Back to Journals » Journal of Inflammation Research » Volume 19
Treatment Approaches for Omalizumab-Refractory Chronic Spontaneous Urticaria
Authors Ensina LF ![]() , Ferrer M, Al-Ahmad M, Fomina D, Kocatürk E, Bizjak-Suran M
, Ferrer M, Al-Ahmad M, Fomina D, Kocatürk E, Bizjak-Suran M ![]()
Received 11 March 2026
Accepted for publication 29 May 2026
Published 19 June 2026 Volume 2026:19 554124
DOI https://doi.org/10.2147/JIR.S554124
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Anish R. Maskey
Luis Felipe Ensina,1,2 Marta Ferrer,3 Mona Al-Ahmad,4,5 Daria Fomina,6– 8 Emek Kocatürk,9– 11 Mojca Bizjak-Suran12– 14
1Division of Allergy, Immunology and Rheumatology, Department of Pediatrics, Federal University of São Paulo, São Paulo, Brazil; 2Hospital Sírio-Libanês, São Paulo, Brazil; 3Department of Allergy, Clinica Universidad de Navarra, Pamplona, Spain; 4Department of Microbiology, College of Medicine, Kuwait University, Kuwait City, Kuwait; 5Department of Allergy, Al-Rashed Allergy Center, Ministry of Health, Kuwait City, Kuwait; 6Moscow City Research and Practical Center of Allergy and Immunology, Moscow Clinical Science and Research Center 52, Moscow Healthcare Department, Moscow, Russia; 7Department of Clinical Immunology and Allergy, The First Sechenov State Medical University, Moscow, Russia; 8Department of Pulmonology, Astana Medical University, Astana, Kazakhstan; 9Institute of Allergology, Charité - Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universität Zu Berlin, Berlin, Germany; 10Fraunhofer Institute for Translational Medicine and Pharmacology (ITMP), Immunology and Allergology, Berlin, Germany; 11Department of Dermatology, Bahçeşehir University, Istanbul, Turkey; 12Division of Allergy, University Clinic of Respiratory and Allergic Diseases Golnik, Golnik, Slovenia; 13Faculty of Medicine, University of Ljubljana, Ljubljana, Slovenia; 14Faculty of Medicine, University of Maribor, Maribor, Slovenia
Correspondence: Luis Felipe Ensina, Email [email protected]
Abstract: Chronic spontaneous urticaria (CSU) is a mast cell–driven disease that impairs health-related quality of life. Although omalizumab is a cornerstone treatment for patients uncontrolled with up-dosed second-generation H1-antihistamines, some patients remain partially responsive or refractory. This narrative review summarizes current concepts in defining, predicting, and managing omalizumab-refractory CSU. Response assessment should rely on validated patient-reported outcome measures, particularly the 7-day Urticaria Activity Score (UAS7) and Urticaria Control Test (UCT), to distinguish complete response, partial response, and true non-response, while also helping to identify pseudo-resistance related to poor adherence or misdiagnosis. Emerging biomarker data support an endotype-driven approach: higher total immunoglobulin E (IgE) is generally associated with type I autoallergic CSU and a better response to omalizumab, whereas low total IgE, basopenia, positive basophil histamine release assay (BHRA) or basophil activation test (BAT) results, and other autoimmune markers suggest type IIb autoimmune CSU and a greater likelihood of inadequate anti-IgE response. For patients with persistent disease despite omalizumab, cyclosporine A remains an evidence-based option, while newer targeted therapies, including dupilumab, Bruton’s tyrosine kinase inhibitors, and anti-KIT antibodies, are expanding the treatment landscape. Overall, management of omalizumab-refractory CSU is shifting toward precision medicine that integrates validated outcome measures, biomarker-informed endotyping, comorbidities, access, safety, and patient preferences. However, standardized switching algorithms, comparative effectiveness data, and validated predictive biomarkers are still needed to optimize individualized care.
Keywords: biomarkers, chronic urticaria, omalizumab, patient-reported outcome measures, therapeutics
Introduction
Chronic spontaneous urticaria (CSU) is characterized by the spontaneous development of wheals, angioedema, or both for more than 6 weeks, without a definite eliciting factor.1 The pathophysiology of CSU is multifactorial, involving complex interactions among autoimmune mechanisms, complement activation, coagulation pathways, and inflammatory pathways. Current evidence supports the presence of two principal CSU endotypes, both characterized by mast cell–activating autoantibodies: (1) type I or autoallergic, driven by immunoglobulin E (IgE) autoantibodies against self-antigens and (2) type IIb or autoimmune, mediated by immunoglobulin G (IgG) autoantibodies targeting the high-affinity IgE receptor (FcεRI) or IgE. These mechanisms converge on mast cell activation but differ in therapeutic responsiveness.2 The global point prevalence of CSU is estimated at 0.7%.3 CSU imposes a substantial burden through high treatment costs, healthcare resource use, productivity loss, and impaired health-related quality of life (HR-QoL), including effects on sleep, work, and social activities.4
Omalizumab is a cornerstone treatment for CSU. It binds circulating IgE, reducing its levels and promoting downregulation of FcεRI on mast cells and basophils, thereby increasing their activation threshold and limiting degranulation. This disrupts IgE-mediated mast cell activation and decreases the release of inflammatory mediators. Additionally, IgE–omalizumab complexes may sequester autoantigens and anti-IgE autoantibodies, while binding to membrane IgE on B cells may reduce ongoing IgE production, further attenuating activity along the IgE–FcεRI–mast cell pathway.5 Because omalizumab targets the IgE–FcεRI axis, it is generally more effective in patients with the type I autoallergic endotype of CSU, in which IgE autoantibodies play a central pathogenic role. In contrast, patients with type IIb autoimmune CSU tend to exhibit a slower and often less robust response to anti-IgE therapy.2
Clinical trials demonstrated symptom reduction in 52–66% of patients, while real-world data indicate response rates up to 85%, with 68% achieving complete remission.6,7 Consequently, omalizumab has been the therapy of choice for patients who remain refractory to high-dose second-generation H1-antihistamines (sgH1AH) since 2016.1 However, for patients who do not respond to omalizumab, cyclosporine A (CsA) was, until recently, the only available option supported by sufficient clinical evidence of efficacy, albeit with the risk of significant adverse effects, particularly with long-term use.8
With improved understanding of CSU pathophysiology and the development of new targeted therapies, options for patients with inadequate response to omalizumab are expanding. However, post-omalizumab management remains challenging because definitions of inadequate response, predictive biomarkers, and switching algorithms are not yet standardized. Here, we summarize strategies for assessing omalizumab response and discuss current and emerging options for omalizumab-refractory CSU. The literature was identified through targeted searches of PubMed/MEDLINE and Google Scholar, supplemented by international guidelines, key clinical trials, systematic reviews, and relevant recent reviews. No formal risk-of-bias assessment or meta-analysis was performed.
Definition of Response to Omalizumab
CSU management has undergone a profound transformation, moving away from a reactive, symptom-based approach toward a proactive, goal-oriented strategy focused on complete disease control and normalization of HR-QoL.8 Because CSU is unpredictable, with spontaneous remissions and recurrent lesions, defining response is challenging. Defining response, timing assessment, and distinguishing response speed and depth are essential for precision-based care.9 Most response definitions are based on omalizumab,10 sgH1AH,11 or CsA12 and may not fully apply to newer treatments. Defining response in CSU requires moving from subjective impressions to validated patient-reported outcome measures (PROMs) that capture disease activity, disease control, and HR-QoL impact.13
Time to Evaluate Response
Response assessment should reflect the expected onset of action of each therapy.14 Standardized evaluation windows prevent premature switching. In the case of sgH1AH, the evaluation window for initial response evaluation is 2 to 4 weeks.15,16 If the patient remains symptomatic after this period, the dose can be increased up to four-fold the standard licensed dose. A definitive evaluation of response to high-dose sgH1AH should again occur after 2 to 4 weeks of the up-dosed regimen. Patients who do not achieve a 7-day Urticaria Activity Score (UAS7) ≤6 or an Urticaria Control Test (UCT) score ≥12 after this duration are classified as sgH1AH-refractory and qualify for second-line therapy.17
In the case of omalizumab, a longer evaluative period is required due to its mechanism of action involving the sequestration of free IgE and the subsequent downregulation of FcεRI receptors on mast cells and basophils. Expert consensus suggests the following timeline for response assessment:
- Early assessment (4−6 weeks): This identifies fast responders who achieve early control.17
- Standard evaluation point (12 weeks): Physicians should determine if the patient has achieved a complete, partial, or non-response after the third injection. This is also an appropriate time point to consider a skin biopsy if diagnosis is questioned because of lack of response to omalizumab.17,18
- Extended trial period (24 weeks): For patients who show a partial or slowly improving response, the trial should be extended to at least six months before concluding that the drug is ineffective.6
Fast versus Slow Response
Fast responders constitute approximately 70% of patients responding to omalizumab. These patients improve within days to 1−4 weeks after the first injection.17 Slow or late responders do not demonstrate significant improvement until 12−14 weeks. Although low IgE levels are associated with reduced response to omalizumab, a considerable proportion of patients with severe CSU and low IgE levels may still show a rapid response, indicating that IgE levels alone are not definitive predictors of treatment outcome.19 Therefore, response speed alone should not be used to define a CSU phenotype. One possible explanation for the rapid response observed in some patients with type IIb CSU20 is that omalizumab may detach IgE and inhibit downstream signaling pathways.
Non-Response versus Partial Response
Complete control of CSU is defined as the absence of signs and symptoms while the patient remains on treatment. Good control corresponds to low disease activity with minimal impairment in HR-QoL, whereas partial control reflects persistent active disease with a relevant impact on HR-QoL. Absence of control is assumed when criteria for complete, good, or partial control are not fulfilled, indicating the need for treatment adjustment. These response categories should be determined using validated PROMs.14
Patient-Reported Outcome Measures (PROMs)
Validated PROMs are increasingly emphasized because they provide standardized assessment in both clinical trials and routine practice.1,21 Their use at each visit is recommended.1,22 PROMs support timely treatment transitions, particularly for non-responders.
