Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Translation and Validation of the TANGO Nocturia Screening Tool into Greek
Authors Zachariou A ![]() , Filiponi M, Kaltsas A
, Filiponi M, Kaltsas A ![]() , Dimitriadis F
, Dimitriadis F ![]() , Sapouna V, Giannakis I, Mamoulakis C
, Sapouna V, Giannakis I, Mamoulakis C ![]() , Karagiannis A
, Karagiannis A ![]() , Zikopoulos A, Paschopoulos M, Takenaka A, Sofikitis N
, Zikopoulos A, Paschopoulos M, Takenaka A, Sofikitis N
Received 26 March 2021
Accepted for publication 23 June 2021
Published 20 July 2021 Volume 2021:14 Pages 1883—1891
DOI https://doi.org/10.2147/JMDH.S312393
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Athanasios Zachariou,1,2 Maria Filiponi,2 Aris Kaltsas,1 Fotios Dimitriadis,3 Vagia Sapouna,2 Ioannis Giannakis,1 Charalampos Mamoulakis,4 Andreas Karagiannis,1 Athanasios Zikopoulos,1 Minas Paschopoulos,5 Atsushi Takenaka,6 Nikolaos Sofikitis1
1Urology Department, Ioannina University, Ioannina, Greece; 2Physical Medicine and Rehabilitation Centre EU PRATTEIN, Volos, Greece; 3 1st Urology Department, School of Medicine, Aristotle University, Thessaloniki, Greece; 4Department of Urology, University General Hospital of Heraklion, University of Crete, Medical School, Crete, Greece; 5Department of Obstetrics and Gynaecology, Medical School, University of Ioannina, Ioannina, Greece; 6Urology Department, School of Medicine, Tottori University, Yonago, Japan
Correspondence: Athanasios Zachariou
Urology Department, Ioannina University, 3 Spyridi Street, Volos, 38221, Greece
Tel +306937227778
Fax +302421026932
Email [email protected]
Purpose: The present study aimed to translate the Targeting the individual’s Aetiology of Nocturia to Guide Outcomes Questionnaire (TANGO) into the Greek language to create TANGO-Gr. A relative reliability study in prospective samples of community dwellers and rehabilitation centre residents was undertaken in order to validate the translation. In terms of nocturia severity, these groups were considered to be representative of patients at both ends of the scale, and therefore suitable validation purposes.
Patients and Methods: The prospective descriptive study took place between 07 and 09/2020. Fifty residents in a rehabilitation centre and thirty-seven community dwellers were included in the study. All participants had more than one episode of nocturia per night. They were asked to complete the newly translated TANGO-Gr Questionnaire twice (test–retest procedure). TANGO-Gr includes three possible answers (“yes”, “no”, and “DK/NA”) to facilitate increased validity. The study group evaluated the socio and demographic characteristics, the level of independence and the comprehensive frailty of all participants.
Results: Both groups satisfactorily completed questionnaire responses. The overall Cronbach’s alpha coefficient was 0.753 (community-dwelling people: 0.776; rehabilitation centre residents: 0.531). A test–retest statistical analysis to determine reliability found an overall median Kappa of 0.88 (IQR: 0.79– 0.94) in community dwellers and 0.91 (IQR: 0.84– 1.00) in rehabilitation centre residents, thereby confirming an almost perfect respective agreement.
Conclusion: The validity of the newly translated TANGO-Gr Questionnaire was proven. It should be considered to be a reliable, self-administered screening tool suitable for clinical practice, and therefore invaluable for Greek-speaking people. The study also determined that certain environment-related variables may contribute to nocturia in rehabilitation centre populations, which is a finding which invites further study.
Keywords: nocturia, TANGO Questionnaire, translation, validation, Greek
Introduction
The International Continence Society (ICS) defines nocturia as the number of times urine is passed during the main sleep period. Having woken to pass urine for the first time, each subsequent urination must be followed by sleep or the intention to sleep. Conventionally, the condition is quantified using a bladder diary.1
Nocturia is a multifactorial condition with many possible contributing etiological factors. Physicians have to evaluate numerous issues such as ageing, urological symptoms, psychogenic conditions, neurological diseases, diabetes mellitus, drugs, etc.2 To ensure the best possible care, in addition to prescribing precise treatment for urinary tract issues, urologists should also advise their patients to consult other specialists to make sure comprehensive treatment.
