")
Back to Journals » Infection and Drug Resistance » Volume 13
Treatment Failure in Urinary Tract Infections: A Warning Witness for Virulent Multi-Drug Resistant ESBL- Producing Escherichia coli
Authors Naziri Z , Derakhshandeh A, Soltani Borchaloee A, Poormaleknia M, Azimzadeh N
Received 2 April 2020
Accepted for publication 1 June 2020
Published 17 June 2020 Volume 2020:13 Pages 1839—1850
DOI https://doi.org/10.2147/IDR.S256131
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Zahra Naziri, Abdollah Derakhshandeh, Arash Soltani Borchaloee, Meisam Poormaleknia, Negar Azimzadeh
Department of Pathobiology, School of Veterinary Medicine, Shiraz University, Shiraz, Iran
Correspondence: Zahra Naziri
Department of Pathobiology, School of Veterinary Medicine, Shiraz University, Shiraz 71345– 1731 Tel +98 71 36138668
Fax +98 71 32286940
Email [email protected]
Background: Global increase in the prevalence of virulent extended-spectrum beta-lactamase (ESBL)-producing uropathogenic Escherichia coli (UPEC), which is also multi-drug resistant (MDR), leads to increase in severity of urinary tract infections (UTIs), decrease in the efficacy of the first-line antibiotics, and therefore increase in the morbidity and mortality rates.
Methods: We investigated the distribution of ESBL-producing UPEC in 78 E. coli isolates from community-acquired UTI patients in southern Iran. The prevalence of three major ESBL genes, antimicrobial resistance patterns against 15 conventional antibiotic disks, and the presence of 11 important virulence genes that involve in the development and progression of UTIs were evaluated in these isolates.
Results: Of the UPECs, 34.6% were ESBL-positive and 96.3% of the ESBL-producers were MDR. Among the ESBL-producers, 100% harbored blaCTX-M, 63% harbored blaSHV, and 11.1% harbored blaTEM genes. ESBL-producers showed a higher level of resistance to the tested cephalosporins, fluoroquinolones, trimethoprim-sulfamethoxazole, and tetracycline than non-ESBL producers. All isolates were resistant to the tested penicillins. Prevalence of resistance to about two-third of the tested antibiotics was higher than 50% and 93.6% of the isolates were MDR. High prevalence of virulence factors particularly the adhesins (82.1% csgA, 73.1% fimH genes) and siderophore (73.1% sitA gene) was seen in the UPECs. But fortunately in MDR isolates, the virulence score and prevalence of hemagglutinin (tsh), hemolysin toxin (hlyD) and invasin (ibeA) genes were lower than in non-MDR UPECs. Shockingly, among the 15 common antibiotics, only nitrofurantoin (< 20% resistance) could be recommended as an appropriate drug for the treatment of UTIs due to our ESBL-producer UPECs.
Conclusion: The alarming level of virulent MDR ESBL-producer E. coli strains in this study necessitates the performing of an antibiotic stewardship program, regional screening of ESBL-producers and their virulence properties to select appropriate antibiotic, or designing new therapeutic methods for UTIs by inactivation of the essential virulence factors of UPECs.
Keywords: uropathogenic Escherichia coli, extended spectrum beta-lactamases, multi-drug resistance, virulence factor, urinary tract infection
Introduction
Urinary tract infections (UTIs) due to uropathogenic Escherichia coli (UPEC) are common infections in the community, especially in female patients.1,2 The existence of several virulence factors (VFs) in UPEC isolates could affect the occurrence and severity of UTIs.3 Some of these VFs include genes encoding adhesins, such as type-1 fimbriae (fimH), pyelonephritis-associated pili (papA, papC), afimbrial adhesins (afa), curli fimbriae (csgA), and temperature-sensitive hemagglutinin (tsh), which have a role in the colonization of bacteria in the urinary tract and initiation of UTIs, genes encoding toxins that have adverse effects on the host and contribute to the pathogenicity of these strains, such as α-hemolysin (hlyD), genes encoding invasins, such as ibeA which is involved in brain microvascular endothelial cell invasion, genes encoding protectins, such as increased serum survival (iss), which protects E. coli against the serum bactericidal activity, genes encoding siderophores, such as the iron transporter sitA, which assists in the growth of bacteria, and pathogenicity island marker malX, which has a role in the transport of glucose and maltose.4–6
The increase of antibiotic resistance is an emergency health issue in the management of UTIs. One of the most commonly used antibiotics for the treatment of UTIs is beta-lactams.7 Extended-spectrum beta-lactamases (ESBL) are enzymes produced by certain bacteria including some strains of E. coli, and are able to hydrolyze penicillins, first–third generation cephalosporins, and monobactams (aztreonam). Three main groups of ESBL enzymes include TEM, SHV, and CTX-M, which are inhibited by clavulanic acid, tazobactam, or sulbactam.7
Simultaneous resistance to other antibiotic classes such as fluoroquinolones, aminoglycosides, trimethoprim-sulfamethoxazole, tetracyclines, and chloramphenicol, which are often encoded in the same plasmids that harbore the ESBL genes, can complicate and limit the therapeutic options for treatment of infections due to ESBL-producing E. coli. This may increase the morbidity costs and mortality rate of UTI patients.7
Regarding the geographical variation and the changes over time, it is critical to perform periodic regional and global epidemiological studies to find the frequencies and patterns of drug resistance, and also the occurrence of ESBL producers among UPEC isolates. These data could be useful for choosing better therapeutic strategies and for infection control measures and also help to reduce the public health complications due to untreated or recurrent UTIs. So, the present investigation was done for phenotypic and genotypic evaluation of the distribution of ESBL-producing UPEC in isolates from community-acquired UTI patients in southern Iran. In addition, the antimicrobial resistance patterns and the presence of some important VFs that are involved in the development, progression, and severity of UTIs were evaluated in these isolates.
Materials and Methods
Sample Collection and Isolation of E. coli
We designed this study on 78 urinary E. coli isolates which were collected during 8 months from midstream urine samples of outpatients suspected to UTIs [This study was approved by the Shiraz Medical University Ethics Committee, Shiraz, Iran. Informed consent was obtained from participating patients]. These patients had been referred to the microbiology laboratory of Shahid Faghihi hospital (Shiraz, Iran) from various regions of southern Iran (one colony from each patient). The isolates were confirmed as E. coli by observation of their phenotypic characteristics on Eosin methylene blue agar (Merck, Darmstadt, Germany) and MacConkey agar (Merck), and also by using conventional biochemical tests.8 The confirmed isolates were cultured in Tryptic soy broth (Merck) and conserved with 20% glycerol at −70°C.
Phenotypic Identification of ESBL-Producing UPEC
We used the CLSI phenotypic confirmatory test for identification of ESBL-producing isolates.9 In this method, discs containing cefotaxime (30 μg) and ceftazidime (30 μg) alone and combination of cefotaxime-clavulanic acid (30/10 μg) (Padtan Teb, Iran) were applied and the isolates which exhibited at least a 5-mm increase in the inhibition zone diameter for the cefotaxime-clavulanic acid disc versus cefotaxime disc alone were considered as ESBL producers.9 Escherichia coli ATCC® 25922 strain was used as quality control.9
Molecular Identification of ESBL-Producing UPEC
We used PCR and electrophoresis techniques to determine the presence of three main types of β- lactamase genes including blaCTX-M, blaSHV, and blaTEM in E. coli isolates. DNA of isolates was extracted by the boiling method.8 The primer sequences and PCR conditions for detection of β- lactamase genes are shown in Table 1.