Disease Activity Instruments
The Urticaria Activity Score (UAS) is the gold standard for assessing daily disease activity and is recorded once daily. It captures the number of wheals and pruritus intensity, each scored from 0 to 3, resulting in a maximum daily score of 6. The UAS7 represents the sum of daily scores over 7 consecutive days, resulting in a total score of 0 to 42.1,21,23 UAS7 values of ≤6 are generally considered to reflect minimal disease activity, whereas scores of ≥16 and ≥28 are indicative of moderate and severe disease activity, respectively.24 The UAS requires a high level of patient compliance and does not capture angioedema. The Angioedema Activity Score (AAS) consists of five daily questions, each scored from 0 to 3, with a maximum daily score of 15 and a weekly maximum of 105. The AAS28, a 4-week cumulative score, is used to assess long-term angioedema activity.1,25
Disease Control Instruments
The UCT evaluates disease control in patients who develop wheals, with or without angioedema.1 It is a 4-item retrospective questionnaire that evaluates symptom burden, HR-QoL impact, perceived treatment effectiveness and the patient’s overall perception of disease control over the previous 4 weeks.26 Each item is scored from 0 to 4, with a total score ranging from 0 to 16. A score ≥12 indicates well-controlled urticaria, while a score of 16 reflects complete control.1,27 The UCT helps guide treatment escalation. The Angioedema Control Test (AECT) assesses disease control in patients who experience angioedema, with or without wheals. It is a retrospective questionnaire consisting of 4 questions. A score ≥10 indicates well-controlled angioedema. Two validated versions are available, with recall periods of 4 weeks and 3 months.1,24,28
Health-Related Quality of Life (HR-QoL) Instruments
CSU affects functional capacity (including sleep, work, and social activities) and patients’ emotional and psychological well-being.1,4,29 To assess HR-QoL impairment in CSU, the Chronic Urticaria Quality of Life (CU-Q2oL) and the Angioedema Quality of Life (AE-QoL) questionnaire can be used.1
Defining Omalizumab Non-Response Using PROMs
In clinical practice and trials, patients are generally considered treatment non-responders if they fail to achieve meaningful improvement in disease activity or control, reflected by persistent UAS7 ≥16 and/or UCT <12. Complete response is usually defined as UAS7 = 0 and UCT = 16.21 In omalizumab-refractory patients, the integration of multiple PROMs is essential for distinguishing non-responders from partial responders. PROMs may also be useful in raising suspicion of pseudo-resistance, for example in cases of poor treatment adherence, misdiagnosis, or psychiatric comorbidities. We summarize criteria for treatment response in Table 1.
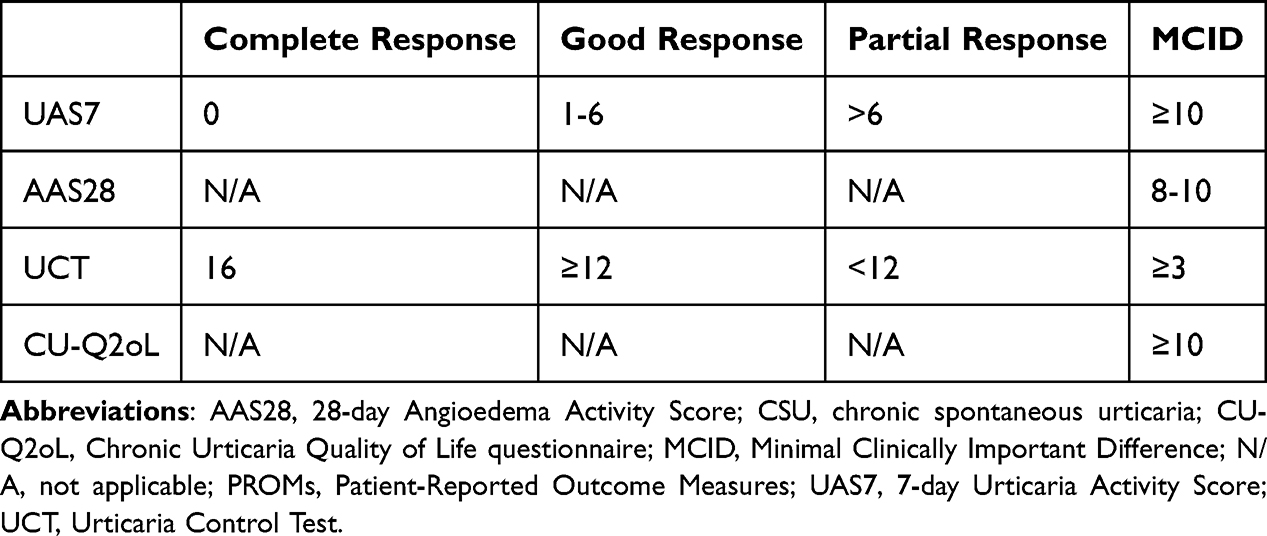 |
Table 1 Validated PROMs for Assessing Disease Activity, Control, and Impact in CSU |
Biomarkers of Response to Omalizumab
In CSU, numerous biomarkers have been investigated to predict response to omalizumab. An ideal biomarker should demonstrate high sensitivity and specificity, reproducibility, feasibility for routine clinical use, and broad validity across patient populations.30 Currently, accessible markers such as total IgE, blood basophil counts, D-dimer, and IgG anti-thyroid peroxidase (anti-TPO) antibodies may support clinical endotyping when interpreted alongside disease activity and comorbidities. Functional basophil assays, cytokine and complement markers, and detailed autoantibody profiling remain largely investigational or restricted to specialized centers. The following sections summarize the main biomarker groups proposed to predict omalizumab response and their clinical limitations.
Total IgE and IgE/FcεRI–Related Markers
Total IgE and FcεRI-related markers are central to CSU biomarker research and may inform endotyping and omalizumab response, although they are insufficient as standalone switching tools.31 Approximately half of patients with CSU have elevated total IgE, but levels vary widely.32 High baseline IgE typically identifies a type I autoallergic endotype characterized by rapid, optimal responses to omalizumab and a higher risk of relapse upon withdrawal, whereas low total IgE frequently signals a type IIb autoimmune profile associated with IgG/IgM autoantibodies, antinuclear antibodies (ANA) or IgG anti-TPO positivity, and significant resistance to both sgH1AH and omalizumab.33 Although recent data suggest that higher IgE levels (often with a predictive cutoff around 60 IU/mL) correlate with better treatment outcomes, the reliability of these markers remains inconsistent across different populations.9,34
Basophil‑Related Biomarkers
Basophil-related biomarkers provide mechanistic insights into CSU endotypes and treatment response.32,35 Basophil counts in the blood typically show an inverse relationship with disease activity, as these cells are recruited from the circulation into active skin lesions during flares.36 Consequently, basopenia is frequently observed in patients with high UAS7 scores and type IIb autoimmune features.37 In clinical practice, low baseline basophil levels often signal a higher risk of sgH1AH resistance and a poor or delayed response to omalizumab, while the normalization of these counts serves as a dynamic indicator of successful symptom control.38
Functional assays such as the Basophil Histamine Release Assay (BHRA) provide insight into the underlying type IIb autoimmune drivers of the disease, with a positive BHRA supporting a type IIb autoimmune endotype.39,40 Patients with this profile often experience more severe, treatment-refractory disease; they tend to respond slower to omalizumab but may show better efficacy with CsA.39–41
The Basophil Activation Test (BAT) further refines endotyping by using flow cytometry to measure the expression of activation markers like CD63 and CD203c.42 Positive BAT results are highly associated with the autoimmune cluster of CSU that is characterized by low IgE, positive IgG anti-TPO, and basopenia, and correlate with a significantly higher risk of omalizumab failure.43 Although tracking dynamic changes in BAT throughout therapy can help monitor treatment response, the need for fresh blood samples and the lack of global standardization currently limits its routine use as a standalone tool for managing refractory cases.44
Coagulation and Systemic Inflammation Markers
The activation of the extrinsic coagulation pathway is a hallmark of CSU pathobiology. Activated eosinophils and monocytes express tissue factor, which triggers thrombin generation; this thrombin then directly amplifies mast-cell degranulation and wheal formation.45 D-dimer, a fibrin degradation product, serves as the primary marker for this process.46 It correlates with UAS7 severity scores and acts as a dynamic indicator of disease activity, typically normalizing when a patient enters remission.47 High baseline D-dimer levels often flag severe, refractory disease and may identify patients who require anticoagulation or alternative biologics due to incomplete omalizumab control.48
Inexpensive, blood-based composite indices capture the imbalance between innate and adaptive immunity during CSU flares. Markers such as the Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR), and the Systemic Immune-Inflammation Index (SII) tend to rise with disease activity and normalize in omalizumab responders.49,50 These indices, particularly a baseline NLR greater than 3, have shown a better ability to predict early treatment response than isolated C-reactive protein (CRP), though they still lack the specificity of more targeted markers like D-dimer in complex multivariate models.50
Complement–eosinophil crosstalk may also contribute.45,51 C5a levels rise during active flares, promoting degranulation independently of the FcεRI receptor, which may explain why some patients do not respond to IgE-targeted therapies.45 Similarly, eosinophil cationic protein (ECP) tracks with disease flares and links to coagulation activation in autoimmune endotypes. However, their clinical utility is limited by a lack of validated cut-offs.51,52
Emerging multi-omics approaches and composite ratios, such as D-dimer/albumin and fibrinogen/albumin ratio, may improve diagnostic accuracy beyond traditional markers in CSU.53 Additionally, molecular signatures such as upregulated STAT3 expression are associated with low-IgE autoimmune profiles.54 However, these promising biomarkers require prospective validation before informing treatment decisions in omalizumab-refractory patients.52–54
Other Autoimmune/Emerging Biomarkers
Additional autoimmune biomarkers may help define CSU endotypes, although they lack prospective validation as guides for switching therapy.41,55 The presence of IgG anti-TPO and ANA serves as a primary indicator of autoimmune CSU.56,57 Present in 15–30% of cases, these markers are typically associated with low total IgE, basopenia, and a diminished response to omalizumab.56 Research suggests that the IgG anti-TPO/total IgE ratio is a particularly strong predictor; a ratio exceeding 0.4–0.6 significantly increases the odds of treatment non-response and post-treatment relapse.57 Similarly, the Autologous Serum Skin Test (ASST) remains a valuable, if subjective, tool for confirming the presence of functional IgG autoantibodies that drive delayed treatment responses.55,56
In contrast, the identification of IgE autoantibodies against self-antigens, such as IL-24, characterizes the type I autoallergic endotype.55 Anti-IL-24 IgE is nearly universal in CSU patients and correlates with disease severity, yet these patients often remain highly responsive to omalizumab.58 Distinguishing between these IgE autoantibodies and IgG-driven autoimmunity is essential, as high IgE levels often predict the rapid, complete responders, while the absence of these markers combined with positive classical autoimmune signals points toward more refractory disease.35,56
Limitations of Current Evidence and Unmet Needs
Biomarker evidence in CSU remains limited by methodological and translational challenges. Most studies are small, retrospective, and single-center, with inconsistent definitions of treatment response, variable UAS7 thresholds, and different follow-up timepoints.59 Additionally, heterogeneous omalizumab treatment regimens further complicate comparisons across studies and populations.