As its name suggests, TANGO (Targeting the individual’s Aetiology of Nocturia to Guide Outcomes) is a recently developed self-administered screening questionnaire which aims to assess the causes of clinically relevant morbidities associated with nocturia.3 A description of TANGO’s content validity, along with its internal consistency and test–retest reliability has been previously described in the literature.4 Three validated translations are already available; Dutch, Turkish and the Arabian Peninsula dialect.5–7 The present study aimed to create a Greek version of TANGO (ie TANGO-Gr) and validate its relative reliability in prospective samples of community dwellers and rehabilitation centre (RC) residents. In terms of nocturia severity, these groups were considered to be representative of patients at both ends of the scale, making them suitable for determining validity. A secondary outcome was to highlight the need for office and outpatient urologists to consult their nocturia patients in a detailed manner in cooperation with other specialist physicians.
Methods
The prospective descriptive study was carried out between July and September 2020 and involved community dwellers and RC residents of Volos (Greece). During this period, there were no specific lockdown measures caused by the COVID pandemic. The local ethics committee of the Physical Medicine and Rehabilitation Centre EU PRATTEIN approved the study, which was conducted in accordance with the Declaration of Helsinki.
The original TANGO Questionnaire includes 22 items assessing four dysfunction domains: cardiovascular and metabolic status, sleep, urinary tract and wellbeing. If the statement is valid, test-takers score the item. In the TANGO-Gr version, we added two additional answers, “false” and “DK/NA” (ie Do not Know/Not Available). The “DK/NA” option increases the validity of “yes” or “no” answers and reduces missing data since only those who are certain will answer “yes” or “no”. Most others will choose the “DK/NA” option instead of leaving the question unanswered.
Translation and Cross-Cultural Adaptation
To translate the English version of the TANGO Questionnaire into the Greek language, we followed the method described by Sperber.8 Five native speakers did the translation, two were continence nurses, two urologists specialized in functional urology, and one was a biochemist. Only words which are easily understood and consistent with original intent were used. A native English speaker fluent in Greek translated the TANGO-Gr version back into English and subsequently reviewed it by comparing it to the English original.
According to Sperber’s method, we evaluated the translated Questionnaire using two measures. These are the comparability of language and similarity of interpretability. Low scores express extremely comparable/similar translated text and therefore suitable for the clinical practice. The TANGO-Gr Questionnaire displayed excellent comparability of language (mean score 1.89) and similarity of interpretability (mean score 1.91).
The translation team tested the Greek version on five people to check for understandability, interpretation and cultural relevance. After further reviews and appropriate modifications, the final Greek version was ready for statistical validation.
Study Participants
Community dwellers and RC patients participating in the study represented a convenience sample. Inclusion criteria were; a) being 40 years of age or older, and b) having one or more nocturia episodes per night. The study group excluded candidates receiving end-of-life care. Those with end-stage renal disease, terminal malignancies (bladder or otherwise), or who had undergone pelvic radiotherapy, were excluded. So too were those with dementia, cognitive impairment or a limited command of Greek as these would impede Questionnaire comprehension and completion. The participants’ socioeconomic and demographic characteristics, including age, gender, medication and nocturia episodes, were reported.
A continence nurse explained the definition of nocturia and evaluated its severity with a single question “During the night, how many times do you have to get up to urinate, on average?”
Use of the Katz Index permitted the measurement of RC residents’ independence in daily life activities.9 A score of six indicates full function, four indicates moderate impairment, and two or less indicates severe functional impairment.9 Only RC residents with a Katz Index score of four or higher were included in the study. In accordance with reliability testing criteria of the original TANGO Questionnaire, the test–retest analysis only included self-reporting, clinically stable participants.3
The study group evaluated participants’ cognition with the Mini-Mental State Examination (MMSE).10 The MMSE is the commonest tool used in the rapid assessment of a variety of cognitive disorders. A total MMSE score of 24 or more was an additional inclusion criterion.
The community dweller group consisted of patients attending a urology primary care setting, and participants were informed about the TANGO-Gr Questionnaire by a continence nurse. An informed consent form was signed by all those taking part in the study. Each received two TANGO-Gr Questionnaires (test and retest) and two prepaid envelopes for the purpose of submission. The Questionnaires were self-administered and completed in the privacy of home to eliminate any influence a clinical setting might have. A week after the first test was taken, all participants received a call to prompt them to complete and submit the retest. The total number of returned tests and retests was sizable enough to enable test–retest statistical analysis. RC participants were screened by a continence nurse and a urologist who evaluated the eligible individuals. All participants gave their written informed consent before a study assistant outlined the details of the Questionnaire. It was then completed in private, with no comprehension difficulties reported. The retest Questionnaire was completed one week later in the same way.
The minimum recommended sample size for a Cohen Kappa agreement test is between 10 to 30 participants.11 Therefore we chose a sample size of more than 30 per group.