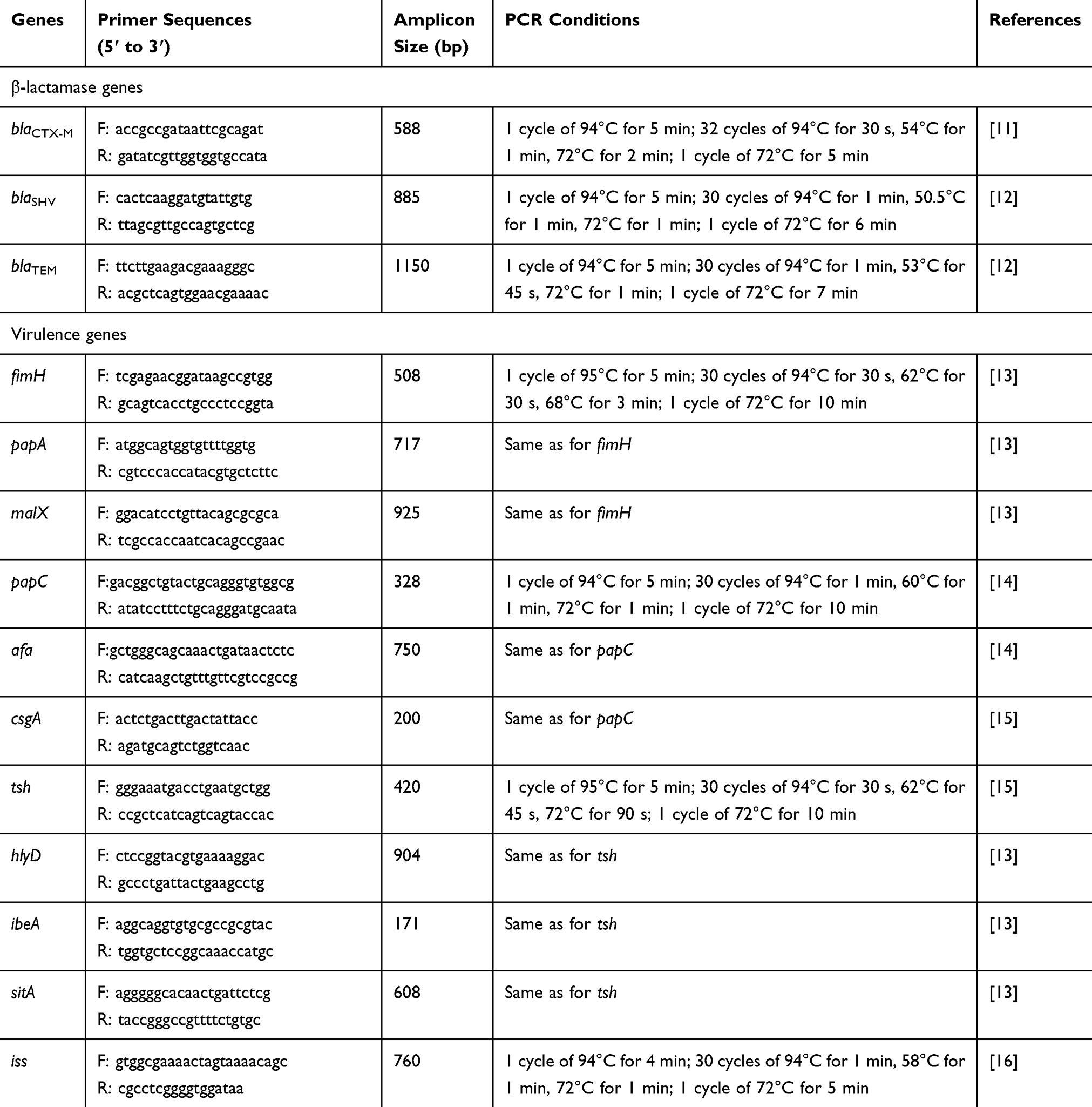 |
Table 1 List of Primers, Expected Amplicon Size, and the PCR Conditions |
Antimicrobial Susceptibility Testing
Antimicrobial susceptibility against penicillin, ampicillin, amoxicillin, cephalexin, cefixime, ceftriaxone, ceftazidime, cefotaxime, gentamicin, amikacin, ciprofloxacin, levofloxacin, trimethoprim-sulfamethoxazole (TMP-SMX), nitrofurantoin, and tetracycline (Padtan Teb) was evaluated by the Kirby–Bauer disk diffusion method according to the National Committee for Clinical Laboratory Standards Institute (CLSI).9 Escherichia coli ATCC® 25922 strain was used as quality control.9
Multi-drug resistance (MDR) was defined as non-susceptibility to at least one agent in three or more antimicrobial classes.10
Detection of Virulence Factor
For evaluation of the prevalence of fimH, papA, papC, afa, csgA, tsh, hlyD, sitA, ibeA, malX, and iss genes in UPECs, we used the genomic DNA of the isolates, which was extracted by the boiling method in the previous step. Three multiplex PCR processes were designed for groups of fimH, papA, and malX genes, papC, afa, and csgA genes, and tsh, hlyD, ibeA, and sitA genes. The iss gene was amplified by uniplex PCR. The primer sequences and the PCR conditions for the detection of these virulence genes are shown in Table 1. Finally, all the PCR products were electrophoresed on a 1% agarose gel (Parstous, Iran) which contained Safe Stain (YTA, Iran), and visualized using a UV-transilluminator (UVitec, Cambridge, UK).
Statistical Analysis
Results were analyzed using the t-test, Pearson’s chi-square test, or Fisher’s exact test. A value of p≤0.05 was regarded as statistically significant (SPSS 16.0, SPSS Inc., Chicago, IL, USA).
Results
The 78 urine samples which contain E. coli belonged to 53 (67.9%) female and 25 (32.1%) male patients suffering from community-acquired UTIs.
Phenotypic and Genotypic Identification of ESBL-Producing UPEC
By using the CLSI phenotypic confirmatory test, among the 78 E. coli isolates, 27 (34.6%) isolates were detected as ESBL producers. Thus, 14 strains of them belonged to female patients and 13 strains belonged to male patients.
Overall, the prevalences of β-lactamase genes including blaCTX-M, blaSHV, and blaTEM in 78 E. coli isolates were 29 (37.2%), 37 (47.4%), and 12 (15.4%), respectively. Based on the gender of the source of UPEC isolates, the prevalence of blaCTX-M gene was 16 (30.2%) and 13 (52%), blaSHV gene was 25 (47.2%) and 12 (48%), and blaTEM was 8 (15.1%) and 4 (16%), for females’ and males’ isolates, respectively.
All the 27 (100%) UPEC isolates that phenotypically confirmed as ESBL producers harbored blaCTX-M gene, 17 (63%) harbored blaSHV gene, and 3 (11.1%) harbored blaTEM gene.
The distribution of three main types of β-lactamase genes in UPEC isolates that were phenotypically confirmed as ESBL producers revealed four patterns. Two isolates (7.4%) harbored all the three tested ESBL genes, 15 isolates (55.6%) harbored blaCTX-M and blaSHV, one isolate (3.7%) harbored blaCTX-M and blaTEM, and 9 isolates (33.3%) only harbored blaCTX-M gene.
