Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Trends in Glycemic and Cardiovascular Risks Control in Cantonese Adults in Primary Healthcare Settings: 2018 to 2022
Authors Wu X ![]() , Fan L, Chen X
, Fan L, Chen X ![]() , Huang M, Zhang X
, Huang M, Zhang X
Received 21 February 2025
Accepted for publication 8 June 2025
Published 1 July 2025 Volume 2025:18 Pages 2095—2106
DOI https://doi.org/10.2147/DMSO.S519612
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ernesto Maddaloni
Xueji Wu,1,2 Liumei Fan,3 Xiongfei Chen,2,4 Meiting Huang,5 Xinghua Zhang3
1Corporate Operations Office, Guangzhou Center for Disease Control and Prevention, Guangzhou, Guangdong, People’s Republic of China; 2Institute of Public Health, Guangzhou Medical University & Guangzhou Center for Disease Control and Prevention (Guangzhou Health Supervision Institute), Guangzhou, Guangdong, People’s Republic of China; 3Department of Non-Communicable Disease Control and Prevention, Baiyun Center for Disease Control and Prevention, Guangzhou, Guangdong, People’s Republic of China; 4Department of Primary Healthcare, Guangzhou Center for Disease Control and Prevention(Guangzhou Health Supervision institute), Guangzhou, Guangdong, People’s Republic of China; 5Department of Health Statistics, School of Public Health, Dalian Medical University, Dalian, Liaoning, People’s Republic of China
Correspondence: Xueji Wu, Email [email protected]
Background: Glycemic and cardiovascular risks control in patients with type 2 diabetes (T2DM) managed in primary healthcare (PHC) settings remains challenging in urbanizing areas like Guangzhou. This study analyzes 2018– 2022 trends to identify care gaps and inform policy.
Methods: We collected and analyzed real-world data (RWD) from 81,709 adults aged 30 years or older with T2DM who voluntarily participated in health examinations across 24 primary healthcare settings in Baiyun district, Guangzhou. The assessed targets included fasting blood glucose(FBG), blood pressure (BP), lipid panel with total cholesterol(TC), triglycerides(TG),low-density lipoprotein(LDL) and high-density lipoprotein(HDL), and BMI. Associated factors encompassed socioeconomic and lifestyle variables, and anthropometric measurement as waist circumference (WC). Linear and logistic regression models were used to analyze the trend in the percentage of participants with clinical target achievements and associated factors.
Results: The study population comprised predominantly older female participants with prolonged diabetes duration and high hypertension comorbidity prevalence (87.6%).Trends in the standardized percentage of participants with control of FG, TC, TG, LDL, and BMI were improved; however, those for BP and HDL decreased from 2018 to 2022 (p< 0.05). Lifestyle modifications presented a paradoxical pattern: despite alcohol, diet, physical activity were improved, smoking (+2.8%) and waist circumference (WC, +0.7cm) increased significantly. Patients with uncontrolled FG, BP, and LDL were less physically active if older, female, or single, while those with higher WC more often had unhealthy lifestyles and poorer metabolic control.
Conclusion: While metabolic parameters improved, suboptimal BP and HDL control reveal ongoing primary care challenges.Advanced age, female sex, longer diabetes duration, unmarried status, and increased WC are key barriers to uncontrolled FG, BP, and LDL. The findings highlight the need to prioritize enhanced BP and HDL control strategies and implement precision lifestyle interventions for high-risk patient subgroups in PHC.
Keywords: trends, diabetes control, Cantonese, physical examination, primary health care
Introduction
Type 2 diabetes mellitus (T2DM), characterized by the presence of hyperglycaemia in the absence of treatment, is usually found in adults and significantly increases the risk of cardiovascular events, microvascular diseases and premature death. International Diabetes Federation (IDF) estimates there were 463 million adults with diabetes worldwide in 2021, >90% have T2DM and nearly half live in two large developing countries: India and China.1 The interplay of socioeconomic transition (rapid urbanization, economic growth), health system constraints, demographic shifts (aging), persistent unhealthy lifestyle factors and population-specific pathophysiology (Asian T2DM phenotypes) jointly explain the dual challenges of rising diabetes prevalence and inadequate metabolic control in India and China.2,3
To address the increasing prevalence of diabetes, since 2009, China has increased its financial investment and strengthened the primary healthcare (PHC) system for the prevention and management of diabetes.4 Diabetic patients were identified through systematic community-based screening initiatives and subsequently enrolled in a structured diabetes management program, which included mandatory clinical follow-ups and optional annual comprehensive physical examinations for free. A physical examination is crucial to identify T2DM complications.5 Due to budget constraints, the government-supported primary diabetes care covers basic diabetes screening items, including routine physical examinations (height, weight, waist circumference(WC)), blood pressure (BP), fasting blood glucose(FBG), and lipid panel with total cholesterol(TC), triglycerides(TG),low-density lipoprotein(LDL) and high-density lipoprotein(HDL). Despite guideline emphasis,6,7 real-world comprehensive diabetes control -glycemic control (HbA1c, FBG) and cardiovascular risk factors control (BP, lipid profiles, BMI)- remains poor.8,9 Diabetic patients managed by primary healthcare settings tend to be middle-aged or older,8 which poses additional challenges (e.g., significantly higher prevalence of comorbidities10 in achieving comprehensive diabetes control targets. This is evidenced by increasing prevalence of T2DM,11 deteriorating health education (76% to 70%), stagnant treatment adherence (79% to 81%), and rising hospitalizations (4% to 6%) with nearly doubled readmissions (18.9% to 28.5%).12 Systematic gaps in care coordination - including fragmented longitudinal management, protocol-practice discrepancies, and disintegrated screening - lead to suboptimal condition-specific care.13 However, longitudinal data tracking the temporal dynamics of glycemic control and cardiovascular risk factor trajectories in China’s real-world diabetic population remain critically lacking, especially in primary care settings.