Statistical Analysis
Continuous outcome variables were tested using the Mann Whitney U-test. Categorical outcome variables were analyzed using the Fisher’s exact test. The internal consistency was analyzed by Cronbach’s alpha coefficient and item analysis. TANGO-Gr data were recoded into the binary category of the original TANGO Questionnaire to determine Cohen Kappa statistics. In this analysis, a “DK/NA” answer was considered a missing value. There was no estimation or replacement of missing data points. When the variables under analysis had missing data, pairwise deletion was undertaken. Providing that the missing data is not in excess of 20%, pairwise deletion is a suitable technique if the missing data are completely at random.12 Descriptive statistics for continuous data are presented as a mean (standard deviation [SD]) or median (interquartile range [IQR]), as appropriate. Rates were expressed as number of patients (%). IBM SPSS Statistics for Windows, v.26.0 (IBM Corp. Released 2019. Armonk, NY: IBM Corp) was used for data analysis. A two-tailed p ≤ 0.050 was considered significant.
Psychometric Evaluation
Evaluation of the Translation and Adjustment of Response Categories
Based on the assumption that a large amount of missing data for any given TANGO-Gr Questionnaire item indicates a translation problem, both the determination of missing values and the frequency distribution of all answer choices are necessary factors of the evaluation process. Moreover, the examination of frequency distribution determined if all answers were used, suggesting that the additional choices “DK/NA” and “false” have inherent value. Generally, a symmetrical response distribution and substantial variability indicate high levels of validity. However, because of the widespread presence of morbidity, symmetrical distribution was not expected.13 Another evaluation factor concerns any comprehension and/or interpretation difficulties faced by RC residents, spontaneously reported during or immediately after taking the TANGO Questionnaire. A final evaluation factor involves any Cohen Kappa statistical correlation between participant medications and TANGO-Gr items about diabetes, diuretic and hypertensive drugs. On a scale ranging from −1 to +1, the Cohen Kappa coefficients delineating strength of correlation are as follows: < 0: poor; 0–0.20: slight; 0.21–0.40: fair; 0.41–0.60: moderate; 0.61–0.80: substantial; 0.81–1: almost perfect.14
Test–Retest Reliability
The purpose of the test–retest procedure is to determine the similarity between results of the same test taken on two separate occasions. It presupposes that a high level of similarity indicates a correspondingly high level of validity. We undertook a Cohen Kappa statistical analysis between participant responses of the first TANGO-Gr test and the re-test administered one week later. Cohen Kappa statistics measure the degree of correlation between the two tests, excluding any correlation based on chance. The proportion of concordance (Po), prevalence index (PI), bias index (BI), prevalence-adjusted bias-adjusted Kappa (PABAK), maximum attainable Kappa (Kappamax) and pooled Kappa (Kappa pooled) were also calculated so as to derive an appropriate interpretation of results. Kappa pooled is used to summarize inter-rater agreement across many items. Kappa values of ≥ 0.4 were considered acceptable.4,15 More detailed information about the way of Po, PI, BI, PABAK, Kappamax and Kappapooled computation and about the interpretation of Kappa statistic can be sought by interested readers elsewhere.15–18
Results
Participant Characteristics
Fifty-four community dwellers were recruited for the study, and 41 accepted to fill in the TANGO-Gr questionnaire (response rate 75.9%). Four people refused to fill the retest one week later and excluded from the study (total response rate 68.5%). Sixty-six RC patients were recruited, and 55 accepted to fill in the translated questionnaire (response rate 83.3%). Five people refused to fill the retest one week later and excluded from the study (total response rate 75.8%).
RC patients were generally older and thinner, took fewer diuretic drugs and presented with a higher frequency of nocturia compared to community dwellers. Cronbach’s alpha coefficient was 0.727 in the total population of the study (Table 1).