The prevalence of blaCTX-M (p<0.001) and blaSHV (p=0.04) genes was significantly higher in ESBL producers than non-ESBL producers, but for blaTEM gene prevalence no significant difference (p>0.05) was found in these two groups of isolates. The prevalence of blaCTX-M, blaSHV, and blaTEM in MDR and non-MDR isolates was not significantly different (p>0.05).
Antimicrobial Susceptibility Testing
Results of antimicrobial susceptibility testing against 15 antimicrobial agents showed that all 78 (100%) UPEC isolates were resistant to penicillins (penicillin, ampicillin, and amoxicillin). The lowest prevalence of resistance was seen against aminoglycosides (16.7% to gentamicin, 21.8% to amikacin) and then nitrofurantoin (23.1%) (Table 2). Also, 2/78 (2.6%) of UPEC isolates were resistant to all 15 tested antimicrobial agents and 41/78 (52.6%) of UPEC isolates were resistant to at least half (≥8) of the tested antimicrobial agents. Also, four (5.1%) UPEC isolates only show resistance against the tested penicillins.
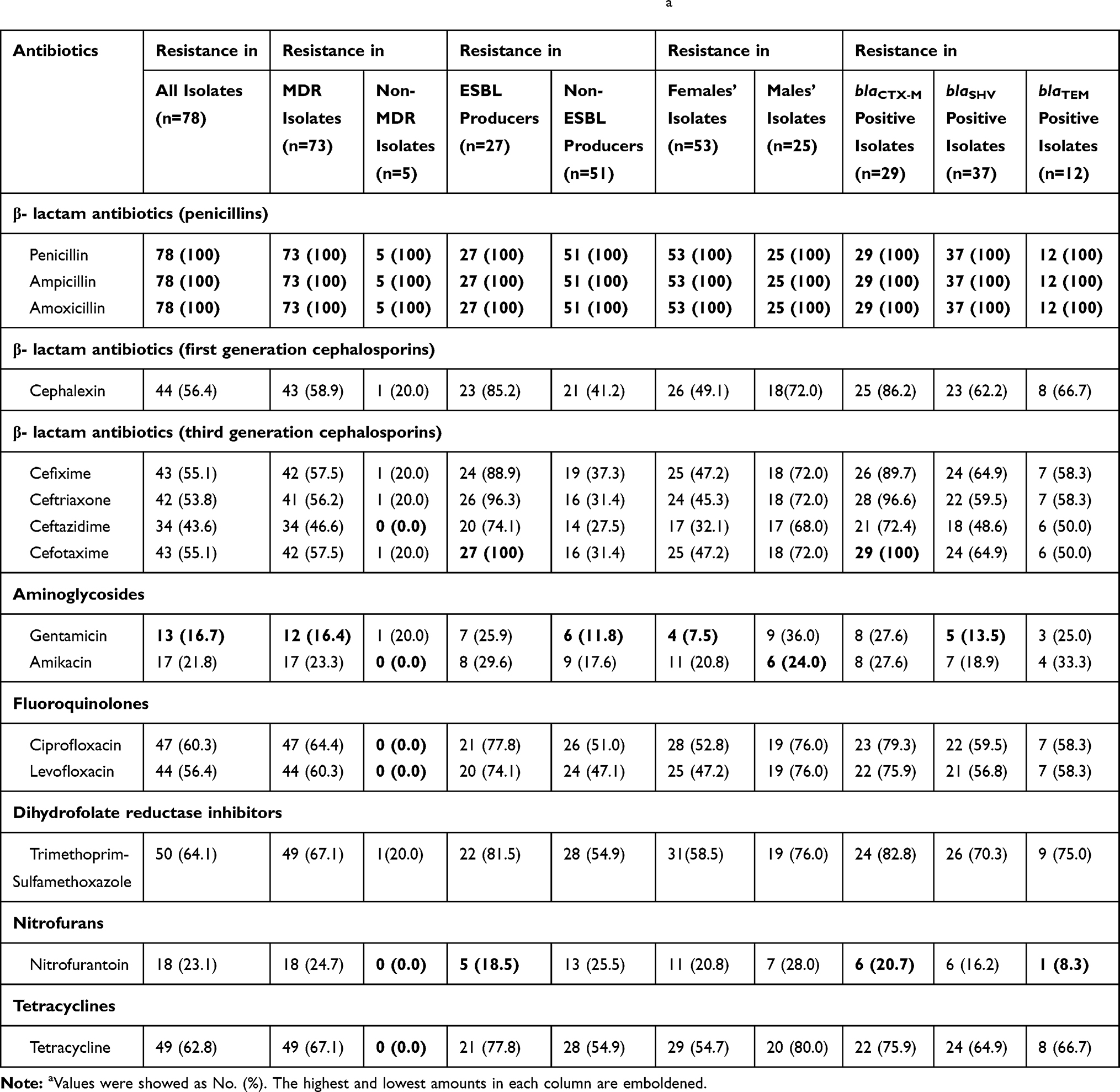 |
Table 2 Prevalence of the Antimicrobial Resistance Among the UPEC Isolatesa |
Overall, 53 different resistance patterns were found among the 78 tested isolates, of which the resistance pattern of penicillin, ampicillin, amoxicillin, cephalexin, cefixime, ceftriaxone, ceftazidime, cefotaxime, ciprofloxacin, levofloxacin, trimethoprim- sulfamethoxazole, and tetracycline that was seen in six UPEC isolates was the predominant pattern.
Approximately 93.6% (73/78) of the UPEC isolates were multi-drug resistant (MDR). So that the 94.3% (50/53) of females’ isolates and 92% (23/25) of males’ were MDR. Also, the frequency of MDR in ESBL-producer isolates was 96.3% (26/27). The prevalence of MDR was not significantly different in ESBL-producer and non-ESBL producer isolates (p>0.05).
The prevalence of antimicrobial resistance against the 15 tested antimicrobial agents in all UPEC isolates, and also separately in MDR and non-MDR, ESBL producers and non-ESBL producers, females’ and males’ isolates, and isolates which harbored each of the tested bla genes is showed in Table 2.
Comparatively, antimicrobial resistance against cephalexin (p=0.03), ceftriaxone (p=0.03), ciprofloxacin (p=0.007), levofloxacin (p=0.009), trimethoprim-sulfamethoxazole (p=0.04), and tetracycline (p=0.006) was more prevalent in MDR isolates than non-MDR isolates. However, for resistance against other tested antibiotics, no significant differences were seen in these two groups of isolates (p>0.05) (Table 2).
Antimicrobial resistance against the tested cephalosporins (p<0.001), Fluoroquinolones (p<0.05), trimethoprim-sulfamethoxazole (p=0.02), and tetracycline (p=0.04) was higher in ESBL-producer isolates than non-ESBL producers, but for the tested penicillins, aminoglycosides, and nitrofurantoin, the prevalence of resistance was not significantly different in these two groups of isolates (p>0.05) (Table 2).
Furthermore, the frequencies of antimicrobial resistance against cefotaxime (p=0.04), gentamicin (p=0.003), levofloxacin (p=0.04), and tetracycline (p=0.03) were higher in males’ isolates than females’; however, resistance to other tested antibiotics was not significantly different in females’ and males’ isolates (Table 2).
Statistical analysis showed significant correlations between resistance to ciprofloxacin (p=0.01), levofloxacin (p=0.02), trimethoprim-sulfamethoxazole (p=0.007), and all the tested cephalosporins (p<0.001) and presence of the blaCTX-M gene in the UPEC isolates. The presence of the blaSHV gene also contributed to the high prevalence of resistance to cefotaxime (p=0.04). But resistance to nitrofurantoin was more prevalent in isolates which did not harbor the blaSHV gene (p=0.02). No significant association was found between resistance to the tested antibiotics and the presence of the blaTEM gene (p>0.05) (Table 2).
