")
Back to Journals » Vascular Health and Risk Management » Volume 20
Trends in Lower Extremity Artery Disease Repair Incidence, Comorbidity, and Mortality: A Danish Nationwide Cohort Study, 1996–2018
Authors Møller A , Eldrup N, Wetterslev J , Hellemann D, Nielsen HB, Rostgaard K , Hjalgrim H, Pedersen OB
Received 11 August 2023
Accepted for publication 23 January 2024
Published 14 March 2024 Volume 2024:20 Pages 125—140
DOI https://doi.org/10.2147/VHRM.S427211
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roland Asmar
Anders Møller,1,2 Nikolaj Eldrup,3– 5 Jørn Wetterslev,6 Dorthe Hellemann,1,5 Henning Bay Nielsen,7,8 Klaus Rostgaard,9,10 Henrik Hjalgrim,5,9– 11,* Ole Birger Pedersen5,10,12,*
1Department of Anesthesia and Intensive Care, Næstved-Slagelse-Ringsted, Slagelse Hospital, Slagelse, Denmark; 2Department of Anaesthesia and Intensive Care, Copenhagen University Hospital - Bispebjerg and Frederiksberg, Copenhagen, Denmark; 3Department of Vascular Surgery, Rigshospitalet, Copenhagen, Denmark; 4Danish Vascular Registry, Aarhus, Denmark; 5Department of Clinical Medicine, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark; 6Private Office, Tuborg Sundpark, Hellerup, 2900, Denmark; 7Department of Anesthesia and Intensive Care, Zealand University Hospital Roskilde, Roskilde, Denmark; 8Department of Nutrition, Exercise and Sport, Faculty of Science, University of Copenhagen, Copenhagen, Denmark; 9Danish Cancer Institute, Danish Cancer Society, Copenhagen, Denmark; 10Department of Epidemiology Research, Statens Serum Institut, Copenhagen, Denmark; 11Department of Hematology, Copenhagen University Hospital, Copenhagen, Denmark; 12Department of Clinical Immunology, Zealand University Hospital, Køge, Denmark
*These authors contributed equally to this work
Correspondence: Anders Møller, Department of Anesthesia and Intensive Care, Næstved-Slagelse-Ringsted Hospital, Fælledvej 11, Slagelse, DK-4200, Denmark, Tel +45 58 55 92 02, Email [email protected]
Background: The prevalence of occlusive lower extremity artery disease (LEAD) is rising worldwide while European epidemiology data are scarce. We report incidence and mortality of LEAD repair in Denmark from 1996 through 2018, stratified on open aorto-iliac, open peripheral, and endovascular repair.
Methods: A nationwide cohort study of prospective data from population-based Danish registers covering 1996 to 2018. Comorbidity was assessed by Charlson’s Comorbidity Index (CCI). Incidence rate (IR) ratios and mortality rate ratios (MRR) were estimated by multivariable Poisson and Cox regression, respectively.
Results: We identified 41,438 unique patients undergoing 46,236 incident first-time LEAD repairs by either aorto-iliac- (n=5213), peripheral surgery (n=18,665) or percutaneous transluminal angioplasty (PTA, n=22,358). From 1996 to 2018, the age- and sex-standardized IR for primary revascularization declined from 71.8 to 50.2 per 100,000 person-years (IRR, 0.70; 95% CI, 0.66– 0.75). Following a 2.5-fold IR increase of PTA from 1996 to 2010, all three repair techniques showed a declining trend after 2010. The declining IR was driven by decreasing LEAD repair due to claudication, and by persons aged below 80 years, while the IR increased in persons aged above 80 years (p interaction< 0.001). LEAD repair was more frequent in men (IRRfemale vs male, 0.78; 95% CI, 0.77– 0.80), which was consistent over calendar time (p interaction=0.41). Crude mortality decreased following open/surgical repair, and increased following PTA, but all three techniques trended towards lower adjusted mortality comparing the start and the end of the study period (MRRaorto-iliac, 0.71; 95% CI, 0.54– 0.93 vs MRRperipheral, 0.76; 95% CI, 0.69– 0.83 vs MRRPTA, 0.96; 95% CI, 0.86– 1.07). Increasing age and CCI, male sex, smoking, and care dependency associated with increased mortality.
Conclusion: The incidence rate of LEAD repair decreased in Denmark from 1996 to 2018, especially in persons younger than 80 years, and primarily due to reduced revascularization for claudication. Adjusted mortality rates decreased following open surgery, but seemed unaltered following PTA.
Keywords: vascular surgery, critical limb ischemia, claudication, Danish Vascular Registry, Danish National Patient Registry, registers
Introduction
Atherosclerosis affects more than 200 million persons worldwide, making it a public health concern.1 Occlusive lower extremity artery disease (LEAD), which is the third leading cause of atherosclerotic morbidity after stroke and coronary artery disease, has seen a global increase in prevalence due to factors such as population growth, aging, and higher rates of diabetes and smoking in low- and middle-income countries.1,2 LEAD is prevalent in 11% of Danish men aged 65–74 years, 18% of Swedish men aged 60–90 years, and 18% of German individuals aged above 65 years.1–4 However, data on the incidence rates (IR) of LEAD diagnoses and repair are otherwise limited in Europe.2,5–7
The severity of LEAD varies, ranging from asymptomatic cases to intermittent claudication to critical limb ischemia (CLI), which includes rest pain, ulcers, and tissue loss.1 Vascular surgery may restore blood flow and has traditionally been offered for claudication and CLI. However, recent recommendations suggest that LEAD repair should be focused on CLI, while intermittent claudication should be managed conservatively with exercise and medication.2 Failure to manage CLI can lead to significant risks such as loss of ambulatory function, severe pain, infections, and amputation.8,9
The choice of revascularization technique is influenced by the availability of autogenous veins for open bypass surgery, patient comorbidity, and the complexity and location of the stenosis.10 Open vascular surgery, particularly aortic-iliac surgery, is considered high-risk due to frequent post-operative complications.11,12 This has led to the development of endovascular techniques like percutaneous transluminal angioplasty (PTA) with or without a stent. Guidelines recommend endovascular treatment for aorto-iliac disease.10 However, for peripheral occlusions recent clinical trials are conflicting. In a US trial, lower limb bypass has demonstrated superior outcomes when compared to endovascular approaches if a suitable vein is available for conduit,13 whereas a smaller UK trial reported higher mortality associated with bypass surgery.14 The proportion of endovascular techniques used for revascularization varies internationally, with Russia at 24% and Italy at 88%.6
Despite successful initial revascularization, LEAD repair often requires recurrent procedures due to loss of patency or progression of atherosclerotic lesions locally or in other vascular territories.2,9 Previous studies have mainly focused on primary revascularization, and there is a need to establish frequencies of adverse outcomes following both index and recurrent surgeries using different techniques.5 This information is essential for sample size calculations in clinical trials for LEAD repair interventions. Additionally, changing recommendations calls for an overview of the trend in LEAD repair IRs.
In this study, we aimed to describe the trends over a 23-year period in the incidence, comorbidity, and mortality of both first-time and recurrent LEAD repair. We utilized prospectively collected data from well-validated population-wide Danish registers to provide comprehensive insights into LEAD epidemiology in Denmark. The results include an analysis of the risk factors associated with the observed incidence- and mortality rates. In an accompanying manuscript, we have also documented the epidemiology of abdominal aortic aneurysm repair in Denmark from 1996 to 2018.15
Methods
Study Design and Setting
We conducted a nationwide, longitudinal cohort study on prospectively collected data from the Danish Vascular Registry (DVR) and population-based medical and administrative registers.16 The Danish National Health Service ensures tax-supported healthcare to all Danish citizens. The Danish Civil Registration System (CPR), established in 1968, enables individual-level linkage across registers.17 The Danish population was 5,781,190 persons in 2018.
Study Population
We used the DVR to identify Danish patients undergoing LEAD repair from January 1st, 1996 to December 31st, 2019. The 2019 data, however, were exclusively used graphically in the standardized incidence rate plot, not in any tables or the result section, as we did not have Danish National Patient Registry (DNPR) data for 2019.
