Back to Journals » Pragmatic and Observational Research » Volume 15
Trends in Systemic Glucocorticoid Utilization in the United Kingdom from 1990 to 2019: A Population-Based, Serial Cross-Sectional Analysis
Authors Menzies-Gow AN, Tran TN, Stanley B ![]() , Carter VA, Smolen JS, Bourdin A
, Carter VA, Smolen JS, Bourdin A ![]() , Fitzgerald JM, Raine T, Chapaneri J, Emmanuel B
, Fitzgerald JM, Raine T, Chapaneri J, Emmanuel B ![]() , Jackson DJ, Price DB
, Jackson DJ, Price DB ![]()
Received 3 October 2023
Accepted for publication 23 February 2024
Published 15 March 2024 Volume 2024:15 Pages 53—64
DOI https://doi.org/10.2147/POR.S442959
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Andrew N Menzies-Gow,1,2 Trung N Tran,3 Brooklyn Stanley,4 Victoria Ann Carter,4 Josef S Smolen,5 Arnaud Bourdin,6 J Mark Fitzgerald7 ,† Tim Raine,8 Jatin Chapaneri,2 Benjamin Emmanuel,3 David J Jackson,9,10 David B Price4,11
1Royal Brompton and Harefield Hospitals, Guys & St Thomas’ NHS Foundation Trust, London, UK; 2AstraZeneca, Cambridge, UK; 3AstraZeneca, Gaithersburg, MD, USA; 4Observational and Pragmatic Research Institute, Singapore; 5Medical University of Vienna, Vienna, Austria; 6Université de Montpellier, CHU Montpellier, PhyMedExp, INSERM, CNRS, Montpellier, France; 7The University of British Columbia, Vancouver, British Columbia, Canada; 8Cambridge University Hospitals NHS Foundation Trust, Addenbrooke’s Hospital, Cambridge, UK; 9Guy’s Severe Asthma Centre, Guy’s & St Thomas’ NHS Trust, London, UK; 10School of Immunology & Microbial Sciences, King’s College London, London, UK; 11Centre of Academic Primary Care, Division of Applied Health Sciences, University of Aberdeen, Aberdeen, UK
†J. Mark Fitzgerald passed away on January 18, 2022
Correspondence: David B Price, Centre of Academic Primary Care, Division of Applied Health Sciences, University of Aberdeen, Polwarth Building-Foresterhill, Aberdeen, AB25 2ZD, UK, Tel +65 3105 1489, Email [email protected]
Purpose: Associations between systemic glucocorticoid (SGC) exposure and risk for adverse outcomes have spurred a move toward steroid-sparing treatment strategies. Real-world changes in SGC exposure over time, after the introduction of steroid-sparing treatment strategies, reveal areas of successful risk mitigation as well as unmet needs.
Patients and Methods: A population-based ecological study was performed from the Optimum Patient Care Research Database to describe SGC prescribing trends of steroid-sparing treatment strategies in primary care practices before and after licensure of biologics in the United Kingdom from 1990 to 2019. Each analysis year included patients aged ≥ 5 years who were registered for ≥ 1 year with a participating primary care practice. The primary analysis was SGC exposure, defined as total cumulative SGC dose per patient per year, for asthma, severe asthma, chronic obstructive pulmonary disease (COPD), nasal polyps, Crohn’s disease, rheumatoid arthritis, ulcerative colitis, and systemic lupus erythematosus. Secondary outcomes were percentages of patients prescribed SGCs and number of SGC prescriptions per patient per year.
Results: The number of patients who met study inclusion criteria ranged from 219,862 (1990) to 1,261,550 (2019). At the population level, patients with asthma or COPD accounted for 67.7% to 73.2% of patients per year with an SGC prescription. Over three decades, decreases in SGC total yearly dose ≥ 1000 mg have been achieved in multiple conditions. Patients with COPD prescribed SGCs increased from 5.8% (1990) to 34.8% (2017). SGC prescribing trends for severe asthma, Crohn’s disease, and ulcerative colitis show decreased prescribing trends after the introduction of biologics.
Conclusion: Decreases in total yearly SGC doses have been shown in multiple conditions; however, for conditions such as severe asthma and COPD, an unmet need remains for increased awareness of SGC burden and the adoption or development of SGC-sparing alternatives to reduce overuse.
Keywords: glucocorticoids, practice patterns, drug prescriptions, biological products, drug utilization
Introduction
Increasing recognition of the risks associated with SGC use has led patient management guidelines to embrace SGC-sparing treatment strategies.1–6 Acute (eg, pneumonia, opportunistic infections, and gastrointestinal events) and longer-term adverse outcomes (eg, new-onset type 2 diabetes mellitus, weight gain, osteoporosis, and cataracts) have been linked to SGC exposure,7–9 with both intermittent and long-term use conferring increased risk of mortality.10 The likelihood of experiencing complications escalates with dose and cumulative exposure, and evidence suggests that as little as 0.5 to 1 g of cumulative SGC prescribed intermittently is associated with adverse outcomes.8,11,12
Systemic glucocorticoids (SGCs) are frequently used to treat asthma and chronic obstructive pulmonary disease (COPD).13,14 Changes in asthma guidelines (eg, consider long-term SGC use as a last resort due to the serious side effects and screening patients for adrenal insufficiency if they are on maintenance SGC or high-dose inhaled corticosteroids [ICSs]/long-acting beta-agonists) and the introduction of SGC-sparing alternatives, including biologic therapies, for example, should decrease SGC exposure.13,15,16 In Crohn’s disease (CD), following recommendations, there has been a decrease in prolonged steroid exposure over time.17,18 However, there is often a lag between the introduction of new guidelines or therapies and their integration into clinical practice.19 A longitudinal population-based study of patients with rheumatoid arthritis (RA) showed that initiation of glucocorticoids within 6 months of diagnosis are occurring earlier in their disease compared with prescribing patterns from previous years.20 Indeed, long-term use of SGC has continued to be observed in conditions with approved and readily available alternatives to steroids, such as severe asthma, rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), and ulcerative colitis (UC).7,17,21–23 Although long-term use may be waning, short-term and recurrent intermittent use persists24 and continues to contribute to SGC-related adverse outcomes.7
Insights into successful SGC reduction approaches can be gained by assessing changes in prescription patterns across disease states over time and relative to milestones that would be expected to affect utilization, such as the availability of new therapies. To that end, this population-based ecological study was performed using data extracted from electronic medical records (EMRs) to describe temporal trends in SGC utilization for chronic disease conditions in the United Kingdom (UK), overlayed with approval dates for relevant biologic therapies.