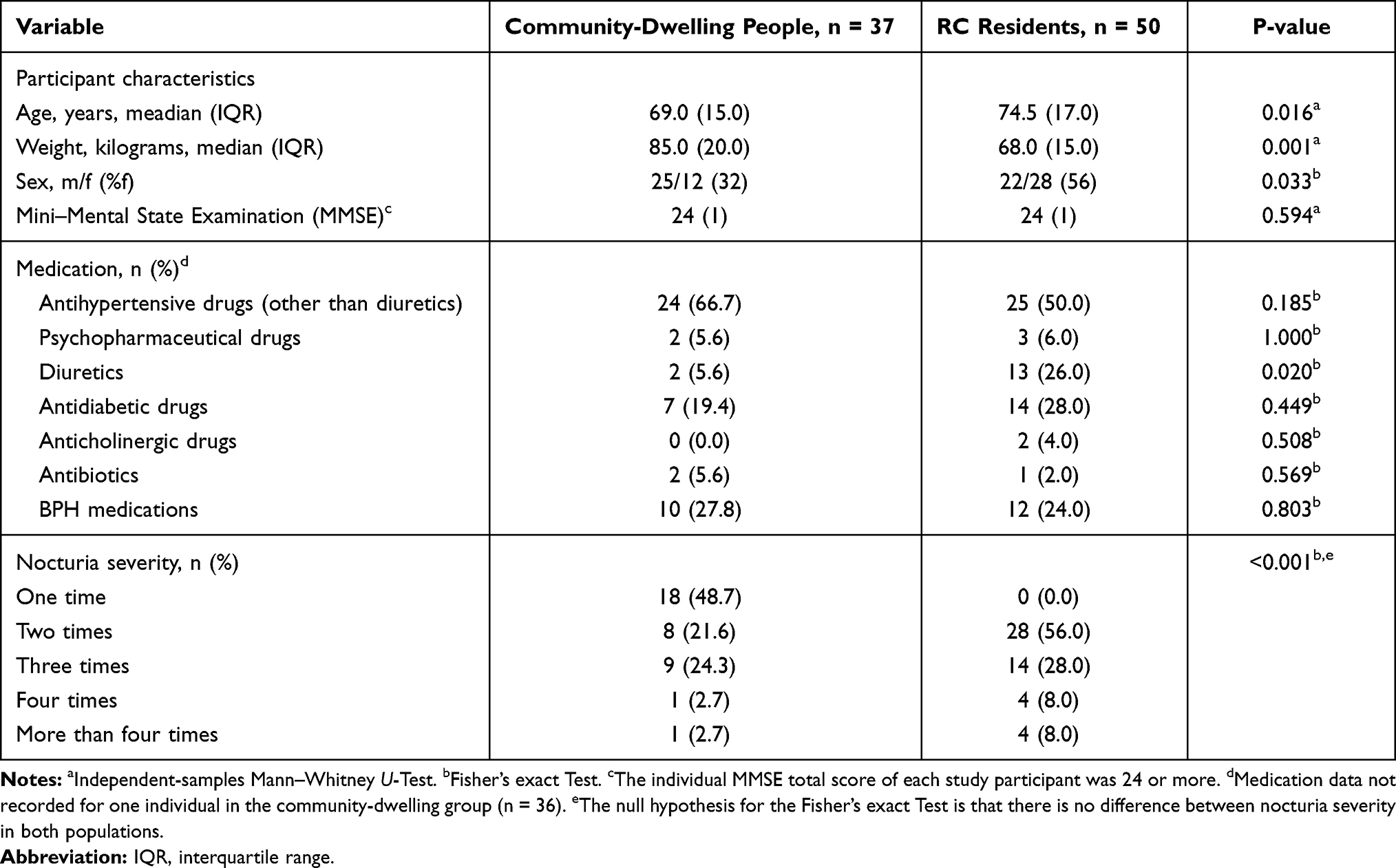 |
Table 1 Characteristics and Nocturia Severity of the Community-Dwelling People and Rehabilitation Centre (RC) Residents with Nocturia |
Evaluation of the Translation and Adjustment of Response Categories
The number of responses made by the community-dwelling group was adequate; only two items (Q13 and Q19) had three missing values each (8.1%). This represents answers from four of the participants. The vast majority of community-dwellers (89.2%) responded to all items. Almost all the questionnaire items elicited a “true” or “false” response, only four items were registered as “DK/NA” (representing two participants). Overall, 4% of men were unaware whether they had benign prostate hyperplasia (BPH) (Table 2). “DK/NA” answer choice frequency indicates that 94.6% of community dwellers could answer every question with either a “true” or “false” response (Supplementary File 1). Cronbach’s alpha coefficient was 0.776 in community-dwelling people. The correlation between TANGO-Gr items and community dweller medication list varied from poor for diuretic drugs (Kappa 0.11), to moderate for hypertensive drugs (Kappa 0.57) and almost perfect for antidiabetic drugs (Kappa 0.92) (Supplementary File 2).