Guangzhou, the third largest city in China, its rapid urbanization, aging population (11.1% ≥60y in 2020), severe primary care workforce (PHCW) shortages (2.3/1,000 vs WHO’s 4.45 recommendation), exacerbating primary healthcare fragmentation across its 18-million resident population. A previous municipal cross-sectional analysis demonstrated that comorbid hypertension-hyperlipidemia significantly impaired blood pressure control in primary care-managed hypertensive patients,14 suggesting that suboptimal cardiovascular risk factors management may also represent a critical gap in achieving comprehensive diabetes control targets in PHC settings. Baiyun, one administrative district of Guangzhou, has the largest resident population (3,300,996 aged ≥15 years in 2022), with an estimated 400,000 (National diabetes prevalence: 12.4%)11 adult diabetes cases. However, only 55,628 (14%) were managed by primary healthcare settings, highlighting a critical gap in diabetes surveillance and intervention. Baiyun has leveraged health information technologies since 2018 to achieve marked improvements in the standardized management of patient health records.
To rectify this fundamental data shortfall, we conducted a population-based longitudinal study analyzing 5-year trends (2018–2022) in comprehensive diabetes control among patients with T2DM managed in primary healthcare settings in Baiyun. Utilizing standardized regional physical examination data, we are about to map longitudinal trajectories of diabetes control, benchmark management quality against current guidelines and identified associated factors.
Methods
Annual cross-sectional diabetes care data obtained from physical examinations from 2018 to 2022 were obtained from primary healthcare settings in Baiyun administrative district. Guangzhou Centers for Disease Control and Prevention Ethics Committee waived the informed consent requirement because it was obtained from the Health Record System in accordance with the declaration of Helsinki. This paper does not involve personal identification information and biological sample testing and it was approved by the Guangzhou Centers for Disease Control and Prevention Ethics Committee.
Inclusion Criteria
Subjects aged 30 years or older with a diagnosis of T2DM and at least one physical examination during the period 2018–2022 were included in this study. For each year, the physical examination “cut off” date was December 31. The assessed measurement for comprehensive diabetes control are BMI, BP, FG and blood lipids (TC, TG, LDL and HDL) in accordance with standardized diabetes control protocol developed by China Diabetes Society (CDS).6 Subjects who refused all laboratory examinations were excluded from the survey. We established a pre-specified threshold of ≤15% missing data for all physical examination variables to mitigate potential bias.
Sociodemographic Characteristics and Weight Status
Participants reported age, age ≥ 65 is defined as old age, age at the diagnosis of T2DM, sex (male or female), marital status (married or single), health-insurance status (uninsured or any health insurance), T2DM family history, hypertension comorbidity, smoking status (non-smoker or current smoker), alcohol consumption (current consumer or non-consumer), dietary balance (Proper proportion between meat and vegetables or not) and regular physical activity engagement (Engage in various forms of physical activity for at least 30 minutes, ≥one time/week, yes or no). Data on the clinical variables (SBP, DBP, and BMI) and laboratory parameters (FG and lipid profile) were collected as well.
Statistical Analysis
A descriptive analysis of the study variables was performed for each year. We calculated the mean and standard deviation for all quantitative variables and frequencies and percentages for qualitative variables. We calculated the crude rate of FG, BP, lipid, and BMI control, according to guidelines (See Supplementary Table 1) and standardized them using the 2020 municipal population census for each year. For the continuous variables, we applied linear regression (stepwise/enter) to analyze the trends in the clinical outcomes, which were adjusted by age, sex, T2DM duration, marital status, health insurance status, T2DM family history, and hypertension comorbidity. We assessed the association between percentage control of FG, BP, LDL, HDL and socio-demographic-behavioral factors by logistic regression (forward LR process). All analyses were conducted with the use of SPSS, version 26.0.
Results
Study Participants
A total of 81,797 patients with T2DM in primary healthcare settings participated in a physical examination from 2018 through 2022. The rate of physical examination among managed patients increased from 47.4% in 2018 to 60.5% in 2019, and then dropped significantly to 34.0% in 2020, growing slowly to 40.9% in 2022. All patients underwent a valid FG test. Of eligible patients enrolled in the diabetes management program, 85.0%-100% completed their scheduled laboratory examination during the study period. (Supplementary Table 2).
Among the participants, the mean age was 67.8 years (95% confidence interval (CI): 67.8–67.9 years), 62.1% aged 65-year or older, and the T2DM duration was 6.8 years (95% CI: 6.7–6.8 years). Furthermore, 60.8% (95% CI: 60.4–61.2%) were female, 90.2% (95% CI: 90.0–90.5%) were married, 95.4% (95% CI: 95.2–95.5%) had health insurance, 1.7% (95% CI: 1.6–1.8) had family history of T2DM, 87.6% (95% CI: 87.4–87.9) had hypertension comorbidity.
The age and hypertension comorbidity distribution of patients increased, whereas the percentage of females, those with a single status, and those with health insurance decreased. The distribution of the age at diagnosis of T2DM and participants who had a family history of T2DM remained stable Details and changes in demographic characteristics are provided in Table 1.