Technical barriers also hinder reproducibility. Assays for critical signals like D-dimer, BAT, and IgE are not standardized across laboratories, leading to inter-laboratory variability that can exceed 30%.60 Functional tests, such as the BHRA or BAT, remain largely confined to specialized research centers because they require fresh blood and high-level operator expertise.61 Furthermore, while dynamic markers such as the decline of D-dimer or the normalization of basophil counts during treatment show stronger predictive signals than baseline snapshots,48,62 they require longitudinal sampling that is rarely performed in standard real-world care.
CSU heterogeneity limits predictive performance. While markers can partially distinguish between the type I autoallergic and type IIb autoimmune CSU, over 40% of patients exhibit mixed features.63,64 This overlap results in area under the curve (AUC) values of 0.65–0.75, which are insufficient for a clinician to rely on as a sole decision-making tool.65 Even composite indices (combining markers like the IgG anti-TPO/IgE ratio with basophil counts) modestly improve accuracy but fail to reliably predict a patient’s specific need for dose escalation or their likelihood of responding to alternative treatments.9,40 Validated algorithms and feasible biomarker panels are needed. The future of CSU management lies in prospective randomized controlled trials that stratify refractory patients by their biomarker profiles. Table 2 summarizes key biomarker profiles associated with distinct CSU endotypes and outlines potential therapeutic considerations.
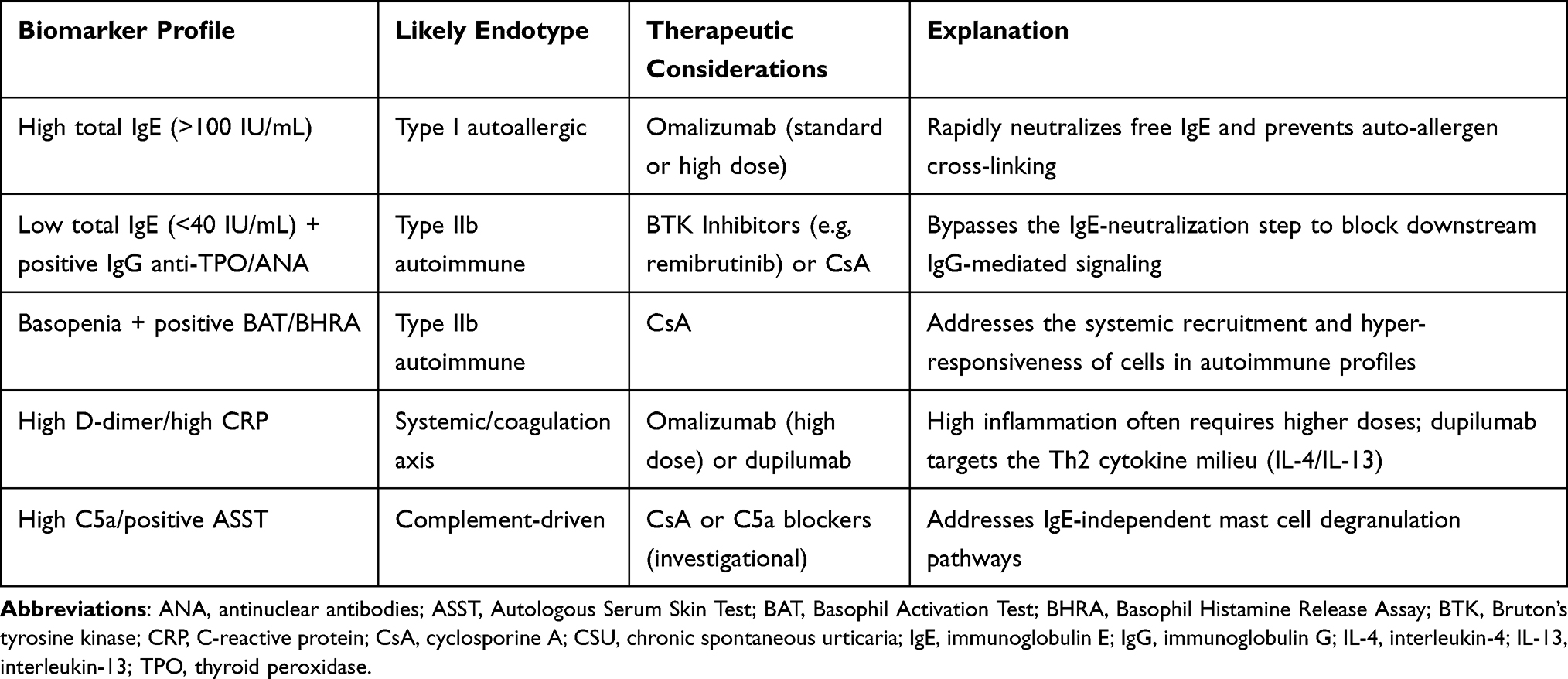 |
Table 2 Biomarker-Guided Endotyping and Therapeutic Selection in Omalizumab-Refractory CSU |
Management of Omalizumab-Refractory CSU: Current and Emerging Therapies
Although omalizumab is effective for many patients with CSU, a significant subset remains partially responsive or refractory, as defined by persistent activity on validated PROMs. The integration of tools such as UAS7, UCT, and emerging biomarkers has improved identification of true non-responders and highlighted disease heterogeneity beyond the IgE–FcεRI axis. This has driven interest in therapies targeting alternative pathogenic pathways, including type 2–mediated inflammation, autoantibody-driven mechanisms, and intracellular signaling cascades. These agents may provide more personalized options after omalizumab failure. Figure 1 summarizes a practical treatment algorithm for patients with CSU uncontrolled despite up-dosed sgH1AH. Post-omalizumab treatment selection should consider clinical profile, comorbidities, safety, access, and patient preferences. CsA remains an established option but requires monitoring. Dupilumab may be favored in patients with type 2 comorbidities, whereas remibrutinib offers a rapid oral option, and anti-KIT therapy, particularly barzolvolimab, remains investigational.
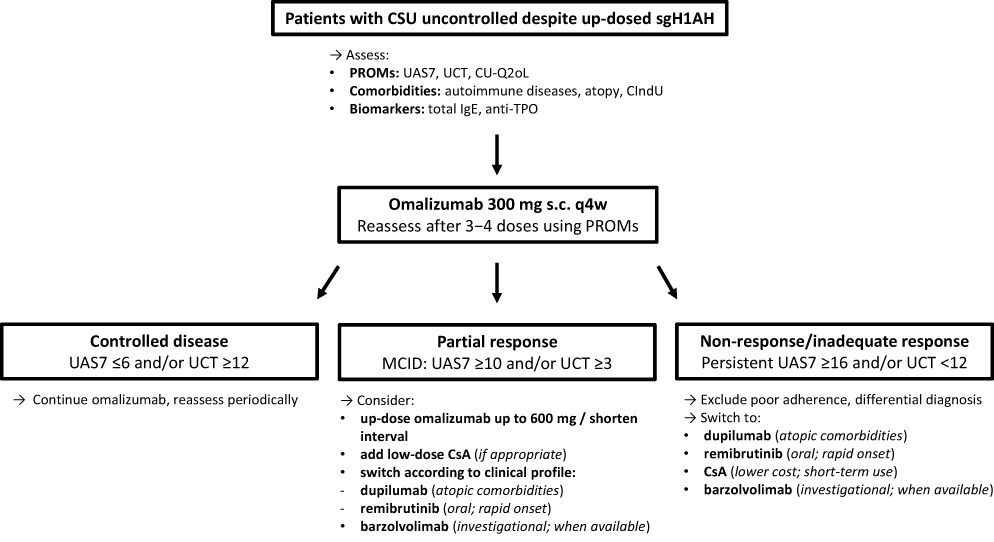 |
Figure 1 Proposed practical treatment algorithm for patients with CSU uncontrolled despite up-dosed sgH1AH. Baseline assessment includes PROMs, comorbidities, and selected biomarkers. After omalizumab 300 mg s.c. q4w, response is reassessed after 3–4 doses using PROMs to guide continuation, optimization, or switching of therapy. Abbreviations: CsA, cyclosporine A; CSU, chronic spontaneous urticaria; CU-Q2oL, Chronic Urticaria Quality of Life Questionnaire; CIndU, chronic inducible urticaria; MCID, Minimal Clinically Important Difference; PROMs, Patient-Reported Outcome Measures; q4w, every 4 weeks; s.c., subcutaneous; sgH1AH, second-generation H1-antihistamines; anti-TPO, IgG anti-thyroid peroxidase; UAS7, 7-day Urticaria Activity Score; UCT, Urticaria Control Test. |
Dupilumab: Targeting Type 2 Inflammation in CSU
CSU exhibits a type 2 helper T-cell (Th2)-skewed immune profile within its perivascular dermal infiltrate, characterized by increased expression of cytokines such as interleukin (IL)-4, IL-5, IL-13, IL-31, and IL-33. These mediators promote IgE class switching, upregulate FcεRI expression on mast cells and basophils, enhance eosinophil recruitment and survival, and contribute to pruritus and vascular inflammation. Their increased expression in lesional skin supports a localized type 2 milieu that may amplify wheal formation.66
Dupilumab is a fully human IgG4 monoclonal antibody that binds to the interleukin-4 receptor alpha (IL-4Rα) subunit, a shared component of the IL-4 and IL-13 receptor complexes expressed on multiple immune cells, including T and B lymphocytes. By blocking IL-4Rα–mediated signaling, dupilumab inhibits the biological activity of both IL-4 and IL-13, two key cytokines driving the Th2 inflammatory response.2
In the Phase 3 LIBERTY-CSU CUPID A and C studies, dupilumab significantly improved disease control in omalizumab-naïve patients with CSU uncontrolled by sgH1AH. At week 24 in the pooled population, well-controlled CSU (UAS7 ≤6) was achieved by 43.1% of patients treated with dupilumab compared with 23.4% in the placebo group, and complete control occurred in 30.6% versus 15.9%, respectively; additionally, UCT scores increased significantly, supporting improved overall disease control. In Study A, the sustained efficacy of dupilumab was maintained throughout the off-treatment follow-up period to week 36, indicating persistence of clinical benefit beyond the 24-week treatment phase.67,68
Dupilumab responses were observed regardless of baseline total IgE levels, with consistent improvements in urticaria activity in patients with IgE concentrations both below and above predefined cutoffs (eg, 40 IU/mL and 60 IU/mL). Additionally, treatment efficacy was comparable irrespective of the presence of common atopic comorbidities, indicating that dupilumab’s therapeutic benefit in CSU is not restricted to patients with elevated IgE or an atopic background.69 Improvement in HR-QoL was also demonstrated, with reductions versus placebo in CU-Q2oL (−8.6) scores by week 24. More dupilumab-treated patients reported “no or little” impact of CSU on daily activities.67
Across CUPID studies, the safety findings aligned with the established dupilumab safety profile, with treatment-emergent adverse events occurring at comparable rates between dupilumab and placebo (53.5% vs 55.9%). Serious adverse events were infrequent (4.9% vs 4.1%), and discontinuations due to adverse events were uncommon and numerically less frequent with dupilumab than with placebo.69
In the phase 3 CUPID B trial that investigated patients with CSU who were refractory to 3 months of omalizumab therapy, a nominally significant reduction in UAS7 from baseline compared with placebo (−14.4 vs −8.5; P =0.0390) was observed at week 24. However, the primary endpoint was not achieved as no statistically significant differences were observed between groups in Itch Severity Score over 7 days (ISS7).70
Dupilumab has recently received approval for the treatment of CSU in several countries, where it is indicated for patients aged 2 years and older. Following approval and updated guideline recommendations, real-world evidence is expected from observational studies and registries.1,71
Zhu et al reported that 33 patients with CSU were treated with omalizumab, of whom 30.3% were non-responders. Among these omalizumab-refractory patients, 7 required additional therapy after also failing CsA and were subsequently treated with dupilumab; all 7 (100%) achieved complete response (UAS7 = 0) within 1–6 months. These findings suggest that dupilumab may represent an effective alternative for patients with CSU refractory to omalizumab.72
BTK Inhibitors: Blocking Mast Cell and Basophil Activation
Bruton’s tyrosine kinase (BTK) is a key non-receptor tyrosine kinase involved in FcεRI-mediated activation of mast cells and basophils and in B-cell receptor (BCR) signaling. Dysregulation of these pathways contributes to the development of allergic and autoimmune diseases, including CSU. First, BTK inhibition reduces effector cell activation by blocking FcεRI-dependent signaling in mast cells and basophils, preventing intracellular calcium influx and the subsequent release of inflammatory mediators. Second, it disrupts BCR signaling, leading to decreased production of pathogenic IgG autoantibodies involved in autoimmune forms of CSU.73,74 By modulating mast cells, basophils, and B cells, BTK inhibition may provide rapid symptom control, with clinical data suggesting faster suppression of histamine release and basophil activation compared with IgE-targeting therapies such as omalizumab.75
Second-generation BTK inhibitors (Table 3) offer improved selectivity and tolerability. Remibrutinib is a highly selective, irreversible BTK inhibitor with a short half-life and has demonstrated rapid symptom control and a favorable safety profile in clinical trials involving patients with CSU. Fenebrutinib, a reversible BTK inhibitor with strong selectivity and a moderate half-life, is currently under investigation for autoimmune diseases, including CSU. Similarly, rilzabrutinib, a reversible and orally bioavailable BTK inhibitor, has been evaluated in immune-mediated disorders such as pemphigus and CSU.76–78