The resistance score ranges, means, and medians in different groups of UPEC isolates are demonstrated in Table 3. The resistance score in ESBL producers (p<0.001), MDR isolates (p=0.003), males’ isolates (p=0.002), and isolates which harbored the blaCTX-M gene (p<0.001) were significantly higher than in other comparable isolates (Table 3).
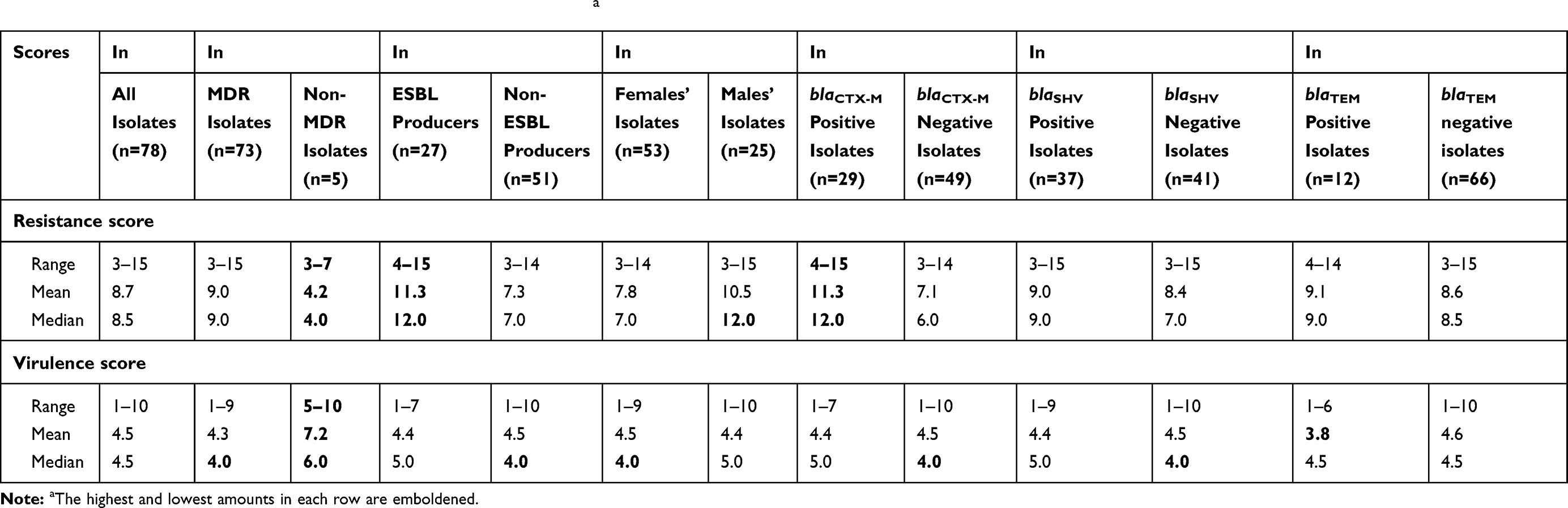 |
Table 3 Resistance and Virulence Scores Among the UPEC Isolatesa |
Detection of Virulence Factor
Among the 11 examined VFs, the highest prevalence was detected for csgA (82.1%), fimH (73.1%), and sitA (73.1%) genes, respectively. The prevalence of other VFs in the UPEC isolates was below 50%. The afa and ibeA genes with 14.1% frequency had the lowest prevalence (Table 4).
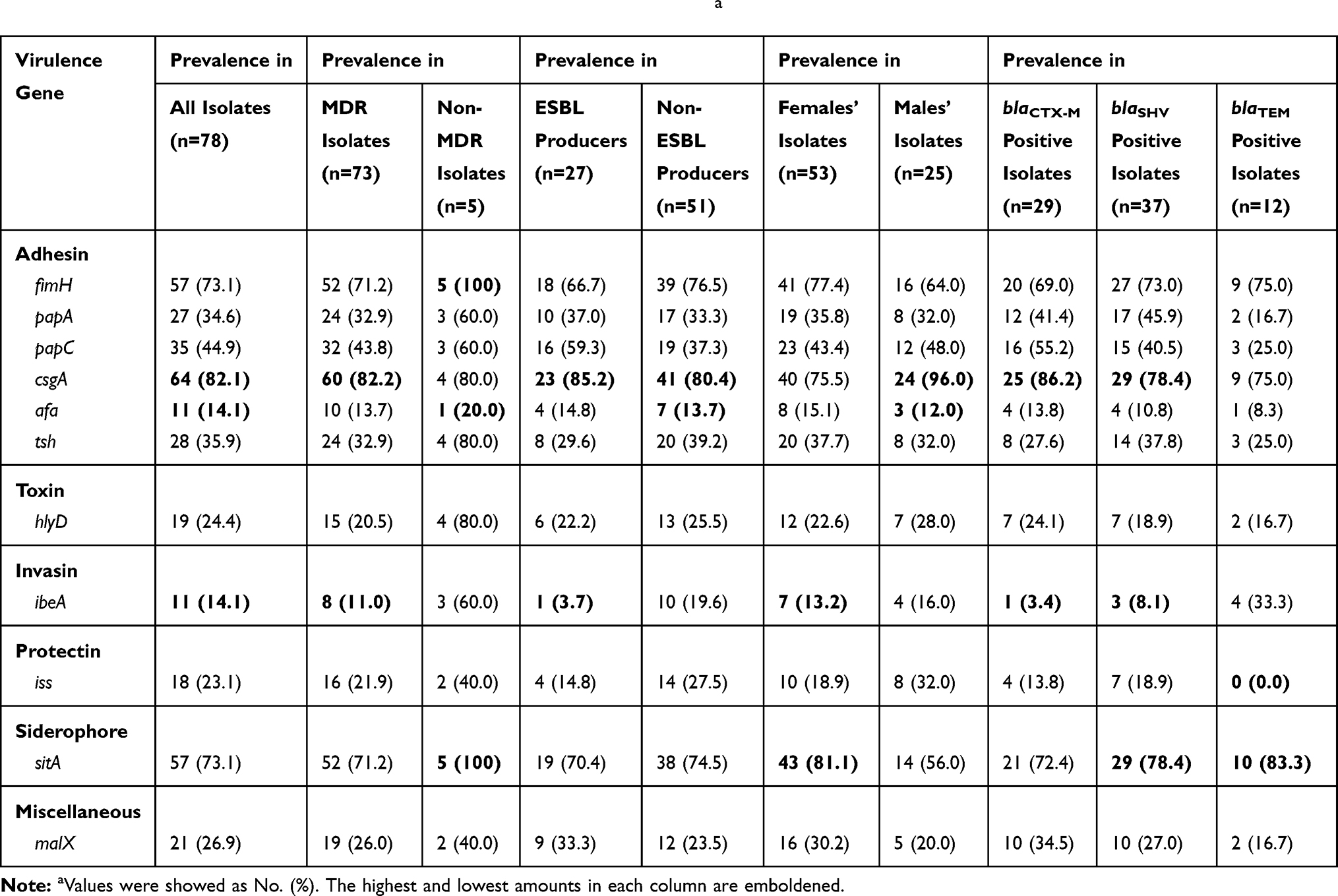 |
Table 4 Prevalence of the Virulence Genes Among the UPEC Isolatesa |
One (1.3%) of the UPEC isolates harbored 10 out of the 11 tested VFs and only lacked the papA gene. Of the UPEC isolates, 23/78 (29.5%) harbored at least half (≥6) of the tested VFs. All isolates harbored at least one of the tested VFs; three isolates only had csgA, two isolates only had fimH, and one isolate only had the sitA gene.
