")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Treatment Goals in Schizophrenia: A Real-World Survey of Patients, Psychiatrists, and Caregivers in the United States, with an Analysis of Current Treatment (Long-Acting Injectable vs Oral Antipsychotics) and Goal Selection
Authors Fitzgerald HM , Shepherd J , Bailey H , Berry M, Wright J, Chen M
Received 27 July 2021
Accepted for publication 1 October 2021
Published 21 October 2021 Volume 2021:17 Pages 3215—3228
DOI https://doi.org/10.2147/NDT.S330936
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Heather M Fitzgerald,1 Jason Shepherd,2 Hollie Bailey,2 Mia Berry,2 Jack Wright,2 Maxine Chen3
1Lundbeck LLC, Deerfield, IL, USA; 2Adelphi Real World, Bollington, UK; 3Otsuka Pharmaceutical & Commercial Development, Inc., Princeton, NJ, USA
Correspondence: Maxine Chen
Otsuka Pharmaceutical & Commercial Development, Inc., 508 Carnegie Center, Princeton, NJ, 08540, USA
Tel +1 609-524-6788
Email [email protected]
Purpose: To understand similarities and differences in patient treatment goals as selected by US psychiatrists, adult patients with schizophrenia, and their caregivers in a real-world setting in the United States, including stratification by current medication and age.
Patients and Methods: Data were drawn from the Adelphi Schizophrenia Disease Specific Programme™, a point-in-time survey of psychiatrists and their consulting adult patients with schizophrenia, conducted from June to October 2019. Psychiatrists completed record forms for their next 8 consecutive outpatients and (where possible) 2 inpatients matching inclusion criteria. Participating psychiatrists, patients, and caregivers completed treatment goal questionnaires as part of the survey.
Results: Psychiatrists (n = 124) provided data on 1204 patients with schizophrenia, including 1135 on drug treatment (207 inpatients [18%] and 928 outpatients [82%]); questionnaires were completed by 555 patients and 135 caregivers. Decrease in disease symptoms was identified as the most important patient treatment goal by patients (64%), psychiatrists (selecting for 63% of patients), and caregivers (selecting for 68% of patients). Patients, psychiatrists, and caregivers similarly rated the least important goals (less sexual problems and less weight gain). Patients indicated their current medication helped to reach their most important goals: decrease in disease symptoms (68%) and thinking more clearly (39%). Findings based on analysis of treatment goals by treatment and age were similar to overall trends.
Conclusion: These findings, including identification of a primary consensus goal of decrease in disease symptoms, may help with discussions between patients with schizophrenia, psychiatrists, and caregivers to inform effective management strategies and encourage shared decision-making.
Keywords: long-acting injectable antipsychotic, oral antipsychotic, real-world survey, schizophrenia, treatment goals, treatment preferences
Introduction
Schizophrenia is a chronic and disabling severe mental illness with considerable impact, not only on patients’ health, well-being, and functioning, but also on their surrounding environment.1 Relapses are common among patients with schizophrenia; thus, prevention of relapse and subsequent hospitalization is an important public health concern.2,3
The introduction of long-acting injectable antipsychotics (LAIs) was an important step forward in addressing relapse and rehospitalization in patients with schizophrenia, but these agents remain underused in clinical practice.4,5 Compared with oral antipsychotics (OAPs), LAIs may improve treatment adherence and continuity.2 Based on the strong link between nonadherence and relapse, LAIs may thus potentially reduce risk of relapse, slow disease progression, and improve long-term outcomes.3,5–10 Currently, however, the American Psychiatric Association only recommends LAIs for patients who prefer such treatment or have a history of poor or uncertain adherence.4,5
Survey data indicate that healthcare providers consider LAIs primarily for patients who have had repeated hospitalizations due to relapses,11,12 although recent studies have demonstrated the advantage of LAIs over OAPs in first-episode or early-phase schizophrenia.13–15 The recent US PRELAPSE study3 also showed that aripiprazole once-monthly use in patients with early-phase schizophrenia can significantly delay first hospitalization compared with clinician’s choice (treatment as usual, which could include LAIs, as well as OAPs).
Patient preferences related to treatment goals and outcomes in schizophrenia treatment, and the relative importance of certain treatment goals have been assessed in several studies,16–18 including one focused on early-phase schizophrenia in patients from Germany, Italy, and the UK.19 Among the findings of these studies was that patients with schizophrenia judged improvement in positive symptoms as the most important potential treatment benefit,17,18 and although psychiatrists and patients had general concordance on treatment goals, psychiatrists tended to emphasize traditional outcomes (for example, the absence of positive and negative symptoms), whereas patients placed greater value on global measures such as improved quality of life.16 The early-phase European study by Bridges et al19 found that half of the 100 participants emphasized clinical goals, including reduced disease symptoms, while the remainder focused on functional goals; patients emphasizing functional goals were more likely to be receiving an LAI (44% vs 26%) and to state a preference for LAIs (46% vs 32%) compared with the overall group, which preferred OAPs to LAIs (61% vs 39%). In general, however, US data on patient attitudes and perceptions toward treatment goals and pharmacotherapy options in schizophrenia (particularly LAIs) are lacking. Additionally, greater understanding of the perspectives of patients with schizophrenia, including the impact of disease severity on treatment goals, is needed in routine clinical practice.
Given that benefits of effective schizophrenia treatment may include improvements in both physical and psychosocial facets of life, a deeper understanding of how patients prioritize treatment goals may facilitate patient engagement and shared decision-making, inform effective clinical management strategies, and yield insight on patients’ willingness to receive LAI treatment.19 A US, real-world, point-in-time survey was undertaken to understand priorities in patient treatment goals as selected by patients with schizophrenia and their psychiatrists and caregivers, taking into consideration differences in patient treatment goals by treatment group (LAIs vs OAPs), age group, and disease severity.
Methods
Survey Study Design
Data were drawn from the Adelphi Schizophrenia Disease Specific Programme™, a point-in-time survey of psychiatrists and their consulting adult patients with schizophrenia conducted from June to October 2019 in the United States. Participating psychiatrists had to be actively involved in management and treatment of patients with schizophrenia; they completed questionnaires about themselves, their practice, and their workload, as well as patient record forms (PRFs) for their next 8 consecutively consulting outpatients and 2 consecutive inpatients who matched the inclusion criteria. If inpatients were not available, then 2 additional outpatients were allowed to be included in the survey by the responding psychiatrist. The PRFs included patient demographics, diagnosis information, disease severity, consultation and hospitalization history, and clinical and subjective assessments of the patients and their treatments. Participation of psychiatrists was financially incentivized, with reimbursement upon survey completion according to fair market research rates.
Patients were eligible if they were aged ≥18 years, had a physician-confirmed diagnosis of schizophrenia, and were not currently participating in a clinical study. Patients meeting inclusion criteria were invited by their psychiatrist to voluntarily complete a patient self-completion questionnaire (PSC). If a caregiver was present at the consultation for a patient for whom the psychiatrist had completed a PRF, the caregiver was invited to voluntarily complete a caregiver self-completion questionnaire (CSC).