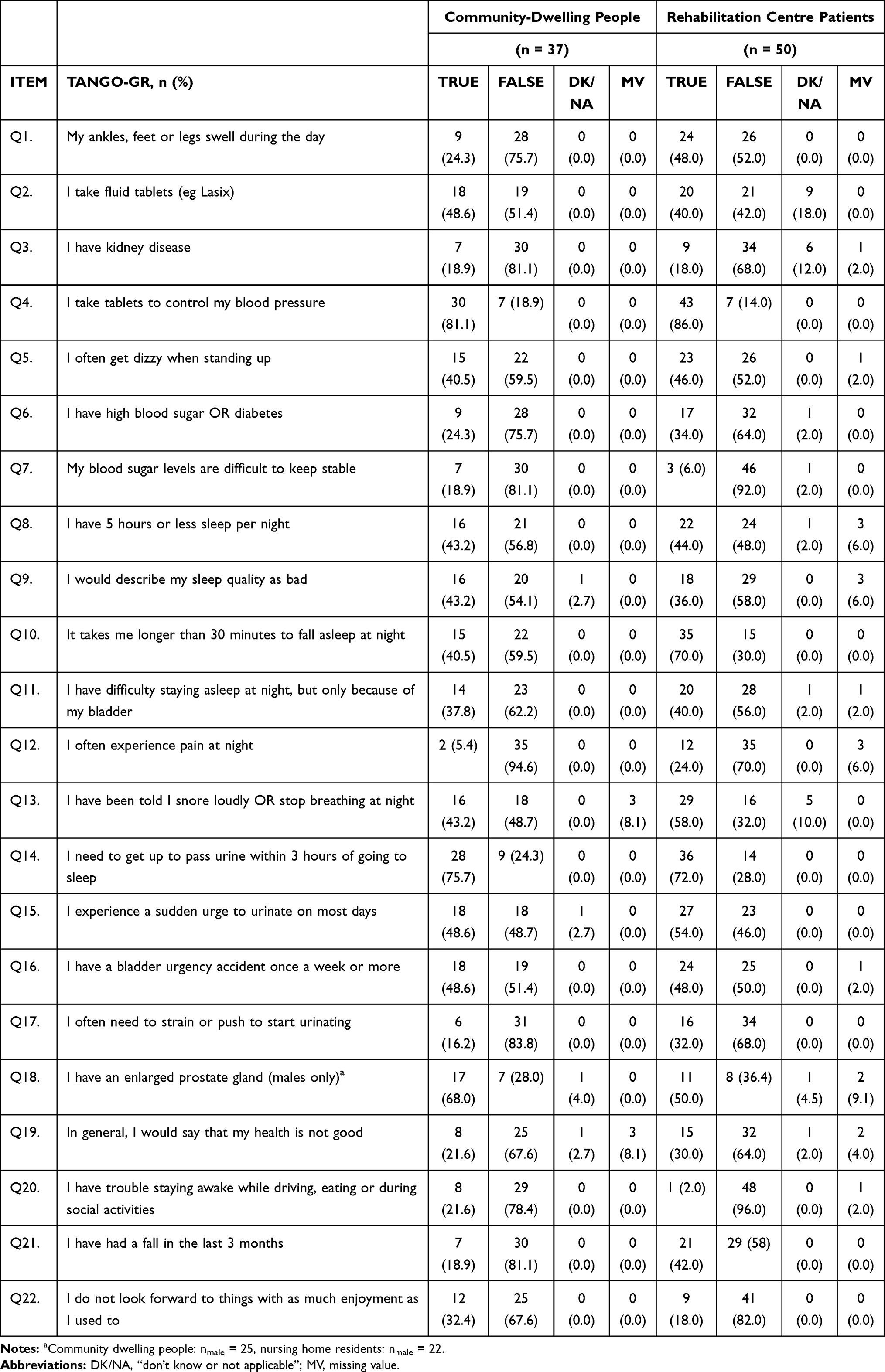 |
Table 2 Scores on TANGO-GR in Community-Dwelling People and Rehabilitation Centre Patients with Nocturia |
Rehabilitation Center Residents
Among the RC residents, significantly more items had missing answers compared to community dwellers (10 vs 2) (Table 2). This represents the responses of 14 participants. The majority of RC residents responded to all items (72%). The number of participants with missing answers did not differ significantly between groups (14/50 vs 4/37). “True” and “false” responses were found on all items. Nine RC residents had “DK/NA” answers compared to four community dwellers (Table 2), representing the answers of 21 participants. The number of participants with “DK/NA” answers was significantly higher in the RC residents group (21/50 vs 2/37). Overall, 4.5% of men were unaware that they had BPH (Table 2). “DK/NA” answer choice frequency indicates that 58% of RC residents could answer every question with either a “true” or “false” response (Supplementary File 1). Cronbach’s alpha coefficient was 0.531 in rehabilitation centre residents. The correlation between TANGO-Gr items and RC resident medication list varied from poor for antihypertensive drugs (Kappa 0.12), to slight for diuretic drugs (Kappa 0.21) and moderate for antidiabetic drugs (Kappa 0.48) (Supplementary File 2).
