Back to Journals » Patient Preference and Adherence » Volume 17
Treatment Patterns, Healthcare Resource Utilization, and Direct Costs Among Patients Initiating Concomitant Use of a Calcitonin Gene-Related Peptide Monoclonal Antibody (CGRP mAb) and Novel Acute Medication in the United States
Authors Varnado OJ, Gulati T, Wheeler A, Hoyt M
Received 18 September 2023
Accepted for publication 25 November 2023
Published 18 December 2023 Volume 2023:17 Pages 3449—3459
DOI https://doi.org/10.2147/PPA.S435782
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Oralee J Varnado,1 Tania Gulati,2 Anthony Wheeler,3 Margaret Hoyt1
1Value Evidence Outcomes – Research & Neuroscience, Indianapolis, IN, USA; 2Value Evidence Outcomes, Real World Evidence, Eli Lilly Services India, Private Limited, Bengaluru, Karnataka, India; 3Value Evidence Outcomes – Outcomes Liaisons, Indianapolis, IN, USA
Correspondence: Oralee J Varnado, Value Evidence Outcomes – Research & Neuroscience, Lilly Corporate Center, Indianapolis, IN, 46285, USA, Email [email protected]
Purpose: To describe treatment patterns, all-cause and migraine-related healthcare resource utilization (HCRU), and direct costs among people with migraine treated with concomitant calcitonin gene-related peptide monoclonal antibody (CGRP mAb) and novel acute migraine medications (ubrogepant, rimegepant, lasmiditan) in the United States (US).
Patients and Methods: This retrospective, observational cohort study utilized data from the IBM MarketScan® Research Databases and included adults initiating CGRP mAb or novel acute migraine medication as index medications between May 01, 2018, and Feb 28, 2021. All-cause and migraine-related HCRU (number of visits) and costs at baseline (12 months pre-index) and at follow-up (12 months post-index) were descriptively analyzed; differences between values at follow-up and baseline were reported.
Results: Of 4,167 included in the analysis (mean [SD] age: 43.7 [11.2] years), 89.2% were women, and 59.7% had chronic migraine. Adherence to the indexed CGRP mAb was 47% (using proportion of days covered [PDC]) and 80.1% (using medication possession ratio [MPR]); mean (SD) persistence was 273.4 (115.3) days). At follow-up, 43.9% of the patients discontinued their index preventive medication of which 80.2% switched to a different preventive migraine medication; 17.0% restarted their index preventive medication. Reductions in all-cause inpatient HCRU, all-cause inpatient and outpatient costs, and migraine-related outpatient HCRU were observed at follow-up vs. baseline, whereas increases in all-cause outpatient HCRU, all-cause medication costs, migraine-related inpatient HCRU, and migraine-related inpatient, outpatient, and medication costs were observed.
Conclusion: In this study, observed treatment patterns with the indexed CGRP mAb were consistent with prior reports. Concomitant treatment with CGRP mAb and novel acute migraine medications led to reductions in some outcomes of HCRU and direct costs, however, increases were also observed. Treatment utilization, reductions in HCRU and cost savings identified in this study in favor of concomitant CGRP mAb and novel acute medications may help clinicians and other healthcare decision makers assessing appropriate therapeutic options for migraine management.
Plain Language Summary: What was known before?The American Headache Society recommends concomitant use of preventive and acute medications for migraine.Data on treatment outcomes, and healthcare resource utilization (HCRU) and medical costs are limited for patients with migraine who use preventive and acute migraine medications concomitantly.
What does this study add?Patients with migraine started treatment with preventive medications – calcitonin gene-related peptide monoclonal antibodies [CGRP mAb] such as galcanezumab/fremanezumab followed by newer acute medications (ubrogepant, rimegepant, and lasmiditan).About half the patients who started their migraine treatment with CGRP mAb continued to use the same medication after 1-year on treatment.Of those patients who stopped their initial CGRP mAb medication, most switched to other preventive migraine medications such as antiepileptics and beta blockers.Patients taking CGRP mAb and newer acute migraine medications had fewer overall inpatient healthcare visits but a higher number of overall outpatient healthcare visits and lower overall inpatient and outpatient costs after 1-year of follow-up.