 |
Table 3 Comparison of BTK Inhibitors for the Treatment of CSU |
REMIX-1 and REMIX-2 were pivotal phase 3, randomized, double-blind, placebo-controlled trials evaluating the efficacy and safety of remibrutinib in adults with CSU inadequately controlled by sgH1AH.79 Remibrutinib demonstrated significant and clinically meaningful reductions in disease activity compared with placebo at Week 12 in both trials (P < 0.001), with parallel improvements in itch and hives severity scores. Symptom improvement was observed as early as Week 1. At Week 12, approximately half of remibrutinib-treated patients achieved well-controlled disease (UAS7 ≤6), and around 30% achieved complete response (UAS7 = 0). These response rates further increased through Week 52 (UAS7≤6 in 62%), confirming sustained efficacy over long-term treatment. Remibrutinib also improved daily activity interference and sleep impairment. Benefits were consistent across prespecified subgroups, including patients with prior omalizumab exposure and low baseline IgE levels, suggesting robust efficacy across diverse clinical phenotypes.80
Serious adverse events were infrequent, occurring in 3.3% of patients receiving remibrutinib and 2.3% of those receiving placebo. No serious adverse event was reported in more than one patient, and none were considered by investigators to be related to the study treatment. Adverse events occurring more frequently in the remibrutinib group compared with placebo included nasopharyngitis (9.1% vs 4.9%), upper respiratory tract infections (5.7% vs 2.0%), and petechiae (4.0% vs 0.3%). Rates of treatment discontinuation due to adverse events were similar between groups, and no deaths were reported during the study period.79,81 Overall, the REMIX trials support remibrutinib as an effective, rapidly acting, and well-tolerated therapeutic option for patients with sgH1AH-refractory CSU.
Currently, indirect comparisons from network meta-analyses suggest that remibrutinib and omalizumab have comparable efficacy and safety profiles. Notably, remibrutinib demonstrated clinical benefit in patients who had previously not responded to omalizumab, likely due to its distinct mechanism of action targeting BTK. This feature is particularly relevant for patients with autoimmune CSU, a population in which omalizumab may be less effective.82,83
Further research is needed to identify predictors of remibrutinib response, which could improve patient selection and optimize outcomes. Long-term studies are also warranted to assess the durability of response and extended safety profile, providing insight into sustained efficacy and tolerability over prolonged treatment periods.
Anti-KIT Antibodies: Mast Cell Depletion
KIT regulates mast cell development, survival, and activation through its interaction with stem cell factor (SCF). Mast cells maintain high KIT expression throughout their lifespan, and SCF-induced KIT dimerization triggers tyrosine kinase activation and downstream signaling pathways that promote proliferation, maturation, chemotaxis, adhesion, survival, and, at higher levels of stimulation, mediator release.84
Barzolvolimab
Barzolvolimab (CDX-0159) is an IgG1 monoclonal antibody directed against KIT, a receptor tyrosine kinase essential for mast cell development, survival, and activation. By blocking the interaction between KIT and its ligand, SCF, barzolvolimab inhibits downstream signaling pathways critical for mast cell maintenance. KIT inhibition may reduce mast cell numbers and activity, thereby attenuating wheal formation, angioedema, and pruritus.7
In a phase 1b trial of sgH1AH-refractory moderate-to-severe CSU, barzolvolimab demonstrated rapid and sustained clinical efficacy, with symptom improvement observed within 1 week and maintained through Week 24. By Week 12, 71% of barzolvolimab-treated patients achieved well-controlled disease (UAS7 ≤6) and 57% achieved complete response (UAS7 = 0), compared with 30% and 20% in the placebo group, respectively. Overall, 44% of patients had prior biologic exposure, and responses were similar in those with and without previous omalizumab use, including patients who had discontinued omalizumab due to lack of efficacy.85
The most common treatment-emergent adverse event with barzolvolimab was hair color change, occurring in 26% of treated patients; this was mild and reversible, with seven of nine cases resolving by the end of the study. Mild-to-moderate neutropenia occurred in 14% of patients, was not associated with increased infections, and resolved during the study.85
In a Phase 2 trial involving patients with CSU refractory to sgH1AH, barzolvolimab was administered at doses of 75 mg every 4 weeks, 150 mg every 4 weeks, and 300 mg every 8 weeks. At week 12, treatment with the 150 mg and 300 mg regimens resulted in statistically significant reductions in UAS7 compared with placebo.86 In a separate 52-week phase 2 study, barzolvolimab demonstrated a rapid onset of action, with marked improvements in UAS7 observed as early as week 1. At week 52, 87.1% of patients had complete disease control. These responses were sustained over time and were consistent irrespective of previous omalizumab exposure. Notably, both disease activity scores and HR-QoL measures remained improved in 50% of patients for up to 28 weeks following the final dose, suggesting prolonged effects and possible disease modification.87
Briquilimab
Briquilimab is another subcutaneously administered monoclonal antibody targeting KIT that is currently being evaluated in the ongoing BEACON phase 1b/2 study in patients with CSU. Preliminary results show favorable efficacy signals, with substantial mean reductions in UAS7 at week 12 for the 120 mg and 180 mg doses administered every 8 weeks.70
Cyclosporine A (CsA): An Established Third-Line Option in CSU
CsA selectively inhibits calcineurin-dependent T-cell activation and proliferation. It also inhibits primed T-cells, preventing the activation of autoreactive B-cells and subsequent autoantibody production.88 CsA’s anti-inflammatory effects include dose-dependent inhibition of IgE-mediated histamine release from mast cells and basophils, as well as suppression of leukotriene C4 (LTC4) synthesis.89 In patients with CSU, CsA treatment has been shown to significantly reduce serum levels of IL-2R, IL-5, and tumor necrosis factor alpha (TNF-α), correlating with clinical improvement.90
In CSU studies, CsA has been used over a broad dose range, most commonly between 3 and 5 mg/kg/day. Higher doses are often avoided because of dose-related toxicity.91 Evidence from a large systematic review and meta-analysis indicates that meaningful clinical benefit can be achieved with lower dosing strategies. In this analysis, CsA administered at low (2 to <4 mg/kg/day) and moderate (4 to 5 mg/kg/day) doses was effective, with approximately 70% of patients showing significant improvement at low doses.92 On this basis, several authors have proposed initiating therapy at lower doses and, in selected cases, combining CsA with omalizumab to enhance efficacy while minimizing adverse effects.93,94
CsA response is often rapid and increases over time. Pooled data show response rates rising from approximately 50% within the first month to over 70% by 12 weeks, indicating that lack of early improvement does not necessarily predict treatment failure.92 Additional real-world studies have reported even faster symptom relief, with the majority of patients improving within the first 2–4 weeks of therapy.95 Similar findings have been reported in pediatric populations, where CsA at 3 mg/kg/day led to marked reductions in disease activity by one month and complete symptom resolution by two months, with sustained disease control during longer follow-up.96,97 CsA treatment duration varies widely across studies, extending from short courses of a few weeks to continuous therapy over several years.92 In clinical practice, many patients can be successfully treated with limited-duration courses, whereas a smaller subset requires prolonged or repeated therapy.93
Long-term outcomes following CsA withdrawal are generally favorable. Several studies report durable remission in the majority of patients after stopping therapy, with disease-free intervals extending over multiple years.98 Importantly, patients who experience relapse often respond quickly and completely to reintroduction of CsA, supporting the feasibility of retreatment.97,99 However, the likelihood of relapse appears to be influenced by treatment length. Shorter courses are associated with higher relapse rates compared with extended treatment durations, suggesting that maintaining therapy beyond the initial response phase may improve long-term disease control.100 Early relapse with recurrence of baseline disease severity has also been observed shortly after CsA discontinuation in some cohorts.95 Thus, CsA duration should be individualized. Longer initial courses or repeat treatment cycles may be required to minimize relapse and achieve sustained remission.