LEAD repair was classified as either open aorto-iliac surgery, open peripheral surgery, or endovascular (PTA). If multiple records fulfilled the inclusion criteria on the same day, we selected the most comprehensive surgical procedure using the following hierarchy reflecting the magnitude of surgical trauma: i) aorto-iliac surgery (aorto-iliac > iliac) > ii) peripheral axillo(bi)femoral bypass > peripheral open lower limb bypass (below knee > above knee > femoro-femoral crossover graft) > endarterectomy > iii) isolated PTA. Hybrid procedures were reported as peripheral surgery when open arterial reconstruction was combined with PTA during normal working hours 08:00 to 18:00. This timeframe was chosen to exclude reoperations on the same day.
If a patient had both an aneurysm and LEAD indication registered in the DVR variables (3 indications can be entered per record), aneurysm was chosen as the main indication, and the patient was excluded from the population in this study and included in the accompanying manuscript.15 The methods used in the two studies were alike, except that patients undergoing LEAD repair could be included more than once as described in the following.
If a patient had undergone multiple LEAD repairs, and the two cases were more than 90 days apart, the patient could enter one of the other two LEAD repair groups, but patients were not reported in the same group twice. Ninety days were chosen as the cut-off timeframe to limit the reporting of reoperations or redo surgery of the same atherosclerotic lesion because graft patency loss occurs in around 5–8% at discharge in Danish patients and 8–14% by day 30 in Swedish patients.7 The baseline table provides details on vascular repair history and we used a Sankey plot to visualize how patients changed LEAD repair technique/group.
The DVR was established in 1996 for quality improvement and research purposes and contains prospective data on all vascular procedures.18 Patient data are registered into DVR prospectively. The DVR is continuously validated against the DNPR for the most frequent procedures, infra-inguinal bypass, abdominal aortic aneurysm, and carotid endarterectomies with data completeness of 95%.18 We used the CPR to add information on sex, age, vital status, and migration. The CPR version was last updated on October 31st, 2019. From the Danish National Patient Registry (DNPR), we gathered information on all somatic inpatient hospitalizations since 1977 and all hospital outpatient and emergency visits since 1995, including discharge diagnoses according to the International Classification of Diseases [Eighth Revision (ICD-8) until 1993 and Tenth Revision (ICD-10) hereafter].19 The DNPR data set was last updated on May 7th, 2020.
Inclusion was based on the DVR and the criteria were i) operation code relevant to aortoiliac or lower extremity reconstruction with details provided in the Supplementary Data . ii) indication being either claudication, rest pain, or wound/gangrene defined by the DVR-variable “GC_PI_INDIK1” takes on the value 16–19. iii) age above 40 and below 100 years. The age cut-off was chosen to fit the general vascular surgery target population as used in previous trials.20 Exclusion criteria were i) acute limb ischemia using the DVR, and ii) patients with LEAD repair before 1996 using the DNPR to ensure all patients were LEAD repair naive at entry into our study base; criteria are provided in the Supplementary Data.
We use the term surgery for open procedures, peripheral and aorto-iliac surgery. The common term for all three techniques was repair.
Comorbidity
Patients were described at baseline by Charlson’s Comorbidity Index (CCI) score using both in- and outpatient records in the DNPR accrued since 1977.21 We exclusively used DNPR records concluded before the date of surgery, so peripheral vascular disease diagnosed on the day of surgery or in ongoing outpatient records could not contribute to the CCI score. We grouped patients with a CCI score of 0, 1, 2, or 3 and above, as having normal, moderate, severe, or very severe comorbidity, respectively. We chose moderate CCI as the reference group because peripheral vascular disease accounts for one CCI point. Baseline characteristics disaggregated by calendar period are available in the Supplementary Data.
Mortality
We obtained vital status from the CPR and reported 5-year survival following LEAD repair. Five-year survival was the primary analysis, as open and endovascular repair may have different short- and long-term mortality.
Statistical Analyses
Aorto-iliac surgery, peripheral surgery, and PTA were analyzed separately and only aggregated for the incidence reporting of any first-time repair (ie, primary revascularization). We described the population by sex, age group (of six decades from 41 to 99 years), CCI group, and calendar period (5 intervals from 1996 to 2018). We exclusively included the year 2019 in the age-and sex-standardized incidence plots.
Based on the CPR, we identified residents in Denmark aged above 40 and below 100 years as of January 1st from 1996 to 2019. We computed each resident’s annual accrued CCI score using the DNPR and calculated person-years at risk for LEAD operation in the population as follow-up time resident in Denmark by age, sex, calendar year, and CCI group. Incidence rates (IR) were reported as i) crude IRs by calendar period, age, sex, and CCI group, ii) adjusted IR ratios (IRR) using a log-linear Poisson regression model including the covariates: calendar period, age category, sex, and CCI group offset by the logarithm of person-years at risk, and iii) annual IRs standardized to the year 2000 age- and sex composition of the Danish population using direct standardization.
To compare the CCI of LEAD patients to the Danish population, we calculated a mean observed CCI by each sex-, age-, and calendar year strata and standardized this to the Danish population’s corresponding strata of the year 2000, as a reference. We then used Poisson regression to estimate CCI ratios with 95% confidence intervals. The same method was applied to compare CCI ratios across age groups with persons aged 71–75 years as a reference.
Five-year mortality risks were computed using the Kaplan-Meier estimator. Patients were censored five years following surgery, on migration, or on October 31st, 2019, whichever occurred first. Using Cox regression, we calculated the five-year mortality rate ratio (MRR, via hazard ratios for death) for each calendar period. We present crude MRR, and MRRs adjusted for age, sex, CCI group, health care region (five regions), tobacco use (none, previous, smoker), alcohol abuse (no, >5 units/day), and care dependency (independent, home care, nursing home), priority (elective, subacute, acute), and stratified for surgical sub-technique when relevant (aorto-iliac surgery stratum: aorto-iliac vs isolated iliac surgery. Peripheral surgery stratum: open bypass or endarterectomy vs hybrid vs axillobifemoral bypass. PTA: no stratum). In the adjusted survival analysis, the set of confounders adjusted for varied between exposures to maintain causal methodological coherence.22 Missing data were included as separate parameter levels (dummy variables) in the analyses. In our secondary analysis, we ran a Cox model excluding variables with missing data (tobacco, alcohol, care dependency, priority).
The adequacy of the models for estimating incidence and mortality was examined by tentatively adding an interaction term between calendar year, as a linear predictor, and each of the remaining covariates. The effect of adding an interaction term was assessed by the likelihood ratio test.
The increase in mean age over the study period was calculated by univariate linear regression.
Ethics
The study was submitted to Region Zealand’s record of research-related processing activities (record no. REG-144-2017) and was approved by Statens Serum Institut, SSI QA and Compliance (journal no. 21/00805). We did not need to obtain permission from the Danish Ethical Committee as this study did not involve contact with study participants. The accessed data complied with relevant data protection and privacy regulations.
Results
We identified 46,236 incident arterial reconstructions for LEAD based on 41,438 unique patients registered in the DVR from 1996 to 2018. See Supplemental Material for the study flow chart, eFigure 1. Figure 1B, the Sankey plot, visualizes how patients changed groups in case of recurrent LEAD repair. 4646 patients underwent more than one type of LEAD repair with a median number of months from first to second revascularization of 32 months (interquartile range, 11 to 72). Of those patients, 151 underwent a third procedure, and thus all three types of LEAD repair with a median time elapsed between the second and third repair of 25 months (interquartile range, 11 to 63). The Supplemental Material provides further details on the Sankey plot, including the count of recurrent repair patients in eFigure 2 and an alternative Sankey plot presentation in eFigure 3.
