the Netherlands: influence and future implications. J Comp Eff Res. 2012;1(6):527–538. doi:10.2217/cer.12.52
59. Macbride-stewart S, Mctaggart S, Kurdi A, et al. Initiatives and reforms across Scotland in recent years to improve prescribing, findings and global implications of drug prescriptions. PLoS One. 2021;14(12):2563–2586.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.