A complete description of the methods of the survey has been previously published and validated.20 Using a check box, participating patients, psychiatrists, and caregivers provided informed consent for use of their anonymized and aggregated data for research and publication in scientific journals. Psychiatrists provided informed consent during their self-completion of an electronic screening questionnaire; patients and caregivers provided their informed consent via a check box on the front of a self-completed pen-and-paper questionnaire, which was provided by the psychiatrists. Data were collected in such a way that respondents could not be identified directly; all data were aggregated and de-identified before receipt. The survey was conducted according to the EphMRA Code of Conduct and was approved by the Western Institutional Review Board (study protocol number AG8618).
Among other questions, psychiatrists, patients, and caregivers were each asked to select the 3 most important and 3 least important treatment goals for the patient from a list of 13 possible goals. Patients and caregivers also chose up to 3 treatment goals that the current medication helped to reach and up to 3 goals that were not met by the current medication. The full list of treatment goals included in the PRF, PSC, and CSC is provided in Table 1. Psychiatrist-reported data from the survey reflect the percentage of patients under the care of the responding psychiatrist for whom the psychiatrist had completed a PRF. For patients and caregivers, the percentages reported reflect the percentage of responding patients and caregivers.
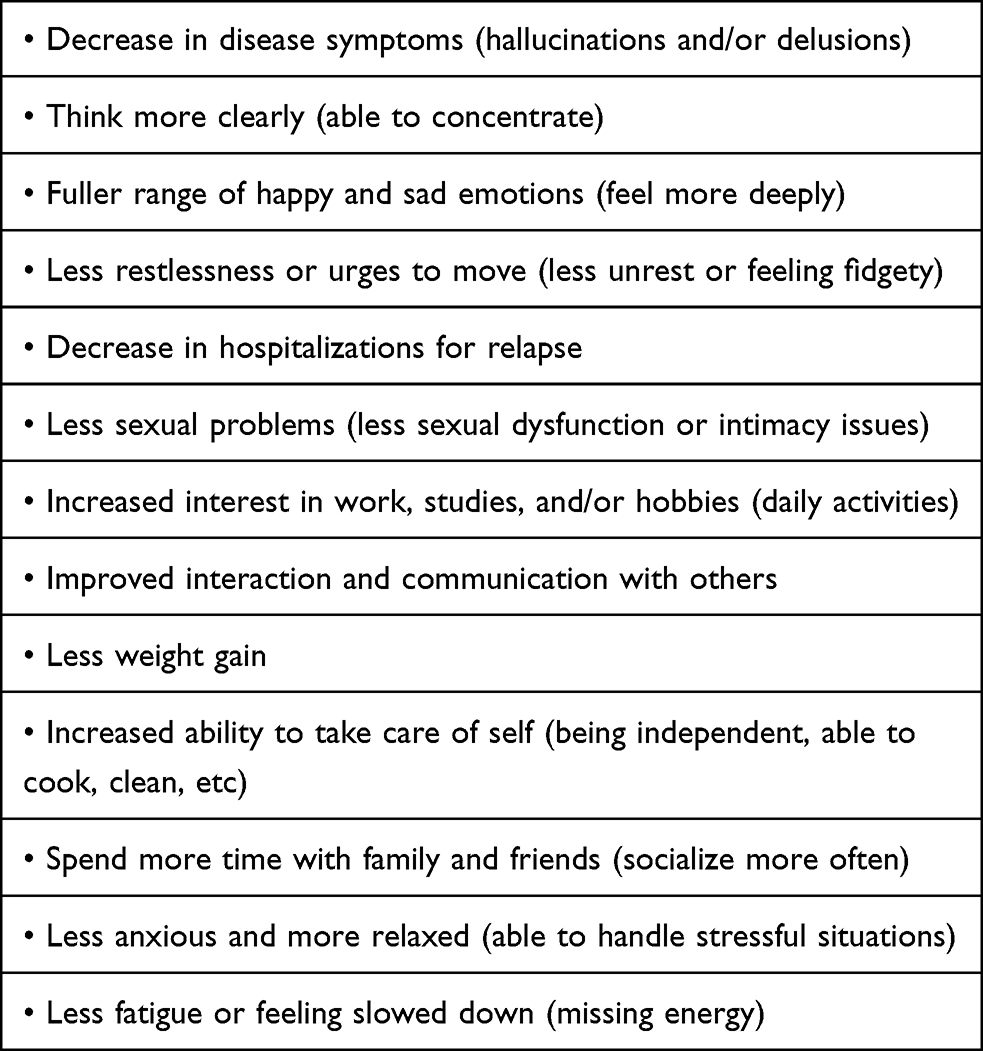 |
Table 1 Potential Treatment Goals Listed in Survey |
In each PRF, psychiatrists rated disease severity using the 7-point Clinical Global Impression-Severity scale (CGI-S)21 to answer the question: “Considering your total clinical experience with this particular population, how mentally ill is the patient at this time?” The choices available were: 1 = normal, not at all ill; 2 = borderline mentally ill; 3 = mildly ill; 4 = moderately ill; 5 = markedly ill; 6 = severely ill; and 7 = among the most extremely ill patients. As part of the PSC, patients completed the Work Productivity and Activity Impairment questionnaire (WPAI) about employment, absenteeism, impairment at work, productivity loss, and activity impairment.22 Caregivers also completed the WPAI in relation to how the patient’s condition has impacted their employment and activities. Differences in patient treatment goals stratified by treatment group (LAIs vs OAPs), age group (18–35, 36–65, and >65 years), and disease severity based on CGI-S23 and WPAI24 were also assessed.
Statistical Methods
This was an exploratory survey and the statistical analyses were primarily descriptive in nature. Descriptive statistics (mean, standard deviation, frequency) are presented for demographic and clinical information to describe the survey sample. Categorical variables are presented as frequency and percentage distributions when appropriate. Categorical variables were compared using either Fisher’s exact test for variables with two categories or chi-squared test for variables with more than two categories. Ordinal variables are reported as frequencies and percentages and/or medians and interquartile ranges, as appropriate for the individual variables. Continuous variables (for example, age, time since diagnosis, and questions with numeric rating scale responses) are presented as means and standard deviations, medians and interquartile ranges, and score ranges. Continuous variables from two groups were compared using the t-test or Mann–Whitney test depending on the distribution.
Data completeness are indicated by frequencies and percentages. The majority of variables for this analysis represent observed responses to individual closed-ended questions. These variables were analyzed as observed, with no imputation of missing data or aggregation across questions. Analyses that required statistical comparisons were conducted using STATA® 10 (StataCorp LP, College Station, Texas) and SPSS® 15.0 (IBM®, Armonk, New York).
Results
Survey Participants
Overall, 124 psychiatrists provided data for 1204 patients with schizophrenia, including 1135 on drug treatment comprising 207 inpatients (18%) and 928 outpatients (82%). A total of 247 patients (34%) had a caregiver. In all, 555 patients completed a PSC and 135 caregivers completed a CSC. Of the 1135 patients on drug treatment, more were receiving an OAP (884 [78%]) than a LAI (251 [22%]). A significantly greater proportion of patients in the LAI-treatment group (68 [27%]) than in the OAP-treatment group (139 [16%]) were being treated as inpatients (P <0.001).