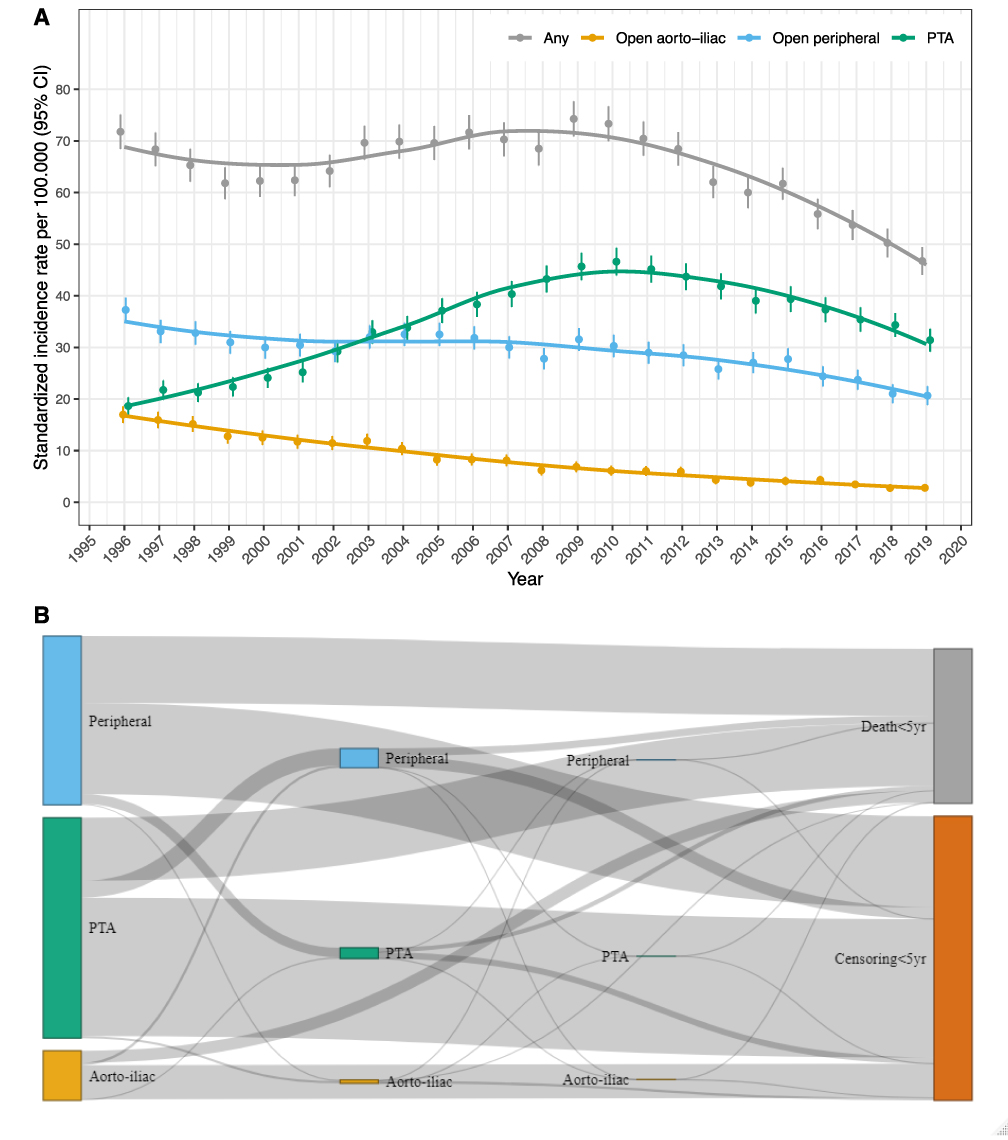 |
Figure 1 Standardized incidence rate by technique (A) and Sankey plot visualizing the distribution of techniques used for vascular repair between 90 days and 5 years following primary revascularization (B). Notes: (A) Incidence rate standardized to the age and sex distribution of the Danish population aged above 40 and below 100 years in 2000. Note, the 2019 data are exclusively used graphically in this plot and not in any tables or the result section, as we did not have Danish National Patient Registry (DNPR) data for 2019. (B) The size of each node (box) corresponds to the number of patients having vascular repair for occlusive lower extremity artery disease (LEAD) for that technique. The three nodes in the far left of the figure represents any first-time “primary” LEAD repair (grey line in panel A above). First-time peripheral vascular surgery is represented by the three blue colored nodes (blue line in panel A). Correspondingly, PTA is colored green, and aorto-iliac surgery is colored light orange. Please refer to baseline Table 1 under “Vascular Surgical history” for details on LEAD repair history by each group. As patients could not be reported in the same group twice, the third column of nodes (the smallest nodes to the right of the middle and to the left of the censoring and death nodes) are patient that had undergone all three LEAD repair techniques. Exclusive to the Sankey plot visualization, we censored patients 5 years following LEAD repair since the most frequent technique changed over time. |
Incidence Rate
The age- and sex-standardized incidence rate for primary revascularization (any first-time LEAD repair) decreased from 71.8 to 50.2 per 100,000 person-years between 1996 and 2018, Figure 1A; corresponding to a 30% decline (IRR, 0.70; 95% CI, 0.66 to 0.75). When adjusting for age, sex, and CCI, the decline in incidence rate was 40% (IRR, 0.60, 95% CI, 0.58 to 0.62; Figure 2).
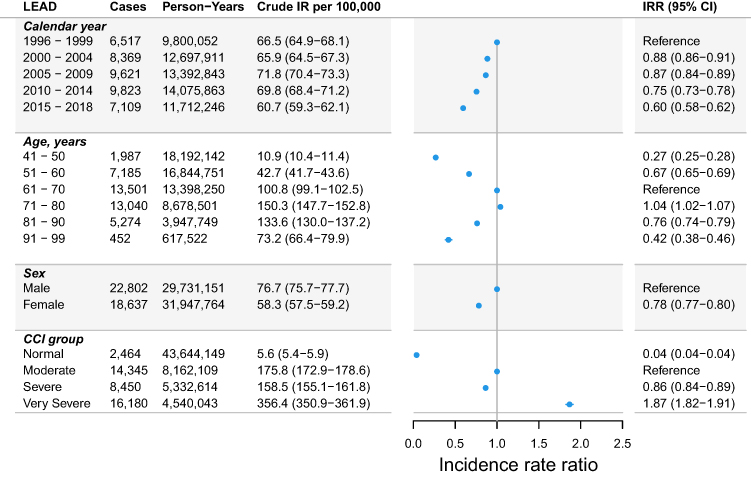 |
Figure 2 Incidence rate of primary vascular repair for lower extremity artery disease. Abbreviations: CCI, Charlson’s comorbidity index; CI, confidence interval; IR, incidence rate; IRR, incidence rate ratio; LEAD, lower extremity artery disease. Notes: Shows the crude incidence rate (IR) and adjusted incidence rate ratio (IRR) with Forest plot of primary repair for lower extremity artery disease (LEAD). The IRRs were computed by a multivariable Poisson regression model adjusted for calendar year, age group, sex, and Charlson’s comorbidity index (CCI) score. The CCI score was based on records concluded before the date of surgery, which meant that LEAD diagnosed on the day of repair, or in ongoing outpatient records, could not contribute to the CCI score. Thus, some patients were characterized with normal CCI. |
From 1996 to 2018, there was a steady IR decline of both aorto-iliac surgery from 17.0 to 2.8 per 100,000 person-years (Figure 1A) corresponding to an 84% decrease (IRR, 0.16; 95% CI, 0.13 to 0.20), and in peripheral surgery from 37.3 to 21.0 per 100,000 person-years (Figure 1A) corresponding to a 43% decline (IRR, 0.57; 95% CI, 0.51 to 0.63). For PTA, the IR trend varied over time with a 2.5-fold IR increase from 18.6 to 46.6 per 100,000 person-years (Figure 1A) between 1996 and 2010 followed by an IR decrease to 34.3 per 100,000 person-years in 2018. Overall, the IR of PTA increased by 87% from 1996 to 2018 (IRR, 1.87; 95% CI, 1.67 to 2.08, Figure 1A).
Incidence by Age and Sex
Figure 2 presents the age-, sex-, CCI-, and calendar year-adjusted IR of primary revascularization, which was highest in patients aged 71–80. Overall, we observed significant age heterogeneity in the IR trend with a decreasing IR in persons up to 80 years and an IR increase in persons older than 80 years (p interaction < 0.001, eTable 1) and this was observed for all types of LEAD repair. However, eFigure 4 reveals a declining IR of primary revascularization for all age groups from 2015 to 2018. A heat map of age-specific incidence rate per calendar year is shown in eFigure 5, stratified by sex in eFigure 6.
LEAD repair was more common in men than in women (IRRfemale vs male, 0.78; 95% CI, 0.77 to 0.80), but for aorto-iliac surgery, the IR was equal between the two sexes (Figure 3). Overall, there was no sex heterogeneity in the IR change over time (Annual percent change (APC)male −0.7% vs APCfemale −0.8%, p interaction=0.41).