InterpretationIncreases in healthcare costs for migraine treatment over a 1-year period were observed in patients who used CGRP mAb and newer acute migraine medications.At follow-up, greater cost savings were seen for non-migraine treatment utilization and some migraine-related healthcare utilization in concomitant CGRP mAb and newer acute medication users.This study may help healthcare providers and payors to better understand how patients who use acute and preventive treatments for migraine perform after one year of their initial treatment. This may inform them to make informed decisions on long-term treatment for patients with migraine.
Keywords: migraine, CGRP mAb, adherence, persistence, cost savings
Introduction
Migraine is a disabling, neurologic disease manifested as recurrent, pulsating headache with moderate-to-severe pain, often on one side of the head. It can be accompanied by nausea, vomiting, and sensitivity to sound, light, or head movements.1 An estimated 36 million people in the United States (US) are affected by migraine. Women are two times more likely than men to have migraine attacks.2–4 Migraine is associated with substantial health care resource utilization (HCRU) and costs in the US. People with migraine can experience significant functional disability at work, school, or social events, leading to higher indirect costs relative to the general population.5 In 2016, the total annual indirect costs associated with migraine was estimated to be $19.3 billion (inflated to 2019 US dollars).5,6 Furthermore, more than four million migraine-related emergency department (ED) visits were reported in 2016, leading to higher annual total direct health care expenses for people with migraine relative to the general population ($22,364 vs $15,697; inflated to 2019 US dollars).4–6
Treatment for migraine broadly includes acute and preventive medications. Whereas acute treatments (for example, triptans) are prescribed for relief from pain and associated migraine-related symptoms, preventive medications (for example, antidepressants, etc.) are used to reduce the severity or frequency of migraine attacks.7 Generally, older preventive migraine medications were not designed to treat migraine, and some preventive medications have inconsistent efficacy and safety. Furthermore, acute medications such as triptans are associated with insufficient response in some patients with migraine.7 In 2018, the US Food and Drug Administration (FDA) approved three subcutaneous self-injectable calcitonin gene-related peptide monoclonal antibodies (CGRP mAb) for migraine prevention: galcanezumab and fremanezumab (CGRP ligand antagonist) and erenumab (CGRP receptor antagonist).8–10 In 2020, the FDA approved an intravenously administered CGRP mAb, eptinezumab, for migraine prevention.11 The FDA has also approved several novel acute medications including ubrogepant (2019) and rimegepant (2020) (oral CGRP receptor antagonists), and oral lasmiditan (2020; a selective serotonin [5-HT1F] receptor agonist).12–14 The American Headache Society (AHS) 2021 consensus statement recommends considering the use of preventive migraine medications for people with migraine using acute migraine medications for ≥4 migraine headache days per month.7 With the approval of new acute and preventive migraine medications, a range of therapeutic options have become available for people with migraine.7,15 In light of these developments in the migraine treatment paradigm, it becomes important to understand the characteristics and treatment utilization patterns of people treating migraine with concomitant acute and preventive medications. However, there are limited real-world studies assessing treatment patterns, HCRU, and direct costs in this population.16 To bridge this gap, this study aimed to describe the treatment patterns, HCRU, and direct costs among people with migraine who initiated self-injectable CGRP mAb and novel acute migraine medications concomitantly.
Materials and Methods
Data Source and Study Design
In this retrospective observational cohort study, data were accessed from the IBM® MarketScan® Research Databases between May 01, 2017, and February 28, 2022 (study period). The IBM MarketScan Databases include de-identified, patient-level claims data of over 245 million lives in the US and are considered nationally representative of patients with Medicare or supplemental employer-sponsored insurance in the US. This study included people with migraine who initiated treatment with self-injectable CGRP mAb and novel acute migraine medications between May 01, 2018, and February 28, 2021 (index period). The CGRP mAb of interest in the study were erenumab, fremanezumab, and galcanezumab, and novel acute migraine medications included ubrogepant, rimegepant, and lasmiditan. Since the IBM MarketScan databases are fully de-identified and compliant with HIPAA, this study was exempt from Institutional Review Board approval.