Prevalences of the tested VFs in all UPEC isolates, and also separately in MDR and non-MDR, ESBL producers and non-ESBL producers, females’ and males’ isolates, and isolates harboring each of the tested bla genes are showed in Table 4.
In the ESBL producer and non-ESBL producer isolates, the prevalence of none of the tested VFs was significantly different (p>0.05). But fortunately in the MDR UPECs with limited inhibitory options, prevalence of tsh (p=0.05), hlyD (p=0.01) and ibeA (p=0.02) genes were lower than in the non-MDR UPECs. Furthermore, the prevalence of the tested VFs in females’ and males’ UPEC isolates was not significantly different (p>0.05), except for the csgA gene which was more prevalent in males’ isolates (p=0.03), and the sitA gene which was more prevalent in females’ isolates (p=0.02). Also, higher blaSHV gene was found in the isolates which had the papA gene than the isolates which lack this gene (p=0.04). The prevalence of the blaCTX-M gene was higher in isolates which did not have the ibeA gene than the isolates which carried this gene (p=0.04). For other genes, no significant association was found (p>0.05) (Table 4).
A total of 65 virulence patterns were found among the isolates, among which the virulence pattern of “fimH, csgA” that was seen in four UPEC isolates was the predominant pattern.
The virulence score ranges, means, and medians in different groups of UPEC isolates are demonstrated in Table 3. The virulence score in non-MDR isolates was higher than in MDR isolates (p=0.002). But no significant difference was found for the virulence score of ESBL and non-ESBL producers, males’ and females’ isolates, and isolates with or without each of the tested bla genes (p>0.05) (Table 3).
The associations between the antibiotic resistance and presence of the virulence factors and also the associations of the presence of the virulence genes with each other are shown in Supplementary Materials and Tables S1–S4.
Discussion
In the recent decade, there has been universal concern about the management of UTIs caused by E. coli. The worldwide increase in the prevalence of virulent ESBL-producing UPEC which are also MDR has led to increased severity of UTIs, decreased the efficacy of first-line antibiotics, and therefore increased medical costs and the rate of morbidity and mortality. Accurate global estimation of these problems is very difficult, since according to the World Health Organization (WHO) global report on surveillance of antimicrobial resistance there was not enough information about the worldwide extent of the antimicrobial resistance, particularly in developing countries.17 So we conducted the present research to find the effective drug to combat E. coli infections on the basis of the regional rate and pattern of antimicrobial resistance and also to prognose the severity of UTIs by the evaluation of essential VFs in the UPEC isolates.
During the period of sampling, frequencies of UTIs and isolation of E. coli from urine samples of female patients were higher (more than twice) than those of the males, which is in agreement with the previous reports in Iran and other countries.18–21 This may be due to the difference in the anatomical structure of the females’ and males’ genital tract, as comparatively the females’ urethra is shorter and therefore infectious agents (eg, E. coli) can more easily reach the bladder. In addition, the position of the females’ urethral opening near the anus and vagina also plays a role in easier entry of the bacteria from these sites to the urinary tract system.19
ESBL-Producing UPEC
The β-lactam antibiotics were mainly used for the treatment of infections due to E. coli strains, but recently the worldwide increase of the ESBL-producing E. coli is a major concern of clinicians.7 Lee et al22 in 2018 reviewed and reported that the prevalence of ESBL-producing E. coli isolates was increased in UK (from 4.6% to 6.6%), France (from 1.1% to 3.3%), Spain (from 2.4–18.2% to 8.9–23.6%), Italy (from 3.5% to 6.7%), Turkey (from 8.0–13.1% to 24.0%), South Asia (from 21.7% to 33.2%), Far East Asia (from 4.8–7.5% to 7.6–10.7%), Latin America (from 1.7% to 7.1–12.5%), USA and Canada (from 7.4% to 1.8–8.0%) before and after 2010.
In our study, 34.6% of the UPEC isolates were ESBL producers. As a result, it can be said that common β-lactam drugs could not effect at least one-third of these UPECs. In another study23 on E. coli isolates from UTIs in Kerman, Iran, 41% of outpatients had ESBL-positive isolates. A somewhat similar (40%) rate of ESBL producers was reported in UPECs in a study in Pakistan.20 This high prevalence of ESBL-producer E. coli in Iran and other developing countries in contrast with developed countries may be a result of ample use of β-lactam drugs and the absence of a strict policy for consumption and even prescription of the antibiotics in these regions.
Unlike the lower incidence of UTIs in males, the UPEC isolates from male patients were higher ESBL producers than those from females (52% versus 26.4%) (p=0.03). But the differences in the prevalence of blaCTX-M, blaSHV, and blaTEM genes in females’ and males’ isolates were not significant (p>0.05). Similarly, in a study from Spain,24 a significant association was found between UTIs due to ESBL-positive E. coli and male sex. In contrast, in another study in Iran,23 the production of ESBLs in UPEC isolates of different gender was not significantly different.
Since several studies revealed that the ESBL producers also show a high level of resistance to non-β-lactam antibiotics, the global concerns about ESBL-producing E. coli are increasing. As in our study, antimicrobial resistance against the tested cephalosporins (p<0.001), fluoroquinolones (p<0.05), trimethoprim-sulfamethoxazole (p=0.02), and tetracycline (p=0.04) were higher in ESBL-producer isolates than non-ESBL producers. Similarly, in a study by Azap et al25 on UPEC isolates from community-acquired UTIs in Turkey, resistance to ciprofloxacin and trimethoprim-sulfamethoxazole in ESBL producers was higher than in non-ESBL producers (p<0.001). In their study,25 the gentamicin resistance was also higher in ESBL-producer isolates than non-ESBL producers (57% vs 9%) (p<0.001). But in our study, although the rate of gentamicin resistance in ESBL-producers was higher than in non-ESBL producers (25.9% vs 11.8%), this difference is not statistically significant (p>0.05). Additionally, in a study from Spain,26 the prevalence of resistance to ciprofloxacin was 31.5% vs 9.1% in ESBL-producer and non-ESBL-producer E. coli isolated from community-acquired UTIs.
In ESBL-positive isolates, resistance to nitrofurantoin had the lowest prevalence (18.5%). A low nitrofurantoin resistance rate also reported in other studies.19,25 Lee et al22 declared a 90% sensitivity to nitrofurantoin in E. coli isolates from community-acquired UTIs in most countries around the world. Therefore, the European Association of Urology (EAU) and Infectious Diseases Society of America (IDSA) recommended nitrofurantoin as the first-line treatment for UTIs, if the regional prevalence of resistance to this drug is below 20%.22 This drug was also suggested as the first-line treatment option for UTIs in other studies from Iran and other countries.2,19,20,22,27 In the study by Derakhshandeh et al,28 resistance against nitrofurantoin (12.9%) had the lowest frequency compared to the other tested antibiotics. But a comparison of our results with their study, which was conducted in the same area as ours, revealed that from 2012 to the present the rates of resistance to nitrofurantoin have increased in this area. This could be due to a recent increase in the prescription of this antibiotic for the empirical treatment of UTIs in this area.