Patient Demographics and Characteristics
Patient demographics and characteristics reported by psychiatrists are presented in Table 2. Compared with patients receiving OAPs, those on LAIs had a significantly longer mean time since their schizophrenia diagnosis (10.3 vs 7.8 years; P = 0.031) and a shorter mean time on their current medication regimen (1.7 vs 2.5 years; P = 0.009). More patients treated with LAIs were unable to finish their education due to schizophrenia (51% vs 38%; P = 0.002) and did not complete high school (25% vs 16%; P = 0.003), and fewer were employed full-time (4% vs 11%; P <0.001). Furthermore, more patients on LAIs were unemployed due to disability (56% vs 40%; P <0.001) and had a caregiver (37% vs 26%; P = 0.001) than those taking OAPs.
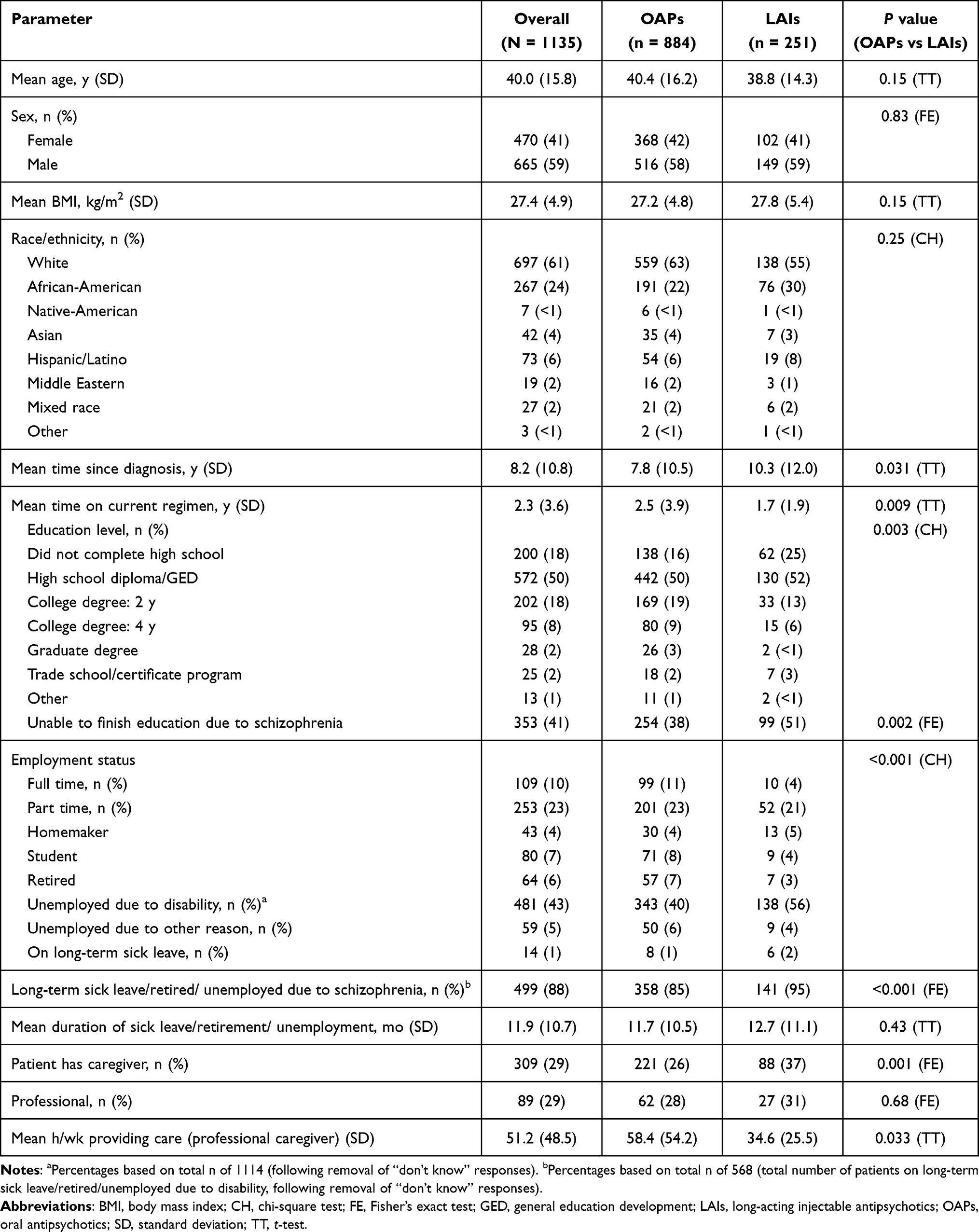 |
Table 2 Patient Demographics and Characteristics |
Differences in Patient Treatment Goals by Participant Group
Data for patient treatment goals most frequently selected as being most important and least important are presented in Figure 1 (top 5 goals selected based on average of patient, psychiatrist, and caregiver responses; data for all 13 goals are shown in Supplementary Table 1). “Decrease in disease symptoms” was most frequently selected as one of the top three choices for most important treatment goals for patients (64%), psychiatrists (selected for 63% of patients), and caregivers (selected for 68% of patients; Figure 1A). “Decrease in hospitalizations for relapse” was the second most important patient treatment goal for both psychiatrists (selected for 41% of patients) and caregivers (selected for 38% of patients), but was the seventh most important goal for patients (21%). The second most important treatment goal for patients (47%) was to “think more clearly,” a goal that was the fourth most important for psychiatrists (selected for 29% of patients) and caregivers (selected for 29% of patients). For least important treatment goals, patients, psychiatrists, and caregivers all included “less sexual problems” (43–59%) and “less weight gain” (38–44%) among their top 3 choices (Figure 1B).