Materials and Methods
Data Source and Study Population
With guidance from an external international steering committee of leading respiratory experts, the Observational and Pragmatic Research Institute performed a serial cross-sectional analysis using data from the Optimum Patient Care Research Database (OPCRD; www.opcrd.co.uk).25 The OPCRD dataset comprises medical records for >20 million patients from >1000 primary care practices (approximately 22% of the total UK population) drawn from all UK clinical EMR systems with median follow-up in excess of 13 years. Most UK residents are registered at one primary care practice, and secondary or tertiary care is only accessible through referral from a primary care physician. The study population is, therefore, a nonselective, representative sample of the population from catchment areas of the participating practices.
Patients were eligible for study inclusion if they were aged ≥5 years and registered for ≥1 full calendar year with a participating primary care practice during the study period (1990–2019). All analyses were performed by calendar year; hence, inclusion criteria were applied relative to the analysis year. Additional study methods, including patient exclusion criteria, are presented in the Supplementary Materials.
Data-Sharing Statement
The dataset supporting the conclusions of this article was derived from the OPCRD. The authors do not have permission to give the public access to the study dataset; researchers may request access to OPCRD data for their own purposes. Requests for access to OPCRD can be made via the OPCRD website (https://opcrd.co.uk/our-database/data-requests/) or via the inquiries email, [email protected].
Ethics Approval
The study was approved by the Anonymised Data Ethics Protocols and Transparency (ADEPT) committee (approval number ADEPT1719) and was registered with the European Union electronic Register of Post-Authorisation Studies (EU PAS Register Number EUPAS30943).
Assessments
SGC exposure was defined as the total SGC prescription dosage per patient per year, as indicated by the patient’s medical record, during the analysis year. Doses of individual SGCs were converted to prednisolone equivalents using the defined daily dose and aggregated at the population level (Table S1). For the primary analysis and evaluation of the total prescribed SGC dose per year (Figure 1), the International Steering Committee identified 7 demonstration conditions of interest (asthma, COPD, nasal polyps, CD, UC, RA, and SLE) that were prevalent within the dataset and for which SGCs are used as part of standard practice for at least a significant percentage of patients but are not mandated for all patients with the condition. Conditions were considered active within an analysis year according to the following definitions. Owing to their persistent nature, COPD, nasal polyps, RA, and SLE, once diagnosed, were considered always active. Given their relapsing and remitting clinical course, asthma, CD, and UC were considered active during the analysis year only if the patient had a disease-specific diagnostic code using READ or SNOWMED terms at any time plus a relevant medication prescription (including SGC) used to treat the disease in the analysis year or if the patient had a disease-specific diagnostic code using READ or SNOWMED terms in the analysis year. Biologics are indicated in the charts in the year they became available.