Study Population (Figure 1)
Adults (aged ≥18 years) with migraine were included in the study if they:
- initiated use of self-injectable CGRP mAb (erenumab, fremanezumab, galcanezumab) and novel acute migraine medications (ubrogepant, rimegepant, lasmiditan) during the index period (May 01, 2018–February 28, 2021), and
- had at least three months overlap between the index medication (CGRP mAb or novel acute migraine medications) and the second initiated drug (novel acute migraine medications if CGRP mAb was the index medication and vice versa). The overlap could have the below scenarios (Figure 1):
- Novel acute migraine medication (index) ➔ CGRP mAb (1st fill) ➔ novel acute migraine medication (2nd fill), or
- CGRP mAb (index) ➔ novel acute migraine medication (1st fill) ➔ CGRP mAb (2nd fill), or
- CGRP mAb (index) ➔ novel acute migraine medication (1st fill) ➔ novel acute migraine medication (2nd fill), or
- Novel acute migraine medication (index) ➔ CGRP mAb (1st fill) ➔ CGRP mAb (2nd fill), and
- had at least one inpatient claim (including ED visits) or one outpatient claim with a diagnosis of migraine at index or in the 12 months pre-index, and
- were continuously enrolled with medical and pharmacy benefits in the 12-month pre- and post-index periods (a 45-day gap was allowed), and
- had no evidence of cluster headache during the study period, and
- had no evidence of galcanezumab 300 mg dosing for preventive treatment indicated for cluster headache.
 |
Figure 1 Patient attrition and overlap conditions in the study cohort. Abbreviations: CGRP mAb, calcitonin gene-related peptide monoclonal antibodies; N, total number in the population; n, number in sub-group. Note: *Overlap was defined as ≥2 fills of the index drug (CGRP mAb or novel acute medication, whichever started first) followed by 2 fills of the second drug, or ≥1 fill each of the index and second drug within 3 months of index drug initiation. |
Measures
In this study, we described treatment patterns (based on CGRP mAb index date), HCRU, and direct costs in people with migraine who initiated self-injectable CGRP mAb and novel acute migraine medications; demographic and clinical characteristics of the cohort were also described.
Demographic and Clinical Characteristics
Characteristics of the study cohort that were measured at baseline included age, sex, geographical region of residence, payor type, Deyo-Charlson Comorbidity Index (DCI), comorbid conditions, and healthcare costs. Healthcare costs were estimated based upon paid amounts of adjudicated claims which included insurer and health plan payments, and patient cost-sharing (copayments, deductibles, and coinsurance).
Treatment Patterns
At 12 months of follow-up, the following treatment patterns were assessed: adherence, persistence, discontinuation, switching, restart, length of therapy, and overlapping days of supply. Definitions for these outcomes are listed below:
- Adherence to index medication (based on either of the three CGRP mAb) was described by the proportion of days covered (PDC) and medication possession ratio (MPR).
- PDC was calculated as the number of days with the medication on hand, or the number of days exposed to the medication divided by the number of days during the follow-up period regardless of discontinuation. Those with PDC ≥80% were classified as adherent.
- MPR was calculated as the ratio of the sum of days’ supply from all prescriptions divided by the total number of days in the follow-up period. Those with MPR ≥80% were classified as adherent.
- Persistence (based on either of the three CGRP mAb) was defined as the number of days of continuous therapy from index date until the end of the follow-up period allowing for a maximum fixed gap between fills of 60 days.
- Discontinuation of index medication (based on either of the three CGRP mAb) was reported as a dichotomous variable and defined as the failure to refill the index medication within 60 days after the depletion of the days’ supply from previous fills.
- Switching to a non-index preventive medication was defined as the first switch to a medication different to the indexed CGRP mAb after its discontinuation (based on 60-day gap).
- Restart was defined as refilling of their index CGRP mAb after the discontinuation date. Time to restart was defined as the number of days from the day of discontinuation until the first restart of the index CGRP mAb during the follow-up period.
- The length of therapy was defined as the sum of days’ supply of the index medication during the follow-up period, including those who discontinued.
- Overlapping days of supply with novel acute migraine medications was defined as the sum of days’ supply where both the CGRP mAb and novel acute migraine medication overlapped during the follow-up period.
HCRU and Direct Costs
All-cause and migraine-related HCRU and costs were described over the 12 months pre- and post-index periods. Differences between values between these time points were reported as means and standard deviations (SDs) and all dollar estimates were inflated to 2021 dollars using the Medical Care Component of the Consumer Price Index.17
Statistical Analyses
Outcomes were presented descriptively using frequencies with percentages for categorical variables and means with SD for continuous variables. Descriptive analysis was used to compute and measure the all-cause and migraine-related HCRU during the follow-up period.