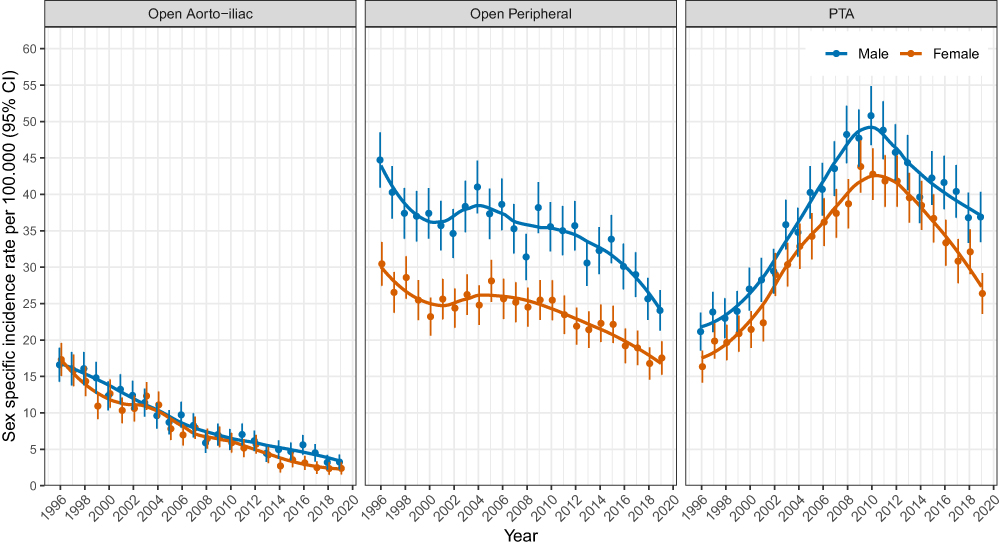 |
Figure 3 Sex specific incidence rate in repair for lower extremity artery disease. Notes: Sex-specific trends in the incidence rate of LEAD repair, standardized to the age distribution of the Danish population in 2000. |
Incidence by Comorbidity
LEAD repair was exceedingly rare in persons with no history of comorbidity in the DNPR (IRR, 0.04; 95% CI, 0.04–0.04), and most frequent in the population with very severe comorbidity (IRR, 1.87; 95% CI, 1.82–1.91), compared to moderate comorbidity (Figure 2). The trend in CCI-specific IR is plotted in eFigure 7.
Incidence by Indication and Technique
The age- and sex-standardized IR of primary revascularization for claudication increased between 1996 and 2009 from 31.5 to 44.8 repairs per 100.000 person-years, followed by a steady decline to 22.0 repairs per 100.000 person-years in 2018. Overall, the standardized IR decreased for other indications than wound/gangrene (APCclaudication −0.43%; 95% CI, −0.63 to −0.23 vs APCpain at rest −0.46%; 95% CI, −0.77 to −0.16 vs APCwound/gangrene +0.21%; 95% CI, −0.03 to +0.45, eFigure 8).
Figure 4 shows the indication-specific standardized IR by vascular repair technique. The IR declined in surgical revascularization for all indications, and especially aorto-iliac surgery performed on the claudication indication decreased markedly from 9.7 to 1.2 surgeries per 100.000 person-years between 1996 and 2018. The standardized IR of PTA increased for all indications over the study period; with marked variation in the claudication indication which increased 2.4-fold from 12.2 to 29.0 repairs per 100.000 person-years between 1996 and 2009 followed by a steep decline to 14.9 repairs per 100.000 person-years in 2018.
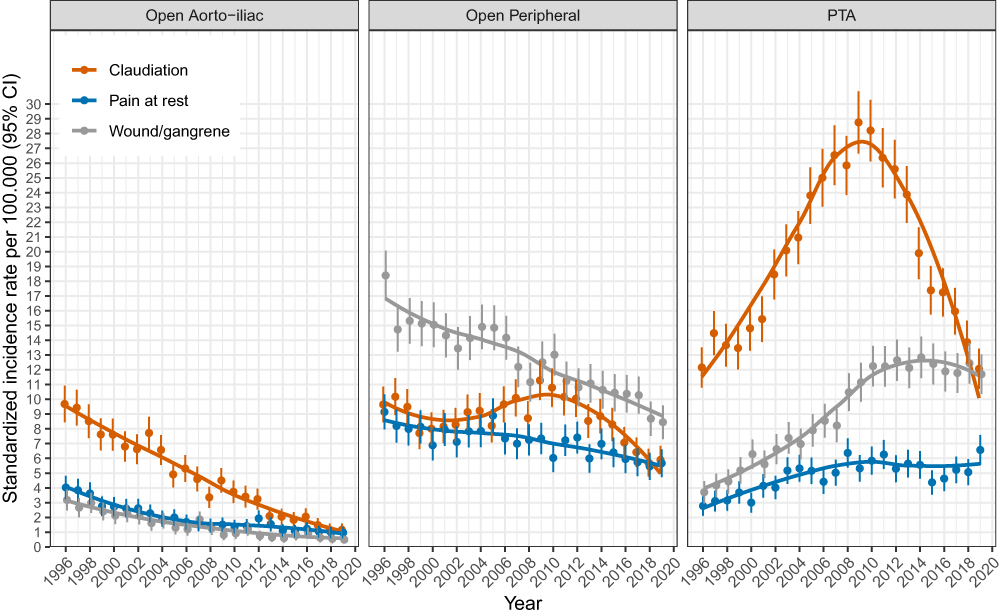 |
Figure 4 Indication specific standardized incidence rate in repair for lower extremity artery. Abbreviation: PTA, percutaneous transluminal angioplasty. Notes: Incidence rate of revascularization for occlusive lower extremity artery disease by technique and indication, standardized to the age- and sex-composition of the Danish population in the year 2000. |
Patient Characteristics
Table 1 shows the baseline characteristics of patients undergoing aorto-iliac surgery (n=5213), open peripheral surgery (n=18,665), and PTA (n=22,358). Aorto-iliac surgery patients were younger at baseline with a mean age of 64 years compared to 71 years in the peripheral surgery and 69 years in the PTA group. From 1996 to 2018 the mean age increased by 1.26 years in aorto-iliac surgery, by 1.08 years in peripheral surgery, and by 6.10 years in PTA (eFigure 9).