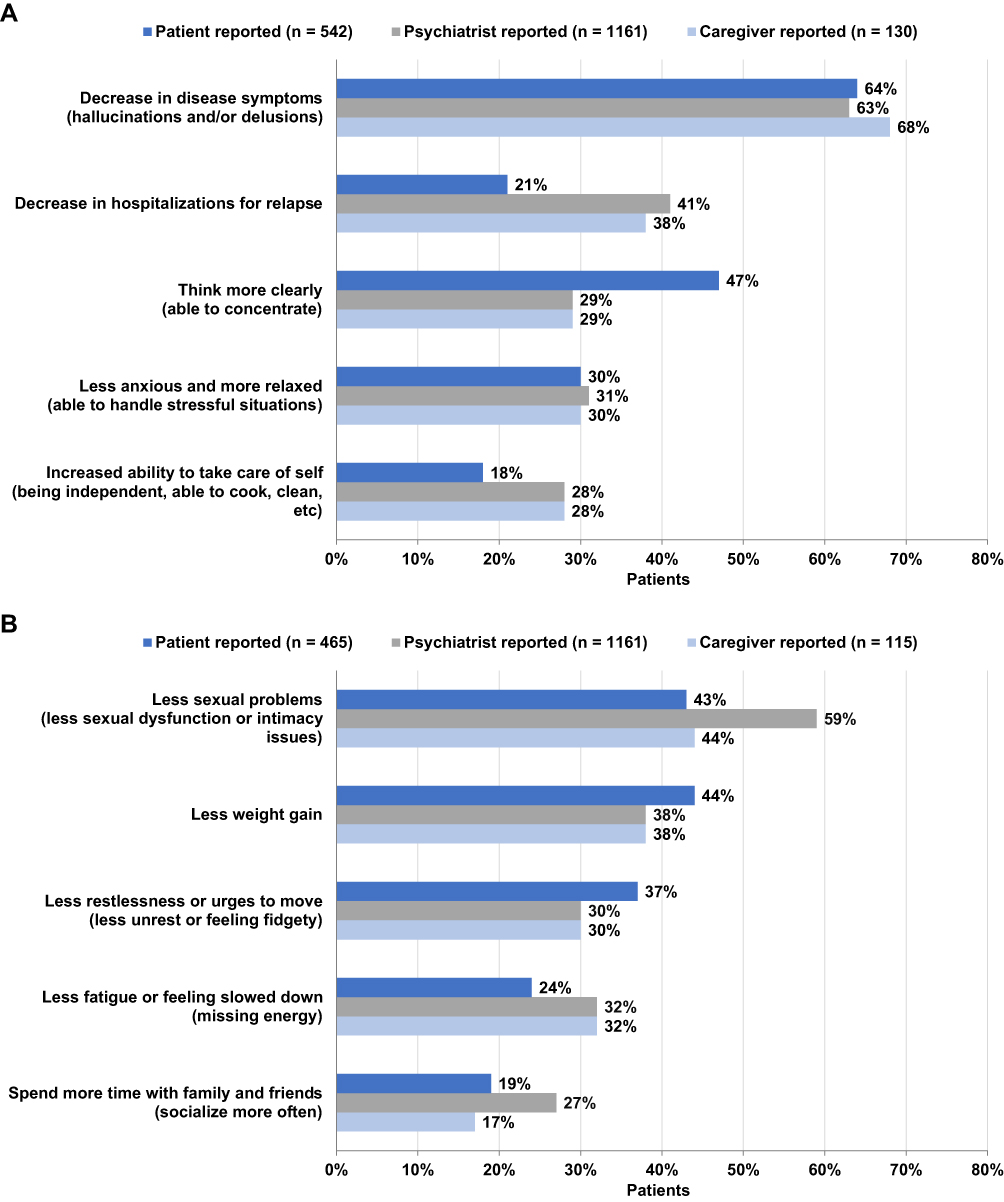 |
Figure 1 Most important (A) and least important (B) Patient treatment goals. Respondents were instructed to select the top 3 most important treatment goals and the top 3 least important treatment goals for patients; categories represent the 5 most frequently selected treatment goals (based on average of patient, psychiatrist, and caregiver responses). |
Patient treatment goals “met” and “not met” by the current medication as reported by patients and caregivers are presented in Figure 2 (top 5 goals selected based on average of patient and caregiver responses; data for all 13 goals are shown in Supplementary Table 2). Patients indicated that the treatment goals “decrease in disease symptoms” (68%) and “think more clearly” (39%) were met by their current medication (Figure 2A). Caregivers reported that the patient treatment goals “decrease in disease symptoms” (70%) and “decrease in hospitalizations for relapse” (41%) were met by patients’ current medication. A greater proportion of caregivers (30%) than patients (11%) identified “think more clearly” as a treatment goal that was not being met by the patients’ current medication (Supplementary Table 2).
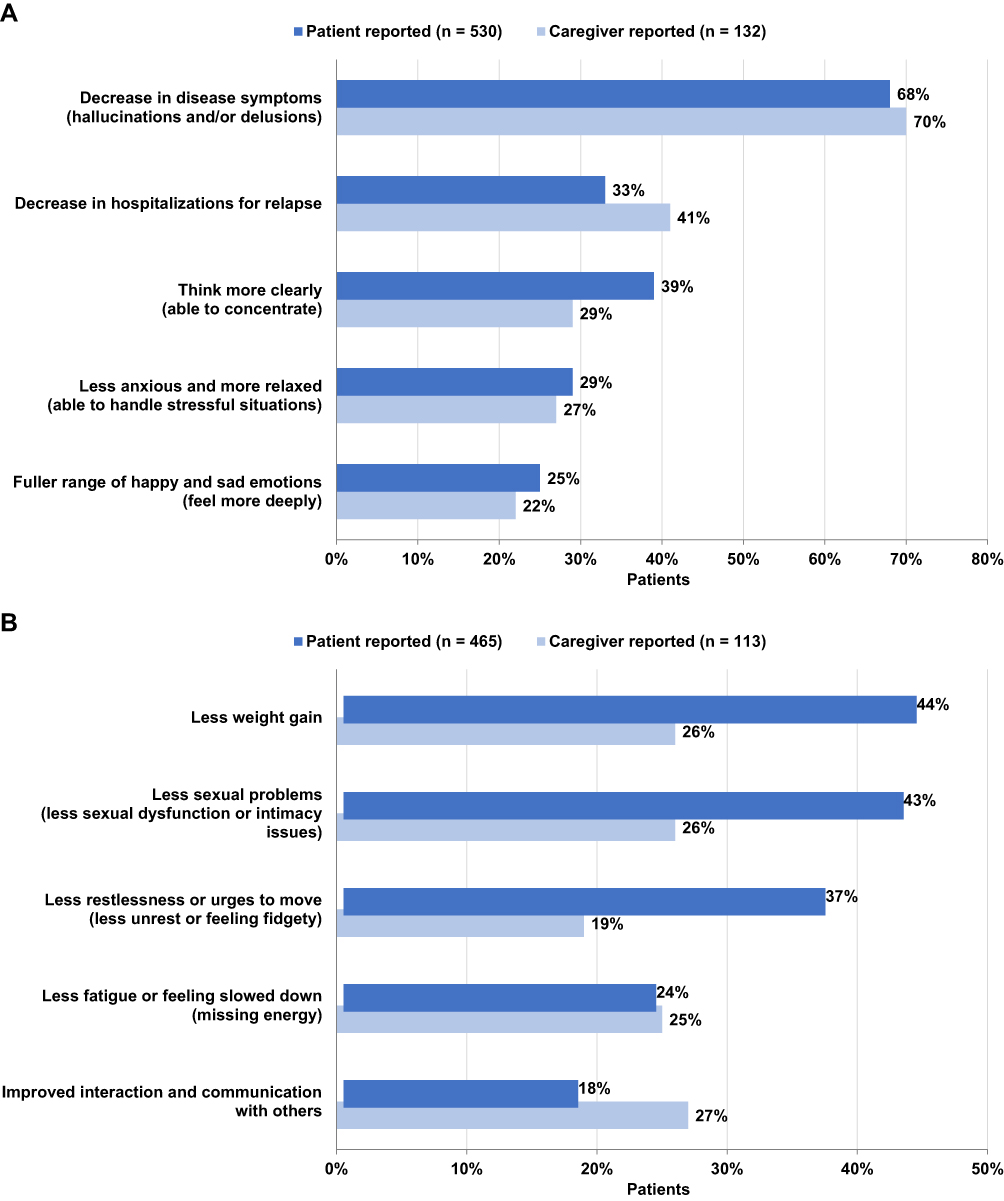 |
Figure 2 Patient treatment goals met (A) And not met (B) by current medication. Respondents were instructed to select up to 3 goals; categories represent the 5 most frequently selected goals (based on average of patient and caregiver responses). |
Differences in Treatment Goals Stratified by Treatment
Focusing on patient-reported treatment goals by drug therapy, patients in each treatment group reported similar preferences for their most important treatment goals (“decrease in disease symptoms” [OAPs: 65%; LAIs: 62%] and “think more clearly” [OAPs: 46%; LAIs: 53%]) and least important treatment goals (“less sexual problems” [OAPs: 42%; LAIs: 48%] and “less weight gain” [OAPs: 43%; LAIs: 46%]; Table 3).