Results
Demographic and Clinical Characteristics of the Cohort
Of the 4167 people with migraine included in the analyses (mean age [SD]: 43.7 [11.2]), 89.2% were women, 59.7% had chronic migraine, and a majority had commercial insurance coverage (99.3%; Table 1). The mean (SD) CCI score in the 12-month pre-index period (baseline) was 0.7 (1.2), and the most common comorbid conditions reported were anxiety (41.3%), depression (30.5%), sleep disorder (29.2%), and hypertension (27.4%; Table 1).
 |
Table 1 Demographic and Clinical Characteristics of Patients with Migraine at Baseline |
Baseline and Follow-Up Preventive and Acute Medication Utilization
A large proportion of people with migraine (85.0%) in our study cohort initiated a self-injectable CGRP mAb as their index medication and 11.4% initiated a novel acute migraine medication; 3.7% initiated a combination of a CGRP mAb and a novel acute migraine medication on the index date (Figure 2A). A majority (83.5%) were prescribed ≥1 preventive migraine medications during baseline, and 88.3% were prescribed ≥1 acute migraine medications during the same time period (Figure 2B). Among those who received a combination of preventive and acute migraine medications, the most commonly prescribed medications were galcanezumab or fremanezumab + ubrogepant or rimegepant (53.4%), followed by erenumab + ubrogepant or rimegepant (42.7%; Figure 2B).
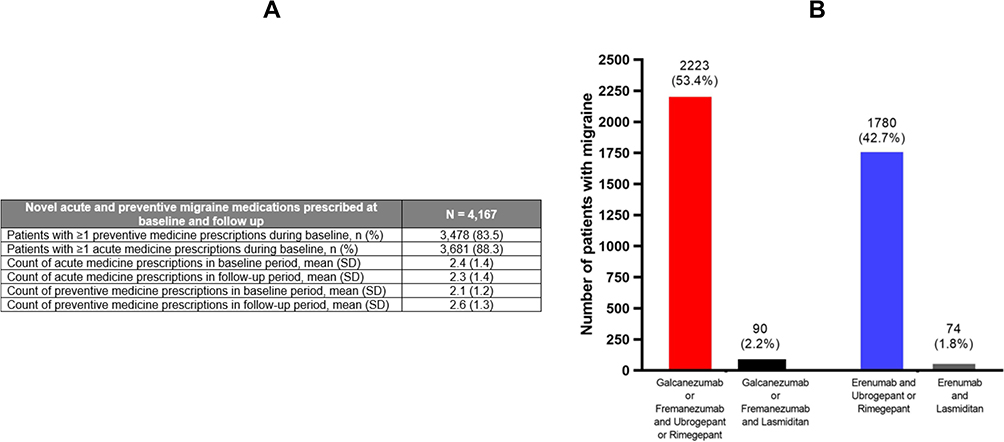 |
Figure 2 Treatment patterns. (A) Proportion of patients using novel acute or preventive migraine medications at baseline and summary measures of migraine medications used at baseline and follow-up. (B) Proportion of patients with migraine who were prescribed a combination of novel acute and preventive migraine medications at baseline. Abbreviations: N, total number in the population; n, number in sub-group; SD, standard deviation. |
Adherence to Index CGRP mAb
The mean (SD) length of index CGRP mAb treatment was 270.4 (119.9) days and the mean (SD) overlapping days of supply with CGRP mAb and novel acute migraine medications was 25.7 (51.4) days (Table 2). About 47.1% and 80.1% of the study population were adherent to the initiated CGRP mAb based on PDC and MPR, respectively.
 |
Table 2 Outcomes Associated with Treatment Patterns in the Study Cohort |
Persistence and Discontinuation of Index CGRP mAb
The mean (SD) number of days of persistence with the index CGRP mAb was 273.4 (115.3; Table 2). A total of 1831 (43.9%) people with migraine discontinued their index CGRP mAb.