Stability (Test–Retest Reliability)
The period of time between TANGO-Gr test and retest completion was one week in both groups.
Community-Dwelling People
The overall median Kappa was 0.88 [IQR: 0.79–0.94] and pooled Kappa was 0.83; demonstrating almost perfect agreement.16 Correlation on all items varied from substantial to almost perfect (Kappa 0.61–1.0). The items related to night sleep duration (Q8) and pain at night (Q12) were the exceptions, demonstrating slight agreement (Kappa 0.27 and 0.30, respectively). The test - retest reliabilities of TANGO-Gr items in the community dwelling group are presented in Supplementary File 3.
Rehabilitation Center Residents
The overall median Kappa was 0.91 [IQR: 0.84–1.00] and pooled Kappa was 0.87; demonstrating almost perfect agreement.16 Correlation on all items varied from substantial to almost perfect (Kappa 0.61–1.0). The item related to night sleep duration (Q8) was the exception, demonstrating moderate agreement (Kappa 0.51). The test–retest reliabilities of TANGO-Gr items in RC residents are presented in Supplementary File 4.
Discussion
TANGO is a self-administered screening tool designed to assist clinicians in identifying coexisting clinical issues in patients presenting with nocturia. The study’s primary outcome was to translate the TANGO questionnaire into the Greek language, validate the translation and establish test–retest reliability in community-dwelling individuals and RC residents (Supplementary File 5).
In the original version of TANGO, participants answered the items with a “yes” or “no” response. Drawing from modifications made when a Dutch version of TANGO was created and validated, the Greek version includes “false” and “DK/NA” as two additional choices.5 There are two schools of thought regarding “DK/NA” responses. The first regards DK/NA responses as equivalent to the most conservative response. If there is no option of a “DK/NA” answer, the individuals who do not know the answer to the question or are not aware of their health condition would be required to indicate an opinion. In that case, they would possibly choose the most convenient solution (non-attitude reporting). The second hypothesis assumes that DK/NA answers are middle responses. It is expected that a “DK/NA” answer only attracts individuals that do not know the correct response to the question or do not have an attitude on the topic. In that case, physicians should analyze them separately because they represent patients unaware of their disease status.19 The practice of converting DK/NA responses into “no” answers does not seem to be recommendable.19
There is a statistically significant difference between “DK/NA” answers elicited from community dwellers and RC residents in an item (Q2) concerning the use of diuretics. Diuretics are the second most commonly prescribed class of antihypertensive medication, and the “DK/NA” response cannot be associated with the quality of translation.20 Functional health literacy is markedly lower among older age groups even after adjusting for differences in contributing factors. Nevertheless, it is uncertain whether functional literacy declines with age or cognitive function deterioration.21 According to Baumeister, in 3.7–29.5% of “DK/NA” cases, the physicians regard the respective disease as the present situation. Concerning participants who responded with a “DK/NA” answer, the probability of a physician’s successful diagnosis was increased in cases of advanced age and a higher number of somatic co-morbidities.19 Diuretics, renal disease and snoring presented in RC resident patients justifies the inclusion of the additional options. In our study, 12% of RC residents answered “DK/NA” to items about renal disease while 10% indicated they were unaware of snoring. In developed countries, diabetes and hypertension usually attribute to chronic kidney disease (CKD). However, less than 5% of patients with early CKD report awareness of their disease.22 A prevalence study of “DK” answers to questions related to snoring awareness indicates a comparable prevalence of 5–44% in older populations.23 5.7% of community dwellers and 40% of RC residents gave at least one “DK/NA” response. Furthermore, a “DK/NA” answer can serve as an invitation to discuss the point with the physician. Overall, these findings suggest that the inclusion of “DK/NA” choice in TANGO-Gr seems to reduce misclassification bias and allow better identification of clinically relevant variables, be they the present issue, entirely absent or requiring further investigation.