CsA may cause renal impairment and hypertension, along with gastrointestinal symptoms such as nausea, vomiting, and diarrhea. Neurological complaints including headache, tremor, and paresthesia, as well as flu-like symptoms such as myalgias and fatigue, can occur. Other possible adverse effects include hypertrichosis, gingival hyperplasia, metabolic abnormalities (hypertriglyceridemia, hypomagnesemia, hyperkalemia, and hyperbilirubinemia), and an increased risk of infections. Long-term use is also associated with a higher risk of malignancies, particularly cutaneous cancers and lymphoproliferative disorders.101 However, in CSU studies most adverse events are mild and typically resolved after the dosage is reduced.92
Before starting CsA, patients should be evaluated to exclude infections or tumors, have their blood pressure checked, and review other medications for possible interactions. Baseline laboratory tests should include kidney and liver function, blood counts, electrolytes, uric acid, and lipid levels. During follow-up, patients should be reassessed every two weeks for the first 1–2 months and then monthly, with blood pressure checked at every visit. Laboratory monitoring should follow the same schedule, focusing on renal function, urinalysis, blood counts, and liver enzymes, while lipid levels can be monitored less frequently unless abnormal.101 The optimal timing for CsA discontinuation is unclear. Dose reduction is generally considered after at least three months of complete disease control.102
For CsA, gradual tapering rather than abrupt cessation is generally advised. One proposed approach involves decreasing the daily dose by 1 mg/kg at two-week intervals.103 Alternatively, a structured stepwise regimen has been described, beginning with 3 mg/kg/day for six weeks, followed by sequential reductions to 2 mg/kg/day for three weeks and 1 mg/kg/day for one week before stopping treatment.104 Such tapering strategies aim to preserve remission while reducing the likelihood of relapse.
Evidence from systematic analyses suggests that functional assays indicating autoreactivity—such as positive autologous serum skin tests, BHRA and BAT—are associated with better treatment outcomes.12 In addition, elevated inflammatory markers, including plasma D-dimer and higher circulating levels of cytokines such as IL-2, IL-5, and TNF, alongside low baseline total IgE, have been linked to improved responsiveness to CsA.98,105,106 Supporting these findings, data from a multicenter cohort demonstrated that patients responding to CsA more frequently had increased CRP levels, a positive family history of urticaria, and lower total IgE concentrations compared with non-responders.107
In general, CsA has a solid evidence base supporting its efficacy and acceptable safety profile in CSU patients who are refractory to—or lack access to—omalizumab. Accordingly, it is positioned as a third-line option in the most recent international guideline treatment algorithms, although important concerns remain regarding tolerability and safety in special populations and with long-term use.1
Other Emerging or Alternative Agents
A broad range of therapeutic strategies has been explored to target distinct molecular and cellular pathways involved in the pathophysiology of CSU. However, several approaches have yielded disappointing results. Agents directed against eosinophil-related cytokines (benralizumab and mepolizumab), thymic stromal lymphopoietin (tezepelumab), and Siglec-8 (lirentelimab) did not meet their primary efficacy endpoints in clinical trials. In addition, development of a Mas-related G protein-coupled receptor X2 (MRGPRX2) antagonist was discontinued after a phase 1b study due to concerning preclinical in vivo toxicology findings.70 In contrast, clinical investigations evaluating Janus kinase (JAK) inhibitors are ongoing and may offer a novel therapeutic avenue for patients with CSU, including those who are refractory to omalizumab.70
Future Directions: The 2026 Precision Paradigm
Management of omalizumab-refractory CSU is moving from a one-size-fits-all strategy toward a personalized, endotype-driven approach.2 With the approval of dupilumab and remibrutinib by international agencies and the positive results from barzolvolimab studies, the clinician’s role is now to identify the “dominant driver” early, using biomarkers to identify specific endotypes. These targeted therapies may also advance biomarker development and disease-modifying strategies. The latest version of the international guidelines recommends omalizumab, dupilumab, and remibrutinib as second-line treatment options for patients with CSU refractory to sgH1AH, with the possibility of switching between these agents in cases of inadequate response before proceeding to CsA.1 Ongoing Phase III trials with barzolvolimab are expected to provide important data, likely confirming the efficacy observed in Phase II studies. These developments support maintaining guidelines as a “living” document, as barzolvolimab may soon warrant inclusion among second-line therapeutic options. Real-world practice must identify which patients benefit most from each treatment. More precise initial treatment selection may reduce apparent anti-IgE non-response. Key differences among dupilumab, remibrutinib, and barzolvolimab are summarized in Table 4. Treatment selection should consider:
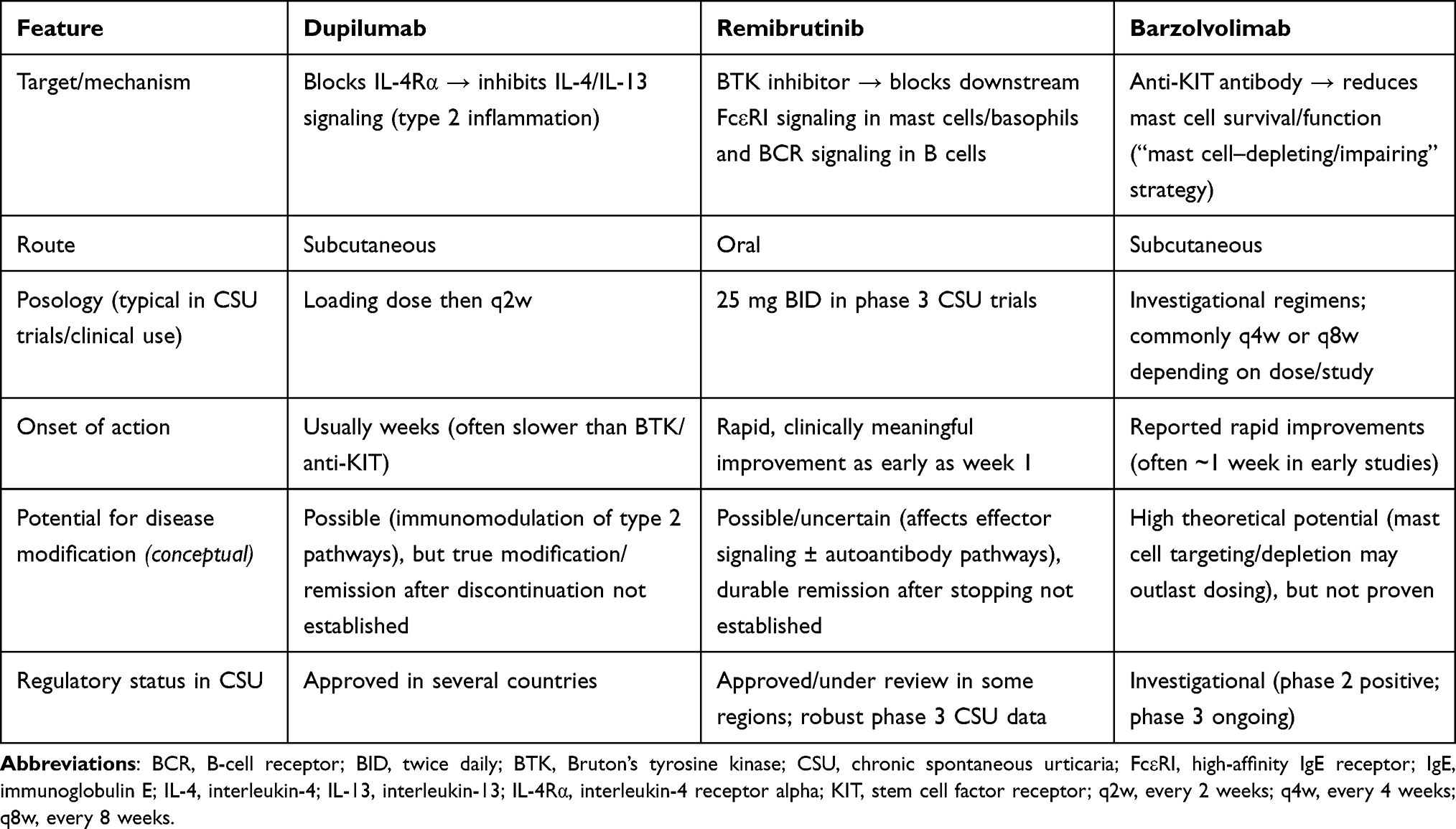 |
Table 4 Comparative Overview of Dupilumab, Remibrutinib, and Barzolvolimab in CSU |
1. Route of administration: Biologics such as omalizumab, dupilumab, and anti-KIT antibodies are administered subcutaneously every 2–8 weeks. In contrast, remibrutinib is orally administered on a daily basis, but requires consistent adherence.
2. Onset of action: Remibrutinib provides rapid symptom relief, useful when early control is needed. However, fast responses are also observed in a substantial proportion of patients treated with omalizumab and barzolvolimab, and less frequently with dupilumab. Conversely, patients classified as late responders to omalizumab (after approximately 2–5 months of treatment) may require dose escalation or switching to another second-line agent. Finally, the potential for sustained disease control and possible disease modification should also be considered when selecting a long-term therapeutic strategy.
3. Treatment history and comorbidities: Prior response to therapy and underlying endotype should guide selection. In patients refractory to omalizumab, particularly those with features suggestive of type IIb autoimmune CSU (eg, low IgE, autoimmune markers), anti-KIT therapies and BTK inhibitors may represent rational options. In contrast, patients with a type I autoallergic profile or concomitant atopic diseases (such as asthma, allergic rhinitis, or atopic dermatitis) may particularly benefit from dupilumab. Chronic inducible urticaria (CIndU) and other comorbidities should also be considered.