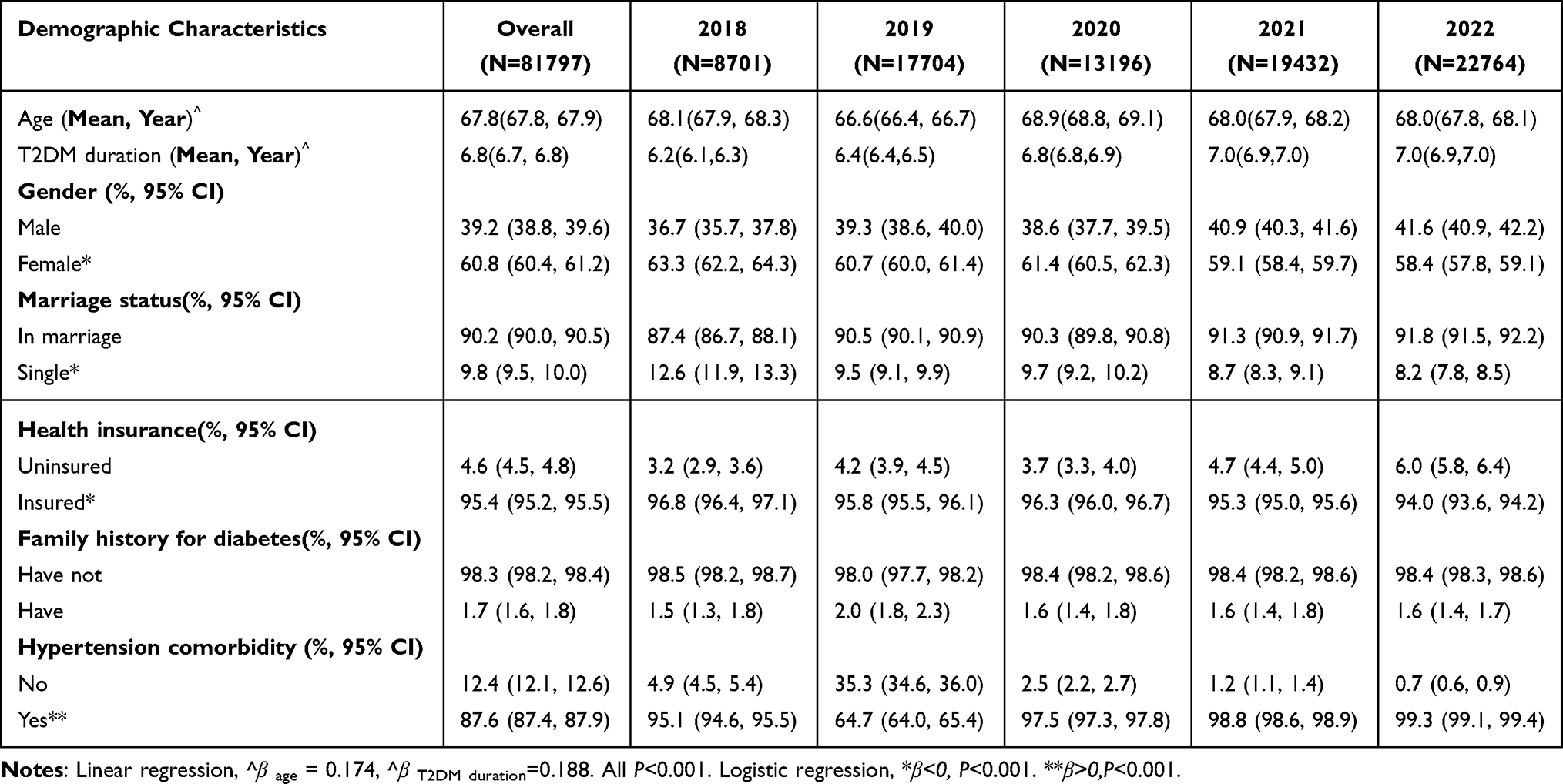 |
Table 1 Changes on the Demographic Characteristics of Adults with Diabetes in Primary Healthcare Settings From 2018–2022 |
Standardized Percentage Control of Diabetes Clinical Targets
Trends in the standardized percentage of participants with control of FG, TC, TG, LDL, and BMI were improved; however, those for BP and HDL decreased in 2018–2022 (Figure 1). The standardized percentage of participants in whom FG control was achieved increased from 45.0% in 2018 to 48.7% in 2020, and then declined to 47.9% in 2022. However, the percentage of participants in whom BP control was achieved rose from 51.5% in 2018 to 59.0% in 2019, but then dropped to 47.1% in 2021, and then leveled off to 51.3% in 2022. The percentage of participants in whom lipid control (LDL level < 2.6 mmol/L) was achieved increased from 33.8% in 2018 to 37.7% in 2022. The percentage of participants in whom BMI control was achieved reached the highest level (44.3%) in 2019, and then plateaued to approximately 40%. When adjusted by age, T2DM duration, sex, marital status, health insurance status, T2DM family history, and hypertension comorbidity, the annual rate of change in the crude percentage of participants with diabetes control was similar to the standardized percentage of participants with diabetes control (Supplementary Table 3).
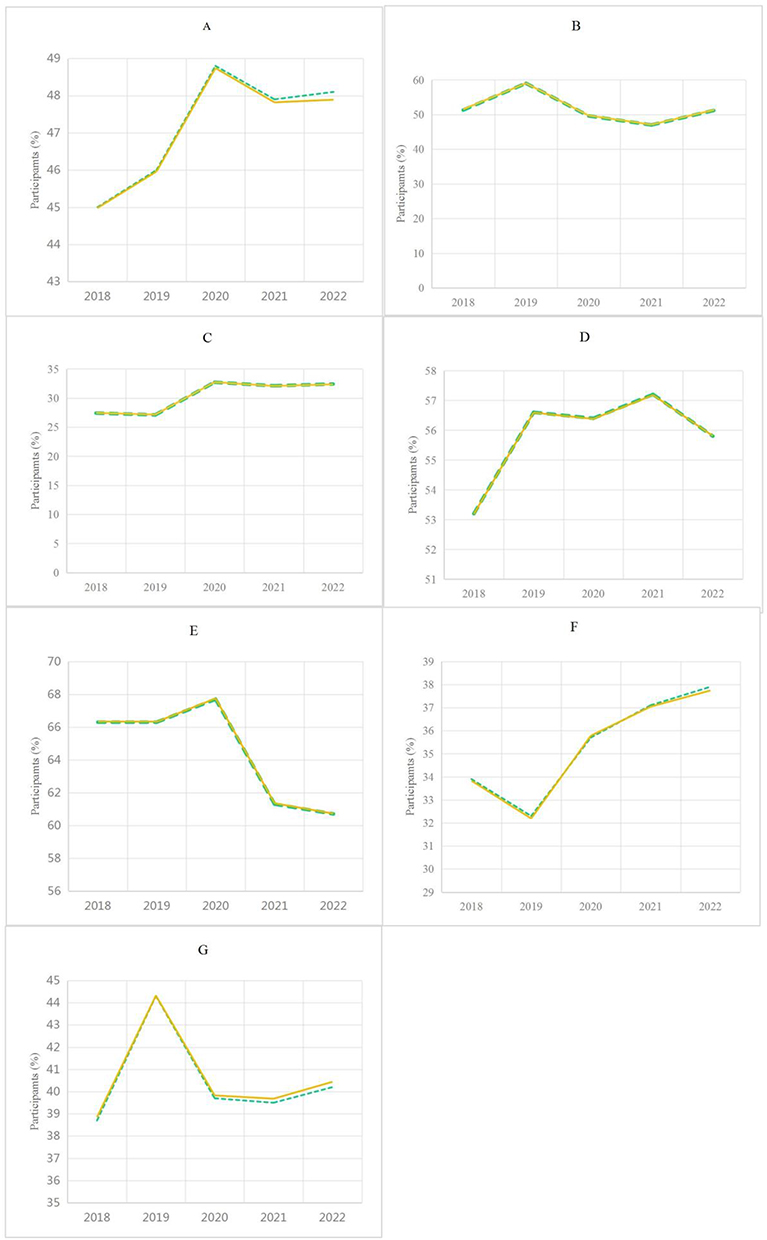 |
Figure 1 Trends in diabetes control among patients managed in primary health care settings, 2018–2022.(A) FG control (4.4–7.0 mmol/L), (B) BP control (<130/80 mmHg), (C) TC control (<4.5 mmol/L), (D) TG control (<1.7 mmol/L), (E) HDL control (Males >1.0 mmol/L; Females >1.3 mmol/L), (F) LDL control (<1.7 mmol/L), (G) BMI control (<24 kg/m²).Data are shown as crude rate (solid line) and age-standardized rate (dashed line). |
Changes in Diabetes Clinical Outcomes
In 2018–2022, participants had an average FG of 7.7 ± 3.0 mmol/L, SBP of 142.8 ± 18.3 mmHg, DBP of 82.4 ± 10.4 mmHg, TC of 5.2 ± 1.4 mmol/L, TG of 1.8 ± 0.9 mmol/L, LDL of 3.0 ± 1.0 mmol/L, HDL of 1.3 ± 0.4 mmol/L, and BMI of 25.0 ± 3.6 kg/m2. After adjusting for age, T2DM duration, sex, marriage status, health insurance status, T2DM family history, and hypertension comorbidity, the linear regression analysis showed that the FG and DBP levels were no-linear (both Ptrend > 0.05), but the SBP, TC, TG, LDL, HDL, and BMI level declined significantly from 2018 to 2022 (Figure 2).