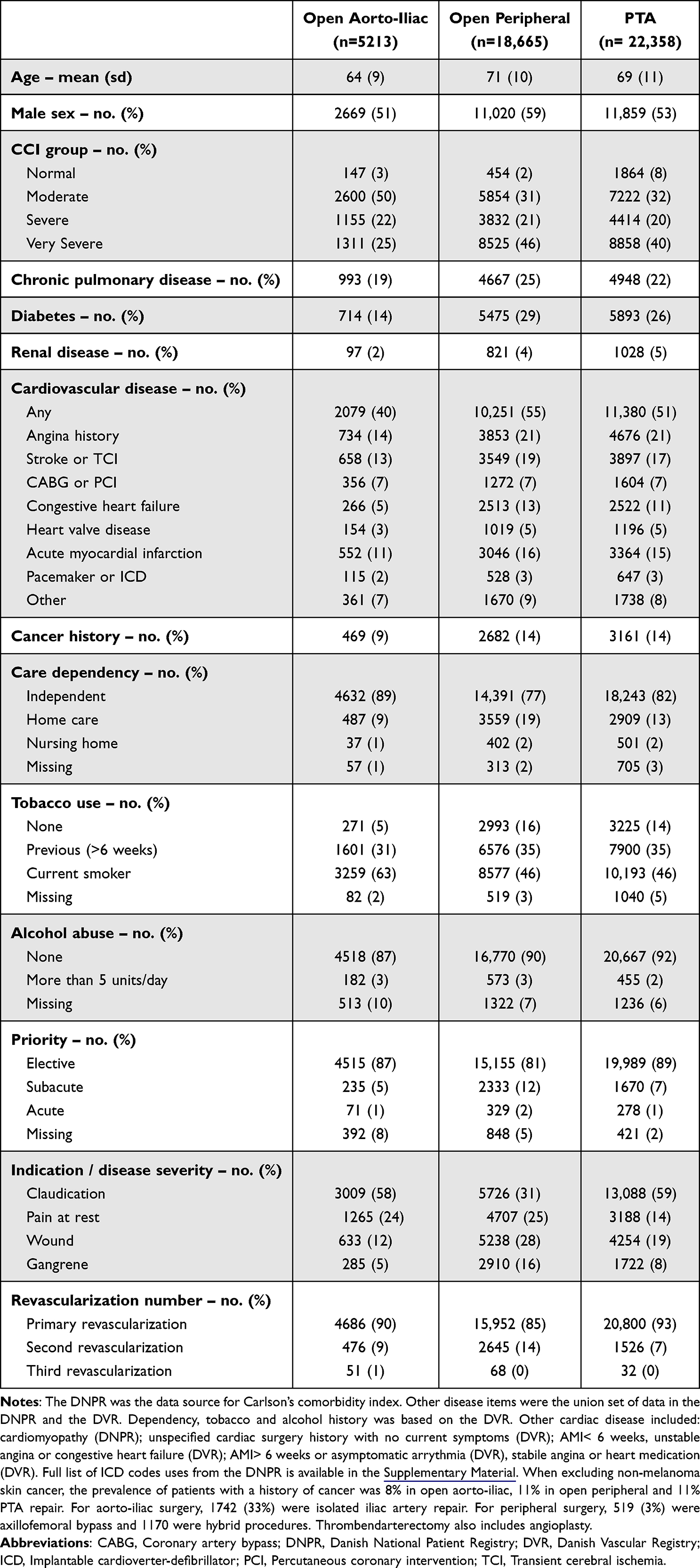 |
Table 1 Baseline Characteristics of Patients Undergoing Surgery for Lower Extremity Artery Disease in Denmark 1996–2018 |
Aorto-iliac surgery patients most frequently had moderate comorbidity (50%), whereas very severe comorbidity was most prominent in peripheral surgery- and PTA patients (46% and 40%, respectively). Diabetes was prevalent in 29% of peripheral surgery patients, 26% of PTA patients, and 14% of patients undergoing aorto-iliac surgery. Notably, 15% of patients in the peripheral group had undergone previous LEAD repair, whereas this was only the case for 10% of patients in the aorto-iliac group and for 7% of PTA patients.
Compared to the Danish population during the study period, the age- and sex-adjusted CCI-score was 2.91-fold higher in open aorto-iliac surgery (95% CI, 2.85−2.97), 2.82-fold higher in peripheral surgery (95% CI, 2.79−2.85), and 2.71-fold higher in PTA patients (95% CI, 2.68−2.73). The APC in CCI was 0.3% for aorto-iliac surgery (95% CI, 0.0–0.7%), 0.8% in peripheral surgery (95% CI, 0.7–1.0%), and 0.7% in PTA patients (95% CI, 0.5–0.8%), compared to 2.4% (CI 95%, 2.4–2.4%) in the Danish population. For a more detailed presentation, see eFigure 10.
Figure 5 shows the sex- and calendar-year-adjusted increase in CCI by age. The CCI peaked in LEAD repair patients aged 76–85 years followed by a declining trend in CCI. In the Danish residents, the CCI peaked in age group 86–90 years before declining. PTA was the only LEAD repair group that demonstrated a higher CCI for age groups 76 to 85 compared to the reference age group, 70–75 years.
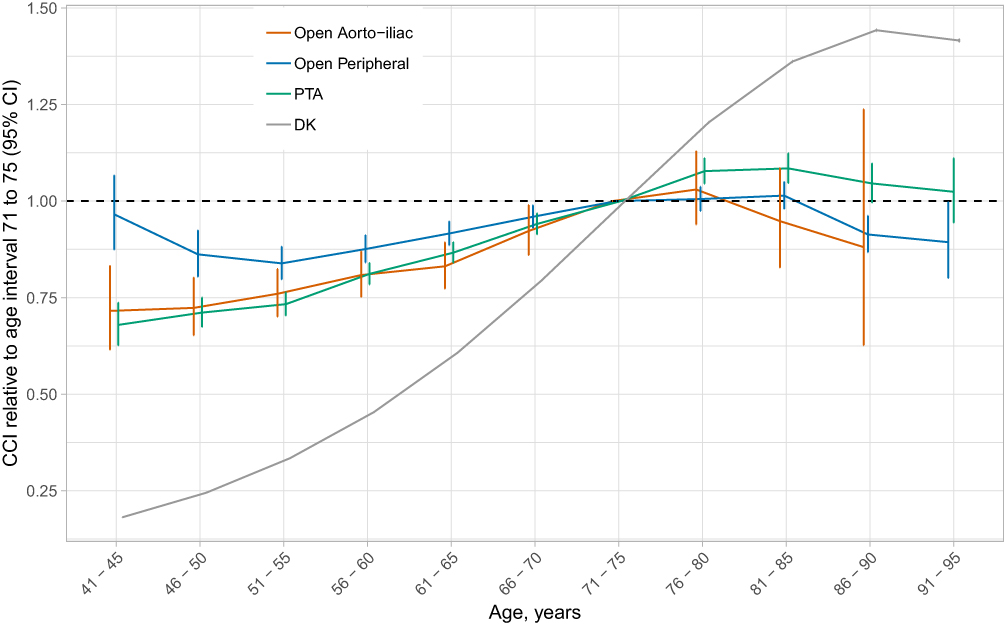 |
Figure 5 Age trend in Charlson’s comorbidity index score relative to age group 71–75 by population. Abbreviations: DK, The Danish population; PTA, percutaneous transluminal angioplasty. Notes: Age trend in Charlson’s comorbidity index (CCI) score presented as ratios standardized to the calendar year and sex distribution of persons aged 71–75 years within each population. The bars indicate the 95% confidence intervals and were computed by Poisson regression including the covariates calendar year, age, sex and CCI score. |
Mortality
Table 2 shows the mortality risks, and the crude- and adjusted mortality rates of the three techniques over the study period. Comparing the calendar period 2015–2018 to 1996–1999, the crude mortality rate reduced by 22% to 27% in open surgery (MRRaorto-iliac, 0.73; 95% CI, 0.57–0.95 vs MRRperipheral, 0.78; 95% CI, 0.71–0.85) and increased by 33% in PTA (MRRPTA, 1.33; 95% CI, 1.21–1.47). In the adjusted analyses, mortality rates reduced by 24–29% following open surgery and by 4% following PTA (MRRaorto-iliac, 0.71; 95% CI, 0.54–0.93 vs MRRperipheral, 0.76; 95% CI, 0.69–0.83 vs MRRPTA, 0.96; 95% CI, 0.86–1.07).