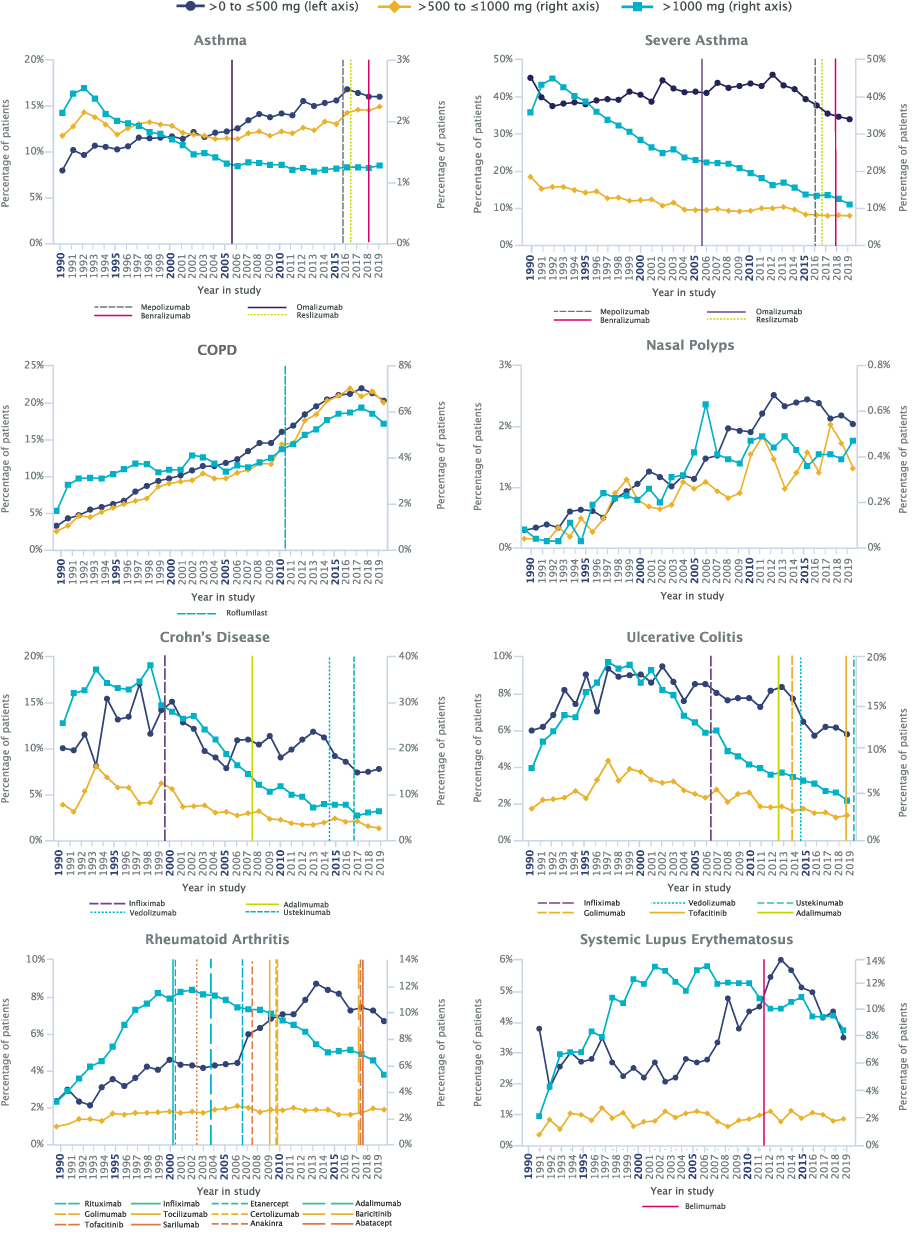 |
Figure 1 Total yearly SGC dose by category. Percentage of patients per analysis year for asthma, severe asthma, COPD, nasal polyps, Crohn’s disease, ulcerative colitis, rheumatoid arthritis, and systemic lupus erythematosus. European Medicines Agency approval dates for biologic therapies are marked by vertical lines In order to minimize the misattribution of an SGC indication, only one condition per patient per year for which an SGC could have been prescribed was used for these analyses. Abbreviations: COPD, chronic obstructive pulmonary disease; SGC, systemic glucocorticoid. |
Additional SGC evaluations across the 7 identified conditions included the number and percentage of SGC prescriptions per patient per analysis year (Figure 2), average number of SGC prescriptions per patient per year (Figure 3), average total SGC dose per course (Figure S1), percentage of patients prescribed SGC by average daily dose (Figure S2), and average total SGC dose prescribed per year (Figure S3). These data were aggregated annually at the population level.
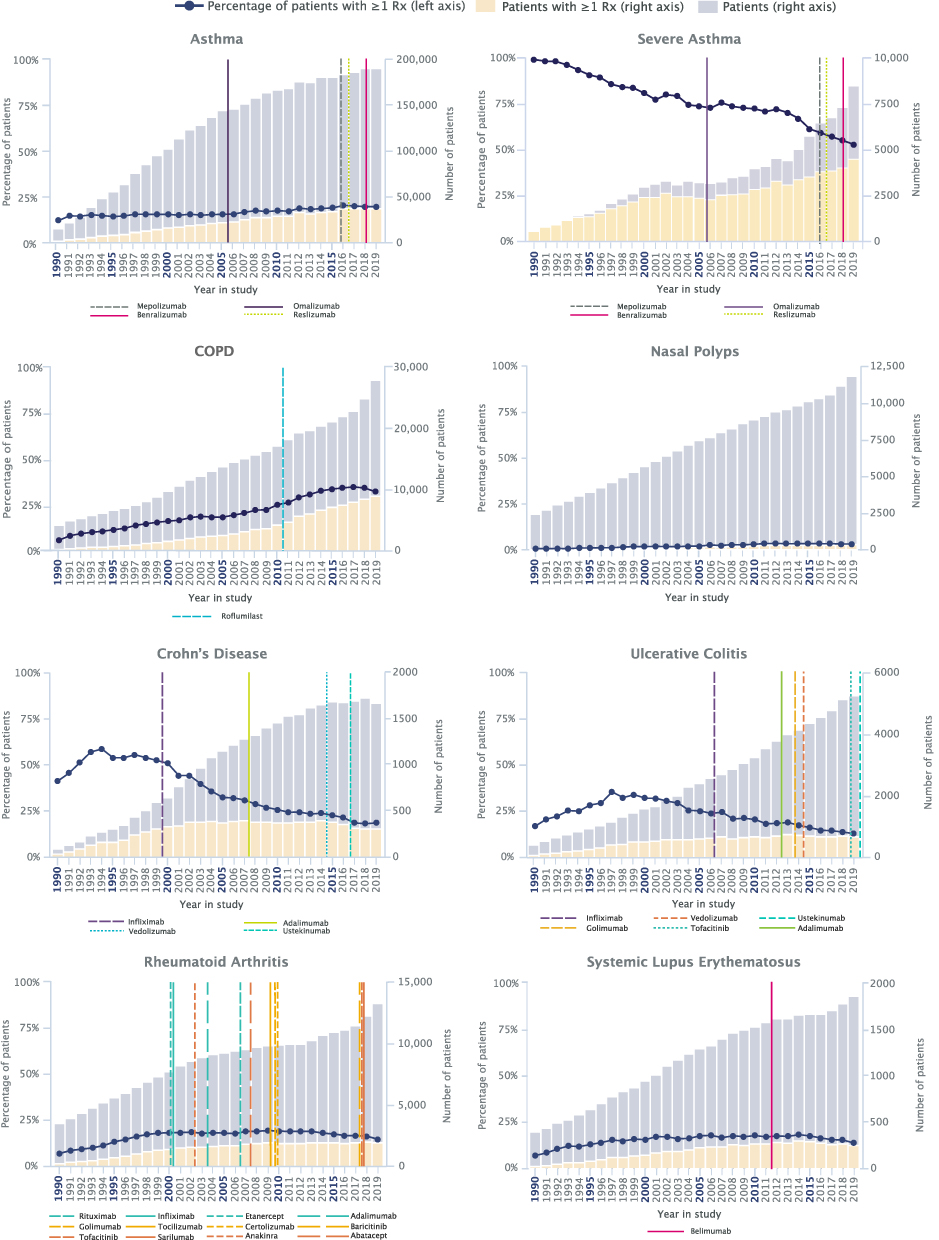 |
Figure 2 Patients with one or more prescriptions of SGCs. Number and percentage of SGC prescriptions per patient per analysis year for asthma, severe asthma, COPD, nasal polyps, Crohn’s disease, ulcerative colitis, rheumatoid arthritis, and systemic lupus erythematosus. European Medicines Agency approval dates for biologic therapies are marked by vertical lines In order to minimize misattribution of an SGC indication, only one condition per patient per year for which an SGC could have been prescribed was used for these analyses. Abbreviations: COPD, chronic obstructive pulmonary disease; SGC, systemic glucocorticoid. |
 |
Figure 3 Average number of SGC prescriptions per patient. Number of prescriptions per patient per analysis year for asthma, severe asthma, COPD, nasal polyps, Crohn’s disease, ulcerative colitis, rheumatoid arthritis, and systemic lupus erythematosus. European Medicines Agency approval dates for biologic therapies are marked by vertical lines In order to minimize misattribution of an SGC indication, only one condition per patient per year for which an SGC could have been prescribed was used for these analyses. Abbreviations: COPD, chronic obstructive pulmonary disease; SGC, systemic glucocorticoid. |
In order to understand the overall SGC use in the UK primary care population, we included an expanded array of 27 conditions for which SGC can be prescribed (Table S2) in an analysis of the relative contribution of each indication to SGC prescriptions and total yearly prescribed dose.