The rates and order of prevalence of β-lactamase genes were different in various studies from distinct and even similar regions, which could indicate their epidemiological diversity.21,29,30
In the present study, all (100%) of the ESBL producers harbored cefotaximase (blaCTX-M) gene. Confirming this result, all (100%) of the ESBL-producer isolates were resistant to cefotaxime. Likewise, 100% of ESBL producers in a study from Bolivia,27 99.5% of ESBL-positive E. coli in a study from western Saudi Arabia,30 and 98.0% of ESBL-positive UPECs from community-acquired UTIs in the study from Turkey25 were found to harbor the blaCTX-M gene. This revealed that the blaCTX-M type is the most frequent ESBL gene in different regions around the world.
The majority (66.7%) of ESBL-producer E. coli isolates harbored more than one ESBL gene. The combination of blaCTX-M and blaSHV (55.6%) was the most common pattern for β-lactamase genes. A combination of all the three tested ESBL genes was detected in 7.4% of the UPECs. In contrast, in a study from western Saudi Arabia,30 82.5% of E. coli isolates contained more than one ESBL gene; the frequent ESBL gene pattern in ESBL producers was a combination of blaCTX-M and blaTEM (79.1%); and a combination of CTX-M, TEM, and SHV types of β-lactamase genes was detected in only 2.4% of E. coli isolates.
Antimicrobial Resistance
In the present study, the overall rates of antimicrobial resistance were relatively high, as the prevalence of resistance to 11/15 (73.3%) of the tested antibiotics was higher than 50%. Furthermore, all (100%) of the isolates were resistant to penicillin, ampicillin, and amoxicillin, and the lowest prevalence of resistance was seen against aminoglycosides (16.7% to gentamicin, 21.8% to amikacin). These results are consistent with the results of a similar study in Mexico5 which reported that 97.4% of E. coli isolates were resistant to ampicillin, and the lowest rate of resistance was seen against amikacin (14.4%). Also, in a study from western Saudi Arabia,30 the rate of ampicillin resistance in E. coli isolates was 99.5% and the lowest antibiotic resistance was reported against amikacin. So, because of the increase in the prevalence of resistance to the penicillins, these antibiotics are not currently recommended for empiric therapy of UTIs.
Following the resistance to penicillins, most of our UPECs were resistant to trimethoprim-sulfamethoxazole (64.1%), which is a drug of choice for treatment of UTIs. Ali et al20 also reported the high (82%) prevalence of trimethoprim-sulfamethoxazole resistance in UPECs isolated in Pakistan. In a study from Mexico,21 more than 70% of UPECs were resistant to trimethoprim-sulfamethoxazole. In another study in Mexico,5 this prevalence was 66%. Additionally, Sanchez et al31 found a great increase in the rate of resistance to trimethoprim-sulfamethoxazole in urinary E. coli isolates among US outpatients from 2000 to 2010. So, the application of this antibiotic in the treatment of UTIs may become limited.
Since fluoroquinolones are frequently recommended for the treatment of uncomplicated pyelonephritis and complicated UTIs, the resistance of UPECs to these antibiotics is very important. In our study, more than half of the isolates were fluoroquinolone-resistant and all the fluoroquinolone-resistant strains showed MDR phenotype. This was comparable to the results of studies in North America32 and Mexico.21 The increased resistance against fluoroquinolones may be due to the excessive use of these antibiotics which could restrict their recommendation for the treatment of UPEC infections.
In our UPECs, the mean of resistance rates against the tested cephalosporins was above 50%. Relatively similar or different antimicrobial resistance rates have been determined in UPEC isolates from other regions of Iran19,23,33 and also other countries including Pakistan,20 Turkey,25 Mexico,5,21 Saudi Arabia,30 Brazil,34 Mongolia,2 etc.22 Therefore, without the regional and even case by case evaluation of antimicrobial susceptibilities of infecting E. coli should not use the cephalosporins as the empirical drugs for the treatment of UTIs.
Unfortunately, we found a high level (93.6%) of MDR E. coli isolates in this study. This result may be due to easy access to the common antimicrobial drugs without prescription in our region. This serious public health problem could strongly limit the choice of antibiotics for the treatment of UTIs due to E. coli.
A high prevalence of MDR E. coli was also reported in relative studies in China,35 western Saudi Arabia,30 Mexico,5 and Mongolia2 (100%, 100%, 96.9%, and 93.9%, respectively). Due to the rules and prescribing behaviors in different regions, the rate of MDR isolates was varied in different countries. For example, in studies from Turkey,25 Spain,26 Mexico,21 and Pakistan,20 the rates of MDR E. coli were 70.6%, 70%, 63%, and 59%, respectively. However, in a study from the Kerman province of Iran, 55.6% of UPECs from outpatients were reported as MDR isolates.23 In comparison with a previous study28 in the same area as our study (Shiraz, Iran), the MDR rate in UPEC isolates of outpatients with UTIs has increased from 82.3% to 93.6% during 2012 to the present study.
In contrast with the results of the study in Mexico,21 which reported that the UPECs from male patients were associated with the MDR phenotype, in our study the prevalence of MDR in females’ and males’ UPEC isolates was not significantly different (p>0.05). However, the resistance score was higher in males’ isolates than females’ (p=0.002). Differences in the rates of resistance against certain antibiotics in isolates of males and females may be due to differences in the pattern of antibiotic consumption. For example, similar to our study, in the studies in Pakistan20 and Mexico,21 fluoroquinolone-resistant UPECs were significantly more prevalent among male patients than females (p<0.05). That could be because of using fluoroquinolones as a first choice for the treatment of UTIs in men. This may lead to an increase in the UTI treatment failure in male patients.
Virulence Factors
The presence of multiple VFs in the UPECs could indicate the high level of their pathogenicity. Furthermore, the presence of MDR and expression of the beta-lactamase genes in more virulent bacteria also could restrict the practical use of antibiotics for the treatment of their infections.
In agreement with the study36 in Tehran, Iran, all isolates in our study harbored at least one of the tested VFs. However, in other studies from Iran19,33 and also in two studies from Brazil,34,37 41.1%, 43.2%, 10%, and 51% of UPECs had none of the tested VFs, respectively. These results could show a difference in the number and distribution of the VFs among UPEC strains of various geographical regions.36
An essential stage for UTI development is the adhesion of pathogenic E. coli to different parts of the urinary tract system. Thereafter, UPECs can colonize, invade, and replicate within the uroepithelial cells.5 That is why the high frequencies of adhesin-encoding genes were detected in the tested UPEC isolates. The csgA (82.1%) and fimH (73.1%) genes were the most prevalent adhesion genes in our UPEC isolates, followed by papC (44.9%), and afa gene had the lowest prevalence (14.1%) among the adhesin genes. The csgA gene has a main role in biofilm formation and also can function in adhesion processes in human cystitis. The fimH gene, which encodes the type 1 fimbriae, has a role in bacterial survival, induction of inflammation, invasion, and mediating bacterial colonization and biofilm formation in the murine UTI model, but as expressed in both pathogenic and commensal E. coli, their role in the pathology of human UTIs is unclear. P fimbriae and the papC gene have a principal role in the pathophysiology of pyelonephritis due to UPECs, and finally the afa gene is involved in chronic and recurrent UTIs.3,38,39
In a study38 from Brazil, the prevalence of the csgA gene in 31 E. coli isolates from recurrent cystitis was 100%, and those of fimH and papC were 87.1% and 25.8%, respectively. Similarly, in a study from Mexico,21 the afa gene had the lowest distribution (8.2%) among the UPEC isolates and the prevalences of fimH and papC were 73.4% and 40.5%, respectively. Also, in a study from Tunisia,3 afa (20.0%) had the lowest prevalence among the tested adhesion genes and the prevalences of fimH and pap were 60.0% and 28.0%, respectively. In another study from Mexico,5 iha (64.9%) followed by fim (61.3%) and pap (24.7%), were the most frequent adhesion genes in the UPEC isolates. In a study40 from Karaj, Iran, the fimbriae type 1 (fimH; 73.0%) and P fimbriae (pap; 46.0%) were the most prevalent adhesins. The difference in the percentage of individual adhesin genes in various studies may be because of the presence of a variety of adhesins which UPECs can use for binding to the uroepithelial cells.