Restart of Index CGRP mAb and Switch to Non-Index Preventive After Discontinuation
Of those who discontinued their index CGRP mAb, 1468 (80.2%) switched treatment and 312 (17.0%) restarted their indexed CGRP mAb medication (Table 2). The time to switch treatment was 34.5 (41.1) days and time to restart CGRP mAb treatment was 111.70 (47.1) days (Table 2). Following discontinuation of the indexed CGRP mAb, a switch to Level A medication included the largest proportion of patients (erenumab: 328 [38.6%]; fremanezumab: 157 (40.2%); galcanezumab: 221 [37.5%]) (Figure 3). Of those who switched to a different CGRP mAb from their indexed CGRP mAb, 274 (32.2%) switched from erenumab at index to galcanezumab, 79 (20.2%) switched from fremanezumab at index to galcanezumab, 71 (18.2%) switched from fremanezumab at index to erenumab, 109 (18.5%) switched to erenumab from galcanezumab at index, and 154 (18.1%) switched to fremanezumab from erenumab at index (Figure 3). Migraine preventives, classified as per the American Academy of Neurology (including Level A medications), are reported in Supplementary Table 1.
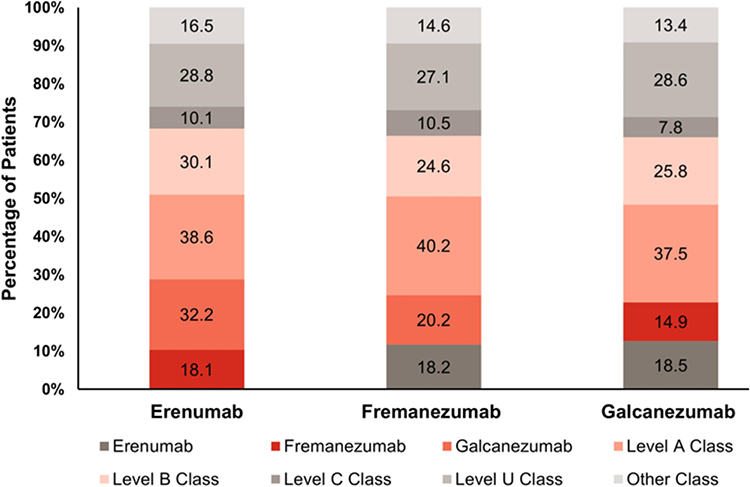 |
Figure 3 Treatment patterns at follow-up: Subsequent preventive medications among switchers. Notes: Level A class: preventive medications established as effective, including antiepileptics and beta-blockers; Level B class: preventive medications that are probably effective, including antidepressants and beta-blockers; Level C class: preventive medications that are possibly effective, including Angiotensin-converting enzyme inhibitors, Angiotensin receptor blockers, Alpha-Agonists, Antiepileptic drugs, beta-blockers; Level U class: preventive medications that are inadequate or conflicting data to support or refute medication use, including Anti-epileptic drugs, Antidepressants, Anti-thrombotic, Beta-blockers, Calcium-channel blockers; Other class: preventive medications that are possibly or probably ineffective. Classification of migraine preventive medication drug class is based on American Academy of Neurology guidelines. |
HCRU
At follow-up, the mean ± SD all-cause inpatient HCRU was 0.18 ± 0.79, decreasing by 0.03 + 0.17 from baseline (0.21 ± 0.96), whereas all-cause outpatient HCRU increased at follow-up by 0.22 ± 0.91 (follow-up: 24.07 ± 19.69; baseline: 23.85 + 18.78). Migraine-related inpatient HCRU increased to 0.07 ± 0.37 at follow-up from 0.06 ± 0.35 at baseline and a decrease of 0.15 ± 0.04 was observed in migraine-related outpatient HCRU from follow-up (5.20 ± 5.26) to baseline (5.35 ± 5.22).
Direct Costs
From baseline to follow-up, a mean ± SD reduction of $362.78 ± 2476.78 in all-cause inpatient costs were observed (follow-up: $3352.76 ± 16,394.54; baseline: $3715.54 ± 18,871.32). Similarly, all-cause outpatient costs decreased at follow-up by $253.01 ± 355.56 (follow-up: $9745.69 ± 14,608.65; baseline: $9998.70 ± 14,964.21). We observed a substantial increase in all-cause and migraine-related medication costs from baseline (all-cause: $9807.05 ± 17,272.50; migraine-related: $3101.40 ± 4878.35) to follow-up (all-cause: $17,782.76 ± 19,975.71; migraine-related: $10,080.43 ± 6052.59). Furthermore, migraine-related inpatient costs increased by $406.47 ± 723.88 (follow-up: $1609.15 ± 10,645.99; baseline: $1202.68 ± 9922.11), and migraine-related outpatient costs increased marginally at follow-up to $1679.46 ± 3855.96 from $1676.31 ± 3427.04; Figure 4.