Statistical Analysis
In order to minimize the misattribution of an SGC indication, we limited analyses to patients with only 1 condition for which an SGC could have been prescribed in the analysis year. This approach ensured that SGC prescriptions were attributable to a specific disease and not prescribed to treat a comorbidity or unrelated condition. Owing to the frequent overlap between asthma, nasal polyps, and atopic dermatitis,26 patients with asthma and either of these comorbidities were included in the asthma category. An additional analysis was performed for patients with asthma who had treatment-defined severe disease, as indicated by receipt of Global Initiative for Asthma step 4 or 5 treatment.13 Dosage-related results are reported in milligrams among the patient population.
Descriptive statistics were used to characterize SGC utilization. Imputation for missing data was performed as described in Table S3. In order to gauge the potential effect of biologic therapies on prescription practices, European Medicines Agency approval dates (Table S4) are marked on plots of SGC utilization. In addition, exploratory linear regression analyses were used to compare trends in total SGC dose prescribed per year before versus after European Medicines Agency approval of the first biologic therapy for the condition of interest. Data processing and analyses were performed using Stata MP/6 version 15.1 (StataCorp LLC, College Station, Texas, USA).
Results
The number of patients per annum who met study inclusion criteria increased from 219,862 (25.2% of the database) in 1990 to 1,261,550 in 2019 (20.8% of the database) (Figure S4). Increases in patient numbers reflect increasing practice size due to primary care practice mergers and the closing of smaller practices. Of the conditions assessed, asthma was the most prevalent, followed by COPD and RA.
SGC Utilization
The range of total SGC-prescribed doses per year and patients per year with an SGC prescription by specific conditions were aggregated and analyzed at the population level. Asthma and COPD accounted for 38.5% to 55.6% of the total SGC prescribed per year and 67.7% to 73.2% of patients per year with an SGC prescription (Figure S5). Over time, the relative contributions of asthma, UC, RA, and CD decreased, whereas that of COPD approximately doubled.
The percentage of patients with asthma who had a total yearly SGC dose >1000 mg decreased by approximately half from 1992 to 2006, whereas the percentage of patients with doses ≤500 mg per year nearly doubled from 1990 to 2016 (Figure 1). The percentage of patients with daily SGC doses >15 mg/day prescribed increased from 6.6% in 1990 to 18.2% in 2016 (Figure S2), yet the average total dose per course for patients with ≥1 SGC prescriptions decreased over time (Figure S1). A slight decrease in average total SGC doses per year was noted after the introduction of biologics (Figure S3). The percentage of patients with asthma with ≥1 SGC prescription was stable through the mid-2000s, after which a slight increase was noted (Figure 2).
The number of patients with severe asthma in this study population increased from 3.7% in 1990 to 4.5% in 2019 (Figure 2). Within this population, large decreases in the percentage of patients receiving a cumulative yearly dose >1000 mg were observed, along with decreases in the percentage of patients with ≥1 prescription (Figures 1 and 2). The percentage of patients with an average prescribed daily dose >15 mg/day increased from 1990 (0.4%) to 2014 (24.9%) before declining (Figure S2). The average total SGC dose per course decreased for the overall population but to a lesser extent in patients with ≥1 SGC prescription (Figure S1). Starting around 1992, decreases in SGC doses >1000 mg occurred before the introduction of biologics; however, the decrease continued with the introduction of biologics starting in 2006 with newer biologics introduced as late as 2018 (Figures 1 and S3).
Among patients with COPD, the percentages of patients in each average total yearly dose strata increased over time (Figure 1); however, average prescribed daily dose percentages only increased for the >15 mg/day category (Figure S2). The percentage of patients with COPD with ≥1 SGC prescription increased from 5.8% in 1990 to 34.8% in 2017 (Figure 2). The average dose per course decreased over time for patients with ≥1 SGC prescription (Figure S1). There were no biologic therapies approved for the treatment of COPD during the observation period.
Among patients with nasal polyps, the total yearly SGC dose increased over time (Figure 1), as did the percentage of patients prescribed with average daily SGC doses ≤7.5 mg/day and >15 mg/day (Figure S2). During the observation period, no biologic therapies were approved by the European Medicines Agency to treat nasal polyps. The percentage of patients with nasal polyps with ≥1 SGC prescription was low (<1–3%) and did not change appreciably over time (Figure 2).