In addition to adhesion, iron acquisition is critical for the pathogenesis of UPECs. In our isolates subsequent to the csgA gene and equal to the fimH gene, the sitA gene (73.1%) had the highest prevalence among the other tested VFs. This may reveal that the majority of our UPECs could survive in an iron-limited urinary tract system, overcome the host defense mechanism, and develop the UTIs.41 Concerning the other VFs, the ibeA (14.1%) invasion gene had the lowest prevalence among the tested UPECs, which supports the results of the previous study28 in the same area.
Overall, 24.4% of our isolates harbored the hlyD gene, which indicated that these strains could produce α-hemolysin toxin potentially. Hemolysin has roles in the pathogenesis of UPECs, causes inflammation and permanent renal scarring and contributes to the severity and development of cystitis.39 The prevalence of the hemolysin gene in UPEC isolates was 17.6% in a study from Kurdistan, Iran;19 21.2% in a study from Shiraz, Iran;28 47.0% in a study from Karaj, Iran;40 13% in a study from Tunisia,3 and 9.1% in a study from Mexico.21
In previous studies28,33 in the same area as our study (Shiraz, Iran), UPECs which were isolated from UTI outpatients in 2012 harbored lower rates of fimH (34.1%), papA (9.4%), hlyD (21.2%), sitA (15.3%), tsh (27.1%), iss (20.0%), malX (16.5%), and ibeA (9.4%) genes than our UPECs, which could indicate the increase of the VFs in UPEC isolates during this period in this area. Relatively similar or different prevalences of VFs have been determined in UPEC isolates from other regions of Iran19 and also other countries including Tunisia,3 Brazil,34 and Mongolia.2
In agreement with our study, in another study from Iran19 the prevalence of most tested VFs in females’ and males’ UPEC isolates was not significantly different (p>0.05). In contrast, the results of the study from Mexico21 indicated that the females’ isolates had a higher mean of VFs compared to those from males’.
Conclusion
Alarmingly, in the present study more than one-third of the UPECs were ESBL-positive and almost all of the ESBL-producer strains were MDR. These strains are a crucial problem for public health because they can play a role in the dissemination of antimicrobial resistance in the community and cause most of the commonly used antibiotics for treatment of UTIs to become ineffective in the near future in this area. Shockingly, among the 15 common antibiotics, only nitrofurantoin could be recommended as an appropriate drug for the treatment of UTIs due to our ESBL-producer UPECs. Overall, due to differences in the characteristics of E. coli strains from various geographical regions and their alterations over time, regular regional screening of ESBL producers and their virulence properties is necessary for selecting the appropriate antibiotic or designing new therapeutic methods for UTIs, especially in developing countries.
Acknowledgments
This work was supported by Shiraz University [Grant number 96GRD1M344385]. We acknowledge Dr. Mohammad Motamedifar for helping in sample collection and also we thank Nafiseh Karimi, Azar Ghaedi, and Bahare Behzadnia for their contribution to a part of this research.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Mazzulli T. Diagnosis and management of simple and complicated urinary tract infections (UTIs). Can J Urol. 2012;19(1):42–48.
2. Munkhdelger Y, Gunregjav N, Dorjpurev A, et al. Detection of virulence genes, phylogenetic group and antibiotic resistance of uropathogenic Escherichia coli in Mongolia. J Infect Dev Ctries. 2017;11(01):51–57. doi:10.3855/jidc.7903
3. Tarchouna M, Ferjani A, Ben-Selma W, et al. Distribution of uropathogenic virulence genes in Escherichia coli isolated from patients with urinary tract infection. Int J Infect Dis. 2013;17(6):e450–453. doi:10.1016/j.ijid.2013.01.025
4. Baby S, Karnaker VK, Geetha R. Adhesins of uropathogenic Escherichia coli (UPEC). Int J Med Microbiol Trop Dis. 2016;2(1):10–18.
5. Paniagua-Contreras GL, Monroy-Perez E, Rodriguez-Moctezuma JR, et al. Virulence factors, antibiotic resistance phenotypes and O-serogroups of Escherichia coli strains isolated from community-acquired urinary tract infection patients in Mexico. J Microbiol Immunol Infect. 2017;50(4):478–485. doi:10.1016/j.jmii.2015.08.005
6. Frommel U, Lehmann W, Rodiger S, et al. Adhesion of human and animal Escherichia coli strains in association with their virulence-associated genes and phylogenetic origins. Appl Environ Microbiol. 2013;79(19):5814–5829. doi:10.1128/AEM.01384-13
7. Demirel I, Kinnunen A, Önnberg A, et al. Comparison of host response mechanisms evoked by extended spectrum beta lactamase (ESBL)-and non-ESBL-producing uropathogenic E. coli. BMC Microbiol. 2013;13(1):181. doi:10.1186/1471-2180-13-181
8. Derakhshandeh A, Firouzi R, Naziri Z. Phylogenetic group determination of faecal Escherichia coli and comparative analysis among different hosts. IJVR. 2014;15(1):13–17.
9. CLSI. Performance Standards for Antimicrobial Susceptibility Testing CLSI Supplement M100.
10. Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
11. Tabar MM, Mirkalantari S, Amoli RI. Detection of ctx-M gene in ESBL-producing E. coli strains isolated from urinary tract infection in Semnan, Iran. Electron Physician. 2016;8(7):2686–2690. doi:10.19082/2686
12. Brinas L, Zarazaga M, Saenz Y, et al. Beta-lactamases in ampicillin-resistant Escherichia coli isolates from foods, humans, and healthy animals. Antimicrob Agents Chemother. 2002;46(10):3156–3163. doi:10.1128/AAC.46.10.3156-3163.2002
13. Rodriguez-Siek KE, Giddings CW, Doetkott C, et al. Comparison of Escherichia coli isolates implicated in human urinary tract infection and avian colibacillosis. Microbiology. 2005;151(Pt 6):2097–2110. doi:10.1099/mic.0.27499-0
14. Le Bouguenec C, Archambaud M, Labigne A. Rapid and specific detection of the pap, afa, and sfa adhesin-encoding operons in uropathogenic Escherichia coli strains by polymerase chain reaction. J Clin Microbiol. 1992;30(5):1189–1193. doi:10.1128/JCM.30.5.1189-1193.1992
15. Maurer JJ, Brown TP, Steffens WL, et al. The occurrence of ambient temperature-regulated adhesins, curli, and the temperature-sensitive hemagglutinin tsh among avian Escherichia coli. Avian Dis. 1998;42(1):106–118. doi:10.2307/1592582
16. Horne SM, Pfaff-McDonough SJ, Giddings CW, et al. Cloning and sequencing of the iss gene from a virulent avian Escherichia coli. Avian Dis. 2000;44(1):179–184. doi:10.2307/1592522
17. World Health Organization. Antimicrobial resistance: global report on surveillance. 2014. Available from: http://www.who.int/drugresistance/documents/surveillancereport/en.