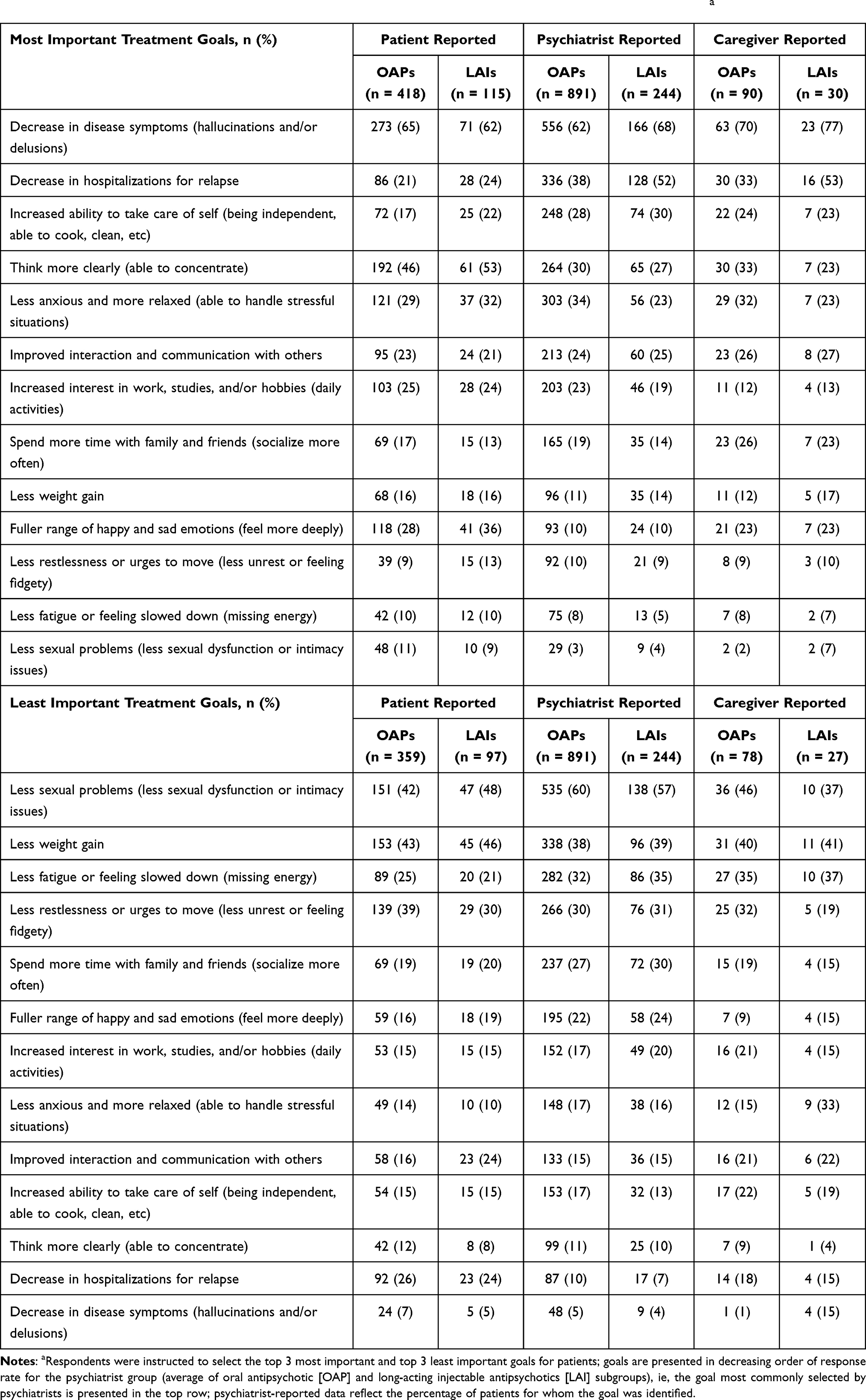 |
Table 3 Most Important and Least Important Patient Treatment Goals by Responder Group and Treatmenta |
A higher proportion of patients receiving LAIs than those receiving OAPs rated “fuller range of happy and sad emotions” (36% vs 28%) and “increased ability to take care of self” (22% vs 17%) as the most important treatment goals and “improved interaction and communications” (24% vs 16%) as a least important treatment goal. “Improved interaction and communication” was also more frequently an unmet treatment goal in patients receiving LAIs vs OAPs (24% vs 16%). “Less restlessness or urges to move” was chosen as a least important treatment goal by a higher percentage of patients taking OAPs than LAIs (39% vs 30%) and was more frequently indicated as an unmet goal with the current treatment (39% vs 30%; Table 4). Furthermore, patients taking LAIs reported more frequently that their current medication helped to achieve a “decrease in hospitalizations for relapse” than patients taking OAPs (39% vs 31%).