In test–retest evaluation in the community-dwellers’ group, the overall median Kappa was 0.88 and pooled Kappa was 0.83, demonstrating almost perfect agreement. This is in agreement with the paper of Decalf et al where the overall median Kappa was 0.75, demonstrating substantial test–retest reliability.5 In nursing home residents there was a moderate score for test–retest reliability (median Kappa 0.54).5 In our paper, the RC residents exhibited an overall median Kappa 0.91 and a pooled Kappa 0.87, demonstrating almost perfect agreement. In the evaluation of original TANGO Questionnaire in a single group of 40 patients a substantial to perfect agreement (Kappa 0.61–1.0) was demonstrated on 17 of the 22 items. An additional four items returned with moderate levels of agreement.4 In the paper of Culha et al there was a single group of 124 patients presenting a total Kappa value of 0.715 (individual item score weighted kappa coefficients, 0.696–0.731).6
There is a strong correlation between nocturia and the nocturia index in men seeking LUTS treatment or in community-dwellers with or without LUTS. It has been supposed that the severity of nocturia correlates poorly with maximum bladder storage during the night but moderately corresponds with nocturnal polyuria.24 Currently, nocturnal polyuria is classified as >33% of total 24-hour urine production occurring overnight in individuals more than 65 years of age.25 The TANGO Questionnaire and bladder diary create a valuable arrangement, allowing office urologists to identify causative pathways other than LUTS contributing to nocturia. Such essential factors have been categorized into global polyuria (eg diabetes or polydipsia) or nocturnal polyuria (eg congestive cardiac failure, sleep apnea, and peripheral edema). Of the causes of nocturia correlated to a decreased night time bladder capacity proposed by Weiss, TANGO comprises all excluding calculi and prostate hyperplasia.26
Urologists are familiar with the LUTS, especially with benign prostatic hyperplasia and overactive bladder. According to previous data, the median time up to 3 hours for the first nocturia episode recognized a statistically significant relationship between this period and the severity of nocturia.3,24 TANGO offers additional help, including the item “I need to get up to pass urine within three hours of going to sleep,” indicating a possible discrepancy between urine production and functional bladder capacity.
Understanding nocturia’s aetiology reflects a more effective treatment that efficiently decreases nocturnal voiding frequency and improves the overall health-related quality of life. Although the TANGO questionnaire does not ensure a complete symptom resolution, it permits a more comprehensive nocturia evaluation and management approach. Several recent developments in pharmacotherapy for nocturnal polyuria create the prospective to remodel treatment and improve the standard of care for patients suffering from nocturia.27
There are additional factors that influence sleep quality, especially for nursing home (NH) residents. Aspects that disturbed the residents’ sleep three or more times a week were, apart from nocturia, environment-related noise or light, pain, feeling too hot and leg cramps.28 Unfortunately, there has been no further evaluation of a possible relationship between these factors. A previous reliability study of TANGO in RC patients likewise revealed that environmental factors affect self-reported sleep quality.4 The TANGO questionnaire does not include an independent domain regarding the special situations regarding NH or RC, which should be considered a drawback. Another limitation of the study is that community-dwellers and RC residents did not complete a 3-day bladder diary and a continence nurse assessed nocturia with a single question. However, Culha et al described the same methodology in validating TANGO questionnaire in the Turkish language.6 Finally, a possible limitation is that patients and community-dwellers were not evaluated with the translated questionnaire after the prescribed nocturia management.
To summarize, we were able to successfully translate the original English version of TANGO, thereby creating and later validating TANGO-Gr. As a reliable, self-administered screening tool for clinical practice, it will greatly assist urologists in their diagnosis and treatment of patients suffering from nocturia. Furthermore, it offers an important starting-point for further consultation concerning co-existing issues. We also found that additional studies may target specific environment-related variables that can contribute to nocturia in the RC population.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hashim H, Blanker MH, Drake MJ, et al. International Continence Society (ICS) report on the terminology for nocturia and nocturnal lower urinary tract function. Neurourol Urodyn. 2019;38:499–508. doi:10.1002/nau.23917
2. Lee KC, Weiss J. Etiology, pathophysiology, and risk factors, chapter 2. In: Lee KC, Weiss J, editors. Nocturia: Etiology, Pathology, Risk Factors, Treatment and Emerging Therapies. London, UK: Academic Press; 2019:9–21.
3. Bower WF, Rose GE, Ervin CF, Goldin J, Whishaw DM, Khan F. TANGO - a screening tool to identify comorbidities on the causal pathway of nocturia. BJU Int. 2017;119(6):933–941. doi:10.1111/bju.13774
4. Rose GE, Bower WF, Ervin CF, Whishaw D, Khan F. Reliability testing of the TANGO short-form nocturia screening tool. Aust N Z Continence J. 2017;23(3):68–74.