Over time, the total yearly SGC dose, total dose course, and average number of SGC prescriptions decreased among patients with CD (Figures 1, 3 and S1). A concomitant decrease in the percentage of patients prescribed SGCs across all three average prescribed daily dose strata was observed from the early 2000s through 2009 (Figure S2), and the decrease continued after the introduction of biologics (Figure S3). The percentage of patients with CD with ≥1 SGC prescription decreased from a high of 58.5% in 1994 to a low of 18.0% in 2018 (Figure 2).
The percentage of patients with UC had a steady decrease in SGC average total yearly dose, total dose per course, and percentage of patients prescribed >15 mg/day starting in the late 1990s (Figures S1 and S2), and the decrease continued after the introduction of biologics (Figure S3).
The percentage of patients with RA receiving a cumulative SGC dose >1000 mg/year decreased from a high of 11.7% in 2002 to a low of 5.3% in 2019 (Figure 1). The average total SGC dose per course decreased, whereas the percentage of patients prescribed SGC at a dose >15 mg/day increased over time (Figures S1 and S2). There was a decrease in the total SGC prescribed noted after the introduction of biologics (Figure S3).
The percentage of patients with SLE who received an SGC dose >1000 mg per year and the average number of prescriptions per patient initially increased before declining in the early- to mid-2010s (Figures 1 and 2). The average SGC dose per course peaked at ≈450 mg in 1999 and decreased to ≈300 mg from 2010 onward (Figure S1). There was no decrease noted in SGC total prescriptions after the introduction of biologics (Figure S3).
Discussion
This large, population-based ecological study highlights the variability in SGC utilization prescribing trends in respiratory and nonrespiratory diseases in the UK over the past three decades. The results reveal that success in reducing SGC exposure, in some instances, appears to have occurred around or after the availability of biologics. Rates of SGC utilization for asthma showed a downward trend over time for patients with high-dose prescriptions (ie, >1000 mg) and an upward trend in prescriptions ≤1000 mg. Downward trends in severe asthma, CD, UC, and RA were also observed. In contrast, measures of SGC utilization were mixed for SLE. The overall population prescription trends in which biologics were not yet approved for use remained largely neutral for nasal polyps and demonstrated a worsening pattern for COPD.
Asthma and COPD are two conditions in which certain measures of SGC utilization showed a worsening over time. For asthma, usage metrics yielded mixed results, with a combination of increasing and decreasing trends over time. Recent increases in SGC utilization may be linked to greater implementation of asthma action plans in which patients are provided with an emergency course of SGC to self-administer when they experience deterioration of asthma control.5
In contrast, SGC use in patients with severe asthma showed an overall decrease. A recent downward trend in the use of >15 mg/day for severe asthma coincides with the availability of newer biologic therapies, including reslizumab, mepolizumab, and benralizumab, the latter two having demonstrated steroid-sparing effects in patients with asthma.27,28 As the current analysis only explored SGC, it is not known whether ICS utilization, particularly in the form of ICS/long-acting beta-agonists, demonstrated compensatory longitudinal trends in this patient population. Notably, although decreases in some utilization metrics were observed on a per-patient basis for patients with asthma, the number of patients with asthma in the UK is increasing; hence, the burden associated with SGC use continues to be considerable. Indeed, asthma was consistently the greatest contributor to SGC utilization in our dataset.
The SGC utilization trend in COPD visually shows an upturn in nearly all metrics through 2017. SGCs are not recommended for maintenance therapy in COPD but are used in the treatment of exacerbations.3 Rising levels of SGC use, therefore, could suggest that exacerbation risk is not well managed and/or that SGCs are being used inappropriately. At least in part, SGC use in COPD may be a result of patients using rescue packs, which include SGC tablets that patients can self-administer for a presumed exacerbation. Data regarding the effectiveness of rescue packs/action plans are mixed.29,30 For both COPD and asthma, the presence of symptoms does not always indicate uncontrolled, steroid-responsive type 2 (T2) inflammation. More routine use of T2 biomarkers in clinical practice could help to identify patients who will benefit from steroids in a more precise way, allowing for the avoidance of inappropriate SGC courses for non-T2 bacterial events.
Beginning in the early 2000s, utilization of SGC for CD in our dataset decreased by all metrics. The first biologic therapy for CD, infliximab, was approved in Europe in 1999. Although uptake of infliximab in clinical practice was initially slow,31 biologic therapy use for CD has subsequently increased considerably, with approximately one-third of patients in a recent regional UK cohort reporting receipt of biologic therapy as first- or second-line treatment.32 Patients are also initiating biologic therapy earlier in the course of the disease.32 A 2019 analysis found that maintenance treatment with antitumor necrosis factor agents (eg, infliximab and adalimumab) was associated with a decreased likelihood of excess steroid use in patients with CD.33 These observations suggest that the combination of guideline-advocated limitations in SGC use4 and a rise in the use and availability of biologic therapy may have contributed to the reduction of the SGC burden in CD.
For UC, the influence of biologic therapy on SGC use is difficult to ascertain, as the decreasing trend preceded biologic availability. In our dataset, SGC use peaked in the late 1990s and subsequently declined across metrics, but the first biologic was not approved in Europe until 2006. There was, however, considerable worldwide off-label use of biologic therapies for UC that preceded their approval.34,35 Nonetheless, there was a further acceleration of decreasing SGC total dose per year observed after biologic therapy approval. It is worth noting that despite these improvements, SGC use continues to be prevalent for UC in the UK,17 with a reported high degree of avoidable steroid dependency or excess.33,36
In our analysis, several measures of SGC use for RA visually show an upturn in prescriptions prior to the introduction of biologic therapies. Overall, the decrease in SGC use for RA was lower relative to changes observed in CD, which may reflect restricted biologic therapy access in the UK. Owing to the stringency of national reimbursement criteria, the UK is considered to offer low access to biological disease-modifying antirheumatic drugs.37 There may also be a differential focus on SGC reduction for RA in clinical practice, with continued SGC use in prevalent patients who are well-managed and a greater emphasis on avoiding SGC initiation for incident patients.