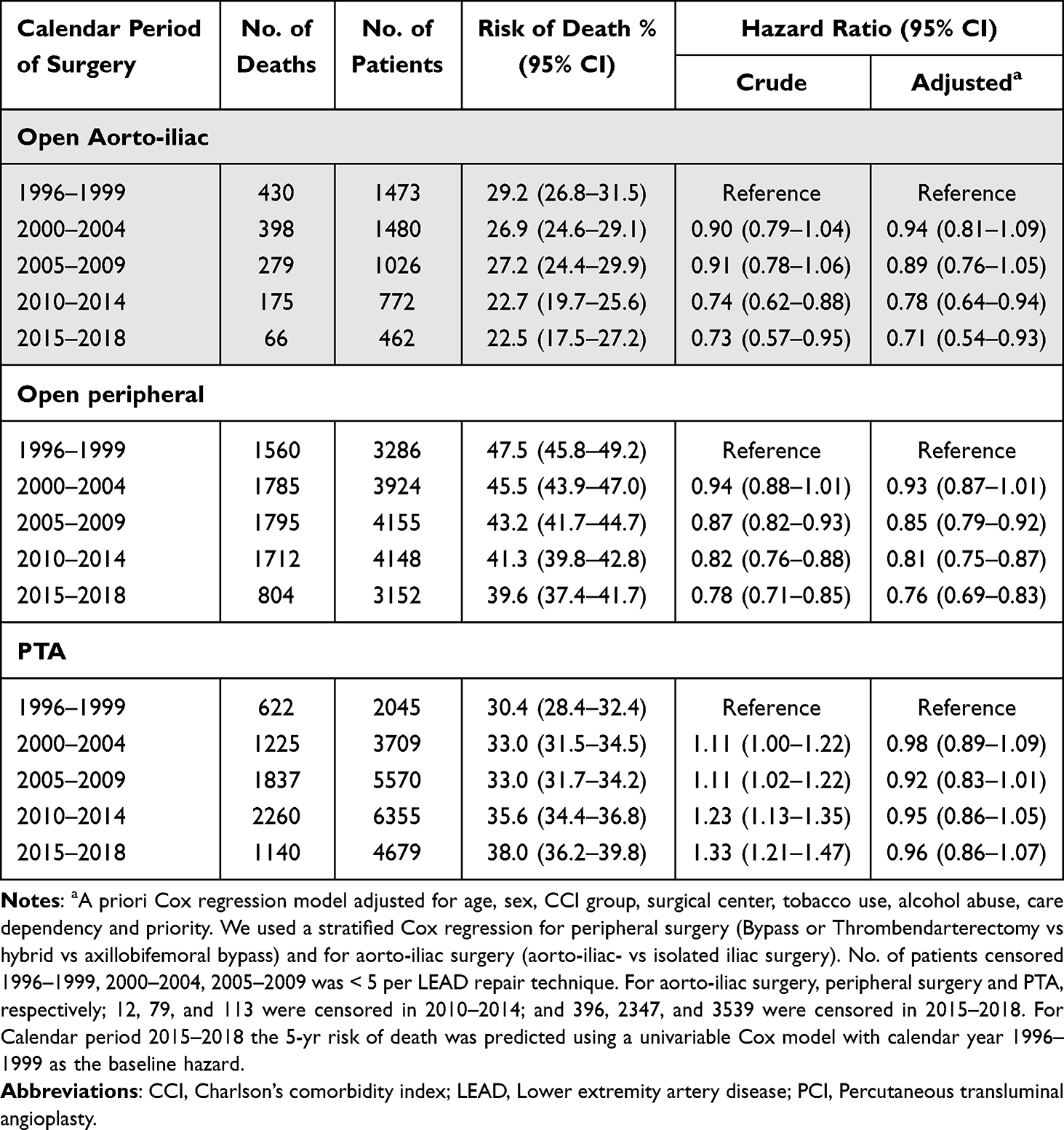 |
Table 2 Five-Year Mortality Following LEAD Surgery in Denmark 1996–2018 |
In a secondary analysis, where we excluded covariates with missing data (tobacco, alcohol, care dependency, priority), a more pronounced reduced mortality rate was demonstrated for all three LEAD repair techniques (MRRaorto-iliac, 0.62; 95% CI, 0.48–0.81 vs MRRperipheral, 0.65; 95% CI, 0.59–0.71 vs MRRPTA, 0.88; 95% CI, 0.80–0.98) however, when adjusting for tobacco use and care dependency, which both were significant risk factors for mortality and were less frequent at the end of the study period (eTable 2), the adjusted MRR estimate increased toward one by 0.09 to 0.11 (eTables 3 and 4). Thus, tobacco use and care dependency largely explained the estimate differences between the two models.
Case priority was poorly registered in 1996 with 90% missingness followed by <1% missingness in the following years. When excluding priority from the primary analyses, the adjusted 5-year MRR increased by 0.01, 0.04, and 0.03 in aorto-iliac surgery, peripheral surgery, and PTA, respectively.
When also adjusting the primary analyses for previous vascular repair during the study period, the point estimates of the adjusted 5-year MRR decreased by 0.00 to 0.01 for the three repair techniques.
The 5-year mortality rate was also reduced in the Danish population aged 41–99 during the same period ([sex, age, and CCI-adjusted MRR, 0.56; 95% CI, 0.56–0.56]; [sex and age-adjusted MRR 0.72; 95% CI, 0.72–0.72]; eFigure 11).
Mortality by Age, Sex, Comorbidity, and Smoking
The models in this section are adjusted for calendar year, age, and sex.
Compared to the reference age group 61–70 years, the adjusted five-year mortality rate increased significantly in patients aged 71–80 years and especially in aorto-iliac surgery (MRRaorto-iliac, 2.10; 95% CI, 1.85–2.38 vs MRRperipheral, 1.55; 95% CI, 1.47–1.64 vs MRRPTA, 1.79; 95% CI, 1.68–1.90). The age effect on mortality did not change over calendar time (P interactionaorto-iliac=0.56, P interactionperipheral=0.09, P interactionPTA=0.24).
Compared to males, females had a 20% to 27% reduced adjusted 5-year mortality (MRRaorto-iliac, 0.80; 95% CI, 0.72–0.89 vs MRRperipheral, 0.78; 95% CI, 0.74–0.81 vs MRRPTA, 0.73; 95% CI, 0.70–0.77), which was independent of calendar time (P interactionaorto-ilica= 0.34, P interactionperipheral=0.10, P interactionPTA=0.42).
Compared with moderate comorbidity, severe comorbidity associated to a 43% to 51% higher adjusted five-year mortality rate (MRRaorto-iliac, 1.43; 95% CI, 1.24 to 1.65 vs MRRperipheral, 1.51; 95% CI, 1.41–1.62 vs MRRPTA, 1.49; 95% CI, 1.38 to 1.61); and very severe comorbidity associated to a 120% to 149% higher adjusted MRR (MRRaorto-iliac, 2.20; 95% CI, 1.94 to 2.49 vs MRRperipheral, 2.33; 95% CI, 2.20 to 2.46 vs MRRPTA, 2.49; 95% CI, 2.34 to 2.65). The mortality rate changed similarly over time for all CCI subgroups (P interaction > 0.47 for all three repair techniques).
Compared to no tobacco use, registered smoking was associated with a 10% greater age, sex, and calendar year-adjusted mortality rate in peripheral surgery (MRRaorto-iliac, 1.14; 95% CI, 0.92 to 1.43 vs MRRperipheral, 1.10; 95% CI, 1.03 to 1.17 vs MRRPTA 1.00; 95% CI, 0.93 to 1.07).
Mortality by Care Dependency
Compared to care independence, patients with home care had an 85% to 120% higher age, sex, CCI, and calendar year-adjusted mortality rate (MRRaorto-iliac, 1.85; 95% CI, 1.60–2.14 vs MRRperipheral, 1.92; 95% CI, 1.82–2.03 vs MRRPTA 2.20; 95% CI, 2.07–2.33).
Discussion
In this nationwide register study of LEAD repair epidemiology, we observed a 30% IR decline of first-time LEAD repair in the Danish population from 1996 to 2018, mainly due to reduced repair from claudication and in individuals below 80 years. Opposingly, repair became more frequent in persons above 80 years due to increased use of PTA in this age group. The adjusted mortality rates decreased following open surgery and seemed unaltered following PTA despite increasing age and comorbidity. Age, male sex, CCI group, care dependency and smoking were important predictors of mortality.
Incidence Findings
Comparing our results with other studies is challenging due to evolving LEAD definitions.23 Most LEAD repair studies focus on disease prevalence, or surgical caseload without taking alterations in the sex- and age-composition of the risk population into account.6,7 However, a UK national representative cohort study established a 15% decline (IRR, 0.85; 95% CI, 0.82–0.88) in the standardized incidence of peripheral artery disease diagnoses from 2006 to 2015 which seems lower than our finding, as we observed an approx. 22% IR reduction in first-time LEAD repair from ~ 71 to 56 per 100.000 person-year between 2006 and 2015 (Figure 1).24
The IR for LEAD peaked at age 71–80 years in our study. The mean age was around 71 years for peripheral surgery, which is comparable to an international report.6
LEAD prevalence is generally higher in men than in women, except in low- and middle-income countries.2 Our study found a 22% lower IR in females, with the proportion of women ranging from 49% in aorto-iliac to 41% in peripheral surgery. This is higher than the 25–43.5% reported in other Western countries from 2005–2017.6,7 This variation from previous studies may reflect a historically high prevalence of smoking among Danish women and/or other socio-demographic differences between Denmark and the other reporting countries.25
The IR by comorbidity was 87% higher in the population with very severe comorbidity compared with moderate comorbidity. This finding may not be surprising as vascular surgical patients are notoriously comorbid.26,27
The overall decrease in Denmark’s LEAD repair IR could be due to reduced patient risk factors, increased use of secondary atherosclerosis prophylaxis, and changes in repair policies, because conservative management of claudication (medicines, exercise) is currently promoted.2 Despite reduced tobacco consumption and increased use of secondary preventive antihypertensive-, antithrombotic- and lipid-lowering drugs in Denmark,25,28 the male claudication prevalence has remained stable from 2010 to 2016,3,4 which might be explained by improved survival among persons with claudication. Diabetes mellitus and smoking are the most significant risk factors for LEAD development,29 and while glycemic control may have improved, diabetes prevalence is rising in Denmark.30 More distal, atherosclerotic ulcerations are pathognomonic to LEAD following diabetes.10,31 In line with this, we found that the IR of LEAD repair due to wound/gangrene was temporally more stable than the IR of LEAD repair due to claudication and pain at rest.