 |
Figure 4 Direct costs at baseline and follow-up in the study cohort. |
Discussion
The 2019 AHS position statement identifies the value of combining acute and preventive migraine treatments for the effective management of migraine and reducing economic burden associated with migraine attacks.7 Given the limited real-world evidence on treatment patterns, HCRU and medical costs associated with concomitant use of newer preventive and acute migraine medications, this study may help clinicians with treatment decisions and inform payers on utilization patterns of CGRP mAb and novel acute medications. In this study, we observed that a majority of people with migraine in our study cohort first initiated a CGRP mAb followed by a novel acute migraine medication. Most received a preventive agent that binds the CGRP ligand (galcanezumab or fremanezumab) and a novel acute agent that binds the CGRP receptor (ubrogepant or rimegepant). Furthermore, at 12 months from initiation of a CGRP mAb, nearly half remained adherent to their indexed CGRP mAb. These findings are in line with another real-world study where users were most commonly prescribed a combination of preventive medications that bind the CGRP ligand and acute medications that bind to the CGRP receptor.16 Data from two small clinical studies and a real-world study have reported favorable safety and tolerability for this combination.18,19 However, our study did not assess safety or tolerability of concomitant CGRP mAb and novel acute migraine medications. There is a need to investigate the safety and efficacy of these medication combinations from larger sample sizes of people with migraine.
There is limited real-world evidence on treatment patterns for CGRP mAb.16,20,21 Those studies have reported adherence rates of 31% (PDC ≥ 80%) and 42% (MPR ≥ 80%) for erenumab at 6 months of follow-up, and 73% to 83% (PDC ≥ 80%) and 78% to 84% (MPR ≥ 80%) for monthly/quarterly fremanezumab at 6-month follow-up.20,21 Among patients who discontinued their index CGRP mAb treatment, most patients switched to other non-CGRP mAb preventive treatments and very few restarted their index CGRP mAb treatment. These findings are comparable to other real-world studies where discontinuation rates were reported to be 23%/16% for monthly/quarterly fremanezumab users.21 High adherence to index CGRP mAb in our study may also be the result of favorable treatment outcomes. The difference in mean PDC and MPR scores could have been due to the difference in the methodologies used in their calculation.
At the 12-month follow-up (versus baseline), our analyses found lower all-cause inpatient HCRU, inpatient and outpatient costs, and higher outpatient HCRU and medication costs. We also observed higher migraine-related inpatient HCRU and inpatient, outpatient, and medication costs. However, there was a reduction in migraine-related outpatient HCRU. The higher all-cause outpatient visits, medication costs, and migraine-related direct costs could be due to healthcare costs associated with comorbid conditions such as chronic migraine, anxiety, depression, sleep disorder and hypertension in our cohort of people with migraine. Similar results were also reported in prior observational studies that had higher healthcare costs in cohorts that had a high burden of comorbidities.22,23 A 2017 study reported that the annual migraine-related healthcare costs were almost twice as large for people with migraine who had >4 comorbid conditions compared to those without any comorbid conditions.23 The AHS 2019 consensus statement recommends the concomitant use of acute and preventive migraine medications;7 therefore, it will be important to understand the extent to which this recommendation is being followed in the real world. Furthermore, given the gap in real-world evidence of concomitant use of more recently approved acute and preventive migraine medications, more research is needed to understand what type of patients use both types of medications concomitantly and how effective this combination is in management of migraine. Clinical trials and real-world evidence are needed to fully understand the efficacy, safety and tolerability profile, and long-term effectiveness associated with concomitant use of acute and preventive migraine medications that both target the CGRP pathway.