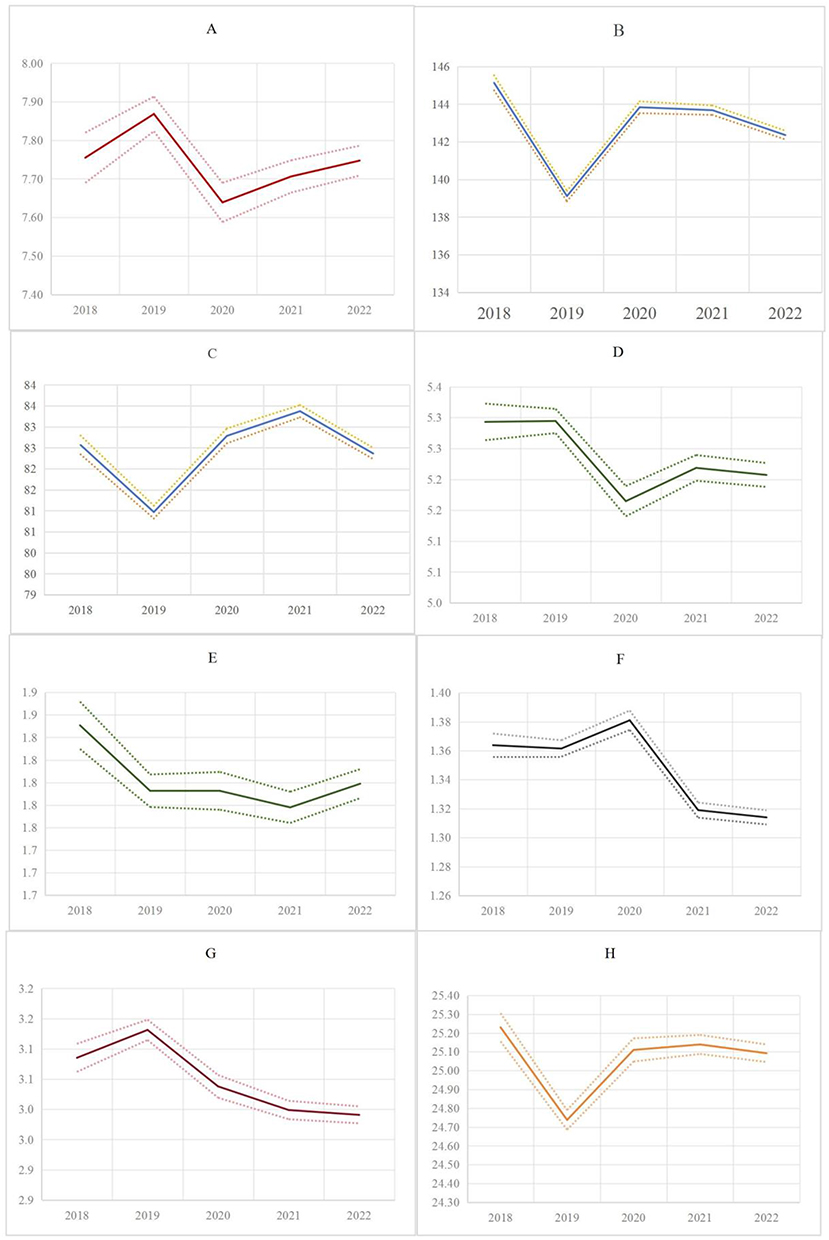 |
Figure 2 Changes in FG, BP, lipid, and BMI levels among patients managed in primary health care settings, 2018–2022.(A) Fasting glucose (mmol/L), (B) Systolic blood pressure (mmHg), (C) Diastolic blood pressure (mmHg), (D) Total Cholesterol (mmol/L), (E) Triglycerides (mmol/L),(F) high-density lipoprotein (mmol/L), (G) Low-density lipoprotein (mmol/L), (H) Body mass index (Kg/m2).Data are presented as mean ± 95% CI. Shaded areas indicate seasonal variation. |
Trends in Lifestyle Modification
Of participants, 11.8% were current smokers, 8.9% consumed alcohol, 96.9% of participants reported maintaining dietary balance, while 71.9% engaged in physical activity, with walking being the predominant exercise choice (≥90% of active respondents). Participants had a mean WC of 88.2 cm (95% CI: 88.1–88.2). Despite decreases in alcohol use and improvements in diet/exercise participation, smoking prevalence significantly rose from 9.8% (95% CI:9.2–10.5) to 12.6% (12.2–13.0) during 2018–2022, accompanied by a concerning increase in average waist circumference (87.8cm to 88.5cm; p-trend<0.05) (Table 2). While older patients with T2DM showed lower rates of smoking and alcohol consumption, they demonstrated poorer adherence to balanced diets and physical activity when failing to achieve glycemic (FG), blood pressure (BP), and lipid (LDL, HDL) control targets (Table 3). Similarly, hypertensive patients were less likely to maintain proper diet and exercise when FG, BP, or LDL targets were unmet, though interestingly showed increased physical activity when HDL targets were not achieved. More females were non-smokers or non-alcohol consumers and adhered to a balanced diet; however, they were less likely to participate in regular physical activity when FG, BP, and LDL control were not achieved. Adults with health insurance tended to smoke and were unable to adhere to a balanced diet when FG, BP, LDL and HDL were not achieved. Furthermore, adults with a higher WC were more inclined to smoke, consume alcohol, adhere to a balanced diet when FG, BP, LDL and HDL control were not achieved, and increase physical activity when BP was not achieved but decrease physical activity when LDL control was not achieved.