Our results are consistent with the decreasing IR of first-time hospitalization for acute myocardial infarction in Denmark from 1984 to 2008, which may be less influenced by surgical or cardiologic selection, as it includes all diagnoses regardless of subsequent coronary intervention.32 Our findings contribute to the general picture of the trends in atherosclerosis in Denmark, by showing that the health care burden from atherosclerosis requiring LEAD repair is now coming down, predominantly in the younger age groups.
Patient Characteristics
The most striking change in patient characteristics was a six-year increase in age of PTA patients as opposed to only one year increase in age for open surgery. Additionally, the CCI increased over calendar time independently of age and sex. The age effect on CCI score varied by population. Patients undergoing open vascular surgery peaked in CCI at the age 71–80 years, PTA patients at the age of 81–85 years, while the Danish population’s CCI peaked at age 86–90 years before declining. These findings likely reflect the underlying selection of the patients for the surgical procedures; that patients with both advanced age and comorbidity may be more likely to be offered PTA due to this revascularization technique being less invasive.
When comparing the CCI scores of patients in our cohort to Danish patients hospitalized for acute myocardial infarction and hip fracture from approximately 1980 to 2010, we found that the CCI scores were substantially higher in the LEAD repair patients. The proportion of patients with no/normal comorbidity in our cohort was rare at around 8%, whereas it ranged from 64% to 75% for acute myocardial infarction patients and 33% to 66% in hip fracture patients.32,33
Diabetes was prevalent in 14% of aorto-iliac surgery patients, set against 29% in peripheral surgery and 26% in PTA. This may partially be confounded by age as diabetes 2 increases with age and aorto-iliac patients were younger.30 It may also be explained by a different set of risk factors for the central and peripheral stenoses. Diabetes more often causes more general and distal lower extremity atherosclerotic occlusions, as opposed to aorto-iliac lesions which are more often caused by smoking and hypercholesterolemia.10
Mortality Findings
A key mortality finding is an improved survival following surgical revascularization, but rather unaltered survival following PTA. This could indicate that endovascular treatment is increasingly offered to patients who are more comorbid and frailer, and for whom surgery is considered too risky. This indicates that the results may be confounded by unknown risk factors that are not captured in the Danish registers. The severity and complexity of the atherosclerotic stenosis itself may also have a causal link with mortality,34 and these details are not registered into the DVR as they are difficult to condense into covariates. Historically, severe lesions have been managed with open surgery, but recent PTA techniques have provided a treatment option for widespread stenoses in the aorta, iliac, and peripheral arteries that were previously not suitable for endovascular therapy.
Age was a significant risk factor for the adjusted 5-year mortality rate, particularly following aorto-iliac surgery. The mortality rate doubled for patients in their 70s compared to those in their 60s in aorto-iliac surgery, while there was only a 50% increase in mortality for less invasive procedures like peripheral surgery and PTA. This finding substantiates the general clinical impression, that patients with advanced age are particularly vulnerable to open aortic-iliac surgery.
We established several important mortality predictors and confounders for the trend in mortality. For aorto-iliac and peripheral surgery, both crude and adjusted 5-year mortality rates were reduced by approximately 25% over the study period. Following PTA, the crude mortality rate increased by 33%, while the adjusted estimate (IRR=0.96) indicated unaltered survival. For all three repair techniques, adjusting for age, CCI, and healthcare region demonstrated reduced adjusted mortality rates. However, adjusting for tobacco use and care dependency increased the estimates for all three procedures, likely due to a reduction in active smokers and care dependent patients over the study period, which is supported by the general pattern in Denmark.25,35 The analyses leave us with the general impression, that innovations in endovascular techniques have led to a shift in repair from open surgery to PTA in older patients who potentially have more complex atherosclerotic lesions and co-morbidities. This likely explains the divergent mortality finding between the LEAD repair groups.
Strengths and Limitations
Strengths of our study include a longitudinal design spanning twenty-three years of data from well-validated registers securing completeness, and enabling estimation of sex-, age-, and comorbidity-specific incidence and mortality rates following both primary and recurrent LEAD repair using other techniques.
However, there are some limitations to consider. Firstly, the variable of care dependency, which was a significant confounder for mortality, has not been validated in the DVR, which could impact the accuracy of our mortality findings.36,37 Secondly, the study lacks IRs for LEAD diagnoses due to a low positive predictive value in the DNPR of 70–90%.38,39 This may have introduced bias in the observed IR, as altered surgical selection including conservative management of claudication has been introduced over the study period. Thirdly, the differences in adjusted mortality rates between open/surgical vs endovascular repair may be biased by unknown patient risk factors, as PTA is increasingly being offered to older and more frail patients with complex and severe atherosclerotic lesions that were previously managed by open repair. Fourthly, the temporal CCI increase in LEAD patients may be due to increased diagnosis registration at discharge, despite reimbursement for registration in the Danish healthcare system throughout the study period. Finally, it is important to note that extrapolation of these findings to other countries might be limited because of differences in risk behavior and clinical practice.
Conclusion
In conclusion, our study showed an overall declining IR of LEAD repair in the Danish population, increasing IR and shift towards endovascular treatment of persons aged above 80 years, and reduced LEAD repair due to claudication. Adjusted five-year mortality rates declined following open surgery, and despite changes in patient characteristics remained stable following PTA.
Acknowledgments
The authors wish to thank the vascular surgeons and secretaries for data entry into the Danish Vascular Registry. We also wish to thank all other health care personnel for data registration into the Danish national registers.
A. Møller was enrolled as a PhD student at the University of Copenhagen while preparing data for analysis for this manuscript as a partial fulfillment of the requirement for the PhD. A preliminary account of the results were included in the thesis of A. Møller and is available on the institutional website: https://ctu.dk/wp-content/uploads/2021/08/Anders-Moller_PhD-thesis.pdf.
Funding
This work was supported by the local research fund of Region Zealand, Naestved, Slagelse, Ringsted Hospital (2015-01- 315 26; A. Møller) and by Region Zealand Health Research Fund (RSSF, PFI) (15-000342; A. Møller). The funds had no role in study design; management, analysis, and interpretation of data; report writing; or the decision to submit the report for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fowkes FG, Rudan D, Rudan I, et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet. 2013;382(9901):1329–1340. doi:10.1016/S0140-6736(13)61249-0
2. Aboyans V, Ricco JB, Bartelink MEL, et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteriesEndorsed by: the European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur Heart J. 2018;39(9):763–816. doi:10.1093/eurheartj/ehx095
3. Lindholt JS, Rasmussen LM, Sogaard R, et al. Baseline findings of the population-based, randomized, multifaceted Danish cardiovascular screening trial (DANCAVAS) of men aged 65–74 years. Br J Surg. 2019;106(7):862–871. doi:10.1002/bjs.11135
4. Lindholt JS, Sogaard R. Population screening and intervention for vascular disease in Danish men (VIVA): a randomised controlled trial. Lancet. 2017;390(10109):2256–2265. doi:10.1016/S0140-6736(17)32250-X
5. Londero LS, Hogh A, Houlind K, Lindholt JS. Danish trends in major amputation after vascular reconstruction in patients with peripheral arterial disease 2002–2014. Eur J Vasc Endovasc Surg. 2019;57(1):111–120. doi:10.1016/j.ejvs.2018.08.047
6. Behrendt CA, Sigvant B, Kuchenbecker J, et al. Editor’s choice - international variations and sex disparities in the treatment of peripheral arterial occlusive disease: a report from VASCUNET and the international consortium of vascular registries. Eur J Vasc Endovasc Surg. 2020;60(6):873–880. doi:10.1016/j.ejvs.2020.08.027
7. Lees T, Troeng T, Thomson IA, et al. International variations in infrainguinal bypass surgery - A VASCUNET report. Eur J Vasc Endovasc Surg. 2012;44(2):185–192. doi:10.1016/j.ejvs.2012.05.006
8. Farber A, Rosenfield K, Menard M. The BEST-CLI trial: a multidisciplinary effort to assess which therapy is best for patients with critical limb ischemia. Tech Vasc Interv Radiol. 2014;17(3):221–224. doi:10.1053/j.tvir.2014.08.012
9. Vartanian SM, Conte MS. Surgical intervention for peripheral arterial disease. Circ Res. 2015;116(9):1614–1628. doi:10.1161/CIRCRESAHA.116.303504
10. Conte MS, Bradbury AW, Kolh P, et al. Global vascular guidelines on the management of chronic limb-threatening ischemia. J Vasc Surg. 2019;69(6S):3S–125S e140.