Strengths and Limitations
This study adds to the limited real-world data on treatment patterns, HCRU, and costs associated with the use of concomitant novel migraine therapies. This study focuses on CGRP mAb and treatment patterns such as adherence and persistence to CGRP mAb. This is a follow-up to another study where patients with migraine were characterized and in the present study, we reported 12-month follow-up data on HCRU and costs. The use of data from a large claims-based database that is nationally representative of the US commercially insured adult population with migraine is another strength of this study. Despite the strengths of our study, a few limitations should be mentioned. Administrative claims data are subject to data coding limitations and data entry errors leading to misclassification of diagnosis and prescription codes. From a clinician’s perspective, data associated with safety or efficacy are not captured in claims data. Furthermore, prescription fill data was used to assess treatment patterns and it was not possible to validate whether the medications were actually used by those filling the prescriptions. The results of this study may not be generalizable to those in the US who have a different type of insurance or lack insurance coverage. The results may not be comparable to the patients outside the US. Lastly, we did not have data on when patients discontinued acute medications as we did not follow-up on the use of acute medications, and this could be a limitation to our study’s findings.
Conclusions
In this real-world, observational cohort study, the combination of fremanezumab/galcanezumab and ubrogepant/rimegepant was most commonly used by people with migraine-initiating concomitant CGRP mAb and novel acute migraine medications. At the 12-month follow-up, about half of those who initiated CGRP mAb continued to use their index CGRP mAb. Among those who discontinued, a majority switched to other preventive therapies. There were cost savings in terms of reduced all-cause inpatient and outpatient HCRU and costs as well as migraine-related outpatient HCRU, potentially reflective of better migraine management and comorbid conditions. These results may help clinicians and population-based decision makers in the selection of appropriate preventive and acute migraine medications for effective migraine management.
Acknowledgments
The authors thank Jerry Hall (Eli Lilly and Company, Indianapolis, IN, USA) for providing inputs during study design and implementation. Rahul Nikam and Rajiv Ravishankar Ulpe from Eli Lilly Services India Pvt. Ltd. provided writing and editorial support.
A portion of the data reported in this paper were presented at the American Academy of Neurology 2023 Annual Meeting as a poster presentation (poster ID P10.007) and published in the April 2023 Supplement issue of Neurology: https://n.neurology.org/content/100/17_Supplement_2/3127. Data from this paper were also presented at the 65th Annual Scientific Meeting of the American Headache Society as poster presentations (P-12; P-13) and published in the Supplement issue of the journal Headache: https://headachejournal.onlinelibrary.wiley.com/doi/10.1111/head.14523 in June 2023.
Funding
This study was sponsored by Eli Lilly and Company, Indianapolis, IN, USA.
Disclosure
Oralee Varnado, Tania Gulati, Anthony Wheeler, and Margaret Hoyt are full-time employees and minor shareholders of Eli Lilly and Company. The authors report no other conflicts of interest in this work.
References
1. Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition. Cephalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
2. American Migraine Foundation. Migraine through a woman’s life; 2019. Available from: https://americanmigrainefoundation.org/resource-library/migraine-through-a-womans-life/.
3. Lipton RB, Silberstein SD. Episodic and chronic migraine headache: breaking down barriers to optimal treatment and prevention. Headache. 2015;55(2):103–122. doi:10.1111/head.12505_2
4. Burch R, Rizzoli P, Loder E. The prevalence and impact of migraine and severe headache in the United States: updated age, sex, and socioeconomic-specific estimates from government health surveys. Headache. 2021;61(1):60–68. doi:10.1111/head.14024
5. Yucel A, Thach A, Kumar S, et al. Estimating the economic burden of migraine on US employers. Am J Manag Care. 2020;26(12):e403–e408.
6. CPI for all urban consumers (CPI-U). Bureau of labor statistics. Available from: https://www.bls.gov/news.release/archives/cpi_06122019.pdf.
7. Ailani J, Burch RC, Robbins MS; Board of Directors of the American Headache Society. The American Headache Society consensus statement: update on integrating new migraine treatments into clinical practice. Headache. 2021;61(7):1021–1039. doi:10.1111/head.14153
8. Markham A. Erenumab: first Global Approval. Drugs. 2018;78(11):1157–1161. doi:10.1007/s40265-018-0944-0
9. Hoy SM. Fremanezumab: first global approval. Drugs. 2018;78(17):1829–1834. doi:10.1007/s40265-018-1004-5
10. Lamb YN. Galcanezumab: first global approval. Drugs. 2018;78(16):1769–1775. doi:10.1007/s40265-018-1002-7
11. VYEPTI™ (eptinezumab-jjmr intravenous injection) [package insert]. Bothell WA: Lundbeck Seattle BioPharmaceuticals, Inc.; 2020.