5. Decalf V, Everaert K, De Witte N, Petrovic M, Bower W. Dutch version of the TANGO nocturia screening tool: cross-culturally translation and reliability study in community-dwelling people and nursing home residents. Acta Clin Belg. 2019. doi:10.1080/17843286.2019.1653511
6. Culha MG, Culha Y, Buyukyilmaz F, Turan N, Bower W. ‘TANGO” nocturia scaning tool: turkish validity and reliability study. Low Urin Tract Symptoms. 2021;13:88–92. doi:10.1111/luts.12336
7. Altaweel W, Alrumayyan M, Seyam R. Arabic language validation of TANGO questionnaire for nocturia: a translation into the Arabian Peninsula dialect. Neurourol Urodyn. 2020;39(8):2146–2152. doi:10.1002/nau.24412
8. Sperber AD. Translation and validation of study instruments for cross-cultural research. Gastroenterology. 2004;126(Suppl 1):S124–S128. doi:10.1053/j.gastro.2003.10.016
9. Wallace M, Shelkey M; Hartford institute for geriatric nursing. Katz index of independence in activities of daily living (ADL). Urol Nurs. 2007;27(1):93–94.
10. Devenney E, Hodges JR. The Mini-Mental State Examination: pitfalls and limitations. Pract Neurol. 2017;17:79–80. doi:10.1136/practneurol-2016-001520
11. Bujang MA, Baharum N. Guidelines of the minimum sample size requirements for Cohen’s Kappa. Epidemiol Biostat Public Health. 2017;14(2):
12. Roth PL. Missing data: a conceptual review for applied psychologists. Personnel Psychol. 1994;47:537–560. doi:10.1111/j.1744-6570.1994.tb01736.x
13. Ware JEJ, Gandek B. Methods for testing data quality, scaling assumptions and reliability: the IQOLA project approach. International quality of life assessment. J Clin Epidemiol. 1998;51:945–952. doi:10.1016/S0895-4356(98)00085-7
14. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33:159–174. doi:10.2307/2529310
15. Sim J, Wright CC. The kappa statistic in reliability studies: use, interpretation, and sample size requirements. Phys Ther. 2005;85(3):257–268. doi:10.1093/ptj/85.3.257
16. De Vries H, Elliott MN, Kanouse DE, Teleki SS. Using pooled kappa to summarize interrater agreement across many items. Field Methods. 2008;20:272–282. doi:10.1177/1525822X08317166
17. Nurjannah I, Siwi SM. Guidelines for analysis on measuring interrater reliability of nursing outcome classification. Int J Res Med Sci. 2017;5(4):1169–1175. doi:10.18203/2320-6012.ijrms20171220
18. Tooth LR, Ottenbacher KJ. The kappa statistic in rehabilitation research: an examination. Arch Phys Med Rehabil. 2004;85(8):1371–1376. doi:10.1016/j.apmr.2003.12.002
19. Baumeister H. “Don’t know” answers concerning somatic disease status should not be regarded as “no” responses. Ger Med Sci. 2008;6:Doc03.
20. Roush GC, Sica DA. Diuretics for hypertension: a review and update. Am J Hypertens. 2016;29(10):1130–1137. doi:10.1093/ajh/hpw030
21. Baker DW, Gazmararian JA, Sudano J, Patterson M. The association between age and health literacy among elderly persons. J Gerontol B Psychol Sci Soc Sci. 2000;55(6):S368–S374. doi:10.1093/geronb/55.6.S368
22. Chen TK, Knicely DH, Grams ME. Chronic kidney disease diagnosis and management: a review. JAMA. 2019;322(13):1294–1304. doi:10.1001/jama.2019.14745
23. Bliwise DL, Swan GE, Carmelli D, La Rue A. Correlates of the ‘don’t know’ response to questions about snoring. Am J Respir Crit Care Med. 1999;160(6):1812–1815. doi:10.1164/ajrccm.160.6.9807082
24. Avulova S, Blanker MH, van Doorn B, et al. Determinants of nocturia severity in men, derived from frequency-volume charts. Scand J Urol. 2015;49(2):185–188. doi:10.3109/21681805.2014.973901
25. Bliwise DL, Holm-Larsen T, Goble S, Nørgaard JP. Short time to first void is associated with lower whole-night sleep quality in nocturia patients. J Clin Sleep Med. 2015;11:53–55. doi:10.5664/jcsm.4364
26. Weiss JP. Nocturia:”do the math”. J Urol. 2006;175:S16–8. doi:10.1016/S0022-5347(05)00312-5
27. Monaghan T, Weiss J, Everaert K, Wein A. Pharmacologic management of nocturnal polyuria: a contemporary assessment of efficacy, safety, and progress toward individualized treatment. Ther Adv Urol. 2021;13:1–22. doi:10.1177/1756287220988438
28. Gentili A, Weiner DK, Kuchibhatil M, Edinger JD. Factors that disturb sleep in nursing home residents. Aging Clin Exp Res. 1997;9:207–213. doi:10.1007/BF03340151
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.