11. Duceppe E, Parlow J, MacDonald P, et al. Canadian cardiovascular society guidelines on perioperative cardiac risk assessment and management for patients who undergo noncardiac surgery. Can J Cardiol. 2017;33(1):17–32. doi:10.1016/j.cjca.2016.09.008
12. Schwarze ML, Barnato AE, Rathouz PJ, et al. Development of a list of high-risk operations for patients 65 years and older. JAMA Surg. 2015;150(4):325–331. doi:10.1001/jamasurg.2014.1819
13. Farber A, Menard MT, Conte MS, et al. Surgery or endovascular therapy for chronic limb-threatening ischemia. N Engl J Med. 2022;387:2305–2316. doi:10.1056/NEJMoa2207899
14. Bradbury AW, Moakes CA, Popplewell M, et al. A vein bypass first versus a best endovascular treatment first revascularisation strategy for patients with chronic limb threatening ischaemia who required an infra-popliteal, with or without an additional more proximal infra-inguinal revascularisation procedure to restore limb perfusion (BASIL-2): an open-label, randomised, multicentre, Phase 3 trial. Lancet. 2023;401(10390):1798–1809.
15. Møller A, Eldrup N, Wetterslev J, et al. Trends in abdominal aortic aneurysm repair incidence, comorbidity, treatment, and mortality: a Danish Nationwide Cohort Study, 1996–2018. Clinical Epidemiology. 2024.
16. Sorensen HT. Regional administrative health registries as a resource in clinical epidemiology: a study of options, strengths, limitations and data quality provided with examples of use. Int J Risk Saf Med. 1997;10(1):1–22. doi:10.3233/JRS-1997-10101
17. Schmidt M, Pedersen L, Sorensen HT. The Danish civil registration system as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–549. doi:10.1007/s10654-014-9930-3
18. Eldrup N, Cerqueira C, de la Motte L, Rathenborg LK, Hansen AK. The Danish vascular registry, karbase. Clin Epidemiol. 2016;8:713–718. doi:10.2147/CLEP.S99506
19. Schmidt M, Schmidt SA, Sandegaard JL, Ehrenstein V, Pedersen L, Sorensen HT. The Danish national patient registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. doi:10.2147/CLEP.S91125
20. Moller A, Nielsen HB, Wetterslev J, et al. Low vs high hemoglobin trigger for transfusion in vascular surgery: a randomized clinical feasibility trial. Blood. 2019;133(25):2639–2650. doi:10.1182/blood-2018-10-877530
21. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
22. Arnold KF, Davies V, de Kamps M, Tennant PWG, Mbotwa J, Gilthorpe MS. Reflection on modern methods: generalized linear models for prognosis and intervention-theory, practice and implications for machine learning. Int J Epidemiol. 2021;49(6):2074–2082. doi:10.1093/ije/dyaa049
23. Criqui MH, Aboyans V. Epidemiology of peripheral artery disease. Circ Res. 2015;116(9):1509–1526. doi:10.1161/CIRCRESAHA.116.303849
24. Sundaram V, Bloom C, Zakeri R, et al. Temporal trends in the incidence, treatment patterns, and outcomes of coronary artery disease and peripheral artery disease in the UK, 2006–2015. Eur Heart J. 2020;41(17):1636–1649. doi:10.1093/eurheartj/ehz880
25. Clemmensen KK, Lynge E, Clemmensen IH. Nationwide tobacco surveys and sales data in Denmark from 1920 to 2010. Dan Med J. 2012;59(6):1.
26. Moridzadeh RS, Sanaiha Y, Madrigal J, Antonios J, Benharash P, Baril DT. Nationwide comparison of the medical complexity of patients by surgical specialty. J Vasc Surg. 2021;73(2):683–688 e682. doi:10.1016/j.jvs.2020.05.072
27. Hertzer NR, Beven EG, Young JR, et al. Coronary artery disease in peripheral vascular patients. A classification of 1000 coronary angiograms and results of surgical management. Ann Surg. 1984;199(2):223–233. doi:10.1097/00000658-198402000-00016
28. Authority TDHD; 2022. Available from: https://medstat.dk/.
29. Dua A, Lee CJ. Epidemiology of peripheral arterial disease and critical limb ischemia. Tech Vasc Interv Radiol. 2016;19(2):91–95. doi:10.1053/j.tvir.2016.04.001
30. Carstensen B, Ronn PF, Jorgensen ME. Prevalence, incidence and mortality of type 1 and type 2 diabetes in Denmark 1996–2016. BMJ Open Diabetes Res Care. 2020;8(1). doi:10.1136/bmjdrc-2019-001071
31. Diehm N, Shang A, Silvestro A, et al. Association of cardiovascular risk factors with pattern of lower limb atherosclerosis in 2659 patients undergoing angioplasty. Eur J Vasc Endovasc Surg. 2006;31(1):59–63. doi:10.1016/j.ejvs.2005.09.006
32. Schmidt M, Jacobsen JB, Lash TL, Botker HE, Sorensen HT. 25 year trends in first time hospitalisation for acute myocardial infarction, subsequent short and long term mortality, and the prognostic impact of sex and comorbidity: a Danish nationwide cohort study. BMJ. 2012;344:e356. doi:10.1136/bmj.e356
33. Pedersen AB, Ehrenstein V, Szepligeti SK, et al. Thirty-five-year trends in first-time hospitalization for hip fracture, 1-year mortality, and the prognostic impact of comorbidity: a Danish Nationwide Cohort Study, 1980–2014. Epidemiology. 2017;28(6):898–905. doi:10.1097/EDE.0000000000000729
34. DeRubertis BG, Pierce M, Chaer RA, et al. Lesion severity and treatment complexity are associated with outcome after percutaneous infra-inguinal intervention. J Vasc Surg. 2007;46(4):709–716. doi:10.1016/j.jvs.2007.05.059
35. Statistics Denmark [homepage on the Internet]. Flere tildeles hjemmehjælp, men får færre timer [More are assigned home care, but get fewer hours]; 2023. Available from: https://www.dst.dk/da/Statistik/nyheder-analyser-publ/nyt/NytHtml?cid=46131.
36. Altreuther M, Menyhei G. International validation of the Danish vascular registry karbase: a vascunet report. Eur J Vasc Endovasc Surg. 2019;58(4):609–613. doi:10.1016/j.ejvs.2019.04.008
37. Laustsen J, Jensen LP, Hansen AK; Danish National Vascular R. Accuracy of clinical data in a population based vascular registry. Eur J Vasc Endovasc Surg. 2004;27(2):216–219. doi:10.1016/j.ejvs.2003.11.011
38. Lasota AN, Overvad K, Eriksen HH, Tjonneland A, Schmidt EB, Gronholdt M-LM. Validity of peripheral arterial disease diagnoses in the Danish national patient registry. Eur J Vasc Endovasc Surg. 2017;53(5):679–685. doi:10.1016/j.ejvs.2016.12.031
39. Sundboll J, Adelborg K, Munch T, et al. Positive predictive value of cardiovascular diagnoses in the Danish National Patient Registry: a validation study. BMJ Open. 2016;6(11):e012832. doi:10.1136/bmjopen-2016-012832
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.