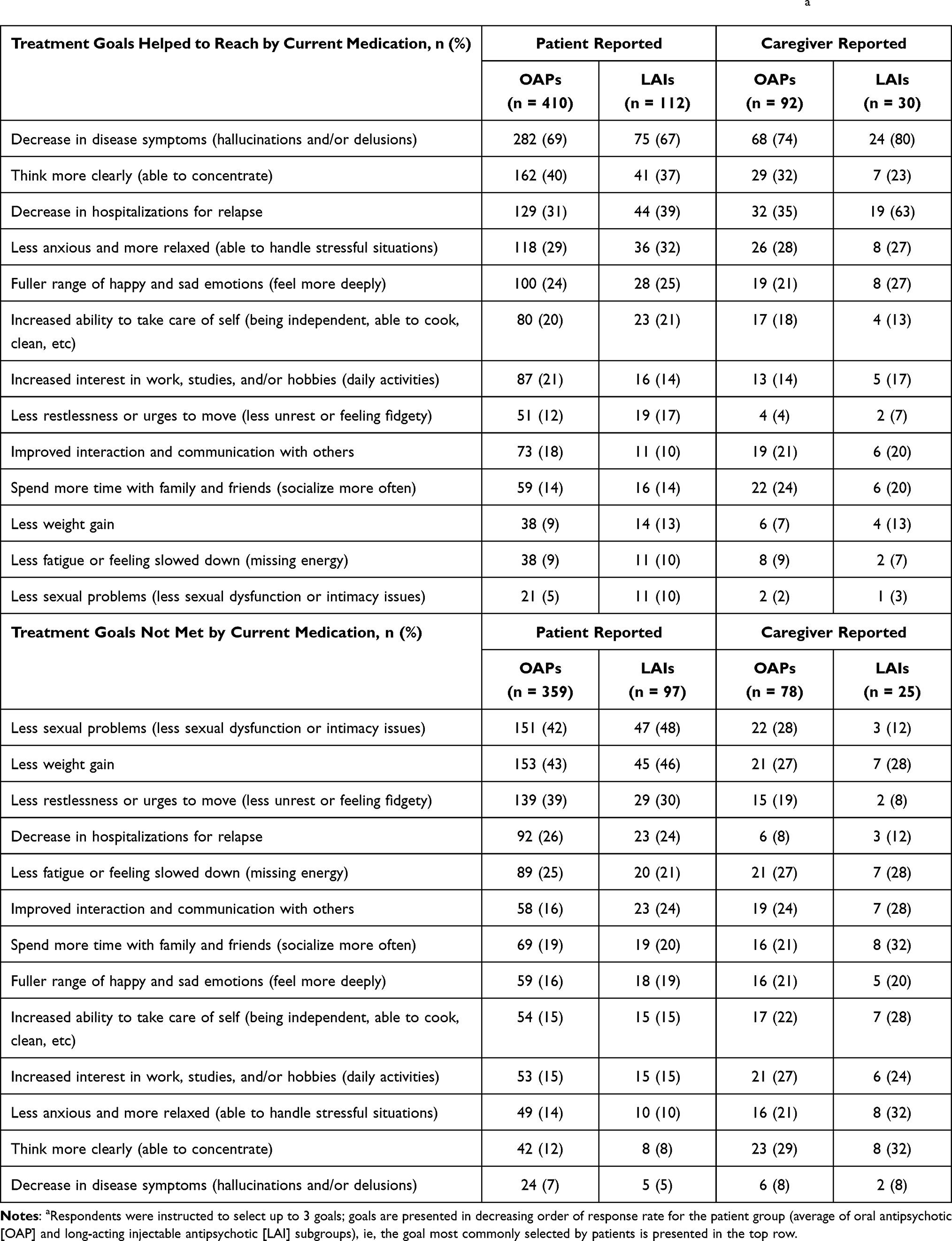 |
Table 4 Patient Treatment Goals Met or Not Met by Current Medication by Responder Group and Treatmenta |
In both treatment groups, patients’ most important treatment goals tended to overlap with the goals they selected as having been met by their current medication, and their least important treatment goals tended to coincide with those selected as not having been met by their current medication (Figures 1 and 2).
When treatment goals for the patient (most/least important; met/unmet by treatment) were examined by responder type (psychiatrist, patient, and caregiver), few differences were seen between goals for patients on LAIs and those on OAPs, similar to the trends observed for the overall (combined) responder population (Tables 3 and 4).
A “decrease in disease symptoms” was identified as an important patient treatment goal for a larger proportion of patients on LAIs vs OAPs based on responses from psychiatrists (68% vs 62%) and caregivers (77% vs 70%; Table 3). These responder groups also selected “less anxious and more relaxed” as an important treatment goal for a larger proportion of patients taking OAPs compared with LAIs (psychiatrists: 34% vs 23%; caregivers: 32% vs 23%).
Caregivers more often identified the most important patient treatment goals for patients receiving LAIs compared with OAPs as “decrease in disease symptoms” (77% vs 70%) and “decrease in hospitalizations for relapse” (53% vs 33%; Table 3), and reported larger proportions of patients receiving LAIs vs OAPs met these goals (80% vs 74% and 63% vs 35%, respectively; Table 4). For patients receiving OAPs vs LAIs, a larger proportion of caregivers chose “think more clearly” as an important treatment goal for the patient (33% vs 23%; Table 3).
Differences in Treatment Goals by Age Group
Overall, no significant differences in patient treatment goals by age group were identified and findings were generally similar to overall trends. Psychiatrists (selecting goals for 40% of patients) were more concerned about the ability of their patients aged >65 years to take care of themselves than either caregivers or patients (both 31%). Sexual problems were categorized as a lesser concern for patients aged >65 years by all 3 responder groups (patients, psychiatrists, and caregivers).
Differences in Treatment Goals by Psychiatrist-Reported Clinical Global Impression-Severity Scale Score and Treatment
Surveyed psychiatrists reported that 74% of all patients in the survey who were currently receiving LAIs (n = 239) had moderate-to-severe disease (CGI-S scores of 4–7) compared with 55% of patients receiving OAPs (n = 834). Similar levels of CGI improvement (much improved/very much improved) were reported for both treatment groups (68–69%). For moderately to severely ill patients receiving LAIs (grouping moderately, markedly, severely, and extremely ill patients: n = 178) compared with their counterparts receiving LAIs who had mild disease (grouping borderline and mildly ill patients: n = 61), psychiatrists more commonly chose “decrease in disease symptoms” (71% vs 52%) and “think more clearly” (31% vs 18%) as the most important treatment goals. For patients with mild disease severity compared with those with more severe disease, “increased interest in work, studies, and/or hobbies” (33% vs 16%), “spend more time with family and friends” (28% vs 11%), and “less anxious and more relaxed” (25% vs 18%) were more common treatment goals selected by psychiatrists.
Unemployment among patients was higher with moderate and severe disease than mild disease (mild disease: 63% [n = 35; normal/borderline/mildly ill]; moderate disease: 84% [n = 49]; severe disease: 82% [n = 28; markedly/severely/extremely ill]). Likewise, in patients who completed the WPAI questionnaire, the mean proportion of activity impairment due to schizophrenia increased with disease severity (mild: 32% [n = 32]; moderate: 49% [n = 47]; severe: 56% [n = 28]).
For patients with severe disease compared with those with mild disease, psychiatrists more often chose “decrease in disease symptoms” (71% vs 52%), “decrease in hospitalizations for relapse” (59% vs 54%), “increased ability to take care of self” (41% vs 31%), and “think more clearly” (34% vs 18%) as the most important treatment goals. For patients with mild disease compared with their counterparts with severe disease, psychiatrists more often chose social treatment goals: “increased interest in work, studies, and/or hobbies” (33% vs 12%), “spend more time with family and friends” (28% vs 7%), and “less anxious and more relaxed” (25% vs 16%).
Regardless of disease severity (mild [normal/borderline/mildly ill]: n = 61; moderate: n = 102; severe [markedly ill/severely ill/extremely ill]: n = 76), the top 2 patient treatment goals selected by psychiatrists for patients were “decrease in disease symptoms” (52%, 72%, and 71%, respectively) and “decrease in hospitalizations for relapse” (54%, 52%, and 59%, respectively).
Work Productivity and Activity Impairment Questionnaire: Caregiver Assessments
Results for the WPAI questionnaire showed that there were no significant differences among patients receiving LAIs vs OAPs with respect to work time missed, impairment while working, overall work impairment, or activity impairment as assessed by caregivers.