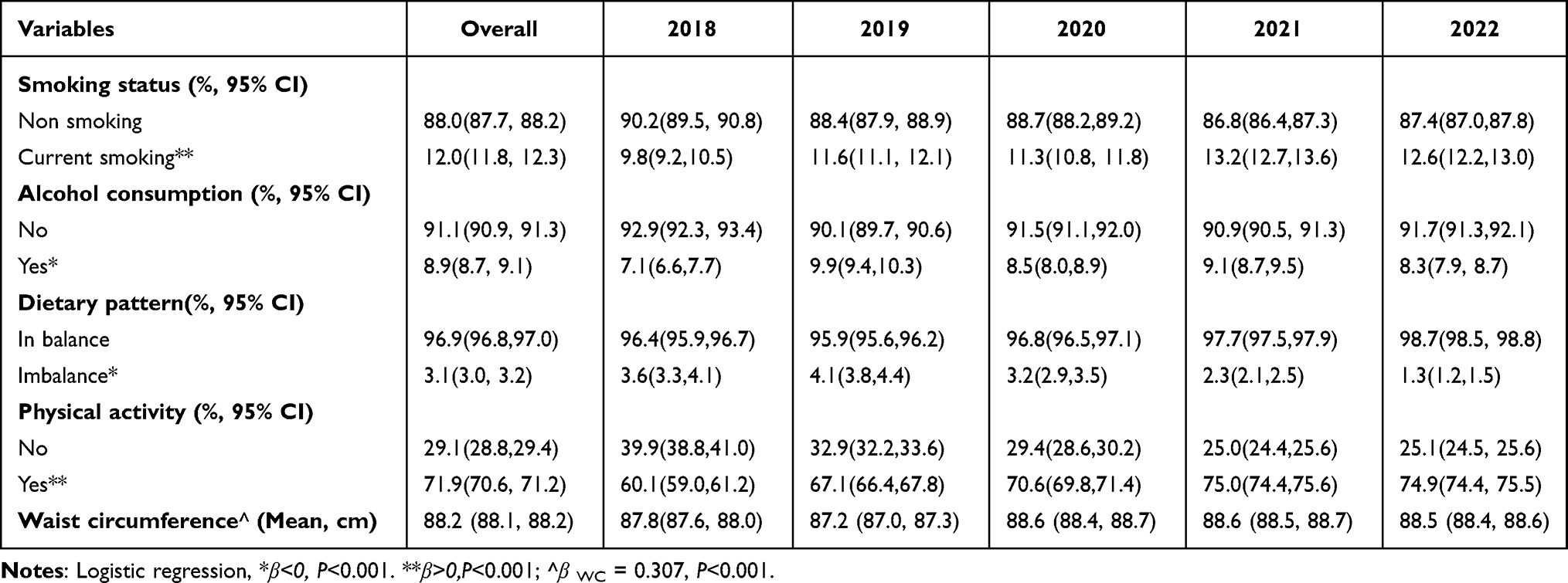 |
Table 2 Changes on the Lifestyles Variables and Waist Circumference of Adults with Diabetes in Primary Healthcare Settings From 2018–2022 |
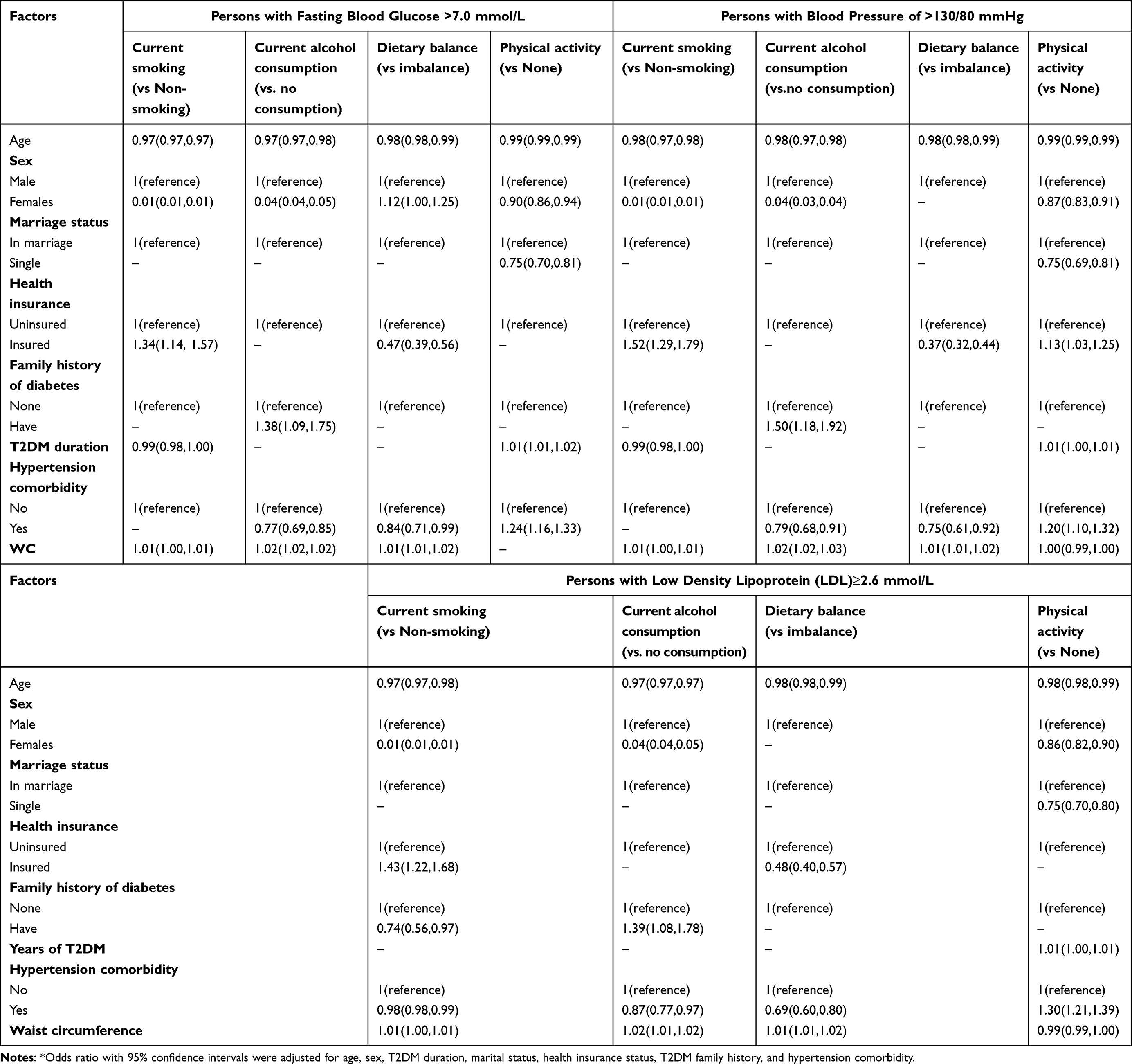 |
Table 3 Association Between Risk Factors and FG,BP and LDL Control in Adults with Diabetes in Primary Healthcare Settings From 2018–2022* |
Discussion
Unlike national cross-sectional survey,8 diabetic patients managed in this district’s primary care system (2018–2022) exhibited distinct vulnerability profiles: advanced age (62.1% ≥65 years), female predominance (60.8%), prolonged disease duration (mean 6.8 years), and extreme hypertension burden (87.6% comorbidity). These findings indicate that primary care services predominantly serve a clinically high-risk population with compounded healthcare needs. In comprehensive diabetes management, glycemic control serves as the primary outcome measure, with secondary emphasis on BP regulation, lipid profile optimization, and BMI management. While metabolic parameters control (FG, TC,TG,LDL and BMI) showed positive trends, the parallel deterioration in BP and HDL control suggests potential gaps in holistic risk factor management, particularly for hypertension and cardioprotective lipid profiles.
FG control rates showed modest improvement from 2018 to 2022, while the overall percentage of patients with FG target control (<7.0 mmol/L) was lower (47.4%) than the reported 49.3–50.1% in a nationwide study including treated patients,11,15 but higher than the 27.5% reported in another study16 or 21.0% from Nepal.17 This observation may be attributed to the unique demographic characteristics of our cohort - predominantly older women. When female patients generally exhibited better medication adherence, advancing age was associated with reduced treatment continuity,11 due to comorbidities, frailty, and cognitive decline. Hypertension comorbidity was highly prevalent (87.6%, 95% CI:87.4, 87.9), representing a major clinical challenge in our patient population. The overall percentage of patients with target BP control (<130/80 mmHg) in our study (51.6%) was similar to that among adults diagnosed with diabetes in the United States from 2007 to 2010 (51.2%), higher than that reported from a nationwide cross-sectional survey8 and municipal data in China.18 However, BP control rates showed in a decline from 2018 to 2022. The reasons might be: the existing primary diabetes care quality metrics, which notably exclude mandatory benchmarks for BP and lipid profile management. The parallel hypertension management framework mandates strict 140/90 mmHg thresholds for diagnosed cases, with an adjusted threshold of 150/100 mmHg for elderly patients (≥65 years), creating a clinical practice dichotomy. From 2018 to 2022, the proportion of elderly individuals among the diabetic patients in this study ranged between 56.2% (2019) and 66.5% (2020). Consequently, physicians may have been more inclined to apply hypertension management criteria when intervening in diabetic patients’ blood pressure control. The observed average blood pressure of 142.8/82.4 mmHg among study participants further supports this clinical practice pattern. Furthermore, SBP decreased but DBP was stable in 2018–2022, suggesting that an intensive SBP lowering strategy to < 130 mmHg in primary diabetes care is a priority.