This study is subject to the limitations inherent to EMR data. In particular, because the study time period encompassed the introduction of the Quality and Outcomes Framework in 2004,38 there may be a difference in the data quality and completeness before and after 2004. Reliance on EMR data could also result in insufficient medical history information to identify conditions of interest, principally when data available before the analysis year were limited. In addition, EMR data do not distinguish a prescription for a current medical need from a prescription for future use, as occurs with action plans for asthma and COPD. The data for this study were also pre–COVID-19. The inclusion of data during and after the COVID-19 pandemic could have led to different results.
As a population-based ecological study, causation or any direct relationship cannot be established for changes in prescription patterns; temporal relationships between the availability of new biologic therapies and changes in SGC prescription trends are speculative. The interplay of multiple factors, including emerging clinical evidence, availability of new therapies, changes to guidelines, introduction of SGC-sparing initiatives, development and management of adrenal insufficiency, and changes in reimbursement, contributes to SGC utilization. Across diseases, low-dose SGC use continued to be prevalent and may, in some cases, reflect the challenges of tapering therapy in patients who have developed adrenal insufficiency due to long-term steroid dependency.39 Future studies should expand on these findings with statistical tests to evaluate relationships and causation between the prescribing patterns they report and relevant aspects of patient clinical care and treatment.
Another limitation is the lack of distinction of patients by disease severity. As shown from the asthma analyses, SGC utilization trends differed for those with severe disease compared with the overall population. Patterns of SGC use may also be affected by changes in diagnostic criteria that have allowed for the identification of patients at earlier/milder stages of disease when SGC use is less applicable. Lastly, because the indication for SGC must be inferred from the diagnostic data, analyses were primarily restricted to patients with only one condition for which SGC may have been prescribed during the analysis year. These data, therefore, reflect the monocondition patient experience, which may differ from that of patients with comorbid conditions who are also treated with SGC. Notably, the monocondition categorization for asthma included patients with nasal polyps and/or atopic dermatitis. As these conditions are treated by different specialists and differ in terms of SGC-sparing therapy availability, SGC prescription patterns may have been influenced by nonasthma condition presence. Additional research into SGC use in patients with monocondition and comorbid inflammatory diseases is needed.
A greater appreciation for the adverse consequences of SGC, even when used at low doses and infrequently, accompanied by the introduction of biologics, has led to declining SGC utilization across a variety of conditions. Severe asthma serves as an example of this principle. Decreases in SGC utilization were also observed in CD, UC, and RA, conditions for which there are multiple biologic therapies available. Nonetheless, overall SGC utilization and persistent exposure to high daily or cumulative doses indicate a need for increased awareness of SGC burden and steroid-sparing options to minimize overuse, particularly in conditions such as asthma and COPD, in which SGC use continues to be prevalent.
Acknowledgments
The authors thank the members of the Forum for reducing Oral Corticosteroid Use in Severe asthma (FOCUS) for their involvement in the conception of the study (Table S5). Medical writing support, including preparation of the draft manuscript under the direction and guidance of the authors, incorporating author feedback, and manuscript submission, was provided by Lea Anne Gardner, PhD, RN (Citrus Health Group), in accordance with Good Publication Practice 2022 (GPP 2022) guidelines. This support was funded by AstraZeneca (Cambridge, UK). Data from OPCRD were obtained under license from Optimum Patient Care Limited. The interpretation and conclusions contained in this report are those of the authors alone.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This work was funded by AstraZeneca. In collaboration with the steering committee, AstraZeneca was involved in the study design; in the collection, analysis, and interpretation of data; in the writing of the manuscript; and in the decision to submit the article for publication. All authors had full access to the data, agreed to be accountable for the accuracy and integrity of the work, and shared responsibility for the decision to submit the article for publication. Steering committee members were not compensated for their participation.
Disclosure
All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare support from AstraZeneca for the submitted work.
AMG is an employee of AstraZeneca and has attended advisory boards for AstraZeneca, GlaxoSmithKline, Novartis, Sanofi, and Teva; received speaker fees from AstraZeneca, Novartis, Sanofi, and Teva; participated in research with AstraZeneca for which his institution has been remunerated; and had consultancy agreements with AstraZeneca and Sanofi.
TNT, JC, and BE are employees of AstraZeneca.
BS and VC report no conflict of interest.
JSS has received research grants for his institution from AbbVie, AstraZeneca, Lilly, Novartis, and Roche; and honoraria for consultancies and/or speaking engagements from AbbVie, Amgen, AstraZeneca, Astro, Bristol-Myers Squibb, Celgene, Celltrion, Chugai, Gilead, ILTOO, Janssen, Lilly, Merck Sharp & Dohme, Novartis-Sandoz, Pfizer, R-Pharm, Roche, Samsung, Sanofi, and UCB.
AB has received personal fees and a grant from Boehringer Ingelheim; personal fees from AstraZeneca, Chiesi, GSK, Novartis, and Sanofi-Regeneron; and is an investigator in clinical trials from Acceleron, Actelion, Galapagos, MSD, Nuvaira, Pulmonx, United Therapeutic, and Vertex.
JMF has attended advisory boards for AstraZeneca, GSK, Novartis, Sanofi Regeneron, and Theravance; received speaker fees/honoraria from AstraZeneca, GSK, Sanofi-Regeneron, and TEVA; received research funding from AllerGen National Centre for Excellence, AstraZeneca, Canadian Institute for Health Research, GSK, National Institutes of Health, Novartis, Sanofi-Regeneron, and TEVA, all paid directly to his institution; and has been a member of the steering committee for the International Severe Asthma Registry, principal investigator for Canadian Severe Asthma Registry, and a member of the GINA Science and Executive Committees.