Discussion
Based on the results of this exploratory, real-world survey of US psychiatrists, patients, and their caregivers, patients with schizophrenia who were receiving LAIs appeared to have a longer duration of disease since their diagnosis and greater disease severity, and were significantly more likely to have a caregiver compared with patients taking OAPs. The survey results suggest that LAIs may represent an underused treatment option in clinical practice (in other words, these agents are mainly prescribed to patients who are later in the disease course with more severe illness), despite a growing body of evidence of utility in younger patients who are earlier in the course of their illness;3,9,14,15,25–27 however, longitudinal studies of prescribing patterns over the course of disease would be required to determine if this were true. Similar proportions of patients in each treatment group chose “decrease in disease symptoms” and “think more clearly” as their most important treatment goals; “less sexual problems” and “less weight gain” were selected as the least important. Caregivers reported that the treatment goal of “decrease in hospitalizations for relapse” was met more frequently for patients treated with LAIs than with OAPs. There was consensus among patients, psychiatrists, and caregivers on the most important treatment goal—“decrease in disease symptom”—regardless of patients’ current medication or age. This treatment goal was also the top choice of psychiatrists for patients with moderate and severe schizophrenia.
Identification of a primary consensus goal—“decrease in disease symptoms”—across the patient journey may help with discussions between patients, psychiatrists, and caregivers to inform effective management strategies early in the course of illness and encourage shared decision-making. The untapped potential of this collaborative process was highlighted by the findings of a study by Potkin et al,28 which found that the majority (67%) of patients and caregivers were not involved in antipsychotic treatment decision-making, and that psychiatrists offered LAIs as a treatment option to their patients only 50% of the time, despite all of the patients being indicated for a change in therapy. The authors of the study stressed the importance of increasing patient engagement in the decision-making process, as well as providing both psychiatrists and patients with more information on the simplicity, safety, and tolerability of LAIs, including positive feedback based on experiences/outcomes, to reduce resistance to new therapies on the part of patients and their providers. More recently, the PRELAPSE study3,29 concluded that proper training of practitioners can facilitate effective communications with patients regarding the advantages of LAIs and foster engagement in shared decision-making, resulting in high LAI acceptance rates even in early-stage disease.
The analysis by disease severity in the present survey showed a clear shift in psychiatrists’ perceptions regarding their patients’ most important treatment goals moving from one end of the disease severity spectrum to the other. The top goals selected for their patients with mild disease were more focused on improving productivity and social functioning (“increased interest in work, studies, and/or hobbies,” “spend more time with family and friends,” and “less anxious and more relaxed”), whereas the goals selected for their patients with severe disease were more focused on symptoms and activities of daily living (“decrease in disease symptoms,” “decrease in hospitalizations for relapse,” and “increased ability to take care of self”). As expected, unemployment and disability were shown to increase in parallel with disease severity. Information regarding the correlation of disease severity and treatment goals, in conjunction with the broader analysis of treatment goals discussed above, can be crucial to psychiatrists as they engage with patients and caregivers in the shared decision-making process regarding the optimal individualized treatment strategy.
There were several limitations associated with this survey. First, the only patients included in the sample were consecutively consulting patients of the surveyed psychiatrists who met the patient inclusion criteria, and they may not fully represent the overall US population of patients with schizophrenia. In addition, patients who consult their psychiatrist frequently were more likely to be included in this sample. Second, although psychiatrists were requested to collect data on a series of consecutively consulting patients to avoid selection bias, in the absence of randomization, adherence was contingent on the integrity of the participating psychiatrists rather than via a formalized source-verification procedure. Moreover, diagnosis in the target patient group was based primarily on the judgement and diagnostic skills of the respondent psychiatrist rather than on a formalized diagnostic checklist, although patients were managed in accordance with the same routine diagnostic procedures representative of that clinical practice setting. Third, the quality of data was largely dependent on the accurate reporting of information by psychiatrists, patients, and caregivers, which may be subject to recall bias. Fourth, the inclusion criteria that governed the selection of psychiatrists (treatment of a minimum number of patients with schizophrenia and active involvement in patient management and treatment decisions) were minimal and, consequently, inclusion was likely influenced by willingness to take part in the survey. Selection bias was therefore possible because the participating psychiatrists were a pragmatic sample and may not represent the overall population of psychiatrists treating patients with schizophrenia. Finally, due to the point-in-time design of the survey, it cannot be used to demonstrate cause and effect.
Conclusions
This survey identified a primary consensus goal of a decrease in disease symptoms across the patient journey, as well as partial discordance among the responder groups with respect to their top 3 treatment goals. The findings of this survey highlight the importance of shared decision-making and may help facilitate and encourage discussions among patients, psychiatrists, and caregivers to inform effective management strategies early in the course of illness.
Abbreviations
CGI-S, Clinical Global Impression-Severity scale (CGI-S); CSC, caregiver self-completion questionnaire; LAI, long-acting injectable antipsychotic; OAP, oral antipsychotic; PRF, patient record form; PSC, patient self-completion questionnaire; WPAI, Work Productivity and Activity Impairment questionnaire.
Data Sharing Statement
All data that support the findings of this study are the intellectual property of Adelphi Real World. Legitimate research requests for supportive data will be considered. Requests for access should be addressed directly to Jason Shepherd at [email protected].
Ethics Approval and Informed Consent
Participating patients, psychiatrists, and caregivers provided informed consent for use of their anonymized and aggregated data for research and publication in scientific journals. Data were collected in such a way that respondents could not be identified directly; all data were aggregated and de-identified before receipt. The survey was conducted according to the EphMRA Code of Conduct and was approved by the Western Institutional Review Board (study protocol number AG8618).
Acknowledgments
Editorial support, funded by Otsuka Pharmaceutical Development & Commercialization, Inc., was provided by BioScience Communications, New York, New York, USA. All authors reviewed this manuscript in draft form and provided critical input during the development process, and all authors approved its submission for publication. These findings were presented, in part, at NEI Max, Colorado Springs, Colorado, November 5–8, 2020.
Author Contributions
All authors were involved in 1) conception or design, or analysis and interpretation of data; 2) drafting and revising the article; 3) providing intellectual content of critical importance to the work described; and 4) final approval of the version to be published, and therefore meet the criteria for authorship in accordance with the International Committee of Medical Journal Editors (ICMJE) guidelines (accessible at: http://www.icmje.org/). In addition, all named authors take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Funding
Data collection was undertaken by Adelphi Real World as part of an independent survey entitled the Adelphi Schizophrenia Disease Specific Programme™, sponsored by multiple pharmaceutical companies, of which two were Otsuka Pharmaceutical Europe Ltd. and Lundbeck LLC. The survey study described here using data from the Adelphi Schizophrenia Disease Specific Programme and the resultant publication were funded by Otsuka Pharmaceutical Development & Commercialization, Inc. and Lundbeck LLC.The sponsors were involved in the survey questionnaire design and conduct, analysis of the results, generation of the manuscript, and approval to submit the manuscript for publication.
Disclosure
Dr Fitzgerald is an employee of Lundbeck LLC. J. Shepherd, H. Bailey, M. Berry, and J. Wright are employees of Adelphi Real World. Dr Chen is an employee of Otsuka Pharmaceutical & Commercial Development, Inc. Abilify Maintena® (aripiprazole once-monthly 400 mg), a long-acting injectable antipsychotic indicated in the US for the treatment of schizophrenia and maintenance monotherapy of bipolar I disorder in adult patients, is distributed by Otsuka America Pharmaceutical, Inc., Rockville, MD, USA and co-marketed by Otsuka and Lundbeck, Deerfield, IL, USA. The authors report no other conflicts of interest in this work.