12. Lamb YN. Lasmiditan: first approval. Drugs. 2019;79(18):1989–1996. doi:10.1007/s40265-019-01225-7
13. Scott LJ. Rimegepant: first approval. Drugs. 2020;80(7):741–746. doi:10.1007/s40265-020-01301-3
14. Scott LJ. Ubrogepant: first approval. Drugs. 2020;80(3):323–328. doi:10.1007/s40265-020-01264-5
15. Ashina M, Buse DC, Ashina H, et al. Migraine: integrated approaches to clinical management and emerging treatments. Lancet. 2021;397(10283):1505–1518. doi:10.1016/S0140-6736(20)32342-4
16. Varnado OJ, Hoyt M, Ye W, et al. Patient characteristics and treatment utilization among patients with migraine initiating self-injectable calcitonin gene-related peptide monoclonal antibody and novel acute medication. Curr Med Res Opin. 2022;38(8):1451–1457. doi:10.1080/03007995.2022.2091333
17. US Bureau of Labor Statistics. Measuring price change in the CPI: medical care. Washington, DC; 2020 [cited October 25, 2021]. Available from: https://www.bls.gov/cpi/factsheets/medical-care.htm.
18. Mullin K, Kudrow D, Croop R, et al. Potential for treatment benefit of small molecule CGRP receptor antagonist plus monoclonal antibody in migraine therapy. Neurology. 2020;94(20):e2121–e2125. doi:10.1212/WNL.0000000000008944
19. Berman G, Croop R, Kudrow D, et al. Safety of rimegepant, an oral CGRP receptor antagonist, plus CGRP monoclonal antibodies for migraine. Headache. 2020;60(8):1734–1742. doi:10.1111/head.13930
20. Hines DM, Shah S, Multani JK, et al. Erenumab patient characteristics, medication adherence, and treatment patterns in the United States. Headache. 2021;61(4):590–602. doi:10.1111/head.14068
21. Tangirala K, Cohen JM, Pandya S, et al. Real-world adherence, persistence, switching, and reinitiation by quarterly and monthly dosing regimen in patients prescribed AJOVY in US physician practices (2145). Neurology. 2021;96(15 Supplement):2145.
22. Buse DC, Reed ML, Fanning KM, et al. Comorbid and co-occurring conditions in migraine and associated risk of increasing headache pain intensity and headache frequency: results of the migraine in America symptoms and treatment (MAST) study. J Headache Pain. 2020;21(1):23. doi:10.1186/s10194-020-1084-y
23. Thorpe K. Prevalence, health care spending and comorbidities associated with chronic migraine patients. The Headache & Migraine Policy Forum; 2017.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Practice Management of Primary Open-Angle Glaucoma in the United States: An Analysis of Real-World Evidence
Imperato JS, Zou KH, Li JZ, Hassan TA
Patient Preference and Adherence 2022, 16:2213-2227
Published Date: 18 August 2022
Palbociclib Adherence and Persistence in Patients with Hormone Receptor Positive/Human Epidermal Growth Factor Receptor 2 Negative (HR+/HER2-) Metastatic Breast Cancer
Engel-Nitz NM, Johnson MG, Johnson MP, Cha-Silva AS, Kurosky SK, Liu X
Patient Preference and Adherence 2023, 17:1049-1062
Published Date: 18 April 2023
Adherence to Overactive Bladder Syndrome Treatments Recent Developments and Future Perspectives
Robinson D, O'Kane M, Cardozo L
International Journal of Women's Health 2023, 15:799-811
Published Date: 23 May 2023
Comparison of Treatment Patterns in Patients with Migraine Initiating Calcitonin Gene-Related Peptide Monoclonal Antibodies: A Retrospective Real-World US Study
Varnado OJ, Brady BL, Zagar AJ, Robles YP, Hoyt M
Patient Preference and Adherence 2024, 18:69-88
Published Date: 9 January 2024
Measuring the Influence of Side Effect Expectations, Beliefs, and Incident Side Effects on the Risk for Drug Discontinuation Among Individuals Starting New Medications, a Cross-sectional Study
Blackburn DF, Yao S, Taylor JG, Alefan Q, Lix LM, Eurich DT, Choudhry NK
Patient Preference and Adherence 2024, 18:979-989
Published Date: 17 May 2024