TR has received research/educational grants and/or speaker/consultation fees from AbbVie, Arena, AstraZeneca, BMS, Celgene, Ferring, Galapagos, Gilead, GSK, LabGenius, Janssen, MSD, Mylan, Novartis, Pfizer, Sandoz, Takeda, and UCB.
DJJ has attended advisory boards and has received speaker fees from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis, and Sanofi.
DBP has board membership with AstraZeneca, Boehringer Ingelheim, Chiesi, Mylan, Novartis, Regeneron Pharmaceuticals, Sanofi Genzyme, and Thermofisher; consultancy agreements with Airway Vista Secretariat, AstraZeneca, Boehringer Ingelheim, Chiesi, EPG Communication Holdings Ltd, FIECON Ltd, Fieldwork International, GlaxoSmithKline, Mundipharma, Mylan, Novartis, OM Pharma SA, PeerVoice, Phadia AB, Spirosure Inc., Strategic North Limited, Synapse Research Management Partners SL, Talos Health Solutions, Theravance, and WebMD Global LLC; grants and unrestricted funding for investigator-initiated studies (conducted through Observational and Pragmatic Research Institute Pte Ltd) from AstraZeneca, Boehringer Ingelheim, Chiesi, Mylan, Novartis, Regeneron Pharmaceuticals, Respiratory Effectiveness Group, Sanofi Genzyme, Theravance, and the UK National Health Service; received payment for lectures/speaking engagements from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, GlaxoSmithKline, Kyorin, Mylan, Mundipharma, Novartis, Regeneron Pharmaceuticals, and Sanofi Genzyme; received payment for travel/accommodation/meeting expenses from AstraZeneca, Boehringer Ingelheim, Mundipharma, Mylan, Novartis, and Thermofisher; stock/stock options from AKL Research and Development Ltd, which produces phytopharmaceuticals; ownership of 74% of the social enterprise Optimum Patient Care Ltd (Australia, UK) and 92.61% of Observational and Pragmatic Research Institute Pte Ltd (Singapore); 5% shareholding in Timestamp, which develops adherence monitoring technology; a peer reviewer role for grant committees of the UK Efficacy and Mechanism Evaluation program and the Health Technology Assessment; and served as an expert witness for GlaxoSmithKline.
References
1. Scadding GK, Durham SR, Mirakian R, et al. BSACI guidelines for the management of rhinosinusitis and nasal polyposis. Clin Exp Allergy. 2008;38(2):260–275. doi:10.1111/j.1365-2222.2007.02889.x
2. Gordon C, Amissah-Arthur MB, Gayed M, et al. The British Society for Rheumatology guideline for the management of systemic lupus erythematosus in adults. Rheumatology. 2018;57(1):e1–e45. doi:10.1093/rheumatology/kex286
3. Chronic obstructive pulmonary disease in over 16s: diagnosis and management National Institute for Health and Care Excellence (NICE) Guideline (NG115); 2018. Available from: https://www.nice.org.uk/guidance/ng115.
4. Lamb CA, Kennedy NA, Raine T, et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut. 2019;68(Suppl 3):s1–s106. doi:10.1136/gutjnl-2019-318484
5. British guideline on the management of asthma: a national clinical guideline (Scottish Intercollegiate Guidelines Network [SIGN 158] Evidence-based Clinical Guidelines; British Thoracic Society); 2019. Available from: https://www.sign.ac.uk/media/1773/sign158-updated.pdf
6. Smolen JS, Landewe RBM, Bijlsma JWJ, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheum Dis. 2020;79(6):685–699. doi:10.1136/annrheumdis-2019-216655
7. Bleecker ER, Menzies-Gow AN, Price DB, et al. Systematic literature review of systemic corticosteroid use for asthma management. Am J Respir Crit Care Med. 2020;201(3):276–293. doi:10.1164/rccm.201904-0903SO
8. Volmer T, Effenberger T, Trautner C, Buhl R. Consequences of long-term oral corticosteroid therapy and its side-effects in severe asthma in adults: a focused review of the impact data in the literature. Eur Respir J. 2018;52(4):1800703. doi:10.1183/13993003.00703-2018
9. Sullivan PW, Ghushchyan VH, Globe G, Schatz M. Oral corticosteroid exposure and adverse effects in asthmatic patients. J Allergy Clin Immunol. 2018;141(1):110–116 e7. doi:10.1016/j.jaci.2017.04.009
10. Ekstrom M, Nwaru BI, Hasvold P, Wiklund F, Telg G, Janson C. Oral corticosteroid use, morbidity and mortality in asthma: a nationwide prospective cohort study in Sweden. Allergy. 2019;74(11):2181–2190. doi:10.1111/all.13874
11. Price DB, Trudo F, Voorham J, et al. Adverse outcomes from initiation of systemic corticosteroids for asthma: long-term observational study. J Asthma Allergy. 2018;11:193–204. doi:10.2147/JAA.S176026
12. Blakey J, Chung LP, McDonald VM, et al. Oral corticosteroids stewardship for asthma in adults and adolescents: a position paper from the Thoracic Society of Australia and New Zealand. Respirology. 2021;26(12):1112–1130. doi:10.1111/resp.14147
13. Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention, 2022 report; 2022. Available from: https://ginasthma.org/wp-content/uploads/2022/05/GINA-Main-Report-2022-FINAL-22-05-03-WMS.pdf.
14. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease 2021 report; 2021. Available from: https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf.