Conclusion
Although omalizumab remains a highly effective therapy for most patients with CSU, some continue to have inadequate disease control. In these patients, true refractoriness should be confirmed using validated PROMs, assessment of adherence and dosing, and reconsideration of differential diagnoses or CIndU. Post-omalizumab treatment should then be individualized according to response pattern, endotype features, comorbidities, safety, access, route of administration, and patient preference. CsA remains an established option, while dupilumab, BTK inhibitors, and anti-KIT antibodies offer mechanistically distinct alternatives. However, validated predictive biomarkers, comparative effectiveness data, long-term safety evidence, and standardized switching algorithms are still needed to support precision-based care.
Data Sharing Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Author Contributions
L. F. Ensina: Conceptualization; Literature search and interpretation; Writing - original draft; Writing - review and editing. M. Ferrer: Conceptualization; Literature search and interpretation; Writing - original draft; Writing - review and editing. M. Al-Ahmad: Conceptualization; Literature search and interpretation; Writing - original draft; Writing - review and editing. D. Fomina: Conceptualization; Literature search and interpretation; Writing - original draft; Writing - review and editing. E. Kocatürk: Conceptualization; Literature search and interpretation; Writing - original draft; Writing - review and editing. M. Bizjak-Suran: Conceptualization; Literature search and interpretation; Writing - original draft; Writing - review and editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this study.
Disclosure
Dr. Luis Felipe Ensina has served as a speaker for Novartis, Sanofi, Celldex, and AbbVie, and as an advisor for Lilly, and reports personal fees from Novartis, Sanofi, Celldex, AbbVie, and Lilly, outside the submitted work.
Prof. Dr. Emek Kocatürk reports personal fees from Novartis, Sanofi, Menarini, during the conduct of the study.Dr. Marta Ferrer has received research funding from the Carlos III Health Institute (ISCIII), Novartis, GSK, and Thematic Networks for Cooperative Research Centres, and reports honoraria for advisory board and speaker bureau participation from FAES, Genentech, Menarini, MSD, Novartis, Pfizer, Regeneron, Sanofi, and Uriach. Professor Mojca Bizjak-Suran has served as a speaker and advisor for Novartis and Swixx BioPharma, and reports personal fees from these companies outside the submitted work. All other authors declare that they have no competing interests.
References
1. Zuberbier T, Ansari ZAH, Latiff AHA, et al. The international guideline for the definition, classification, diagnosis and management of urticaria. Allergy. 2026. doi:10.1111/all.70210
2. Zuberbier T, Ensina LF, Giménez-Arnau A, et al. Chronic urticaria: unmet needs, emerging drugs, and new perspectives on personalised treatment. Lancet. 2024;404(10450):393–16. doi:10.1016/s0140-6736(24)00852-3
3. Fricke J, Ávila G, Keller T, et al. Prevalence of chronic urticaria in children and adults across the globe: systematic review with meta-analysis. Allergy. 2020;75(2):423–432. doi:10.1111/all.14037
4. Gonçalo M, Gimenéz-Arnau A, Al-Ahmad M, et al. The global burden of chronic urticaria for the patient and society*. Brit J Dermatol. 2021;184(2):226–236. doi:10.1111/bjd.19561
5. Chang TW, Chen C, Lin CJ, Metz M, Church MK, Maurer M. The potential pharmacologic mechanisms of omalizumab in patients with chronic spontaneous urticaria. J Allergy Clin Immunol. 2015;135(2):337–342. doi:10.1016/j.jaci.2014.04.036
6. Kaplan A, Ferrer M, Bernstein JA, et al. Timing and duration of omalizumab response in patients with chronic idiopathic/spontaneous urticaria. J Allergy Clin Immunol. 2016;137(2):474–481. doi:10.1016/j.jaci.2015.08.023
7. Bernstein JS, Sussman G, Pite H, Bernstein JA. Advancements in novel therapeutics for chronic spontaneous urticaria. J Allergy Clin Immunol Pract. 2025;13(9):2272–2285. doi:10.1016/j.jaip.2025.05.035
8. Zuberbier T, Latiff AHA, Abuzakouk M, et al. The international EAACI/GA2LEN/EuroGuiDerm/APAAACI guideline for the definition, classification, diagnosis, and management of urticaria. Allergy. 2022;77(3):734–766. doi:10.1111/all.15090
9. Fok JS, Kolkhir P, Church MK, Maurer M. Predictors of treatment response in chronic spontaneous urticaria. Allergy. 2021;76(10):2965–2981. doi:10.1111/all.14757
10. Soegiharto R, Aghdam MA, Sørensen JA, et al. Multinational drug survival study of omalizumab in patients with chronic urticaria and potential predictors for discontinuation. JAMA Dermatol. 2024;160(9):927–935. doi:10.1001/jamadermatol.2024.2056
11. Kolkhir P, Church MK, Altrichter S, et al. Eosinopenia, in chronic spontaneous urticaria, is associated with high disease activity, autoimmunity and poor response to treatment. J Allergy Clin Immunol Pract. 2019. doi:10.1016/j.jaip.2019.08.025
12. Kulthanan K, Subchookul C, Hunnangkul S, Chularojanamontri L, Tuchinda P. Factors predicting the response to cyclosporin treatment in patients with chronic spontaneous urticaria: a systematic review. Allergy Asthma Immunol Res. 2019;11(5):736–755. doi:10.4168/aair.2019.11.5.736
13. Katelaris CH, Lima H, Marsland A, Weller K, Shah A, Waserman S. How to measure disease activity, impact, and control in patients with recurrent wheals, angioedema, or both. J Allergy Clin Immunol Pract. 2021;9(6):2151–2157. doi:10.1016/j.jaip.2021.02.026
14. Giménez-Arnau AM, Jáuregui I, Silvestre-Salvador JF, et al. Consensus on the definition of control and remission in chronic urticaria. J Investig Allergy Clin Immunol. 2022;32(4):261–269. doi:10.18176/jiaci.0820
15. Ornek SA, Orcen C, Church MK, Kocaturk E. An evaluation of remission rates with first and second line treatments and indicators of antihistamine refractoriness in chronic urticaria. Int Immunopharmacol. 2022;112:109198. doi:10.1016/j.intimp.2022.109198
16. Guillén-Aguinaga S, Presa IJ, Aguinaga-Ontoso E, Guillén-Grima F, Ferrer M. Updosing nonsedating antihistamines in patients with chronic spontaneous urticaria: a systematic review and meta-analysis. Br J Dermatol. 2016;175(6):1153–1165. doi:10.1111/bjd.14768
17. Ferrer M, Boccon-Gibod I, Gonçalo M, et al. Expert opinion: defining response to omalizumab in patients with chronic spontaneous urticaria. Eur J Dermatol. 2017;27(5):455–463. doi:10.1684/ejd.2017.3085
18. Kaplan AP, Ferrer M. Algorithms in allergy: diagnosis, pathogenesis, and treatment of chronic spontaneous urticaria. Allergy. 2024;79(9):2567–2569. doi:10.1111/all.16113
19. Chuang KW, Hsu CY, Huang SW, Chang HC. Association Between Serum Total IgE Levels and Clinical Response to Omalizumab for Chronic Spontaneous Urticaria: a Systematic Review and Meta-Analysis. J Allergy Clin Immunol Pract. 2023;11(8):2382–2389.e3. doi:10.1016/j.jaip.2023.05.033
20. Serrano-Candelas E, Martinez-Aranguren R, Valero A, et al. Comparable actions of omalizumab on mast cells and basophils. Clin Exp Allergy. 2016;46(1):92–102. doi:10.1111/cea.12668
21. Weller K, Zuberbier T, Maurer M. Clinically relevant outcome measures for assessing disease activity, disease control and quality of life impairment in patients with chronic spontaneous urticaria and recurrent angioedema. Curr Opin Allergy Cl. 2015;15(3):220. doi:10.1097/aci.0000000000000163
22. Neisinger S, Pinto BS, Ramanauskaite A, et al. CRUSE®—An innovative mobile application for patient monitoring and management in chronic spontaneous urticaria. Clin Transl Allergy. 2024;14(1). doi:10.1002/clt2.12328
23. Młynek A, Zalewska-Janowska A, Martus P, Staubach P, Zuberbier T, Maurer M. How to assess disease activity in patients with chronic urticaria? Allergy. 2008;63(6):777–780. doi:10.1111/j.1398-9995.2008.01726.x
24. Weller K, Podder I, Salman A, Gimenez-Arnau AM, Neisinger S, Altrichter S. Clinical evaluation and outcome measures of chronic spontaneous urticaria and chronic inducible urticaria. J Allergy Clin Immunol. 2025;13(9):2229–2241. doi:10.1016/j.jaip.2025.07.008
25. Weller K, Groffik A, Magerl M, et al. Development, validation, and initial results of the Angioedema Activity Score. Allergy. 2013;68(9):1185–1192. doi:10.1111/all.12209
26. Weller K, Groffik A, Church MK, et al. Development and validation of the Urticaria Control Test: a patient-reported outcome instrument for assessing urticaria control. J Allergy Clin Immun. 2014;133(5):1365–1372.e6. doi:10.1016/j.jaci.2013.12.1076
27. Ohanyan T, Schoepke N, Bolukbasi B, et al. Responsiveness and Minimal Important Difference of the Urticaria Control Test (UCT). J Allergy Clin Immunol. 2017;140(6):1710–1713.e11. doi:10.1016/j.jaci.2017.04.050
28. Weller K, Donoso T, Magerl M, et al. Validation of the Angioedema Control Test (AECT) - a patient reported outcome instrument for assessing angioedema control. J Allergy Clin Immunol Pract. 2020;8(6):2050–2057.e4. doi:10.1016/j.jaip.2020.02.038