18. Rezaei-Tavirani M, Ghafourian S, Sayehmiri F, et al. Prevalence of cotrimoxazole resistance uropathogenic bacteria in Iran: a systematic review and meta-analysis. Arch Clin Infect Dis. 2018;13(5):e63256.
19. Derakhshan S, Pourzare M, Roshani D. Distribution of virulence factors according to antibiotic susceptibility among Escherichia coli isolated from urinary tract infection. Indian J Nephrol. 2018;28(3):191–197. doi:10.4103/ijn.IJN_30_17
20. Ali I, Rafaque Z, Ahmed S, et al. Prevalence of multi-drug resistant uropathogenic Escherichia coli in Potohar region of Pakistan. Asian Pac J Trop Biomed. 2016;6(1):60–66. doi:10.1016/j.apjtb.2015.09.022
21. Ramirez-Castillo FY, Moreno-Flores AC, Avelar-Gonzalez FJ, et al. An evaluation of multidrug-resistant Escherichia coli isolates in urinary tract infections from Aguascalientes, Mexico: cross-sectional study. Ann Clin Microbiol Antimicrob. 2018;17(1):34. doi:10.1186/s12941-018-0286-5
22. Lee DS, Lee SJ, Choe HS. Community-acquired urinary tract infection by Escherichia coli in the era of antibiotic resistance. Biomed Res Int. 2018;2018:7656752. doi:10.1155/2018/7656752
23. Hashemizadeh Z, Kalantar-Neyestanaki D, Mansouri S. Clonal relationships, antimicrobial susceptibilities, and molecular characterization of extended-spectrum beta-lactamase-producing Escherichia coli isolates from urinary tract infections and fecal samples in Southeast Iran. Rev Soc Bras Med Trop. 2018;51(1):44–51. doi:10.1590/0037-8682-0080-2017
24. Briongos-Figuero LS, Gomez-Traveso T, Bachiller-Luque P, et al. Epidemiology, risk factors and comorbidity for urinary tract infections caused by extended-spectrum beta-lactamase (ESBL)-producing enterobacteria. Int J Clin Pract. 2012;66(9):891–896. doi:10.1111/j.1742-1241.2012.02991.x
25. Azap OK, Arslan H, Serefhanoglu K, et al. Risk factors for extended-spectrum β-lactamase positivity in uropathogenic Escherichia coli isolated from community-acquired urinary tract infections. Clin Microbiol Infect. 2010;16(2):147–151. doi:10.1111/j.1469-0691.2009.02941.x
26. Calbo E, Romani V, Xercavins M, et al. Risk factors for community-onset urinary tract infections due to Escherichia coli harbouring extended-spectrum β-lactamases. J Antimicrob Chemother. 2006;57(4):780–783. doi:10.1093/jac/dkl035
27. Bartoloni A, Sennati S, Di Maggio T, et al. Antimicrobial susceptibility and emerging resistance determinants (bla CTX-M, rmtB, fosA3) in clinical isolates from urinary tract infections in the Bolivian Chaco. Int J Infect Dis. 2016;43:1–6. doi:10.1016/j.ijid.2015.12.008
28. Derakhshandeh A, Firouzi R, Motamedifar M, et al. Distribution of virulence genes and multiple drug-resistant patterns amongst different phylogenetic groups of uropathogenic Escherichia coli isolated from patients with urinary tract infection. Lett Appl Microbiol. 2015;60(2):148–154. doi:10.1111/lam.12349
29. Rodriguez-Bano J, Navarro MD, Romero L, et al. Epidemiology and clinical features of infections caused by extended-spectrum beta-lactamase-producing Escherichia coli in nonhospitalized patients. J Clin Microbiol. 2004;42(3):1089–1094. doi:10.1128/JCM.42.3.1089-1094.2004
30. Yasir M, Ajlan AM, Shakil S, et al. Molecular characterization, antimicrobial resistance and clinico-bioinformatics approaches to address the problem of extended-spectrum β-lactamase-producing Escherichia coli in western Saudi Arabia. Sci Rep. 2018;8(1):14847. doi:10.1038/s41598-018-33093-8
31. Sanchez GV, Master RN, Karlowsky JA, et al. In vitro antimicrobial resistance of urinary Escherichia coli isolates among U.S. outpatients from 2000 to 2010. Antimicrob Agents Chemother. 2012;56(4):2181–2183. doi:10.1128/AAC.06060-11
32. Karlowsky JA, Hoban DJ, Decorby MR, et al. Fluoroquinolone-resistant urinary isolates of Escherichia coli from outpatients are frequently multidrug resistant: results from the North American Urinary Tract Infection Collaborative Alliance-Quinolone Resistance study. Antimicrob Agents Chemother. 2006;50(6):2251–2254. doi:10.1128/AAC.00123-06
33. Derakhshandeh A, Firouzi R, Motamedifar M, et al. Virulence characteristics and antibiotic resistance patterns among various phylogenetic groups of uropathogenic Escherichia coli isolates. Jpn J Infect Dis. 2015;68(5):428–431. doi:10.7883/yoken.JJID.2014.327
34. Oliveira FA, Paludo KS, Arend LN, et al. Virulence characteristics and antimicrobial susceptibility of uropathogenic Escherichia coli strains. Genet Mol Res. 2011;10(4):4114–4125. doi:10.4238/2011.October.31.5
35. Zhao L, Chen X, Zhu X, et al. Prevalence of virulence factors and antimicrobial resistance of uropathogenic Escherichia coli in Jiangsu province (China). Urology. 2009;74(3):702–707. doi:10.1016/j.urology.2009.01.042
36. Tabasi M, Karam MR, Habibi M, et al. Genotypic characterization of virulence factors in Escherichia coli isolated from patients with acute cystitis, pyelonephritis and asymptomatic bacteriuria. J Clin Diagn Res. 2016;10(12):Dc01–dc7. doi:10.7860/JCDR/2016/21379.9009
37. Santo E, Macedo C, Marin JM. Virulence factors of uropathogenic Escherichia coli from a university hospital in Ribeirao Preto, Sao Paulo, Brazil. Rev Inst Med Trop Sao Paulo. 2006;48(4):185–188. doi:10.1590/S0036-46652006000400002
38. Cordeiro MA, Werle CH, Milanez GP, et al. Curli fimbria: an Escherichia coli adhesin associated with human cystitis. Braz J Microbiol. 2016;47(2):414–416. doi:10.1016/j.bjm.2016.01.024
39. Bien J, Sokolova O, Bozko P. Role of uropathogenic Escherichia coli virulence factors in development of urinary tract infection and kidney damage. Int J Nephrol. 2012;2012:681473. doi:10.1155/2012/681473
40. Jalali HR, Pourbakhsh A, Fallah F, et al. Genotyping of virulence factors of uropathogenic Escherichia coli by PCR. Novel Biomed. 2015;3(4):177–181.
41. Terlizzi ME, Gribaudo G, Maffei ME. UroPathogenic Escherichia coli (UPEC) infections: virulence factors, bladder responses, antibiotic, and non-antibiotic antimicrobial strategies. Front Microbiol. 2017;8:1566. doi:10.3389/fmicb.2017.01566
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.