Diabetes-related increases in TG, LDL, and low HDL have a shared pathology with chronic inflammation, oxidative stress, and certain miRNA and epigenetic modifications.19,20 HDL particles are considered as protective factors to cardiovascular disease, but do not prevent oxidation of LDL.21 Accumulating clinical evidence suggests both high LDL and TG are predictors of ASCVD and alterations in HbA1c.20,22 The trend in the control of TC, TG, and LDL was improved, which was combined with an HDL target control decreased, even though it had the highest overall percentage (63.8%) among lipid control measurements in 2018–2022. This divergent trend may be attributed to the differential effects of lipid-modifying therapies: LDL-lowering agents (statins, PCSK9 inhibitors, and ezetimibe) and TG-lowering agents (fibrates and niacin)23 by an increase in statin sales in Guangdong Province was observed in commercial reports during 2017–2018. Importantly, randomized controlled trials have consistently demonstrated no incremental cardiovascular benefit from HDL-elevating therapies when added to background statin regimens.24 Remarkably, while TG control rates (56.1%) exceeded those reported in the China National HbA1c Surveillance System (CNHSS) 2009–2013 cohort, LDL-C control (35.7%) remained suboptimal compared to historical data.25 These findings imply that timely and aggressive lipid-lowering therapy is warranted in primary diabetes care. Weight loss medications will also improve dyslipidemia of TG, LDL-C reduced and HDL-C increased.26 Cantonese population generally has a lower prevalence of obesity (BMI ≥28km/m2) due to economic development, dietary patterns, physical constitution, social welfare, and cultural background.27 The observed improvements in BMI control rates coincide with the implementation of enhanced obesity prevention measures in primary diabetes care quality metrics since 2017, particularly through community health education initiatives.
Lifestyle modification is an essential component of cardiovascular risk factor reduction in adults with T2DM, it includes smoking cessation, not consuming alcohol, medical nutritional therapy, physical activity, weight management, diabetes self-management education and support, and psychosocial care.6 The trends in the percentage of alcohol consumption, imbalanced diet intake, and physical inactivity decreased, but the prevalence of smoking and WC, a measurement of visceral adiposity, increased significantly in our study. The prevalence of smoking in our study appeared to be less than half of that in the general population,3 although the decreased trend observed in the general population3 did not occur. Smoking induces dyslipidemia includes HDL dysfunction through oxidative modification, while visceral adiposity accelerates HDL catabolism via hepatic lipase activation.28 Despite increased activity participation, reliance on low-intensity walking fails to meet national standards6 (CDS: 150+ mins moderate exercise weekly), limiting potential metabolic improvements. Therefore, tackling smoking cessation and prescribing personalized exercise for the target population with T2DM requires greater efforts and the investment of additional resources in primary healthcare settings. Among patients failing to achieve control targets for FG, BP, and LDL, key barriers included advanced age, female sex, longer diabetes duration, unmarried status, and increased WC - all associated with unfavorable lifestyle factors. These findings underscore the need for personalized lifestyle interventions in primary diabetes management, particularly targeting high-risk subgroups above.
Our study had several strengths.It represented a real-world data: (i) it includes patients of different ages or disease severities, avoiding the bias of “severely ill patient concentration” seen in tertiary hospitals; (ii) annual physical examinations provide 5 years of longitudinal data, superior to cross-sectional survey; (iii) data collected in a systematic manner by a trained primary healthcare team who used renewed, standardized management protocols. The current study also evaluated numerous relevant social-behavioral factors and comprehensive clinical outcomes, making a meaningful contribution to identifying the factors affecting diabetes control.
There are also some limitations that should be considered. (i) voluntary participation may over-represent health-conscious individuals while under-representing mobility-impaired elderly. Although we adjusted for age/sex, residual confounding remains. Findings are primarily generalizable to medically reachable populations rather than all diabetes patients. (ii) the primary outcome for diabetes control is FG rather than HbA1c, which may have led to an underestimation of the prevalence of poor glycemic control. That is, FG was used due to HbA1c’s higher cost and limited insurance coverage in primary care, restricting its community-wide feasibility. (iii)information on the use of glucose-lowering, BP-lowering, and blood lipid-lowering medications was unavailable, because such prescription information was not routinely documented in the standardized physical examination reports used for this study, which may have caused a confounding bias in the evaluation of the comprehensive control of diabetes.
Conclusions
In study period, diabetic patients with advanced age, female, prolonged disease duration, and extreme hypertension burden showed higher utilization rates of primary diabetes care services. Fewer than half of patients achieved target levels for FG, BP, and LDL control. Key barriers included advanced age, female sex, longer diabetes duration, unmarried status, and increased WC are associated with uncontrolled FG, BP and LDL-C. The prevalence of comprehensive diabetes control in FG, TG, TC, LDL and BMI showed improvements, while BP and HDL control declined.Observed rises in smoking and WC demand tailored lifestyle interventions. A stratified management approach prioritizing:1 high-risk groups with tailored interventions2 Enhance BP, especially SBP and HDL-C Control3 integrated with social support systems to facilitate individualized behavior change could bridge current gaps.
Data Sharing Statement
The data will be available upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Xueji Wu and Liumei Fan contributed equally to the article and share the first authorship.
Funding
This research received funding from the Medical Science and Technology Foundation of Guangdong Province (CN) (A2023215), the Key Project of Medicine Discipline of Guangzhou No. 2025-2027-12) and the Guangzhou Municipal Science and Technology Project (2023A03J0462).
Disclosure
All the authors declare that they have no financial or personal relationships with other people or organizations that can inappropriately influence our work. There is no professional or other personal interest of any nature or kind in any product, service or company that could be construed as influencing the position presented in, or the review of, the manuscript entitled.
References
1. IDF (International Diabetes Federation). An Authoritative Source of Country-Specific Estimates of the Prevalence of Diabetes Mellitus.
2. Ke C, Narayan KMV, Chan JCN, Jha P, Shah BR. Pathophysiology, phenotypes and management of type 2 diabetes mellitus in Indian and Chinese populations. Nat Rev Endocrinol. 2022;18(7):413–432. doi:10.1038/s41574-022-00669-4
3. Peng W, Chen S, Chen X, Ma Y, Wang TT, Sun XM, et al. Trends in major non-communicable diseases and related risk factors in China 2002-2019: an analysis of nationally representative survey data. Lancet Reg Health West Pac. 2024;43:100809. doi:10.1016/j.lanwpc.2023.100809
4. Li X, Krumholz HM, Yip W, et al. Quality of primary health care in China: challenges and recommendations. Lancet. 2020;395(10239):1802–1812. doi:10.1016/S0140-6736(20)30122-7
5. Malik A, Ananthakrishnan S. Diabetes physical examination. Med Clin North Am. 2022;106(3):483–494. doi:10.1016/j.mcna.2021.12.007
6. Zhu D, Chinese Diabetes Society. Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 edition). Chin J Diabetes. 2021;13(4):315–409.