29. Maurer M, Abuzakouk M, Bérard F, et al. The burden of chronic spontaneous urticaria is substantial: real-world evidence from ASSURE-CSU. Allergy. 2017;72(12):2005–2016. doi:10.1111/all.13209
30. Atkinson AJ, Colburn WA, DeGruttola VG, et al. Biomarkers and surrogate endpoints: preferred definitions and conceptual framework. Clin Pharmacol Ther. 2001;69(3):89–95. doi:10.1067/mcp.2001.113989
31. Altrichter S, Fok JS, Jiao Q, et al. Total IgE as a marker for chronic spontaneous urticaria. Allergy Asthma Immunol Res. 2021;13(2):206–218. doi:10.4168/aair.2021.13.2.206
32. Tbakhi B, Ware K, Park HS, Bernstein JS, Bernstein JA. An overview of chronic spontaneous urticaria: diagnosis, management, and treatment. Allergy Asthma Immunol Res. 2025;17(5):531–546. doi:10.4168/aair.2025.17.5.531
33. Ensina LF, Brandão L, Arruda LK, et al. IgE as a predictor to omalizumab response in patients with chronic spontaneous urticaria. Front Allergy. 2025;5:1451296. doi:10.3389/falgy.2024.1451296
34. Cetinkaya PO, Arslan Z, Dirliktutan B, Karaosmanoglu N. A 10-year real-world analysis of omalizumab use in chronic spontaneous urticaria patients at a dermatology clinic. Méd Bull Sisli Etfal Hosp. 2025;59(2):194–199. doi:10.14744/semb.2025.79059
35. Bracken SJ, Abraham S, MacLeod AS. Autoimmune theories of chronic spontaneous urticaria. Front Immunol. 2019;10:627. doi:10.3389/fimmu.2019.00627
36. Poddighe D, Vangelista L. Effects of omalizumab on basophils: potential biomarkers in asthma and chronic spontaneous urticaria. Cell Immunol. 2020;358:104215. doi:10.1016/j.cellimm.2020.104215
37. Yanase Y, Matsubara D, Takahagi S, Tanaka A, Ozawa K, Hide M. Basophil characteristics as a marker of the pathogenesis of chronic spontaneous urticaria in relation to the coagulation and complement systems. Int J Mol Sci. 2023;24(12):10320. doi:10.3390/ijms241210320
38. Lee HY, Jeon HS, Jang JH, et al. Predicting responses to omalizumab in antihistamine-refractory chronic urticaria: a real-world longitudinal study. J Allergy Clin Immunol. 2024;3(2):100245. doi:10.1016/j.jacig.2024.100245
39. Marcelino J, Baumann K, Skov PS, et al. What basophil testing tells us about CSU patients – results of the CORSA study. Front Immunol. 2021;12:742470. doi:10.3389/fimmu.2021.742470
40. Cain WV, Jandarov RA, Priya M, Rao M, Bernstein JA. Utility of serum biomarkers in real-world practice for predicting response to omalizumab therapy in patients with chronic spontaneous urticaria. J Allergy Clin Immunol. 2025;4(1):100386. doi:10.1016/j.jacig.2024.100386
41. Lang DM, Sheikh J, Joshi S, Bernstein JA. Endotypes, phenotypes, and biomarkers in chronic spontaneous urticaria evolving toward personalized medicine. Ann Allergy Asthma Immunol. 2025;134(4):408–417.e3. doi:10.1016/j.anai.2024.10.026
42. Curto-Barredo L, Yelamos J, Gimeno R, Mojal S, Pujol RM, Giménez-Arnau A. Basophil activation test identifies the patients with chronic spontaneous urticaria suffering the most active disease. Immun, Inflamm Dis. 2016;4(4):441–445. doi:10.1002/iid3.125
43. Pesqué D, Andrades E, Torres-Bosó P, et al. Relevance of the basophil activation test in a cohort of 240 patients with chronic spontaneous urticaria. Clin Exp Dermatol. 2024;50(3):551–557. doi:10.1093/ced/llae441
44. Endo T, Toyoshima S, Hayama K, et al. Relationship between changes in the 7-day urticaria activity score after treatment with omalizumab and the responsiveness of basophils to FcεRI stimulation in patients with chronic spontaneous urticaria. Asia Pac Allergy. 2020;10(2):e12. doi:10.5415/apallergy.2020.10.e12
45. Yanase Y, Takahagi S, Ozawa K, Hide M. The role of coagulation and complement factors for mast cell activation in the pathogenesis of chronic spontaneous urticaria. Cells. 2021;10(7):1759. doi:10.3390/cells10071759
46. Folci M, Heffler E, Canonica GW, Furlan R, Brunetta E. Cutting edge: biomarkers for chronic spontaneous urticaria. J Immunol Res. 2018;2018:1–12. doi:10.1155/2018/5615109
47. Criado RF, Bensi CG, Criado PR, Henriques MT, de Espindola BAR, Filho CDM. Evaluation of serum levels of C-reactive protein, D-dimer and autologous serum skin test in patients with chronic spontaneous urticaria in a Brazilian tertiary center: a cross-sectional study. An Bras Dermatol. 2021;96(2):148–154. doi:10.1016/j.abd.2020.07.006
48. Baskurt D, Sarac E, Asero R, Kocatürk E. D-dimer levels decline after immunosuppressive treatment rather than anticoagulant treatment in severe autoimmune chronic spontaneous urticaria. Eur Ann Allergy Clin Immunol. 2024;56(01):42. doi:10.23822/eurannaci.1764-1489.272
49. Tarkowski B, Ławniczak J, Tomaszewska K, Kurowski M, Zalewska-Janowska A. Chronic urticaria treatment with Omalizumab—verification of NLR, PLR, SIRI and SII as biomarkers and predictors of treatment efficacy. J Clin Med. 2023;12(7):2639. doi:10.3390/jcm12072639
50. Pedersen NH, Sørensen JA, Ghazanfar MN, Zhang DG, Vestergaard C, Thomsen SF. Biomarkers for monitoring treatment response of omalizumab in patients with chronic urticaria. Int J Mol Sci. 2023;24(14):11328. doi:10.3390/ijms241411328
51. Zhou B, Li J, Liu R, Zhu L, Peng C. The role of crosstalk of immune cells in pathogenesis of chronic spontaneous urticaria. Front Immunol. 2022;13:879754. doi:10.3389/fimmu.2022.879754
52. Asero R, Cugno M. Biomarkers of chronic spontaneous urticaria and their clinical implications. Expert Rev Clin Immunol. 2021;17(3):247–254. doi:10.1080/1744666x.2021.1882304
53. Metin Z, Akca HM, Tur K, Akogul S. Intersecting pathways: evaluating inflammatory markers and metabolism in chronic spontaneous urticaria with a multi-marker approach. Int J Dermatol. 2024;63(5):604–610. doi:10.1111/ijd.17147
54. Sauer M, Scheffel J, Frischbutter S, et al. STAT3 gain-of-function is not responsible for low total IgE levels in patients with autoimmune chronic spontaneous urticaria. Front Immunol. 2022;13:902652. doi:10.3389/fimmu.2022.902652
55. Sella JA, Ferriani MPL, Melo JML, et al. Type I and type IIb autoimmune chronic spontaneous urticaria: using common clinical tools for endotyping patients with CSU. J Allergy Clin Immunol. 2023;2(4):100159. doi:10.1016/j.jacig.2023.100159
56. Mateu-Arrom L, Nogueira XAV, Puig L, Spertino J. Predictors of response to omalizumab and relapse in chronic spontaneous urticaria: a narrative review focusing on parameters available in routine clinical practice. Front Allergy. 2025;6:1688464. doi:10.3389/falgy.2025.1688464
57. Golušin Z, Maletin N, Denda N, Nišavić M, Radovanović B, Nikolić O. Autoimmune thyroid diseases in chronic spontaneous urticaria: the role of hormones, anti-thyroid antibodies, and ultrasound. Diagnostics. 2025;15(5):608. doi:10.3390/diagnostics15050608
58. Kaplan A, Lebwohl M, Giménez-Arnau AM, Hide M, Armstrong AW, Maurer M. Chronic spontaneous urticaria: focus on pathophysiology to unlock treatment advances. Allergy. 2022. doi:10.1111/all.15603
59. Güner ME, Öztürk P, Yaray OC, Kılıç EME, Kuş MM. Predictors of early response and relapse in chronic spontaneous urticaria treated with omalizumab: the role of age, sex, disease duration, and UAS7. Dermatol Pr Concept. 2025;15(4):e20256169. doi:10.5826/dpc.1504a6169
60. Selby R, Meijer P, Favaloro EJ. D-dimer diagnostics: can I use any D-dimer assay? Bridging the knowledge-to-action gap. Res Pr Thromb Haemost. 2024;8(1):102335. doi:10.1016/j.rpth.2024.102335
61. Kim T, Yu J, Li H, et al. Validation of inducible basophil biomarkers: time, temperature and transportation. Cytom Part B. 2021;100(6):632–644. doi:10.1002/cyto.b.21991
62. Rijavec M, Košnik M, Koren A, et al. A very low number of circulating basophils is predictive of a poor response to omalizumab in chronic spontaneous urticaria. Allergy. 2021;76(4):1254–1257. doi:10.1111/all.14577
63. Xiang YK, Guloglu S, Elieh-Ali-Komi D, Kocatürk E. Chronic spontaneous urticaria: new evidences on the role of autoimmunity. Curr Opin Allergy Clin Immunol. 2023;23(5):438–445. doi:10.1097/aci.0000000000000927
64. Ridge K, Ahmad R, Moran B, et al. Towards personalised therapy in chronic spontaneous urticaria: advancing from endotype to clinical response. Clin Exp Allergy. 2025;55(11):1070–1082. doi:10.1111/cea.70100
65. Aktaş ÖÖ, Çimşir DÖ, Bülbül EN, et al. Biomarkers of response to omalizumab in patients with chronic spontaneous urticaria. Allergol Immunopathol. 2025;52(4):7–13. doi:10.15586/aei.v53i4.1443
66. Giménez-Arnau AM, DeMontojoye L, Asero R, et al. The pathogenesis of chronic spontaneous urticaria: the role of infiltrating cells. J Allergy Clin Immunol Pract. 2021;9(6):2195–2208. doi:10.1016/j.jaip.2021.03.033
67. Giménez-Arnau AM, Casale TB, Yosipovitch G, et al. Dupilumab improves health-related quality of life in omalizumab-naïve patients with chronic spontaneous urticaria. Dermatol Ther. 2025:1–14. doi:10.1007/s13555-025-01605-w