References
1. Millier A, Schmidt U, Angermeyer MC, et al. Humanistic burden in schizophrenia: a literature review. J Psychiatr Res. 2014;54:85–93. doi:10.1016/j.jpsychires.2014.03.021
2. Kane KM, Correll CU. Optimizing treatment choices to improve adherence and outcomes in schizophrenia. J Clin Psychiatry. 2019;80(5):IN18031AH1C. doi:10.4088/JCP.IN18031AH1C
3. Kane JM, Schooler NR, Marcy P, et al. Effect of long-acting injectable antipsychotics vs usual care on time to first hospitalization in early-phase schizophrenia. A randomized clinical trial. JAMA Psychiatry. 2020;77(12):1217–1224. doi:10.1001/jamapsychiatry.2020.2076
4. American Psychiatric Association. The American psychiatric association practice guideline for the treatment of patients with schizophrenia, third edition; 2021. Available from: https://psychiatryonline.org/doi/book/10.1176/appi.books.9780890424841.
5. Correll CU, Citrome L, Haddad PM, et al. The use of long-acting injectable antipsychotics in schizophrenia: evaluating the evidence. J Clin Psychiatry. 2016;77(suppl 3):1–24. doi:10.4088/JCP.15032su1
6. Carbon M, Correll CU. Clinical predictors of therapeutic response to antipsychotics in schizophrenia. Dialogues Clin Neurosci. 2014;16(4):505–524.
7. Heres S. Long-acting injectable antipsychotics: an underutilized treatment option. J Clin Psychiatry. 2014;75(11):1263–1265. doi:10.4088/JCP.14com09541
8. Kane JM, Kishimoto T, Correll CU. Non-adherence to medication in patients with psychotic disorders: epidemiology, contributing factors and management strategies. World Psychiatry. 2013;12(3):216–226. doi:10.1002/wps.20060
9. Novick D, Haro JM, Suarez D, et al. Predictors and clinical consequences of non-adherence with antipsychotic medication in the outpatient treatment of schizophrenia. Psychiatry Res. 2010;176(2–3):109–113. doi:10.1016/j.psychres.2009.05.004
10. Tiihonen J, Mittendorfer-Rutz E, Majak M, et al. Real-world effectiveness of antipsychotic treatments in a nationwide cohort of 29 823 patients with schizophrenia. JAMA Psychiatry. 2017;74(7):686–693. doi:10.1001/jamapsychiatry.2017.1322
11. Iyer S, Banks N, Roy M-A, et al. A qualitative study of experiences with and perceptions regarding long-acting injectable antipsychotics: part II-physician perspectives. Can J Psychiatry. 2013;58(5Suppl 1):23S–29S. doi:10.1177/088740341305805s04
12. Sajatovic M, Ross R, Legacy SN, et al. Identifying patients and clinical scenarios for use of long-acting injectable antipsychotics – expert consensus survey part I. Neuropsychiatr Dis Treat. 2018;14:1463–1474. doi:10.2147/NDT.S167394
13. Kishimoto T, Hagi K, Nitta M, et al. Effectiveness of long-acting injectable vs oral antipsychotics in patients with schizophrenia: a meta-analysis of prospective and retrospective cohort studies. Schizophr Bull. 2018;44(3):603–619. doi:10.1093/schbul/sbx090
14. Schreiner A, Aadamsoo K, Altamura AC, et al. Paliperidone palmitate versus oral antipsychotics in recently diagnosed schizophrenia. Schizophr Res. 2015;169(1–3):393–399. doi:10.1016/j.schres.2015.08.015
15. Subotnik KL, Casaus LR, Ventura J, et al. Long-acting injectable risperidone for relapse prevention and control of breakthrough symptoms after a recent first episode of schizophrenia. A randomized clinical trial. JAMA Psychiatry. 2015;72(8):822–829. doi:10.1001/jamapsychiatry.2015.0270
16. Bridges JFP, Slawik L, Schmeding S, et al. A test of concordance between patient and psychiatrist valuations of multiple treatment goals for schizophrenia. Health Expect. 2013;16(2):164–176. doi:10.1111/j.1369-7625.2011.00704.x
17. Eiring Ø, Landmark BF, Aas E, et al. What matters to patients? A systematic review of preferences for medication-associated outcomes in mental disorders. BMJ Open. 2015;5(4):e007848. doi:10.1136/bmjopen-2015-007848
18. Levitan B, Markowitz M, Mohamed AF, et al. Patients’ preferences related to benefits, risks, and formulations of schizophrenia treatment. Psychiatr Serv. 2015;66(7):719–726. doi:10.1176/appi.ps.201400188
19. Bridges JFP, Beusterien K, Heres S, et al. Quantifying the treatment goals of people recently diagnosed with schizophrenia using best-worst scaling. Patient Prefer Adherence. 2018;12:63–70. doi:10.2147/PPA.S152870
20. Anderson P, Benford M, Harris N, et al. Real-world physician and patient behaviour across countries: disease-specific programmes – a means to understand. Curr Med Res Opin. 2008;24(11):3063–3072. doi:10.1185/03007990802457040
21. Busner J, Targum SD. The clinical global impressions scale. Applying a research tool in clinical practice. Psychiatry. 2007;4(7):28–37.
22. Reilly Associates. WPAI scoring. Available from: http://www.reillyassociates.net/WPAI_Scoring.html.
23. Guy W. Clinical Global Impressions. ECDEU Assessment Manual for Psychopharmacology, Revised (DHEW Publ. No. ADM 76-338). Rockville, MD: National Institute of Mental Health; 1976:218–222.
24. Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. PharmacoEconomics. 1993;4(5):353–365. doi:10.2165/00019053-199304050-00006
25. Giordano G, Tomassini L, Cuomo I, et al. Aripiprazole long-acting injection during first episode schizophrenia – an exploratory analysis. Front Psychiatry. 2020;10:935. doi:10.3389/fpsyt.2019.00935
26. Zhornitsky S, Stip E. Oral versus long-acting injectable antipsychotics in the treatment of schizophrenia and special populations at risk for treatment nonadherence: a systematic review. Schizophr Res Treat. 2012;2012:407171.
27. Peitl V, Stefanovic M, Orlovic I, et al. Long acting aripiprazole influences cognitive functions in recent onset schizophrenia. Psychopharmacology. 2021;238(6):1563–1573. doi:10.1007/s00213-021-05788-w
28. Potkin S, Bera R, Zubek D, Lau G. Patient and prescriber perspectives on long-acting injectable (LAI) antipsychotics and analysis of in-office discussion regarding LAI treatment for schizophrenia. BMC Psychiatry. 2013;13:261. doi:10.1186/1471-244X-13-261
29. Kane JM, Schooler NR, Marcy P, et al. Patients with early-phase schizophrenia will accept treatment with sustained-release medication (long-acting injectable antipsychotics): results from the recruitment phase of the PRELAPSE trial. J Clin Psychiatry. 2019;80(3):18m12546. doi:10.4088/JCP.18m12546
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.