7. Jia W, Weng J, Zhu D, et al. Standards of medical care for type 2 diabetes in China 2019. Diabetes Metab Res Rev. 2019;35(6):e3158. doi:10.1002/dmrr.3158
8. Zhong VW, Yu D, Zhao L, et al. Achievement of guideline-recommended targets in diabetes care in china: a nationwide cross-sectional study. Ann Intern Med. 2023;176(8):1037–1046. doi:10.7326/M23-0442
9. Zhang YQ, Li Y, Dong YG, et al. A nationwide assessment of blood pressure control and the associated factors in Chinese type 2 diabetes mellitus patients. J Clin Hypertens. 2019;21(11):1654–1663. doi:10.1111/jch.13675
10. Ohsugi M, Eiki JI, Iglay K, Tetsuka J, Tokita S, Ueki K. Comorbidities and complications in Japanese patients with type 2 diabetes mellitus: retrospective analyses of J-DREAMS, an advanced electronic medical records database. Diabet Res Clin Pract. 2021;178:108845. doi:10.1016/j.diabres.2021.108845
11. Wang L, Peng W, Zhao Z, et al. Prevalence and treatment of diabetes in China, 2013-2018. JAMA. 2021;326(24):2498–2506. doi:10.1001/jama.2021.22208
12. Sun M, Rasooly A, Fan X, Jian W. Assessing the quality of primary healthcare for diabetes in China: multivariate analysis using the China Health and Retirement Longitudinal Study (CHARLS) Database. BMJ Open. 2020;10(12):e035192. doi:10.1136/bmjopen-2019-035192
13. Xiong S, Jiang W, Meng R, et al. Factors associated with the uptake of national essential public health service package for hypertension and type-2 diabetes management in China’s primary health care system: a mixed-methods study. Lancet Reg Health West Pac. 2023;31:100664. doi:10.1016/j.lanwpc.2022.100664
14. Zhang S, Yang Y, Chen X, et al. Diabetes mellitus and hyperlipidemia status among hypertensive patients in the community and influencing factors analysis of blood pressure control. J Clin Hypertens. 2025;27(2):e14965. doi:10.1111/jch.14965
15. Zhang Y, Tong M, Wang B, et al. Geographic, gender, and seasonal variation of diabetes: a nationwide study with 1.4 million participants. J Clin Endocrinol Metab. 2021;106(12):e4981–e92. doi:10.1210/clinem/dgab543
16. Wang S, Ji X, Zhang Z, Xue F. Relationship between lipid profiles and glycemic control among patients with type 2 diabetes in Qingdao, China. Int J Environ Res Public Health. 2020;17(15). doi:10.3390/ijerph17155317
17. Gyawali B, Hansen MRH, Povlsen MB, et al. Awareness, prevalence, treatment, and control of type 2 diabetes in a semi-urban area of Nepal: findings from a cross-sectional study conducted as a part of COBIN-D trial. PLoS One. 2018;13(11):e0206491. doi:10.1371/journal.pone.0206491
18. Ma AJ, Dong J, Wei YQ et al. Comprehensive control rate and related factors of diabetes mellitus in Beijing (In Chinese). Zhonghua Yu Fang Yi Xue Za Zhi. 2020;54(11):1283–1288. doi:10.3760/cma.j.cn112150-20200616-00887
19. Kane JP, Pullinger CR, Goldfine ID, Malloy MJ. Dyslipidemia and diabetes mellitus: role of lipoprotein species and interrelated pathways of lipid metabolism in diabetes mellitus. Curr Opin Pharmacol. 2021;61:21–27. doi:10.1016/j.coph.2021.08.013
20. Poznyak A, Grechko AV, Poggio P, Myasoedova VA, Alfieri V, Orekhov AN. The diabetes mellitus-atherosclerosis connection: the role of lipid and glucose metabolism and chronic inflammation. Int J Mol Sci. 2020;21(5):1835. doi:10.3390/ijms21051835
21. Beckman JA, Creager MA, Libby P. Diabetes and atherosclerosis: epidemiology, pathophysiology, and management. JAMA. 2002;287(19):2570–2581. doi:10.1001/jama.287.19.2570
22. Ye X, Kong W, Zafar MI, Chen LL. Serum triglycerides as a risk factor for cardiovascular diseases in type 2 diabetes mellitus: a systematic review and meta-analysis of prospective studies. Cardiovasc Diabetol. 2019;18(1):48. doi:10.1186/s12933-019-0851-z
23. Joint Committee on the Chinese Guidelines for Lipid Management WZ. Li jianjun,zhao shuiping,gao runlin. Chinese guideline for lipid management (primary care version 2024) (in Chinese). Chinese J Cardiol. 2024;52(4):330–337. doi:10.3760/cma.j.cn112148-20240102-00002
24. Bahiru E, Hsiao R, Phillipson D, Watson KE. Mechanisms and Treatment of Dyslipidemia in Diabetes. Curr Cardiol Rep. 2021;23(4):26. doi:10.1007/s11886-021-01455-w
25. Yuan Y, Zhou X, Lu J, Guo X, Ji L. Lipid control in adult Chinese patients with type 2 diabetes: a retrospective analysis of time trends and geographic regional differences. Chin Med J. 2021;135(3):356–358. doi:10.1097/CM9.0000000000001895
26. Hasan B, Nayfeh T, Alzuabi M, et al. Weight loss and serum lipids in overweight and obese adults: a systematic review and meta-analysis. J Clin Endocrinol Metab. 2020;105(12):3695–3703. doi:10.1210/clinem/dgaa673
27. Pan XF, Wang L, Pan A. Epidemiology and determinants of obesity in China. Lancet Diabetes Endocrinol. 2021;9(6):373–392. doi:10.1016/S2213-8587(21)00045-0
28. Kosmas CE, Sourlas A, Guzman E, Kostara CE. Environmental factors modifying HDL functionality. Curr Med Chem. 2022;29(10):1687–1701. doi:10.2174/0929867328666210714155422
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.