68. Maurer M, Casale TB, Saini SS, et al. Dupilumab in patients with chronic spontaneous urticaria (LIBERTY-CSU CUPID): two randomized, double-blind, placebo-controlled, phase 3 trials. J Allergy Clin Immunol. 2024;154(1):184–194. doi:10.1016/j.jaci.2024.01.028
69. Casale TB, Saini SS, Ben-Shoshan M, et al. Dupilumab in patients with chronic spontaneous urticaria. JAMA Dermatol. 2026;162(4):350. doi:10.1001/jamadermatol.2025.6023
70. Hsu FI, Bernstein JA, Chhiba KD, Saini SS. Systemic treatments for chronic spontaneous urticaria: anti-IgE and beyond. J Allergy Clin Immunol Pract. 2026;14(2):361–372. doi:10.1016/j.jaip.2025.11.038
71. Weller K, Giménez-Arnau A, Grattan C, et al. The chronic urticaria registry: rationale, methods and initial implementation. J Eur Acad Dermatol Venereol. 2021;35(3):721–729. doi:10.1111/jdv.16947
72. Zhu C, BinJadeed H, Gabrielli S, et al. Prevalence of omalizumab-resistant chronic urticaria and real-world effectiveness of dupilumab in patients with omalizumab-refractory chronic urticaria: a single-centre experience. Clin Exp Dermatol. 2024;49(10):1227–1231. doi:10.1093/ced/llae145
73. Bernstein JA, Maurer M, Saini SS. BTK signaling—a crucial link in the pathophysiology of chronic spontaneous urticaria. J Allergy Clin Immunol. 2024;153(5):1229–1240. doi:10.1016/j.jaci.2023.12.008
74. Mendes-Bastos P, Brasileiro A, Kolkhir P, et al. Bruton’s tyrosine kinase inhibition—An emerging therapeutic strategy in immune-mediated dermatological conditions. Allergy. 2022;77(8):2355–2366. doi:10.1111/all.15261
75. Bondt MD, Renders J, Struyf S, Hellings N. Inhibitors of Bruton’s tyrosine kinase as emerging therapeutic strategy in autoimmune diseases. Autoimmun Rev. 2024;23(5):103532. doi:10.1016/j.autrev.2024.103532
76. Pulz R, Angst D, Cenni B. Next generation Bruton’s tyrosine kinase inhibitors – characterization of in vitro potency and selectivity. Eur J Pharmacol. 2025;1002:177747. doi:10.1016/j.ejphar.2025.177747
77. Burhan M, Ashraf S, Ali A, et al. Safety and efficacy of remibrutinib for chronic spontaneous urticaria: a systematic review and meta-analysis. Int Arch Allergy Immunol. 2025:1–12. doi:10.1159/000548302
78. Jain V, Giménez-Arnau A, Hayama K, et al. Remibrutinib demonstrates favorable safety profile and sustained efficacy in chronic spontaneous urticaria over 52 weeks. J Allergy Clin Immunol. 2024;153(2):479–486.e4. doi:10.1016/j.jaci.2023.10.007
79. Metz M, Giménez-Arnau A, Hide M, et al. Remibrutinib in chronic spontaneous urticaria. N Engl J Med. 2025;392(10):984–994. doi:10.1056/nejmoa2408792
80. Giménez-Arnau AM, Szalewski R, Hide M, et al. Remibrutinib in chronic spontaneous urticaria: 52-week results from two phase 3 studies. J Allergy Clin Immunol. 2026;157(1):143–154. doi:10.1016/j.jaci.2025.09.028
81. Khan AA, Riaz AA, Naseer F, et al. Efficacy, safety, and quality-of-life outcomes of remibrutinib in chronic spontaneous urticaria: a systematic review and meta-analysis. J Allergy Clin Immunol Pract. 2025;13(12):3406–3419. doi:10.1016/j.jaip.2025.09.023
82. Chu AWL, Oykhman P, Chu X, et al. Comparative efficacy and safety of biologics and systemic immunomodulatory treatments for chronic urticaria: systematic review and network meta-analysis. J Allergy Clin Immunol. 2025;156(4):1008–1023. doi:10.1016/j.jaci.2025.06.004
83. Zhao Z, Zheng Y, Song X, et al. Biological and target synthetic treatments for chronic spontaneous urticaria: a systematic review and network meta-analysis. Clin Transl Allergy. 2025;15(5):e70052. doi:10.1002/clt2.70052
84. Tsai M, Valent P, Galli SJ. KIT as a master regulator of the mast cell lineage. J Allergy Clin Immunol. 2022;149(6):1845–1854. doi:10.1016/j.jaci.2022.04.012
85. Maurer M, Metz M, Anderson J, et al. Anti-KIT barzolvolimab for chronic spontaneous urticaria. Allergy. 2025;80(8):2178–2186. doi:10.1111/all.16598
86. Maurer M, Kobielusz-Gembala I, Mitha E, et al. Barzolvolimab significantly decreases chronic spontaneous urticaria disease activity and is well tolerated: top line results from a phase 2 trial. J Allergy Clin Immunol. 2024;153(2):AB366. doi:10.1016/j.jaci.2023.11.873
87. Chaudhry U, Metz M, Anderson J, et al. Prolonged off-treatment efficacy of barzolvolimab in chronic spontaneous urticaria. J Allergy Clin Immunol. 2026;157(2):AB26. doi:10.1016/j.jaci.2025.12.081
88. Lafferty KJ, Paris LL. Cyclosporine A and the regulation of autoimmune disease. J Autoimmun. 1988;1(6):519–532. doi:10.1016/0896-8411(88)90045-5
89. Amon EU. Cyclosporin A inhibits histamine release from human peripheral basophils and human skin mast cells. Agents Actions. 1992;36(Suppl 2):C250–C252. doi:10.1007/bf01997343
90. INALOZ HS, OZTURK S, Akcali C, KIRTAK N, TARAKCIOGLU M. Low-dose and short-term cyclosporine treatment in patients with chronic idiopathic urticaria: a clinical and immunological evaluation. J Dermatol. 2008;35(5):276–282. doi:10.1111/j.1346-8138.2008.00466.x
91. Kocatürk E, Chu DK, Türk M, et al. Management of chronic spontaneous urticaria made practical: what every clinician should know. J Allergy Clin Immunol Pract. 2025;13(9):2252–2269. doi:10.1016/j.jaip.2025.07.021
92. Kulthanan K, Chaweekulrat P, Komoltri C, et al. Cyclosporine for chronic spontaneous urticaria: a meta-analysis and systematic review. J Allergy Clin Immunol Pract. 2018;6(2):586–599. doi:10.1016/j.jaip.2017.07.017
93. Kessel A, Toubi E. Cyclosporine-A in severe chronic urticaria: the option for long-term therapy. Allergy. 2010;65(11):1478–1482. doi:10.1111/j.1398-9995.2010.02419.x
94. Sánchez J, Alvarez L, Cardona R. Cyclosporine and omalizumab together: a new option for chronic refractory urticaria. J Allergy Clin Immunol Pract. 2020;8(6):2101–2103. doi:10.1016/j.jaip.2020.02.012
95. Sehgal S, Agarwal S, Balai M, Meghwal L, Mittal A. Real-world clinical experience with oral cyclosporine in antihistamine refractory cases of chronic spontaneous urticaria. Indian Dermatol Online J. 2024;15(5):887–890. doi:10.4103/idoj.idoj_745_23
96. Parsad D, Janaani P, Bishnoi A, et al. Efficacy and safety of oral cyclosporine in antihistamine refractory chronic urticaria among children and adolescents: a retrospective study. Clin Exp Allergy. 2025;55(9):877–879. doi:10.1111/cea.70069
97. Neverman L, Weinberger M. Treatment of Chronic Urticaria in Children with Antihistamines and Cyclosporine. J Allergy Clin Immunol Pract. 2014;2(4):434–438. doi:10.1016/j.jaip.2014.04.011
98. Santiago L, Ferreira B, Ramos L, Gonçalo M. IgE levels are negatively correlated with clinical response to ciclosporin in chronic spontaneous urticaria. Br J Dermatol. 2019;180(1):199–200. doi:10.1111/bjd.17005
99. Alves F, Calado R, Relvas M, Gomes T, Gonçalo M. Short courses of ciclosporin can induce long remissions in chronic spontaneous urticaria. J Eur Acad Dermatol Venereol. 2022;36(8):e645–e646. doi:10.1111/jdv.18107
100. Vena GA, Cassano N, Colombo D, Peruzzi E, Pigatto P; Group NI 30S. Cyclosporine in chronic idiopathic urticaria: a double-blind, randomized, placebo-controlled trial. J Am Acad Dermatol. 2006;55(4):705–709. doi:10.1016/j.jaad.2006.04.078
101. Kocaturk E, Saini SS, Rubeiz CJ, Bernstein JA. Existing and investigational medications for refractory chronic spontaneous urticaria: safety, adverse effects, and monitoring. J Allergy Clin Immunol Pract. 2022;10(12):3099–3116. doi:10.1016/j.jaip.2022.09.038
102. Türk M, Kocatürk E, Ertaş R, et al. A global perspective on stepping down chronic spontaneous urticaria treatment: results of the urticaria centers of reference and excellence SDown-CSU study. Clin Transl Allergy. 2024;14(2):e12343. doi:10.1002/clt2.12343
103. Terhorst-Molawi D, Fox L, Siebenhaar F, Metz M, Maurer M. Stepping down treatment in chronic spontaneous urticaria: what we know and what we don’t know. Am J Clin Dermatol. 2023;24(3):397–404. doi:10.1007/s40257-023-00761-z
104. Bonilla PAG, Segade JB, Torrijos EG, Brito FF. Urticaria and cyclosporine. Allergy. 2002;57(7):650–651. doi:10.1034/j.1398-9995.2002.23685.x
105. Endo T, Toyoshima S, Kanegae K, et al. Identification of biomarkers for predicting the response to cyclosporine A therapy in patients with chronic spontaneous urticaria. Allergol Int. 2019;68(2):270–273. doi:10.1016/j.alit.2018.09.006
106. Xiang YK, Hu M, Elieh-Ali-Komi D, Salman A, Smola A, Kocatürk E. Biomarkers in chronic spontaneous urticaria: are we ready for its use in clinical practice? Curr Treat Options Allergy. 2025;12(1):15. doi:10.1007/s40521-025-00391-2
107. Kocatürk E, Başkan EB, Küçük ÖS, et al. Omalizumab versus cyclosporin-A for the treatment of chronic spontaneous urticaria: can we define better-responding endotypes? An Bras Dermatol. 2022;97(5):592–600. doi:10.1016/j.abd.2022.03.003
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Insulin Resistance Across Cerebrovascular and Related Disorders: Mechanisms, Measurement, Genetics, and Clinical Implications
Chen K, Nong Y, Liu Y, Ye Z
Neuropsychiatric Disease and Treatment 2026, 22:575306
Published Date: 30 April 2026