15. Menzies-Gow A, Canonica GW, Winders TA, Correia de Sousa J, Upham JW, Fink-Wagner AH. A charter to improve patient care in severe asthma. Adv Ther. 2018;35(10):1485–1496. doi:10.1007/s12325-018-0777-y
16. Menzies-Gow A, Jackson DJ, Al-Ahmad M, et al. A renewed charter: key principles to improve patient care in severe asthma. Adv Ther. 2022;39(12):5307–5326. doi:10.1007/s12325-022-02340-w
17. Chhaya V, Saxena S, Cecil E, et al. Steroid dependency and trends in prescribing for inflammatory bowel disease - a 20-year national population-based study. Aliment Pharmacol Ther. 2016;44(5):482–494. doi:10.1111/apt.13700
18. Fardet L, Petersen I, Nazareth I. Prevalence of long-term oral glucocorticoid prescriptions in the UK over the past 20 years. Rheumatology. 2011;50(11):1982–1990. doi:10.1093/rheumatology/ker017
19. Taylor PC, Alten R, Reino JJG, et al. Factors influencing the use of biologic therapy and adoption of treat-to-target recommendations in current European rheumatology practice. Patient Prefer Adherence. 2018;12:2007–2014. doi:10.2147/PPA.S170054
20. Crowson LP, Davids JM, Hanson AC, et al. Time trends in glucocorticoid use in rheumatoid arthritis during the biologics era: 1999–2018. Semin Arthritis Rheum. 2023;61. doi:10.1016/j.semarthrit.2023.152219
21. Kariburyo F, Xie L, Sah J, Li N, Lofland JH. Real-world medication use and economic outcomes in incident systemic lupus erythematosus patients in the United States. J Med Econ. 2020;23(1):1–9. doi:10.1080/13696998.2019.1678170
22. Yates M, MacGregor AJ, Ledingham J, et al. Variation and implications of treatment decisions in early rheumatoid arthritis: results from a nationwide cohort study. Rheumatology. 2020;59(8):2035–2042. doi:10.1093/rheumatology/kez550
23. Tran TN, King E, Sarkar R, et al. Oral corticosteroid prescription patterns for asthma in France, Germany, Italy and the UK. Eur Respir J. 2020;55(6):1902363. doi:10.1183/13993003.02363-2019
24. Bénard-Laribière A, Pariente A, Pambrun E, Bégaud B, Fardet L, Noize P. Prevalence and prescription patterns of oral glucocorticoids in adults: a retrospective cross-sectional and cohort analysis in France. BMJ Open. 2017;7(7):e015905. doi:10.1136/bmjopen-2017-015905
25. OPCRD optimum patient care research database; 2022. Available from: https://opcrd.co.uk/about-opcrd/our-team/.
26. Busse WW, Kraft M, Rabe KF, et al. Understanding the key issues in the treatment of uncontrolled persistent asthma with type 2 inflammation. Eur Respir J. 2021;58(2):2003393. doi:10.1183/13993003.03393-2020
27. Bel EH, Wenzel SE, Thompson PJ, et al. Oral glucocorticoid-sparing effect of mepolizumab in eosinophilic asthma. N Engl J Med. 2014;371(13):1189–1197. doi:10.1056/NEJMoa1403291
28. Nair P, Wenzel S, Rabe KF, et al. Oral glucocorticoid-sparing effect of benralizumab in severe asthma. N Engl J Med. 2017;376(25):2448–2458. doi:10.1056/NEJMoa1703501
29. Fan VS, Gaziano JM, Lew R, et al. A comprehensive care management program to prevent chronic obstructive pulmonary disease hospitalizations: a randomized, controlled trial. Ann Intern Med. 2012;156(10):673–683. doi:10.7326/0003-4819-156-10-201205150-00003
30. Farias R, Sedeno M, Beaucage D, et al. Innovating the treatment of COPD exacerbations: a phone interactive telesystem to increase COPD action plan adherence. BMJ Open Respir Res. 2019;6(1):e000379. doi:10.1136/bmjresp-2018-000379
31. Bardhan KD, Simmonds N, Royston C, Dhar A, Edwards CM, Rotherham IBDDUG. A United Kingdom inflammatory bowel disease database: making the efFort worthwhile. J Crohns Colitis. 2010;4(4):405–412. doi:10.1016/j.crohns.2010.01.003
32. Jenkinson PW, Plevris N, Siakavellas S, et al. Temporal trends in surgical resection rates and biologic prescribing in Crohn’s disease: a population-based cohort study. J Crohns Colitis. 2020;14(9):1241–1247. doi:10.1093/ecco-jcc/jjaa044
33. Selinger CP, Parkes GC, Bassi A, et al. Assessment of steroid use as a key performance indicator in inflammatory bowel disease-analysis of data from 2385 UK patients. Aliment Pharmacol Ther. 2019;50(9):1009–1018. doi:10.1111/apt.15497
34. Rossetti S, Actis GC, Fadda M, Rizzetto M, Palmo A. The use of the anti-tumour necrosis factor monoclonal antibody--infliximab--to treat ulcerative colitis: implications and trends beyond the available data. Dig Liver Dis. 2004;36(6):426–431. doi:10.1016/S1590-8658(04)00088-X
35. Ljung T, Karlen P, Schmidt D, et al. Infliximab in inflammatory bowel disease: clinical outcome in a population based cohort from Stockholm County. Gut. 2004;53(6):849–853. doi:10.1136/gut.2003.018515
36. Selinger CP, Parkes GC, Bassi A, et al. A multi-centre audit of excess steroid use in 1176 patients with inflammatory bowel disease. Aliment Pharmacol Ther. 2017;46(10):964–973. doi:10.1111/apt.14334
37. Kalo Z, Voko Z, Ostor A, et al. Patient access to reimbursed biological disease-modifying antirheumatic drugs in the European region. J Mark Access Health Policy. 2017;5(1):1345580. doi:10.1080/20016689.2017.1345580
38. National Health Service. Quality and outcomes framework. NHS. Available from: https://digital.nhs.uk/data-and-information/data-collections-and-data-sets/data-collections/quality-and-outcomes-framework-qof.
39. Suehs CM, Menzies-Gow A, Price D, et al. Expert consensus on the tapering of oral corticosteroids for the treatment of asthma. A Delphi study. Am J Respir Crit Care Med. 2021;203(7):871–881. doi:10.1164/rccm.202007-2721OC
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.